 Provia Ainembabazi1
Provia Ainembabazi1 Letisha Najjemba1Joseph Musaazi1
Letisha Najjemba1Joseph Musaazi1 Mario Hönemann2
Mario Hönemann2 Barbara Castelnuovo1†
Barbara Castelnuovo1† Amrei von Braun3*†
Amrei von Braun3*†- 1Infectious Diseases Institute, College of Health Sciences Makerere University, Kampala, Uganda
- 2Institute of Medical Microbiology and Virology, Leipzig University, Leipzig, Germany
- 3Division of Infectious Diseases and Tropical Medicine, Leipzig University Medical Centre, Leipzig, Germany
A cross-sectional study on severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) seroprevalence among unvaccinated people living with HIV (PLWH) was conducted in Kampala, Uganda, in 2022. Data collection was done using a structured questionnaire. SARS-CoV-2 serologies were done using the Roche Elecsys Anti-SARS-CoV-2 S immunoassay, which assesses the adaptive humoral immune response to the SARS-CoV-2 Spike protein. A total of 575 PLWH (female n=355, 61.7%) with a median age of 49 years (IQR 39-55) were included. SARS-CoV-2 seroprevalence was 93%. The majority had antibody concentration levels ≥ 250 U/ml (n=383, 66.6%). Participants aged >55 years were significantly more likely to have lower antibody concentrations compared to younger participants (p-value < 0.001). A high BMI (≥ 30 kg/m2) was significantly associated with higher antibody concentrations (p-value 0.001). Concerning COVID-19 history, a small proportion of participants (n=79, 13.6%) reported contact with a known COVID-19 patient. Only 8.1% (n=47) had ever had a nasopharyngeal swab for SARS-CoV-2 RT-PCR done, and 3.1% (n=18) actually had a laboratory-confirmed SARS-CoV-2 infection in the past. SARS-CoV-2 seroprevalence was high among our study population, which may be attributed to the fact that the study took place right after all restrictions were lifted and the population was exposed to the dominant Omicron variant. Interestingly, only a small proportion of infections had been laboratory-confirmed.
1 Introduction
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) causes the communicable respiratory coronavirus disease 2019 (COVID-19), which resulted in the death of over 7 million people worldwide since the start of the recent pandemic in March 2020 (1). The clinical course of COVID-19 is highly variable depending largely on host factors such as age, comorbidities, and preexisting immune status. Generally, people of older age, as well as people with underlying health conditions such as immunodeficiency, heart disease, and chronic obstructive pulmonary disease are at higher risk of severe courses of illness including death (2–4).
In people living with HIV (PLWH), the impact of SARS-CoV-2 infection on morbidity and mortality is not entirely clear and remains subject to further research (5). Some evidence suggests that PLWH are at higher risk of severe COVID-19 outcomes (6, 7). However, this may not be true for patients with sustained viral suppression and good immunological response on antiretroviral treatment (ART) in the absence of known risk factors for severe COVID-19 (8–11). Since the availability of effective SARS-CoV-2 vaccines, PLWH are included in the vaccine priority group by the World Health Organization’s (WHO) Strategic Advisory Group of Experts on Immunization (SAGE). The WHO particularly recommends that PLWH with advanced-stage HIV disease, low CD4 cell count, and co-morbidities be prioritized for COVID-19 vaccination (12).
In many low and middle-income countries (LMIC), vaccines against COVID-19 became available during the first half of 2021. In Uganda, the vaccination program started in a phased manner with the initial phase targeting selected high-risk groups such as healthcare workers, teachers, persons above the age of 50 years, as well as persons with comorbidities. However, widespread vaccine hesitancy resulted in low uptake of the recommended vaccinations even in high-risk populations (13, 14). By January 2022, vaccination coverage had reached less than one-fifth of the targeted population in Uganda. For clinicians in HIV care, knowing a patient’s SARS-CoV-2 serostatus at the time was of benefit to guide hesitant high-risk patients towards vaccination.
The aim of our study was to assess the seroprevalence of SARS-CoV-2 among unvaccinated PLWH in Kampala, Uganda, and to analyze factors potentially associated with the level of antibody concentrations in this population. Our assessment took place right after all preventive measures to curb the spread of SARS-CoV-2, including tight “lock-down” procedures, had been lifted by the Ugandan government and testing as well as vaccination were widely available. To the best of our knowledge, this is the first assessment of SARS-CoV-2 seroprevalence in PLWH from Uganda during the recent pandemic.
2 Methods
2.1 Study site
This study was conducted at the Infectious Diseases Institute (IDI) in Kampala, Uganda, which serves a population of over 8,000 PLWH. The clinic provides a range of outpatient services including routine HIV care and treatment, integrated TB-HIV services, sexual and reproductive health services, and others. During the recent COVID-19 pandemic, IDI served as a SARS-CoV-2 immunization center.
