 Taleb Al Khamis
Taleb Al Khamis Turke Shawaf
Turke Shawaf Adel Almubarak
Adel Almubarak Mohammed Ali Al-Ali
Mohammed Ali Al-Ali- Department of Clinical Sciences, College of Veterinary Medicine, King Faisal University, Al-Ahsa, Saudi Arabia
Background: Personalized healthcare technology has grown explosively through the use of portable and smart monitoring devices for diagnosis. The objective of this study was to determine the practicality and usability of the EquimetreTM fitness tracker on camels in comparison to the standard base-apex system in normal and clinical cases.
Methods: Five apparently healthy adult camels, five clinical adult cases and two clinical calves were enrolled in this study. The camels were equipped with two monitoring systems: EquimetreTM and a standard base-apex electrocardiogarphy. Each tracing was evaluated for the normal ECG variable's measure, including heart rate beats per min, P-R, QRS, R-R, Q-T, S-T intervals, and P-R and S-T segments in seconds. The amplitudes for P, Q, R, S, and T-peaks were evaluated in millivolts.
Results: EquimetreTM showed stability on ECG tracing with less movement artifacts compared with the standard base-apex system. Different polarities were observed for the P-waves and T-waves between the standard base-apex system and EquimetreTM. Both devices showed perfect agreement for heart rate (ICC = 1.00, P ≥ 0.0001, 95% = 1.00–1.00) in healthy and clinical adults. A good correlation was observed for the R-R interval between the devices in healthy and clinical adults. A moderate correlation was observed between the devices for Q-peak in clinical adults, with no correlation in clinical calves.
Conclusions: This study demonstrated acceptable ECG measurements between the standard base-apex and EquimetreTM device. This suggests that EquimetreTM could be a useful device in camels for initial electrocardiographic examinations in remote areas such as deserts.
1. Introduction
Waller (1) was the first to find electrocardiograms from humans, horses, dogs, cats, and rabbits using the capillary electrometer. Since then, aside from the huge literatures on animal experimentation, modest literature has accumulated on useful electrocardiography (2). Currently, personalized healthcare technology has grown explosively using portable and smart monitoring devices for diagnosis (3–5). Telemedicine techniques and tools provide professionals with rapid access to health monitoring and care implementation (6–8). Wearable medical devices play an essential role in continuous real-time medical data generation, helping in track metabolic status, diagnosis, and treatment (9). Teleconsultation using mobile health and wearable devices for monitoring animal health in veterinary medicine has become more effective, especially in areas with limited care access or lack of resources (10).
The applications of wearable devices are wide, ranging from biomedical to healthcare monitoring systems (11). Moreover, wearable sensor-based monitors enable the understanding of animals' activities to assess their safety and welfare, in addition to emotional behavior (12). New wearable medical devices in the field of cardiology have been increasingly used to measure heart activity, rate, and rhythm (13). The trend in the development of electrocardiogram (ECG) wireless body multi-functional sensors has shown accurate and reliable solutions for heart rhythm on long-term monitoring (14). The presence of several commercially available wearable and portable ECGs devices in human and veterinary fields has been demonstrated in recent studies on humans (15, 16), dogs (17), ruminants (18), and horses (19, 20).
Interest in camel's (Camelus Dromedarius) has increased dramatically over the past decades as a result of the innovation of many sports activities related to this animal. Thus, there has been an increasing need to provide the best medical care for this species (21).
The method for assessing camels heart rhythm through ECG has traditionally used the base-apex system (22, 23). Based on our knowledge obtaining a good quality ECG using an inexpensive, user-friendly, and digitalized device for data acquisition and evaluation has not been validated in camels. Therefore, in this study, we used the equine fitness tracker EquimetreTM (Arinoneo, Paris, France), which has been validated in horses (24). This fitness tracker designed for a daily exercise monitoring by owners, riders and trainers providing a comprehensive data acquisition of speed, distance, stride frequency, and stride length, in addition to its capability of recording heart rate and ECG. The objective of this study was to determine the practicality and usability of the fitness tracker EquimetreTM on camels and to compare it with the standard base-apex system in healthy and clinical cases.
2. Materials and methods
2.1. Animals
A total of five apparently healthy adult camels (Camelus dromedaries) owned by King Faisal University, Camel Research Center, five clinical adult cases [two male patients complaining of paraphimosis, one male patient with inflamed dulla (soft palate), one male patient with an open mandibular wound, and one female patient with an ear infection], and two clinical calves with cloudy eyes admitted to King Faisal Veterinary Teaching Hospital were enrolled in this study. The body score condition (BSC) of the camels was determined based on a previous report and rated from 1 (very thin) to 5 (fat) (25). Apparently healthy camels were determined based on a full clinical examination and history. Furthermore, all healthy camels were maintained in single-stall barns with free access to feed and water according to the standard care of King Faisal University Research and Training Station, Al Hasa.
2.2. Equipment
The camels were equipped with two monitoring systems: an EquimetreTM (EquimetreTM, Arinoneo Paris, France) consisting of a two-electrode sensor on an elastic girth and a standard base-apex ECG (BM7 VET; Bionet, Republic of Korea) with surface electrodes attached to the skin using alligator clips. All camels were restrained in the sternal position unsedated. The electrodes were placed after shaving the electrode area (Figure 1A) using a Panasonic hair trimmer machine (Panasonic, hair trimmer ER2051, China) in three apparently healthy and two clinical adult camels. However, no shavings were made for two apparently healthy camels, three clinical adult camels, and two clinical calves. The first electrode of the EquimetreTM girth was positioned on the left side of the chest, just behind the elbow joint, caudal to the olecranon at the cardiac apex. The second electrode was positioned two-thirds of the way down the thoracic girth (about 20 cm ventral to thoracic vertebrae). Modification on the girth was only made to fit the camel morphemically to secure the girth for better ECG reading (Figure 1B, C).
