 Eric Vieira Januário1*
Eric Vieira Januário1* Samanta Rios Melo1
Samanta Rios Melo1 Durvanei Augusto Maria2
Durvanei Augusto Maria2 Carla Aparecida Batista Lorigados1
Carla Aparecida Batista Lorigados1 Aline Magalhães Ambrósio1Marcia Mery Kogika3Bruno Cogliati4
Aline Magalhães Ambrósio1Marcia Mery Kogika3Bruno Cogliati4 Helio Junji Shimozako5
Helio Junji Shimozako5 Julia Maria Matera1
Julia Maria Matera1- 1Department of Surgery, School of Veterinary Medicine and Animal Science, University of São Paulo (FMVZ-USP), São Paulo, Brazil
- 2Laboratory of Development and Innovation, Institute Butantan, Butantan, São Paulo, Brazil
- 3Department of Internal Medicine, School of Veterinary Medicine and Animal Science, University of São Paulo, São Paulo, Brazil
- 4Department of Pathology, School of Veterinary Medicine and Animal Science, University of São Paulo, São Paulo, Brazil
- 5Laboratory of Bovine Viruses, Biological Institute of São Paulo, São Paulo, Brazil
Canine mast cell tumor is a malignant neoplasm, and a gold standard treatment remains to be determined despite the proposed chemotherapies or other therapies in dogs. This study aimed to determine therapeutic, adverse effects and toxicity, tumor-free, and overall survival times of 10 dogs with surgically excised mast cell tumors evaluated by histopathological/immunohistochemistry and treated with four weekly intravenous administrations of 2-Aminoethyl Dihydrogen Phosphate (70 mg/kg) as adjuvant therapy. No adverse events were noted. Laboratory changes were limited (p < 0.05) in red blood cell, hemoglobin, and platelet counts. Mean tumor-free and overall survival were 599.1 ± 469 and 755.5 ± 423.5 days, respectively. In conclusion, 2-Aminoethyl Dihydrogen Phosphate administration was safe in dogs. However, 2-Aminoethyl Dihydrogen Phosphate was not sufficiently effective to prevent a recurrence, new tumor, or metastasis of canine mast cell tumors with poor immunohistochemical prognostic factors.
Introduction
Canine mast cell tumors (MCT) affect the skin and subcutaneous tissues and may be also found in other tissues and organs, such as lymph nodes, the gastrointestinal tract, the liver, and the spleen. The relevance of these tumors stems from their malignancy and metastatic potential, with significant impacts on quality of life and survival of affected dogs (1–4). Disease progression varies according to clinical stage and MCT histological grade (5–7).
Skin MCT may be classified into three types (Grade I, II, or III) based on histopathological features, or described as well or poorly differentiated (high and low grade, respectively) (5, 6). Subcutaneous MCT are classified as circumscribed, infiltrative or combined (8, 9). Anatomical location (10), breed (1, 11), local recurrence (12), systemic manifestations (13), genomic (14), c-kit mutation (15, 16), expression of cell proliferation and growth rate markers such as AgNor, PCNA, and Ki67 (16–18), microvascular density and mitotic index (19) are other prognostic factors involved in MCT clinical progression.
MCT treatment includes surgical resection, cryosurgery, chemotherapy and radiotherapy, alone or in combination (3). Chemotherapy with vinblastine (12, 20), lomustine (21), clorambucil (22) or other antineoplastics such as masitinib mesilate (23), and toceranib (20) may be combined with
glucocorticoids such as prednisone and prednisolone (20, 24). However, a gold standard treatment for MCT remains to be determined (20). The aforementioned drugs are not free of adverse effects and toxicity in dogs and their use has been associated with neutropenia (21, 25), gastrointestinal toxicity (21, 25), pyrexia (21, 25), liver toxicity (24, 25) and pancreatitis (25), among other problems.
The search for novel antitumor therapies led to the investigation of a new class of drugs: antineoplastic phospholipids. Phospholipids are antitumor analogs, such as 2-Aminoethyl Dihidrogen Phosphate (2-AEH2F), which is a phosphorylated compound capable of controlling cellular proliferation and inducing apoptosis in several types of tumor cells (26). One drug has been derived from 2-AEH2F, a phospholipid cell membranes substrate (27). Although its mechanism is not fully understood, it is demonstrated that its effects are dependent on the incorporation in the cell membrane, modifying its structure and leading to cell death. It has been proposed that the internalization of 2-AEH2F into the cell membrane occurs via endocytosis mediated by lipid rafts. Recent studies have demonstrated the crucial requirement of Phosphoethanolamine (PE) in regulating mitochondrial function, change morphology and important role in autophagy (28, 29). PE constitutes about 25% of mammalian phospholipids and in brain tissue it reaches 45% of this composition. PE plays an important role in contractile ring disassembly at the cleavage furrow during cytokinesis of mammalian cells and a lack of PE inhibits progression of the cell cycle; demonstrating its antiproliferative potential similar to 2-AEH2F (30, 31).
The phospholipid compound 2-AEH2F is cytotoxic for a variety of cell tumors, such as human melanoma (SK-MEL-28, MEWO), murine melanoma (B16-F10) (32), human leukemia cell (33), murine hepatocellular carcinoma (Hepa1c1c17) (34), human breast cancer (MCF-7) (35), Ehrlich ascitic tumor (36), and murine renal cell carcinoma (37). In dogs 2-AEH2F was recently tested as an intravenous neoadjuvant therapy for soft tissue sarcoma and promoted a decrease in peritumoral skin temperature, which suggested the physiological effects of the substance on this type of neoplasia (38).
Given the need to develop novel antineoplastic therapies targeting MCT, this study set out to determine the in vivo effects of four weekly intravenous administrations of 2-AEH2F soluble preparation in dogs with skin or subcutaneous MCT, to evaluate treatment effects on overall (OS) and tumor-free survival (TFS), and to investigate adverse events and laboratory changes in treated patients. The hypothesis is that 2-AEH2F may be effective in preventing canine MCT recurrence, new tumor growth or metastasis, aside its immunohistochemical classification.
