
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Endocrinol. , 26 April 2017
Sec. Thyroid Endocrinology
Volume 8 - 2017 | https://doi.org/10.3389/fendo.2017.00092
This article is part of the Research Topic The Association of Other Autoimmune Diseases in Patients with Thyroid Autoimmunity View all 19 articles
 Miriam Cellini
Miriam Cellini Maria Giulia Santaguida
Maria Giulia Santaguida Camilla Virili
Camilla Virili Silvia Capriello
Silvia Capriello Nunzia Brusca
Nunzia Brusca Lucilla Gargano
Lucilla Gargano Marco Centanni*
Marco Centanni*
The term “thyrogastric syndrome” defines the association between autoimmune thyroid disease and chronic autoimmune gastritis (CAG), and it was first described in the early 1960s. More recently, this association has been included in polyglandular autoimmune syndrome type IIIb, in which autoimmune thyroiditis represents the pivotal disorder. Hashimoto’s thyroiditis (HT) is the most frequent autoimmune disease, and it has been reported to be associated with gastric disorders in 10–40% of patients while about 40% of patients with autoimmune gastritis also present HT. Some intriguing similarities have been described about the pathogenic mechanism of these two disorders, involving a complex interaction among genetic, embryological, immunologic, and environmental factors. CAG is characterized by a partial or total disappearance of parietal cells implying the impairment of both hydrochloric acid and intrinsic factor production. The clinical outcome of this gastric damage is the occurrence of a hypochlorhydric-dependent iron-deficient anemia, followed by pernicious anemia concomitant with the progression to a severe gastric atrophy. Malabsorption of levothyroxine may occur as well. We have briefly summarized in this minireview the most recent achievements on this peculiar association of diseases that, in the last years, have been increasingly diagnosed.
The thyrogastric syndrome was initially described in the early 1960s and initially characterized by the presence of thyroid autoantibodies in patients with pernicious anemia, the latter being used as synonymous for atrophic gastritis (1). More recently, the autoimmune gastritis has been better characterized classifying chronic atrophic gastritis, with or without the PA, based on the histological evaluation and the presence of serum parietal cell (PCA) and/or intrinsic factor (IFA) autoantibodies (2, 3). Based on these criteria, the association between autoimmune thyroid disorders and chronic autoimmune gastritis (CAG) has also been reassessed (4, 5) and nowadays is included in the adult form of polyglandular autoimmune syndrome (PAS), characterized by two or more endocrine and non-endocrine autoimmune disorders (6). In particular, Betterle and colleagues have proposed the inclusion of thyrogastric syndrome in the PAS Type 3b, in which Hashimoto’s thyroiditis (HT) occurs also associated with non-endocrine autoimmune gastrointestinal disorders and where it plays a pivotal role (7, 8). This is in keeping with the evidence that chronic autoimmune thyroiditis represents the more prevalent autoimmune disorder worldwide making the frequency of thyrogastric syndrome quite high (4). This notion is supported by the high percentage (12–40%) of positivity of PCA in adult patients with HT (9) which, in turn, is present in approximately 40% of patients with atrophic gastritis (10). Besides the fact that the thyroid and the stomach share some embryological and biochemical features (11), some intriguing similarities have been observed even in the putative pathogenic mechanisms, which characterize the thyrogastric syndrome (12). Furthermore, some specific clinical features characterize or lead to the suspicion of the coexistence of both thyroid and gastric autoimmune (13, 14) disorders. These similar peculiar features will be briefly described in this minireview.
The thyroid gland and stomach, despite the different localization and function, share some similar morphologic and functional characteristics, likely due to their common embryologic origin (11). In fact, the thyroid gland develops from the primitive gut and therefore thyroid follicular share with parietal cells the same endodermal origin. Also, both these cells are polarized and are characterized by the presence of apical microvilli housing enzymatic activities.