2.2 Eligibility criteria and study procedures
This cross-sectional study was conducted from January to September 2022. From 25 January 2022 to 10 June 2022, we recruited PLWH who were not vaccinated against SARS-CoV-2 and at high risk of a clinically severe course of COVID-19 (presence of comorbidities or aged > 50 years) with the ability to speak either English or Luganda and give written informed consent. Following an amendment, from 11 June 2022 onwards we expanded study eligibility to all non-vaccinated PLWH above the age of 18 years. Consecutive sampling was used to recruit participants from the IDI clinic. Thus, approached PLWH above the age of 18 years who confirmed non-vaccination status were screened for eligibility.
Data collection was done by a structured questionnaire designed in RedCap (version 10.0.25 - © 2023 Vanderbilt University). The sociodemographic and clinical characteristics of participants, including age, sex, and comorbidities, were collected. Furthermore, we assessed exposure to known COVID-19 cases, previous COVID-19 diagnosis, COVID-19 symptom history, and complications from COVID-19. Additional clinical information (ART regimen and duration, HIV viral load, HIV WHO stage, body mass index (BMI) values) were extracted from routinely collected data in the IDI clinic’s electronic database known as the Integrated Clinical Enterprise Application version 3.0.3.4 (15).
All study participants were evaluated for SARS-CoV-2 seropositivity. Serology testing was performed in serum separated from whole blood through centrifugation. Laboratory tests were done at the IDI Core Lab, which is a College of American Pathologists (CAP) accredited laboratory based in Kampala, Uganda, using the Elecsys Anti-SARS-CoV-2 S immunoassay and the Cobas e411 instrument (both Roche, Basel, Switzerland), which assess the adaptive humoral immune response to the SARS-CoV-2 Spike (S) protein.
Ethical approval was granted from the IDI Research Ethics Committee (IDIREC REF 038/2021) and Uganda National Council of Science and Technology (UNCST) (HS1956ES). Informed consent was obtained from all subjects involved in the study.
2.3 Data management and statistical analysis
Data was exported into Microsoft Excel and analysis was performed using R version 4.1.1 and the tidyverse package (16, 17). Participants were categorized as “high-risk” if they were 50 years old or above at enrolment and had at least one comorbidity. Participants’ characteristics were described using frequencies and percentages. SARS-CoV-2 antibody concentrations were considered negative at values below 0.8 according to the manufacturer (18). For the purpose of comparison, positive antibody concentration levels were grouped into the following categories: <2.5, 2.5 - 19, 20 - 149, 150 – 249, and ≥250 U/ml, based on the manufacturer´s sensitivity testing tables. Antibody concentration groups were summarized using medians and inter-quartile range (IQR), as well as frequencies and proportions, and were compared across participants’ characteristics using Pearson’s chi-square test. For multivariate analysis, we used an ordinal logistic regression model to examine adjusted associations between SARS-CoV-2 antibody concentration groups and participants’ characteristics. To explore the effect of high-risk groups, we fitted a separate model including high-risk as a covariate, however, we excluded age groups as they were highly collinear. The appropriateness of the assumption of proportional odds assumed by the ordinal logistic regression model was checked by using the Brant test. Statistical significance was assumed at a 5% level.
3 Results
3.1 Study participants
A total of 787 PLWH were screened for eligibility, of which 580 were enrolled in the study. Five participants were withdrawn from the study after enrolment as no blood sample was given. The final analysis included 575 study participants. All study participants were on ART with fully suppressed viral loads. Almost two-thirds (n=347, 60.3%) were classified as WHO stage 3 or 4 at the time of HIV diagnosis and recent CD4 cell counts were not available. A total of 79 participants (13.6%) reported that they had previous contact with a known patient with COVID-19. The majority of study participants (n=567, 99%) reported that they had at least one COVID-19-related symptom during the pandemic. The most common symptoms reported by participants were rhinorrhoea (n=524, 91%), cough (n=502, 87.3%), and sore throat (n=495, 86.1%). However, only 47 (8.1%) had a nasopharyngeal swab for SARS-CoV-2 RT-PCR done, and 18 (3.1%) actually had a laboratory-confirmed SARS-CoV-2 infection in the past. Study participants´ characteristics are shown in Table 1.