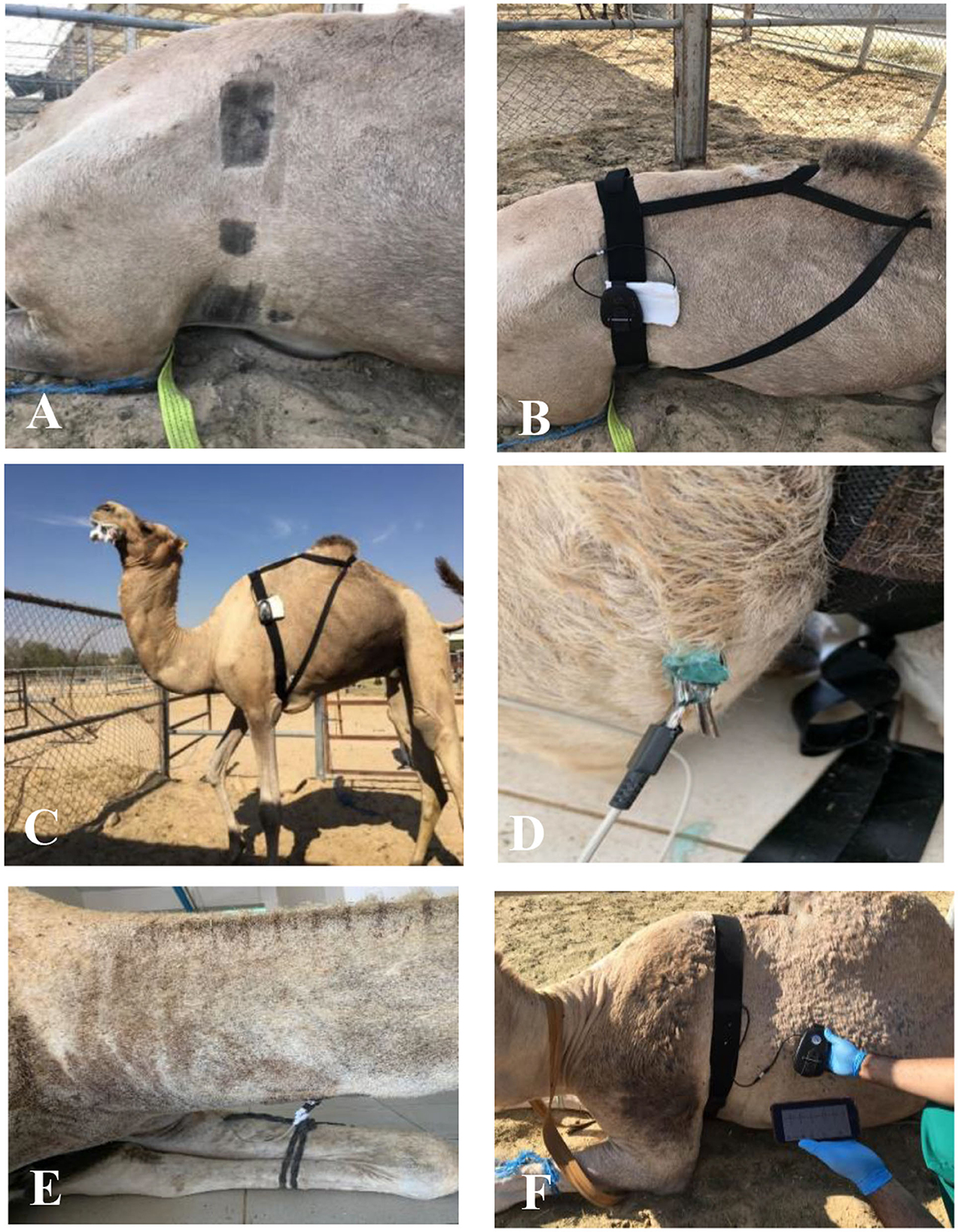
Figure 1. Positioning electrodes of both devices on camels (A) Shaving area of electrodes (B) Fixing Equimetre Vet (C) Girth after modification (D) Negative standard base-apex electrode (E) Positive standard base-apex electrode (F) Display of live ECG from EquimetreTM.
The left arm electrode (positive) of the standard base-apex was placed above the olecranon, just near the first electrode of the EquimetreTM device (Figure 1D), and the right arm electrode (negative) was placed two-thirds of the way down the right jugular groove (Figure 1E). The third electrode was placed cranial and parallel to the second thoracic girth electrode of the Equimetre TM on the left chest. The electrodes were moistened with tap water to maintain electrical conduction and obtain a high-quality ECG signal from both devices. Gel was used for the standard base-apex system.
2.3. Data collection
The measurements were recorded by the same operator. The EquimetreTM device was linked through Bluetooth to the EquimetreTM ECG application downloaded from the App store on an iPhone 7 (Apple, USA). The ECG was digitally displayed at a paper speed of 25 mm/s on a smartphone (Figure 1F), and ECG tracing was automatically digitalized by the device. For the standard base-apex method, the ECG tracing was viewed and printed at a paper speed of 25 mm/s with a gain of 40 mm/mV using lead III. Once a satisfactory ECG from each device was determined, a 30 s reading was obtained. One to three readings from each camel were obtained depending on the stress level of the camel. The tracing time setup was simultaneously recorded for both devices at the same time. Moreover, both methods were assessed in terms of time to fix and ECG quality.
2.4. Data acquisition
Raw data of ECG were downloaded from EquimetreTM unit in laptop through a specific program supported by the manufacturer (EquimetreUSB_2.0.1 for windows: Arioneo, France) and the data were exported in excel format. Raw ECG data was imported by Kubios software (Kubios Version3.2 for windows: Kubios Oy, Finland) for ECG complexes view and subtraction the none records ECG time before and after ECG reading. All tracings were reviewed for baseline artifacts of P wave, QRS complex and T wave segments were could not be identified. Tracings ECGs were considered acceptable for interpretation if the baseline artifacts were absent for at least 80% (26).
2.5. Data analysis
A 15 s reading from the reviewed ECG tracing was selected for the analysis. Each tracing was anonymized and randomized to evaluate the normal ECG variables, including heart rate (HR) in beats per min, by multiplying the number of PQRST complexes from the 15 s trace by 4; P–R interval (s); QRS duration (s); R-R interval (s); Q–T interval (s); S–T interval; P–R segment, and S–T segment (s). Additionally, the amplitudes for the P-peak, Q-peak, R-peak, S-peak, and T-peak (millivolts) and presence of an abnormal complex were recorded. The first and last three complexes from the 15-s ECG tracing were measured for each single measurement, and the average of the measurements over the three complexes was used for analysis. Three trained examiners blinded to the ECG trace identity performed the reading of the trace. The source of the trace was not blinded because of the difference in the trace displayed by each piece of the equipment (Figure 2). All measurements were performed manually (by hand) for both the EquimetreTM and standard ECG without the assistance of ECG interpretation software (19, 24, 26, 27). The data were categorized into three groups: apparently healthy adults, clinical adult cases, and clinical calves (Table 1).
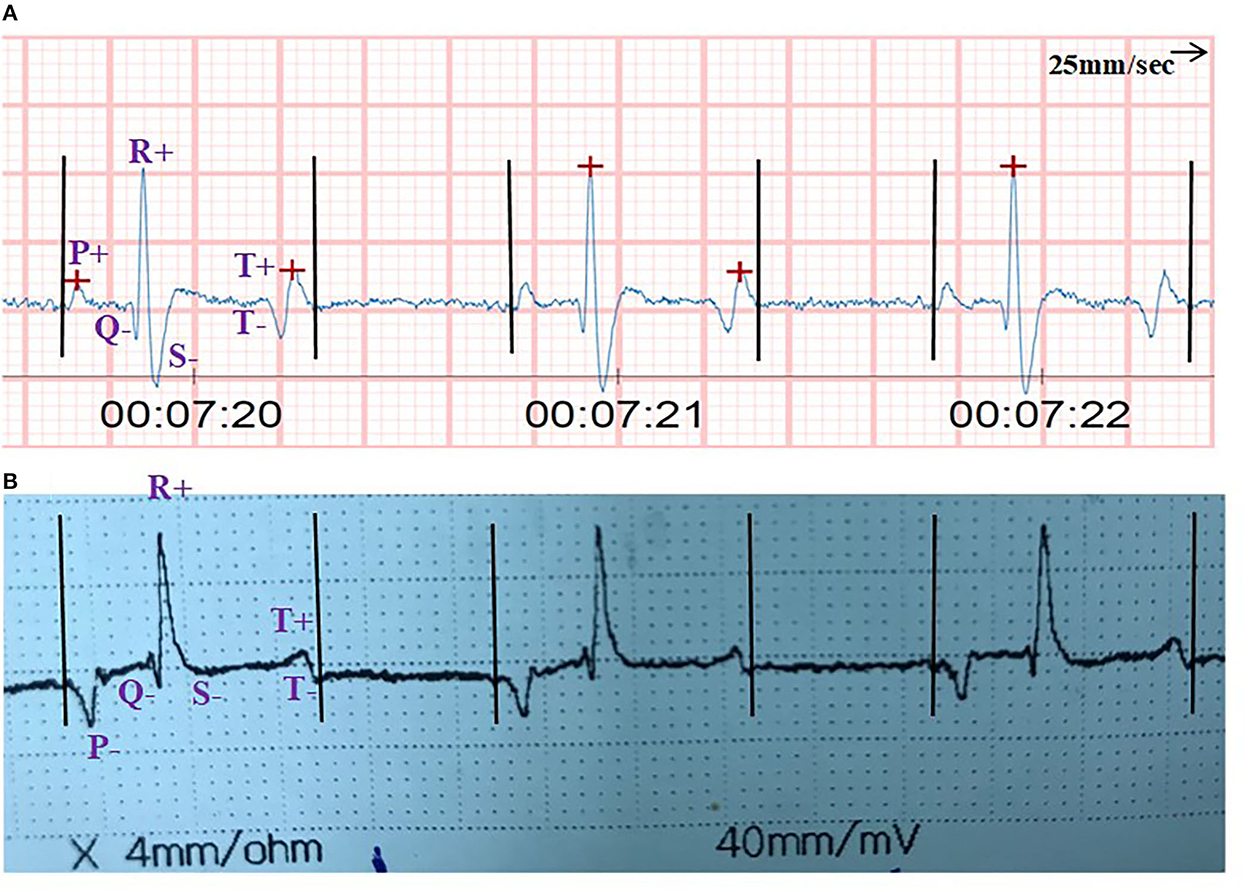
Figure 2. Show ECG tracing from (A) EquimetreTM (B) Gold standard base-apex for clinical female calf. Camel suffering cloudy eyes referred to King Faisal veterinary teaching hospital. Variation between EquimetreTM and Base-apex system in the complex morphology was noticed, P-Wave showed different polarity (+) in EquimetreTM and (-) in base-apex. Moreover, absence of S-Peak in base-apex system compared to EquimetreTM where S-Peak is present and clear. Additionally, Q-Wave, R-Wave, and T-Wave determined in both devices with respect to the difference between the device in terms of duration and amplitude.