Furthermore, gastric mucosal and thyroid follicular cells both show the ability to concentrate and transport iodine across the cell membrane (15). This process is mediated by the Na+/I− symporter (15) and involves similar enzymes with an efficient peroxidase activity (12) (Table 1). Furthermore, besides its essential role for the synthesis of thyroid hormones, iodine regulates the proliferation of gastric mucosal cells (16). In fact, in the presence of gastric peroxidase, iodine acts as an electron donor and participates in the removal of free oxygen radicals, thus playing an antioxidant action (17). These effects may explain the regulatory role of iodine in the proliferation of mucosal cells and its protective role against gastric carcinogenesis (11, 16). This hypothesis has been confirmed by the reported link among iodine deficiency, goiter, and increased risk of developing gastric cancer (18).
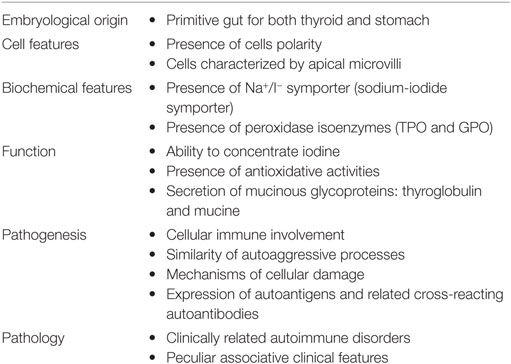
Table 1. Shared characteristics between thyroid and stomach.
Chronic lymphocytic thyroiditis is the most frequent autoimmune disorder and represents the prototype of organ-specific autoimmunity (19). Its prevalence, despite some difference of sex, age, race, and iodine intake, reaches about 5% in the general population (20). Much less frequent is the chronic autoimmune atrophic gastritis (type A gastritis or body/fundus gastritis), which represents only some 5% of the whole spectrum of chronic gastritis and must be differentiated from the one associated with chronic Helicobacter pylori (Hp) infection (type B gastritis or antral gastritis) (21, 22). HT is characterized by diffuse inflammatory changes with lymphocytic infiltration of the thyroid gland, leading to the destruction of the thyroid epithelial cells with subsequent fibrosis (23). Similarly, autoimmune gastritis is a chronic inflammatory disease involving gastric body and fundus, with the progressive reduction and/or disappearance of the native gastric glands that are sometimes replaced by intestinal or pyloric epithelium (metaplasia) (3). The natural history of HT is the progressive reduction of thyroid function till overt hypothyroidism (24) with a rate of progression of 2–4% per year (23), while that of gastric atrophy features the progressive reduction, till disappearance, of parietal cells, leading to reduced or absent acid production (3, 22). These alterations interfere with absorption of essential nutrients leading, at first, to iron-deficient anemia, followed by PA if the self-injurious process involves the IFA (13). Increased risk of developing neuroendocrine tumors and gastric adenocarcinoma is also associated with the severity of damage of gastric mucosa (22).
Both these autoimmune disorders are characterized by a complex interaction between genetic susceptibility and environmental factors that results in the loss of immune tolerance to self-antigens and in the development of autoimmune diseases. The loss of immune tolerance may involve alteration both in the central tolerance with reactive T cells escaped from intrathymic deletion and in the peripheral tolerance as in the case of defective T regulatory lymphocytes (25, 26). Genetic susceptibility has been confirmed for both diseases since their incidence is higher among identical twins and first-degree relatives as well as their presence may be observed in association with further autoimmune disorders (6, 7, 20, 26). Both of these disorders show a definite association with different HLA aplotypes; in HT, it has also been proven that the involvement of many other immunoregulatory genes (27), while this issue has not been elucidated in the pathogenesis of human autoimmune gastritis (26).
