
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Vet. Sci. , 05 April 2024
Sec. Oncology in Veterinary Medicine
Volume 11 - 2024 | https://doi.org/10.3389/fvets.2024.1359426
This article is part of the Research Topic Advancements and Challenges in Veterinary Oncology View all 9 articles
 Gerry Polton1*
Gerry Polton1* Juan F. Borrego2
Juan F. Borrego2 Francisco Clemente-Vicario3
Francisco Clemente-Vicario3 Craig A. Clifford4
Craig A. Clifford4 Dariusz Jagielski5
Dariusz Jagielski5 Martin Kessler6
Martin Kessler6 Tetsuya Kobayashi7Didier Lanore8
Tetsuya Kobayashi7Didier Lanore8 Felisbina L. Queiroga9Annika Tranaeus Rowe10
Felisbina L. Queiroga9Annika Tranaeus Rowe10 Péter Vajdovich11
Péter Vajdovich11 Philip J. Bergman12
Philip J. Bergman12Melanoma of the dog and cat poses a clinical challenge to veterinary practitioners across the globe. As knowledge evolves, so too do clinical practices. However, there remain uncertainties and controversies. There is value for the veterinary community at large in the generation of a contemporary wide-ranging guideline document. The aim of this project was therefore to assimilate the available published knowledge into a single accessible referenced resource and to provide expert clinical guidance to support professional colleagues as they navigate current melanoma challenges and controversies. Melanocytic tumors are common in dogs but rare in cats. The history and clinical signs relate to the anatomic site of the melanoma. Oral and subungual malignant melanomas are the most common malignant types in dogs. While many melanocytic tumors are heavily pigmented, making diagnosis relatively straightforward, melanin pigmentation is variable. A validated clinical stage scheme has been defined for canine oral melanoma. For all other locations and for feline melanoma, TNM-based staging applies. Certain histological characteristics have been shown to bear prognostic significance and can thus prove instructive in clinical decision making. Surgical resection using wide margins is currently the mainstay of therapy for the local control of melanomas, regardless of primary location. Radiotherapy forms an integral part of the management of canine oral melanomas, both as a primary and an adjuvant therapy. Adjuvant immunotherapy or chemotherapy is offered to patients at high risk of developing distant metastasis. Location is the major prognostic factor, although it is not completely predictive of local invasiveness and metastatic potential. There are no specific guidelines regarding referral considerations for dogs with melanoma, as this is likely based on a multitude of factors. The ultimate goal is to provide the best options for patients to extend quality of life and survival, either within the primary care or referral hospital setting.
Tumors of melanin-producing cells in dogs and cats pose a significant challenge to all practitioners, regardless of experience and facilities. There is a broad spectrum of malignancy and, while patterns of behavior exist, tumors comply with these rules with variable veracity. The following basic rule always applies: advanced clinical stage and evidence of elevated proliferation rate correlate with poorer outcomes. No single treatment is consistently best, and all treatment modalities have a potential application. The purpose of this guideline document is to provide a succinct yet comprehensive overview of melanoma management in dogs and cats.
Melanocytic tumors are common in dogs (1, 2) [LOE 2c, OEG B]. Malignant melanoma accounts for 70% of all melanin-producing tumors and 7% of all malignant tumors (1, 3) [LOE 2c-3a, OEG B]. Benign forms are called melanocytomas and account for 30% of melanin-producing tumors (1) [LOE 2c, OEG B]. Middle-aged to older dogs and heavily pigmented breeds are more commonly affected (1, 2) [LOE 2c, OEG B]. Scottish terriers, golden retrievers, poodles, dachshunds, and chow-chows are predisposed to oral melanoma (2) [LOE 2c, OEG B]. Schnauzers, rottweilers, Scottish terriers, golden retrievers, and Irish setters are at increased risk of developing subungual melanoma (4, 5) [LOE 2c-4a, OEG B].
Melanomas are most frequently identified in oral (62%), cutaneous (27%), digital (6%), and subungual (4%) sites (1) [LOE 2c, OEG B]. Melanomas of ocular structures, footpads, nasal cavity, gastrointestinal tract, and anal sacs have been reported (2) [LOE 2c, OEG B]. Oral melanoma is the most common oral malignancy in dogs (2) [LOE 2c, OEG B], representing 14.4 to 45.5% of all oral tumors (6) [LOE 3a, OEG C]. Cutaneous melanoma accounts for 0.8 to 2% of all canine skin tumors (6) [LOE 3a, OEG C]. In dogs, ocular melanocytic tumors exhibit distinct phenotypes: tumors of conjunctiva are usually malignant, whereas limbal, iridal, and uveal tumors are predominantly benign (7, 8) [LOE 3a-4c, OEG C].
Melanocytic tumors are rare in cats. They account for less than 1% of all cancer diagnoses (9) [LOE 5, OEG D], 0.8 to 7.0% of all feline skin tumors and < 1% of feline oral tumors (10, 11) [LOE 4b, OEG C]. They occur most commonly in the eye (limbus and intraocular), the haired skin (especially pinna), and the oral cavity (12) [LOE 4b, OEG C]. Melanoma of the nasal planum has been reported (13) [LOE 4c, OEG C]. The typical age of affected cats is 11–13 years (11, 12) [LOE 4b, OEG C]. Melanoma of the pinna has been reported in a younger patient group (median age 7 years) (11) [LOE 4b, OEG C]. No sex or breed predispositions have been reported (11, 12) [LOE 4b, OEG C].
The history and clinical signs relate to the anatomic site of the melanoma.
Oral melanoma arises primarily in the gingiva, lips, tongue, and hard palate (3, 14–16) [LOE 3a-4a, OEG B]. The tumor may be friable and ulcerated. Clinical signs include halitosis, drooling, bleeding from the mouth, dysphagia, and weight loss (3) [LOE 3a, OEG B]. Enlarged draining lymph nodes may or may not be palpable (17) [LOE 4a, OEG C]. The majority of cases are malignant (2, 3, 14) [LOE 2c-4a, OEG B] but it is noteworthy that a population exists with well-differentiated and slowly progressive tumors arising from the mucous membranes of the lip and oral cavity (18) [LOE 4a, OEG C]. There is variation in the degree of pigmentation; some tumors are completely unpigmented (14) [LOE 4a, OEG C].
Melanocytic tumors of the haired skin typically manifest as raised pigmented mass lesions; signs of inflammation are usually absent. Small brown or black masses are the most common; however, the lesions can be large, flat, or wrinkled (2, 19) [LOE 2c-5, OEG B]. Lesions can be multiple. They may be present for a long time. Cutaneous melanomas are commonly phenotypically benign (1, 2, 19, 20) [LOE 2c-5, OEG B]. Whereas melanocytomas are usually solitary, small, pigmented, firm, and freely moveable over deeper structures, malignant melanomas tend to be fast-growing tumors, often ulcerated and pigmented (21) [LOE 4b, OEG C]. Certain sites may be associated with malignancy: for example, the digit, footpad, and scrotum (2, 21) [LOE 2c-4b, OEG B].
Subungual lesions usually present as a swollen painful distal phalanx or a non-healing lesion near the claw. Patients present with lameness or excessive licking of the site (22) [LOE 4c, OEG C]; subungual melanomas frequently metastasize (5, 22, 23) [LOE 2c-4c, OEG B].
Clinical signs of ocular melanoma relate to the structure affected and may include a mass lesion, glaucoma, hyphema, anterior uveitis, epiphora, conjunctival vascular injection, mucopurulent ocular discharge, and/or protrusion of the third eyelid, depending on the site of the lesion (7) [LOE 3a, OEG C].
1. Multiple expressions are used to describe tumors of melanocytic origin. It is recommended that clear and transparent terms are used to ensure a common language and comparability between studies. We would like to reinforce the meanings of the following expressions: Melanoma and Malignant melanoma have the same meaning and refer to malignant tumors derived from melanocytes; Melanocytoma refers to a benign tumors derived from melanocytes; Melanocytic tumors refers to tumors derived from melanocytes, regardless of whether they are benign or malignant.
2. Incidence and prevalence: in dogs, there are known breed predispositions to melanoma. Whether prognoses with melanoma differ according to breed is not known. Given the significance of genotype in human melanoma subtypes, this may be an interesting area of future study.
3. In cats, peak age incidence differs between melanomas of the pinna and melanomas of other sites. Although it is reasonable to presume an aetiological difference between melanomas occurring in sun-exposed and non-exposed sites, there is no evidence to suggest a difference in clinical progression or prognosis.
There are two important differences between human and canine melanomas: 1. canine melanoma is not induced by ultraviolet (UV) light; and 2. whereas ocular and cutaneous truncal melanomas are most common malignant forms in humans, in dogs these anatomic forms are typically benign. Instead, oral and subungual malignant melanomas are the most common malignant types in dogs; these are rare but also aggressive in humans (18, 23) [LOE 2b-5, OEG B].
Melanomas in the oral cavity are similar to human mucosal melanomas in that benign and malignant forms cannot be discriminated by visual examination (3, 24–26) [LOE 2a-5, OEG D]. Pigmentation can vary within a single tumor (Figure 1). Tumor burden and pigmentation are inconsistent indicators of malignant potential.
