 Flavio H. Alonso
Flavio H. Alonso Kevin D. Niedringhaus1
Kevin D. Niedringhaus1- 1Veterinary Medical Teaching Hospital, School of Veterinary Medicine, University of California, Davis, Davis, CA, United States
- 2Department of Biomedical Sciences, Ross University School of Veterinary Medicine, Basseterre, Saint Kitts and Nevis
- 3Department of Veterinary Clinic and Surgery, School of Veterinary Medicine, Federal University of Minas Gerais, Belo Horizonte, Brazil
This case report describes for the first time the cytologic characteristics of a hormonally secreting pituitary adenoma in a cat. An 8-year-old female spayed domestic long-haired cat was referred with a previous diagnosis of hypersomatotropism and secondary diabetes mellitus 7 months prior. Clinical signs included weight loss, polyphagia, polyuria, and polydipsia. Serum insulin-like growth factor-1 was 340 nmol/L (RI: 12-92), and CT scan revealed a hypophyseal mass, and a presumptive diagnosis of acromegaly was made. A transsphenoidal hypophysectomy was performed. A fragment of the pituitary gland was subjected to a squash preparation and cytology revealed a neuroendocrine neoplasm characterized by anisokaryosis and prominent nucleoli. Additional cytologic findings included cell cohesiveness, indistinct cytoplasmic borders, nuclear crowding, molding, and fragmentation. A diagnosis of adenoma was based on a lack of histopathologic or imaging evidence of invasion. A week later, during post-surgical hospitalization, the patient worsened and died. Histopathology from a necropsy procedure revealed fibrinosuppurative meningitis as a post-surgical complication. Pituitary adenomas might have an aggressive cytologic appearance, despite a lack of histopathologic invasion or dissemination.
Introduction
The prevalence of pituitary adenomas varies from 15 to 20% in people (1, 2) and represented 30 to 61% of the pituitary masses found in dogs in multiple studies (3–5). These can be classified based on size (microadenomas when they are smaller than 10 mm and macroadenomas when 10 mm or larger) and secretory pattern (e.g., corticotroph, somatotroph, melanotroph, or plurihormonal) (6). Somatotroph adenomas represent the most common pituitary tumor in cats and, when associated with hypersomatotropism, present with weight gain, broad facial and limb features, abdominal organomegaly, heart murmur, and diabetes mellitus-related clinical signs (7–9). In a recent study (9), the median survival time in cats with pituitary adenomas varied from 515 to 730 days, depending on the tumor type (9). Diagnosis and treatment normally depend on clinical signs, advanced imaging investigation, histopathology, transsphenoidal surgery, medical management, or radiotherapy (6, 10).
Anatomic and histopathologic findings have been extensively described in animals, but scientific reports approaching the cytologic features of pituitary neoplasms are still lacking. The objective of this report is to describe the findings of an intraoperative imprint smear cytology from a somatotroph pituitary adenoma in a cat, in the context of a complete diagnostic work-up protocol. This case report was written in agreement with the most updated version of the CARE guidelines (11).
Case Description
An 8-year-old female spayed domestic long-haired cat was referred to the neurology and neurosurgery service of the UC Davis William Pritchard Veterinary Medical Teaching Hospital for transsphenoidal hypophysectomy. The patient received a diagnosis of hypersomatotropism (serum insulin-like growth factor-1 = 340 nmol/L, RI = 12–92) and secondary diabetes mellitus 7 months prior to admission. Insulin therapy had been discontinued for about 6 months, and since then, the patient had lost ~680 g in weight and developed polyuria and polydipsia. On physical examination, the patient weighed 3 kg (body condition score = 3/9), and was bright, alert, responsive, and hydrated. Prognathism and prominent facial features were noted. No apparent cardiovascular, respiratory, integumentary, gastrointestinal, or neurologic abnormalities were noted, and no relevant familial history was reported.