Materials and Methods
Experimental Design
A small, single-arm, open-label, uncontrolled experimental research with 10 dogs diagnosed with skin or subcutaneous MCT. The study was not blinded with the objective that the dog owners knew and agreed with the instituted therapy. As it is a descriptive study on tolerability and efficacy, it was decided to describe such circumstances in a limited number of 10 dogs, because it is a sample size that we could achieve in our hospital.
All experiments were carried out in accordance with the Ethics Committee for the Use of Animals of the Faculty of Veterinary Medicine and Zootechnics of the University of São Paulo (FMVZ-USP, São Paulo - Brazil) (protocol number 9825270116). In the clinical trial, informed consent to participate in the study was obtained from the dog owners prior to any study procedure.
Inclusion criteria were the presence of one or more skin neoformations eligible for surgical removal, diagnosis of cutaneous or subcutaneous MCT by post-surgical histopathological examination. Exclusion criteria were dogs with previous tumor history, other concomitant neoplasms, MCT metastases, except in excisable lymph nodes, non-operable tumors, anesthetic, surgery, and chemotherapy contraindications.
Animals and Tumors
Ten household dogs (7 males, 3 females) were seen at the Small Animal Surgery Department of the Veterinary Hospital (HOVET) of the School of Veterinary Medicine and Animal Science of the University of São Paulo (FMVZ-USP, São Paulo - Brazil) and diagnosed with skin or subcutaneous MCT. The median age of dogs was 9.5 years (range: 5–13 years) and the median weight was 15.9 kg (range: 1.7–39.2 kg). The dogs resided and fed freely with their owners. Dogs presented with skin or subcutaneous masses, erythematous (n = 5) or not (n = 7), sessile (n = 10), or pedunculated (n = 2) and no other clinical manifestations. The initial diagnosis was obtained using fine-needle aspiration using a 25-ga needle. The material collected was gently spread on glass slides, smeared and stained by Panoptic technique. All dogs underwent surgical excision of MCT. The tumors were excised with dogs under general inhalation anesthesia (isofluorane). A 3.0 cm safety margin for all sides and a fascial plane was removed. Surgical wound closure was performed with simple suture or advancement or transposition flaps. Excisional tissue specimens had diameters of 0.4–8.0 cm (median = 2.2 cm), soft (n = 7) or firm (n = 5), ulcerated (n = 2) or not (n = 10), irregular surface (n = 4) or smooth (n = 8), alopecic (n = 4) or not (n = 8), hyperpigmented (n = 3) or not (n = 9). The characteristics of the dogs and MCT are listed in Table 1.
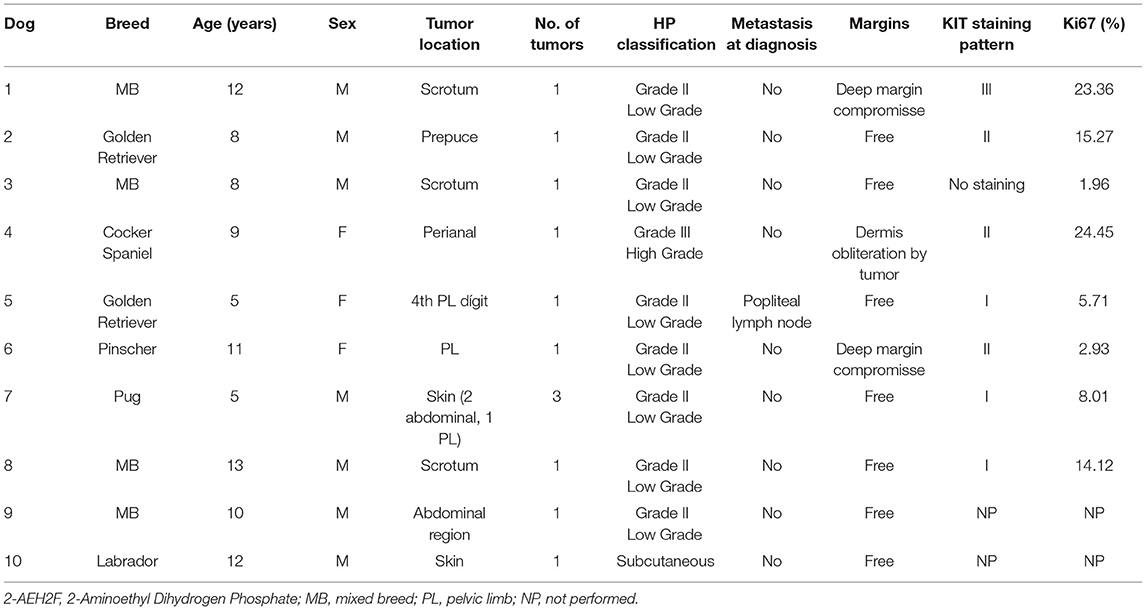
Table 1. Signalment and tumor characteristics of dogs treated with 2-AEH2F.
Product
The 2-AEH2F, sterile solution (pH = 7.2) was synthesized by the Chemistry and Polymer Technology Laboratory of the University of São Paulo (USP- São Carlos, Brazil) and prepared to achieve 99% analytical purity, confirmed by high-performance liquid chromatography (HPLC). For in vivo trials, the 1M stock sterile solution is dissolved in water and stored at room temperature. Stability has been demonstrated elsewhere (33, 35–37).
Histological and Immunohistochemical Analysis
Surgical specimens (n = 10) were stored in 10% formaldehyde, then embedded in paraffin, cut, and stained with hematoxylin and eosin for histological examination. Patnaik, Kiupel and Thompson classifications were used (5, 6, 9). Immunohistochemical analyses (kit immunostaining and Ki67 expression, n = 8) were also run for prognostic factor determination (Table 1).
2-AEH2F Therapy
Following surgical resection and histopathological confirmation of MCT diagnosis, patients (n = 10) were treated with four doses of intravenous 2-AEH2F (70 mg/kg diluted in sterile 0.9% saline solution) at weekly intervals (D1, D8, D15, and D22).