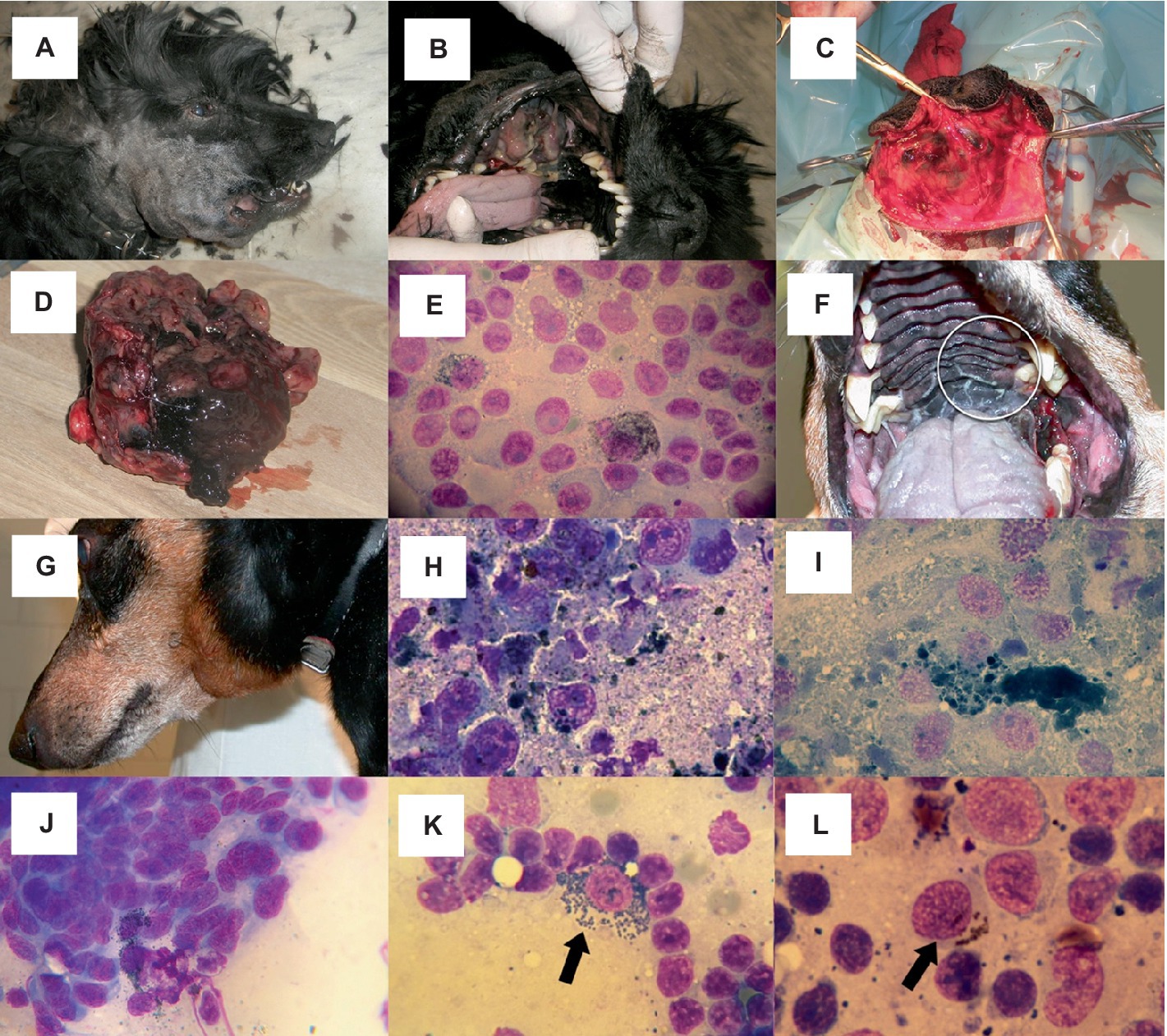
Figure 1. Oral melanoma. (A–D) Heterogenous appearance of oral melanoma in a cocker spaniel. (A) Outward appearance. (B) Visualization of the intraoral aspect illustrates the importance of oral examination in forming the clinical suspicion of melanoma. (C,D) The intraoperative and excision specimen images reveal the absence of an appreciable surgical margin. This is acceptable when the goal of surgery is palliation of the consequences of the presence of a large mass or as a precursor to definitive radiotherapy. (D) Heterogenous appearance of oral melanoma: the tumor grossly exhibits melanotic and amelanotic parts. (E) Malignant melanoma cytology from mandibular gingiva. Cellular borders are usually distinct, though sometimes faint. Cytoplasm is basophilic or light basophilic and granulated; occasionally, small vacuoles or light black to deep green small cytoplasmic granules are seen. Nuclei are eccentrically located and may be irregular; they often show large, dark, prominent nucleoli. (F–I) Oral malignant melanoma with lymph node metastasis in a dachshund. (F) A small primary tumor was located medial to a left upper molar tooth. (G) The patient was presented with left submandibular lymph node enlargement. (H,I). Tumor cells are spindle-shaped and contain large amounts of melanin pigment. The melanoma cells are large and elongated, with length 4-5x and width 2-3x accompanying red blood cells. The cytoplasmic margins are indistinct, the cytoplasm is vacuolated and black/green cytoplasmic granules are apparent. The nuclei are round to oval with stippled, coarse chromatin; nucleoli are distinct and vary in size and number. (J) Spindle-shaped form of malignant melanoma cytologically resembles a sarcoma, though melanin granules are also evident in this sample. (K,L) Oral melanoma with lymph node metastasis; melanophages versus malignant melanoma. (K) A macrophage (melanophage) with intracytoplasmic melanin pigment (arrow) is seen among reactive lymphoid population. Free melanin granules are also visible. Melanophages in themselves do not indicate tumor metastasis, as they can be seen in reactive or normal lymph nodes from dogs without melanocytic tumors. (L) Intracytoplasmic melanin pigment is evident in a large epithelioid melanoma cell (arrow) among a population of reactive lymphoid cells. (E,I,J–L) Original magnification x 1,000. (H) Original magnification x 800.
In humans, BRAF mutation plays an important role in the pathogenesis of UV-exposed cutaneous melanoma; there is a low frequency of BRAF mutations in dogs, consistent with their differing etiologies (27) [LOE 2b, OEG B]. In canine malignant melanoma and melanocytoma, abnormalities of tumor suppressor expression or localization affecting p16, PTEN, p53, Rb and p21 have been noted, but explicit causal associations with malignant progression are yet to be demonstrated (28) [LOE 4b, OEG A]. In canine malignant forms, there is a gain of chromosomes (CFA) CFA 13 and CFA 17 and loss of CFA 22. Melanocytomas show fewer aberrations but gain locus CFA 20q15.3–17 (29) [LOE 4a, OEG A]. As in human mucosal melanomas, canine mucosal melanomas show a conserved deletion and insertion event on CFA 30 (HSA 15 in human melanoma), gain of c-MYC, and deletion of CDKN2A (30–32) [LOE 4a-5, OEG A]. Investigations into the genetics of canine melanoma have also revealed alterations in CFA 30 and CFA 10, causing MDM2 and CDK4 changes, and mutations on NRAS, KRAS, PTEN, and TP53 (29, 32, 33) [LOE 4a-4b, OEG A] are noted. PTPRJ has been shown to be inactivated in some canine mucosal melanomas (32) [LOE 4b, OEG B].
Melanoma subtypes exhibit great variation in their cytomorphology. Cells may mimic round cell, epithelioid, or spindle-shaped (Figure 1) neoplasms. Balloon-cell variants are occasionally seen (19, 25, 34, 35) [LOE 5, OEG D]. Individual neoplastic cells have a round to oval nucleus and prominent, large, pale to dark-staining nucleoli (6, 34, 36) [LOE 5, OEG D]. Anisocytosis and anisokaryosis are frequent. Variable numbers of mitoses can be observed (35, 36) [LOE 5, OEG D]. Inflammatory cell infiltrates will be present if there is tissue necrosis.
While many melanocytic tumors are heavily pigmented, making diagnosis relatively straightforward, melanin pigmentation is variable (35, 36) [LOE 5, OEG D]. The cytoplasmic melanin pigment granules may be fine and dust-like, needle-shaped, or coarse and granular. Small amounts of intracellular gray/black/green pigment may be seen (36) [LOE 5, OEG D]. If the neoplastic cells are disrupted during sample collection or preparation, melanin pigment may be evident in the background of the smear. Infrequently, melanomas may be devoid of melanin pigmentation, rendering cytological diagnosis challenging or impossible (6, 34) [LOE 5, OEG D].
Fine needle aspirates from lymph nodes can be extremely helpful for staging dogs with melanoma, particularly in patients with gross lymphadenomegaly (17) [LOE 4a, OEG A] (Figure 1). However, diagnosis of lymph node metastasis can be challenging due to the varied appearance of metastatic melanocytes and the presence of melanin-containing macrophages (melanophages) (37) [LOE 4b, OEG A]. Dermal melanin is taken up by macrophages, which then traffic to the lymph nodes. Differentiation between melanocytes and melanophages may require histology, immunohistochemistry, or other histochemical staining techniques.
The identification of neoplastic cells containing melanin pigment allows for a cytologic diagnosis of melanoma in many cases (2, 38) [LOE 5, OEG D]. However, poorly pigmented or amelanotic melanomas are more challenging to diagnose cytologically, and histopathology with or without immunohistochemistry is required to confirm a diagnosis (38) [LOE 5, OEG D].
Differentials for oral melanoma include squamous cell carcinoma, fibrosarcoma, lymphoma, and odontogenic tumors. Cutaneous melanoma can resemble any neoplastic and non-neoplastic skin mass, and for subungual melanoma, SCC and nail-bed infections are differentials (39) [LOE 5, OEG D]. Since oral tumor surfaces, especially those of the large melanocytic tumors, are often ulcerated and/or necrotic, large incisional biopsies, such as deep wedge or core punch biopsies are frequently required to make a definitive diagnosis. For oral tumors, biopsies should only be obtained through the mucosa and not the skin to avoid tumor seeding (40) [LOE 5, OEG D]. Tru-cut biopsy needles can be used, but samples obtained using this method are generally small, making melanin granule detection challenging and potentially limiting a diagnosis to “sarcoma” or “malignant tumor” on histopathology. If Tru-cut biopsies are used, sampling several different areas should be performed. Electrocautery should only be used for hemostasis once the biopsy tissue is removed since biopsy tissues could be damaged by the heat (41) [LOE 5, OEG D]. Finally, all resected tissues should be submitted and properly prepared with an optimized fixation ratio of 1-part tissue to 9-parts 10% neutral buffered formalin (41) [LOE 5, OEG D].
On histopathology, a proliferation of neoplastic cells at dermo-epidermal junctions referred to as “junctional activity,” and neoplastic cells found in intraepithelial nests can aid in the diagnosis of oral melanoma (35, 38) [LOE 5, OEG D]. These features are often observed because of the preservation of epithelium over melanocytic tumors. Thus, if one suspects a poorly pigmented or amelanotic melanoma, a biopsy should be taken, preserving part of the epithelium and improving diagnostic accuracy.
Specific histochemical staining techniques are employed to demonstrate the presence of melanin: Fontana-Masson (black) and Schmorl’s (blue–green). Bleaching helps visualization of intracellular structures by removing melanin from the tissues. Prussian blue stain aids differentiation of melanin granules from hemosiderin by identifying the presence of iron.
In amelanotic melanoma specimens, immunohistochemistry achieves a definitive diagnosis in almost all cases (19, 37) [LOE 4b-5, OEG B]. Melan-A, melanoma-associated antigen (PNL-2), tyrosine reactive protein (TRP)-1, and TRP-2 are all useful markers. Diagnostic sensitivities of these markers are reported as follows: Melan-A: 81.6%; PNL2: 89.8%; TRP-1: 55.1%; and TRP-2: 79.6%. An immunodiagnostic cocktail comprising all four of these antibodies had 100% specificity and 93.9% sensitivity for identification of canine oral amelanotic melanomas (42) [LOE 4b, OEG B]. For amelanotic spindle cell tumors that lack overlying epithelium, the immunodiagnostic cocktail may still fail to define tumor histogenesis. In that circumstance, RNA expression of TYR, CALD1 and CD34 has been shown to be discriminatory between spindloid oral melanoma and soft tissue sarcoma lesions (43) [LOE 5, OEG D].
The proliferation marker Ki-67 is useful to distinguish benign and malignant forms, and has prognostic value (26, 44, 45) [LOE 4a-4b, OEG A]. A higher percentage of cells express c-kit in melanocytomas than in malignant types (46) [LOE 4b, OEG A], but c-kit expression did not correlate with prognosis in malignant melanomas (46, 47) [LOE 4b, OEG A]. A further summary of prognostically-relevant histological features follows in section: Consideration of Prognostic Indicators and in Table 1.