Table 1. Details of participated camels.
2.6. Statistics analysis
All camel categories were described according to age, sex, BSC, and health status. Each measurement using either device (EquimetreTM vs. standard ECG) was first averaged over the three examiners and summarized for each category of camels using the median and range. The correlation between devices was determined using intracluster correlation (ICC) statistics. The agreement between examiners for either device was also assessed using ICC statistics. ICC values were interpreted as having a weak correlation, fair, moderate, good, very good, and perfect agreement for values ≤0.20, 0.21–0.40, 0.41–0.60, 0.61–0.80, 0.81–0.99, and 1, respectively, as described previously (18). All analyses were performed using R software version 3.6.1. Statistical significance was set at a two-sided p-value < 0.05.
3. Results
ECG traces were obtained from all 12 camels using an EquimetreTM and the standard base-apex system.
3.1. Feasibility of ECGs devices
The fixing time of electrodes for the EquimetreTM on camels was estimated to be between 2–3 min, whereas that of the standard base-apex system was 5–6 mindue to the thickness of the camel skin and the grip of the small tip alligator electrodes. Moreover, the standard base-apex system displays the ECG trace immediately after fixing the electrodes, whereas a connection to the mobile app is needed to view the ECG trace of the EquimetreTM. EquimetreTM showed stability on ECG tracings with fewer movement artifacts compared with the standard base-apex system. However, the baseline ECG trace from the EquimetreTM showed irregularity compared with the standard base-apex system. A difference in polarity in the ECG complexes was noticed between the devices in P and T waves. The standard base-apex system showed a negative P-wave, whereas the EquimetreTM P-wave was positive. A biphasic T-wave in EquimetreTM showed a negative wave followed by a positive wave, whereas the standard base-apex system started with a positive T-wave followed by a negative T-wave. Furthermore, S-waves were not present in the standard base-apex system in all ECG traces, whereas in EquimetreTM, S-waves were present and clear in all ECG traces from all camels.
3.2. Heart rhythm
Two camels from the clinical adult category complaining of paraphimosis were detected to have a junctional premature beat (JPB) on continuous ECG tracing using Equimetre TM,; the junctional premature beats seen ranged from 30 to 36 bpm in a total of 15–17 JPB per ECG record. Changes in T-wave polarity were observed in one case of paraphimotic male camel associated with JPB, as shown in Figure 3. The ECG trace showed a normal heartbeat associated with biphasic T-waves, whereas premature junctional beat complexes were associated with negative T-waves. Sinus tachycardia was identified in the normal adult category, with heart rates ranging from 60 to 96 bpm.
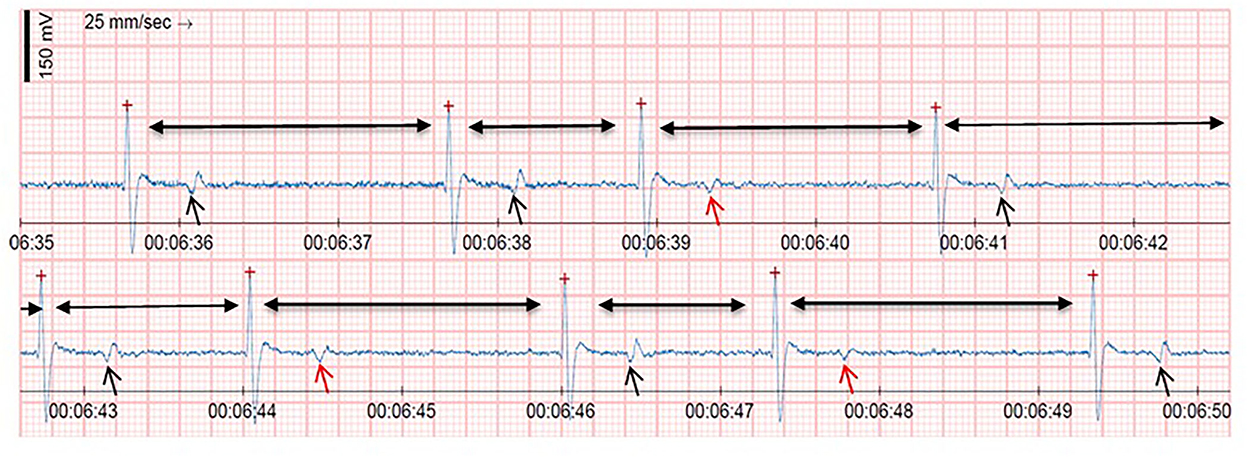
Figure 3. Shows continuous ECG trace from EquimetreTM for clinical male camel suffering paraphimosis referred to King Faisal Veterinary Teaching Hospital. ECG trace revealed heart rate of 36 bpm associated with three junctional premature beats (JPB). Moreover, ECG trace showed a different T-waves polarity in which black arrows showed a normal complex followed by biphasic T-Waves and red arrow showed JPB followed by T(−) waves.
3.3. Heart rate
The heart rate median and range of each camel category are listed in Table 2 for both devices. The HR agreement over the examiners for the average correlation between standard base-apex and EquimetreTM is shown in Table 3. HR correlation was very good for the apparently healthy camel category, (ICC = 0.90, P ≤ 0.0001, 95% = 0.73–0.97), good for clinical adults (ICC = 0.71, P = 0.0269, 95% = −0.02 0.95), and moderate for clinical calves (ICC = 0.46, P = 0.1265, 95% = −0.37 0.9). The intraclass correlation coefficients between examiners of HR and each device for each category are shown in Table 4. A perfect correlation was observed between examiners of HR in apparently healthy and clinical adult categories for both devices. However, a weak correlation between examiners was observed in the clinical calves category for both devices for HR.
