 Daniel Felipe Barrantes Murillo1†
Daniel Felipe Barrantes Murillo1† Stephanie Anderson2
Stephanie Anderson2 Christian Capobianco3
Christian Capobianco3 Gregory A. Lewbart3†
Gregory A. Lewbart3† Nathan P. Wiederhold4†Connie F. Cañete-Gibas4
Nathan P. Wiederhold4†Connie F. Cañete-Gibas4 Tatiane Terumi Negrão Watanabe2,5*†
Tatiane Terumi Negrão Watanabe2,5*†- 1Department of Pathobiology, College of Veterinary Medicine, Auburn University, Auburn, AL, United States
- 2Department of Population Health and Pathobiology, College of Veterinary Medicine, North Carolina State University, Raleigh, NC, United States
- 3Department of Clinical Science, College of Veterinary Medicine, North Carolina State University, Raleigh, NC, United States
- 4Fungus Testing Laboratory, Department of Pathology and Laboratory Medicine, University of Texas Health Science Center at San Antonio, San Antonio, TX, United States
- 5Antech Diagnostics, Los Angeles, CA, United States
Phaeohyphomycosis is an infection caused by melanized fungi. This disease has been reported in several animal species including invertebrates, cold-blooded vertebrates, mammals, and humans. Melanized fungi have similar phenotypical features and confirmation requires culture and molecular diagnostics. To exemplify this we present a case of a 333 g adult of unknown age, free-ranging, male Eastern box turtle (Terrapene carolina carolina) that was referred to the Turtle Rescue Team at North Carolina State University for evaluation of multilobulated masses occupying the entire left orbit and at the right forelimb on the plantarolateral aspect of the foot. A fine needle aspirate cytologic examination of the mass on the right forelimb revealed large numbers of inflammatory cells and fungal organisms. Histopathology of the skin biopsies from the right forefoot was consistent with phaeohyphomycosis. A course of antifungal medication was started (Fluconazole 21 mg/kg loading dose IV then 5 mg/kg PO SID q 30 days). Due to concern for the patient's quality of life and the lack of a curative treatment plan, humane euthanasia was elected. Gross and histological postmortem examination confirmed the presence of multiple coelomic masses similar in appearance to those observed in the left orbit and right forefoot indicating disseminated phaeohyphomycosis. A swab of the periocular mass was submitted for fungal culture and phenotypic identification. The isolate was later identified as Exophiala equina through a combination of phenotypic characterization and sequencing of the ITS region of the nuclear rDNA. Exophiala is a genus in the family Herpotrichiellaceae, order Chaetothyriales and is considered an opportunistic “black yeast” causing infection in aquatic invertebrates, fish, amphibians, reptiles, and mammals including humans. Exophiala equina is infrequently reported in animals, with only three cases in the literature including the herein report.
1. Introduction
Exophiala is a genus in the family Herpotrichiellaceae, order Chaetothyriales, that produces opportunistic “black yeast” by budding an annellidic conidiogenesis (1). Exophiala species are associated with opportunistic infection in animals and humans. The most relevant species usually reported as pathogens in humans are Exophiala dermatitidis, E. spinifera, and E. asiatica (1). Exophiala spp. infections also have been reported in crustaceans (Ucides cordatus), captive and farmed fish (Salmo salar, Mustelus canis, among others), amphibians (Hyla caerulae, H. sptentrionali, Phyllobatest rinitatis, among others), aquarium animals, and other cold-blooded vertebrates (2). Exophiala spp. infection is also reported in humans and mammals including dogs, cats, and a horse (2). Table 1 summarizes the selected cases of Exophiala spp. infection in vertebrate animals. Cold-blooded vertebrates usually develop a systemic infection, unlike mammals where localized skin or subcutaneous infections are reported. E. equina was first described as the causative pathogenic agent in a lower limb infection of a horse (3) and to our knowledge, it has not been described in mammals since then. There is a report of systemic infection caused by strain CBS 116009 of E. equina causing disseminated infection in a Galapagos giant tortoise (Geochelone nigra) (4). Other reported species of Exophiala causing disease in turtles are Aldabra tortoise (Geochelone gigantea) and Eastern box turtle (Terrapene carolina carolina) infected by Exophiala oligospermia and Exophiala jeanselmei respectively (5, 6). There is a case of oral granuloma and disseminated granulomas caused by Exophiala spp in a Radiated tortoise (Astrochelys radiata) (7). To our knowledge, this is the first report of Exophiala equina infection in an Eastern box turtle (Terrapene carolina carolina) and the third reported infection in animals.

Table 1. Selected cases of Exophiala infection in vertebrate animals.
