 Cecilia Salazar1,2†
Cecilia Salazar1,2† Alicia Costabile2,3,4,5†Ignacio Ferrés1,2Paula Perbolianachis4,5
Alicia Costabile2,3,4,5†Ignacio Ferrés1,2Paula Perbolianachis4,5 Marianoel Pereira-Gómez4,5
Marianoel Pereira-Gómez4,5 Diego Simón4,5Antonio Galiana6,7Beatriz Pi7Virginia Antelo7Rosario García7
Diego Simón4,5Antonio Galiana6,7Beatriz Pi7Virginia Antelo7Rosario García7 Pilar Moreno2,4,5*
Pilar Moreno2,4,5* Gonzalo Moratorio2,4,5*
Gonzalo Moratorio2,4,5* Gregorio Iraola1,2,8*
Gregorio Iraola1,2,8*- 1Laboratorio de Genómica Microbiana, Institut Pasteur de Montevideo, Montevideo, Uruguay
- 2Centro de Innovación en Vigilancia Epidemiológica (CiVE), Institut Pasteur de Montevideo, Montevideo, Uruguay
- 3Sección Bioquímica y Biología Molecular, Facultad de Ciencias, Universidad de la República, Montevideo, Uruguay
- 4Laboratorio de Evolución Experimental de Virus, Institut Pasteur de Montevideo, Montevideo, Uruguay
- 5Laboratorio de Virología Molecular, Facultad de Ciencias, Universidad de la República, Montevideo, Uruguay
- 6Hospital Maciel, Montevideo, Uruguay
- 7Asistencial Médica de Maldonado, Maldonado, Uruguay
- 8Wellcome Sanger Institute, Hinxton, United Kingdom
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variant B.1.1.7 causes a more transmissible and apparently more severe disease. We report its early introduction from Europe to South America from a traveler who arrived in Uruguay from the United Kingdom, even before B.1.1.7 was recognized as a variant of concern. This highlights the risk of introduction of SARS-CoV-2 variants despite strict contingency protocols and underscores the need of improving real-time surveillance worldwide.
Introduction
On December 14, 2020, the United Kingdom (UK) reported a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variant of concern (VOC), currently known as VOC 202012/01, 20I/501Y.V1 or lineage B.1.1.7. The emergence of this variant has been estimated to September 2020 and then quickly become the main circulating SARS-CoV-2 variant in England (1). The higher transmission capacity of this variant and its apparent capacity to cause a more severe illness (2) are rising concerns internationally (3), triggering specific efforts to contain its spread.
Case Description
On December 15, 2020, a 27-year-old male Uruguayan citizen who has been residing in the UK during the past 18 months, flew from the UK to Uruguay (Figure 1A). The trip consisted in a direct flight from London (UK) to Madrid (Spain), where he remained in transit (not leaving the airport) during 2 h to subsequently take a connection flight to Montevideo (Uruguay). The COVID-19 contingency protocol in Uruguay requires a negative SARS-CoV-2 RT-qPCR test up to 72 h before arrival to the country, which had been performed and resulted negative in the UK on December 12, 2020. Also, as part of the national protocol, the patient was isolated at his arrival to fulfill a preventive 14-day quarantine. Five days after arrival, on December 20, 2020, the patient developed symptoms compatible with COVID-19 such as fever, cough, headache, and myalgia. Then, on December 22, 2020, the patient tested positive for SARS-CoV-2 by RT-qPCR performed in a private lab. Two days after, on December 24, 2020, the patient developed dyspnea requiring of hospitalization. Clinical evaluation revealed lympophenia, azotemia and elevated levels of C-reactive protein. Chest X-ray showed diffuse interstitial infiltrate with slight opacity erasing the right costophrenic angle. These observations were compatible with COVID-19 pneumonia and a probable bacterial secondary infection, so thromboprophylaxis was started together with corticosteroids, ampicillin-sulbactam and clarithromycin. The patient remained admitted for 6 days in a moderate care area with excellent evolution. On December 30, 2020, the patient recovered and was remitted from hospital with absence of any clinical signs of COVID-19. After that, the patient remained in quarantine at his home co-inhabiting but isolated from his family (five people ranging from 15 to 85 years old). Due to a quarantine protocol misinterpretation, the family was in contact with the patient during 48 h, on January 2, 2021 so all they were subsequently quarantined for 7 days being asymptomatic during this period. On January 9, 2021, patient's family members were tested for SARS-CoV-2 and resulted negative. A retrospective epidemiological investigation evidenced two additional contacts. First, the day before the patient's pre-trip test was performed in the UK, he was in contact during 1 h and without using face masks with a person who developed COVID-19 symptoms on December 20, 2020, and then tested positive in the UK. Second, a friend took the patient at his arrival from the airport to his home in Montevideo in a particular car. Once the patient was diagnosed with COVID-19, his friend was quarantined for 14 days being asymptomatic and testing negative at the end of this period.