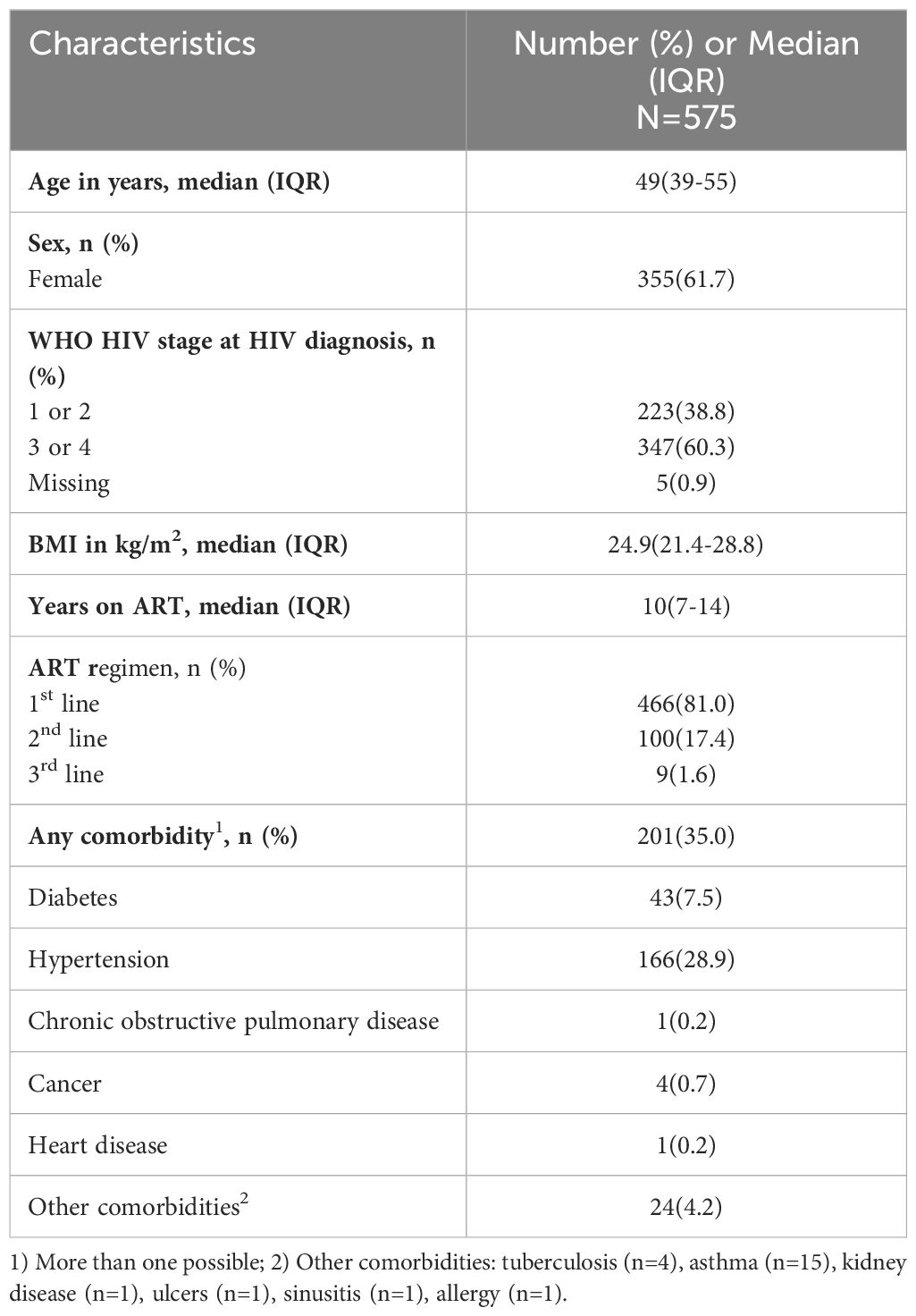
Table 1 Study participants´ characteristics.
3.2 SARS-CoV-2 seroprevalence
SARS-CoV-2 seroprevalence was 93% (n= 534) in our study population. The majority of participants had antibody concentration levels ≥ 250 U/ml (n=383, 66.6%). Twenty-one (3.7%) had levels 150 – 249 U/ml, 73 (12.7%) 20 – 149 U/ml, 46 (8%) 2.5 – 19 U/ml, and 12 (2.1%) had levels 0.8 - 2.4 U/ml. Fifty-one (8.9%) had levels <2.5 U/ml. Figure 1 shows the proportion of participants per antibody concentration level category for each month of recruitment. The proportion of participants with high concentration values increased from approximately 60% at the beginning of recruitment to 80% at the end of our study period. Furthermore, the proportion of participants with very low antibody concentration levels was smallest (3% of participants recruited during the month of September) at the end of the recruitment period.