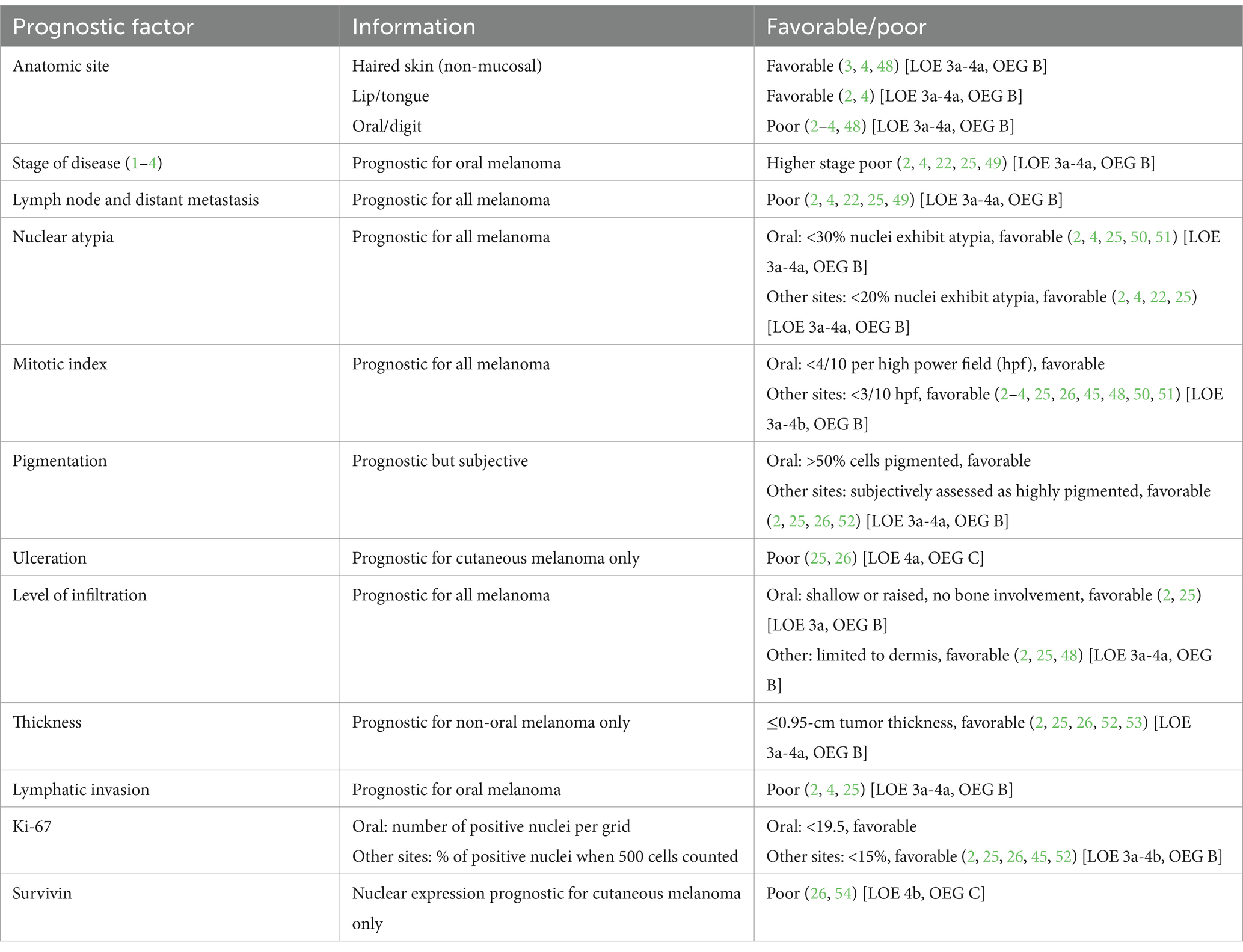
Table 1. Prognostic factors for canine melanoma.
In human studies, diagnostic biomarkers currently used to assist in the diagnosis of melanoma are usually specific only for melanocytic neoplasms and not necessarily for their ability to metastasize (55) [LOE 5, OEG D]. In dogs, the high molecular weight melanoma-associated antigen chondroitin sulfate proteoglycan-4 (CSPG4) was found to be a biomarker for malignant melanoma. However, there was no association between CSPG4 staining and clinical stage (56) [LOE 4a, OEG C]. High MicroRNA-126 was prognostic in canine melanoma for a shorter survival time (57) [LOE 4a, OEG C]. For uveal melanomas in dogs, 4 genes demonstrated increased expression in metastasizing compared with non-metastasizing tumors: HTR2B, FXR1, LTA4H, and CDH1 (58) [LOE 4c, OEG C]. For oral melanomas, a reduced expression of CXCL12 and an increased expression of APOBEC3A was associated with metastasis with classification accuracies of 94% in metastasizing tumors and 86% in non-metastasizing tumors (59) [LOE 4a, OEG C].
Circulating tumor DNA is detectable in the plasma of cancer-affected dogs. By performing droplet digital PCR (ddPCR) or PCR for antigen receptor rearrangement (PARR) methods, tumor-specific point mutations, copy number alterations, and chromosomal rearrangements were detected in cancer-affected dogs, including in 25% of oral malignant melanoma cases in one study (60) [LOE 4b, OEG B].
• A large and/or deep incisional/core biopsy, avoiding ulcerated or necrotic areas, is recommended to make an ACCURATE diagnosis of a melanocytic tumor. This is particularly pertinent in amelanotic or poorly pigmented melanoma.
• Oral melanoma must be biopsied via the mucosal surface, not the skin, to avoid the risk of preventing future curative surgery by iatrogenic tumor seeding.
• If a definitive diagnosis of a suspected melanoma is not made on routine histology, immunohistochemistry is indicated.
• In the coming years, it is likely that genomic testing will be able to yield a definitive melanoma diagnosis in cases in which histology and immunohistochemical evaluations have proved non-diagnostic.
Clinical staging of canine oral melanomas is straightforward. The goals are to determine the clinical stage according to the World Health Organization (61) [LOE 5, OEG D] (Box 1), to provide prognostic criteria and to guide therapeutic decision-making. Clinical staging evaluates three classical segments: the primary tumor (size and local extension, T segment), the locoregional lymph nodes (N segment), and the presence of distant metastasis (M segment), mainly in the lungs. A validated clinical stage scheme has been defined for canine oral melanoma. For all other locations and for feline melanoma, TNM-based staging applies.
BOX 1. Traditional world health organization TNM-based staging scheme for oral melanoma.
T: Primary tumor (longest diameter)
T1 <2 cm
T2 2-4 cm
T3 >4 cm
N: Locoregional lymph nodes
N0 No evidence of node involvement
N1 Histologic/cytologic evidence of node involvement
N2 Fixed nodes
M: Distant metastasis
M0 No evidence
M1 Evidence
Stage 1 = T1 N0 M0
Stage 2 = T2 N0 M0
Stage 3 = T1 N1 M0 or T2 N1 M0 or T3 N0 M0
Stage 4 = Any T, any N and M1
The size of the local tumor is the first criterion to evaluate. Primary tumor size is of prognostic significance and corresponds to the fundamentals of the TNM classification as follows:
Stage 1: a tumor less than 2 cm in diameter without any metastasis; Stage 2: a tumor greater than 2 and less than 4 cm in diameter without any metastasis; and Stage 3: a tumor greater than 4 cm in diameter and/or with confirmed lymph node involvement.
The tumor size can be clinically measured with a caliper or by cross-sectional imaging with computed tomography (CT). The longest diameter should be used for the classification. Although depth and nature of tissue invasion can be presumed to be prognostically significant, they have not been shown to supersede tumor size and are not included in the recognized clinical stage scheme.
Lymph node evaluation is an important step in the clinical staging of dogs with melanoma (2, 4, 22, 25, 49) [LOE 3a-4a, OEG B]. In a study with 100 dogs with oral melanomas, cytological or histopathological evidence of mandibular lymph node metastasis could be demonstrated in 53% of the cases, including in nodes of normal size (17) [LOE 4a, OEG C]. Likewise, subungual melanoma is highly malignant, with 19 to 30% of the dogs reportedly having regional lymph node metastasis at time of diagnosis (22, 62) [LOE 4a-4b, OEG C].
Lymph node size is an unreliable predictor of metastasis (17) [LOE 4a, OEG C]. Similarly, CT (63) [LOE 4c, OEG C] and cytology (37) [LOE 4b, OEG C] have been shown to carry low sensitivity and accuracy for assessment of cervical lymph node metastasis in dogs with oral melanoma. Thus, when lymph node status is uncertain, histopathology should remain the gold standard for the assessment of lymph nodes for metastatic disease with, in some instances, the need for immunohistochemistry (Melan-A) to aid differentiation between melanocytes and melanophages.
In oropharyngeal melanoma, bilateral or contralateral lymph node metastasis is not uncommon. Determination and selective biopsy of the sentinel lymph node is regarded by some to be a more advanced method of staging (37, 64–66) [LOE 4b-4c, OEG C]. However, when an oral tumor is present, the local lymphatic drainage may be abnormal. Metastasis to contralateral lymph nodes and to the retropharyngeal lymph nodes without mandibular lymph node involvement have been described (64, 67, 68) [LOE 4b, OEG B]. Currently, bilateral excisional biopsy of mandibular and retropharyngeal nodes for staging is advocated (62); removal via a single incision has been described (69) [LOE 4b, OEG D]. The parotid lymph node can also be included in the clinical staging. Furthermore, there is not only 1 lymph node per lymphocenter (e.g., dogs can have between 2 and 5 mandibular lymph nodes), and each could be metastatic.
Detection of lung metastasis is fundamental in clinical staging of dogs with melanoma. It can be performed by radiography with 3-view thoracic radiographs (70) [LOE 4a, OEG B]. However, CT is more sensitive than radiography for the detection of small pulmonary nodules, especially in large dogs (71–73) [LOE 4b-4c, OEG C]. The lower size threshold for detection is approximately 1 mm by CT, whereas it is between 7 and 9 mm by radiography. In canine cancer generally, only 9% of pulmonary nodules that can be detected by CT are visible on radiographs. In patients with thoracic radiographs without pulmonary nodules, 13 to 39% show nodules on a CT scan (71) [LOE 4c, OEG C].
Abdominal metastases are rare in dogs with melanoma, but have been described in the abdominal lymph nodes, liver, adrenal glands, and other sites (2, 74, 75) [LOE 4a-5, OEG B]. The use of abdominal ultrasonography or CT should be considered. Skeletal metastases are also recognized; clinically occult lesions would not be expected to be identified except by CT.
• Clinical stage determination is fundamental to therapeutic decision-making for canine and feline melanoma.
• We recommend that the size and site of the primary tumor are recorded prior to further intervention to improve communication between colleagues in the event that patient care might be shared.
• Thoracic imaging can be performed by radiography (3-view radiography is preferred), but CT is more sensitive.
• Abdominal metastases are rare but have been described so abdominal imaging would be required to achieve thorough clinical stage determination.
Surgical resection using wide margins is currently the mainstay of therapy for the local control of melanomas, regardless of primary location.
In canine oral melanoma, surgical planning using thin-slice contrast CT with multiplanar reconstruction is regarded as the gold standard, especially in all maxillary and caudal mandibular locations. Because resection of melanomas affecting the jaw usually involves a segmental mandibulectomy or maxillectomy, resection width in the bone is based on the detectable bony changes on CT (76) [LOE 4b, OEG B]. For the surgical techniques of jaw resection, please refer to the respective surgical textbooks or monographs.
A minimal surgical margin for melanomas has not been established but, in our experience, a minimum of 1 to 2 cm of healthy-looking bone is usually sufficient to attain clean margins. On the soft tissue side (e.g., lip, sublingual floor of the mouth, soft palate), the surgeon should strive for wider margins (i.e., a minimum of 2 cm). Histopathologic confirmation of completeness of excision is important; all bony and soft tissue margins should be histologically evaluated. There is no consensus among veterinary pathologists regarding surgical margin assessment. Therefore, the veterinarian should discuss with their pathology lab how completeness of resection is assessed and how assessment can be optimized (77, 78) [LOE 3a, OEG D]. Helpful techniques to improve margin assessment include applying surgical ink to the cut surfaces before fixation in formalin or taking resection margin biopsies from bony and soft tissue margins, which are submitted in a separate container. With the latter technique, the surgeon can define which and how many sites are examined histologically. In 70 dogs treated with curative-intent jaw resections (49) [LOE 4a, OEG C], resection of 2 to 3 cm bone margins and 1 cm soft tissue margins resulted in tumor-free margins in almost 73% of cases. Only 17% developed local tumor recurrence. The progression-free interval in this study was 508 days, with a median survival time (MST) of 723 days. In a separate study (79) [LOE 4a, OEG C], almost 80% of resections (73/92) were considered complete after “wide” excision. Recurrence rate was 8.3% (6/73) and the MST was 354 days.
