 László Lehner
László Lehner Kálmán Czeibert
Kálmán Czeibert Péter Csébi3
Péter Csébi3 Kristóf Diószegi
Kristóf Diószegi- 1Fuziovet Veterinary Clinic and Hospital, Budapest, Hungary
- 2LimesVet Ltd, Budapest, Hungary
- 3Radiovet Bt, Budapest, Hungary
- 4Medivet Birstall, Birstall, United Kingdom
- 5National Institute of Mental Health, Neurology and Neurosurgery, Budapest, Hungary
This case series describes the surgical removal of lateral ventricular tumors using a transcallosal approach, long-term follow-up, and magnetic resonance imaging (MRI) results of 3 dogs. Two tumors were benign choroid plexus tumors (CPT). One was a grade 2 astrocytoma. Complete tumor removal was achieved using the transcallosal approach. All dogs had ventriculomegaly which remained static or progressed during the follow-up period. All dogs had epileptic seizures before the surgical procedure which persisted despite tumor removal. One dog with CPT was alive after 3 years and 5 months and had minor focal seizures every 3–4 months. No other clinical signs were observed. The second dog with CPT was neurologically free for 17 months after the surgical procedure but died due to acute-onset therapy-resistant generalized epileptic seizures. The third dog with intraventricular astrocytoma experienced epileptic seizures 2 and 4 months after the surgical procedure. The second event was therapy-resistant which led to death.
1. Introduction
Choroid plexus tumors (CPTs) are the most common type of intraventricular tumor in veterinary medicine (1). CPTs represent 7–10% of all primary brain tumors in dogs (2, 3) and can be histologically classified as papillomas, atypical papillomas, and carcinomas (2). Almost half (49%), 29, and 22% of the CPTs occur in the fourth, lateral, and third ventricle, respectively (4). Other rare ventricular tumors include astrocytomas. The origin of astrocytomas remains controversial, although these are known to occur in the subventricular zone of the lateral ventricle (5). Astrocytomas are the most prevalent type of glioma, accounting for approximately 17% of all primary tumors of the central nervous system (6). Intraventricular tumors can cause secondary hydrocephalus due to obstruction of cerebrospinal fluid (CSF) circulation in the foramen of Monro or fourth ventricle (7) or due to overproduction of CSF (7).
Widely accepted standard treatment protocols have not yet been established for intraventricular tumors in veterinary medicine (8). In humans, surgical excision with or without adjunctive radiotherapy is considered the most effective treatment for CPTs (9). Surgical excision can eliminate the tumor and tumor induced local brain tissues compression and cease the obstruction of CSF circulation which increases intracranial pressure. Moreover, it can provide a histopathological diagnosis (1). Radiotherapy is an invasive palliative treatment that is recommended for inoperable cases if possible or after tumor removal (10). Additionally, palliative ventriculoperitoneal shunting (VPS) is an option in rapidly deteriorating cases where radiation therapy does not relieve the clinical signs of elevated intracranial pressure caused by hydrocephalus quickly or the location of the mass prevents surgical excision or after tumor elimination if progressive ventricle growth occurred (11, 12).
The surgical excision of intraventricular tumors presents a significant challenge owing to their location. Transcortical, transcallosal, and parasplenial approaches can be applied to lateral ventricles (13). A transcallosal approach provides relatively simple access to the ventricles and minimizes the morbidity associated with the resection of these lesions (13). The corpus callosum is one of the 3 main commissures connecting the 2 hemispheres of the cerebrum (14). These commissures are responsible for communication between cortical areas (15). In humans, partial transection of the corpus callosum (callosotomy) does not cause significant neurological deficits. However, if the surgery induces additional brain injury, callosotomy can increase the severity of neurological deficits (13). Preservation of the splenium of the corpus callosum mitigates the postoperative neuropsychological effects of this approach (16, 17), collectively called disconnection syndrome. In humans, the clinical symptoms include affected motor control, spatial orientation, vision, hearing, and language (16). Although minimal data exists, animals exhibit minimal to no defects after 2 weeks of partial or complete callosotomy (18, 19). The transcallosal approach for intraventricular CPT removal in a dog with 9 months follow up was first reported by our group (20).
2. Materials and methods
Six dogs were referred to the FuzioVet Veterinary Referral Clinic, Budapest, Hungary between 2019 and 2022 with rostrotentorial intraventricular tumors based on magnetic resonance imaging (MRI). In 3 cases, owners elected for surgery. The remaining 3 cases were treated conservatively with prednisolone and/or antiseizure medications (ASMs) according to owners will. All of the conservatively treated dogs died within 3 months due to deterioration of clinical signs (obtundation and uncontrolled seizures). We summarized the clinical signs, treatments, pre- and postoperative MRI findings, and survival times of the conservatively and surgically treated cases in Table 1.