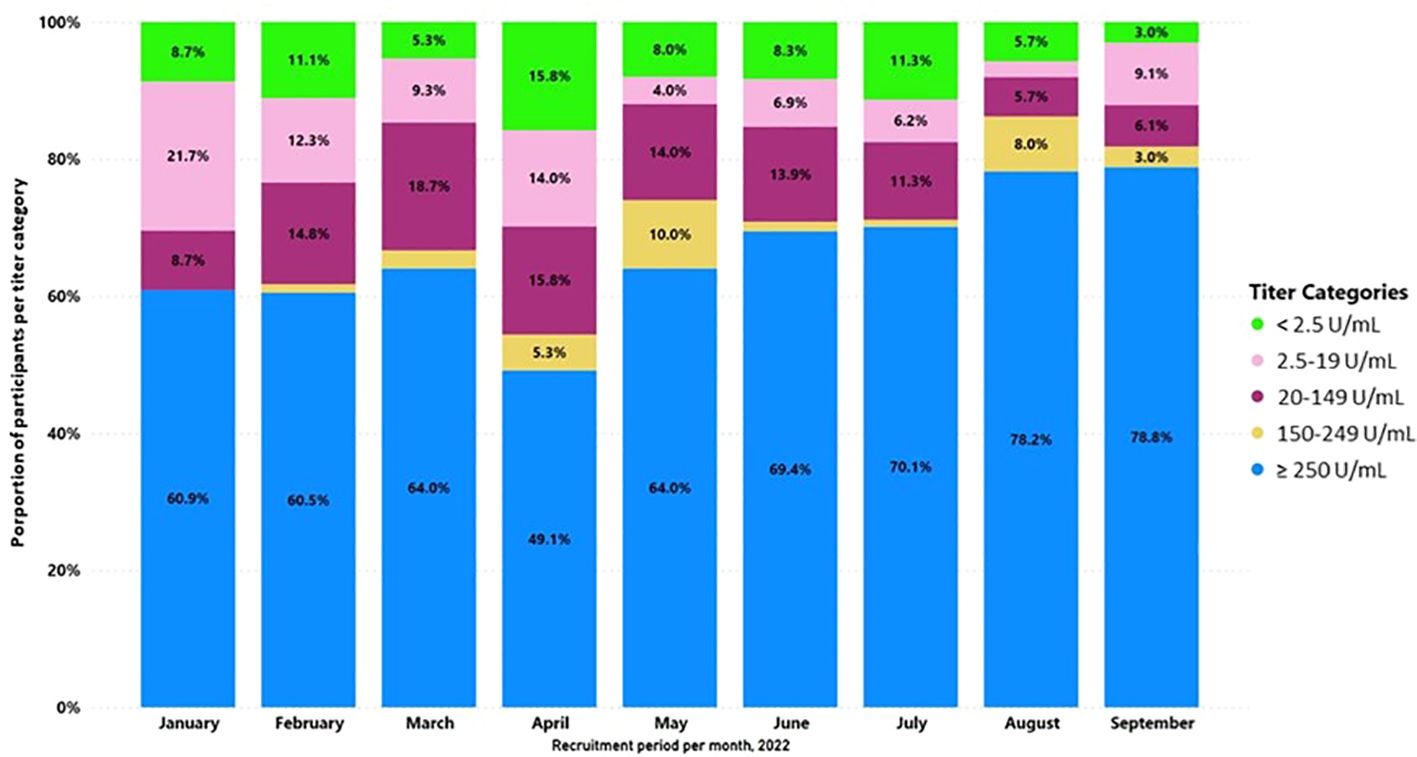
Figure 1 Proportion of participants per antibody concentration level category for each month of recruitment. Antibody concentration level categories by color.
As shown in Table 2, participants aged <50 years, those who had a high (≥ 30 kg/m2) BMI, those who received a first-line ART regimen, and those defined as non-high-risk had higher proportions in antibody concentration category ≥250 U/ml compared to their counterparts (p-value <0.05).
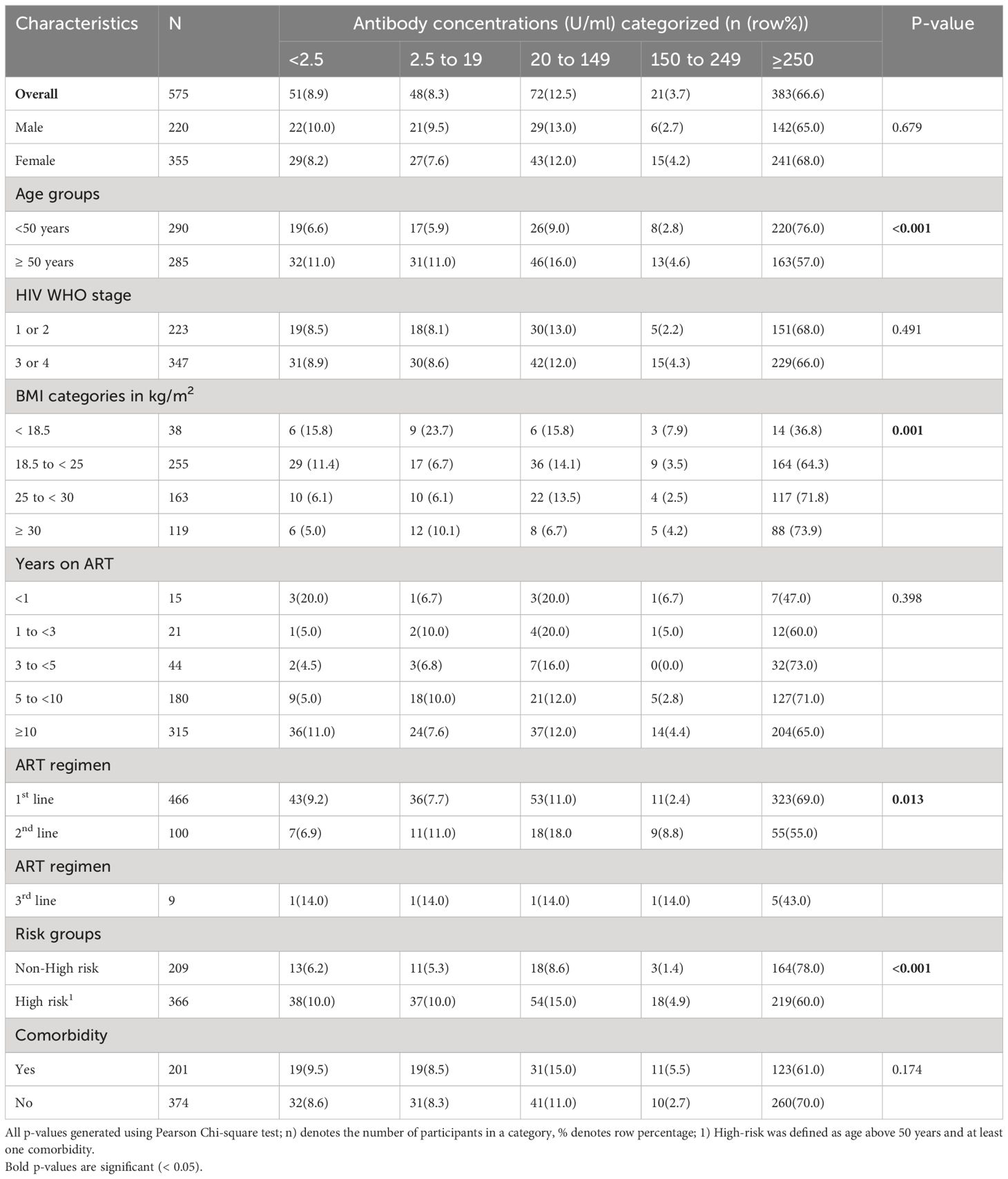
Table 2 SARS-CoV-2 antibody concentration levels per category in relation to study participants´ characteristics.