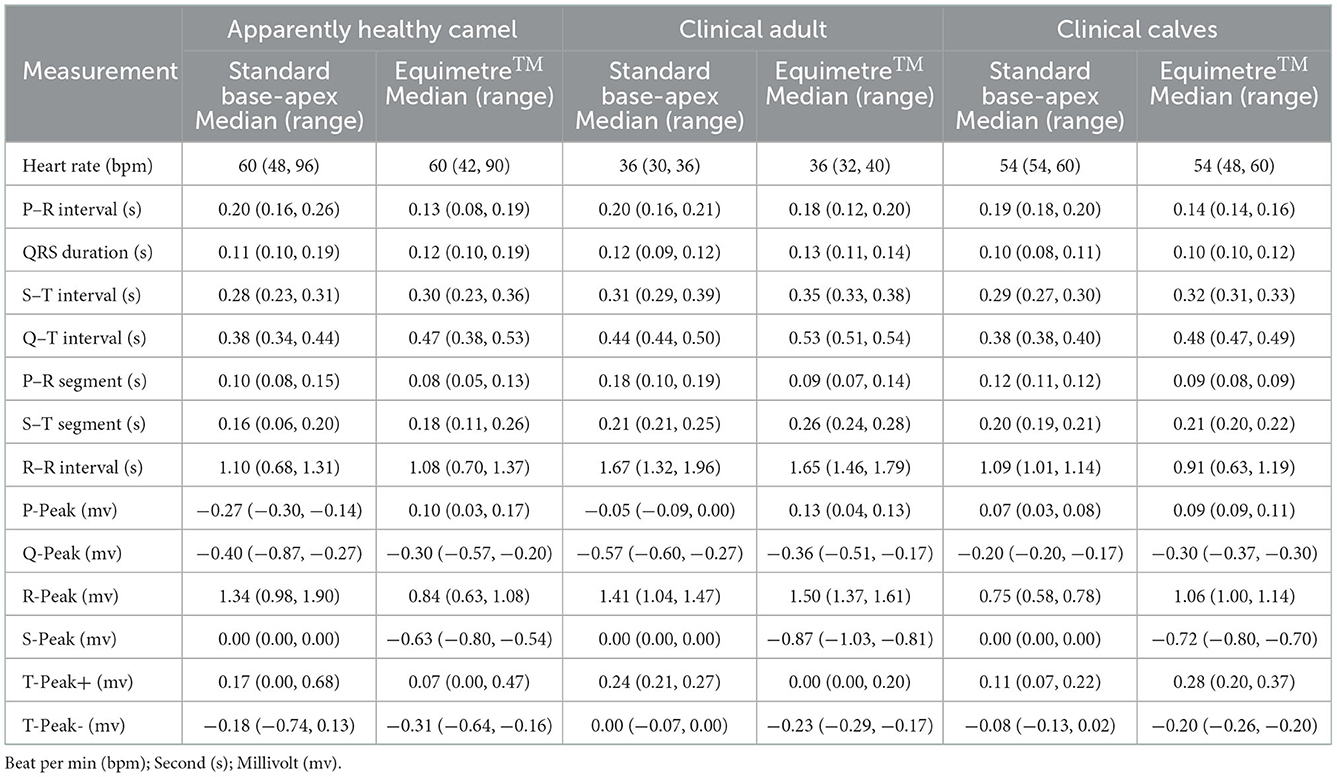
Table 2. Summary of ECG measurements for healthy adult, clinical adult, and clinical calves camel.
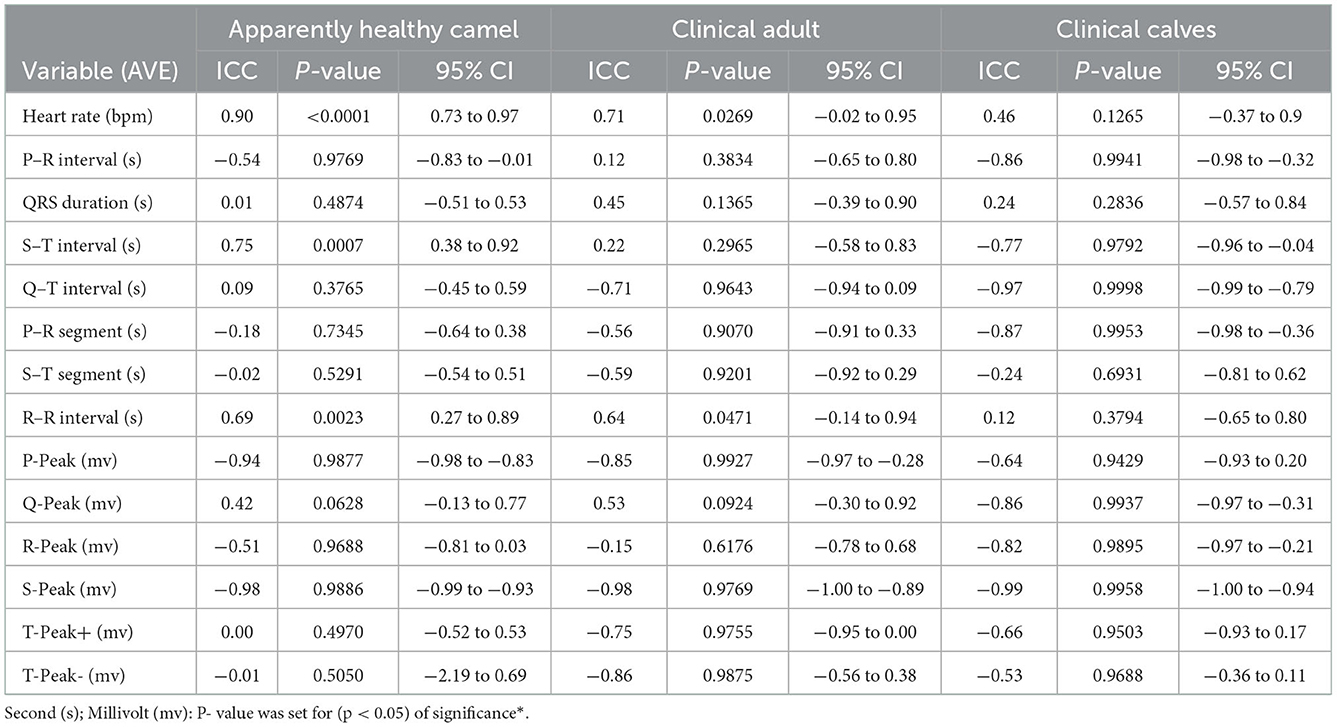
Table 3. Agreement between two methods of ECG trace for intraclass correlation coefficient (ICC) and average (AVE) over three examiners for each category.