Several environmental factors seem to be involved in the pathogenesis of HT (excessive iodine intake, selenium deficiency, and specific drugs use), while very weak evidence supports a role for infectious agents as trigger for this disease (hepatitis C virus, HHV-6, and Yersinia) (27). The role of environmental factors in triggering autoimmune gastritis has been more studied and a stronger link between H. pylori infection and CAG has been detected, despite not sufficient to establish a causative relationship between these two diseases (21). H. pylori infection affects approximately 50% of the world population and is in turn the most common cause of chronic gastritis. At first, the H. pylori infection involves the gastric antrum, but in some patients it may extend into the gastric body (pangastritis) and, in genetically predisposed individuals, it may be a trigger for autoimmune atrophic gastritis, being this hypothesis still debated (3, 28, 29). The pathogenic link may be found in a cross-reactivity mechanism (molecular mimicry) (30): in fact, the Hp infection may induce the proliferation of CD4+ T lymphocytes that recognize epitopes of H. pylori structurally similar to those of H+/K+ATPase, an enzyme found on the apical membrane of parietal cells (31). Indeed, dendritic cells may present these shared epitopes to naïve T cells and, in the absence of peripheral tolerance, a Th1-driven autoreactive clone is activated (28). Again, the cellular immune mechanisms of autoimmune thyroiditis show some similarities with those of CAG. In HT, inflammation leads to secretion of IFN-γ, a cytokine turning thyrocytes into antigen-presenting cells (32). The variation of costimulatory factors that drive the binding between an autoantigen and the T-cell receptor allows the proliferation and polarization of autoreactive effector lymphocytes (27). Due to a Th17 cell polarization, the inflammatory process and the subsequent fibrosis seem to prevail in the early phase of thyroiditis (33); in a later phase, when the lymphocytic infiltration and the parenchymal destruction are prevalent, a polarized Th1 profile has been reported (34, 35). The Th1 lymphocytes are able to aid cytotoxic T-lymphocytes and to produce specific cytokines (TNF-α and IFN-γ) able to induce the cellular apoptosis (35) in thyroid cells. The association of a gastric autoimmune disorder has been shown to add a Th2 cytokine profile to the described ones (36). The precise mechanism leading to thyrocytes and/or parietal cell death is still unknown. However, the involvement of Fas upregulation in thyrocytes, due to IL-1beta produced by activated macrophages, has been proven (37). Normal thyrocytes, in fact, express FasL but not Fas, while their concomitant expression induces an autocrine interaction that may represent the main mechanism inducing apoptosis (37). In experimental autoimmune gastritis, also parietal cells express Fas that, in this case, could trigger apoptosis by binding Fas-ligand on infiltrating T cells (28). Following cells damage, the production of specific autoantibodies ensues in epiphenomenal fashion (34). Cellular and humoral immune cooperation characterizes both autoimmune thyroiditis and gastritis leading to the production of specific autoantibodies (antithyroperoxidase, antithyroglobulin, and antiparietal cell antibodies). These autoantibodies are of paramount importance in the diagnosis but of little, if any, in the pathogenesis of these autoimmune disorders.
Clinical pathological aspects of this association are attributable to malabsorption of iron and thyroxine, both linked to a reduced gastric acid secretion.
Chronic atrophic gastritis is clinically silent in most cases and only a small percentage of patients may complain about dyspeptic symptoms. A well-described clinical feature of thyrogastric syndrome is represented by the presence of an iron-deficient and/or a PA. In fact, it has been demonstrated that an iron-deficient anemia, refractory to oral iron therapy, in patients with HT, may be due to chronic atrophic gastritis (13). The clinical signs of this disease appear after several years of its onset, when the progressive reduction to disappearance of the parietal cells leads to atrophy of the gastric mucosa, impairing the absorption of iron, vitamin B12 (cobalamin), folate, and other nutrients (22). At the physiologic acid pH (1.5–2) of the stomach, ascorbic acid, the most active form of vitamin C, allows iron reduction from the nutritional ferric (Fe +++) to the ferrous form (Fe ++), thus forming a complex that drives the absorption in the upper portion of the small intestine (22). In the initial phase of the atrophic gastritis, the damage of parietal cells can lead to iron deficiency microcytic anemia as the only clinical sign (38). When the gastric atrophy becomes severe and/or the IFA is no longer produced, even the absorption of cobalamin becomes compromised. Besides hydrochloric acid that promotes the separation of vitamin B12 from food, the parietal cells also produce the IFA that binds cobalamin and pipes it to the distal ileum, where it is absorbed following a binding to specific receptors (39). Vitamin B12 deficiency is responsible for hematologic changes (macrocytic anemia) and specific neurological disorders (paresthesia and neuritis) which are peculiar of PA (22).