The distribution of antibody concentrations by study month is shown in Supplementary Figure S1. Concerning the correlation between continuous antibody concentrations and participant characteristics, we found a weak negative correlation between continuous antibody concentrations and age (correlation coefficient -0.207, p-value < 0.001).
Results from the multivariable analysis using ordinal logistic regression are shown in Table 3.
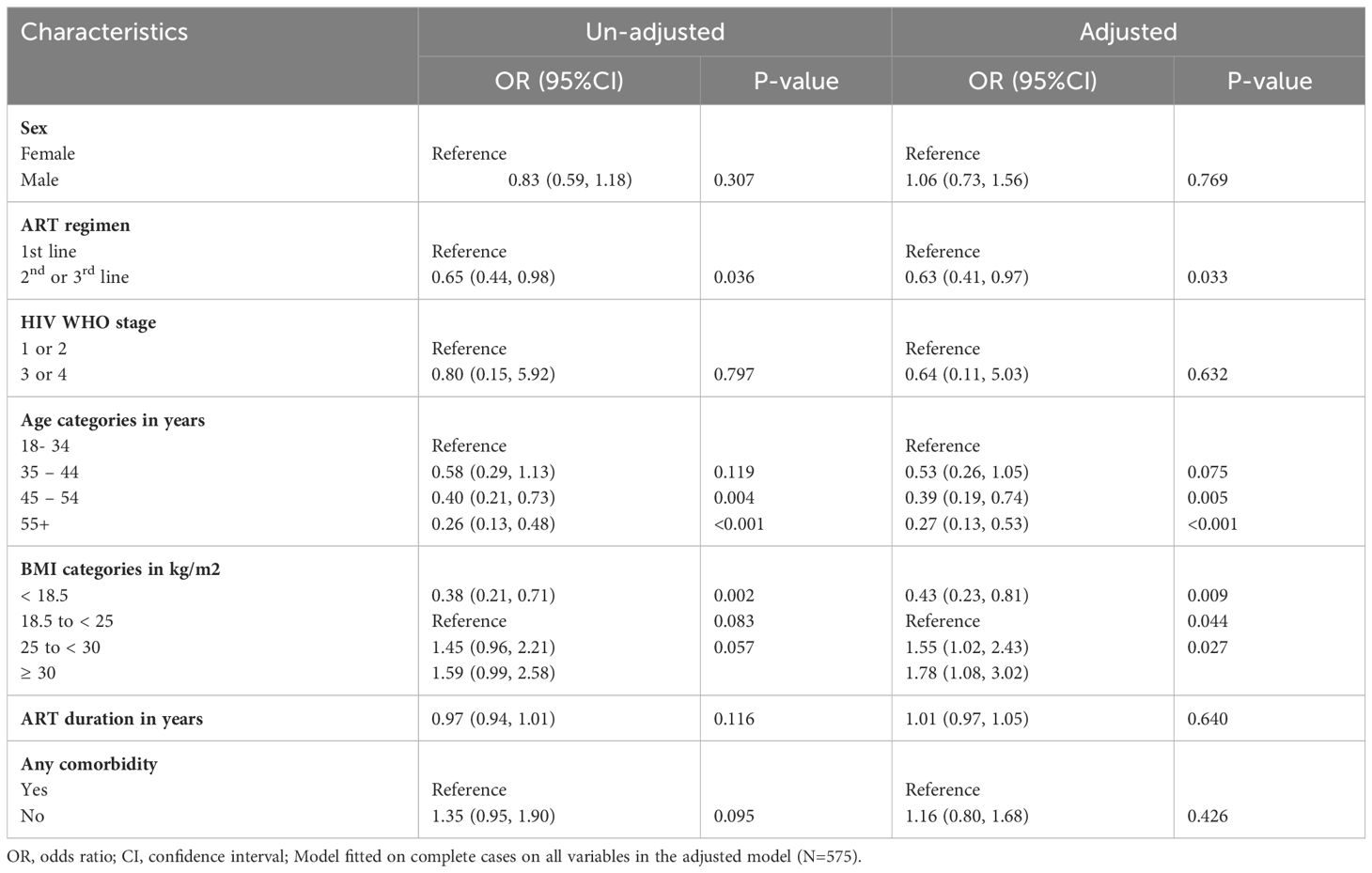
Table 3 Associations between SARS-CoV-2 antibody concentration groups and participants’ characteristics (ordinal logistic regression model).