Prior to the surgical procedure, a complete blood count (CBC, Advia 120 hematology analyzer; Siemens) revealed moderate lymphopenia (486 lymphocytes/μl, RI = 1,000–7,000), and slight thrombocytosis (576,000 platelets/μl, RI = 180,000–500,000). The biochemical panel (Cobas 6000 C501; Roche) revealed mixed metabolic acidosis and alkalosis (anion gap = 31 mmol/L, RI = 13–27 and bicarbonate = 19 mmol/L, RI = 15–21), selective chloride loss (chloride = 101 mmol/L, RI = 117–126 and sodium = 145 mmol/L, RI = 151–158), mild hyperkalemia (5.5 mmol/L, RI = 3.6–4.9), marked hyperglycemia (560 mg/dL, RI = 63–118) and mild hypertriglyceridemia (129 mg/dL, RI = 8–80). Serum fructosamine levels were 683 μmol/L (RI = 190–365) and a thyroid panel (Immulite 2000; Siemens) revealed total T4 < 0.5 μg/dL (RI = 1.1–3.3), free T4 <0.3 ng/dL (RI = 0.59–3.04) and TSH <0.03 (RI = 0-0.07). Urinalysis was performed on a sample obtained by cystocentesis, which revealed marked glucosuria, mild proteinuria and hypersthenuria (USG = 1.036, RI > 1.035).
Pre-surgical transverse contrast-enhanced CT images of the brain revealed a hyperintense large ovoid-shaped mass in the area of the pituitary gland measuring 8.6 by 8.3 by 6.8 mm (Figure 1).
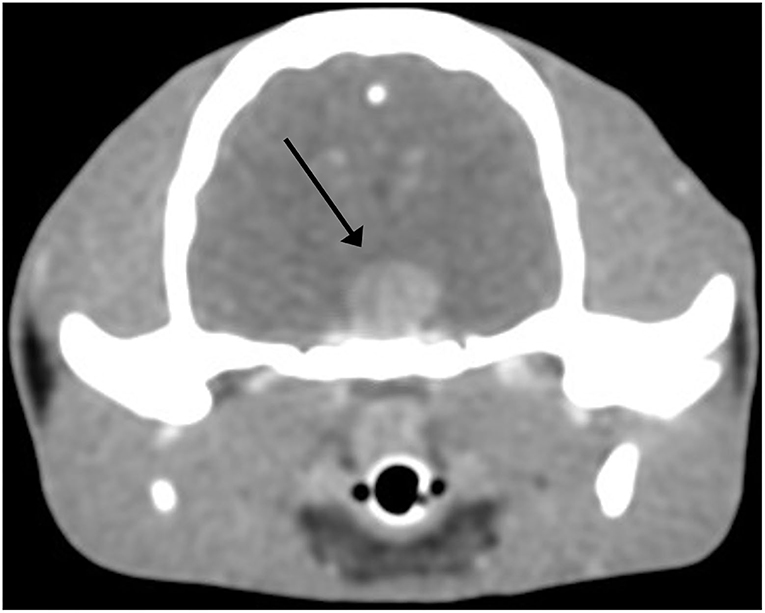
Figure 1. Pituitary adenoma, cat. Postcontrast transverse CT image of the skull in soft tissue window. An 8.6 by 8.3 by 6.8 mm mass (arrow) is noted at the anatomical region of the pituitary gland. A slice thickness of 0.62 mm was used.
During the transsphenoidal hypophysectomy, imprint smears from the pituitary mass were prepared and submitted for cytologic analysis. The specimen was highly cellular, and the background contained a diffuse and amorphous light pink material (consistent with fragmented cytoplasms) and a low number of red blood cells, admixed with many naked nuclei and other cellular debris. Intact nucleated cells were scattered throughout in vaguely cohesive sheets and clusters and presented indistinct borders, intermediate nucleus:cytoplasm (N:C) ratio, and a pale blue to pink smooth cytoplasm. The nuclei of this population of cells were oval to polygonal with finely granular chromatin patterns and multiple small and prominent nucleoli. Anisokaryosis and anisocytosis were marked. Nuclear crowding, molding, and fragmentation were noted. Rare endothelial cells were also noted. Findings were interpreted as neuroendocrine neoplasia (Figure 2).