2. Case presentation
A 333 g, adult of unknown age, free-ranging, male Eastern box turtle (Terrapene carolina carolina) was referred to the Turtle Rescue Team (TRT) at the College of Veterinary Medicine, North Carolina State University for evaluation of multiple proliferative growths on the right foreleg and the left orbit. On physical examination, the turtle was uncomfortable on palpation of the masses. One mass was occupying the entire left orbit and along the right forelimb on the plantar and lateral aspect of the foot (Figure 1). The clinical management timeline is summarized in Table 2. There was no purulent material on aspiration of the forelimb lesion, however reptile's abscesses have caseous debris, thus the lack of purulent exudate did not rule out an abscess. Given the history of a free-ranging animal, uncomforted upon palpation and a possible caseous abscesses an empiric treatment with a non-steroidal anti-inflammatory drug (ketoprofen 2 mg/kg IM SID for 3 days) and antibiotic medication (ceftazidime, 20 mg/kg, IM, q96hrs, 4 doses) was prescribed at the time of initial evaluation to provide analgesia and cover a potential bacterial infection. The treatment was instituted until the patient was more comfortable to perform cytology and biopsy of the lesions. Five days after the initial presentation, a full physical examination was performed under sedation with alfaxalone (10 mg/kg IV) and morphine (1.5 mg/kg IM). A fine needle aspirate of the mass from the right forelimb was taken. Cytologic examination revealed abundant numbers of macrophages and heterophils, and multinucleated giant cells with numerous intracellular and extracellular, 5–15 μm diameter, round to ovoid elongated, occasionally forming chains, fungal organisms with a refractile wall. Two punch samples of the mass along the right forelimb were taken for histological evaluation. Histopathology of skin biopsies identified heterophilic granulomatous dermatitis, and panniculitis with intralesional pigmented fungal hyphae (consistent with phaeohyphomycosis). On day 13, a course of antifungal medication was started following the results of the cytology and the histopathology reports (fluconazole 21 mg/kg loading dose IV then 5 mg/kg PO SID q 30 days). Fluconazole was chosen due to the previous pharmacokinetic studies supporting its use in marine turtles for treating fungal infections and for being readily available in an oral formulation for use in TRT (34, 35). On day four after starting the antifungal treatment, the turtle was reluctant to medicate PO and the medication was injected into a mealworm and fed to the patient. At the end of the antifungal treatment, the turtle was still eating, drinking, defecating, and urinating. The bloodwork yielded a PCV of 17% (reference value: 8–34%) and total solids were 8.0 g/dL (reference interval: 3–10.6 g/dL) (36). However, there was no resolution of the lesions. The masses were larger, and the lesion on the left eye spread caudally. A CT scan was performed, and the fungal infection had spread to the lungs and other organs. Due to poor prognosis, humane euthanasia was elected 6 weeks after the initial evaluation. The animal was sedated by applying an alfaxalone IV (10 mg/kg) at the subcarapacial plexus. After sedation euthanasia was applied by injecting euthanasia solution of sodium pentobarbital IV (100 mg/kg) at the post-occipital sinus. Death was confirmed by lack of deep pain response, lack of corneal reflex, rigor mortis, and absence of Doppler heart rate.

Figure 1. An adult of unknown age, intact male Eastern box turtle (Terrapene carolina carolina) with a mass was observed occupying the entire orbit of the left eye and right forelimb on the plantar and lateral aspect of the foot.
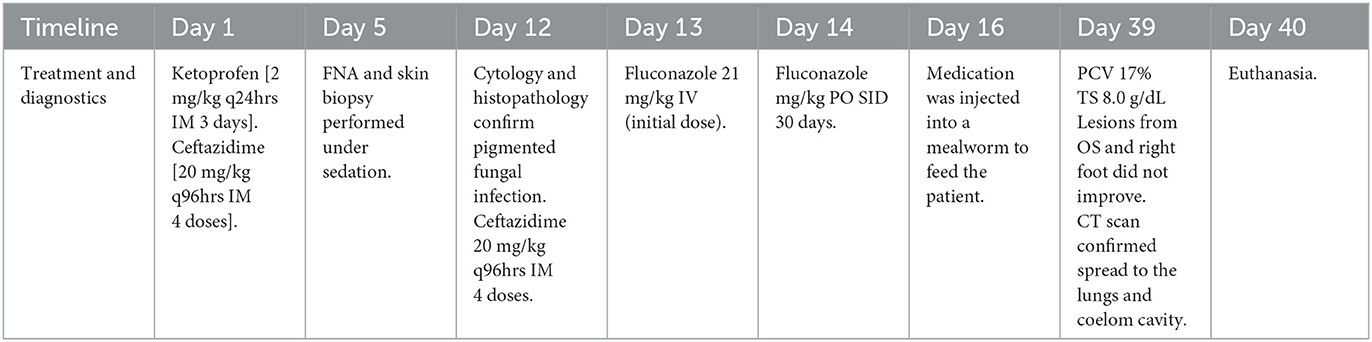
Table 2. Clinical management timeline of a free-ranging, male Eastern box turtle (Terrapene carolina carolina) referred to the Turtle Rescue Team (TRT).