The following factors were significantly associated with a lower probability of being in higher SARS-CoV-2 antibody concentration categories: Other than first-line ART regimen, age ≥45 years, and BMI <18.5 kg/m2 (aOR=0.63 [95%CI 0.41, 0.97], 0.39[0.19, 0.74], 0.43 [0.23, 0.81]. A high BMI (>25 kg/m2) was associated with a higher probability of being in a higher SARS-CoV-2 antibody concentration category (aOR=1.55 [95%CI 1.02, 2.43]. In a separate model fitted by replacing the covariate age group with the high-risk group, participants in the high-risk group were associated with a lower probability of being in the higher SARS-CoV-2 antibody concentration categories (aOR=0.43 [95%CI 0.26, 0.70]) (Supplementary Table S3). WHO HIV stage, duration on ART, sex, and any comorbidity showed no significant association with SARS-CoV-2 antibody concentration categories. The appropriateness of the assumption of proportional odds assumed by the ordinal logistic regression model was verified.
4 Discussion
This study assessed the SARS-CoV-2 seroprevalence among non-vaccinated PLWH in an urban adult population in Uganda in 2022. SARS-CoV-2 seroprevalence was high in our study population at 93%. We attribute this finding to the fact that our research took place after all restrictions of movement were lifted in Kampala, and the majority of the population was exposed to the dominant Omicron virus variant at the time. This interpretation is further supported by the increase in the proportion of participants with high antibody concentrations of ≥250 U/ml, indicating recent infections in approximately 60% to 80% of the participants during the recruitment period.
So far, SARS-CoV-2 seroprevalence in Uganda has been assessed among blood donors, as well as selected rural communities. A recently published study on seroprevalence among Ugandan blood donors, which was conducted during a similar timeframe as our research, found a seropositivity of 82.6% (19). A further analysis, which included rural households in eastern Uganda and sampled during the first months of 2022, found seroprevalence rates of up to 96% (20). To the best of our knowledge, seroprevalence has not been assessed among Ugandan PLWH. Published data on PLWH from other regions of the world, including sub-Saharan Africa, indicate lower seropositivity rates compared to our findings (21, 22).
In our study, people above the age of 45 years were significantly more likely to have lower antibody concentration levels compared to younger age groups. This finding is consistent with a study conducted amongst healthcare workers with COVID-19 infection or vaccination history in Germany (23). Furthermore, our study shows that participants without specific risk factors for a severe course of illness were significantly more likely to have higher antibody concentration values compared to participants categorized as high-risk, which we assume is attributable to the age factor entirely. The lack of association with the presence of any comorbidity supports this conclusion.
We also found that participants with a low BMI were significantly more likely to have lower antibody concentration values compared to other categories. While the underlying mechanism is thus far unclear, similar observations have been made for the humoral response following SARS-CoV-2 vaccination in the general population, as well as in PLWH (24, 25).
In line with the high seropositivity, almost all study participants reported to have suffered from COVID-19-related symptoms during the pandemic. Of note, the time since their last COVID-19-related symptom was not assessed. Despite suffering from symptoms suggestive of COVID-19 during the pandemic, less than 10% had ever undergone testing for SARS-CoV-2 (RT-PCR from nasopharyngeal swab), and less than 5% of all participants actually had a laboratory-confirmed SARS-CoV-2 infection in the past. This low level of testing despite having typical COVID-19 symptoms during the pandemic is quite remarkable, especially considering that our study population is potentially at risk for severe courses of illness due to HIV infection. As testing centers were widely available to the public, we assume that hesitancy rather than inaccessibility led to a low uptake of testing services. During 2021, the second year of the pandemic, testing positive for SARS-CoV-2 in Kampala resulted in home isolation. For many low-income families relying on daily earnings through the informal market, at-home isolation meant considerable economic hardship (26).
In November 2023, the WHO revised the current recommendations for prioritizing the use of COVID-19 vaccines. The revision reflects the impact of the Omicron variant and high levels of population immunity (12). Prioritization continues to focus on persons at increased risk of severe disease or death and aims to take further factors into account, namely vaccine performance, cost-effectiveness, feasibility, and community acceptance. Older adults as well as all PLWH are considered high-priority groups and therefore (booster) vaccination currently continues to be recommended by the WHO. While vaccination rollout was initially slow due to delayed access in many regions of sub-Saharan Africa, including Uganda, vaccines are now widely available. Whether the SAGE recommendations will be followed now depends more on the provision of medical information to high-priority groups through treating clinicians and community acceptance.