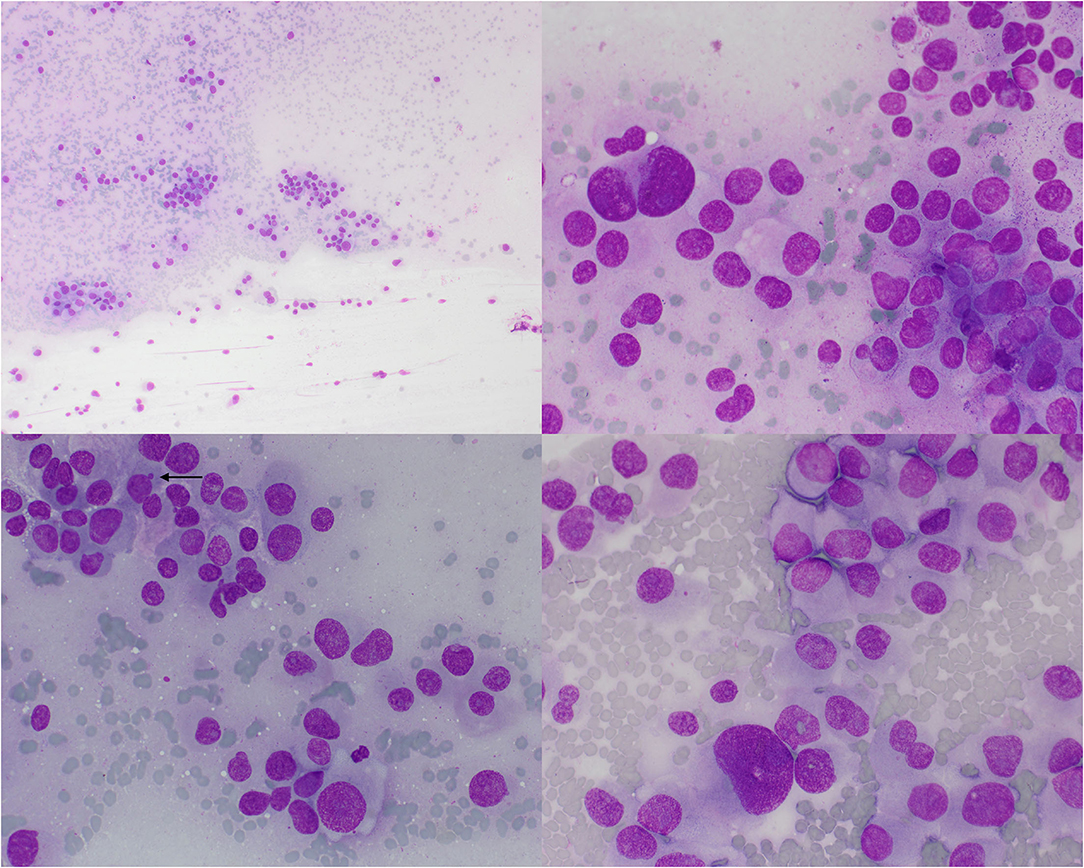
Figure 2. Pituitary adenoma, cat. An imprint smear of the surgically excised pituitary mass revealed moderate numbers of neuroendocrine neoplastic cells arranged individually or in small aggregates. Cells have round to pleomorphic nuclei and a pale gray cytoplasm with poorly distinct borders and occasional vacuolization. The chromatin is finely stippled and contains multiple prominent nucleoli. Anisokaryosis is moderate to marked and occasional micronuclei are noted (arrow). Wright's-Giemsa, 10× (upper left) and 50× objective lenses.
On histopathologic evaluation, the pituitary gland tissue consisted of a densely cellular, expansile, unencapsulated mass composed of nests and cords of polygonal cells on a fine fibrovascular stroma. Neoplastic cells presented distinct cell borders and a moderate amount of brightly eosinophilic glassy to granular cytoplasm. Nuclei were round with vesiculated chromatin and one prominent nucleolus. Anisocytosis and anisokaryosis were mild. Mitotic figures were rare (Figure 3). The periphery revealed compression and mild atrophy of adjacent, non-neoplastic tissue.