The worldwide used pharmaceutical form of thyroxine (sodium levothyroxine, T4) is obtained by native hormone through its salification with sodium hydroxide. The absorption of T4 occurs in all sections of small intestine being anyway incomplete and ranging from 62 to 82% of the ingested dose (40). However, increasing evidence of a relevant role of the intact gastric acid secretion on the subsequent intestinal absorption of sodium levothyroxine has been reported in the last years (41). In fact, an increased therapeutic T4 dose has been described in patients with gastric disorders (Hp infection, chronic gastritis, gastric atrophy) or chronically treated with proton pump inhibitors or in non-fasting patients (41–43). All these conditions are characterized by a modified gastric pH that may affect T4 absorption by changing the ionization status, as already described for iron, or the dissolution process of the pharmaceutical T4 form. Furthermore, in vitro studies have shown the pH dependency of the dissolution profile of different T4 preparations (44). This evidence boosted the research for novel thyroxine formulations as liquid or softgel capsules. These ones showed, as compared to the classic tablet formulation, a similar or better bioavailability as well as a lower number of excipients (45, 46). In clinical studies, softgel or liquid formulations performed better in patients with gastric disorders (47, 48) and in proton pump inhibitors users (49, 50).
In conclusion, the association of thyroid and gastric autoimmune disorders represents a frequent syndrome, included in the autoimmune polyendocrine syndrome. The similar or even common biochemical and pathogenic features fully support the term thyrogastric disease described some 60 years ago. From a clinical standpoint, the presence of iron-deficient anemia and thyroxine malabsorption may represent an alert signal for the presence of a gastric disorder in patients with thyroid autoimmunity and should trigger a specific diagnostic workup.
All authors listed have made substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Doniach D, Roitt IM, Taylor KB. Autoimmune phenomena in pernicious anaemia. Serological overlap with thyroiditis, thyrotoxicosis, and systemic lupus erythematosus. Br Med J (1963) 1:1374–9. doi: 10.1136/bmj.1.5342.1374
2. Sipponen P, Maaroos HI. Chronic gastritis. Scand J Gastroenterol (2015) 50:657–67. doi:10.3109/00365521.2015.1019918
3. Neumann WL, Coss E, Rugge M, Genta RM. Autoimmune atrophic gastritis – pathogenesis, pathology and management. Nat Rev Gastroenterol Hepatol (2013) 10:529–41. doi:10.1038/nrgastro.2013.101
4. Centanni M, Marignani M, Gargano L, Corleto VD, Casini A, Delle Fave G, et al. Atrophic body gastritis in patients with autoimmune thyroid disease: an underdiagnosed association. Arch Intern Med (1999) 159:1726–30. doi:10.1001/archinte.159.15.1726
5. Lahner E, Intraligi M, Buscema M, Centanni M, Vannella L, Grossi E, et al. Artificial neural networks in the recognition of the presence of thyroid disease in patients with atrophic body gastritis. World J Gastroenterol (2008) 14:563–8. doi:10.3748/wjg.14.563
6. Kahaly GJ. Polyglandular autoimmune syndromes. Eur J Endocrinol (2009) 161:11–20. doi:10.1530/EJE-09-0044
7. Betterle C, Dal Pra C, Mantero F, Zanchetta R. Autoimmune adrenal insufficiency and autoimmune polyendocrine syndromes: autoantibodies, autoantigens, and their applicability in diagnosis and disease prediction. Endocr Rev (2002) 23:327–64. doi:10.1210/edrv.23.3.0466