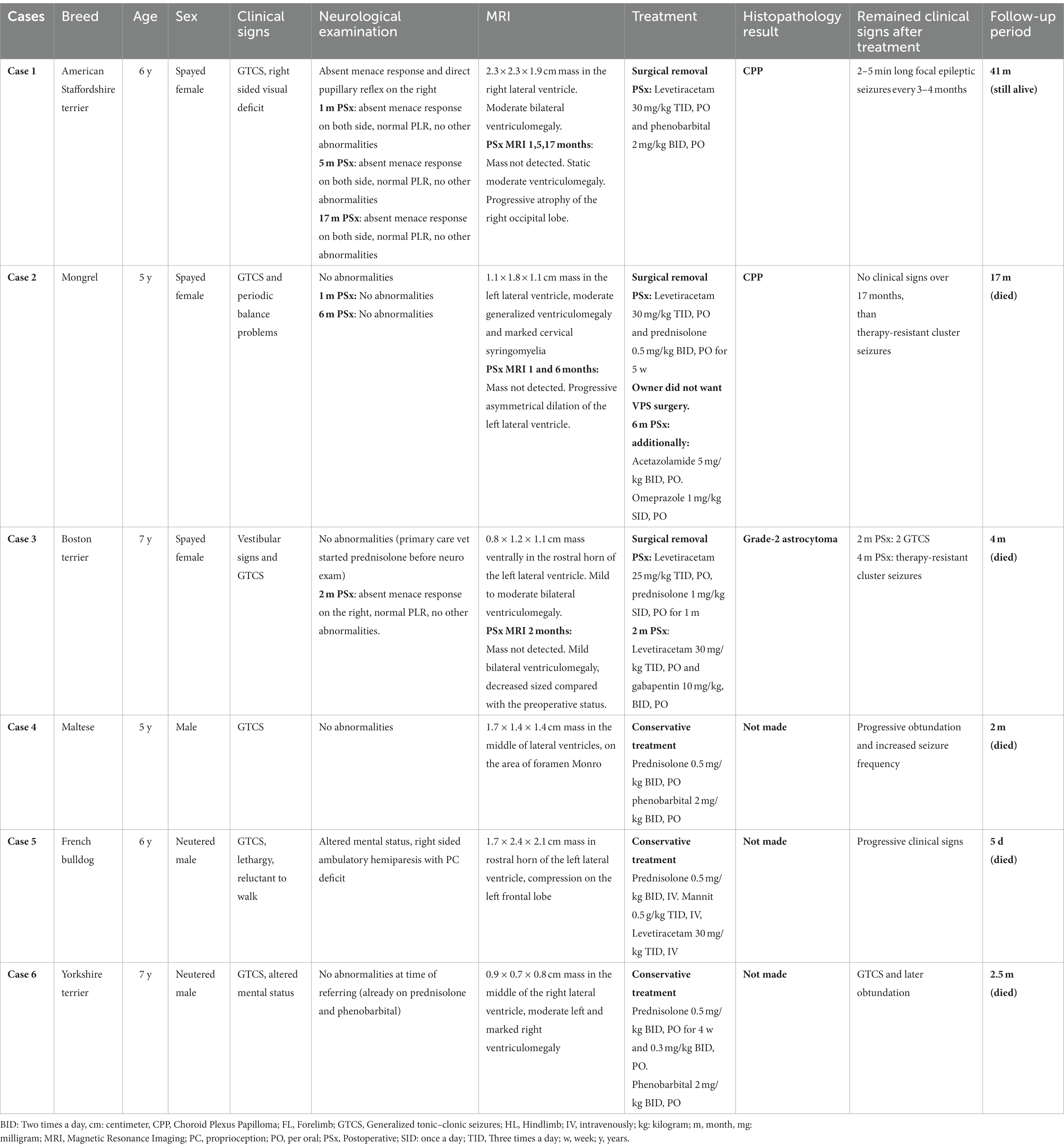
Table 1. Summary of the conservatively and surgically treated cases.
In all surgically treated dogs, preoperative complete blood count, serum biochemistry, urinalysis, abdominal ultrasound, echocardiography, and thoracic radiography were performed, but no significant abnormalities were observed. The anesthetic and surgical protocols used in each case have been described in detail previously (21). Briefly, parieto-parasagittal craniotomy was performed using an oscillating saw. After durotomy, intraventricular CSF was drained using an intravenous catheter to relax the brain for subsequent manipulation. The corpus callosum between the two hemispheres was carefully exposed and partially transected at the midline. We made the smallest feasible incision to access the tumor, thereby minimizing the invasiveness of this procedure. An operation microscope and 8- and 12-Ch Fergusson suction cannulas were used to visualize and remove the tumor fragments from the ventricles. Gelatin sponges and bipolar electrocautery were used to control the bleeding. After tumor removal, the ventricle was cleaned with a sterile physiological NaCl infusion, and the interventricular foramen of Monro was checked for patency. The ventricles were refilled with physiological NaCl infusion, and a gelatin sponge was placed on the surface of the brain. The dura mater was sutured, and the craniotomy bone fragments were replaced. The patients were hospitalized and treated with methylprednisolone (1 mg/kg, IV), cefazolin (30 mg/kg, IV), morphine hydrochloride (2–4 mg/kg, IV), and mannitol to prevent and treat postoperative edema (0.5–1 g/kg TID, IV on the first day, BID on the second day, and discontinued on the third day if no clinical signs were observed). Case-specific medications were continued after hospital discharge. The tissue samples were subjected to histopathological analysis.
3. Case descriptions
The first case has been described in detail in a prior publication (20). We have included this case here because we describe a significantly longer follow-up period (3 years and 5 months post-surgery) than that in the previous paper (9 months), and we believe this adds novel insight to the case.
3.1. Case 1
A 6-year-old spayed female American Staffordshire terrier presented with periodic generalized epileptic seizures and visual deficits. Investigations performed prior to surgery revealed severe, chronic hydrocephalus and the presence of a 2.3 × 2.3 × 1.9 cm large intraventricular tumor. The tumor was T2-weighted (T2W) and T1-weighted (T1W) isointense, mildly hyperintense on Fluid-Attenuated Inversion Recovery sequencies (FLAIR), and strongly contrast enhancing (Figure 1A). Histopathology was consistent with benign choroid plexus papilloma (CPP).