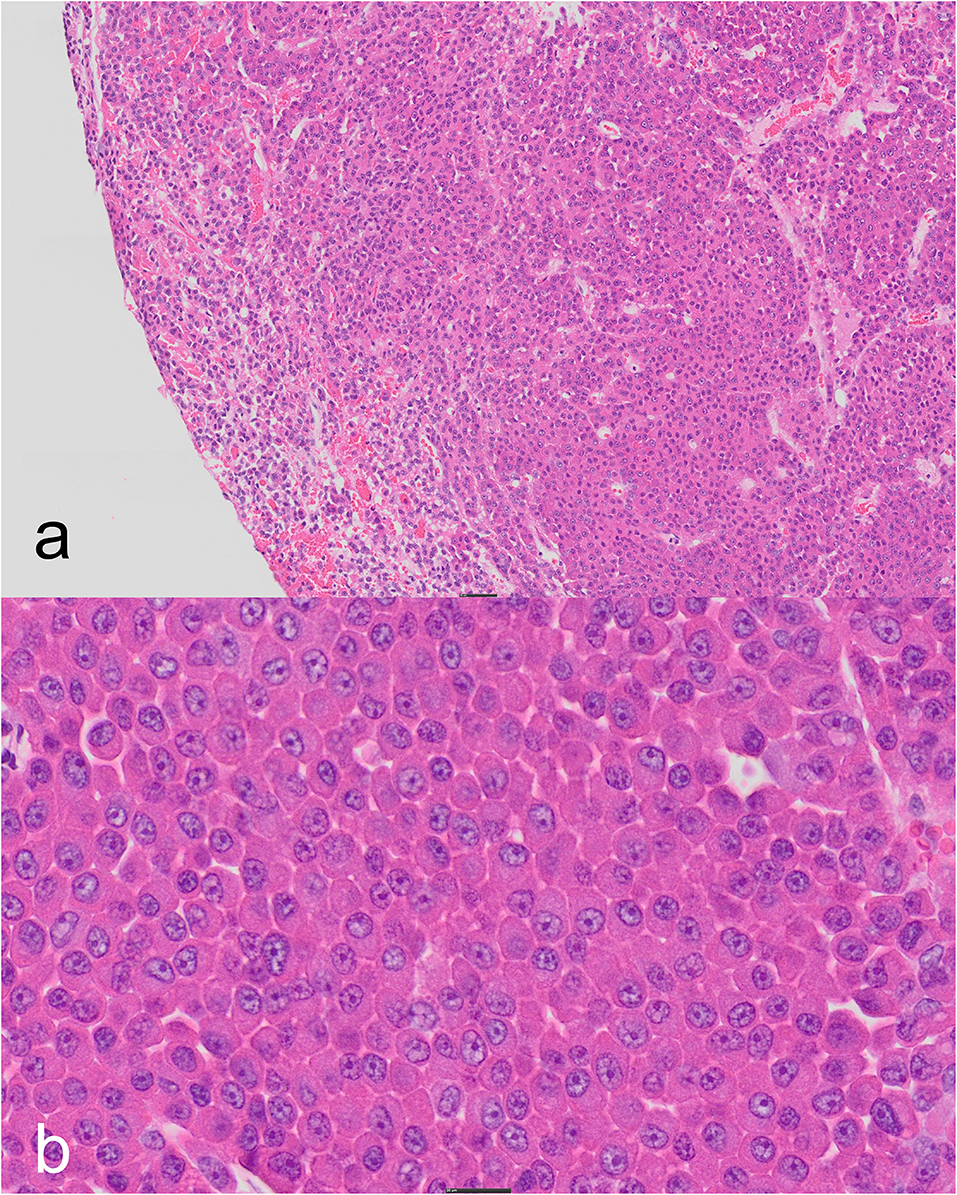
Figure 3. Pituitary adenoma, cat. (a) The center of the tissue contains a non-encapsulated mass consisting of nests and cords of a monomorphic population of cells compressing the peripheral parenchyma with scant, acute hemorrhage (4× objective lens). (b) Densely-packed sheets of well-differentiated, brightly eosinophilic, granular cells with large central nuclei and prominent, single nucleoli (20× objective lens). Hematoxylin-eosin.
Histochemical staining with reticulin and periodic acid Schiff (PAS) and immunohistochemical staining with growth hormone were performed. Reticulin staining revealed a loss of reticular network within the neoplasm with respect to the compressed peripheral, non-neoplastic tissue (Figure 4), and the granules did not stain with PAS (Figure 4). Growth hormone immunohistochemistry revealed many clusters of cells with faint or weak cytoplasmic immunoreactivity within the neoplasm (Figure 4) similar to that in the control. The cellular architecture based on H&E staining, histochemical and immunohistochemical profile and lack of evidence of invasion or metastasis on histology and clinical imaging resulted in a diagnosis of somatotroph adenoma (9).