Patient Examination and Follow-Up
Medical history collection and physical examination were carried out before surgery (D0), on drug delivery days (D1, D8, D15 e D22), and within 30 days of the last 2-AEH2F administration (D52). Changes detected on physical examination, tumor recurrence, and/or development of new tumors were recorded. Dogs were then reassessed every 90 days for 6 months and every 180 days thereafter. Tumor recurrence, new tumor growth, or metastasis development were investigated, and survival rates determined. At time points D0, D8, D15, D22, and D52 dogs were submitted to the following tests: complete blood count, kidney (urea and creatinine) and liver (alanine aminotransferase/ALT, alkaline phosphatase/AP and albumin) biochemical analysis, and fasting triglyceride, total cholesterol, and blood glucose level determination. Dogs were also submitted to eco and electrocardiographic assessment (D0) and transabdominal ultrasonography (D0, D52, then every 90 days for 6 months and every 180 days thereafter).
Laboratory Tests
Laboratory tests were performed at HOVET-FMVZ-USP Clinical Laboratory. Blood samples were collected into dry and EDTA-containing tubes and immediately processed. Dry tube samples were spun at 2,500 rpm for 10 min for blood serum separation. Complete blood count was carried out using automated equipment (ADVIA 2120i - Siemens Healthcare Diagnostics Inc., Camberley, UK) and light microscopy. Liver and kidney biochemical analysis, blood glucose, triglyceride, and total cholesterol level determination were also performed using automated equipment (LabMax, Labtest, Tokyo, Japan). Laboratory result analysis was based on mean values and standard deviations obtained at D0, D8, D15, and D22. Adverse events secondary to chemotherapeutic and antineoplastic agents were also investigated according to the criteria of the Veterinary cooperative oncology group (39).
Statistical Analysis
Dogs in this sample were assessed at five-time points (D0, D8, D15, D22, and D52). The following variables (20) were evaluated: red cell count, hemoglobin levels, packed cell volume, leukocyte count (band and segmented neutrophils, lymphocytes, monocytes, eosinophils, and basophils), platelet count, blood glucose, triglyceride, and total cholesterol levels, and serum ALT, AP, albumin, urea and creatinine levels. Measures of central tendency (means and medians) were calculated for each variable. Measures of dispersion (standard deviations) and upper and lower limits of 95% confidence intervals were calculated for respective means. Data were collected from the same dogs at each time point; therefore, samples were defined as a dependent.
The non-parametric Friedman test was used for variable-specific analysis at different time points, with the level of significance set at 5% (α = 0.05). The non-parametric Wilcoxon post hoc test was then applied with a Bonferroni-adjusted level of significance of 0.5% (αBonf. = 0.005). Overall and TFS data were used to construct Kaplan-Meier survival curves.
Results
Animals
This sample comprised 10 dogs with histological diagnosis of skin (n = 9) or subcutaneous (n = 1) MCT and free from cutaneous or sonographic evidence of metastasis on D0. Enlarged popliteal lymph node was noted only in one dog and metastasis histologically confirmed following surgical resection. MCT were surgically resected and histologically classified as per Patnaik and Kiupel (5, 6), as follows: grade II/low grade (GII/LG), n = 8; grade III/high grade (GIII/HG), n = 1; subcutaneous (SC), n = 1. Tumors were also described as having free or compromised surgical margins (n = 8 and n = 2, respectively). Eight histological samples were submitted to immunohistochemical analysis, whereas two samples were not amenable to this test due to the absence of adequate and enough histopathological material for this examination (Table 1).
2-AEH2F Treatment and Follow-Up
All patients received four courses of intravenous 2-AEH2F (70 mg/kg). Dogs in this sample tolerated IV 2-AEH2F administration (70 mg/kg) well. No changes suggestive of adverse events were reported by owners or noted in physical examination throughout treatment (D1, D8, D15, and D22) or up to D52.
Laboratory Tests
The mean and standard deviation of laboratory test results obtained on D0, D8, D15, D22, and D52 are shown in Table 2. Lower lymphocyte counts (= 160/μL, >50% below lower limit for age range) suggestive of grade 3 toxicity (adverse event potentially related to test agent) was detected in one dog (patient 7) on D22. Other laboratory changes were limited to grade 2 (adverse event unlikely related to test agent) or grade 1 (adverse event clearly unrelated to test agent). The following laboratory parameters reached abnormal levels over the course the study: hemoglobin levels, leukocyte, lymphocyte and platelet counts, blood glucose and serum ALT and urea levels. Remaining laboratory parameters were within normal ranges according to toxicity criteria adopted in this trial (39) (Table 3).
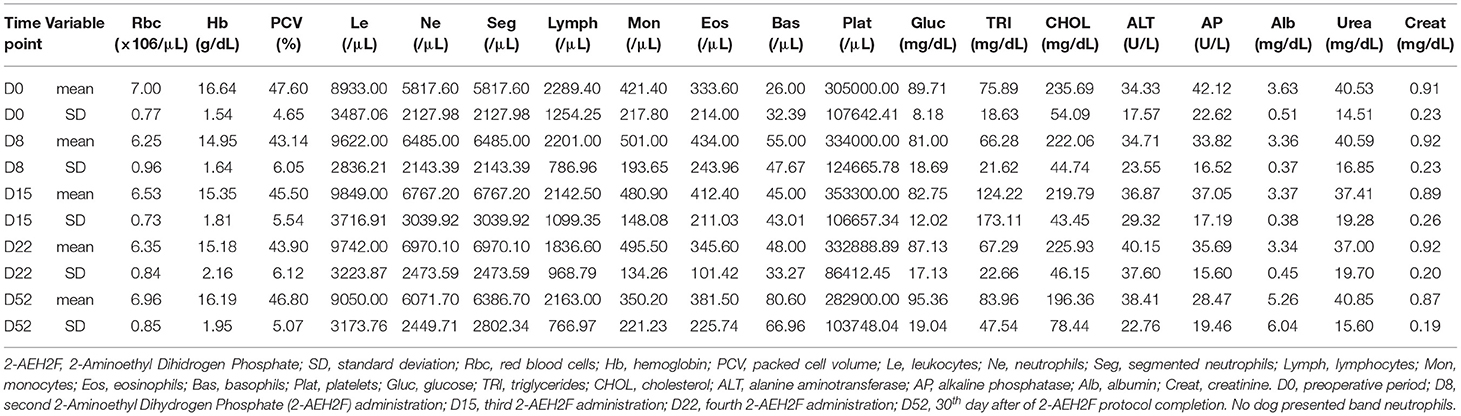
Table 2. Laboratory test results (mean, standard deviation) of dogs treated with 2-AEH2F at different time points.