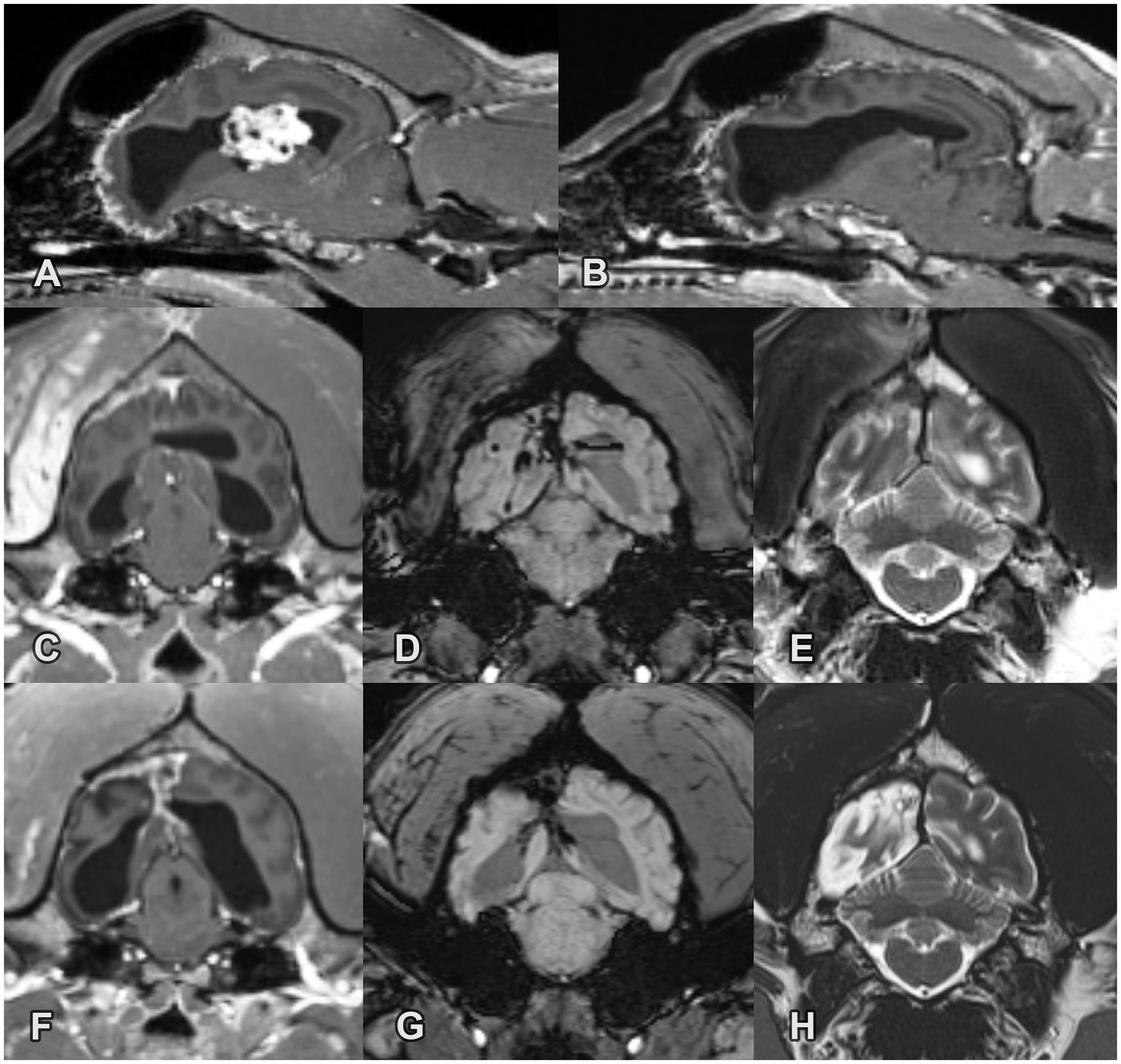
Figure 1. Pre- and post-operative MRI images of a choroid plexus papilloma in the right lateral ventricle in Case 1. (A) Pre-operative sagittal T1W post-contrast image. Note the large cauliflower-like mass with marked contrast enhancement and the secondary moderate chronic ventriculomegaly. (B) 1-month post-operative sagittal T1W post-contrast image. The mass is no longer present. The lateral ventricles remained moderately enlarged without significant change compared to the pre-operative status. (C) 1-month post-operative transverse T1W post-contrast image. Note the marked contrast enhancement along the site of the surgical approach in the right temporal muscle, calvarium and falx cerebri. (D) 1-month post-operative transverse SWI image. Signal void is present along the site of the surgical approach consistent with moderate subacute hemorrhage. (E) 1-month post-operative transverse T2W image. The sulci are mildly widened in the right occipital lobe. (F) 17-month post-operative transverse T1W post-contrast image. The lateral ventricles remained moderately enlarged without significant change compared to the pre-operative status. The contrast enhancement decreased in the temporal muscle but remained static in the brain. (G) 17-month post-operative transverse SWI image. The area of the signal void is mildly decreased. (H) 17-month post-operative transverse T2W image. Note the progressive atrophy of the right occipital lobe.
Two 5-min-long generalized tonic–clonic seizures (GTCS) occurred within 1 month of tumor resection. In the following 3 months, no epileptic seizures were observed, and the dog was in good condition without neurological deficit. Two GTCS occurred 4 months after the intervention. After increasing the ASM dosage, no further seizures were observed for 6 months. Ten months after surgery, the dog started to show 2–3 focal seizures every 2–3 months. Two GTCS occurred 12 months later. The levetiracetam dosage was increased from 20 mg/kg to 30 mg/kg TID, PO, and phenobarbital was administered as an add-on ASM (2 mg/kg BID, PO). Three years and 5 months after surgery the dog had approximately 2–5 min long focal epileptic seizures every 3–4 months and has still visual deficit. To date, the dog has undergone 3 follow-up MRI scans (1, 5, and 17 months after surgery). No additional MRI has been conducted because the owner has declined until the dog shows clinical signs of deterioration. Remnants of the mass or recurrence were not detected. The lateral ventricles remained moderately enlarged without significant changes compared to their pre-operative status. Moderate subacute hemorrhage and contrast enhancement were observed at the surgical site on the first MRI scan. The area of the signal void was slightly decreased in the follow-up MRI. The contrast enhancement remained static in the brain. Progressive atrophy of the right occipital lobe was observed on the second and third MRI scans (Figures 1B-H).
3.2. Case 2
A 5.5-year-old female spayed mongrel presented with periodic GTCS and balance problems. The neurological examination did not show any abnormalities. Brain MRI was performed using a 1.5 Tesla magnet (Siemens Magnetom Avanto, Siemens, Erlangen, Germany) that revealed a 1.1 × 1.8 × 1.1 cm large mass in the left lateral ventricle. The mass was T2W and T1W isointense with the cerebral gray matter and hyperintense on FLAIR and showed marked heterogeneous contrast enhancement. All ventricles were markedly enlarged. Periventricular FLAIR hyperintensity, consistent with edema, was observed around the left lateral ventricle. A mild rightward midline shift and marked syringomyelia in the cervical spine was observed (Figure 2A). Histopathology was consistent with benign CPP.