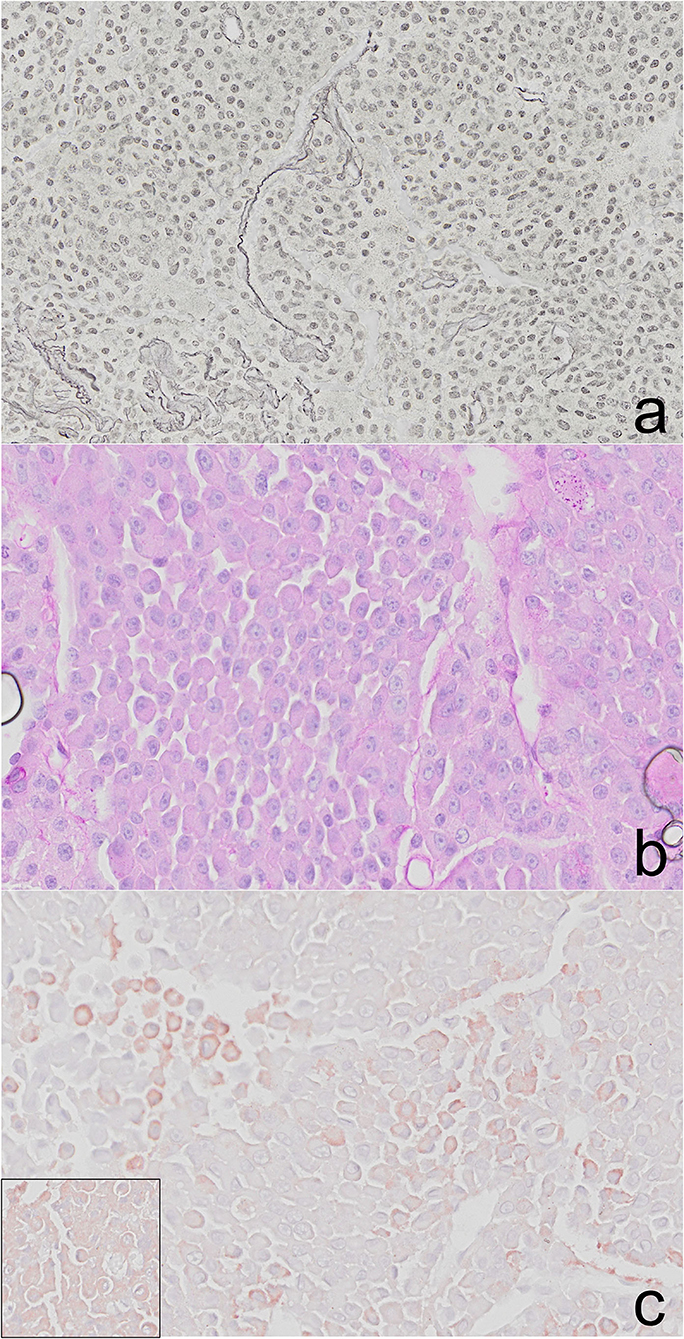
Figure 4. Pituitary adenoma, cat. (a) The reticulin network is lost within the neoplasm and is still present in the compressed, peripheral pituitary tissue. (b) The cytoplasmic granules within the adenoma lack staining with PAS. (c) Clusters of cells throughout the adenoma have faint, cytoplasmic immunoreactivity to growth hormone (GH). GH positive control cells (inset).
A week later, during post-surgical hospitalization, the patient's clinical condition worsened, and it died. A post-mortem examination with histopathology revealed fibrinosuppurative meningitis as a post-surgical complication, which was likely responsible for this patient's death. Other findings included a small focal area of thyroid nodular hyperplasia, vasculitis with thrombi in the lungs, multivacuolar degeneration, associated with focal amyloidosis and atrophy of the endocrine pancreatic islets, focally extensive lymphocytic enteritis, an incidental focal dilation in the esophagus and moderate, and diffuse vacuolar degeneration of the liver. Evaluation of remnant pituitary tissue in the sella turcica, as well as regional lymph nodes, confirmed a lack of invasion into the surrounding vasculature, parenchyma, bone, or lymphatics.
