
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Vet. Sci., 07 July 2022
Sec. Veterinary Epidemiology and Economics
Volume 9 - 2022 | https://doi.org/10.3389/fvets.2022.877534
This article is part of the Research TopicAdvancing the Development and Implementation of Regional, National Tuberculosis Control Programs in Livestock in Africa, Asia, and Latin AmericaView all 10 articles
 Robert F. Kelly1*
Robert F. Kelly1* Lina Gonzaléz Gordon1
Lina Gonzaléz Gordon1 Nkongho F. Egbe2
Nkongho F. Egbe2 Emily J. Freeman1
Emily J. Freeman1 Stella Mazeri1
Stella Mazeri1 Victor N. Ngwa3
Victor N. Ngwa3 Vincent Tanya4
Vincent Tanya4 Melissa Sander5
Melissa Sander5 Lucy Ndip6
Lucy Ndip6 Adrian Muwonge1Kenton L. Morgan7
Adrian Muwonge1Kenton L. Morgan7 Ian G. Handel1
Ian G. Handel1 Barend M. de C. Bronsvoort1
Barend M. de C. Bronsvoort1The interferon-gamma (IFN-γ) assay and single comparative cervical skin test (SCITT) are used to estimate bovine tuberculosis (bTB) prevalence globally. Prevalence estimates of bTB, caused by Mycobacterium bovis, are poorly quantified in many Sub-Saharan African (SSA) cattle populations. Furthermore, antemortem diagnostic performance can vary at different stages of bTB pathogenesis and in different cattle populations. In this study, we aim to explore the level of agreement and disagreement between the IFN-γ assay and SCITT test, along with the drivers for disagreement, in a naturally infected African cattle population. In, 2013, a pastoral cattle population was sampled using a stratified clustered cross-sectional study in Cameroon. A total of 100 pastoral cattle herds in the North West Region (NWR) and the Vina Division (VIN) were sampled totalling 1,448 cattle. Individual animal data and herd-level data were collected, and animals were screened using both the IFN-γ assay and SCITT. Serological ELISAs were used to detect exposure to immunosuppressing co-infections. Agreement analyses were used to compare the performance between the two bTB diagnostic tests, and multivariable mixed-effects logistic regression models (MLR) were developed to investigate the two forms of IFN-γ assay and SCITT binary disagreement. Best agreement using the Cohen's κ statistic, between the SCITT (>2 mm) and the IFN-γ assay implied a ‘fair-moderate' agreement for the NWR [κ = 0.42 (95%CI: 0.31–0.53)] and ‘poor-moderate' for the VIN [κ = 0.33 (95% CI: 0.18–0.47)]. The main test disagreement was the animals testing positive on the IFN-γ assay and negative by the SCITT. From MLR modeling, adults (adults OR: 7.57; older adults OR = 7.21), females (OR = 0.50), bovine leucosis (OR = 2.30), and paratuberculosis positivity (OR = 6.54) were associated with IFN-γ-positive/SCITT-negative disagreement. Subsets to investigate diagnostic test disagreement for being SCITT-positive and IFN-γ-negative also identified that adults (adults OR = 15.74; older adults OR = 9.18) were associated with IFN-γ-negative/SCITT-positive disagreement. We demonstrate that individual or combined use of the IFN-γ assay and SCITT can lead to a large variation in bTB prevalence estimates. Considering that animal level factors were associated with disagreement between the IFN-γ assay and SCITT in this study, future work should further investigate their impact on diagnostic test performance to develop the approaches to improve SSA prevalence estimates.
Bovine tuberculosis is a chronic disease of cattle, caused by Mycobacterium bovis, and is an important zoonosis associated with close interaction with cattle or consumption of raw dairy products (1). Close contact between cattle and people is commonplace in livestock rearing communities in Sub-Saharan Africa (SSA). Consequently, it is vital to understand the potential direct impacts of bTB on livestock health as well as its public health risks in such communities. A key metric in understanding bTB epidemiology is to quantify the burden of disease in cattle by estimating bTB prevalence. However, the prevalence estimates in the live animals rely on the use of diagnostic tests that are imperfect. Identifying characteristic TB lesion pathology has been used to describe the epidemiology of bTB in abattoirs in many African countries (2). Specificity of lesion detection is high (>95%) and can be improved further with culture from lesions or using molecular techniques such as PCR to characterise M. bovis bacilli (3, 4). However, identification of lesions is not a gold-standard diagnostic test, as its sensitivity can be low (28.5%), particularly in the early stages of infection (5) and can only be used in cattle postmortem.