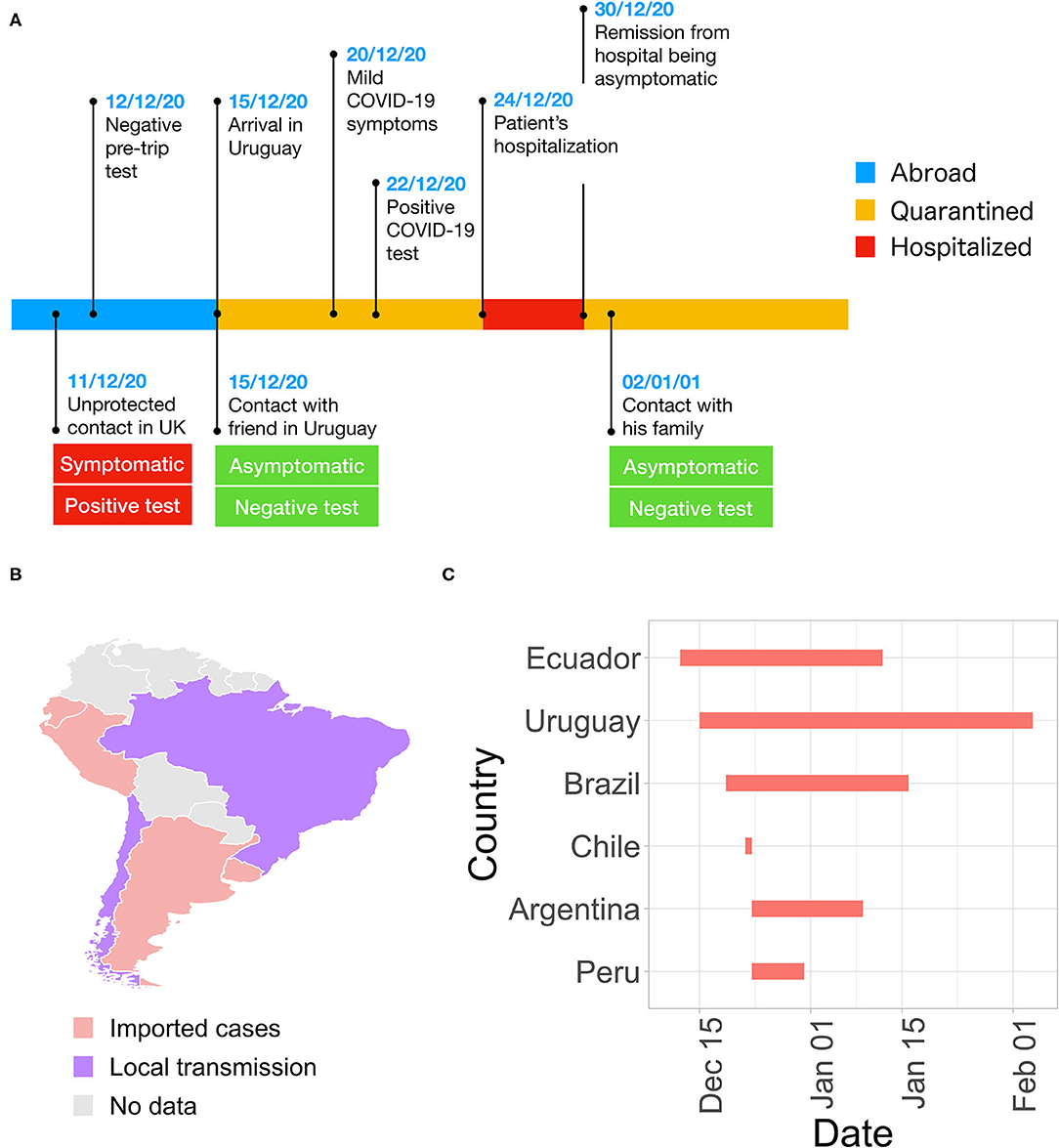
Figure 1. Import of the SARS-CoV-2 variant B.1.1.7 into South America. (A) Timeline of main events related to the B.1.1.7 case imported from the UK to Uruguay on December 20, 2020. (B) Status of B.1.1.7 distribution in South American countries. (C) Elapsed time from B.1.1.7 introduction and report in South America. Horizontal bars span from the date of introduction (when known) to the date of official report of B.1.1.7 presence in each country.