Discussion
This is, to the best of the author's knowledge, the first cytologic description of a pituitary adenoma in animals. The cytologic appearance of the tumor exhibited some malignancy criteria such as marked anisokaryosis, prominent nucleoli, and nuclear molding. Despite these features, histological evaluation, in conjunction with CT and postmortem findings, was consistent with the accepted definition of an adenoma (9, 12). Cellular features are not a reliable indicator of malignant behavior in these neoplasms (12). The immunoreactivity to growth hormone and lack of PAS-positive granules supported a somatotrophic origin. Growth hormone immunoreactivity can vary widely in somatotroph adenomas, but the pattern and location of staining similar to that in the control (i.e., relatively weak in both the sample and the control) warranted the interpretation of immunoreactivity. The lack of intact reticulin network was used to differentiate adenoma from hyperplasia, and there was no evidence of vascular, bone, or local invasion or metastasis based on CT, gross postmortem examination, or postmortem histopathology (9). It is unclear why cytological interpretation in the smear showed cellular features of malignancy while histologically anisocytosis and anisokaryosis were interpreted as mild. This might implicate the higher specificity of Romanowsky-stained FNA samples to assess cytologic features, compared to histopathology. Furthermore, the lack of reference for malignant features in somatotrophs on cytology preparations or variation in cytologic features spatially within the tumor may have contributed to this discrepancy. While it is possible that this neoplasm is a carcinoma that has not yet metastasized, the prolonged clinical course of this patient's hypersomatotropism combined with the notion that carcinomas are less likely to be hormonally functional provide more evidence of a benign nature in this case (12).
Cytology of central nervous system tissues by direct aspiration, cannula, and squash preparation represents an option widely used in human medicine for the diagnosis of neoplasms such as medulloblastomas, germ cell tumors, and choroid plexus papillomas (13). It also seems to be a promising diagnostic technique in the veterinary neurosurgery field, given the recent advances in imaging diagnosis in that area (14). Accurate diagnosis via cytology was achieved in over 90% of human, canine, and feline cases in studies investigating over 4,000 correlated biopsies (15, 16).
Due to the complex range of biologic behavior patterns associated with pituitary tumors in people, the International Pituitary Pathology Club proposed pituitary adenomas, atypical adenomas, and carcinomas, in accordance with the developments involving the terminology of other neuroendocrine neoplasms, should be collectively referred to pituitary neuroendocrine tumors (17). In human pathology, the most updated classification of these tumors is mainly based on the tumor cell lineage, cell type, and related characteristics. It also involves the routine use of immunohistochemistry for pituitary transcription factors (PIT1, TPIT, SF1, GATA3, and ERα), but malignancy has always been associated with histologic evidence of regional or distant dissemination (18).
This patient had evidence of primary diabetes mellitus including islet cell pancreatic amyloidosis, however, diabetes mellitus in cats is considered a common consequence of hypersomatotropism, with hypophysectomy representing the gold standard type of therapy (19, 20). In a study, 59 out of 184 variably controlled diabetic cats had markedly increased (i.e., >1,000 ng/ml, RI = 208–443) serum levels of insulin-like growth factor 1 (21). The mechanism thought to play a role in this association is a GH-induced resistance to insulin at the level of adipocytes and myocytes (22).
Even though this patient was diagnosed with the non-thyroidal disease, which could account for the low total and free T4 serum levels, and the histopathologic evaluation of the thyroid gland revealed a small area affected by nodular hyperplasia, the TSH result was below the assay detection limit and this patient had evidence of pituitary atrophy secondary to the adjacent growth disorder. Also, thyroid nodular hyperplasia, even though highly prevalent, is reported to be non-functional in many cats (23). As such, a diagnosis of central hypothyroidism, due to pituitary atrophy and TSH deficiency, could not be ruled out. In fact, most human patients with active acromegaly have diminished serum TSH concentrations and around 25% have hypothyroidism (24, 25). All seven adult cats with primary spontaneous hypothyroidism in a recent case series had increased levels of TSH (26). Pituitary adenoma is listed as an important cause of central hypothyroidism in people (27), and the formal approach to human patients with clinical signs of hypothyroidism and concomitant pituitary disorders involves the investigation for central hypothyroidism (28).
Even though this was not further explored, the patient herein reported presented with polyuria. That could be merely attributed to osmotic diuresis secondary to glucosuria, but a defect with vasopressin (antidiuretic hormone, ADH) secretion by another pituitary gland impaired function as an additional contributor to the polyuria could be speculated.
One potential limitation of this report might be represented by the lack of cerebrospinal fluid (CSF) analysis done prior to surgery. As stated earlier, according to a recent WHO consensus, cerebrospinal involvement is used in the assessment of pituitary gland malignancy (29). However, this evaluation is still currently restricted to the histopathologic level, and not by using other tools, such as CSF cytologic analysis. Furthermore, the most recent WHO consensus only uses evidence of metastasis to differentiate the diagnosis of pituitary neuroendocrine tumors (18).