Antemortem diagnostic tests for bTB are based upon measuring the specific aspects of the immune response to M. bovis antigens (2, 6, 7). Mycobacterium bovis infections predominately stimulate cell-mediated immunity (CMI) responses in cattle (8–10); therefore, antemortem diagnostic tests have tended to focus on detecting this CMI response in different formats, including the in vivo tuberculin skin tests known as the single intradermal test (SIT) and single comparative intradermal tuberculin test (SCITT) (2, 6, 11) and the in vitro IFN-γ assay. The SCITT is recognised by the World Organisation for Animal Health (OIE) as the primary diagnostic test for bTB diagnosis (3), with a very high specificity (median: 100%; CrI: 99–100%) (7, 12) but low sensitivity (median: 50.0%; CrI: 26–78%) reported in a recent extensive meta-analysis (13). As a result, there is an extremely high risk of infected animals testing negative (i.e., false-negative animals) resulting in gross underestimation of the bTB prevalence and, when used in control programmes, an increased risk of retaining positive animals that may continue to transmit within the herd or to naïve herds when animals are traded. The IFN-γ assay detects the predominant Th1 immune response to M. bovis and experimentally can detect positive animals from 2 weeks post-infection (14). Consequently, the IFN-γ assay is reported to have a higher sensitivity (median: 67%; CrI: 49–82%) than the SCITT with a slightly lower specificity (median: 98%; CrI: 96–99%) (13). In addition to diagnostic performance, the logistics involved in the use of either test is also important to appreciate when applied to a SSA context. The SCITT requires restraint of the animal and injection of the avian and bovine tuberculin intradermally in the neck. It has the drawbacks of requiring a repeat visit to remeasure the skin after 3 days and good handling facilities to assess skin thickness. This is particularly challenging in the SSA setting because of the absence of cattle identification systems in many SSA countries and the dangers when handling African cattle breeds that are predominately horned. The IFN-γ assay on the other hand requires a single blood sample that can be done from the tail vein. The disadvantage compared to the SCITT is that the IFN-γ assay does require local laboratory facilities to conduct the time-limited cell stimulation and incubation stages followed by the collection of the plasma and an ELISA.
The probability of a diagnostic test correctly classifying animals depends on its sensitivity, specificity, and the underlying true prevalence of the disease in the population. The SCITT and IFN-γ assays measure different aspects of the CMI response (15, 16) and therefore may not detect the same population of bTB-positive cattle. In addition, the performance of the two tests may vary between different cattle populations and, depending on the performance requirements for testing, can be adjusted through changing the diagnostic cut-off value for a positive of either test (16–19). Another approach is the so-called parallel testing, where the combination of being positive on one or both tests has been used to improve overall sensitivity of the testing system (20–22). It is important, given that the SCITT and IFN-γ assays detect the different aspects of the CMI response, to understand why these two tests disagree to better interpret their results in the field. Factors that may lead to test disagreement can be classified into those associated with laboratory method, operator error, or host-related factors. Understanding the impact of host-related factors is of particular interest to understand variation in test performance depending on animal's characteristics. For example, diagnostic tests could be selected, or their interpretation adjusted based on the signalment of individual animals. Host-related factors previously identified include animal age, breed, pregnancy status, and causes of immunosuppression such as co-infections (7). Results from a previous study in Cameroon found that co-infection with Fasciola gigantica reduced the sensitivity of the IFN-γ assay (23), and studies elsewhere highlight a similar impact on SCITT sensitivity with other Fasciola species (24). Other immunosuppressive co-infections may also impact bTB antemortem diagnostic test performance (25–27), such as immunosuppressing viruses or Mycobacterium avium subspecies paratuberculosis (MAP), which have been shown to lead to false-negative results (28). Identifying factors that influence IFN-γ assay and SCITT performance and where disagreement is occurring between tests will highlight the potential challenges using these tests and what adjustments may be needed to improve interpretation of the results.
In this study, we investigate the level of agreement between the IFN-γ assay and the SCITT and host-related factors associated with their diagnostic disagreement. We then compare the impact of their different performances on the prevalence estimates of bTB using the IFN-γ assay, the SCITT and the “parallel” test combination for pastoral cattle populations in Cameroon.
The dataset used for this analysis was a part of a larger study investigating the epidemiology of bTB in Cameroonian cattle populations (29). The study sites were the Northwest Region (NWR) and the Vina Division (VIN) of the Adamawa Region (AR) of Cameroon (Figure 1), previously highlighted as important cattle keeping areas of Cameroon (30). A cross-sectional study was conducted, sampling two pastoralist populations (NWR & VIN) where M. bovis has been confirmed present (30, 31). Sampling was conducted between January–May 2013 in the NWR and September–November 2013 in the VIN, respectively. Pastoralist cattle populations in the NWR and VIN were estimated to be 506,548 and 176,257, respectively, from the Ministry of Livestock, Fisheries and Industrial Agriculture /Ministere de l'Elevage des Peches et Industries Animales (MINEPIA) vaccination records (32). The pastoralist cattle population eligible for sampling were herds listed in vaccination records at 81 ZVSCCs in the NWR and 31 ZVSCCs in the VIN in 2012. There were 5,053 cattle herds in the NWR and 1,927 in the VIN, with a range of 1–215 animals per herd. A population weighted stratified random sample of registered herds was sampled in each of the two study sites. The sample was stratified by sublocation within each administrative area; seven divisions in the NWR and eight subdivisions in the VIN. The number of herds sampled from each sublocation was proportional to the total number of herds within that sublocation. The sample size for this bTB focused project was based on an clustered random sample with an estimated animal level bTB prevalence of ~10%, a within herd variance of 0.15 and between herd variance of 0.01, an average herd size of 70, a relative cost of 12:1 for herd/animal and relative error of ± 15% (Survey Toolbox; AusVet) (33). This gave a target sample size of 15 cattle per herd and 88 herds under the simplifying assumption of perfect test performance. The final sample was 100 herds with 50 at each site (NWR and VIN). Within each herd, the 15 samples were stratified to each of three age classes: young (≥0.5 years and <2 years), adult (≥2 and <5 years), and old (≥5 years). If there were insufficient animals of one age group, additional animals of any age were sampled.