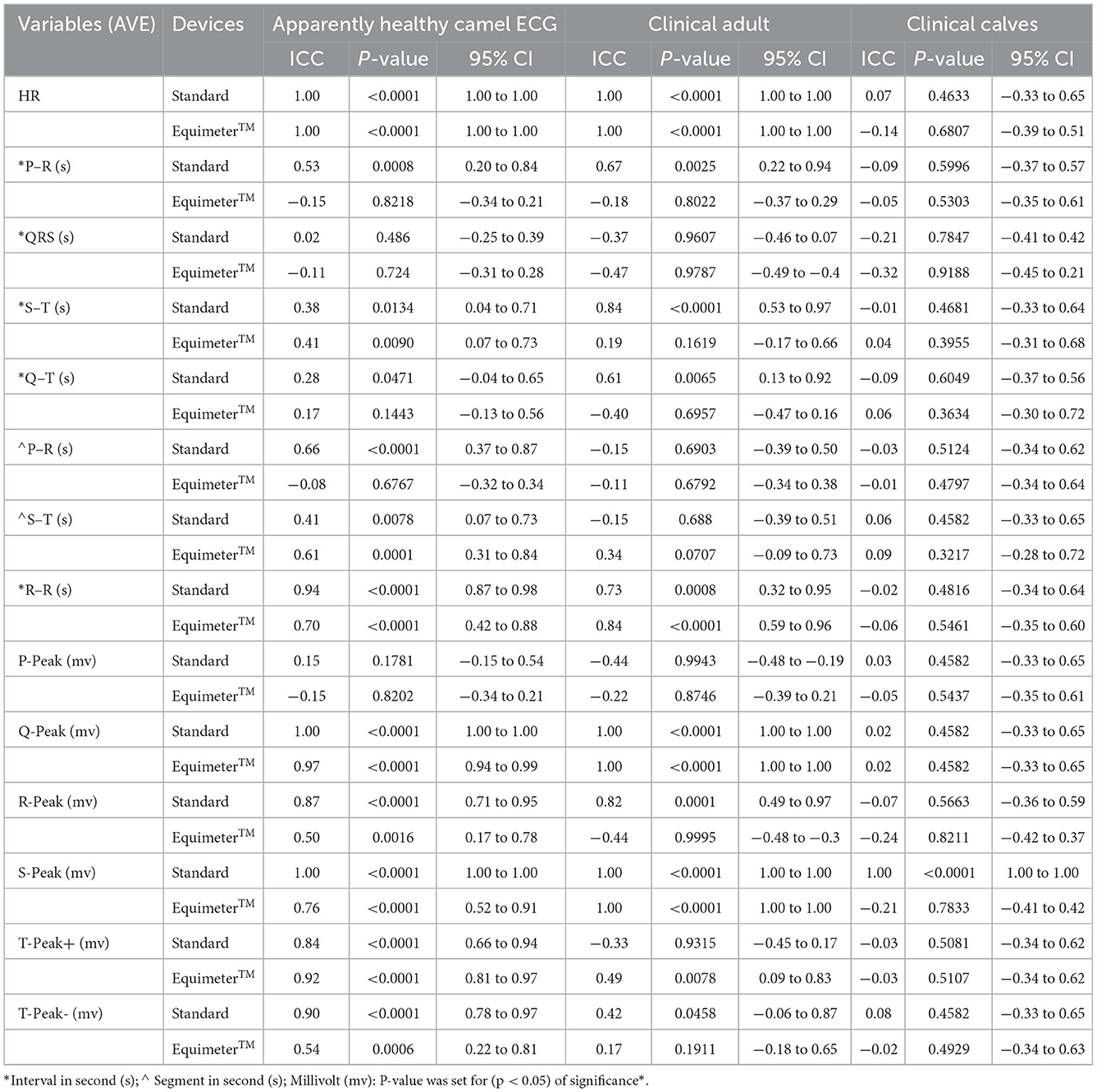
Table 4. Intraclass correlation coefficient (ICC) between examiners and each device for each category.
3.4. P–R, QRS, S-T, Q-T, and R-R intervals
The P-R, QRS, S-T, Q-T, and R-R interval medians and ranges for each camel category are shown in Table 2 for both devices. Agreement between examiners for the average correlation between standard base-apex and EquimetreTM for P–R, QRS, S–T, Q–T, and R-R intervals is shown in Table 3. A moderate correlation of the P-R interval average between devices was found for the apparently healthy category (ICC = −0.54, P = 0.9769, 95% = −0.83 to −0.01). A weak and very good correlations in P-R interval were observed in the clinical adult (ICC = 0.12, P = 0.3834 and 95% = −0.65 to 0.80) and clinical calves (ICC = −0.86, P = 0.9941, 95% = −0.98 to −0.32) categories, respectively.
Intraclass correlation for P–R, QRS, S–T, Q–T, and R-R intervals between examiners and each device for each category are shown in Table 4. The standard base-apex showed variation of correlation between examiners for P-R interval measurements were in apparently healthy was good correlation, very good in clinical adult, and week correlation in clinical calves categories. EquimetreTM showed a weak correlation in the P-R interval between examiners in all camel categories.
Correlations of the QRS interval average between devices was noted to be weak in apparently healthy camels (ICC = 0.01, P = 0.4874, 95% = −0.51 to 0.53), moderate in clinical adults (ICC= 0.45, P = 0.1365, 95% = −0.39 to 0.90), and fair in clinical calves (ICC = 0.24, P = 0.2836, 95% = −0.57 to 0.84). The correlation of the QRS interval between examiners was weak for both devices in apparently healthy camels. Moreover, a fair correlation was observed in clinical calf cases for both devices, and for the standard base-apex system in clinical adult cases. However, the EquimetreTM system showed a moderate correlation between examiners for the QRS interval in the clinical adult category.
A good correlation of the S-T interval between devices was observed in apparently healthy camels (ICC = 0.75, P = 0.0007, 95% = 0.38 to 0.92) and clinical calves (ICC = −0.77, P = 0.9792, 95% = −0.96 to −0.04). However, a fair S–T interval correlation was observed in clinical adults (ICC = 0.22, P = 0.2965, 95% = −0.58 to 0.83). A very good correlation between examiners for standard base-apex system in S-T interval measurement was observed in clinical adult cases. However, fair and moderate correlations between examiners were observed in the S-T interval in apparently healthy camels for the standard base apex and EquimetreTM, respectively. Moreover, a weak correlation between examiners was observed for the S-T interval in clinical calf cases for both devices and in the EquimetreTM system in clinical adult cases.
A weak Q-T interval average correlation between devices was observed in apparently healthy camels (ICC = 0.09, P = 0.3765, 95% = −0.45 to 0.59), good in clinical adults (ICC = −0.71, P = 0.9643, 95% = −0.94 to 0.09), and very good in clinical calves (ICC= −0.97, P = 0.9998, 95% = −0.99 to −0.79). The intraclass correlation coefficient between examiners for the Q-T interval measurements was fair for both devices in clinical calf cases. Moreover, a fair correlation was noted in EquimetreTM for clinical adults and the standard base-apex in apparently healthy categories. Moreover, a good correlation was observed between the examiners for the Q-T interval from the standard base-apex system in the clinical adult category.
A good correlation was observed for the R-R interval between devices in apparently healthy (ICC = 0.69, P = 0.0023 and 95% = 0.27–0.89) and clinical adults (ICC = 0.64, P = 0.0471, 95% = −0.14 to 0.94). However, a weak correlation was observed in the clinical calves category (ICC = 0.12, P = 0.3794, 95% = −0.65 to 0.80). The intraclass correlation coefficient between examiners for the R-R interval measurement was very good for the standard system in the apparently healthy category and the EquimetreTM system in the clinical adult category. A good R-R interval correlation between examiners was observed in the standard system for clinical adults and EquimetreTM in apparently healthy categories. Moreover, a weak correlation was observed between the examiners for the R-R interval for both devices in the clinical calf category.