In cats, oral melanoma is rare. A case series of 8 cats treated with radical mandibulectomy reported 6/8 adequately prehending and swallowing food by 3 months after surgery (80) [LOE 4c, OEG C]. In essence, the same resection guidelines apply in cats and dogs, but in cats, less is known about the resection margins necessary to obtain tumor-free margins. Resection width in cats is limited by the much smaller anatomical size of the oral structures. This makes both critical assessment of the resectability of the tumor by appropriate imaging, as well as examination of surgical bony and soft tissue margins, even more important.
For subungual melanomas, amputation of the affected digit at the metacarpophalangeal or metatarsophalangeal joint is the treatment of choice and usually results in tumor-free margins (81) [LOE 4c, OEG C]. Amputation at the level of the interphalangeal joints is contraindicated because tumor-free soft tissue margins are frequently not achieved. In large tumors, taking resection margin biopsies of the adjacent skin and soft tissue may be indicated to assess completeness of resection.
Melanoma of the foot pad can be addressed by partial or complete full-thickness resection of the affected foot pad, including the entire fat cushion layer. Assessment of the lateral and deep margins is important, and the use of surgical ink or tumor bed biopsies is recommended. Reconstruction of a weight-bearing foot pad surface can be achieved by transposition of one or both of the second and fifth digital pads using a phalangeal fillet technique (82, 83) [LOE 4c-5, OEG C].
In non-metastatic melanoma of the haired skin, wide surgical resection is the treatment of choice, whenever anatomically possible. Again, evidence-based recommendations for the resection width have not been established, but most authors recommend a 2 to 3 cm lateral margin and a subfascial resection for the deep extension. Assessment of completeness of resection, using techniques already described, is recommended.
In ocular melanoma, the location of the tumor on or in the eye is of importance in choosing surgical technique, and outlined as follows (7, 84) [LOE 2a, OEG D]:
1. Conjunctival melanomas in dogs are best treated by surgical resection followed by cryotherapy. If the third eyelid is affected, it should be removed completely. In larger tumors, enucleation is the treatment of choice (7) [LOE 2a, OEG D]. In cats, conjunctival melanomas are highly malignant. Treatment typically comprises orbital exenteration after thorough staging (85) [LOE 4b, OEG C].
2. Limbal melanomas in dogs are frequent and usually affect the dorsal limbus. Most limbal melanomas have a benign behavior, and eye-preserving resection of the tumor by keratectomy/sclerectomy is usually the treatment of choice. Corneal transplant or transplantation of other appropriate tissue (ear cartilage, synthetic material) may be used for reconstruction of large defects. In cases with incomplete resection, adjuvant cryotherapy, photocoagulation, or Strontium-90 usually has a curative effect (86, 87) [LOE 4b, OEG C].
3. Benign iris melanocytomas can be treated successfully by transcorneal laser photocoagulation (7, 84) [LOE 2a, OEG D].
4. Uveal melanomas in dogs and cats are usually locally advanced and therefore best treated by enucleation. The resection margin at the cut edge of the optic nerve should be assessed by histopathology (7, 84) [LOE 2a, OEG D]. A proportion of histologically malignant uveal melanomas in dogs do not progress following complete removal (8) [LOE 4a, OEG C].
In nasal planum melanoma in cats, a wide to radical resection (nosectomy) is recommended for both benign and malignant melanoma. Benign feline nasal planum melanoma may progress to malignancy, and radiation therapy does not result in durable remissions (13) [LOE 4c, OEG C].
Surgical excision of tributary lymph nodes in oral, subungual, and cutaneous melanomas adds important information regarding the clinical stage of the disease and is therefore frequently recommended. However, the therapeutic value of lymph node dissection in canine melanoma has not been studied systematically. Based on the evidence available, lymph node biopsy is more likely a diagnostic rather than a therapeutic procedure and may not offer a survival advantage.
Radiotherapy forms an integral part of the management of canine oral melanomas, both as a primary and an adjuvant therapy (88–95) [LOE 4a-4c, OEG B]. It is also described in the context of feline oral melanomas and in canine non-oral melanoma treatment; although the indications are fewer, responses appear broadly comparable (94, 96–98) [LOE 4a-4c, OEG C].
Although the reason remains controversial, melanoma exhibits sensitivity to coarsely fractionated radiation protocols, with attendant benefits in terms of risk of acute toxicity, costs, and time. This does not mean that melanomas are insensitive to other, more fractionated courses of therapy. An optimal protocol remains undefined. In the context of oral melanoma, it is noteworthy that the canine mandible is a bone that is sensitive to hypofractionation, increasing the risk of osteoradionecrosis (99, 100) [LOE 4c, OEG C]. Lower dose per fraction protocols can be used to reduce late effect incidence in dogs with better prognoses (99) [LOE 5, OEG D].
Treatment protocols reported range from daily 3Gy fractions for 4 weeks (57Gy) through to weekly 10Gy fractions for 3 weeks (30Gy). Most published studies are retrospective (88–90, 95, 96, 101, 102) [LOE 4a-4c, OEG B]. This and the variety of fractionation protocols, equipment used, concomitant therapies, and clinical stage of cancer treated make comparisons between protocols challenging. Outcomes appear to differ between cases that undergo radiotherapy in the macroscopic and the microscopic (post-surgery) settings (89, 93, 94, 101) [LOE 4a-4c, OEG B].
Macroscopic tumors are expected to shrink or disappear in more than 80% of cases; responses become evident within 2 to 3 weeks of initiating therapy. Reported average remission durations range from 3 to 9 months (89, 93, 94, 101) [LOE 4a-4c, OEG B]. Approximately half of all cases experience local recurrence (89, 101) [LOE 4a-4c, OEG C]. Microscopic tumors receiving adjuvant radiotherapy are reported to experience local recurrence in approximately 25% of cases (89) [LOE 4a, OEG C]. Longer remission duration at the primary tumor site is associated with an increasing risk of the development of distant metastasis (90, 101) [LOE 4b-4c, OEG C].
Multiple small studies describe the impact of radiotherapy and chemotherapy in combination. There is an absence of evidence that combining the treatments, with or without surgery, leads to a consistent improvement in outcome (88–90, 101, 102) [LOE 4a-4c, OEG C]. Most studies have failed to demonstrate a positive survival impact of the addition of chemotherapy. However, the small number of cases reported, and a lack of uniformity of tumors and treatments, may mask a genuine difference in outcome. Although statistically significant differences in outcomes may not exist, data from small studies suggested that time to local recurrence was longer in oral melanoma cases receiving adjuvant radiotherapy and chemotherapy in combination compared with adjuvant radiotherapy alone (101) [LOE 4c, OEG C], and time to progression was improved in dogs receiving radiotherapy for melanomas at any site when temozolomide was added to treatment (94) [LOE 4b, OEG C].
There is a general acceptance that technological advances to improve accuracy of radiation targeting will enable greater differentiation between target and non-target tissues, delivery of greater doses of radiation to cancer tissues, and a superior outcome for the patient (103, 104) [LOE 5, OEG D]. Data do not yet exist to substantiate this hypothesis in the field of canine oral melanoma. The complex anatomy of the oral cavity and the infiltrative nature of malignant melanoma apply limits to the improvements that can be gained, but it appears reasonable to believe that further improvements in locoregional melanoma control are possible.
While locoregional tumor control can be achieved by means of resection and/or irradiation of the primary tumor and regional lymph nodes, development of metastatic disease very often leads to death. Adjuvant systemic therapy is offered to patients without evidence of macroscopic metastases that are at high risk of developing microscopic disease, and therefore distant metastasis.
A therapeutic vaccine containing xenogeneic plasmid DNA with an insert encoding human tyrosinase (ONCEPT® Canine Melanoma Vaccine) has been evaluated in a prospective, multicenter clinical trial in dogs with locally controlled (surgically removed primary tumor, regional lymph nodes, and irradiation for incompletely resected tumors) stage 2 and 3 oral malignant melanoma (105) [LOE 2c, OEG B]. The vaccine was delivered transdermally by use of a needle-free intramuscular vaccination device in 4 doses every 2 weeks, followed by booster injections at 6-month intervals. Statistically significant improvement in survival time was observed (MST not reached; >50% of dogs survived longer than 437 days) versus the classic local-control-only treatment protocol received by a historical control group (MST of 324 days). Another group of vaccinated dogs with stage 1 to 3 oral malignant melanoma reached an MST of 445 days (106) [LOE 4a, OEG C]. Two retrospective clinical studies did not reveal any benefit from the use of the vaccine but, in both studies, local control of the disease was not rigorously achieved. In the first study, less than 35% of patients were treated with surgical margin 1 mm or greater (107) [LOE 4b, OEG C], and in the second, 37% of patients had an incomplete surgical margin (79) [LOE 4c, OEG C]. This reinforces the label recommendation that the vaccine should be used with optimal local disease control (complete surgical margin or radiation therapy if surgical margin was incomplete).
Dogs with digit melanoma treated by digit amputation and a murine tyrosinase DNA vaccine lived significantly longer than those classically treated by digit amputation only (62) [LOE 4a, OEG C]. Significant prognostic factors were presence or lack of metastases at the time of diagnosis (MST of 105 and 533 days, respectively) and stage of the disease (MSTs >952, >1,093, 321, and 76 days for dogs with stage 1, 2, 3, and 4, respectively).
The canine ONCEPT® vaccine can be safely administered to cats with oral, ocular/periorbital, dermal, mucocutaneous, lip, and subcutaneous melanomas. There are no data regarding its efficacy (108) [LOE 4b, OEG C].
For canine oral, digital, and cutaneous melanoma, there is no evidence that addition of cytotoxic drugs (carboplatin, cisplatin, melphalan) to surgical treatment or radiotherapy leads to a significant increase in survival time (79, 89, 95, 101, 102, 109) [LOE 4a-c, OEG B]. Cytotoxic drugs (cisplatin 10–30 mg/m2 intravenously or carboplatin 90 mg/m2 intravenously) may have a role as a radiation sensitizer given once weekly approximately 1 h before radiotherapy in the management of dogs with incompletely excised oral melanomas (90) [LOE 4b, OEG C]. The median time to metastasis was 10.2 months, the MST was 11.9 months, and the local recurrence rate was 15% (90) [LOE 4b, OEG C]. As previously mentioned, adjuvant temozolomide after radiotherapy prolonged time to progression without a significant influence on survival time (94) [LOE 4c, OEG C].
Overall response rates for treatment in dogs with measurable disease are disappointing and have not exceeded 18% for dogs treated with cisplatin and piroxicam (110) [LOE 4c, OEG C] or 28% for dogs treated with carboplatin (111) [LOE 4b, OEG C]. Furthermore, complete responses are rare and short in duration. The ONCEPT® vaccine is not indicated for macroscopic disease, but there is information about its use in this setting with an MST of 179 days (106) [LOE 4c, OEG C].