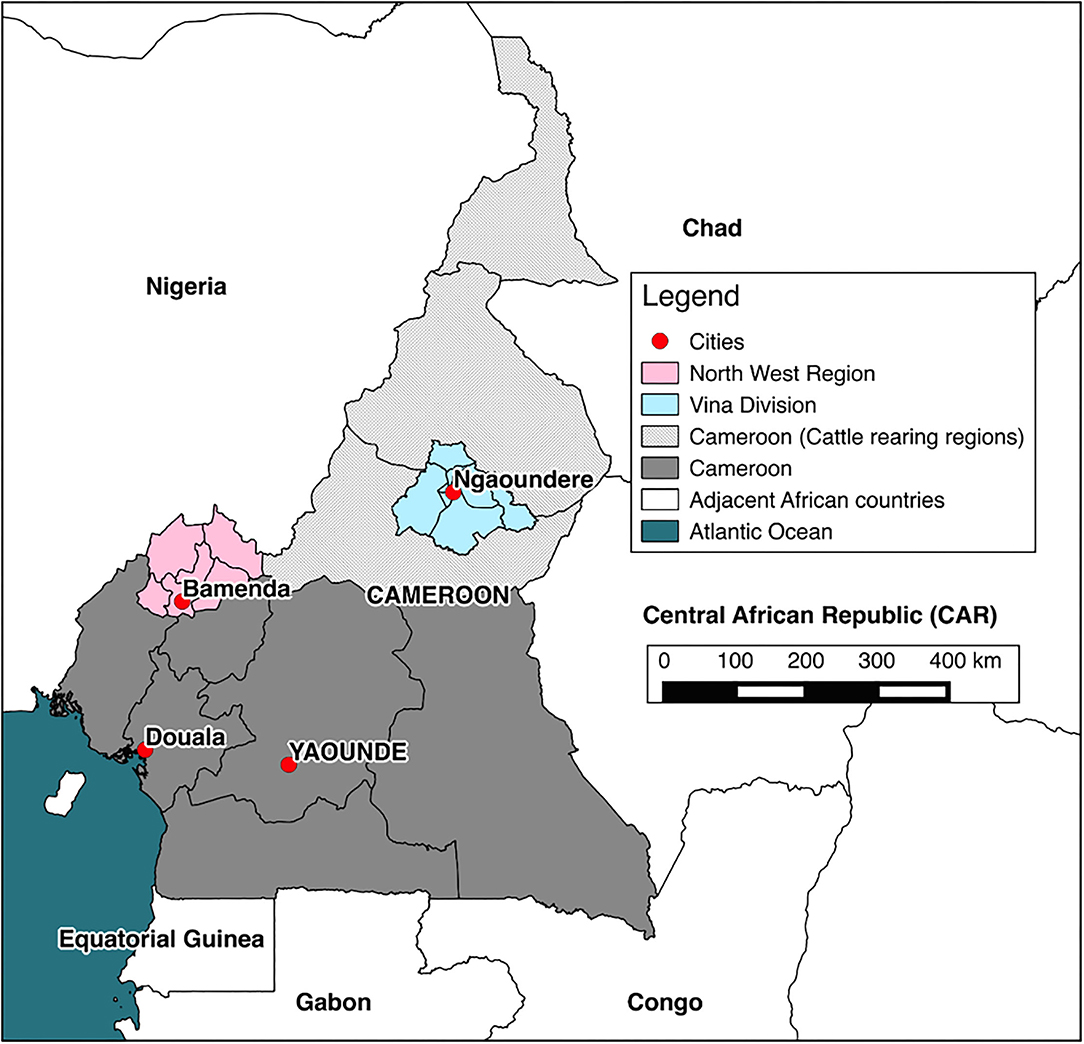
Figure 1. Map of Cameroon. The location of cattle rearing areas (light grey), study sites (pink and blue), and major cities (red).
Pastoral herds were visited and a local translator explained the project to the herdsman in either Foulfulde, Pidgin English, or French. Individuals were asked, in the language in which they were most comfortable, to give verbal consent to participate in the study. The same local translator, who was unaware of animal disease-status, selected 15 animals per herd at random. The animals were identified used disposable numbered Tyvek® wrist bands on the forelimb and horn on the side the SCITT would be conducted on. All sampled animals were then examined by the same veterinarian, with data recorded at an individual animal level to accompany samples. These included signalment [sex, age by dentition score (DS), breed, and body condition score (BCS)]. The method for ageing by DS and BCS was carried out on 5-point scales (34). “Improved” breed cattle were defined as cattle that had the phenotypic appearance of mixed Bos indicus breeding. “Exotic” cattle defined as those cattle that had the phenotypic appearance or which were reported by the farmer to be fully or mixed Bos taurus. Plain and heparinised blood samples were collected from the jugular or tail vein. All information was initially recorded on paper forms, which were later transferred into a relational Access database (Microsoft Access®). Unless otherwise stated, all animals sampled were tested using all infectious disease diagnostic tests.