In conclusion, SARS-CoV-2 seroprevalence was high among our study population of PLWH in urban Uganda. We attribute the high population immunity levels to being exposed to the dominant Omicron variant upon the lifting of movement restrictions before our recruitment period. Older study participants, as well as participants with a low BMI were more likely to have lower SARS-CoV-2 antibody concentrations. Interestingly, only a small proportion of past infections had been laboratory-confirmed. Whether testing was not done due to mild courses of illness or general hesitancy towards testing remains unclear.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was granted from the IDI Research Ethics Committee (IDIREC REF 038/2021) and Uganda National Council of Science and Technology (UNCST) (HS1956ES). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PA: Data curation, Formal analysis, Investigation, Project administration, Validation, Writing – original draft, Writing – review & editing. LN: Data curation, Formal analysis, Methodology, Validation, Writing – review & editing. JM: Data curation, Formal analysis, Methodology, Validation, Writing – review & editing. MH: Writing – review & editing. BC: Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing. AB: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded through the hospital partnerships program of the GIZ GmbH (grant contract number: 81271296). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication. Open access publication was supported by the Open Access Publishing Fund of Leipzig University.
Acknowledgments
We would like to thank the study participants, as well as the clinical and laboratory teams at IDI. We especially thank Stephen Okoboi, Bosco Kafufu, Noela Clara Owarwo, Rejani Opio, and Christine Sekaggya-Wiltshire for their valuable input during the planning of our research study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fviro.2024.1429785/full#supplementary-material
References
1. World Health Organization. WHO COVID-19 dashboard. Available at: https://data.who.int/dashboards/covid19/cases?n=c (Accessed 5 February 2024).
2. Finnerty JP, Hussain ABMA, Ponnuswamy A, Kamil HG, Abdelaziz A. Asthma and COPD as co-morbidities in patients hospitalised with Covid-19 disease: a global systematic review and meta-analysis. BMC Pulm. Med. (2023) 23:462. doi: 10.1186/s12890-023-02761-5
3. Soto-Cabezas MG, Reyes-Vega MF, Soriano-Moreno AN, Ordoñez-Ibargüen L, Martel KS, Flores-Jaime N, et al. Comorbilidades asociadas a la mortalidad por COVID-19 en adultos en Lima, Perú: un estudio de cohorte retrospectiva. Rev Peru. Med Exp Salud Publica. (2023) 40:132–40. doi: 10.17843/rpmesp.2023.402.12170
4. Williams SG, Frain S, Guo H, Carr MJ, Ashcroft DM, Keavney BD. Clinical risk associated with COVID-19 among 86000 patients with congenital heart disease. Open Heart. (2023) 10. doi: 10.1136/openhrt-2023-002415
5. Brolly J, Chadwick DR. COVID-19 infection in people living with HIV. Br Med Bull. (2023) 147:20–30. doi: 10.1093/bmb/ldac031
6. Spinelli MA, Jones BLH, Gandhi M. COVID-19 outcomes and risk factors among people living with HIV. Curr HIV/AIDS Rep. (2022) 19:425–32. doi: 10.1007/s11904-022-00618-w
7. Augello M, Bono V, Rovito R, Tincati C, Marchetti G. Immunologic interplay between HIV/AIDS and COVID-19: adding fuel to the flames? Curr HIV/AIDS Rep. (2023) 20:51–75. doi: 10.1007/s11904-023-00647-z
8. Hanson HA, Kim E, Badowski ME. A Systematic review: impact of SARS-coV-2 infection on morbidity, mortality, and viral suppression in patients living with HIV. SN Compr Clin Med. (2023) 5:144. doi: 10.1007/s42399-023-01480-6
9. Mazzitelli M, Trunfio M, Sasset L, Leoni D, Castelli E, Lo Menzo S, et al. Factors associated with severe COVID-19 and post-acute COVID-19 syndrome in a cohort of people living with HIV on antiretroviral treatment and with undetectable HIV RNA. Viruses. (2022) 14. doi: 10.3390/v14030493
10. Giacomelli A, Gagliardini R, Tavelli A, de Benedittis S, Mazzotta V, Rizzardini G, et al. Risk of COVID-19 in-hospital mortality in people living with HIV compared to general population according to age and CD4 strata: data from the ICONA network. Int J Infect Dis. (2023) 136:127–35. doi: 10.1016/j.ijid.2023.09.015
11. Augello M, Bono V, Rovito R, Tincati C, Bianchi S, Taramasso L, et al. Association between SARS-CoV-2 RNAemia, skewed T cell responses, inflammation, and severity in hospitalized COVID-19 people living with HIV. iScience. (2024) 27:108673. doi: 10.1016/j.isci.2023.108673
12. World Health Organization. WHO roadmap on uses of COVID-19 vaccines in the context of Omicron and high population immunity. Available at: https://iris.who.int/bitstream/handle/10665/373987/WHO-2019-nCoV-Vaccines-SAGE-Prioritization-2023.2-eng.pdf?sequence=1 (Accessed 5 February 2024).