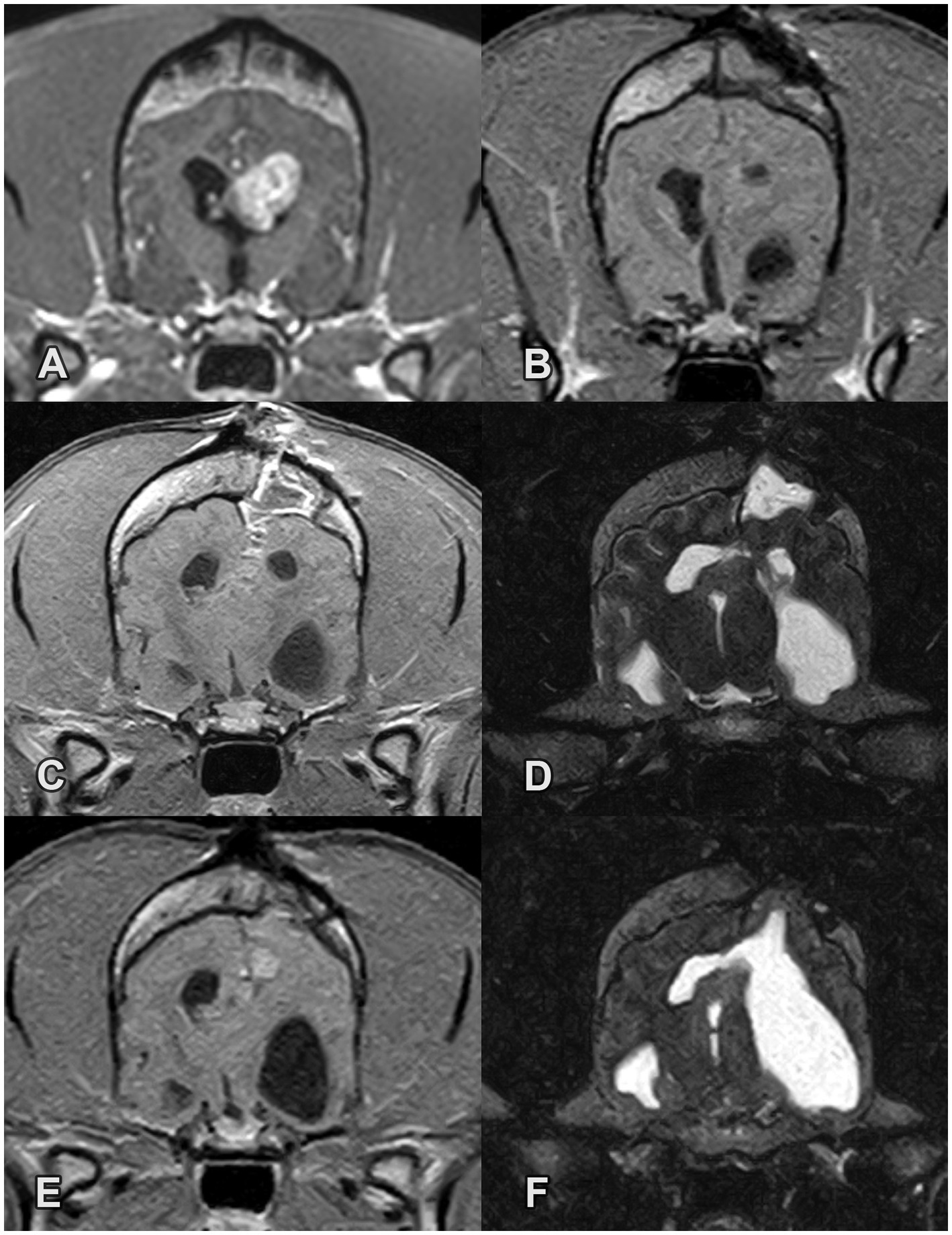
Figure 2. Pre- and post-operative MRI images of a choroid plexus papilloma in the left lateral ventricle in Case 2. (A) Pre-operative transverse T1W post-contrast image. Note the large mass with marked contrast enhancement and the secondary chronic ventriculomegaly. (B) 1-month post-operative transverse T1W post-contrast image at the level of the previous ventricular mass. The mass is no longer present. (C-F) Post-operative images at the level of the surgical site (C) 1-month transverse T1W post-contrast image, (D) 1-month transverse T2W image, (E) 6-month T1W post-contrast image, (F) 6-month transverse T2W image. Note the progressive asymmetrical dilation of the left lateral ventricle with a rightward midline shift and the mild focal contrast enhancement in the region of the surgical approach.
The dog recovered uneventfully after surgery and was discharged with levetiracetam (30 mg/kg TID, PO) and prednisolone (0.5 mg/kg, BID, PO) treatment. Five weeks after the operation, prednisolone was tapered and discontinued, and levetiracetam was continued at the previous dose. Over the next 16 months, the dog was in good general condition with normal neurological exam and no seizures. MRI was repeated 1 and 6 months after surgery. Remnants of the mass and recurrence were not detected. Progressive asymmetrical dilation of the left lateral ventricle with a rightward midline shift was observed. Mild focal T2 hyperintensity and contrast enhancement were noted in the surgical approach region at both follow-up visits (Figures 2B–F) Due to the progression of ventricular dilation (which was seen on the 6 months postoperative MRI), VPS surgery was recommended. However, the owner declined VPS surgery, therefore, we initiated conservative treatment with acetazolamide (5 mg/kg, BID, PO) and omeprazole (1 mg/kg, SID, PO). Therapy-resistant cluster seizures occurred 17 months after surgery leading to death.
3.3. Case 3
A 7-year-old female spayed Boston Terrier was referred for neurological consultation because of central vestibular signs and GTCS. Levetiracetam (25 mg/kg, TID, PO) and prednisolone (1 mg/kg, SID, PO) were administered. Brain MRI was performed with a 0.4 Tesla magnet (Hitachi Airis Vento, Fujifilm Europe GmbH, Ratingen, Germany) that revealed a 0.8 × 1.2 × 1.1 cm large mass ventrally in the rostral horn of the left lateral ventricle. The mass was T2W mildly hyperintense and T1W iso-to-hypointense without contrast enhancement. The left and right lateral ventricles were moderately and mildly enlarged, respectively. A mild rightward midline-shift was observed (Figures 3A–C). The histopathology of the removed tumor tissue was consistent with a grade 2 astrocytoma.