3.5. P–R and S–T segments
The P-segment median and S-range of each camel category are shown in Table 2 for both devices. Agreement between examiners for the average correlation between the standard base-apex and EquimetreTM for the P–R and S–T segments is shown in Table 3. Week correlation in the average of P–R segment (ICC = −0.18, P = 0.7345, 95% = −0.64 to 0.38) and S–T segment (ICC= −0.02, P = 0.5291, 95% = −0.54 to 0.51) for both devices in apparently healthy category. Moreover, a moderate average correlation was observed between the devices for the P-R and S-T segments in the clinical adult category (ICC = −0.56, P = 0.9070, 95% = −0.91 to 0.33/ICC= −0.59, P = 0.9201, 95% = −0.92 to 0.29, respectively). The average correlation of the P–R and S–T segments between devices in clinical calves was very good for the P-R segment (ICC = −0.87, P = 0.9953, 95% = −0.98 to −0.36) and fair for the S–T segment (ICC = −0.24, P = 0.6931, 95% = −0.81 to 0.62).
The correlations for the P–R and S–T segments between examiners and each device for each category are shown in Table 4. The ICC between examiners for the P–R segment measurement was weak for both devices in the clinical adult and clinical calf categories. Moreover, the correlation between examiners in the apparently healthy category for the P–R segment was strong in the standard system and weak in the EquimetreTM system. A good correlation between the examiners for the S–T segment in EquimetreTM and a moderate correlation in the standard system for the apparently healthy category was noted. However, the correlation for the S–T segment between examiners in the clinical calves category was weak for both devices. The standard base-apex system in the clinical adult category showed a weak correlation for the S–T segment, whereas a fair correlation was observed for EquimetreTM.
3.6. P, Q, R, S, and T Peaks
Peaks medians and ranges for P, Q, R, S, and T for each camel category are shown in Table 2 for both devices. Agreement between examiners for the average correlation between the standard base-apex and EquimetreTM for P, Q, R, S, and T peaks is shown in Table 3. The average correlation between devices was very good for the P-peak in the apparently healthy category (ICC = −0.94, P = 0.9877, 95% = −0.98 to −0.83) and the clinical adult category (ICC = −0.85, P = 0.9927, 95% = −0.97 to 0.28). However, the clinical calf category showed a good correlation between devices for the P-peak (ICC = −0.64, P = 0.9429, 95% = −0.93 to 0.20). The ICC between examiners for the P-peak measurement was weak for both devices in the apparently healthy and clinical calf categories. Nevertheless, a moderate correlation between examiners in the clinical adult category for the P-peak was observed in the standard system, whereas the EquimetreTM system showed a fair correlation (Table 4).
A moderate correlation was observed between devices for the Q-peak in apparently healthy cases (ICC = 0.42, P = 0.0628, 95% = −0.13 to 0.77) and clinical adults (ICC = 0.53, P = 0.0924, 95% = −0.30 to 0.92). However, a very good correlation was noted in clinical calves (ICC = −0.86, P = 0.9937, 95% = −0.97 to −0.31) in the Q-peak between devices. The ICC between examiners for the Q-peak was perfect for both devices in the clinical adult category and in the apparently healthy category for the standard system. Moreover, EquimetreTM showed a very good correlation between examiners in the apparently healthy category for the Q-peak. Nevertheless, a weak Q-peak correlation between examiners was observed for both devices in the calves (Table 4).
A moderate, weak, and very good correlation of the R-peak average between devices was noted in apparently healthy camels (ICC = −0.51, P = 0.9688, 95% = −0.81 to 0.03), clinical adult (ICC = −0.15, P = 0.6176, 95% = −0.78 to 0.68), and clinical calves (ICC= −0.82, P = 0.9895, 95% = −0.97 to −0.21). The correlation between examiners for the R-peak was very good for the standard system in apparently healthy and clinical adults. However, in EquimetreTM a moderate correlation between examiners in the apparently healthy and clinical adult categories for R-peak was observed. Nevertheless, a weak R-peak correlation between examiners was observed for both devices in calves (Table 4).
A very good correlation was noted between devices for the S-peak in apparently healthy (ICC = −0.98, P = 0.988, 95% = −0.99 to −0.93), clinical adult (ICC = −0.98, P = 0.9769, 95% = −1.00 to −0.89), and clinical calves (ICC = −0.99, P = 0.9958, 95% = −1.00 to −0.49). The correlation between examiners for the S-peak was perfect for the standard system for all camel categories. However, in EquimetreTM a perfect correlation was observed between examiners in the clinical adult category for the S-peak. Nevertheless, a good S-peak correlation between examiners was observed in apparently healthy adults, and a fair correlation was observed in clinical calves (Table 4).
A good correlation was observed between devices for the T+-peak in clinical adults (ICC = −0.75, P = 0.9755, 95% = −0.95 to 0.00) and clinical calves (ICC = −0.66, P = 0.9503, 95% = −0.93 to 0.17). However, there was a weak correlation between devices in the apparently healthy category (ICC = 0.00, P = 0.4970, 95% = −0.52 to 0.53). The correlation between examiners for the T+-peak was very good for both devices in healthy individuals. However, a weak correlation between examiners in the clinical calves category for the T+-peak was observed. Nevertheless, a moderate T+-peak correlation between examiners was observed in the EquimetreTM system, whereas the standard system was fair in clinical adult cases (Table 4).
The correlation between devices for T− -peak was weak in apparently healthy adults (ICC = −0.01, P = 0.5050, 95% = −2.19 to 0.69), very good in clinical adults (ICC = −0.68, P = 0.9875, 95% = −0.56 to 0.38), and moderate in clinical calves (ICC = −0.53, P = 0.9688, 95% = −0.36 to 0.11). The correlation between examiners for the T−-peak was very good in apparently healthy subjects for the standard system. Moreover, a moderate correlation between examiners was observed for EquimetreTM in the apparently healthy category for T−-peak and the standard system in the clinical adult category. Nevertheless, a weak T−-peak correlation between examiners was observed in clinical calf cases only for both devices (Table 4).
4. Discussion
There is increasing interest in the veterinary field to use mobile health and wearable devices to monitor vital signs (heart rate, heart rate variability, and respiratory rate) in field and farm conditions, with the capability of identifying physiological and pathological correlations with stress, distress, and other emotional states (10, 12). Visualizing the underlying electrical activity of the camel's heart using ECG is critical for determining the type of arrhythmia present (28, 29).
Our study findings proposed that: (1) applying the EquimetreTM fitness health tracker was feasible in camels and provided an acceptable method for ECG recording; (2) adequate ECG tracings for interpretation could be obtained from EquimetreTM; (3) there was a moderate to very good correlation between the EquimetreTM and standard system for the HR; and (4) acceptable measurements of waves, intervals, segments, and peaks could be obtained from EquimetreTM. This suggests the practical usefulness of EquimetreTM for camels.
The stability and minimum movement artifacts in EquimetreTM compared to the standard base-apex complex in the present study were in agreement with (27), who suggested that wearable devices reduce the equipment needed on and around the horse compared to standard ECG, and is therefore potentially less stressful. However, fixing the electrodes on the camel was difficult using the standard base-apex method, as expected from high skin tension while the camel was in a sitting position vs. the small tips of alligator electrodes, which might cause loss of grip and interrupt the ECG recording. Nevertheless, this problem was not observed in the EquimetreTM as a result of the tight electrode fixed to the animal body by the girth. Interestingly, the detection of junctional premature beats in two clinical adult camels in the present study from continuous EquimetreTM ECG recordings that were not present on standard base-apex ECG traces or could be missed on a monitor was in agreement with a previous study on horses using EquimetreTM for detecting arrhythmia in continuous ECG recordings during exercise (24). To the best of our knowledge, there have been no reports in the literature regarding junctional premature beats in camels.