Multiple studies have demonstrated a correlation between the expression of COX-2 in canine melanoma and/or melanoma cell lines and proliferation and survival of cells (112, 113) [LOE 2b, OEG B], but no clinical trials investigating nonsteroidal anti-inflammatory drug (NSAID) effectiveness in canine and feline melanoma cases have been published. Local treatment modalities, such as intralesional cisplatin implants or electrochemotherapy with intralesional bleomycin, have been reported for a limited number of patients (114, 115) [LOE 4a-b, OEG C]. Cytotoxic drugs in a metronomic setting could have some influence for immune cells in the microenvironment of a tumor, but the clinical significance of this remains unknown (79) [LOE 4c, OEG C]. Scientific information concerning the treatment of malignant melanoma with tyrosine kinase inhibitors is anecdotal. Masitinib used for stage 3 and 4 malignant melanoma showed only mild effectiveness (116) [LOE 4c, OEG C]. Checkpoint inhibitors successfully used for human melanomas are not currently available for canine and feline patients though the first caninized anti-PD-1 monoclonal antibody has recently been awarded conditional licensure in the United States for treatment of canine melanoma. Gilvetmab was given to 25 dogs with stage 2 or 3 melanoma. Complete response was noted in 2/25, partial response in 3/25 and stable disease in 10/25 cases (117) [LOE 4b, OEG D].
• Surgical resection using wide margins is currently the mainstay of therapy for the local control of melanomas, regardless of primary location. CT imaging is the optimal strategy for surgical planning of jaw-invasive melanoma.
• Surgical excision of tributary lymph nodes in oral, subungual, footpad and cutaneous melanoma is recommended. It adds important information regarding the clinical stage of the disease and it improves local tumor control.
• When adequate local control cannot be achieved surgically, radiotherapy should be considered.
• Explicit recommendations for treatment of canine oral melanoma are presented in Figure 2.
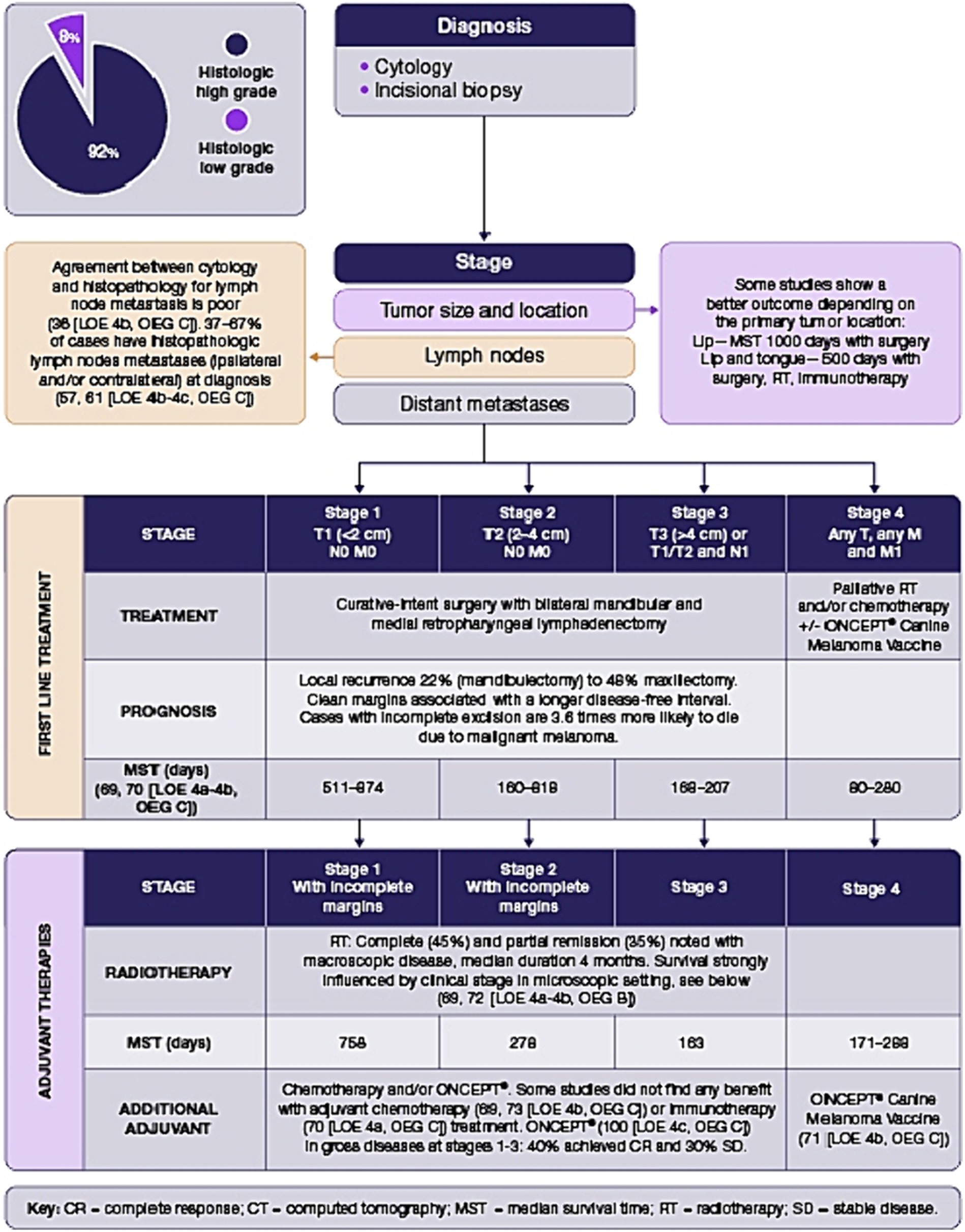
Figure 2. Oral melanoma decision tree.
• An increased array of immunotherapy options is predicted to become available for treatment of melanoma. As a result, radiotherapy is likely to assume greater therapeutic significance because it increases epitope expression.
• Immunotherapy appears to be the optimal method of treating microscopic disease, provided that macroscopic disease is effectively controlled.
• The ONCEPT® Canine Melanoma Vaccine has an evidence base for treatment of stage 2 and 3 malignant melanoma with adequate local tumor control.
• There is limited scientific literature to support the use of other medical therapies for melanoma. A pivotal study of gilvetmab in canine stage 3 melanoma is ongoing at the time of writing.
The definition and identification of existing or new prognostic factors in canine melanoma should follow the regimented, systematic approach already described in the literature to clearly identify and consider these factors as truly valuable to the clinician (25, 118) [LOE 2a-3a, OEG C]. Location is the major prognostic factor, although it is not completely predictive of local invasiveness and metastatic potential. The oral/mucosal subtype carries the worst prognosis, with a high degree of local invasiveness and high metastatic potential, and reported MST between 3 and 24 months, according to the stage. Oral benign melanomas might exist (50) [LOE 4a, OEG C]; however, caution is recommended because of their unpredictable behavior (2) [LOE 5, OEG D]. Lip and tongue locations might have a better prognosis compared with other locations within the mouth; well-differentiated mucosal forms have been described (18) [LOE 4a, OEG C]. Melanomas involving the haired skin are often cured with a clean-margin surgical excision (48) [LOE 4a, OEG C]; however, mitotic index of 3/10hpf or higher, high Ki-67 index, and survivin expression seem to be related to metastatic potential and reduced overall survival (26, 52, 54, 119) [LOE 4a-4b, OEG C]. Ulceration might be a negative prognostic factor in cutaneous tumors (26, 52, 81) [LOE 4a-4b, OEG C]. Melanoma in the digits is generally malignant (86%), and all subungual melanocytic tumors are malignant (5) [LOE 2c, OEG B]. They have a high metastatic propensity, with regional or distant pulmonary metastasis evident at the time of diagnosis in 30 to 40% of cases, and subsequent development of regional or distant metastasis in most of the remainder (22, 62) [LOE 4a, OEG B]. Dogs without lymph node or distant metastasis treated by digit amputation have reported median survival times of approximately 12 months, with 1- and 2-year survival rates of 42 to 57% and 11 to 13%, respectively (22, 23, 62, 120) [LOE 4a, OEG B]. Depth of infiltration has been suggested as a negative prognostic indicator for oral melanoma; lack of invasiveness beyond the dermis might carry a favorable prognosis in the cutaneous form (25, 26, 52) [LOE 2-4a, OEG A]. The Ki-67 index is also prognostic for cutaneous and oral melanoma (2, 26, 45) [LOE 2-4b, OEG A] (Table 1).
Following a modified World Health Organization staging system from I to IV, based on tumor size, lymph node involvement, and metastases in dogs with oral melanomas, has been found to be extremely prognostic (49) [LOE 4a, OEG C]. MSTs for dogs with oral melanoma treated with surgery are 511 to 874 days, 160 to 818 days, and 168 to 207 days with stage 1, 2, and 3 disease, respectively (2, 49) [LOE 2-4a, OEG A]. More recent reports suggest dogs with stage 1 oral melanoma treated with standardized therapies, including surgery, radiotherapy, and/or chemotherapy, have an MST of approximately 12 to 14 months, with most dogs dying of distant metastatic disease, not local recurrence (2, 90) [LOE 3a-4b, OEG B].
In cats, tumor location, mitotic index and presence of intratumoral necrosis have been attributed with prognostic significance. A two-tier grading scheme has been proposed, with tumors of the nose, lip and oral cavity considered high-grade if mitotic index is greater than or equal to four OR if there are confluent aggregates of necrotic neoplastic cells. Other non-ocular tumors are considered high-grade if they exhibited BOTH a high mitotic index and intratumoral necrosis (121) [LOE 4a, OEG C]. With so-defined high-grade tumors, median survival time was 90 days whereas only 19% of low-grade tumors adversely impacted survival.
There are no specific guidelines regarding referral considerations for dogs with melanoma, as this is likely based on a multitude of factors. Clinician experience and comfort level, access to diagnostic imaging, and proximity to referral have an impact. Tumor location impacts decision-making, as mandibular and maxillary tumors are more likely to be referred due to the higher level of expertise needed for surgical excision. Access to ONCEPT® Canine Melanoma Vaccine will also affect decision-making as it is limited to selected veterinarians in some geographies and is not available at all in others.
If a referral is to be sought, tumor size should be recorded before excision/referral, as this is deemed a strong prognostic factor. If a biopsy or excision is performed prior to referral, pre-operative digital photographs of the lesion can greatly assist patient assessment and treatment planning. Similarly, staging (imaging and lymph node assessment), when feasible, is paramount before referral, as this may impact the therapy and prognosis. It is also important to note that incomplete excision is associated with poorer outcomes so, if complete excision may not be possible in primary care, referral should be considered.
The ultimate goal is to provide the best options for patients to extend quality of life and survival, either within the primary care or referral hospital setting.
Enrollment of patients into clinical trials will help to address important unanswered clinical questions.
GP: Writing – review & editing, Writing – original draft, Supervision, Project administration, Methodology, Conceptualization. JB: Writing – review & editing, Writing – original draft. FC-V: Writing – review & editing, Writing – original draft. CC: Writing – review & editing, Writing – original draft. DJ: Writing – review & editing, Writing – original draft. MK: Writing – review & editing, Writing – original draft. TK: Writing – review & editing, Writing – original draft. DL: Writing – review & editing, Writing – original draft. FQ: Writing – review & editing, Writing – original draft. AR: Writing – review & editing, Writing – original draft. PV: Writing – review & editing, Writing – original draft. PB: Writing – review & editing, Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors are very grateful to Vincent Krogmann and Annalena Boeing of Boehringer Ingelheim Animal Health for facilitating and funding in-person and virtual meetings that enabled completion of this project, and to Helen Kedward-Dixon of Circa Healthcare for invaluable editorial support.
PB receives a yearly minority royalty stream payment through Boerhinger Ingelheim Animal Health (BIAH) for a license related to xenogeneic DNA patent #US20020150589A1. He also serves on the BIAH VOAB (Veterinary Oncology Advisory Board) and is a paid speaker on various oncology topics.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gillard, M, Cadieu, E, De Brito, C, Abadie, J, Vergier, B, Devauchelle, P, et al. Naturally occurring melanomas in dogs as models for non-UV pathways of human melanomas. Pigment Cell Melanoma Res. (2014) 27:90–102. doi: 10.1111/pcmr.12170
2. Bergman, P, Selmic, LE, and Kent, MS. Melanoma In: D Vail, D Thamm, and J Liptak, editors. Withrow and MacEwen’s small animal clinical oncology. 6th ed. St. Louis, MO: Elsevier (2020). 367–81.