Given the potential epidemiological relevance of this case, a retrospective genomic and molecular analysis was performed on the patient's positive nasopharyngeal swab sample collected on December 22, 2020. First, we used the “COVID-19 RT-PCR Real TM Fast-HEX/Cy5” (Institut Pasteur de Montevideo, Universidad de la República, ATGen) to re-confirm the presence of SARS-CoV-2 in this sample, that resulted positive again with a cycle threshold of 30. Then, the sample was submitted to the SARS-CoV-2 genome sequencing pipeline at the Institut Pasteur de Montevideo, using the ARCTIC Network protocol for the MinION platform (4), as previously implemented (5). Due to degradation of the original sample, amplification of the whole genome was not achieved. However, mapping of resulting reads against the reference SARS-CoV-2 genome Wuhan-1 (GISAID accession no. EPI_ISL_302124) revealed specific diagnostic mutations of lineage B.1.1.7 in the spike gene, including P681H (C23604A), T716I (C23709T), S982A (T24506G), and D1118H (G24914C). To confirm this, we performed one in-house and one previously published (6) RT-qPCR assay specifically designed for the detection and differentiation of VOC B.1.1.7, B.1.1.351 and P.1. These assays target the ORF1a Δ3675-3677 and spike Δ69-70 deletions, but using different primers and probes. In both cases, results were consistent with the presence of the B.1.1.7 lineage. Together, this evidence supported the classification of this imported case as B.1.1.7. We deposited sequencing data in the SRA database under accession number PRJNA713811.
Discussion
This case represents one of the first documented introductions of the B.1.1.7 lineage to South America. More precisely, it was the second case after the first registered introduction in Ecuador by a traveler that returned from the UK on December 13, 2020 (7). After that, other South American countries including Argentina (8), Chile (9), Perú (10), and Brazil (11), have reported introductions from the UK. Additionally, local transmission has been already observed in Brazil and Chile (Figure 1B). This evidences the rapid transcontinental dissemination of B.1.1.7, that was introduced in South America even before the official communication of the UK government warning about the emergence of this VOC. All these facts highlights that, even maximizing border control and complying with the national and international protocols for COVID-19 containment, is still insufficient to prevent the spread of VOC. The rapid emergence and spread of VOC need an immediate roll out of surveillance tools to perform an active surveillance. In this sense, the time period between the actual introduction and the official report of B.1.1.7 cases in South America has a mean of 22.6 days, ranging from 1 (Chile) to 51 days (Uruguay) (Figure 1C), evidencing a lag in real-time surveillance. This shows the need to improve genomic surveillance capabilities in the region along with the logistics to identify cases of particular concern that may require specific contingency measures. Thus, there is a need to rapidly deploy national programs of genomic surveillance at scale setting a goal of sequencing at least 5% of positive samples to detect VOC that still circulate in low frequency (12).
To date, since hospital records and contact tracing numbers significantly raised in the UK, a salient feature of the B.1.1.7 lineage is its increased transmission capacity (13). In this case, the patient did not transmit the virus to their contacts once him arrived in Uruguay. This could be explained by the fact that these contacts happened when the patient was asymptomatic (one at his arrival to the airport, and the others after being remitted from hospital), being known that asymptomatic patients might be less infective than symptomatic patients (14). Another salient feature of B.1.1.7 is its apparent capacity to cause a more severe illness and to increase the risk of death (2). In this case, the patient developed symptoms that required hospitalization but had a positive outcome after receiving moderate care. Together, we conclude that contact tracing and isolation was successful to identify and quarantine all contacts in adequate time, preventing the potential spread of this variant in Uruguay. Indeed, our lab is performing active genomic surveillance of VOC, typing hundreds of COVID-19 positive samples every week and we have not detected new introductions or local transmission of B.1.1.7 3 months after the time of this introduction in mid-December, 2020.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics Statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
CS, AC, IF, PP, DS, and MP-G generated the data and performed the analyses. AG, BP, VA, and RG collected the data. PM, GM, and GI analyzed the data and wrote the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Centro de Innovación en Vigilancia Epidemiológica (CiVE) from the Institut Pasteur de Montevideo, the Banco de Seguros del Estado (BSE) of Uruguay, and the G4 Research Groups Program from the Institut Pasteur de Montevideo. Also, this work was supported by FOCEM (Fondo para la Convergencia Estructural del Mercosur) Grant Number: COF 03/11. IF was supported by grant ANII-POS_NAC_2018_1_151494 from Agencia Nacional de Investigación e Innovación (ANII), Uruguay.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank to Nathan D. Grubaugh and Chantal Vogels for their helpful collaboration sending their specific primers and probes to detect VOC.
References
1. Public Health England. Investigation of Novel SARS-CoV-2 Variant: Variant of Concern 202012/01 - Technical Briefing 3. (2021). Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/959360/Variant_of_Concern_VOC_202012_01_Technical_Briefing_3.pdf (accessed March 25, 2021).