For the IFN-γ assay (20), three aliquots of 1.5 ml of heparinised blood per animal were stimulated with either 15 μl of avian PPD, bovine PPD (Prionics® Lelystad Tuberculin PPD), or PBS and then incubated for 24 h at 37°C within 8 h of sampling (usually <3 h). Incubated blood was centrifuged at 300 g for 10 min, and then, three plasma aliquots per animal were stored at −20°C in a portable travel freezer. Electrical supplies were maintained by mains electricity, portable generators, or from vehicle batteries where necessary in the field. Plasma samples were transported at −20°C to Laboratory of Emerging Infectious Diseases (LEID), University of Buea, Cameroon, where the IFN-γ assay ELISA was conducted. Prior to starting the protocol, reagents were reconstituted and samples were allowed to reach room temperature (22 +/-5°C). The avian PPD, bovine PPD, and PBS-stimulated plasma samples were diluted 1:1 with dilution buffer. Diluted plasma samples were added to the pre-coated 96 well plate along with duplicates of kit positive, negative, and PBS controls. The 96 well plate was incubated on a microplate shaker, at 600 rpm for 60 min at 22 +/-5°C, and once complete, the plate washed 6 times with wash buffer. About 100 μl of conjugate was added to the 96 well plate incubated for 60 min and washed as previous. About 100 μl of enzyme substrate was added to the 96 well plate incubated for 30 min as previous in the dark. Finally, 50 μl of stopping solution was then added to the 96 well plate and read at 450 nm using an automated microplate reader (Thermoscientific® Multiskan Go). For interpretation, PBS control ODs were subtracted from corresponding sample ODs. The acceptable averaged negative bovine was <0.13 and positive bovine control was >0.70. For each sample, the difference in OD of the sample stimulated with bovine PPD minus the mean OD of the avian PPD was calculated for interpretation. At standard interpretation, as per commercial kit instructions, animals with a bovine PPD plasma sample of ≥0.1 that of avian PPD and PBS were classed as M. bovis infected.
All SCITTs were performed and interpreted by the same experienced veterinarian (RK) following the standard protocol used in the United Kingdom. At the time of sampling, each animal was appropriately restrained by either casting on the ground or tied up to trees using ropes (Day 0). Left or right side of the cervical neck was used, depending upon accessibility, and ID bands were placed on the leg and/or horn on the same side of the animal. Two areas, approximately 12 cm apart, in the mid-cervical neck had the hair clipped (using scissors) to mark the injection sites. The skin thickness was measured using skin callipers and recorded for each site prior to injection. A total of two multidose automatic syringes (McLintock®) were used to inject 0.1 ml of avian and bovine PPD (Prionics® Lelystad Tuberculin PPD) intradermally in the dorsal and ventral sites, respectively. The injection site was palpated to confirm whether PPDs were injected intradermally. Multidose automatic syringe needles were swabbed with surgical spirit between individual cattle. On a return visit, approximately 72 h later (Day 3), the skin thickness of the two injection sites was remeasured using skin callipers. The difference in bovine and avian PPD skin measurements was calculated for each bovine to determine whether the animal is infected with M. bovis. First, the difference between the skin measurement of PPD injection sites on days 0 and 3 was calculated. Then, the difference between bovine and avian was calculated:
• Avian skin reaction difference (A) = skin thickness day 3 – skin thickness day 0 (mm)
• Bovine skin reaction difference (B) = skin thickness day 3 – skin thickness day 0 (mm)
• PPD skin reaction difference = B–A
Second, clinical signs at the injection site (e.g., oedema) were recorded. The results for each animal were then interpreted at two cut-off values. At severe interpretation, animals with a PPD skin reaction difference of >2.0 mm +/- clinical signs at the injection site indicated the presence of M. bovis infection. At standard interpretation, a PPD skin reaction difference of >4.0 mm +/- clinical signs at the injection site indicated the presence of M. bovis infection. These two cut-off values were then evaluated in subsequent agreement analysis.
After collection, all serum samples were heat treated at 56°C for 120 min and stored at −20 oC until tested. Serum samples were then tested for exposure to various infections using serological ELISAs. For the F. gigantica antibody ELISA (35), immulon-2 ELISA 96-well plates were coated with 100 μl of 1 μg/ml F. gigantica E/S antigen in 0.1 M carbonate buffer (pH 9.6). Plates were incubated for 1 h at room temperature and then refrigerated at 2–4°C overnight. Plates were then washed six times (two short washes and one 5-min wash repeated for two times) with pH 7.2 PBS containing 0.05% Tween-20 (PBS-Tween). Each well was blocked with 200 μl of blocking buffer for 1 h at 37°C [4% skimmed powder (Marvel, Premier International Foods®, Spalding UK)] in PBS-Tween. Plates were washed six times, and 100 μl of sera diluted 1:200 in blocking buffer was added to each well. Positive and negative serum controls were added to the plate in duplicate, at the same concentration as the test sera, and incubated at 37°C for 1 h. The plates were again washed, 100 μl of 1:1500 mouse anti-bovine IgG HRP conjugate (Serotec®, UK) in blocking buffer was added, and then, the plates were incubated at 37OC for 1 h. After washing, 100 μl of TMB substrate (acetate buffer pH 5 and tetramethylbenzidine in a methanol-based solution, MAST Diagnostics, Bootle, Merseyside, UK) was added and incubated at room temperature for 20 min in the dark. Finally, 100 μl of stopping solution (10% hydrochloric acid) was added and the colour change measured at 450 nm using an automated microplate reader (Thermoscientific® Multiskan Go). The results were obtained as an optical density (OD) and expressed as a percent positivity value (PPV). For this study, samples PPV <23.4% are considered negative and PPV ≥23.4% are considered positive (35).