Considering that the heart rate of the mature camel ranges from 28 to 50 beats per min (29, 30), the correlation between EquimetreTM and the standard base-apex system of heart rate was good to very good in adult camels for both devices, and the agreement was perfect depending on the examiners. This demonstrated the usability of EquimetreTM as a wearable ECG device for measuring HR in adult camels, similar to horses (19). A few adult camels showing an increase in HR were all from apparently healthy categories in the present study, which may be explained by the stress at the time of ECG recording. The incompatibility between the two devices in calves for the measurement of HR may be explained by the difficulty of fixing the electrode and girth around the chest in these animals and, consequently, the difficulty of obtaining compatibility in the work of the heart during recording.
The variability in the ECG measurements between devices and examiners of intervals, segments, and peaks could be due to the differences in electrode number, type, and placement in the animals. The weak to moderate correlation in the P-R interval and P-R segment measurements between the two devices in the adult camels in this study might be due to the difficulty in identifying P waves by examiners for EquimetreTM in most ECG traces, because the agreement between examiners for the P-R interval was weak, unlike the standard base-apex system. Although EquimetreTM had a weak correlation with the P-R interval in adult camels, the agreement between the standard base-apex and EquimetreTM was very good for calves in the presence of clear P waves on ECG traces. Indeed, the small circumference of the chest in calves and the large electrode size of EquimetreTM might enable heart signals to be recorded by the electrodes more efficiently, and the P wave is clearly identified. Conversely, several studies on smartphone ECG devices in horses and cows have found no agreement on P-wave polarity between the standard base-apex and smartphone ECGs, presumably because of the small dipolar electrodes of the smartphone ECG and the placement of the device on the chest (18, 26, 27).
In essence, the fair to weak correlation for QRS, S-T, and Q-T intervals in most camel categories in the present study could be explained by the difference in the determination of QRS, S-T, and Q-T intervals between examiners for both devices. However, moderate to very good correlations of QRS, S-T, and Q-T intervals between examiners suggested that EquimetreTM may still be acceptable for measuring ECG complex variables in camels, which are difficult to compare due to the lack of available data in camel ECG measurements, to the best of our knowledge. In addition, measurements from ECG EquimetreTM tracings should be carefully evaluated, and future studies should be performed to validate the ECG reliability. This is in agreement with a previous report (19). The similar QRS interval readings in the calf camel category for the standard base-apex and EquimetreTM devices in the present study were in agreement with previous reports (31). Ironically, a good correlation in the R-R interval between devices and examiners in adult camels in the present study was found to be reliable, suggesting that EquimetreTM can be useful for the measurement of the R-R interval as the difference in most cases was minimal. Similarly, a previous study reported the utility of a smartphone ECG for R-R interval measurement in healthy horses (19). The differences in the R-R interval in calf camels between the two devices could be explained by the inappropriate girth size in EquimetreTM for these animals.
A weak to moderate correlation between devices for the S-T segment in the current study may be explained by the lack of the S-wave in standard base-apex monitoring compared to EquimetreTM. This is in contrast with a previous case report by (31) on camel calves with atrioventricular block where the S-wave was present in the standard base-apex. This suggests that EquimetreTM may be useful for measuring this complex region. The difficulty of determining the P-peak, including abnormal P waves for EquimetreTM in adult camels in the present study and its variation among camel categories, led to a lack of correlation between the examiner and devices; as described above, examiners were unable to distinguish the P-wave. Furthermore, there was a weak correlation of the R-peak in the present study among camel categories and between the two recording methods. This is not unexpected because the difference in fixation of the electrodes in both devices and possibly insufficient wetting of EquimetreTM electrodes (as water acts as a conductor for heart electrical impulse), may have a role in the intensity of the ECG recording.
There was no correlation between T+-peak and T−-peaks in the present study between the two recording methods in all camel categories. Nevertheless, the correlation between examiners ranged from very good to weak in most camel categories. The compatibility between the examiners in determining the negative and positive T-peaks can be explained by its good clarity in the camel ECG by both devices, while the reason for the lower correlation between the two devices in determining the T-peak may be explained by the difference in polarity displayed by the ECG on these devices. Based on comments from our examiners, the main challenge with the P-wave, T-wave, P-R, Q-T, and S-T interval measurements was identifying where the P-wave and T-wave started and ended due to undulation in the baseline of standard base-apex and EquimetreTM devices in dromedary camels. Moreover, S-T was determined in the standard base-apex owing to the lack of S-waves. These findings are similar to what has been previously described in studies comparing standard base-apex and other wearable devices (27, 32), in which they noticed some degree of variability in the identification of waveform and polarity between observers and devices. Additional studies using larger numbers of healthy and diseased camels should be conducted to confirm and interpret these observations.
One of the main limitations of this study is the small number of camels included and the difference in breeds, age, sex, and body weight of the camels. Additionally, the healthy camel group may have been under the influence of stress during the recording due to the unfamiliarity of procedures and operators. Unlike for clinical cases, these healthy animals not used to be handled by different animal caretakers.
In conclusion, this study demonstrated acceptable ECG measurements between standard base-apex and EquimetreTM devices. This suggests that EquimetreTM could be a useful device in camels for initial electrocardiograph examination because it is portable and requires no training, especially in remote areas such as deserts. However, EquimetreTM is not a substitute for a standard base apex. Further studies are required to verify the ability of the EquimetreTM to detect arrhythmias and heart performance in a large population of camels. Additionally, future studies are needed to determine the capabilities of EquimetreTM to assess camel heart performance in motion and race as well as other parameters.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The electrocardiogram was done without giving any treatments or causing harm to the animal, and the camels used in the present study were among the camels that visit the Veterinary Teaching Hospital, where they are routinely examined with the approval of the animal breeder.
Author contributions
TS and TA: contributed equally to study design, execution, data analysis, and manuscript construction. AA and MA-A: contributed to data analysis and critically revised manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported through the Annual Funding Track by the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia (Project No. GRANT2.452).
Acknowledgments
We want to thank Camel Research Center at King Faisal University, Saudi Arabia for arranging healthy camels, Guillaume Duboi (Arioneo Company, France) for the technical support, Serigne Lo (University of Sydney, Melanoma institute, Australia) for the statistics analysis, and Mohammed Karam and Ayman Nahass (Faculty of Surgery Department, College of Veterinary Medicine, King Faisal University, KSA) for arranging the clinical cases.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Waller AD. Introductory address on the electromotive properties of the human heart. Br Med J. (1888) 2:751–4. doi: 10.1136/bmj.2.1449.751
2. Detweiler DK. The mammalian electrocardiogram: comparative features. In: Macfarlane PW, van Oosterom A, Pahlm OKP, Janse MJC, editors. Comprehensive Electrocardiology. London: Springer (2010). p. 1909–47.