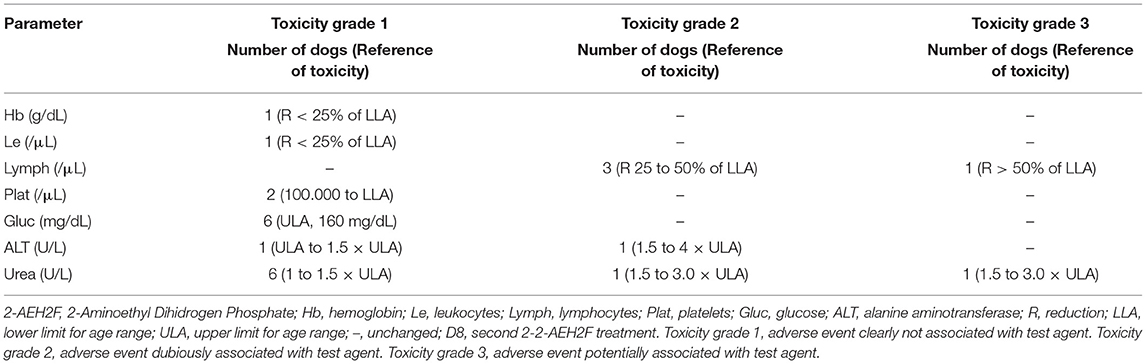
Table 3. Number of dogs showing laboratory changes of toxicity grade following treatment with 2-AEH2F (D8 onwards) (39).
Progression
Tumor recurrence occurred in three out of 10 (33%) dogs in this sample (patients 1, 4, and 6) after D52. Two of these patients (1 and 4) also had MCT metastasis after D52, received chemotherapy with vinblastine or lomustine, and died of MCT-related causes. Patient 6 was reoperated and died of causes unrelated to MCT. Three out of 10 dogs (33%) in this sample died of causes unrelated to MCT, as follows: gastroenteritis (patient 6), skin lymphoma (patient 3), and primary lung cancer (patient 2). Five out of 10 dogs (50%) remain free of recurrence or metastasis to date (Table 4).
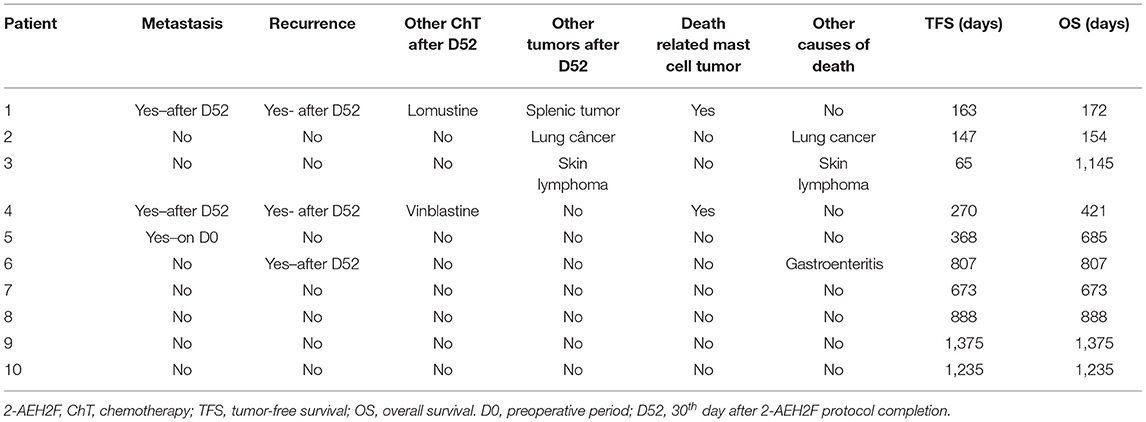
Table 4. Progression of dogs submitted to treatment with 2-AEH2F.
The mean TFS and OS corresponded to 599.1 ± 469 and 755.5 ± 423.5 days, respectively (Figure 1).
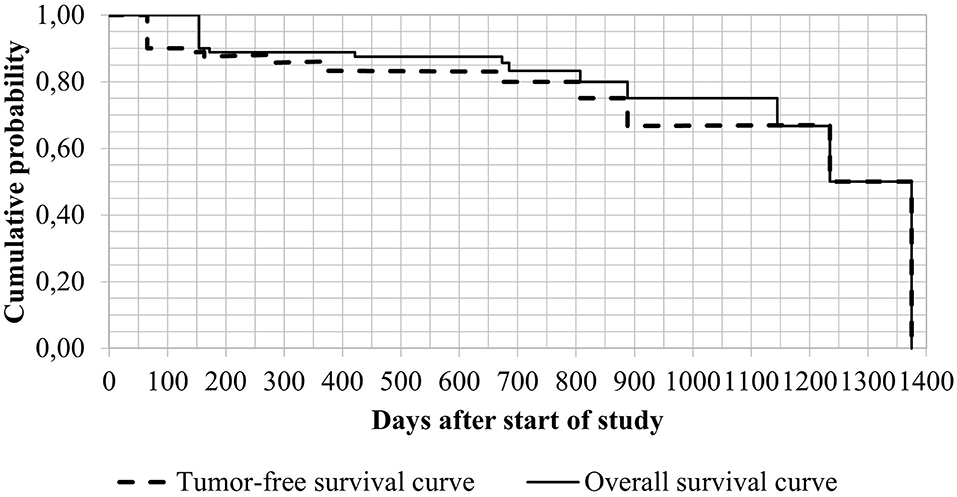
Figure 1. Kaplan-Meier survival curves of patients treated with 2-AEH2F.
Statistics
Laboratory variables other than red blood cell count, hemoglobin level, and platelet count did not differ significantly between time points in this study (Friedman test). However, when the three statistically significant variables were analyzed using the Wilcoxon test, sometime points tended to stand out (p values near αBonf = 0.005). As regards confidence intervals and respective means, the mean values of each variable did not vary across time points (Tables 5, 6).