Screening for MAP exposure was conducted using the ID.vet Screen® Paratuberculosis Serum Indirect Multi-species ELISA (36). In brief, 10 μl of each serum sample was diluted to 1:10 with the provided dilution buffer. The diluted sample was added to a well on the purified MAP antigen coated microplate and incubated at 21°C for 45 min. The microplate was washed three times with 300 μl of wash solution, and 100 μl of supplied conjugate was added for 30 min at 21°C. Using the same method, the microplate was washed again, and 100 μl of substrate solution was added to each well for 15 min at 21°C. To stop the reaction, 100 μl of stop solution was added to each well and the microplate was read at 450 nm. For a microplate to be considered valid, the mean of the duplicate positive (PC) and negative (NC) controls was calculated. For a microplate to pass, mean PC optical density (OD) needed to be > 0.35 and the mean positive and negative OD ratio (ODPC/ ODNC) needed to be >3. For each sample, the sample to positive ratio (S/P%) was calculated by (ODsample–ODNC) / (ODPC -ODNC) X 100. The manufacturers suggest that samples S/P% ≤ 60% are considered negative; S/P% >60% and <70% are considered doubtful; and S/P% ≥70% are considered positive. For this study, samples S/P% <70% are considered negative and S/P% ≥70% are considered positive.
Screening for bovine leukaemia virus (BLV) exposure was conducted using the ID Screen® BLV Serum Competitive ELISA (37). In brief, 25 μl of each serum sample was diluted to 1:4 with the provided dilution buffer. The diluted sample was added to a well on the BLV gP51 antigen-coated microplate and incubated at 21°C for 45 min. The microplate was washed three times with 300 μl of wash solution, and 100 μl of supplied conjugate was added for 30 min at 21°C. Using the same method, the microplate was washed again, and 100 μl of substrate solution was added to each well for 15 min at 21°C. To stop the reaction, 100 μl of stop solution was added to each well, and the microplate was read at 450 nm. For a microplate to be considered valid, the mean of the duplicate PC and NC was calculated. For a microplate to pass, mean NC OD needed to be > 0.7 and the mean positive and negative OD ratio (ODPC/ ODNC) needed to be >0.3. For each sample, competition percentage (S/N%) was calculated by (ODsample / ODNC) x 100. The manufacturers suggest that samples S/N% ≤ 50% are considered positive; S/N% >50% and <60% are considered doubtful; and S/N% ≥60% are considered negative. For this study, samples S/N% ≤ 50% are considered positive and S/N% >50% are considered negative.
Screening for bovine viral diarrhoea virus (BVDV) exposure was conducted using the ID Screen® BVDV Serum Competitive ELISA (38). In brief, 15 μl of each serum sample was diluted to 1:9 with the provided dilution buffer. The diluted sample was added to a well on the BVDV p 80 antigen-coated microplate and incubated at 37°C for 45 min. The microplate was washed three times with 300 μl of wash solution, and 100 μl of supplied conjugate was added for 30 min at 21°C. Using the same method, the microplate was washed again and 100 μl of substrate solution was added to each well for 15 min at 21°C. To stop the reaction, 100 μl of stop solution was added to each well and the microplate was read at 450 nm. For a microplate to be considered valid, the mean of the duplicate PC and NC was calculated. For a microplate to pass, mean NC OD needed to be > 0.7 and the mean positive and negative OD ratio (ODPC/ ODNC) needed to be >0.3. For each sample, competition percentage (S/N%) was calculated by (ODsample / ODNC) x 100. The manufacturers suggest that samples S/N% ≤ 40% are considered positive; S/N% >40% and ≥50% are considered doubtful; and S/N% >50% are considered negative. For this study, samples S/N% ≤ 40% are considered positive and S/N% >40% are considered negative.
All statistical analyses were performed using packages and functions in R version 3.6.1 (39). Graphics were produced using the ggplot2 package (40). Spatial data were displayed using QGIS 2.2® (41) or tidyverse collection of R packages (42) and shapefiles obtained from the GADM database of Global Administrative Areas (www.gadm.org).
Agreement analyses were in this study to compare the performance between diagnostic as no gold-standard diagnostic tests were available. Agreement was defined as how much two diagnostic tests, which measure the same response, agree with each other (43). In the absence of gold-standard diagnostics, agreement analysis is used in this study to explore the positive cut-off values for the SCITT with continuous results for both tests to be converted to categorical results (e.g., positive and negative). For the IFN-γ assay, ≥0.1 was used as the positive cut-off value compared to the SCITT at >2 mm and >4 mm cut-off by study site. Percentage agreement and Cohen's κ statistic were used to quantify binary agreement between two tests. The agree, kappa2, and rater.bias functions in the irr package (44) were used to calculate percentage agreement and Cohen's κ statistic. Percentage agreement was used as a provisional measure of agreement between two diagnostic tests and was calculated as follows (43):
Percentage agreement does not distinguish agreement between positive or negative diagnostic test results and does not adjust for chance. Consequently, the Cohen's κ statistic was also calculated to determine the level of agreement, beyond chance, between two categorical diagnostic tests (e.g., positive or negative) (45):
Cohen's κ statistic was interpreted as =1 (perfect agreement), 0.81–1 (almost perfect agreement), 0.61–0.8 (substantial agreement), 0.41–0.6 (moderate agreement), 0.21–0.4 (fair agreement), 0.01–0.2 (poor agreement), and ≤ 0 (no agreement) (46). The effect of very low or high prevalence is thought to have a negligible effect on the calculation (44, 47).