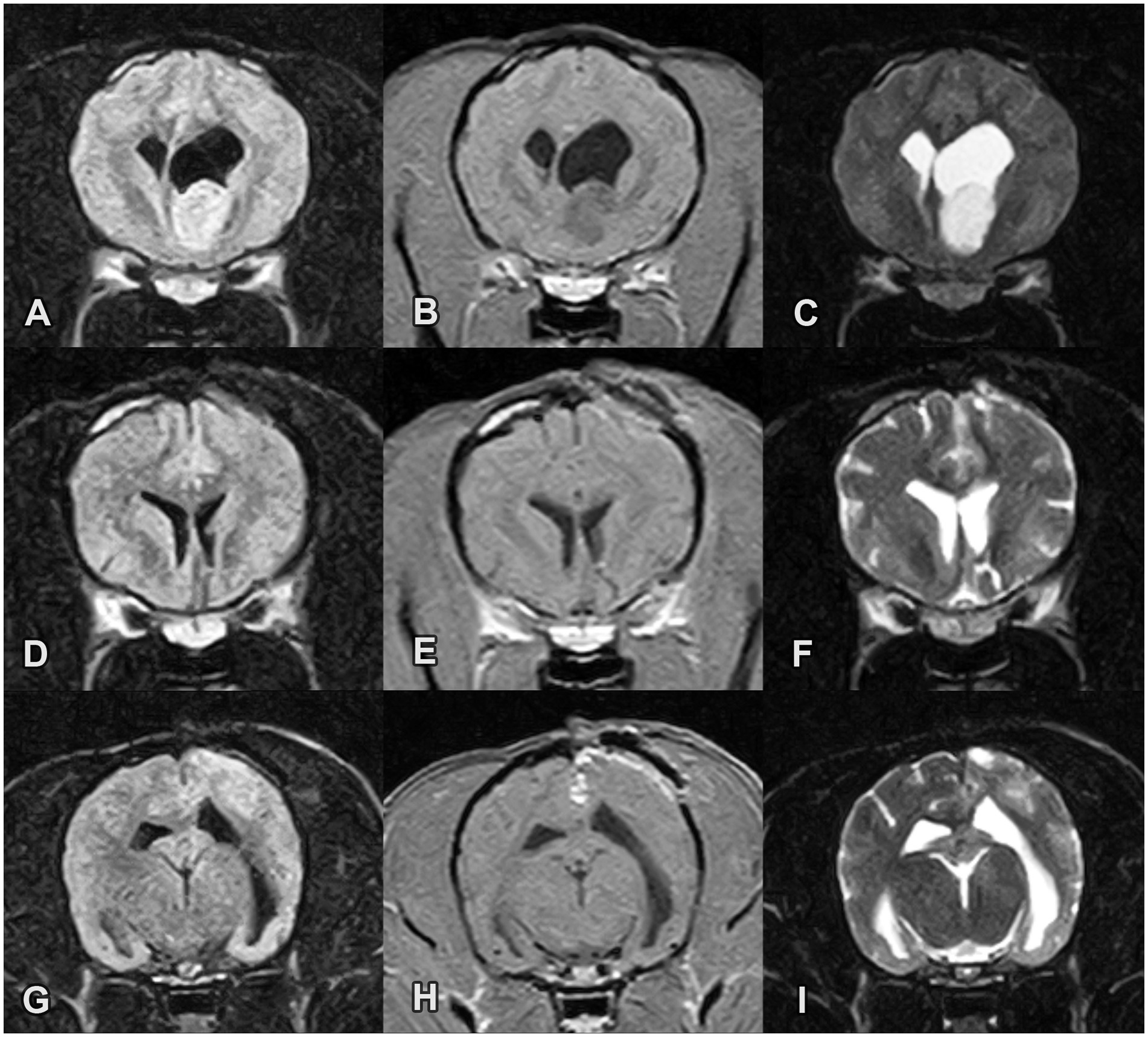
Figure 3. Pre- and post-operative MRI images of an intraventricular astrocytoma in the rostral horn of the left lateral ventricle in Case 3. (A-C) Pre-operative transverse images (A) FLAIR, (B) T1W post-contrast and (C) T2W images reveal a FLAIR/T2W hyperintense and T1W hypointense mass without contrast enhancement. (D–F) Post-operative transverse images at the site of the previous mass. The mass is no longer present. (G-I) 2-month post-operative transverse images (G) FLAIR, (H) T1W post-contrast and (I) T2W image. Multifocal T2 hyperintensities in the subcortical white matter and contrast enhancement in the region of the surgical approach are noted. The lateral ventricles are still mildly enlarged but their size decreased in comparison with the preoperative status.
Computed tomography (CT) was performed immediately after surgery using a multislice CT scanner (General Electronic Optima 520, United States). The intraventricular mass was absent, and the replaced craniotomy bone fragment properly covered the surgical hiatus. After surgery, the dog showed a mild left head tilt and ambulatory hemiparesis on the right side. Menace response was absent on the right side, and the pupillary light reflex was normal. Conscious proprioception of the right limbs was delayed. During hospitalization, proprioceptive deficits improved, but the menace response was still absent.
Levetiracetam and prednisolone treatments were continued at the preoperative doses. Prednisolone was tapered and discontinued 1 month after the surgery. Two months after surgery, 2 GTCS occurred which were treated with a diazepam rectal solution (1 mg/kg) at home. The levetiracetam dose was increased to 30 mg/kg TID, PO, and gabapentin (10 mg/kg BID, PO) was used as an add-on ASM. MRI was repeated 2 months after surgery. The lateral ventricles were still mildly enlarged, but their size decreased compared with the preoperative status. No intraventricular mass was observed. Multifocal T2 hyperintensities in the white matter and contrast enhancement were noted in the region of the surgical approach (Figures 3D–I).
Four months after the surgery, cluster seizures occurred. The seizures did not respond to midazolam treatment (0.3 mg/kg, IV) and medetomidine-ketamine continuous rate infusion (CRI) was initiated (medetomidine 3 mcg/kg/h, ketamine-hydrochloride 1 mg/kg/h, IV) to treat the convulsions. After 12 h, CRI was stopped, and GTCS activity recurred. Propofol (5.5 mg/kg/h, IV) CRI was administered for 12 h, followed by intravenous phenobarbital (2 mg/kg, IV) and levetiracetam (30 mg/kg, IV) administration. During tapering of the propofol CRI dose, GTCS were observed again, which did not respond to any medication, and the dog died.
4. Discussion
Multiple treatment options are available for intraventricular tumors. Conservative palliative treatment involves anticonvulsants, corticosteroids, and analgesics. Other palliative or curative treatments include chemotherapy, radiation therapy, partial or complete surgical tumor removal, VPS or a combination of these.
In human medicine, if technically feasible, intraventricular tumor removal is the first stage because this is the only definitive curative therapy with typically less morbidity as in case of the mainly palliative radiotherapy. Surgical resection has the benefit of reducing or eliminating the local brain tissue compression caused by the tumor, by decreasing the intracranial pressure (CSF flow disturbance caused by tumor obstruction) and providing a histopathological diagnosis of the tumor type and grade (2). Surgical treatment is followed by radiation therapy in case of unsuccessful complete tumor resection (10). VPS dependence after successful tumor removal is rare, but if scar tissue or remaining tumor (partial tumor resection) causes CSF flow disruption and secondary ventriculomegaly, VPS can prevent further deterioration (11). In human medicine, the reported 5-year survival rate of CPTs is highly dependent on histology. Choroid plexus papilloma (87%) had far better outcomes than choroid plexus carcinoma (34%) (21).