Post-mortem evaluation revealed the adipose tissue stores (visceral and subcutaneous) were markedly reduced with mild to moderate, diffuse skeletal muscle atrophy. There was a moderate expansion of the left periorbital tissue by an approximately 2.0 × 2.0 × 0.7 cm, soft, tan to gray, multilobulated mass which obscured the left orbit and partially covered the globe (Figure 1). Similar spherical ovoid masses were found located at the ventral aspect of the right forefoot (1.5 × 1.5 × 0.8 cm), ventricular epicardium (0.4 cm in diameter), both lung lobes (up to 0.3 in diameter) and scattered throughout the coelomic cavity, specifically in regions of lymphatic trunks and sinuses (2.0 × 1.0 × 1.0 cm). On cut surface, these masses had fine, brown-black stippling.
Histologically, the dermis, subcutis of the right front foot, and left periocular subcutaneous tissue were markedly expanded and replaced by coalescing granulomas (Figure 2A) containing abundant central pigmented fungal hyphae and yeast-like cells, single or forming chains with vesicle swellings mixed with eosinophilic necrotic debris (Figure 2B). Hyphae measured ~5–7 μm in diameter with parallel walls and regular septation. Yeast-like cells were irregularly ovoid and ranged from 7 μm to 20 μm in diameter and occasionally formed chains (pseudohyphae). Fungal organisms were surrounded by large numbers of Langhans multinucleated giant cells, epithelioid macrophages, and fewer heterophils which were further surrounded by large numbers of lymphocytes and plasma cells. In the overlying epidermis, the foot mass is focally ulcerated and replaced by abundant necrotic debris, hemorrhage, heterophils, fungal hyphae and yeast, and myriad coccobacilli. Moderate to marked hyperkeratosis was observed on the overlying lesser affected epidermis. Similar histological findings were found upon histological examination of the masses located at the ventricular epicardium, lungs, and coelomic cavity.
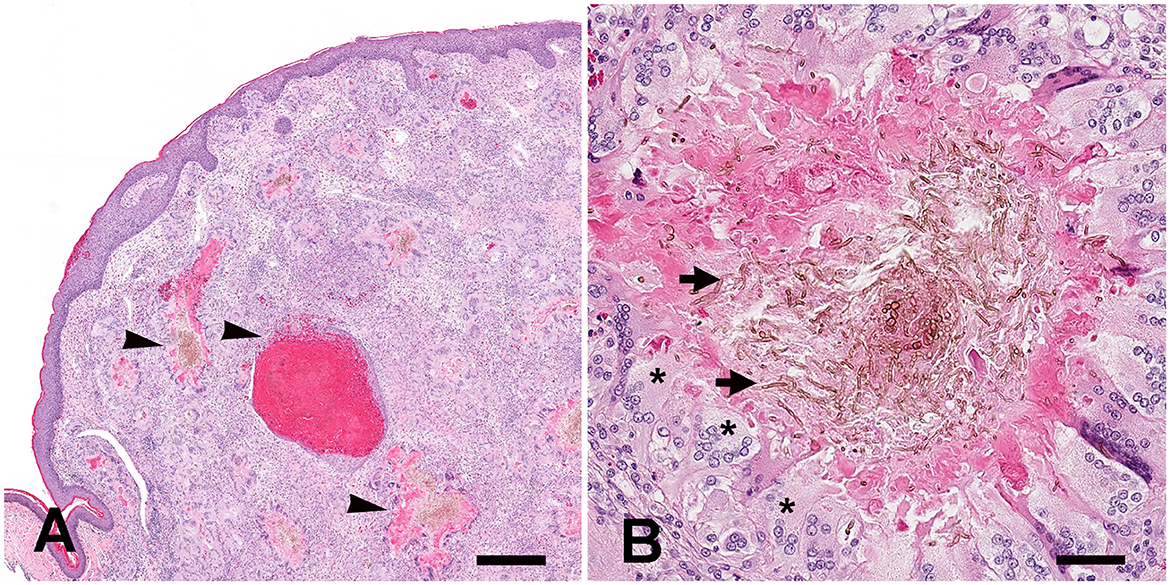
Figure 2. Systemic Exophiala equina infection in an Eastern box turtle (Terrapene carolina carolina). (A) Histologically, the dermis and subcutis of the right front foot were markedly expanded and replaced by coalescing granulomas (arrowheads). H&E stain. Bar size= 400 μm. (B) Granulomas contained large numbers of central pigmented fungal hyphae and yeast-like cells mixed with eosinophilic necrotic debris (arrows). Hyphae measured approximately 5 um to 7 um in diameter with parallel walls and regular septation. Yeast-like cells were irregularly ovoid and ranged from 7 um to 20 um in diameter and occasionally formed chains (pseudohyphae). Fungal organisms were surrounded by large numbers of Langhans multinucleated giant cells (asterisks), epithelioid macrophages. H&E stain. Bar size= 50 μm.