The structure of the cross-sectional study design was incorporated into analyses using the svydesign, confint, and svyby functions in the survey package (48). For estimating bTB prevalence using SCITT, IFN-γ, and combined tests, true prevalence (43) was estimated using the epi.prev function in the epiR package (49) for pastoral cattle population by study site. Specific differences in sample statistics were identified by non-overlapping confidence intervals (CI) at 95% level (50).
Multivariable mixed-effects logistic regression (MLR) models were built to investigate the two forms of IFN-γ assay and SCITT binary disagreement using a combined dataset from both study sites, subsetted by the two forms of diagnostic disagreement:
1. IFN-γ assay-positive and SCITT-negative (Figure 2).
a. Model a): Subset of IFN-γ assay (≥0.1)-positive animals, using SCITT (≤ 2 mm) status as the dependent variable (IFN-γ/SCITT: +/- = 1; +/+ = 0).
b. Model b): Subset of SCITT (≤ 2 mm)-negative animals, using IFN-γ assay (≥0.1) status as the dependent variable (SCITT/ IFN-γ: -/+ = 1; -/- = 0).
2. IFN-γ assay-negative and SCITT-positive (Figure 2).
c. Model c): Subset of IFN-γ assay (<0.1)-negative animals, using SCITT (>2 mm) status as the dependent variable (IFN-γ/SCITT: -/- = 0; -/+ = 1).
d. Model d): Subset of SCITT (>2 mm)-positive animals, using IFN-γ assay (<0.1) status as the dependent variable (SCITT/ IFN-γ: +/- = 1; +/+ = 0).
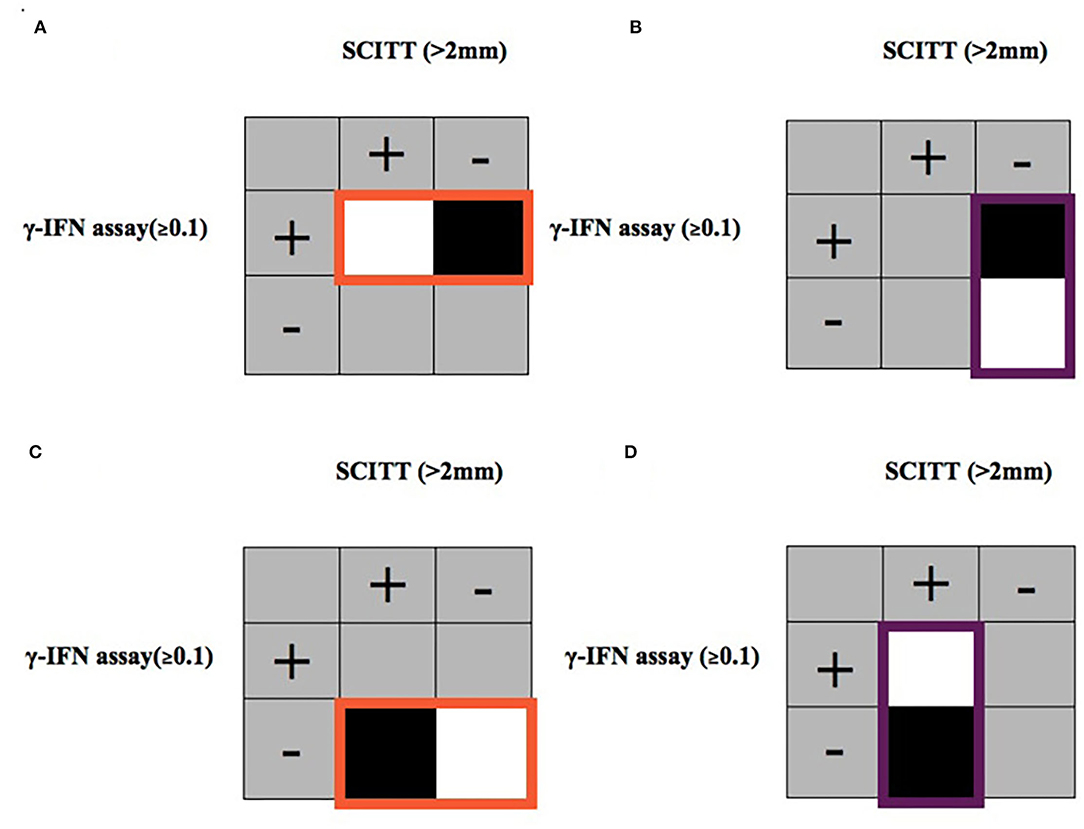
Figure 2. Diagrammatic representation of data subset to investigate two types of test disagreement. 1. IFN-γ assay-positive (≥0.1) and SCITT-negative (≤ 2 mm) using models (A,B). Model (A) Subset of all cattle with a IFN-γ assay-positive response highlighted in orange with SCITT as the dependent variable. Model (B) Subset of all cattle with a SCITT-negative response highlighted in purple with IFN-γ assay as the dependent variable. Black areas indicate “positive” (disparate results) and white areas indicates “negative” (agreeing results) of the dependent variable. 2. IFN-γ assay-negative (<0.1) and SCITT-positive (>2 mm) in pastoral cattle using models (C,D). Model (C) Subset of all cattle with a IFN-γ assay-negative response highlighted in orange with SCITT as the dependent variable. Model (D) Subset of all cattle with a SCITT-positive response highlighted in purple with IFN-γ assay as the dependent variable. Black areas indicate “positive” (disparate results) and white areas indicates “negative” (agreeing results) of the dependent variable.