In veterinary medicine studies have shown a wide range of outcomes and possible impacts of technology in case of intracranial tumors (22). Optimal treatment in dogs with intraventricular tumors are not well described in veterinary medicine. In a study of solitary intraventricular tumors in 7 dogs and 5 cats treated with radiation therapy alone or radiation therapy combined with VPS, the median survival times were 162 days and 1,103 days, respectively. Therefore, VPS can be beneficial in increasing the survival time in the case of ventricular tumors (12). VPS can rapidly decrease intracranial pressure and alleviate the associated clinical signs but does not provide curative treatment, cannot alleviate local brain tissue compression caused by the tumor, does not provide histopathological diagnosis and often associated with complications (12, 23). Therefore, VPS alone is not recommended in human medicine. Radiotherapy is also an invasive treatment, with several possible serious side effects and repeated anesthesia required for the procedure. In the above-mentioned study, two out of six dogs died and four out of six deteriorated during radiotherapy (22).
Due to the very limited veterinarian experience and available literature background in the treatment of intraventricular tumors, we have used the current human treatment protocol in our cases based on a potentially curative neurosurgical approach.
Transcortical and transcallosal approaches are used in human medicine to remove lateral and third ventricle tumors. The interhemispheric transcallosal approach disrupts the commissural fibers of the corpus callosum, whereas the transcortical approach damages the gray and white matter of the brain (24). In humans, transcallosal and transcortical approaches cause the same extent of corpus callosum damage, while the transcortical approach additionally disrupts the frontal white matter tracts (25). The transcallosal approach was associated with a higher incidence (10.8%) of hydrocephaly (shunt dependence) than the transcortical approach (7.0%); however, the difference was not significant.
Based on human neurosurgical experience, we used the transcallosal approach in our cases and all of the tumors were completely removable. We experienced during the procedures, that there is a greater chance of iatrogenic brain damage during dissection because of the small size of a dog’s brain compared to a human. Therefore, the use of a proper operation microscope, and microinstrumenst are recommended during the procedure. Due to rarity of such cases, it is also advised to concentrate the surgical treatment of such cases to reach maximal surgical experience.
In humans, typical postoperative brain tissue changes are present around the surgical site on repeated MRI, including multifocal T2W hyperintensities in the white matter, contrast enhancement along the surgical approach, and occasionally a periventricular cap caused by increased interstitial water content due to dysfunctional transependymal transport (26). Over time, these reduce but may remain visible for months after surgery and developing scar tissue can be present on postoperative MRI scans (26). Postoperative MRI revealed similar morphological alterations in canines. In the first case, a marked intraparenchymal hemorrhage was observed at the surgical site. Additionally, progressive atrophy of the right occipital lobe was observed in MRI scans for one case. This may be the result of an iatrogenic injury to the optic radiation induced by brain retraction, which damaged the afferent pathway, resulting in occipital lobe alterations such as secondary encephalomalacia. Another hypothesis could be that the visual impairment was caused by vascular damage. However, given the location of the current surgical approach, it is less probable. This is because the caudal cerebral artery, which is responsible for supplying blood to the occipital gyrus, runs adjacent to the splenium corporis callosi (further caudally from the surgical site) as it emerges from the caudal communicating artery (27).
In cases 1 and 2, the final histopathological diagnosis was a benign choroid plexus papilloma. In both cases, the mass caused lateral ventriculomegaly due to blockage of CSF circulation.
In case 1, despite complete excision of the intraventricular mass, the ventriculomegaly remained unchanged. Owing to the altered CSF flow caused by intraventricular tumors, chronic dilatation of the ventricles (particularly the lateral ventricles) has been frequently observed in humans (28, 29). According to the Monroe-Kellie theory, brain tissue atrophies when the ventricles dilate slowly. After surgery, the altered chronic CSF circulation resumed, but the loss of cerebral parenchyma and dilatation of the ventricles remain unchanged (28, 29). Chronic hydrocephalus does not require VPS surgery (28).
In case 2, the left lateral ventricle exhibited progressive enlargement. We suspect that the conformation of the scar tissue within the lateral ventricles resulted in altered CSF flow. This altered CSF flow can cause symmetrical or asymmetrical ventricular dilation. After the compensation phase, intracranial pressure elevation can develop and cause clinical signs, including altered state of consciousness, seizures, gait abnormalities, and vestibular signs. VPS is recommended to prevent deterioration of the neurological state if any neurological signs develop or repeated MRI scans reveal any progression of ventricular dilation during follow-up (30). We recommended VPS surgery in this case, but it was declined by the owner.
In case 3, an astrocytoma was confirmed. Given the rostral location of the mass and lack of contrast enhancement our preoperative differential diagnosis based on the MR images included primarily a glioma, lymphoma, ependymoma and we considered CPT unlikely. However, during surgery, we did not observe any macroscopic difference compared to previous cases, except for the location of the tumor. Oligodendroglioma is the most common type of glioma frequently observed in older, brachycephalic breeds and is rarely linked to the ventricular system (31). Moreover, astrocytoma involving the ventricles is extremely uncommon (32). Gliomas growing into the ventricles are considered to be pseudo-intraventricular tumors since they origin from the periphery and not from the ventricle. Nevertheless, the surgical treatment protocol is the same transcallosal approach, as they cannot be removed through the brain parenchyma. The tumor was completely removable and the associated ventriculomegaly show regression in the repeated MRI studies.
Epileptic seizure activity was the main preoperative clinical symptom in all cases. After tumor excision, 2 dogs developed refractory epilepsy. Canine brain neoplasia often causes tumor-associated structural epilepsy. Intraventricular tumors can cause visual difficulties, obtundation, disturbed behavior, and altered consciousness (2). Hydrocephalus-related seizures are suspected in veterinary medicine but have not been proven. However, some articles have mentioned epilepsy-like clinical signs in dogs with hydrocephalus (33–35). In humans, iatrogenic cortical injuries due to surgical procedures can cause epilepsy after craniotomies in 4–5% of cases (36). In one veterinary study, the incidence of early postoperative seizures (EPS) among dogs with rostrotentorial intracranial tumors ranged from 12.8 to 18.2% and was unrelated to previous structural epilepsy and presurgical ASM maintenance protocol. However, canines with EPS had longer hospitalizations, a higher risk of neurologic complications, and a lower probability of surviving to discharge (37). In our case series, as seizures occurred before surgery, we could not determine how cortical damage affected them. However, in our opinion, life-long antiseizure medication is recommended after craniotomy because of the potential for intraoperative iatrogenic cortical damage.