A swab of the periocular mass was submitted for fungal culture and the isolate was sent to the Fungal Testing Laboratory, University of Texas Health at San Antonio, Texas (FTL) for identification and antifungal sensitivity testing (UTHSCSA DI23-28). The isolate was presumptively identified as an Exophiala species based on phenotypic characteristics i.e., restricted suede black colonies on potato flakes agar (PFA) and yeast-like cells shown from slide culture mounts and direct tease mounts for microscopy. A subculture was submitted for sequencing of the internal transcribed spacer region (ITS) and the D1/D2 domain of the large subunit of the nuclear rDNA (LSU). The sequences were used to perform BLASTn searches to compare with available sequences of Exophiala species in GenBank (https://blast.ncbi.nlm.nih.gov/Blast.cgi). The ITS2 portion of the sequence was also subjected to a barcode BLAST using an updated Barcode identifier database for herpotrichiellaceous black yeasts and relatives (37, 38).
Top matches in BLASTn searches (accessed December 18, 2020) for ITS were Exophiala equina CBS 119.13T (100%), Exophiala tremulae CBS 129355T (99.03%), Exophiala radicis CBS 140402T (98.63%) and top matches for LSU were Exophiala equina CBS 128222 (99.84%), Exophiala equina CBS 115143 (99.84%), Exophiala pisciphila CBS 100.68 (99.84%). Barcode analysis using the updated Barcode identifier database for herpotrichiellaceous black yeasts and relatives resulted in a 100% match with Exophiala equina CBS 119.13T confirming the identity of UTHSCSA DI23-28 as Exophiala equina.
3. Discussion and literature review
Phaeohyphomycosis is a subcutaneous or systemic infection caused by melanized fungi characterized by the presence of yeast cells, septate hyphae, or pseudohyphae morphologies within the necrotic tissue sections (39). Fungi genera incriminated as causative agents of phaeohyphomycosis include Exophiala, Hormonema, Dreschlera, Curvularia, Chaetomium, Phoma, Alternaria, Cladosporium, Madurella, Fonsecaea, Cladiophialophora, and Bipolaris (40, 41).
Systemic infections can be categorized as disseminated if multiple organs are affected or localized when targeting a single organ. The two more commonly affected organs are the brain and lungs (2).
Exophiala equina belongs to the salmonis-clade with other related species including E. psychrophila, E. opportunistica, E. salmonis, E. pisciphila, E. aquamarina, E. cancerae, and E. brunnea (42). E. equina is isolated from water sources and watery environments, including drinking water, a cooling system on a packaging machine, the tubing of a gelly installation, silica gel, and washing of Tilia roots, among others (1). E. equina has been isolated from human patients from the Netherlands, Germany, Denmark, and the United States (42).
The diagnosis of Exophiala equina infection and black yeasts mycosis in general is a combined approach between culture, direct microscopy, histopathologic examination of clinical samples, and molecular analysis. Melanin is consistently present among Exophiala species, in the vegetative and reproductive stages, thus colonies are typically olivaceous, with dark gray or black shades on culture. This color is attributed to the presence of dihydroxynaphthalene (DHN)-derived melanin (1, 43). The growth of these fungi is invariably slow. Exophiala is the only genus that can produce a yeast-like phase among the Chaetothyriales (1, 43). Microcyclic conidiation produces the yeast-like appearance of Exophiala species. The liberated cells inflate and reproduce by budding, and change to hyphae by binding inflated cells, this is known as “tortulose mycelium” (1). Exophiala species have subtle distinctive morphological features; e.g., E. spinifera has long conidiophores with long annellated zones, E. dermatitidis has very short annelated zones next to each other in a single cell and Exophiala equina has ellipsoidal conidia and thick-walled, non-deciduous chlamydospores (44). DNA sequencing is required for accurate identification. BLASTn searches in GenBank are also not reliable for accurate identification because many sequences in the GenBank may represent strains that are incorrectly identified. A recently discovered fragment of about 50 bp in the ITS2 region that can be used for barcode analysis to differentiate Exophiala and other herpotrichiellaceous species and allows for accurate identification to the species level (37). Since the strains list for the barcode database was published in 2013, the database needs to be updated every time it is used so newly described Exophiala and other herpotrichiellaceaous species are included.
Phaeohyphomycosis requires a long, multimodal therapy combining antifungal drugs, surgery, thermotherapy, and chemotherapy in humans (2). Phaeohyphomycosis has been treated historically with a combination of antifungal agents, however, there is no standard therapy. Recently itraconazole, voriconazole, and posaconazole demonstrated consistent in vitro activity (2). Several protocols are mentioned in human literature, including a triple combination of amphotericin B, flucytosine, and itraconazole or the recent use of echinocandins (caspofungin, micafungin, and anidulafungin) (2). Itraconazole alone or in combination with Terbinafine is a commonly used protocol in human patients to treat black yeasts (2).
In general, phaeohyphomycosis is seldom reported in reptiles; however, there is a strong representation of box turtles among these cases, suggesting that this species is particularly susceptible or is just a coincidence due to the popularity of this animals as pets (40). Exophiala reported infections in dogs, fish, and cats are usually fatal or require euthanasia (4).