A number of two subsets of each type of disagreement between the two diagnostic tests were used to produce four disagreement models. The outcome variable was the binary result for the alternative test with the result of interest being the contrary binary result, e.g., subset positive and outcome variable negative. Host-related factors (e.g., age, sex, breed, and evidence of co-infections) were included. Model selection was performed through model averaging; this approach allowed us to generate, rank, and weight several models supporting hypothesised associations to the outcome of interest (disagreement) (51). A set of explanatory variables were included in the global model for each disagreement, and this was the starting point to generate a model set to compare and average. Submodels were generated through the dredge function implemented in the MuMIn package (52). Each submodel was assessed by its AIC (53), and submodels with a Δ AIC ≤ 2 were averaged (54). For all models, herd was included as a random effect. Receiver operating characteristic (ROC) curves were used to assess the capacity of the models to discriminate between agreements and disagreements.
In total, 100 pastoral herds were recruited, 50 in the NWR and 50 in the VIN, with 14–15 cattle sampled per herd. Complete dataset for both tests was available for 750 cattle in NWR and 741 cattle in VIN (n = 748 for IFN-γ assay; n = 741 for SCITT). A detailed summary of animal (55) and herd-level data (29) has been previously published. This study utilises the animal-level dataset, accounting for herd and study site in the analysis where appropriate.
The raw continuous results for the SCITT (difference in skin thickness in mm) and IFN-γ assay (OD difference) stratified by site are presented in Figure 3. The frequency of avian PPD greater than bovine PPD reactions for SCITT (at >2 mm: 1.25%, 95% CI: 0.79–1.97%; at >4 mm: 0.01%, 95% CI: 0.00–0.39%) and IFN-γ (at ≥0.1: 7.11%, 95% CI: 5.90–8.55%) was low. The agreement between the binary two test results, with the SCITT at >2 mm and >4 mm positive cut-off values, is presented in Table 1. The percentage agreements were relatively high but do not adjust for agreement by chance and because of the low apparent prevalence can be misleading, and thus, the Cohen's κ statistic gives a better measure adjusting for chance. The agreement at >2 mm cut-off was slightly higher for the NWR compared to at >4 mm cut-off, but the different cut-offs were identical for the VIN. The scores were relatively low suggesting fair-moderate agreement for the NWR but poor-moderate agreement for the VIN. As the confidence interval for the Cohen's κ statistic overlapped for estimates between the study sites, and previous studies highlighting the use of >2 mm positive cut-off (30), the SCITT >2 mm positive cut-off value was chosen for the remainder of the analysis.
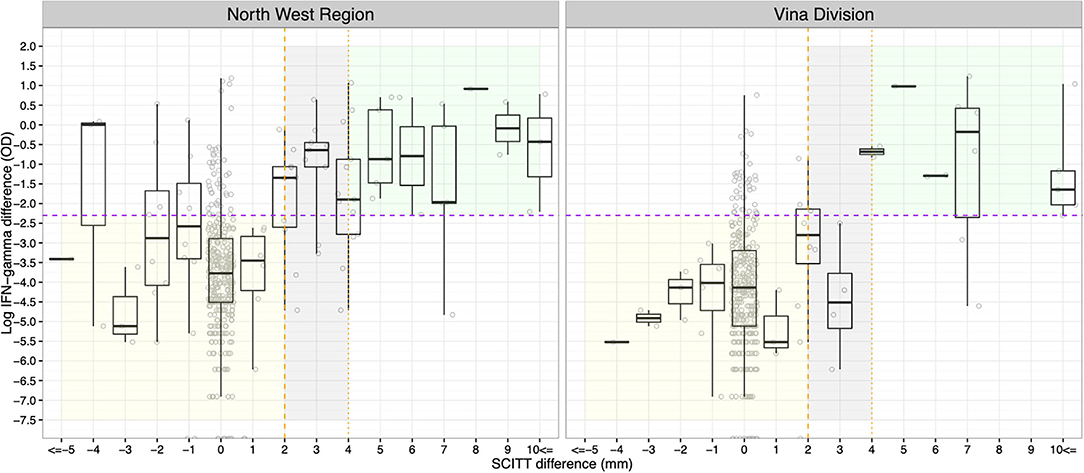
Figure 3. For the IFN-γ assay, results are displayed on a log scale for clarity and ≥0.1 positive cut-off values are shown (horizontal purple dashed line; ln (0.1) = −2.3). For the SCITT >2 mm (vertical orange dashed line) and >4 mm (vertical orange dotted line), positive cut-off values are shown. The green area denotes the test positive cattle for IFN-γ assay (≥0.1) and SCITT (>4 mm). The grey area denotes proportion of additional test positive cattle for IFN-γ assay (≥0.1) and SCITT (≥2 mm). The yellow area denotes test negative cattle for IFN-γ assay (<0.1) and SCITT (≤ 2 mm).