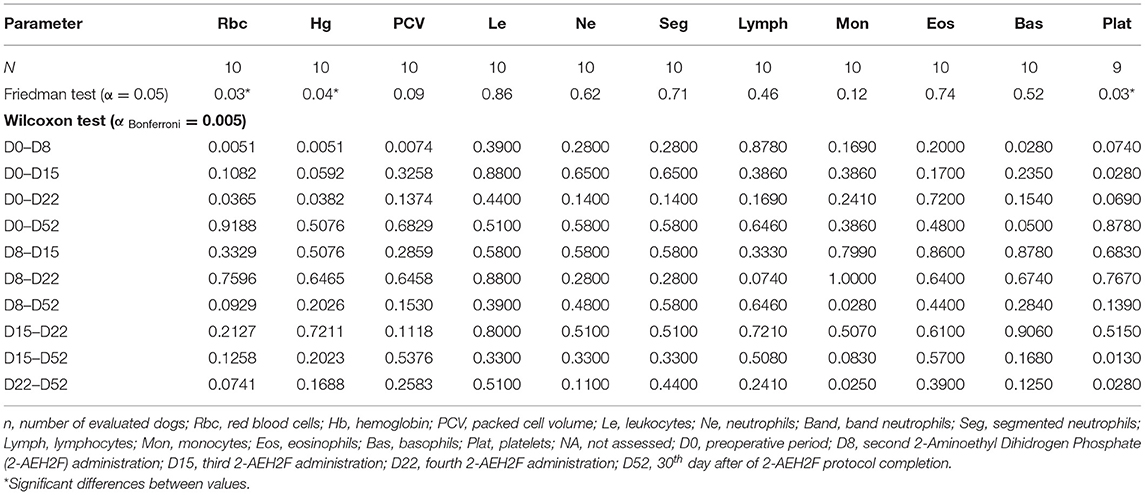
Table 5. Complete blood count parameters and respective p values (Friedman and Wilcoxon tests).
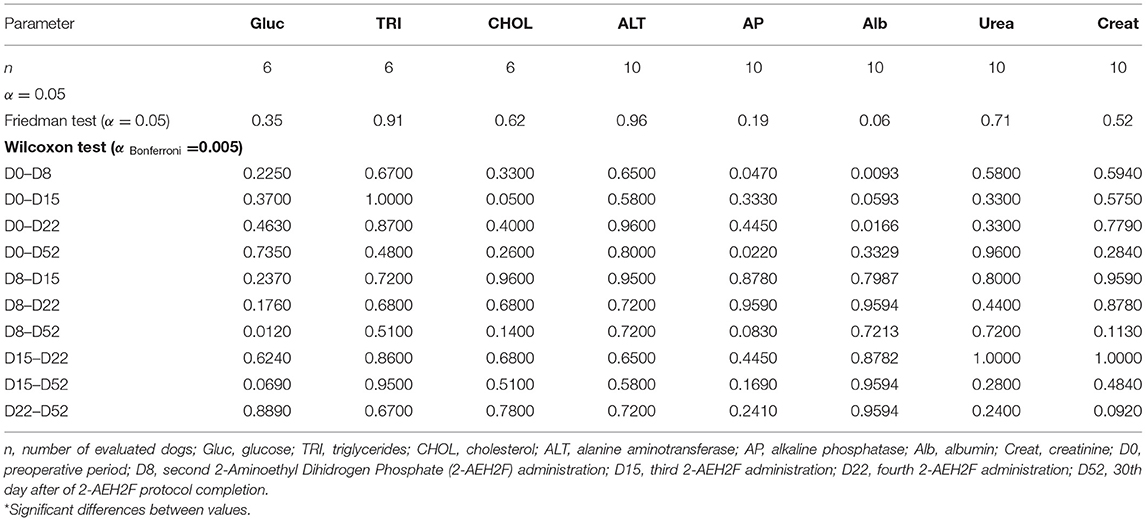
Table 6. Biochemical parameters and respective p values (Friedman and Wilcoxon tests).
Discussion
To the knowledge of the authors, this is the first study on the use of 2-AEH2F in dogs with MCT and has demonstrated its safety in the species, but low efficacy in MCT with poor immunohistochemical prognostic factors.
In this research, weekly intravenous administration of 2-AEH2F solution at 70 mg/kg doses did not induce adverse events or relevant laboratory changes in treated patients. Gastrointestinal signs and fever associated with chemotherapeutic agents such as vinblastine and lomustine (21, 24, 40–42) were therefore not observed in dogs treated with 2-AEH2F. Also, these dogs did not require ancillary therapy with H2 antagonists, as is often the case in patients undergoing chemotherapy (41).
Laboratory parameter values were not significantly affected by therapy with 2-AEH2F in this study. In contrast, neutropenia, sepsis, liver toxicity and azotemia have been widely reported following treatment with drugs such as vinblastine and lomustine (21, 24, 40–43). Despite significant differences in red blood cell count, hemoglobin level and platelet count (Friedman test), it was not possible to determine when these differences occurred (Wilcoxon test), even though p values tended to near 0.005 (αBonf) at some time points (Tables 5, 6). Small sample size may have interfered with this analysis. Laboratory toxicity grade in dogs in this sample was not correlated with the target agent (grades 1 and 2 in most cases, with only one dog presenting with grade 3 lymphocytic toxicity or uremia) (39) (Tables 2, 3). Among the indices that reached grade 3 toxicity in two patients, lymphopenia may be related to the stress situation and uremia alone may reflect dehydration. Therefore, red blood cell count, hemoglobin level and platelet count differences were not clinically relevant.
Antineoplastic phospholipids have been shown to affect cellular cholesterol efflux (42, 43). The mechanism involves structural modifications to the ATP-binding cassette transporter 1 (ABCA1) that mediates the unidirectional efflux of cellular phospholipid to lipid-poor apolipoprotein A-I and other apolipoproteins (44). Still, the mean and the median serum total cholesterol and triglyceride levels remained unchanged in patients treated with 2-AEH2F in this research.