The knowledge of antifungal therapy for phaeohyphomycosis in reptiles is limited. Among the several drug families of antifungal agents, only the kinetics of azole drugs are described in reptiles (45). The most frequently used antifungals in reptiles are polyene macrolides (amphotericin B and nystatin) and azoles (ketoconazole, itraconazole, thiabendazole, fluconazole) (45). Fluconazole is the treatment of choice in reptiles, due to its effectiveness against numerous fungal species (4). The pharmacokinetic properties of fluconazole were investigated in six juvenile loggerhead sea turtles (Caretta caretta) (35). In this study, the authors concluded that fluconazole can be used at a dose of 10 mg/kg every 5 days after a loading dose of 21 mg/kg maintaining a desired stable concentration to effectively treat fungal infections (35). Fluconazole was used as a treatment for carpal osteomyelitis in a Kemp's ridley sea turtle (Lepidochelys kempii) caused by an unidentified non pigmented septate fungal hyphae in combination with Nocardia sp. (34). There was resolution of the lesions after 1 year of therapy, using Fluconazole 2.5 mg/kg SC q24hr and azithromycin (34). Fluconazole was used in this case, and a poor response of the lesions was noted, like the previous case report in a Galapagos tortoise (4). In that case, the treatment was for 3 days after enucleation of the left eye at a dose of 2 mg/kg PO SID (4). The necropsy confirmed a systemic phaeohyphomycosis with granulomatous inflammation within the lungs, epicardium, myocardium coelom, liver, kidney, spleen, oral cavity skeletal muscle, and thyroid (4). In the case reported herein, a poor response to the treatment was documented after 27 days of fluconazole PO, 5 mg/kg, q24 hrs after an initial loading dose of 21 mg/kg IV. Other reported treatments in turtles include combination therapy of oral terbinafine hydrochloride and a topical suspension of fluconazole in combination with surgical debridement (6). The treatment was for 17 months after the clinical presentation and was discontinued due to the patient's stable clinical condition and response to the treatment, however in this case the infection was caused by E. oligospermia and did not extend to the internal organs (6). Treatment was not pursued in the reported case of Exophiala jeanselmei infection in an Eastern box turtle (Terrapene carolina carolina) (5). In our case, we speculated that the disseminated disease precluded the clinical outcome of the patient and the fluconazole efficacy. Fluconazole plasma concentration above 8 μg/ml is targeted on therapies for fungal infections (34, 35), however, no measurements were performed in this case. There is no information available on the treatment of Exophiala equina infection in a horse.
There are several limitations in this case. For instance, this was a free-ranging animal, thus critical information regarding husbandry, diet, immune status, or previous disease was unavailable, unlike pet animals. The incidence of infections caused by Exophiala equina is so low that precludes the identification of specific risk factors in turtles. Although the fungus is isolated from water sources (42); the reported cases start with a cutaneous and subcutaneous infection that progresses to systemic fungi infection. The explanation of how the fungi progress from cutaneous infection to systemic remains unclear. Pathogenic melanized fungi have several virulence factors that enhance virulence and pathogenicity and can contribute to this phenomenon. The most important factors include melanin, cell polymorphism, cell adhesion, and hydrophobicity (43). Thermotolerance is an important virulence factor that allows melanized fungi to infect different hosts. Differences in maximum growth temperatures in Exophiala species establish the predilection for cold-blooded and warm-blooded hosts (43). Exophiala equina growth at a minimum of 4oC, optimum growth at 24–30oC, maximum of 33–36oC, and no growth at 37oC (42). These important features may explain why E. equina infections in warm-blooded hosts take place in the extremities. In humans, even though E. equina does not grow at 37oC, it can cause superficial cutaneous and subcutaneous infections in humans, but not disseminated infections into visceral organs. The only description of Exophiala equina in a domestic animal was causing a localized infection in a distal limb of a horse, like humans (3). The two cases reported in turtles (including the reported case herein), presented disseminated disease with hematogenous spread affecting visceral organs, and the left orbit. The affected animals have a chronic course of the disease, and the underlying initial insult cannot be determined. Traumatic inoculation is a common route of infection for many black yeasts (44). We presumed traumatic inoculation of the agent took place in this case. In cold-blooded vertebrates, predisposing factors include transportation adjacent to basins, stress under aquarium conditions, environmental changes, and pollution (2).