Callosotomy is a well-known intervention for the treatment of severe GTCS in humans. In this, anterior 2/3 corpus callosotomy versus complete/total corpus callosotomy is performed to prevent generalized seizures (16, 17). During the transcallosal approach, only partial callosotomy was performed. In our cases, total callosotomy was not performed, which may have contributed to the development of generalized seizures; however, minimal surgical exposure is recommended during tumor removal to prevent further invasivity. In case 1, it is highly probable that ASMs, rather than partial callosotomy, prevented generalized seizures and led to focal seizures only.
Our study was limited by the small sample size of dogs that underwent transcallosal surgery and conservative treatment. A large sample size is needed to gain robust experience regarding the long-term outcomes of surgically treated intraventricular tumors in dogs.
5. Conclusion
Following and applying current human neurosurgical approaches, our results show that transcallosal excision of lateral ventricular tumors is feasible. In our opinion, if the tumor can be removed by excision, it should be removed as a primary curative treatment, followed by radiotherapy or VPS surgery if necessary. In all 3 cases, complete tumor removal was possible which prolonged the survival times of the dogs compared to those that underwent conservative treatment. In cases with CPT, ventriculomegaly remained static or even showed progressive dilation despite tumor removal, most likely because of scar tissue formation in the ventricles. VPS surgery is recommended when diagnostic imaging reveals progressive ventricular dilation and corresponding neurological symptoms are exhibited. In all cases, epileptic seizures occurred prior to surgery and persisted after the mass was removed. Therefore, lifelong ASM therapy was recommended.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was not required for the studies involving animals in accordance with the local legislation and institutional requirements because we have the written consent from the owners. Written informed consent was obtained from the owners for the participation of their animals in this study.
Author contributions
LL, KC, and GN performed the surgeries. PC assessed the radiological data. LL and KC wrote the first draft of the manuscript. PC, KD, and GN wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to thank VetScan Ltd., Judit Benczik and Borbála Lőrincz for performing the diagnostic imaging. Also, thanks to Csaba Jakab for making histopathological studies and FuzioVet Referral Clinic for the perioperative management of the animals.
Conflict of interest
KC is employed by LimesVet Ltd. PC is employed by RadioVet Bt. KD is employed by Medivet Birstall.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Vail, DM, Thamm, DH, and Liptak, JM. Withrow and MacEwen’s small animal clinical oncology. MO: W.B. Saunders (2020).
2. Miller, AD, Miller, CR, and Rossmeisl, JH. Canine primary intracranial Cancer: a Clinicopathologic and comparative review of glioma, meningioma, and choroid plexus tumors. Front Oncol. (2019) 9:1151. doi: 10.3389/fonc.2019.01151
3. de Witt, AA, Lewis, M, and Schoeman, JP. Choroid plexus carcinoma in a dog—case report. Veterinary Record Case Reports. (2022) 10:e403. doi: 10.1002/vrc2.403
4. Westworth, DR, Dickinson, PJ, Vernau, W, Johnson, EG, Bollen, AW, Kass, PH, et al. Choroid plexus tumors in 56 dogs (1985-2007). J Vet Intern Med. (2008) 22:1157–65. doi: 10.1111/j.1939-1676.2008.0170.x
5. Stoica, G, Levine, J, Wolff, J, and Murphy, K. Canine astrocytic tumors: a comparative review. Vet Pathol. (2011) 48:266–75. doi: 10.1177/0300985810389543
6. Snyder, JM, Shofer, FS, Van Winkle, TJ, and Massicotte, C. Canine intracranial primary neoplasia: 173 cases (1986-2003). J Vet Intern Med. (2006) 20:669–75. doi: 10.1892/0891-6640(2006)20[669:cipnc]2.0.co;2
7. Roth, J, and Constantini, S. Hydrocephalus and brain tumors In: DD Limbrick Jr and JR Leonard, editors. Cerebrospinal fluid disorders: Lifelong implications. Cham: Springer International Publishing (2019). 199–217.
8. Antonakakis, MG, Carletti, BE, Anselmi, C, McGrath, S, and Minguez, JJ. Use of a telovelar approach for complete resection of a choroid plexus tumor in a dog. Vet Surg. (2022) 51:1273–9. doi: 10.1111/vsu.13859
9. Hosmann, A, Hinker, F, Dorfer, C, Slavc, I, Haberler, C, Dieckmann, K, et al. Management of choroid plexus tumors-an institutional experience. Acta Neurochir. (2019) 161:745–54. doi: 10.1007/s00701-019-03832-5