In this study, metastasis and tumor recurrence were documented in 2/10 and 3/10 of dogs treated with 2-AEH2F, respectively. However, two out of three dogs presenting with recurrence were the same dogs who had metastasis (i.e., no more than 3/10 of patients had tumor recurrence overall). Of patients presenting with MCT metastasis or recurrence after D52, three had pattern II or III in KIT stain evaluation and two had ki67 expression over 23%. These findings are thought to be correlated with poor prognostic factors (15, 18) (Table 1) and may have interfered with the effects of 2-AEH2F treatment on TFS in these cases. In remaining patients, KIT staining pattern and Ki67 expression patterns were not indicative of poor prognosis (pattern I and <23%, respectively) (15, 18). Lack of metastasis or recurrence in these patients may therefore not have reflected therapeutic effects of 2-AEH2F. In this study two out of three dogs that developed recurrence or metastasis had grade II (low grade) tumors. Therefore, histological classification of MCT into two or three grades (according to cell differentiation) did not correlate with TFS or OS, as previously reported (6, 45, 46). However, these patients had compromised surgical margins. Low tumor recurrence rates (7%) have been reported in patients with compromised surgical margins submitted to adjuvant therapy with vinblastine and prednisone (40). In this study, 2-AEH2F was not able to prevent tumor cell dissemination in cases with positive margins.
Half (50%; n = 5) of dogs treated with 2-AEH2F in this trial went into remission and remain in remission to date. This remission rate is higher than rates reported in dogs treated with lomustine alone or a combination of vinblastine and lomustine (5 and 25%, respectively) (43), but lower than rates reported following treatment with vinblastine alone (71.4%) (41). Tumor free survival of dogs treated with 2-AEH2F in this study (755 days; minimum of 154 and maximum of 1,375 days) (Figure 1) was longer compared to TFS reported following adjuvant treatment with lomustine (122; 42–347 days) (21), vinblastine and prednisone (304; 37–1,964 days, 322 days and 241.5; 10–1,521 days) (40, 41, 44) or toceranib and prednisone (159; 20–990 days) (44). As in this study, a different one reported TFS of 211 days in dogs developing metastasis following surgical resection and treatment with a combination of vinblastine and prednisone, whereas those not developing metastasis after similar treatment achieved TFS of 757 days (41). Tumor-free survival and tumor remission in this study was longer or similar to TFS data reported in literature. However, the lack of poor prognostic factors (Ki67 <23% and KIT staining pattern I or II) (15, 18) in patients achieving complete remission in this sample may have contributed to longer survival. Longer TFS has been recently reported in dogs with free surgical margins compared to dogs with compromised surgical margins submitted to treatment with vinblastine (893; 70–893 days and 181; 70–548 days, respectively) (20).
Development of new tumors unrelated to MCT after D52 (skin lymphoma and primary lung cancer, respectively) in two dogs suggests 2-AEH2F did not prevent other neoplastic conditions in these patients (Table 4). New tumor growth has also been reported in dogs submitted to chemotherapy with lomustine (24).
The small sample size is a limitation of this study. Also, lack of studies investigating serum 2-AEH2F levels and urinalysis in treated patients and pharmacokinetic aspects of this drug precluded more accurate characterization of the product. Finally, the fact that not all tumors were amenable to immunohistochemical analysis may have interfered with findings in some cases.
In conclusion, intravenous administration of 2-AEH2F at doses and intervals described in this study was thought to be safe in dogs. However, treatment with 2-AEH2F alone was not deemed sufficiently effective to prevent tumor recurrence, new tumor growth or metastasis in cases of canine MCT with poor immunohistochemical prognostic factors. Further studies are warranted to support the use of 2-AEH2F for canine MCT, considering the high safety levels and ease of administration observed in this trial. Based on our results, 2-AEH2F can be investigated as a treatment in association with other forms of therapy for MCT or other types of tumors in canine species.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The animal study was reviewed and approved by Ethics Committee on Animal Use of the School of Veterinary Medicine and Animal Science of University of São Paulo (São Paulo - Brazil). Protocol number 9825270116. Written informed consent was obtained from the owners for the participation of their animals in this study.
Author Contributions
EJ, SM, DM, and JM conceived the study and designed the overall study design. EJ analyzed the data and wrote the paper with support of all authors. EJ and SM diagnosed and treated the dogs and provided all relevant data. AA conducted the anesthetic procedures. JM conducted the laboratory tests. CL conducted the ultrasound exams. BC performed the immunohistochemical tests. HS performed the statistical analysis. All authors critically revised the manuscript, read and approved the final manuscript.
Funding
This study was partially funded by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank Chemistry and Polymer Technology Laboratory of University of São Paulo (USP- São Carlos, Brazil), the Clinical Laboratory of Veterinary Hospital (HOVET) of the School of Veterinary Medicine and Animal Science of the University of São Paulo (FMVZ-USP, São Paulo - Brazil) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
Abbreviations
2-AEH2F, 2-Aminoethyl Dihydrogen Phosphate; ALT, Alanine aminotransferase; AP, Alkaline phosphatase; HPLC, High performance liquid chromatography; MCT, Canine mast cell tumors; OS, overall survival; PE, Phosphoethanolamine; TFS, tumor-free survival.