3. Smith, SH, Goldschmidt, H, and Mcmanus, PM. A comparative review of melanocytic neoplasms. Vet Pathol. (2002) 39:651–78. doi: 10.1354/vp.39-6-651
4. Goldschmidt, MH. Pigmented lesions of the skin. Clin Dermatol. (1994) 12:507–14. doi: 10.1016/0738-081x(94)90217-8
5. Grassinger, JM, Floren, A, Müller, T, Cerezo-Echevarria, A, Beitzinger, C, Conrad, D, et al. Digital lesions in dogs: a statistical breed analysis of 2912 cases. Vet Sci. (2021) 8:136. doi: 10.3390/vetsci8070136
6. Nishiya, AT, Massoco, CO, Felizzola, CR, Perlmann, E, Batschinski, K, Tedardi, MV, et al. Comparative aspects of canine melanoma. Vet Sci. (2016) 3:7. doi: 10.3390/vetsci3010007
7. Finn, M, Krohne, S, and Stiles, J. Ocular melanocytic neoplasia. Compend Contin Educ Vet. (2008) 30:19–25.
8. Wilcock, BP, and Peiffer, RL Jr. Morphology and behavior of primary ocular melanomas in 91 dogs. Vet Pathol. (1986) 23:418–24. doi: 10.1177/030098588602300411
9. Van der Weyden, L, Brenn, T, Patton, EE, Wood, GA, and Adams, DJ. Spontaneously occurring melanoma in animals and their relevance to human melanoma. J Pathol. (2020) 252:4–21. doi: 10.1002/path.5505
10. Miller, WH, Scott, DW, and Anderson, WI. Feline cutaneous melanocytic neoplasms: a retrospective analysis of 43 cases (1979–1993). Vet Dermatol. (1993) 4:19–26. doi: 10.1111/j.1365-3164.1993.tb00185.x
11. Chamel, G, Jérôme Abadie, J, Albaric, O, Labrut, S, Ponce, F, and Catherine, IC. Non-ocular melanomas in cats: a retrospective study of 30 cases. J Feline Med Surg. (2017) 19:351–7. doi: 10.1177/1098612X15625355
12. Patnaik, AK, and Mooney, S. Feline melanoma: a comparative study of ocular, Oral and dermal neoplasms. Vet Pathol. (1988) 25:105–12. doi: 10.1177/030098588802500201
13. Reck, A, and Kessler, M. Melanocytic Tumours of the nasal Planum in cats: 10 cases (2004-2019). J Small Anim Pract. (2021) 62:131–6. doi: 10.1111/jsap.13265
14. Ramos-Vara, J, Beissenherz, M, Miller, M, Johnson, G, Pace, L, Fard, A, et al. Retrospective study of 338 canine Oral melanomas with clinical, histologic, and Immuno-histochemical review of 129 cases. Vet Pathol. (2000) 37:597–608. doi: 10.1354/vp.37-6-597
15. Todoroff, RJ, and Brodey, RS. Oral and pharyngeal neoplasia in the dog: a retrospective survey of 361 cases. J Am Vet Med Assoc. (1979) 175:567–71.
16. Wallace, J, Matthiesen, DT, and Patnaik, AK. Hemimaxillectomy for the treatment of Oral Tumours in 69 dogs. Vet Surg. (1992) 21:337–41. doi: 10.1111/j.1532-950X.1992.tb01707.x
17. Williams, LE, and Packer, RA. Association between lymph node size and metastasis in dogs with Oral malignant melanoma: 100 cases (1987-2001). J Am Vet Med Assoc. (2003) 222:1234–6. doi: 10.2460/javma.2003.222.1234
18. Esplin, DG. Survival of dogs following surgical excision of histologically well-differentiated melanocytic neoplasms of the mucous membranes of the lips and oral cavity. Vet Pathol. (2008) 45:889–96. doi: 10.1354/vp.45-6-889
19. Prouteau, A, and André, C. Canine melanomas as models for human melanomas: clinical, histological, and genetic comparison. Genes (Basel). (2019) 10:501. doi: 10.3390/genes10070501
20. Graf, R, Pospischil, A, Guscetti, F, Meier, D, Welle, M, and Dettwiler, M. Cutaneous tumors in Swiss dogs: retrospective data from the Swiss canine Cancer registry, 2008-2013. Vet Pathol. (2018) 55:809–20. doi: 10.1177/0300985818789466
21. Trappler, MC, Popovitch, CA, Goldschmidt, MH, Goldschmidt, KA, and Ribson, RE. Scrotal tumors in dogs: a retrospective study of 676 cases (1986-2010). Can Vet J. (2014) 55:1229–33.
22. Henry, CJ, Brewer, WG Jr, Whitley, EM, Tyler, JW, Ogilvie, GK, Norris, A, et al. Veterinary cooperative oncology group (VCOG). Canine digital tumors: a veterinary cooperative oncology group retrospective study of 64 dogs. J Vet Intern Med. (2005) 19:720–4. doi: 10.1111/j.1939-1676.2005.tb02751.x
23. Wobeser, BK, Kidney, BA, Powers, BE, Withrow, SJ, Mayer, MN, Spinato, MT, et al. Diagnoses and clinical outcomes associated with surgically amputated canine digits submitted to multiple veterinary diagnostic laboratories. Vet Pathol. (2007) 44:355–61. doi: 10.1354/vp.44-3-355
24. Hernandez, B, Adissu, HA, Wei, B-R, Michael, HT, Merlino, G, and Simpson, RM. Naturally occurring canine melanoma as a predictive comparative oncology model for human mucosal and other triple wild-type melanomas. Int J Mol Sci. (2018) 19:394. doi: 10.3390/ijms19020394
25. Smedley, RC, Spangler, WL, Esplin, DG, Kitchell, BE, Bergman, PJ, Ho, HY, et al. Prognostic markers for canine melanocytic neoplasms: a comparative review of the literature and goals for future investigation. Vet Pathol. (2011) 48:54–72. doi: 10.1177/0300985810390717
26. Smedley, RC, Bongiovanni, L, Bacmeister, C, Clifford, CA, Christensen, N, Dreyfus, JM, et al. Diagnosis and histopathologic prognosis of canine melanocytic neoplasms: a consensus of the oncology-pathology working group. Vet Comp Oncol. (2022) 20:739–51. doi: 10.1111/vco.12827
27. Mochizuki, H, Kennedy, K, Shapiro, SG, and Breen, M. BRAF mutations in canine cancers. PLoS One. (2015) 10:e0129534. doi: 10.1371/journal.pone.0129534
28. Koenig, A, Bianco, SR, Fosmire, S, Wojcieszyn, J, and Modiano, JF. Expression and significance of p53, rb, p21/waf-1, p16/ink-4a, and PTEN tumor suppressors in canine melanoma. Vet Pathol. (2002) 39:458–72. doi: 10.1354/vp.39-4-458
29. Poorman, K, Borst, L, Moroff, S, Roy, S, Labelle, P, Motsinger-Reif, A, et al. Comparative cytogenetic characterization of primary canine melanocytic lesions using Array CGH and fluorescence in situ hybridization. Chromosom Res. (2015) 23:171–86. doi: 10.1007/s10577-014-9444-6
30. Schiffman, JD, and Breen, M. Comparative oncology: what dogs and other species can teach us about humans with Cancer. Philos Trans R Soc Lond Ser B Biol Sci. (2015) 370:20140231. doi: 10.1098/rstb.2014.0231
31. Curtin, JA, Fridlyand, J, Kageshita, T, Patel, HN, Busam, KJ, Kutzner, H, et al. Distinct sets of genetic alterations in melanoma. N Engl J Med. (2005) 353:2135–47. doi: 10.1056/NEJMoa050092
32. Hendricks, WPD, Zismann, V, Sivaprakasam, K, Legendre, C, Poorman, K, Tembe, W, et al. Somatic inactivating PTPRJ mutations and dysregulated pathways identified in canine malignant melanoma by integrated comparative genomic analysis. PLoS Genet. (2018) 14:e1007589. doi: 10.1371/journal.pgen.1007589
33. Wong, K, van der Weyden, L, Schott, CR, Foote, A, Constantino-Casas, F, Smith, S, et al. Cross-species genomic landscape comparison of human mucosal melanoma with canine Oral and equine melanoma. Nat Commun. (2019) 10:353. doi: 10.1038/s41467-018-08081-1
34. Friedrichs, KR, and Young, KM. Diagnostic cytopathology in clinical oncology In: D Vail, D Thamm, and J Liptak, editors. Withrow and MacEwen’s small animal clinical oncology. 6th ed. St. Louis, MO: Elsevier (2020). 141.
35. Goldschmidt, MH, Dunstan, RW, Stannard, AA, Von Tscharner, C, Walder, EJ, and Yager, JA. Histological Classification of Epithelial and Melanocytic Neoplasms of the Skin of Domestic Animals In: World Health Organization, editor. World Health Organization International Histological Classification of Neoplasms of Domestic Animals, 2nd series, vol. 3. Washington, DC: Armed Forces Institute of Pathology (1998). 38–40.
36. Raskin, R, and Meyer, D. “Canine and feline cytology”. A color atlas and interpretation guide. 3rd Edn. Philadelphia, PA: Saunders, pp. 73–75. (2015).
37. Grimes, JA, Matz, BM, Christopherson, PW, Koehler, JW, Cappelle, KK, Hlusko, KC, et al. Agreement between cytology and histopathology for regional lymph node metastasis in dogs with melanocytic neoplasms. Vet Pathol. (2017) 54:579–87. doi: 10.1177/0300985817698209
38. Munday, JS, Lohr, CV, and Kiupel, M. Tumors of the alimentary tract In: DJ Meuten, editor. Tumors in domestic animals. 5th ed. West Sussex, NJ: John Wiley and Sons Ltd. (2017). 499–601.
39. Kobayashi, T. Melanoma In: K Cohn and E Cote, editors. Clinical veterinary advisor: Dogs and cats. 4th ed. St. Louis, MO: Elsevier (2020). 644–5.
40. Liptak, JM, and Lascelles, BDX. Oral tumors In: ST Kudning and B Seguin, editors. Veterinary surgical oncology. West Sussex, NJ: John Wiley and Sons Ltd. (2012). 119–77.