8. Fallahi P, Ferrari SM, Ruffilli I, Elia G, Biricotti M, Vita R, et al. The association of other autoimmune diseases in patients with autoimmune thyroiditis: review of the literature and report of a large series of patients. Autoimmun Rev (2016) 15:1125–8. doi:10.1016/j.autrev.2016.09.009
9. Checchi S, Montanaro A, Ciuoli C, Brusco L, Pasqui L, Fioravanti C, et al. Prevalence of parietal cell antibodies in a large cohort of patients with autoimmune thyroiditis. Thyroid (2010) 20:1385–9. doi:10.1089/thy.2010.0041
10. Lahner E, Centanni M, Agnello G, Gargano L, Vannella L, Iannoni C, et al. Occurrence and risk factors for autoimmune thyroid disease in patients with atrophic body gastritis. Am J Med (2008) 121:136–41. doi:10.1016/j.amjmed.2007.09.025
11. Gołkowski F, Szybiński Z, Rachtan J, Sokołowski A, Buziak-Bereza M, Trofimiuk M, et al. Iodine prophylaxis – the protective factor against stomach cancer in iodine deficient areas. Eur J Nutr (2007) 46:251–6. doi:10.1007/s00394-007-0657-8
12. Kandemir EG, Yonem A, Narin Y. Gastric carcinoma and thyroid status. J Int Med Res (2005) 33:222–7. doi:10.1177/147323000503300210
13. Sibilla R, Santaguida MG, Virili C, Gargano L, Nardo S, Della Guardia M, et al. Chronic unexplained anemia in isolated autoimmune thyroid disease or associated with autoimmune related disorders. Clin Endocrinol (Oxf) (2008) 68:640–5. doi:10.1111/j.1365-2265.2007.03091.x
14. Centanni M. Thyroxine treatment: absorption, malabsorption, and novel therapeutic approaches. Endocrine (2013) 43:8–9. doi:10.1007/s12020-012-9814-9
15. Portulano C, Paroder-Belenitsky M, Carrasco N. The Na+/I- symporter (NIS): mechanism and medical impact. Endocr Rev (2014) 35:106–49. doi:10.1210/er.2012-1036
16. Venturi S, Donati FM, Venturi A, Venturi M, Grossi L, Guidi A. Role of iodine in evolution and carcinogenesis of thyroid, breast and stomach. Adv Clin Path (2000) 4:11–7.
17. Das D, De PK, Banerjee RK. Thiocyanate, a plausible physiological electron donor of gastric peroxidase. Biochem J (1995) 305:59–64. doi:10.1042/bj3050059
18. Tabaeizadeh M, Haghpanah V, Keshtkar A, Semnani S, Roshandel G, Adabi K, et al. Goiter frequency is more strongly associated with gastric adenocarcinoma than urine iodine level. J Gastric Cancer (2013) 13:106–10. doi:10.5230/jgc.2013.13.2.106
19. Caturegli P, De Remigis A, Rose NR. Hashimoto thyroiditis: clinical and diagnostic criteria. Autoimmun Rev (2014) 13:391–7. doi:10.1016/j.autrev.2014.01.007
20. Antonelli A, Ferrari SM, Corrado A, Di Domenicantonio A, Fallahi P. Autoimmune thyroid disorders. Autoimmun Rev (2015) 14:174–80. doi:10.1016/j.autrev.2014.10.016
21. Venerito M, Radünz M, Reschke K, Reinhold D, Frauenschläger K, Jechorek D, et al. Autoimmune gastritis in autoimmune thyroid disease. Aliment Pharmacol Ther (2015) 41:686–93. doi:10.1111/apt.13097
22. Toh BH. Diagnosis and classification of autoimmune gastritis. Autoimmun Rev (2014) 13:459–62. doi:10.1016/j.autrev.2014.01.048
23. Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med (2003) 348:2646–55. doi:10.1056/NEJMra021194
24. Effraimidis G, Wiersinga WM. Mechanisms in endocrinology: autoimmune thyroid disease: old and new players. Eur J Endocrinol (2014) 170:R241–52. doi:10.1530/EJE-14-0047
25. Kristensen B. Regulatory B and T cell responses in patients with autoimmune thyroid disease and healthy controls. Dan Med J (2016) 63:B5177.