2. Davies NG, Jarvis CI, Edmunds WJ, Jewell NP, Diaz-Ordaz K, and Keogh RH. Increased mortality in community-tested cases of SARS-CoV-2 lineage B.1.1.7. Nature. (2021) 539:1–5. doi: 10.1101/2021.02.01.21250959
3. Grubaugh ND, Hodcroft EB, Fauver JR, Phelan AL, and Cevik M. Public health actions to control new SARS-CoV-2 variants. Cell. (2021) 184:1127–32. doi: 10.1016/j.cell.2021.01.044
4. Quick J. nCoV-2019 Sequencing Protocol v3. (2020). Available online at: https://www.protocols.io/view/ncov-2019-sequencing-protocol-v3-locost-bh42j8ye (accessed April 14, 2021).
5. Salazar C, Díaz-Viraqué F, Pereira M, Ferrés I, Moreno P, Moratorio G, et al. Multiple introductions, regional spread and local differentiation during the first week of COVID-19 epidemic in Montevideo, Uruguay. bioRxiv [Preprint]. (2020). doi: 10.1101/2020.05.09.086223
6. Vogels CBF, Breban M, Alpert T, Petrone ME, Watkins AE, Hodcroft EB, et al. PCR assay to enhance global surveillance for SARS-CoV-2 variants of concern. medRxiv [Preprint]. (2021). doi: 10.1101/2021.01.28.21250486
7. Ministerio de Salud Pública de Ecuador. Estudios de Secuenciación Genómica del Inspi Confirman la Presencia de Nueva Variación del SARS-CoV-2 en Ecuador. (2021). Available online at: https://www.salud.gob.ec/estudios-de-secuenciación-genomica-del-inspi-confirman-la-presencia-de-nueva-variación-del-sars-cov-2-en-ecuador (accessed April 14, 2021).
8. MedicalXPress. Argentina Detects First Case of British Virus Variant. (2021). Available online at: https://medicalxpress.com/news/2021-01-argentina-case-british-virus-variant.html (accessed April 14, 2021).
9. Reuters. Chile Records First Case of British Variant of Coronavirus – Health Ministry. (2020). Available online at: https://www.reuters.com/article/uk-health-coronavirus-britain-variants-f/chile-records-first-case-of-british-variant-of-coronavirus-health-ministry-idUSKBN2931CS (accessed April 14, 2021).
10. The Rio Times. Peru Confirms First Case of COVID-19 Variant Strain. (2021). Available online at: https://riotimesonline.com/brazil-news/miscellaneous/covid-19/peru-confirms-first-case-of-covid-19-variant (accessed April 14, 2021).
11. Reuters. Brazil Detects Two Cases of New Coronavirus Variant Found in UK. (2020). Available online at: https://www.reuters.com/article/us-health-coronavirus-brazil-variant-idUSKBN2951LL (accessed April 14, 2021).
12. Vavrek D, Speroni L, Curnow KJ, Oberholzer M, Moeder V, and Febbo PG. Genomic surveillance at scale is required to detect newly emerging strains at an early timepoint. medRxiv [Preprint]. (2021). doi: 10.1101/2021.01.12.21249613
13. Davies NG, Abbott S, Barnard RC, Jarvis CI, Kucharski AJ, Munday JD, et al. Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England. Science. (2021) 372:eabg3055. doi: 10.1126/science.abg3055
Keywords: COVID-19, SARS-CoV-2, B.1.1.7 variant, South America, transcontinental, Uruguay, VOC
Citation: Salazar C, Costabile A, Ferrés I, Perbolianachis P, Pereira-Gómez M, Simón D, Galiana A, Pi B, Antelo V, García R, Moreno P, Moratorio G and Iraola G (2021) Case Report: Early Transcontinental Import of SARS-CoV-2 Variant of Concern 202012/01 (B.1.1.7) From Europe to Uruguay. Front. Virol. 1:685618. doi: 10.3389/fviro.2021.685618
Received: 25 March 2021; Accepted: 30 April 2021;
Published: 28 May 2021.
Edited by:
Jacqueline Weyer, National Institute of Communicable Diseases (NICD), South AfricaReviewed by:
Katherine Laiton Donato, Instituto Nacional de Salud, ColombiaGiuseppe Oliveto, Sapienza University of Rome, Italy
Copyright © 2021 Salazar, Costabile, Ferrés, Perbolianachis, Pereira-Gómez, Simón, Galiana, Pi, Antelo, García, Moreno, Moratorio and Iraola. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pilar Moreno, cG1vcmVub0BwYXN0ZXVyLmVkdS51eQ==; Gonzalo Moratorio, bW9yYXRvcmlvQHBhc3RldXIuZWR1LnV5; Gregorio Iraola, Z2lyYW9sYUBwYXN0ZXVyLmVkdS51eQ==
†These authors have contributed equally to this work