41. Kamstock, DA, Ehrhart, EJ, Getzy, DM, Bacon, NJ, Rassnick, KM, Moroff, SD, et al. American College of Veterinary Pathologists’ oncology committee. Recommended guidelines for submission, trimming, margin evaluation, and reporting of tumor biopsy specimens in veterinary surgical pathology. Vet Pathol. (2011) 48:19–31. doi: 10.1177/0300985810389316
42. Smedley, RC, Lamoureux, J, Sledge, DG, and Kiupel, M. Immunohistochemical diagnosis of canine Oral Amelanotic melanocytic neoplasms. Vet Pathol. (2011) 48:32–40. doi: 10.1177/0300985810387447
43. Tsoi, MF, Thaiwong, T, Smedley, RC, Noland, E, and Kiupel, M. Quantitative expression of TYR, CD34, and CLAD1 discriminates between canine Oral malignant melanomas and soft tissue sarcomas. Front Vet Sci. (2021) 8:701457. doi: 10.3389/fvets.2021.701457
44. Roels, S, Tilmant, K, and Ducatelle, R. PCNA and Ki67 proliferation markers as criteria for prediction of clinical behaviour of melanocytic tumors in cats and dogs. J Comp Pathol. (1999) 121:13–24. doi: 10.1053/jcpa.1998.0291
45. Bergin, IL, Smedley, RC, Esplin, DG, Spangler, WL, and Kiupel, M. Prognostic evaluation of Ki67 threshold value in canine Oral melanoma. Vet Pathol. (2011) 48:41–53. doi: 10.1177/0300985810388947
46. Gomes, J, Queiroga, FL, Prada, J, and Pires, I. Study of C-kit Immunoexpression in canine cutaneous melanocytic tumors. Melanoma Res. (2012) 22:195–201. doi: 10.1097/CMR.0b013e32835273f9
47. Murakami, A, Mori, T, Sakai, H, Murakami, M, Yanai, T, Hoshino, Y, et al. Analysis of KIT expression and KIT exon 11 mutations in canine Oral malignant melanomas. Vet Comp Oncol. (2011) 9:219–24. doi: 10.1111/j.1476-5829.2010.00253.x
48. Laver, T, Feldhaeusser, BR, Robat, CS, Baez, JL, Cronin, KL, Buracco, P, et al. Post-surgical outcome and prognostic factors in canine malignant melanomas of the haired skin: 87 cases (2003-2015). Can Vet J. (2018) 59:981–7.
49. Tuohy, JL, Selmic, LE, Worley, DR, Ehrhart, NP, and Withrow, SJ. Outcome following curative-intent surgery for Oral melanoma in dogs: 70 cases (1998–2011). J Am Vet Med Assoc. (2014) 245:1266–73. doi: 10.2460/javma.245.11.1266
50. Spangler, WL, and Kass, PH. The histologic and epidemiologic bases for prognostic considerations in canine melanocytic neoplasia. Vet Pathol. (2006) 43:136–49. doi: 10.1354/vp.43-2-136
51. Hahn, KA, DeNicola, DB, Richardson, RC, and Hahn, EA. Canine Oral malignant melanoma: prognostic utility of an alternative staging system. J Small Anim Pract. (1994) 35:251–6. doi: 10.1111/j.1748-5827.1994.tb03273.x
52. Laprie, C, Abadie, J, Amardeilh, MF, Net, JL, Lagadic, M, and Delverdier, M. MIB-1 immunoreactivity correlates with biologic behaviour in canine cutaneous melanoma. Vet Dermatol. (2001) 12:139–47. doi: 10.1046/j.1365-3164.2001.00236.x
53. Silvestri, S, Porcellato, I, Mechelli, L, Menchetti, L, Rapastella, S, and Brachelente, C. Tumor Thickeness and modified Clark level in canine cutaneous melanocytic tumors. Vet Pathol. (2019) 56:180–8. doi: 10.1177/0300985818798094
54. Bongiovanni, L, D’Andrea, A, Porcellato, I, Ciccarelli, A, Malatesta, D, Romanucci, M, et al. Canine cutaneous melanocytic Tumours: significance of Beta-catenin and Survivin Immuno-histochemical expression. Vet Dermatol. (2015) 26:270–e59. doi: 10.1111/vde.12211
55. Weinstein, D, Leininger, J, Hamby, C, and Safai, B. Diagnostic and prognostic biomarkers in melanoma. J Clin Aesthet Dermatol. (2014) 7:13–24.
56. Mayayo, SL, Prestigio, S, Maniscalco, L, Rosa, G, Aricò, A, De Maria, R, et al. Chondroitin sulfate Proteoglycan-4: a biomarker and a potential immunotherapeutic target for canine malignant melanoma. Vet J. (2011) 190:e26–30. doi: 10.1016/j.tvjl.2011.02.020
57. Heishima, K, Ichikawa, Y, Yoshida, K, Iwasaki, R, Sakai, H, Nakagawa, T, et al. Circulating MicroRNA-214 and -126 as potential biomarkers for canine neoplastic disease. Sci Rep. (2017) 7:2301. doi: 10.1038/s41598-017-02607-1
58. Malho, P, Dunn, K, Donaldson, D, Dubielzig, RR, Birand, Z, and Starkey, M. Investigation of prognostic indicators for human uveal melanoma as biomarkers of canine uveal melanoma metastasis. J Small Anim Pract. (2013) 54:584–93. doi: 10.1111/jsap.12141
59. Bowlt Blacklock, KL, Birand, Z, Selmic, LE, Nelissen, P, Murphy, S, Blackwood, L, et al. Genome-wide analysis of canine Oral malignant melanoma metastasis-associated gene expression. Sci Rep. (2019) 9:6511. doi: 10.1038/s41598-019-42839-x
60. Prouteau, A, Denis, JA, De Fornel, P, Cadieu, E, Derrien, T, Kergal, C, et al. Circulating tumor DNA is detectable in canine histiocytic sarcoma, oral malignant melanoma, and multicentric lymphoma. Sci Rep. (2021) 11:877. doi: 10.1038/s41598-020-80332-y
61. Owen, LN. TNM classification of Tumours in domestic animals. 1st ed. Geneva: World Health Organization (1980). 52 p.
62. Manley, CA, Leibman, NF, Wolchok, JD, Riviere, IC, Bartido, S, Craft, DM, et al. Xenogeneic murine Tyrosinase DNA vaccine for malignant melanoma of the digit of dogs. J Vet Intern Med. (2011) 25:94–9. doi: 10.1111/j.1939-1676.2010.0627.x
63. Skinner, OT, Boston, SE, Giglio, RF, Whitley, EM, Colee, JC, and Porter, EG. Diagnostic accuracy of contrast-enhanced computed tomography for assessment of mandibular and medial retropharyngeal lymph node metastasis in dogs with Oral and nasal Cancer. Vet Comp Oncol. (2018) 16:562–70. doi: 10.1111/vco.12415
64. Skinner, OT, Boston, SE, and Souza, CHM. Patterns of lymph node metastasis identified following bilateral mandibular and medial retropharyngeal lymphadenectomy in 31 dogs with malignancies of the head. Vet Comp Oncol. (2017) 15:881–9. doi: 10.1111/vco.12229
65. Townsend, KL, Milovancev, M, and Bracha, S. Feasibility of near-infrared fluorescence imaging for sentinel lymph node evaluation of the Oral cavity in healthy dogs. Am J Vet Res. (2018) 79:995–1000. doi: 10.2460/ajvr.79.9.995
66. Brissot, HN, and Edery, EG. Use of indirect Lymphography to identify sentinel lymph node in dogs: a pilot study in 30 Tumours. Vet Comp Oncol. (2017) 15:740–53. doi: 10.1111/vco.12214
67. Herring, ES, Smith, MM, and Robertson, JL. Lymph node staging of Oral and maxillofacial neoplasms in 31 dogs and cats. J Vet Dent. (2002) 19:122–6. doi: 10.1177/089875640201900301
68. Grimes, JA, Mestrinho, LA, Berg, J, Cass, S, Oblak, ML, Murphy, S, et al. Histologic evaluation of mandibular and medial retropharyngeal lymph nodes during staging of Oral malignant melanoma and squamous cell carcinoma in dogs. J Am Vet Med Assoc. (2019) 254:938–43. doi: 10.2460/javma.254.8.938
69. Green, K, and Boston, SE. Bilateral removal of the mandibular and medial retropharyngeal lymph nodes through a single ventral midline incision for staging of head and neck cancers in dogs: a description of surgical technique. Vet Comp Oncol. (2017) 15:208–14. doi: 10.1111/vco.12154
70. Ober, CP, and Barber, D. Comparison of two- vs. three-view thoracic radiographic studies on conspicuity of structured interstitial patterns in dogs. Vet Radiol Ultrasound. (2006) 47:542–5. doi: 10.1111/j.1740-8261.2006.00183.x
71. Nemanic, S, London, CA, and Wisner, ER. Comparison of thoracic radiographs and single breath-hold helical CT for detection of pulmonary nodules in dogs with metastatic neoplasia. J Vet Intern Med. (2006) 20:508–15. doi: 10.1892/0891-6640(2006)20[508:cotras]2.0.co;2
72. Oblak, ML, Boston, SE, Woods, JP, and Nykamp, S. Comparison of concurrent imaging modalities for staging of dogs with appendicular primary bone Tumours. Vet Comp Oncol. (2015) 13:28–39. doi: 10.1111/vco.12016
73. Otoni, CC, Rahal, SC, Vulcano, LC, Ribeiro, SM, Hette, K, Giordano, T, et al. Survey radiography and computerized tomography imaging of the thorax in female dogs with mammary tumors. Acta Vet Scand. (2010) 52:20. doi: 10.1186/1751-0147-52-20
74. Labelle, P, and De Cock, HEV. Metastatic tumors to the adrenal glands in domestic animals. Vet Pathol. (2005) 42:52–8. doi: 10.1354/vp.42-1-52
75. Hyman, JA, Koch, SA, and Wilcock, BP. Canine choroidal melanoma with metastases. Vet Ophthalmol. (2002) 5:113–7. doi: 10.1046/j.1463-5224.2002.00227.x
76. Ghirelli, CO, Villamizar, LA, and Fonseca Pinto, ACBC. Comparison of standard radiography and computed tomography in 21 dogs with maxillary masses. J Vet Dent. (2013) 30:72–6. doi: 10.1177/089875641303000201
77. Liptak, JM. Histologic margins and the residual tumour classification scheme: is it time to use a validated scheme in human oncology to standardise margin assessment in veterinary oncology? Vet Comp Oncol. (2020) 18:25–35. doi: 10.1111/vco.12555
78. Milovancev, M, and Russell, DS. Surgical margins in the veterinary Cancer patient. Vet Comp Oncol. (2017) 15:1136–57. doi: 10.1111/vco.12284
79. Boston, SE, Lu, X, Culp, WTN, Montinaro, V, Romanelli, G, Dudley, RM, et al. Efficacy of systemic adjuvant therapies administered to dogs after excision of Oral malignant melanomas: 151 cases (2001–2012). J Am Vet Med Assoc. (2014) 245:401–7. doi: 10.2460/javma.245.4.401
80. Boston, SE, van Stee, LL, Bacon, NJ, Szentimrey, D, Kirby, BM, van Nimwegen, S, et al. Outcomes of eight cats with oral neoplasia treated with radical mandibulectomy. Vet Surg. (2020) 49:222–32. doi: 10.1111/vsu.13341
81. Schultheiss, PC. Histologic features and clinical outcomes of melanomas of lip, haired skin, and nail bed locations of dogs. J Vet Diagn Invest. (2006) 18:422–5. doi: 10.1177/104063870601800422
82. Neat, BC, and Smeak, DD. Reconstructing weight-bearing surfaces: digital pad transposition. Compend Contin Educ Vet. (2007) 29:39–46.
83. Pavletic, MM. Foot pad reconstruction In: MM Pavletic, editor. Atlas of small animal wound management and reconstructive surgery. 4th Editn ed. Hoboken, NJ: Wiley-Blackwell (2018). 550–1.