4. Conclusion
Exophiala equina is a melanized fungus that causes phaeohyphomycosis in animals and humans. This agent was described for the first time a century ago and is infrequently reported in the veterinary literature, and consists solely of three case reports including the reported case herein. In turtles, the clinical presentation manifests as a systemic infection with hematogenous spread and a mortality rate of 100%. Treatment with fluconazole has been unsuccessful. Although it is zoonotic, this agent does not grow at 37oC, and this is reflected in the clinical presentation in humans and mammals (skin and subcutaneous infection). The limitations of this case are related to the scant available literature, the undetermined route of infection, and the animal's background. This report bolsters the literature on Exophiala in reptiles and helps bring awareness of this pathogen and the clinical signs it produced to veterinary clinicians working with turtles and other reptiles. Unfortunately, the treatment was not successful in controlling the infection, and euthanasia was elected. Patient size and finances further limited reasonable efforts. The strengths of this case include the detailed clinical and pathological findings associated with the disease, the use of therapeutic supported by the literature, and the comprehensive multimodal approach which includes a combination of culture, histopathology, and molecular diagnostics to aim for a definitive diagnosis. Molecular diagnostic methods such as the sequencing of the ITS and proteomics such as MALDI-TOF MS, are necessary to correctly identify Exophiala species. The major takeaway lesson from this case is that if a diagnosis of Exphiala is confirmed the prognosis should be guarded and euthanasia might be the most reasonable clinical course. For those clinicians electing chemotherapy drugs other than fluconazole should be selected. Further experimental studies are required to have a more comprehensive understanding of its pathogenesis in animals and improve the therapeutic approach.
Data availability statement
The original contributions presented in the study are included in the article material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical review and approval were not required for this case, because the turtle was submitted for routine diagnostic postmortem examination to the Department of Pathobiology and as such is not subject to animal ethics guidelines.
Author contributions
CC and GL followed the clinical case. TN performed the postmortem examination, sample collection, final post-mortem report, contributed to the design, supervised the study, and critically revised and edited the manuscript. NW and CC-G performed taxonomic and molecular identification of the agent. DB and SA prepared the manuscript and literature review. SA, DB, CC, GL, NW, CC-G, and TN reviewed the final submission. All authors read and approved the final manuscript.
Acknowledgments
We acknowledge Kent Passingham and the Turtle Rescue Team students for their efforts and support.
Conflict of interest
TN is employed by Antech Diagnostics.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Najafzadeh MJ, Suh MK, Lee MH, Ha GY, Kim JR, Kim TH, et al. Subcutaneous phaeohyphomycosis caused by Exophiala equina, with susceptibility to eight antifungal drugs. J Med Microbiol. (2013) 62:797–800. doi: 10.1099/jmm.0.057406-0
2. Seyedmousavi S, Bosco SMG, de Hoog S, Ebel F, Elad D, Gomes RR, et al. Fungal infections in animals: a patchwork of different situations. Med Mycol. (2018) 56:165–87. doi: 10.1093/mmy/myx104
3. Pollacci G. Miceti del corpo umano e degli animali. Atti dell'Istituto Botanico Università di Pavia. (1923) 18: 1– 9.
4. Manharth A, Lemberger K, Mylniczenko N. Disseminated phaeohyphomycosis due to Exophiala species in a Galapagos tortoise, Geochelone nigra. J Herpetol Med Surg. (2005) 15:20–6. doi: 10.5818/1529-9651.15.2.20
5. Joyner PH, Shreve AA, Spahr J, Fountain AL, Sleeman JM. Phaeohyphomycosis in a free-living eastern box turtle (Terrapene carolina carolina). J Wildl Dis. (2006) 42:883–8. doi: 10.7589/0090-3558-42.4.883
6. Stringer EM, Garner MM, Proudfoot JS, Ramer JC, Bowman MR, Heng HG, et al. Phaeohyphomycosis of the carapace in an Aldabra tortoise (Geochelone gigantea). J Zoo Wildl Med. (2009) 40:160–7. doi: 10.1638/2008-0035.1
7. Frank W. Mycotic Infections in Amphibians and Reptiles in Wildlife Diseases. New York, NY: Plenum Press, 73–88 (1976).