Conclusion
Pituitary adenomas in cats may have a relatively aggressive cytologic picture and care should be taken not to presume malignancy. If tumor growth is causing secondary pituitary atrophy, resulting central endocrinopathies, such as hypothyroidism, should be ruled out.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
FA and KN contributed to conception and design of the case description. FA organized the case data and wrote the first draft of the manuscript. KN and MC wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ezzat S, Asa SL, Couldwell WT, Barr CE, Dodge WE, Vance ML, et al. The prevalence of pituitary adenomas. Cancer. (2004) 101:613–9. doi: 10.1002/CNCR.20412
2. Hall WA, Luciano MG, Doppman JL, Patronas NJ, Oldfield EH. Pituitary magnetic resonance imaging in normal human volunteers: occult adenomas in the general population. Ann Intern Med. (1994) 120:817–20. doi: 10.7326/0003-4819-120-10-199405150-00001
3. Pollard RE, Reilly CM, Uerling MR, Wood FD, Feldman EC. Cross-sectional imaging characteristics of pituitary adenomas, invasive adenomas and adenocarcinomas in dogs: 33 cases (1988–2006). J Vet Intern Med. (2010) 24:160–5. doi: 10.1111/J.1939-1676.2009.0414.X
4. Polledo L, Grinwis GCM, Graham P, Dunning M, Baiker K. Pathological findings in the pituitary glands of dogs and cats. Vet Pathol. (2018) 55:880–8. doi: 10.1177/0300985818784162
5. Sanders K, Galac S, Meij BP. Pituitary tumour types in dogs and cats. Vet J. (2021) 270:105623. doi: 10.1016/J.TVJL.2021.105623
6. Molitch ME. Diagnosis and treatment of pituitary adenomas: A review. JAMA. (2017) 317:516–24. doi: 10.1001/JAMA.2016.19699
7. Mayer MN, Greco DS, LaRue SM. Outcomes of pituitary tumor irradiation in cats. J Vet Intern Med. (2006) 20:1151–4. doi: 10.1111/J.1939-1676.2006.TB00714.X
8. Peterson ME, Taylor RS, Greco DS, Nelson RW, Randolph JF, Foodman MS, et al. Acromegaly in 14 cats. J Vet Intern Med. (1990) 4:192–201. doi: 10.1111/J.1939-1676.1990.TB00897.X
9. Miller MA, Piotrowski SL, Donovan TA, Scott-Moncrieff JC, Owen TJ, Mccue JP, et al. Feline pituitary adenomas: correlation of histologic and immunohistochemical characteristics with clinical findings and case outcome. Vet Pathol. (2021) 58:266–75. doi: 10.1177/0300985820978309
10. Mamelak AN, Owen TJ, Bruyette D. Transsphenoidal surgery using a high definition video telescope for pituitary adenomas in dogs with pituitary dependent hypercortisolism: Methods and results. Vet Surg. (2014) 43:369–79. doi: 10.1111/J.1532-950X.2014.12146.X
11. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D, et al. The CARE guidelines: consensus-based clinical case report guideline development. J Diet Suppl. (2013) 10:381–90. doi: 10.3109/19390211.2013.830679
12. Rosol TJ, Meuten DJ. Tumors of the endocrine glands. In: Tumors in Domestic Animals. Berkeley, CA: University of California Press (2016). p. 766–833 doi: 10.1002/9781119181200.ch18
13. Bigner SH, Carter AL. Central nervous system. In: Bibbo M, Wilbur. D, editors. Comprehensive Cytopathology. Amsterdam: Elsevier Health Sciences (2008). p. 439–52
14. de Lorenzi D, Mandara MT. The central nervous system. In: Raskin RE, Meyer DJBT-C, editors. Canine and Feline Cytology. St. Louis: Elsevier (2016). p. 369–407. doi: 10.1016/B978-1-4557-4083-3.00014-0
15. de Lorenzi D, Mandara MT, Tranquillo M, Baroni M, Gasparinetti N, Gandini G, et al. Squash-prep cytology in the diagnosis of canine and feline nervous system lesions: a study of 42 cases. Vet Clin Pathol. (2006) 35:208–14. doi: 10.1111/J.1939-165X.2006.TB00116.X