84. Wang, AL, and Kern, T. Melanocytic ophthalmic neoplasms of the domestic veterinary species: a review. Top Companion Anim Med. (2015) 30:148–57. doi: 10.1053/j.tcam.2015.06.001
85. Schobert, CS, Labelle, P, and Dubielzig, RR. Feline conjunctival melanoma: histopathological characteristics and clinical outcomes. Vet Ophthalmol. (2010) 13:43–6. doi: 10.1111/j.1463-5224.2009.00758.x
86. Andreani, V, Guandalini, A, D’Anna, N, Giudice, C, Corvi, R, Di Girolamo, N, et al. The combined use of surgical Debulking and diode laser photocoagulation for Limbal melanoma treatment: a retrospective study of 21 dogs. Vet Ophthalmol. (2017) 20:147–54. doi: 10.1111/vop.12383
87. Donaldson, D, Sansom, J, and Adams, V. Canine Limbal melanoma: 30 cases (1992-2004). Part 2. Treatment with lamellar resection and adjunctive strontium-90beta Plesiotherapy—efficacy and morbidity. Vet Ophthalmol. (2006) 9:179–85. doi: 10.1111/j.1463-5224.2006.00468.x
88. Kawabe, M, Mori, T, Ito, Y, Murakami, M, Sakai, H, Yanai, T, et al. Outcomes of dogs undergoing radiotherapy for treatment of Oral malignant melanoma: 111 cases (2006-2012). J Am Vet Med Assoc. (2015) 247:1146–53. doi: 10.2460/javma.247.10.1146
89. Proulx, DR, Ruslander, DM, Dodge, RK, Hauck, ML, Williams, LE, Horn, B, et al. A retrospective analysis of 140 dogs with Oral melanoma treated with external beam radiation. Vet Radiol Ultrasound. (2003) 44:352–9. doi: 10.1111/j.1740-8261.2003.tb00468.x
90. Freeman, KP, Hahn, KA, Harris, FD, and King, GK. Treatment of dogs with Oral melanoma by Hypofractionated radiation therapy and platinum-based chemotherapy (1987-1997). J Vet Intern Med. (2003) 17:96–101. doi: 10.1892/0891-6640(2003)017<0096:todwom>2.3.co;2
91. Bateman, KE, Catton, PA, Pennock, PW, and Kruth, SA. 0-7-21 radiation therapy for the treatment of canine Oral melanoma. J Vet Intern Med. (1994) 8:267–72. doi: 10.1111/j.1939-1676.1994.tb03231.x
92. Blackwood, L, and Dobson, JM. Radiotherapy of Oral malignant melanomas in dogs. J Am Vet Med Assoc. (1996) 209:98–102. doi: 10.2460/javma.1996.209.01.98
93. Théon, AP, Rodriguez, C, and Madewell, BR. Analysis of prognostic factors and patterns of failure in dogs with malignant Oral tumors treated with megavoltage irradiation. J Am Vet Med Assoc. (1997) 210:778–84. doi: 10.2460/javma.1997.210.06.778
94. Cancedda, S, Rohrer Bley, C, Aresu, L, Dacasto, M, Leone, VF, Pizzoni, S, et al. Efficacy and side effects of radiation therapy in comparison with radiation therapy and Temozolomide in the treatment of measurable canine malignant melanoma. Vet Comp Oncol. (2016) 14:e146–57. doi: 10.1111/vco.12122
95. Tollett, MA, Duda, L, Brown, DC, and Krick, EL. Palliative radiation therapy for solid tumors in dogs: 103 cases (2007-2011). J Am Vet Med Assoc. (2016) 248:72–82. doi: 10.2460/javma.248.1.72
96. Farrelly, J, Denman, DL, Hohenhaus, AE, Patnaik, AK, and Bergman, PJ. Hypofractionated radiation therapy of Oral melanoma in five cats. Vet Radiol Ultrasound. (2004) 45:91–3. doi: 10.1111/j.1740-8261.2004.04015.x
97. Meleo, KA. Tumors of the skin and associated structures. Vet Clin North Am Small Anim Pract. (1997) 27:73–94. doi: 10.1016/s0195-5616(97)50007-6
98. Davies, O, Spencer, S, Necova, S, Holmes, E, Taylor, A, Blackwood, L, et al. Intranasal melanoma treated with radiation therapy in three dogs. Vet Q. (2017) 37:274–81. doi: 10.1080/01652176.2017.1387828
99. LaRue, SM, and Gordon, IK. Radiation oncology In: D Vail, D Thamm, and J Liptak, editors. Withrow and MacEwen’s small animal clinical oncology. 6th ed. St. Louis, MO: Elsevier (2020). 367–81.
100. Nemec, A, Arzi, B, Hansen, K, Murphy, BG, Lommer, MJ, Peralta, S, et al. Osteonecrosis of the jaws in previously irradiated fields: 13 cases (1989-2014). Front Vet Sci. (2015) 2:5. doi: 10.3389/fvets.2015.00005
101. Dank, G, Rassnick, KM, Sokolovsky, Y, Garrett, LD, Post, GS, Kitchell, BE, et al. Use of adjuvant carboplatin for treatment of dogs with oral malignant melanoma following surgical excision. Vet Comp Oncol. (2014) 12:78–84. doi: 10.1111/j.1476-5829.2012.00338.x
102. Murphy, S, Hayes, AM, Blackwood, L, Maglennon, G, Pattinson, H, and Sparkes, AH. Oral malignant melanoma – the effect of coarse fractionation radiotherapy alone or with adjuvant carboplatin therapy. Vet Comp Oncol. (2005) 3:222–9. doi: 10.1111/j.1476-5810.2005.00082.x
103. LaRue, SM, and Custis, JT. Advances in veterinary radiation therapy: targeting tumors and improving patient comfort. Vet Clin North Am Small Anim Pract. (2014) 44:909–23. doi: 10.1016/j.cvsm.2014.05.010
104. Nolan, MW, and Gieger, TL. Update in veterinary radiation oncology: focus on stereotactic radiation therapy. Vet Clin North Am Small Anim Pract. (2019) 49:933–47. doi: 10.1016/j.cvsm.2019.05.001
105. Grosenbaugh, DA, Leard, AT, Bergman, PJ, Klein, MK, Meleo, K, Susaneck, S, et al. Safety and efficacy of a xenogeneic DNA vaccine encoding for human Tyrosinase as adjunctive treatment for Oral malignant melanoma in dogs following surgical excision of the primary tumor. Am J Vet Res. (2011) 72:1631–8. doi: 10.2460/ajvr.72.12.1631
106. Verganti, S, Berlato, D, Blackwood, L, Amores-Fuster, I, Polton, GA, Elders, R, et al. Use of Oncept melanoma vaccine in 69 canine Oral malignant melanomas in the UK. J Small Anim Pract. (2017) 58:10–6. doi: 10.1111/jsap.12613
107. Ottnod, JM, Smedley, RC, Walshaw, R, Hauptman, JG, Kiupel, M, and Obradovich, JE. A retrospective analysis of the efficacy of Oncept vaccine for the adjunct treatment of canine Oral malignant melanoma. Vet Comp Oncol. (2013) 11:219–29. doi: 10.1111/vco.12057
108. Sarbu, L, Kitchell, BE, and Bergman, PJ. Safety of administering the canine melanoma DNA vaccine (Oncept) to cats with malignant melanoma – a retrospective study. J Feline Med Surg. (2017) 19:224–30. doi: 10.1177/1098612X15623319
109. Brockley, LK, Cooper, MA, and Bennett, PF. Malignant melanoma in 63 dogs (2001-2011): the effect of carboplatin chemotherapy on survival. N Z Vet J. (2013) 61:25–31. doi: 10.1080/00480169.2012.699433
110. Boria, PA, Murry, DJ, Bennett, PF, Glickman, NW, Snyder, PW, Merkel, BL, et al. Evaluation of cisplatin combined with Piroxicam for the treatment of Oral malignant melanoma and Oral squamous cell carcinoma in dogs. J Am Vet Med Assoc. (2004) 224:388–94. doi: 10.2460/javma.2004.224.388
111. Rassnick, KM, Ruslander, DM, Cotter, SM, Al-Sarraf, R, Bruyette, DS, Gamblin, RM, et al. Use of carboplatin for treatment of dogs with malignant melanoma: 27 cases (1989-2000). J Am Vet Med Assoc. (2001) 218:1444–8. doi: 10.2460/javma.2001.218.1444
112. Gregório, H, Raposo, TP, Queiroga, FL, Prada, J, and Pires, I. Investigating associations of Cyclooxygenase-2 expression with angiogenesis, proliferation, macrophage and T-lymphocyte infiltration in canine melanocytic Tumours. Melanoma Res. (2016) 26:338–47. doi: 10.1097/CMR.0000000000000262
113. Martínez, CM, Peñafiel-Verdú, C, Vilafranca, M, Ramírez, G, Méndez-Gallego, M, Buendía, AJ, et al. Cyclooxygenase-2 expression is related with localization, proliferation, and overall survival in canine melanocytic neoplasms. Vet Pathol. (2011) 48:1204–11. doi: 10.1177/0300985810396517
114. Kitchell, BE, Brown, DM, Luck, EE, Woods, LL, Orenberg, EK, and Bloch, DA. Intralesional implant for treatment of primary Oral malignant melanoma in dogs. J Am Vet Med Assoc. (1994) 204:229–36. doi: 10.2460/javma.1994.204.02.229
115. Tellado, MN, Maglietti, FH, Michinski, SD, Marshall, GR, and Signori, E. Electrochemotherapy in treatment of canine Oral malignant melanoma and factors influencing treatment outcome. Radiol Oncol. (2020) 54:68–78. doi: 10.2478/raon-2020-0014
116. Giuliano, A, and Dobson, J. Prospective clinical trial of Masitinib Mesylate treatment for advanced stage III and IV canine malignant melanoma. J Small Anim Pract. (2020) 61:190–4. doi: 10.1111/jsap.13111
117. Morsey, M, Boekh, A, Lehmann, H, and Stock, M. An anti-canine PD-1 monoclonal antibody for immunotherapy of cancer in dogs. 2021 ACVIM forum research abstract program. J Vet Intern Med. (2021) 35:2943–3204. doi: 10.1111/jvim.16220
118. Webster, JD, Dennis, MM, Dervisis, N, Heller, J, Bacon, NJ, Bergman, PJ, et al. Recommended guidelines for the conduct and evaluation of prognostic studies in veterinary oncology. Vet Pathol. (2011) 48:7–18. doi: 10.1177/0300985810377187
119. Bostock, DE. Prognosis after surgical excision of canine melanomas. Vet Pathol. (1979) 16:32–40. doi: 10.1177/030098587901600103
120. Marino, DJ, Matthiesen, DT, Stefanacci, D, and Moroff, SD. Evaluation of dogs with digit masses: 117 cases (1981–1991). J Am Vet Med Assoc. (1995) 207:726–8. doi: 10.2460/javma.1995.207.06.0726
121. Pittaway, R, Dobromylskyj, MJ, Erles, K, Pittaway, CE, Suarez-Bonnet, A, Chang, Y-M, et al. Nonocular melanocytic neoplasia in cats: characterization and proposal of a histologic classification scheme to more accurately predict clinical outcome. Vet Pathol. (2019) 56:868–77. doi: 10.1177/0300985819854435
Keywords: dog, cat, melanoma, prognosis, consensus, treatment, guidelines
Citation: Polton G, Borrego JF, Clemente-Vicario F, Clifford CA, Jagielski D, Kessler M, Kobayashi T, Lanore D, Queiroga FL, Rowe AT, Vajdovich P and Bergman PJ (2024) Melanoma of the dog and cat: consensus and guidelines. Front. Vet. Sci. 11:1359426. doi: 10.3389/fvets.2024.1359426
Edited by:
Ricardo Marcos, University of Porto, PortugalReviewed by:
Antonella Rigillo, I-Vet S.R.L., ItalyCopyright © 2024 Polton, Borrego, Clemente-Vicario, Clifford, Jagielski, Kessler, Kobayashi, Lanore, Queiroga, Rowe, Vajdovich and Bergman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gerry Polton, R2VycnkuUG9sdG9uQG5kc3IuY28udWs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.