8. McGinnis MR, Ajello L, A. new species of Exophiala isolated from channel catfish. Mycologia. (1974) 66:518–20. doi: 10.1080/00275514.1974.12019633
9. Otis EJ, Wolke RE. Blazer VS. Infection of Exophiala salmonis in Atlantic salmon (Salmo salar L) J Wildl Dis. (1985) 21:61–4. doi: 10.7589/0090-3558-21.1.61
10. Munchan C, Kurata O, Wada S, Hatai K, Sano A, Kamei K, et al. Exophiala xenobiotica infection in cultured striped jack, Pseudocaranx dentex (Bloch & Schneider), in Japan. J Fish Dis. (2009) 32:893–900. doi: 10.1111/j.1365-2761.2009.01068.x
11. Gjessing MC, Davey M, Kvellestad A, Vrålstad T. Exophiala angulospora causes systemic inflammation in atlantic cod Gadus morhua. Dis Aquat Organ. (2011) 96:209–19. doi: 10.3354/dao02381
12. Overy DP, Groman D, Giles J, Duffy S, Rommens M, Johnson G. Exophiala angulospora Causes Systemic Mycosis in Atlantic Halibut: A Case Report. J Aquat Anim Health. (2015) 27:12–9. doi: 10.1080/08997659.2014.953266
13. Camus A, Berliner A, Hyatt M, Hatcher N, Clauss T. Exophiala xenobiotica aerocystitis in a Queensland grouper Epinephelus lanceolatus (Bloch). J Fish Dis. (2015) 38:221–5. doi: 10.1111/jfd.12224
14. Rehulka J, Kubátová A, Hubka V. Swim bladder mycosis in pretty tetra (Hemigrammus pulcher) caused by Exophiala pisciphila and Phaeophleospora hymenocallidicola, and experimental verification of pathogenicity. J Fish Dis. (2018) 41:487–500. doi: 10.1111/jfd.12750
15. Rehulka J, Kolarík M, Hubka V. Disseminated infection due to Exophiala pisciphila in Cardinal tetra, Paracheirodon axelrodi. J Fish Dis. (2017) 40:1015–24. doi: 10.1111/jfd.12577
16. Saraiva M, Beckmann MJ, Pflaum S, Pearson M, Carcajona D, Treasurer JW. Exophiala angulospora infection in hatchery-reared lumpfish (Cyclopterus lumpus) broodstock. J Fish Dis. (2019) 42:335–43. doi: 10.1111/jfd.12940
17. Nyaoke A, Weber ES, Innis C, Stremme D, Dowd C, Hinckley L. Disseminated phaeohyphomycosis in weedy seadragons (Phyllopteryx taeniolatus) and leafy seadragons (Phycodurus eques) caused by species of Exophiala, including a novel species. J Vet Diagn Invest. (2009) 21:69–79. doi: 10.1177/104063870902100111
18. Gaskins JE, Cheung PJ. Exophiala pisciphila. A study of its development. Mycopathologia. (1986) 93:173–84. doi: 10.1007/BF00443521
19. Marancik DP, Berliner AL, Cavin JM, Clauss TM, Dove AD, Sutton DA. Disseminated fungal infection in two species of captive sharks. J Zoo Wildl Med. (2011) 42:686–93. doi: 10.1638/2010-0175.1
20. Erlacher-Reid CD, Nollens HH, Schmitt TL, St Leger J, Sunico S. Phaeohyphomycosis associated with ossification of the skull and cervical vertebrae in a swell shark (Cephaloscyllium Ventriosum). J Zoo Wildl Med. (2016) 47:1081–5. doi: 10.1638/2016-0032.1
21. Bizjak-Mali L, Zalar P, Turk M, Babicč MN, Kostanjšek R, Gunde-Cimerman N. Opportunistic fungal pathogens isolated from a captive individual of the European blind cave salamander Proteus anguinus. Dis Aquat Organ (2018) 129:15–30. doi: 10.3354/dao03229
22. Seilern-Moy K, Fernandez JR, Macgregor SK, John SK, Linton C, Cunningham AA. Fatal phaeohyphomycosis due to Exophiala sp. infection in a free-living common toad Bufo bufo. Dis Aquat Organ. (2019) 133:19–24. doi: 10.3354/dao03341
23. Hopf C, Graham EA, Gibas CFC, Sanders C, Mele J, Fan H, et al. Novel Exophiala species associated with disseminated granulomatous inflammation in a captive eastern hellbender (Cryptobranchus alleganiensis alleganiensis). Front Vet Sci. (2020) 7:25. doi: 10.3389/fvets.2020.00025
24. Davidson WR, Shotts EB, Teska J, Moreland DW. Feather damage due to mycotic infections in wild turkeys. J Wildl Dis. (1989) 25:534–9. doi: 10.7589/0090-3558-25.4.534
25. Bostock DE, Coloe PJ, Castellani A. Phaeohyphomycosis caused by Exophiala jeanselmei in a domestic cat. J Comp Pathol. (1982) 92:479. doi: 10.1016/0021-9975(82)90035-4
26. Helms SR, McLeod CG. Systemic Exophiala jeanselmei infection in a cat. J Am Vet Med Assoc. (2000) 217:1858–61. doi: 10.2460/javma.2000.217.1858
27. Maeda H, Shibuya H, Yamaguchi Y, Miyoshi T, Irie M, Sato T. Feline digital phaeohyphomycosis due to Exophiala jeanselmei. J Vet Med Sci. (2008) 70:1395–7. doi: 10.1292/jvms.70.1395
28. Nuttal W, Woodgyer A, Butler S. Phaeohyphomycosis caused by Exophiala jeanselmei in a domestic cat. N Z Vet J. (1990) 38:123. doi: 10.1080/00480169.1990.35635