10. MDHRW. Youmans and Winn neurological surgery: 4 – volume set. 8th ed. Amsterdam: Elsevier (2022).
11. Teske, N, Chiquillo-Domínguez, M, Skrap, B, Harter, PN, Rejeski, K, Blobner, J, et al. Shunt dependency in supratentorial intraventricular tumors depends on the extent of tumor resection. Acta Neurochir. (2023) 165:1053–64. doi: 10.1007/s00701-023-05532-7
12. Beckmann, K, Kowalska, M, and Meier, V. Solitary intraventricular tumors in dogs and cats treated with radiotherapy alone or combined with ventriculoperitoneal shunts: a retrospective descriptive case series. J Vet Intern Med. (2023) 37:204–15. doi: 10.1111/jvim.16583
13. Kasowski, H, and Piepmeier, JM. Transcallosal approach for tumors of the lateral and third ventricles. Neurosurg Focus. (2001) 10:1–5. doi: 10.3171/foc.2001.10.6.4
14. Raybaud, C. The corpus callosum, the other great forebrain commissures, and the septum pellucidum: anatomy, development, and malformation. Neuroradiology. (2010) 52:447–77. doi: 10.1007/s00234-010-0696-3
15. van der Knaap, LJ, and van der Ham, IJM. How does the corpus callosum mediate interhemispheric transfer? Behav Brain Res. (2011) 223:211–21. doi: 10.1016/j.bbr.2011.04.018
16. Jea, A, Vachhrajani, S, Widjaja, E, Nilsson, D, Raybaud, C, Shroff, M, et al. Corpus callosotomy in children and the disconnection syndromes: a review. Childs Nerv Syst. (2008) 24:685–92. doi: 10.1007/s00381-008-0626-4
17. Markosian, C, Patel, S, Kosach, S, Goodman, RR, and Tomycz, LD. Corpus Callosotomy in the modern era: origins, efficacy, technical variations, complications, and indications. World Neurosurg. (2022) 159:146–55. doi: 10.1016/j.wneu.2022.01.037
18. Bagley, RS, Baszler, TV, Harrington, ML, Pluhar, GE, Moore, MP, Keegan, RD, et al. Clinical effects of longitudinal division of the corpus callosum in normal dogs. Vet Surg. (1995) 24:122–7. doi: 10.1111/j.1532-950X.1995.tb01306.x
19. Asada, R, Mizuno, S, Yu, Y, Hamamoto, Y, Anazawa, T, Ito, D, et al. Corpus Callosotomy in 3 cavalier king Charles spaniel dogs with drug-resistant epilepsy. Brain Sci. (2021) 11:1462. doi: 10.3390/brainsci11111462
20. Lehner, L, Czeibert, K, Jakab, C, Benczik, J, and Nagy, G. Transcallosal removal of a choroid plexus tumor from the lateral ventricle in a dog. Case report. Front Veterinary Sci. (2020) 7. doi: 10.3389/fvets.2020.00536
21. Wrede, B, Liu, P, and Wolff, JEA. Chemotherapy improves the survival of patients with choroid plexus carcinoma: a meta-analysis of individual cases with choroid plexus tumors. J Neuro-Oncol. (2007) 85:345–51. doi: 10.1007/s11060-007-9428-x
22. Dickinson, PJ. Advances in diagnostic and treatment modalities for intracranial tumors. J Vet Intern Med. (2014) 28:1165–85. doi: 10.1111/jvim.12370
23. Orlandi, R, Vasilache, CG, and Mateo, I. Palliative ventriculoperitoneal shunting in dogs with obstructive hydrocephalus caused by tumors affecting the third ventricle. J Vet Intern Med. (2020) 34:1556–62. doi: 10.1111/jvim.15818
24. Palamar, OI, Huk, AP, Teslenko, DS, Aksyonov, RV, Okonskyi, DI, and Lazko, NV. Postoperative complications in endoscopic frontal transcortical surgery of lateral and third ventricle tumours: speech disorders. Romanian Neurosurgery. (2021) 35:444–51. doi: 10.33962/roneuro-2021-075
25. El-Bendary, Y, Apra, C, Aldea, S, Chauvet, D, Dorfmüller, G, Ferrand-Sorbets, S, et al. Preservation of frontal white matter tracts in ventricular surgery: favoring an anterior interhemispheric transcallosal approach vs a transcortical transfrontal transventricular approach. Neurosurg Rev. (2022) 45:3349–59. doi: 10.1007/s10143-022-01841-0
26. Ginat, D, and Westesson, P-LA. Atlas of postsurgical neuroradiology: Imaging of the brain, spine, head, and neck. 2nd ed. United States: Springer International Publishing (2017).
27. Hermanson, JW, De, LA, and Evans, HE. Miller and Evans’ anatomy of the dog. 5th ed. St. Louis, Missouri: Elsevier (2020).
28. Alselisly, AMA, Ashry, AH, and Mahmoud, AT. Hydrocephalus with lateral ventricular lesions: case series and review of literature. Egyptian J Neurol, Psychiatry and Neurosurgery. (2021) 57:31. doi: 10.1186/s41983-021-00283-7
29. Suzuki, T. Treatment for hydrocephalus caused by intraventricular tumors. No Shinkei Geka. (2022) 50:429–40. doi: 10.11477/mf.1436204570
30. Zhang, C, Ge, L, Li, Z, Zhang, T, and Chen, J. Single-center retrospective analysis of risk factors for hydrocephalus after lateral ventricular tumor resection. Front Surgery. (2022) 9:886472. doi: 10.3389/fsurg.2022.886472
31. Pupin, RC, Rissi, DR, Gomes, DC, Gimelli, A, and Palumbo, MIP. High-grade astrocytoma with ventricular invasion in a dog. Veterinary Record Case Reports. (2019) 7:e000958. doi: 10.1136/vetreccr-2019-000958
32. Rissi, DR, Levine, JM, Eden, KB, Watson, VE, Griffin, JF, Edwards, JF, et al. Cerebral oligodendroglioma mimicking intraventricular neoplasia in three dogs. J Vet Diagn Investig. (2015) 27:396–400. doi: 10.1177/1040638715584619
33. Watson, F, Coppi, AA, Volk, HA, Packer, RMA, Tauro, A, and Rusbridge, C. Comparison of volume of the forebrain, subarachnoid space and lateral ventricles between dogs with idiopathic epilepsy and controls using a stereological approach: Cavalieri’s principle. Canine Med Genetics. (2021) 8:3. doi: 10.1186/s40575-021-00101-6
34. Tirrito, F, Cozzi, F, Bonaldi, M, Corazzo, S, Contiero, B, and Lombardo, R. Ventriculomegaly in cavalier king Charles spaniels with Chiari-like malformation: relationship with clinical and imaging findings. J Vet Med Sci. (2022) 84:1185–93. doi: 10.1292/jvms.22-0134
35. Farke, D, Kolecka, M, Czerwik, A, Wrzosek, M, Schaub, S, Kramer, M, et al. Prevalence of seizures in dogs and cats with idiopathic internal hydrocephalus and seizure prevalence after implantation of a ventriculo-peritoneal shunt. J Vet Intern Med. (2020) 34:1986–92. doi: 10.1111/jvim.15890
36. Horiuchi, S, Kanaya, K, and Horiuchi, T. The occurrence and relationship of postoperative seizure and de novo epilepsy after craniotomy surgery: a retrospective single-center cohort study. Front Surg. (2022) 9:881874. doi: 10.3389/fsurg.2022.881874
Keywords: transcallosal, dog, lateral ventricle, choroid plexus tumor, surgery, craniotomy, astrocytoma, ventriculomegaly
Citation: Lehner L, Czeibert K, Csébi P, Diószegi K and Nagy G (2023) Case report: Intraventricular tumor removal using transcallosal approach and follow-up in three dogs. Front. Vet. Sci. 10:1240934. doi: 10.3389/fvets.2023.1240934
Edited by:
Daisuke Hasegawa, Nippon Veterinary and Life Science University, JapanReviewed by:
John Henry Rossmeisl, Virginia Tech, United StatesShinichi Kanazono, Veterinary Specialists and Emergency Center, Japan
Copyright © 2023 Lehner, Czeibert, Csébi, Diószegi and Nagy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: László Lehner, ZHIubGVobmVyLmxhc3psb0BnbWFpbC5jb20=