26. Toh BH, Chan J, Kyaw T, Alderuccio F. Cutting edge issues in autoimmune gastritis. Clin Rev Allergy Immunol (2012) 42:269–78. doi:10.1007/s12016-010-8218-y
27. Ajjan RA, Weetman AP. The pathogenesis of Hashimoto’s thyroiditis: further developments in our understanding. Horm Metab Res (2015) 47:702–10. doi:10.1055/s-0035-1548832
28. Varbanova M, Frauenschläger K, Malfertheiner P. Chronic gastritis – an update. Best Pract Res Clin Gastroenterol (2014) 28:1031–42. doi:10.1016/j.bpg.2014.10.005
29. Smyk DS, Koutsoumpas AL, Mytilinaiou MG, Rigopoulou EI, Sakkas LI, Bogdanos DP. Helicobacter pylori and autoimmune disease: cause or bystander. World J Gastroenterol (2014) 20:613–29. doi:10.3748/wjg.v20.i3.613
30. Amedei A, Bergman MP, Appelmelk BJ, Azzurri A, Benagiano M, Tamburini C, et al. Molecular mimicry between Helicobacter pylori antigens and H+, K+ – adenosine triphosphatase in human gastric autoimmunity. J Exp Med (2003) 198:1147–56. doi:10.1084/jem.20030530
31. D’Elios MM, Bergman MP, Azzurri A, Amedei A, Benagiano M, De Pont JJ, et al. H+/K+-ATPase (proton pump) is the target autoantigen of Th1-type cytotoxic T cells in autoimmune gastritis. Gastroenterology (2001) 120:377–86. doi:10.1053/gast.2001.21187
32. Yu S, Sharp GC, Braley-Mullen H. Thyrocytes responding to IFN-gamma are essential for development of lymphocytic spontaneous autoimmune thyroiditis and inhibition of thyrocyte hyperplasia. J Immunol (2006) 176:1259–65. doi:10.4049/jimmunol.176.2.1259
33. Figueroa-Vega N, Alfonso-Pérez M, Benedicto I, Sánchez-Madrid F, González-Amaro R, Marazuela M. Increased circulating pro-inflammatory cytokines and Th17 lymphocytes in Hashimoto’s thyroiditis. J Clin Endocrinol Metab (2010) 95:953–62. doi:10.1210/jc.2009-1719
34. Weetman AP. Cellular immune responses in autoimmune thyroid disease. Clin Endocrinol (Oxf) (2004) 61:405–13. doi:10.1111/j.1365-2265.2004.02085.x
35. Li D, Cai W, Gu R, Zhang Y, Zhang H, Tang K, et al. Th17 cell plays a role in the pathogenesis of Hashimoto’s thyroiditis in patients. Clin Immunol (2013) 149:411–20. doi:10.1016/j.clim.2013.10.001
36. Santaguida MG, Nardo S, Del Duca SC, Lococo E, Virili C, Gargano L, et al. Increased interleukin-4-positive lymphocytes in patients with Hashimoto’s thyroiditis and concurrent non-endocrine autoimmune disorders. Clin Exp Immunol (2011) 165:148–54. doi:10.1111/j.1365-2249.2011.04419.x
37. De Maria R, Testi R. Fas-FasL interactions: a common pathogenetic mechanism in organ-specific autoimmunity. Immunol Today (1998) 19:121–5. doi:10.1016/S0167-5699(98)80010-8
38. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood (2006) 107:1673–9. doi:10.1182/blood-2005-09-3534
39. Toh BH, Alderuccio F. Pernicious anemia. Autoimmunity (2004) 37:357–61. doi:10.1080/08916930410001705439