References
1. Finnie JW, Bostock DE. Skin neoplasia in dogs. Aust Vet J. (1979) 55:602–4. doi: 10.1111/j.1751-0813.1979.tb07068.x
2. Misdorp W. Mast cells and canine mast cell tumours. A review. Vet Q. (2004) 26:156–69. doi: 10.1080/01652176.2004.9695178
3. Macy DW. Canine mast cell tumors. Vet Clin North Am Small Anim Pract. (1985) 15:783–803. doi: 10.1016/S0195-5616(85)50036-4
4. Murphy S, Sparkes AH, Blunden AS, Brearley MJ, Smith KC. Effects of stage and number of tumours on prognosis of dogs with cutaneous mast cell tumours. Vet Rec. (2006) 158:287–91. doi: 10.1136/vr.158.9.287
5. Kiupel M, Webster JD, Bailey KL, Best S, DeLay J, Detrisac CJ, et al. Proposal of a 2-tier histologic grading system for canine cutaneous mast cell tumors to more accurately predict biological behavior. Vet Pathol. (2011) 48:147–55. doi: 10.1177/0300985810386469
6. Patnaik AK, Ehler WJ, MacEwen EG. Canine cutaneous mast cell tumor: morphologic grading and survival time in 83 dogs. Vet Pathol. (1984) 21:469–74. doi: 10.1177/030098588402100503
7. Camus MS, Priest HL, Koehler JW, Driskell EA, Rakich PM, Ilha MR, et al. Cytologic criteria for mast cell tumor grading in dogs with evaluation of clinical outcome. Vet Pathol. (2016) 53:1117–23. doi: 10.1177/0300985816638721
8. Newman SJ, Mrkonjich L, Walker KK, Rohrbach BW. Canine subcutaneous mast cell tumour: diagnosis and prognosis. J Comp Pathol. (2007) 136:231–9. doi: 10.1016/j.jcpa.2007.02.003
9. Thompson JJ, Pearl DL, Yager JA, Best SJ, Coomber BL, Foster RA. Canine subcutaneous mast cell tumor: characterization and prognostic indices. Vet Pathol. (2011) 48:156–68. doi: 10.1177/0300985810387446
10. Turrel JM, Kitchell BE, Miller LM, Theon A. Prognostic factors for radiation treatment of mast cell tumor in 85 dogs. J Am Vet Med Assoc. (1988) 193:936–40.
11. Bostock DE. The prognosis following surgical removal of mastocytomas in dogs. J Small Anim Pract. (1973) 14:27–41. doi: 10.1111/j.1748-5827.1973.tb06891.x
12. Thamm DH, Mauldin EA, Vail DM. Prednisone and vinblastine chemotherapy for canine mast cell tumor−41 cases (1992-1997). J Vet Intern Med. (1999) 13:491–7. doi: 10.1111/j.1939-1676.1999.tb01468.x
13. Mullins MN, Dernell WS, Withrow SJ, Ehrhart EJ, Thamm DH, Lana SE. Evaluation of prognostic factors associated with outcome in dogs with multiple cutaneous mast cell tumors treated with surgery with and without adjuvant treatment: 54 cases (1998-2004). J Am Vet Med Assoc. (2006) 228:91–5. doi: 10.2460/javma.228.1.91
14. Jark PC, Mundin DBP, de Carvalho M, Ferioli RB, Anai LA, Marchi FA, et al. Genomic copy number variation associated with clinical outcome in canine cutaneous mast cell tumors. Res Vet Sci. (2017) 111:26–30. doi: 10.1016/j.rvsc.2016.11.009
15. Webster JD, Kiupel M, Kaneene JB, Miller R, Yuzbasiyan-Gurkan V. The use of KIT and tryptase expression patterns as prognostic tools for canine cutaneous mast cell tumors. Vet Pathol. (2004) 41:371–7. doi: 10.1354/vp.41-4-371
16. Fonseca-Alves CE, Bento DD, Torres-Neto R, Werner J, Kitchell B, Laufer-Amorim R. Ki67/KIT double immunohistochemical staining in cutaneous mast cell tumors from Boxer dogs. Res Vet Sci. (2015) 102:122–6. doi: 10.1016/j.rvsc.2015.08.007
17. Simoes JP, Schoning P, Butine M. Prognosis of canine mast cell tumors: a comparison of three methods. Vet Pathol. (1994) 31:637–47. doi: 10.1177/030098589403100602
18. Maglennon GA, Murphy S, Adams V, Miller J, Smith K, Blunden A, et al. Association of Ki67 index with prognosis for intermediate-grade canine cutaneous mast cell tumours. Vet Comp Oncol. (2008) 6:268–74. doi: 10.1111/j.1476-5829.2008.00168.x
19. Preziosi R, Sarli G, Paltrinieri M. Prognostic value of intratumoral vessel density in cutaneous mast cell tumors of the dog. J Comp Pathol. (2004) 130:143–51. doi: 10.1016/j.jcpa.2003.10.003
20. Olsen JA, Thomson M, O'Connell K, Wyatt K. Combination vinblastine, prednisolone and toceranib phosphate for treatment of grade II and III mast cell tumours in dogs. Vet Med Sci. (2018) 4:237–51. doi: 10.1002/vms3.106
21. Rassnick KM, Moore AS, Williams LE, London CA, Kintzer PP, Engler SJ, et al. Treatment of canine mast cell tumors with CCNU (lomustine). J Vet Intern Med. (1999) 13:601–5. doi: 10.1111/j.1939-1676.1999.tb02217.x
22. Taylor F, Gear R, Hoather T, Dobson J. Chlorambucil and prednisolone chemotherapy for dogs with inoperable mast cell tumours: 21 cases. J Small Anim Pract. (2009) 50:284–9. doi: 10.1111/j.1748-5827.2009.00732.x
23. Hahn KA, Ogilvie G, Rusk T, Devauchelle P, Leblanc A, Legendre A, et al. Masitinib is safe and effective for the treatment of canine mast cell tumors. J Vet Intern Med. (2008) 22:1301–9. doi: 10.1111/j.1939-1676.2008.0190.x
24. Hosoya K, Kisseberth WC, Alvarez FJ, Lara-Garcia A, Beamer G, Stromberg PC, et al. Adjuvant CCNU (lomustine) and prednisone chemotherapy for dogs with incompletely excised grade 2 mast cell tumors. J Am Anim Hosp Assoc. (2009) 45:14–8. doi: 10.5326/0450014
25. Bavcar S, de Vos J, Kessler M, de Fornel P, Buracco P, Murphy S, et al. Combination toceranib and lomustine shows frequent high grade toxicities when used for treatment of non-resectable or recurrent mast cell tumours in dogs: a European multicentre study. Vet J. (2017) 224:1–6. doi: 10.1016/j.tvjl.2017.04.010