3. Tsikriteas ZM, Roscow JI, Bowen CR, Khanbareh H. Flexible ferroelectric wearable devices for medical applications. iScience. (2021) 24:101987. doi: 10.1016/j.isci.2020.101987
4. Sakphrom S, Limpiti T, Funsian K, Chandhaket S, Haiges R, Thinsurat K. Intelligent medical system with low-cost wearable monitoring devices to measure basic vital signals of admitted patients. Micromachines. (2021) 12:918. doi: 10.3390/mi12080918
5. Lu L, Zhang J, Xie Y, Gao F, Xu S, Wu X, et al. Wearable health devices in health care: narrative systematic review. JMIR Mhealth Uhealth. (2020) 8:e18907. doi: 10.2196/18907
6. Edge C, George J, Black G, Gallagher M, Ala A, Patel S, et al. Using telemedicine to improve access, cost and quality of secondary care for people in prison in England: a hybrid type 2 implementation effectiveness study. BMJ Open. (2020) 10:e035837. doi: 10.1136/bmjopen-2019-035837
7. Cain R, Shafer Klink D, Yunus S. Telemedicine implementation in family medicine: Undergraduate clerkship during COVID-19 pandemic. Med Educ. (2020) 54:1064–5. doi: 10.1111/medu.14313
8. Bagot KL, Moloczij N, Barclay-Moss K, Vu M, Bladin CF, Cadilhac DA. Sustainable implementation of innovative, technology-based health care practices: a qualitative case study from stroke telemedicine. J Telemed Telecare. (2020) 26:79–91. doi: 10.1177/1357633X18792380
9. Yetisen AK, Martinez-Hurtado JL, Unal B, Khademhosseini A, Butt H. Wearables in medicine. Adv Mater. (2018) 30:e1706910. doi: 10.1002/adma.201706910
10. Rowland J. The future of wearable healthcare in the veterinary profession. Vet Rec. (2015) 177:513–4. doi: 10.1136/vr.h6220
11. Guk K, Han G, Lim J, Jeong K, Kang T, Lim EK, et al. Evolution of wearable devices with real-time disease monitoring for personalized healthcare. Nanomaterials. (2019) 9:813. doi: 10.3390/nano9060813
12. Kido N, Tanaka S, Omiya T, Kamite Y, Sawada K, Komatsu Y, et al. Emotion estimation using a wearable heart rate monitoring device in Asian elephants (Elephas maximus) during veterinary clinical procedures. J Vet Med Sci. (2020) 82:856–60. doi: 10.1292/jvms.19-0637
13. Pevnick JM, Birkeland K, Zimmer R, Elad Y, Kedan I. Wearable technology for cardiology: an update and framework for the future. Trends Cardiovasc Med. (2018) 28:144–50. doi: 10.1016/j.tcm.2017.08.003
14. Rashkovska A, Depolli M, Tomasic I, Avbelj V, Trobec R. Medical-grade ECG sensor for long-term monitoring. Sensors. (2020) 20:1695. doi: 10.3390/s20061695
15. Wegner FK, Kochhauser S, Frommeyer G, Lange PS, Ellermann C, Leitz P, et al. Prospective blinded evaluation of smartphone-based ECG for differentiation of supraventricular tachycardia from inappropriate sinus tachycardia. Clin Res Cardiol. (2021) 110:905–12. doi: 10.1007/s00392-021-01856-5
16. Li M, Xiong W, Li Y. Wearable measurement of ECG signals based on smart clothing. Int J Telemed Appl. (2020) 2020:6329360. doi: 10.1155/2020/6329360
17. Gunasekaran T, Olivier B, Griffith L, Sanders R. Comparison of heart rate obtained from shorter duration Holter recordings to 24-hour mean heart rate in dogs with atrial fibrillation. PLoS ONE. (2020) 15:e0241620. doi: 10.1371/journal.pone.0241620
18. Bonelli F, Vezzosi T, Meylan M, Nocera I, Ferrulli V, Buralli C, et al. Comparison of smartphone-based and standard base-apex electrocardiography in healthy dairy cows. J Vet Intern Med. (2019) 33:981–6. doi: 10.1111/jvim.15396
19. Welch-Huston B, Durward-Akhurst S, Norton E, Ellingson L, Rendahl A, McCue M. Comparison between smartphone electrocardiography and standard three-lead base apex electrocardiography in healthy horses. Vet Rec. (2020) 187:e70. doi: 10.1136/vr.105759
20. Vitale V, Vezzosi T, Tognetti R, Fraschetti C, Sgorbini M. Evaluation of a new portable 1-lead digital cardiac monitor (eKuore) compared with standard base-apex electrocardiography in healthy horses. PLoS ONE. (2021) 16:e0255247. doi: 10.1371/journal.pone.0255247
21. Badawy AM, Marzok MA, Eshra EA. Computed tomographic arthrography of the normal dromedary camel carpus. Vet Comp Orthop Traumatol. (2016) 29:188–94. doi: 10.3415/VCOT-15-06-0112
22. Samimi AS. Electrocardiographic and clinico-paraclinical evaluation of a dromedary camel suffered from theileriosis. Comp Clin Path. (2018) 27:1409–15. doi: 10.1007/s00580-018-2768-4
23. Tharwat M, Al-Sobayil F, Buczinski S. Effect of racing on the serum concentrations of cardiac troponin I and creatine kinase myocardial band in racing camels (Camelus dromedarius). Vet Res Commun. (2013) 37:139–44. doi: 10.1007/s11259-013-9556-z
24. Woort T, Dubios G, Didier M, Van Erck-Westergren E. Validation of an equine fitness tracker: heart rate and heart rate variability. Comp Exerc Physiol. (2020) 17:189–98. doi: 10.3920/CEP200028
25. Faye B. Body condition score in dromedary camel: a tool for management of reproduction. Emirates J Food Agri. (2001) 13:1–6. doi: 10.9755/ejfa.v12i1.5193
26. Vezzosi T. Evaluation of a smartphone electrocardiograph in healthy horses: comparison with standard base-apex electrocardiography. J Equi Vet Sci. (2018) 67:61–5. doi: 10.1016/j.jevs.2018.03.006
27. Kraus MS, Rishniw M, Divers TJ, Reef VB, Gelzer AR. Utility and accuracy of a smartphone-based electrocardiogram device as compared to a standard base-apex electrocardiogram in the horse. Res Vet Sci. (2019) 125:141–7. doi: 10.1016/j.rvsc.2019.05.018
28. Samimi AS, Sakhaee E, Iranmanesh F. Evaluation of sedative, analgesic, physiological, and laboratory effects of two doses off medetomidine and xylazine in dromedary calves. J Vet Pharmacol Ther. (2019) 42:411–9. doi: 10.1111/jvp.12779
29. Tharwat M, Al-Sobayil F, Ali A, Buczinski S. Echocardiography of the normal camel (Camelus dromedaries) heart: technique and cardiac dimensions. BMC Vet Res. (2012) 8:130. doi: 10.1186/1746-6148-8-130
30. Tefera M. Observations on the clinical examination of the camel (Camelus dromedarius) in the field. Trop Anim Health Prod. (2004) 36:435–49. doi: 10.1023/B:TROP.0000035006.37928.cf
31. Samimi AS, Molaei MM, Azari O, Ebrahimpour F. Comparative evaluation of sedative and clinical effects of dexmedetomidine and xylazine in dromedary calves (Camelus dromedarius). Vet Anaesth Analg. (2020) 47:224–8. doi: 10.1016/j.vaa.2019.11.004
Keywords: camel, electrocardiograms, EquimetreTM, standard, tracker
Citation: Al Khamis T, Shawaf T, Almubarak A and Al-Ali MA (2023) Comparison between a fitness tracker (EquimetreTM) and standard base-apex electrocardiography in dromedary camels. Front. Vet. Sci. 9:963732. doi: 10.3389/fvets.2022.963732
Received: 07 June 2022; Accepted: 28 December 2022;
Published: 12 January 2023.
Edited by:
Ibrahim Elsohaby, City University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Samir Al-Bulushi, Royal Court Affairs, OmanMoufida Atigui, Institut des Régions Arides, Tunisia
Copyright © 2023 Al Khamis, Shawaf, Almubarak and Al-Ali. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Turke Shawaf,  dHNoYXdhZkBrZnUuZWR1LnNh
dHNoYXdhZkBrZnUuZWR1LnNh