40. Hays MT. Localization of human thyroxine absorption. Thyroid (1991) 1:241–8. doi:10.1089/thy.1991.1.241
41. Centanni M, Gargano L, Canettieri G, Viceconti N, Franchi A, Delle Fave G, et al. Thyroxine in goiter, Helicobacter pylori infection, and chronic gastritis. N Engl J Med (2006) 354:1787–95. doi:10.1056/NEJMoa043903
42. Lahner E, Virili C, Santaguida MG, Annibale B, Centanni M. Helicobacter pylori infection and drugs malabsorption. World J Gastroenterol (2014) 20:10331–7. doi:10.3748/wjg.v20.i30.10331
43. Bach-Huynh TG, Nayak B, Loh J, Soldin S, Jonklaas J. Timing of levothyroxine administration affects serum thyrotropin concentration. J Clin Endocrinol Metab (2009) 94:3905–12. doi:10.1210/jc.2009-0860
44. Pabla D, Akhlaghi F, Zia H. A comparative pH-dissolution profile study of selected commercial levothyroxine products using inductively coupled plasma mass spectrometry. Eur J Pharm Biopharm (2009) 72:105–10. doi:10.1016/j.ejpb.2008.10.008
45. Virili C, Trimboli P, Romanelli F, Centanni M. Liquid and softgel levothyroxine use in clinical practice: state of the art. Endocrine (2016) 54:3–14. doi:10.1007/s12020-016-1035-1
46. Vita R, Fallahi P, Antonelli A, Benvenga S. The administration of l-thyroxine as soft gel capsule or liquid solution. Expert Opin Drug Deliv (2014) 11:1103–11. doi:10.1517/17425247.2014.918101
47. Santaguida MG, Virili C, Del Duca SC, Cellini M, Gatto I, Brusca N, et al. Thyroxine softgel capsule in patients with gastric-related T4 malabsorption. Endocrine (2015) 49:51–7. doi:10.1517/17425247.2014.918101
48. Fallahi P, Ferrari SM, Ruffilli I, Antonelli A. Reversible normalisation of serum TSH levels in patients with autoimmune atrophic gastritis who received l-T4 in tablet form after switching to an oral liquid formulation: a case series. BMC Gastroenterol (2016) 24(16):22. doi:10.1186/s12876-016-0439-y
49. Vita R, Benvenga S. Tablet levothyroxine (l-T4) malabsorption induced by proton pump inhibitor; a problem that was solved by switching to l-T4 in soft gel capsule. Endocr Pract (2014) 20:e38–41. doi:10.4158/EP13316.CR
Keywords: thyroiditis, polyglandular autoimmune syndrome, thyroxine malabsorption, gastric atrophy, pernicious anemia, Helicobacter pylori infection, cellular immunity
Citation: Cellini M, Santaguida MG, Virili C, Capriello S, Brusca N, Gargano L and Centanni M (2017) Hashimoto’s Thyroiditis and Autoimmune Gastritis. Front. Endocrinol. 8:92. doi: 10.3389/fendo.2017.00092
Received: 13 March 2017; Accepted: 07 April 2017;
Published: 26 April 2017
Edited by:
Alessandro Antonelli, University of Pisa, ItalyCopyright: © 2017 Cellini, Santaguida, Virili, Capriello, Brusca, Gargano and Centanni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco Centanni, bWFyY28uY2VudGFubmlAdW5pcm9tYTEuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.