26. Alderliesten MC, Klarenbeek JB, van der Luit AH, van Lummel M, Jones DR, Zerp S, et al. Phosphoinositide phosphatase SHIP-1 regulates apoptosis induced by edelfosine, Fas ligation and DNA damage in mouse lymphoma cells. Biochem J. (2011) 440:127–35. doi: 10.1042/BJ20110125
27. Ellison DW, Beal MF, Martin JB. Phosphoethanolamine and ethanolamine are decreased in Alzheimer's disease and Huntington's disease. Brain Res. (1987) 417:389–92. doi: 10.1016/0006-8993(87)90471-9
28. Martens S, Nakamura S, Yoshimori T. Phospholipids in autophagosome formation and fusion. J Mol Biol. (2016) 428:4819–27. doi: 10.1016/j.jmb.2016.10.029
29. van der Luit AH, Vink SR, Klarenbeek JB, Perrissoud D, Solary E, Verheij M, et al. A new class of anticancer alkylphospholipids uses lipid rafts as membrane gateways to induce apoptosis in lymphoma cells. Mol Cancer Ther. (2007) 6:2337–45. doi: 10.1158/1535-7163.MCT-07-0202
30. Emoto K, Umeda M. An essential role for a membrane lipid in cytokinesis. Regulation of contractile ring disassembly by redistribution of phosphatidylethanolamine. J Cell Biol. (2000) 149:1215–24. doi: 10.1083/jcb.149.6.1215
31. Emoto K, Kobayashi T, Yamaji A, Aizawa H, Yahara I, Inoue K, et al. Redistribution of phosphatidylethanolamine at the cleavage furrow of dividing cells during cytokinesis. Proc Natl Acad Sci U S A. (1996) 93:12867–72. doi: 10.1073/pnas.93.23.12867
32. Ferreira AK, Meneguelo R, Neto SC, Chierice GO, Maria DA. Synthetic phosphoethanolamine induces apoptosis through Caspase-3 pathway by decreasing expression of Bax/Bad protein and changes cell cycle in melanoma. J Cancer Sci Ther. (2011) 3:53–9. doi: 10.4172/1948-5956.1000058
33. Ferreira AK, Santana-Lemos BAA, Rego EM, Filho OMR, Chierice GO, Maria DA. Synthetic phosphoethanolamine has in vitro and in vivo anti-leukemia effects. Br J Cancer. (2013) 109:2819–28. doi: 10.1038/bjc.2013.510
34. Luna AC de L, Saraiva GKV, Chierice GO, Hesse H, Maria DA. Antiproliferative and proapoptotic effects of DODAC/synthetic phosphoethanolamine on hepatocellular carcinoma cells. BMC Pharmacol Toxicol. (2018) 19:44. doi: 10.1186/s40360-018-0225-2
35. Ferreira AK, Meneguelo R, Pereira A, Filho OMR, Chierice GO, Maria DA. Synthetic phosphoethanolamine induces cell cycle arrest and apoptosis in human breast cancer MCF-7 cells through the mitochondrial pathway. Biomed Pharmacother. (2013) 67:481–7. doi: 10.1016/j.biopha.2013.01.012
36. Ferreira AK, Meneguelo R, Pereira A, Mendonca Filho OR, Chierice GO, Maria DA. Anticancer effects of synthetic phosphoethanolamine on Ehrlich ascites tumor: an experimental study. Anticancer Res. (2012) 32:95–104.
37. Ferreira AK, Freitas VM, Levy D, Ruiz JLM, Bydlowski SP, Rici REG, et al. Anti-angiogenic and anti-metastatic activity of synthetic phosphoethanolamine. PLoS ONE. (2013) 8:e57937. doi: 10.1371/journal.pone.0057937
38. de Castro PF, Maria DA, de Campos Fonseca Pinto ACB, Patricio GCF, Matera JM. Local tumour response to neoadjuvant therapy with 2-aminoethyl dihydrogen phosphate in dogs with soft tissue sarcoma. Vet Med Sci. (2022) 8:990–1000. doi: 10.1002/vms3.757
39. LeBlanc AK, Atherton M, Bentley RT, Boudreau CE, Burton JH, Curran KM, et al. Veterinary Cooperative Oncology Group-Common Terminology Criteria for Adverse Events (VCOG-CTCAE v2) following investigational therapy in dogs and cats. Vet Comp Oncol. (2021) 19:311–52. doi: 10.1111/vco.12677
40. Davies DR, Wyatt KM, Jardine JE, Robertson ID, Irwin PJ. Vinblastine and prednisolone as adjunctive therapy for canine cutaneous mast cell tumors. J Am Anim Hosp Assoc. (2004) 40:124–30. doi: 10.5326/0400124
41. Hayes A, Adams V, Smith K, Maglennon G, Murphy S. Vinblastine and prednisolone chemotherapy for surgically excised grade III canine cutaneous mast cell tumours. Vet Comp Oncol. (2007) 5:168–76. doi: 10.1111/j.1476-5829.2007.00135.x
42. Vickery KR, Wilson H, Vail DM, Thamm DH. Dose-escalating vinblastine for the treatment of canine mast cell tumour. Vet Comp Oncol. (2008) 6:111–9. doi: 10.1111/j.1476-5829.2007.00147.x
43. Cooper M, Tsai XR, Bennett P. Combination CCNU and vinblastine chemotherapy for canine mast cell tumours: 57 cases. Vet Comp Oncol. (2009) 7:196–206. doi: 10.1111/j.1476-5829.2009.00190.x
Keywords: canine, chemotherapy, antineoplastic phospholipids, immunohistochemistry, toxicity
Citation: Januário EV, Melo SR, Maria DA, Lorigados CAB, Ambrósio AM, Kogika MM, Cogliati B, Shimozako HJ and Matera JM (2022) Tolerability and Effects of 2-Aminoethyl Dihydrogen Phosphate in Dogs With Mast Cell Tumors. Front. Vet. Sci. 9:898077. doi: 10.3389/fvets.2022.898077
Received: 16 March 2022; Accepted: 07 June 2022;
Published: 12 July 2022.
Edited by:
Benito Soto-Blanco, Federal University of Minas Gerais, BrazilReviewed by:
Alessandro Poli, University of Pisa, ItalyTara Piech, Zoetis Reference Laboratories, United States
Copyright © 2022 Januário, Melo, Maria, Lorigados, Ambrósio, Kogika, Cogliati, Shimozako and Matera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eric Vieira Januário, ZXJpYy52aWVpcmFAYWx1bW5pLnVzcC5icg==