16. Tilgner J, Herr M, Ostertag C, Volk B. Validation of intraoperative diagnoses using smear preparations from stereotactic brain biopsies: intraoperative versus final diagnosis—influence of clinical factors. Neurosurgery. (2005) 56:257–63. doi: 10.1227/01.NEU.0000148899.39020.87
17. Asa SL, Casar-Borota O, Chanson P, Delgrange E, Earls P, Ezzat S, et al. From pituitary adenoma to pituitary neuroendocrine tumor (PitNET): an International Pituitary Pathology Club proposal. Endocr Relat Cancer. (2017) 24:C5–8. doi: 10.1530/ERC-17-0004
18. Asa SL, Mete O, Perry A, Osamura RY. Overview of the 2022 WHO Classification of Pituitary Tumors. Endocrine Pathol. (2022) 33:1 (2022) 33:6–26. doi: 10.1007/S12022-022-09703-7
19. Fenn J, Kenny PJ, Scudder CJ, Hazuchova K, Gostelow R, Fowkes RC, et al. Efficacy of hypophysectomy for the treatment of hypersomatotropism-induced diabetes mellitus in 68 cats. J Vet Intern Med. (2021) 35:823–33. doi: 10.1111/JVIM.16080
20. Fleeman L, Gostelow R. Updates in feline diabetes mellitus and hypersomatotropism. Vet Clin Small Anim Pract. (2020) 50:1085–105. doi: 10.1016/J.CVSM.2020.06.005
21. Niessen SJM, Petrie G, Gaudiano F, Khalid M, Smyth JBA, Mahoney P, et al. Feline acromegaly: an underdiagnosed endocrinopathy? J Vet Intern Med. (2007) 21:899–905. doi: 10.1111/j.1939-1676.2007.tb03041.x
22. Feldman EC, Nelson RW. Acromegaly and hyperadrenocorticism in cats: a clinical perspective. J Feline Med Surg. (2000) 2:153–8. doi: 10.1053/JFMS.2000.0091
23. Norsworthy GD, Adams VJ, Mcelhaney MR, Milios JA. Palpable thyroid and parathyroid nodules in asymptomatic cats. J Feline Med Surg. (2002) 4:145–51. doi: 10.1053/jfms.2001.0163
24. Roelfsema F, Biermasz NR, Frolich M, Keenan DM, Veldhuis JD, Romijn JA. Diminished and irregular thyrotropin secretion with preserved diurnal rhythm in patients with active acromegaly. J Clin Endocrinol Metab. (2009) 94:1945–50. doi: 10.1210/JC.2009-0174
25. Geeldhoed-Duijvestijn PHLM, Bussemaker JK, Roelfsema F. Changes in basal and stimulated TSH and other parameters of thyroid function in acromegaly after transsphenoidal surgery. Eur J Endocrinol. (1989) 121:207–15. doi: 10.1530/ACTA.0.1210207
26. Peterson ME, Carothers MA, Gamble DA, Rishniw M. Spontaneous primary hypothyroidism in 7 adult cats. J Vet Intern Med. (2018) 32:1864–73. doi: 10.1111/jvim.15239
27. Yamada M, Mori M. Mechanisms related to the pathophysiology and management of central hypothyroidism. Nat Clin Pract Endocrinol Metab. (2008) 4:683–94. doi: 10.1038/ncpendmet0995
28. Beck-Peccoz P, Rodari G, Giavoli C, Lania A. Central hypothyroidism—a neglected thyroid disorder. Nat Rev Endocrinol. (2017) 13:588–98. doi: 10.1038/nrendo.2017.47
Keywords: brain, histopathology, central hypothyroidism, hypophysis, diabetes mellitus
Citation: Alonso FH, Niedringhaus KD, Ceregatti MG and Maglaty MA (2022) Case Report: Cytologic Description of Somatotroph Pituitary Adenoma in a Cat. Front. Vet. Sci. 9:934009. doi: 10.3389/fvets.2022.934009
Received: 01 May 2022; Accepted: 20 June 2022;
Published: 18 July 2022.
Edited by:
Anna Oevermann, University of Bern, SwitzerlandReviewed by:
Judith Howard, University of Bern, SwitzerlandLuciana Mandrioli, University of Bologna, Italy
Andreas Beineke, University of Veterinary Medicine Hannover, Germany
Copyright © 2022 Alonso, Niedringhaus, Ceregatti and Maglaty. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Flavio H. Alonso, ZmxhdmlvaGFsb25zb0BnbWFpbC5jb20=