29. Kettlewell P, McGinnis MR, Wilkinson GT. Phaeohyphomycosis caused by Exophiala spinifera in two cats. J Med Vet Mycol. (1989) 27:257–64. doi: 10.1080/02681218980000341
30. Overy DP, Martin C, Muckle A, Lund L, Wood J, Hanna P. Cutaneous Phaeohyphomycosis Caused by Exophiala attenuata in a Domestic Cat. Mycopathologia. (2015) 180:281–7. doi: 10.1007/s11046-015-9909-y
31. Kano R, Kusuda M, Nakamura Y, Watanabe S, Tsujimoto H, Hasegawa A. First isolation of Exophiala dermatitidis from a dog: identification by molecular analysis. Vet Microbiol. (2000) 76:201–5. doi: 10.1016/S0378-1135(00)00229-7
32. Murphy KF, Malik R, Barnes A, Hotston-Moore A, Pearson GR, Barr FJ. Successful treatment of intra-abdominal Exophiala dermatitidis infection in a dog. Vet Rec. (2011) 168:217. doi: 10.1136/vr.c6351
33. Eustis SL, Kirkbride CA, Gates C, Haley LD. Porcine abortions associated with Fungi, Actinomycetes, and Rhodococcus sp. Vet Pathol. (1981) 18:608–13. doi: 10.1177/030098588101800505
34. Harms CA, Lewbart GA, Beasley J. Medical Management of mixed nocardial and unidentified fungal osteomyelitis in a kemp's ridley sea turtle, Lepidochelys kempii. J Herpetol Med Surg. (2002) 12:21–6. doi: 10.5818/1529-9651.12.3.21
35. Mallo KM, Harms CA, Lewbart GA, Papich MG. Pharmacokinetics of fluconazole in loggerhead sea turtles (Caretta caretta) after single intravenous and subcutaneous injections, and multiple subcutaneous injections. J Zoo Wildl Med. (2002) 33:29–35. doi: 10.1638/1042-7260(2002)033[0029:POFILS]2.0.CO;2
36. Adamovicz L, Bronson E, Barrett K, Deem SL. Health assessment of free-living eastern box turtles (Terrapene carolina carolina) in and around the Maryland Zoo in Baltimore 1996-2011. J Zoo Wildl Med. (2015) 46:39–51. doi: 10.1638/2014-0066R.1
37. Heinrichs G, de Hoog GS, Haase G. Barcode identifiers as a practical tool for reliable species assignment of medically important black yeast species. J Clin Microbiol. (2012) 50:3023–30. doi: 10.1128/JCM.00574-12
38. Thitla T, Kumla J, Khuna S, Lumyong S, Suwannarach N. Species Diversity, Distribution, and Phylogeny of Exophiala with the Addition of Four New Species from Thailand. J Fungi. (2022) 8:766. doi: 10.3390/jof8080766
39. Malduin EA, Peters-Kennedy J. Integumentary System in Jubb, Kennedy and Palmer's Pathology of Domestic Animals. Saint Louis, MO; Elsevier, 511–736 (2016).
40. Jacobson ER. Infectious Diseases and Pathology of Reptiles. Color Atlas and Text. CRC Press Taylor Francis Group, Boca Raton (2007).
41. Guarner J, Brandt ME. Histopathologic diagnosis of fungal infections in the 21st century. Clin Microbiol Rev. (2011) 24:247–80. doi: 10.1128/CMR.00053-10
42. de Hoog GS, Vicente VA, Najafzadeh MJ, Harrak MJ, Badali H, Seyedmousavi S. Waterborne Exophiala species causing disease in cold-blooded animals. Persoonia. (2011) 27:46–72. doi: 10.3767/003158511X614258
43. Queiroz-Telles F, de Hoog S, Santos DW, Salgado CG, Vicente VA, Bonifaz A. Chromoblastomycosis. Clin Microbiol Rev. (2017) 30:233–76. doi: 10.1128/CMR.00032-16
44. Seyedmousavi S, Netea MG, Mouton JW, Melchers WJ, Verweij PE, de Hoog GS. Black yeasts and their filamentous relatives: principles of pathogenesis and host defense. Clin Microbiol Rev. (2014) 27:527–42. doi: 10.1128/CMR.00093-13
Keywords: Exophiala equina, phaeohyphomycosis, systemic mycosis, eastern box turtle, reptile
Citation: Barrantes Murillo DF, Anderson S, Capobianco C, Lewbart GA, Wiederhold NP, Cañete-Gibas CF and Negrão Watanabe TT (2023) Systemic Exophiala equina infection in an Eastern box turtle (Terrapene carolina carolina): a case report and literature review. Front. Vet. Sci. 10:1158393. doi: 10.3389/fvets.2023.1158393
Received: 03 February 2023; Accepted: 21 April 2023;
Published: 12 May 2023.
Edited by:
Robert James Ossiboff, University of Florida, United StatesReviewed by:
Zoe Mack, Wildlife Conservation Society, United StatesVeronica Risco-Castillo, INRA École Nationale Vétérinaire d'Alfort (ENVA), France
Copyright © 2023 Barrantes Murillo, Anderson, Capobianco, Lewbart, Wiederhold, Cañete-Gibas and Negrão Watanabe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tatiane Terumi Negrão Watanabe, dGF0aWFuZS53YXRhbmFiZUBhbnRlY2htYWlsLmNvbQ==
†ORCID: Daniel Felipe Barrantes Murillo orcid.org/0000-0002-0744-3774
Gregory A. Lewbart orcid.org/0000-0003-0716-1387
Nathan P. Wiederhold orcid.org/0000-0002-2225-5122
Tatiane Terumi Negrão Watanabe orcid.org/0000-0002-9922-0235