13. Atuheirwe M, Otim R, Male KJ, Ahimbisibwe S, Sackey JD, Sande OJ. Misinformation, knowledge and COVID-19 vaccine acceptance: a cross-sectional study among health care workers and the general population in Kampala, Uganda. BMC Public Health. (2024) 24:203. doi: 10.1186/s12889-024-17678-9
14. Kanyike AM, Olum R, Kajjimu J, Ojilong D, Akech GM, Nassozi DR, et al. Acceptance of the coronavirus disease-2019 vaccine among medical students in Uganda. Trop Med Health. (2021) 49:37. doi: 10.1186/s41182-021-00331-1
15. Castelnuovo B, Kiragga A, Afayo V, Ncube M, Orama R, Magero S, et al. Implementation of provider-based electronic medical records and improvement of the quality of data in a large HIV program in Sub-Saharan Africa. PloS One. (2012) 7:e51631. doi: 10.1371/journal.pone.0051631
16. R Core Team. R: A language and environment for statistical computing (2021). Available at: https://www.R-project.org/.
17. Wickham H, Averick M, Bryan J, Chang W, McGowan L, François R, et al. Welcome to the tidyverse. JOSS. (2019) 4:1686. doi: 10.21105/joss.01686
18. ROCHE. Elecsys Anti-SARS-CoV-2 S factsheet. Available at: https://diagnostics.roche.com/ch/de/products/params/elecsys-anti-sars-cov-2-s.html (Accessed 5 February 2024).
19. Bloch EM, Kyeyune D, White JL, Ddungu H, Ashokkumar S, Habtehyimer F, et al. SARS-CoV-2 seroprevalence among blood donors in Uganda: 2019-2022. Transfusion. (2023) 63:1354–65. doi: 10.1111/trf.17449
20. Briggs J, Takahashi S, Nayebare P, Cuu G, Rek J, Zedi M, et al. Seroprevalence of antibodies to SARS-coV-2 in rural households in eastern Uganda, 2020-2022. JAMA Netw Open. (2023) 6:e2255978. doi: 10.1001/jamanetworkopen.2022.55978
21. Sagna T, Ouedraogo P, Traore L, Obiri-Yeboah D, Yonli A, Tapsoba A, et al. Enigma of the high prevalence of anti-SARS-CoV-2 antibodies in HIV-positive people with no symptoms of COVID-19 in Burkina Faso. J Public Health Afr. (2022) 13:1778. doi: 10.4081/jphia.2022.1778
22. Ghate M, Shidhaye P, Gurav S, Gadhe K, Kale V, Jain P, et al. Seroprevalence of Anti-SARS-CoV-2 IgG Antibodies among HIV Infected Individuals Attending ART Centre at Pune: A Cross-Sectional Study. J Int Assoc Provid. AIDS Care. (2022) 21:23259582221077943. doi: 10.1177/23259582221077943
23. Reusch J, Wagenhäuser I, Gabel A, Eggestein A, Höhn A, Lâm T-T, et al. Influencing factors of anti-SARS-CoV-2-spike-IgG antibody titers in healthcare workers: A cross-section study. J Med Virol. (2023) 95:e28300. doi: 10.1002/jmv.28300
24. Piernas C, Patone M, Astbury NM, Gao M, Sheikh A, Khunti K, et al. Associations of BMI with COVID-19 vaccine uptake, vaccine effectiveness, and risk of severe COVID-19 outcomes after vaccination in England: a population-based cohort study. Lancet Diabetes Endocrinol. (2022) 10:571–80. doi: 10.1016/S2213-8587(22)00158-9
25. Montesi G, Augello M, Polvere J, Marchetti G, Medaglini D, Ciabattini A. Predicting humoral responses to primary and booster SARS-CoV-2 mRNA vaccination in people living with HIV: a machine learning approach. J Transl Med. (2024) 22:432. doi: 10.1186/s12967-024-05147-1
Keywords: SARS-CoV-2, seroprevalence, adaptive humoral response, antibody concentrations, HIV, Uganda
Citation: Ainembabazi P, Najjemba L, Musaazi J, Hönemann M, Castelnuovo B and von Braun A (2024) Severe acute respiratory syndrome coronavirus-2 seroprevalence in non-vaccinated people living with HIV in Uganda during 2022. Front. Virol. 4:1429785. doi: 10.3389/fviro.2024.1429785
Received: 08 May 2024; Accepted: 12 July 2024;
Published: 06 August 2024.
Edited by:
Stefania Varchetta, IRCCS Ca’ Granda Foundation Maggiore Policlinico Hospital, ItalyReviewed by:
Wibke Bayer, Essen University Hospital, GermanyMatteo Augello, University of Milan, Italy
Copyright © 2024 Ainembabazi, Najjemba, Musaazi, Hönemann, Castelnuovo and von Braun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amrei von Braun, YW1yZWkuYnJhdW5AbWVkaXppbi51bmktbGVpcHppZy5kZQ==
†These authors share senior authorship