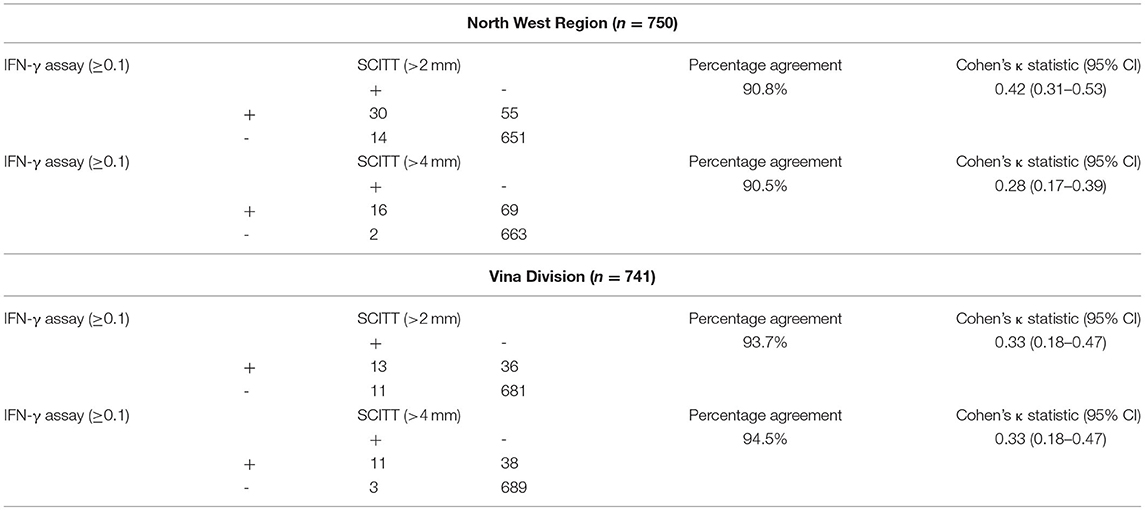
Table 1. Comparisons of agreement and Cohen's κ statistic between IFN-γ assay (≥0.1) and SCITT (>2 mm and >4 mm) for pastoral cattle sampled in the North West Region and Vina Division.
The apparent prevalence estimates between the NWR and VIN are compared in Figures 4, 5; based on the IFN-γ assay (≥0.1), SCITT (>2 mm) and a parallel combination (PC) of the two tests (i.e., positive on either or both tests at the specified cut-offs). The highest estimates were generated when a parallel approach is used, followed by the IFN-γ and SCITT. No significant difference in overall animal-level apparent prevalence was noted between study sites when using any single or PC tests, although the prevalence was consistently lower in the VIN than the NWR (Figure 4). The different tests give quite a different impression of the magnitude in apparent prevalence across administrative areas and herds that are defined as positive (at least 1 positive animal per herd) (Figure 5).
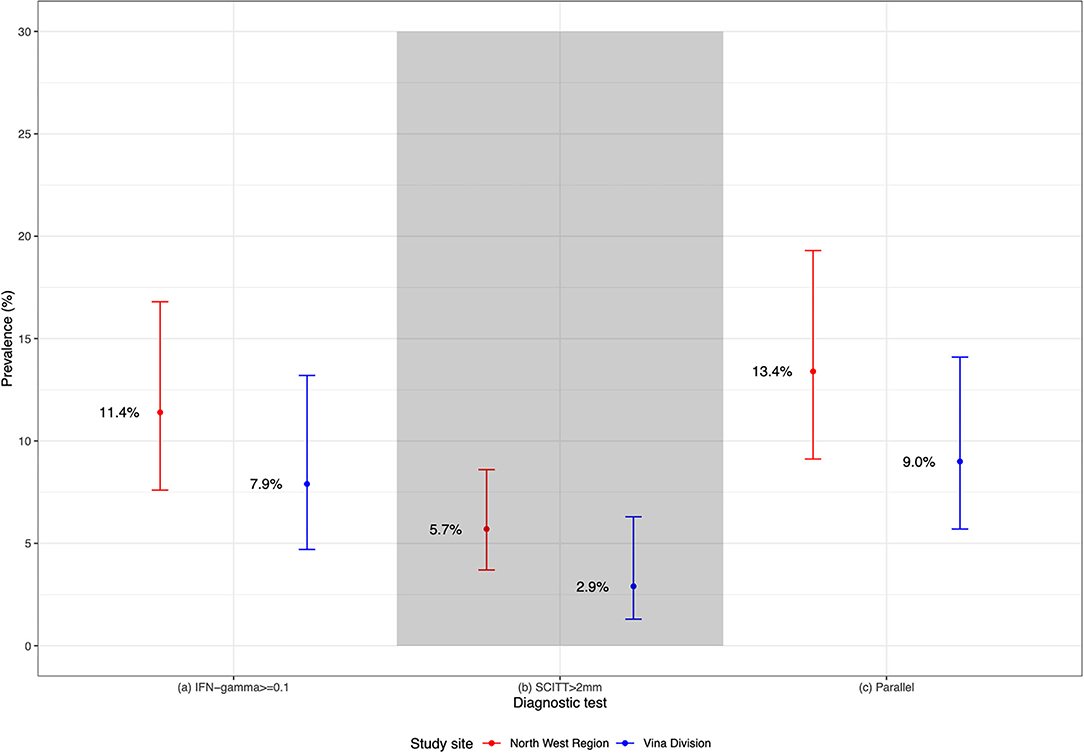
Figure 4. Summary of apparent bTB prevalence, using IFN-γ assay (≥ 0.1), SCITT (>2 mm) and parallel combination testing. IFN-γ assay (≥ 0.1) (NWR n = 750; VIN n = 748); SCITT (>2 mm) and Parallel (NWR n = 750; VIN n = 741).
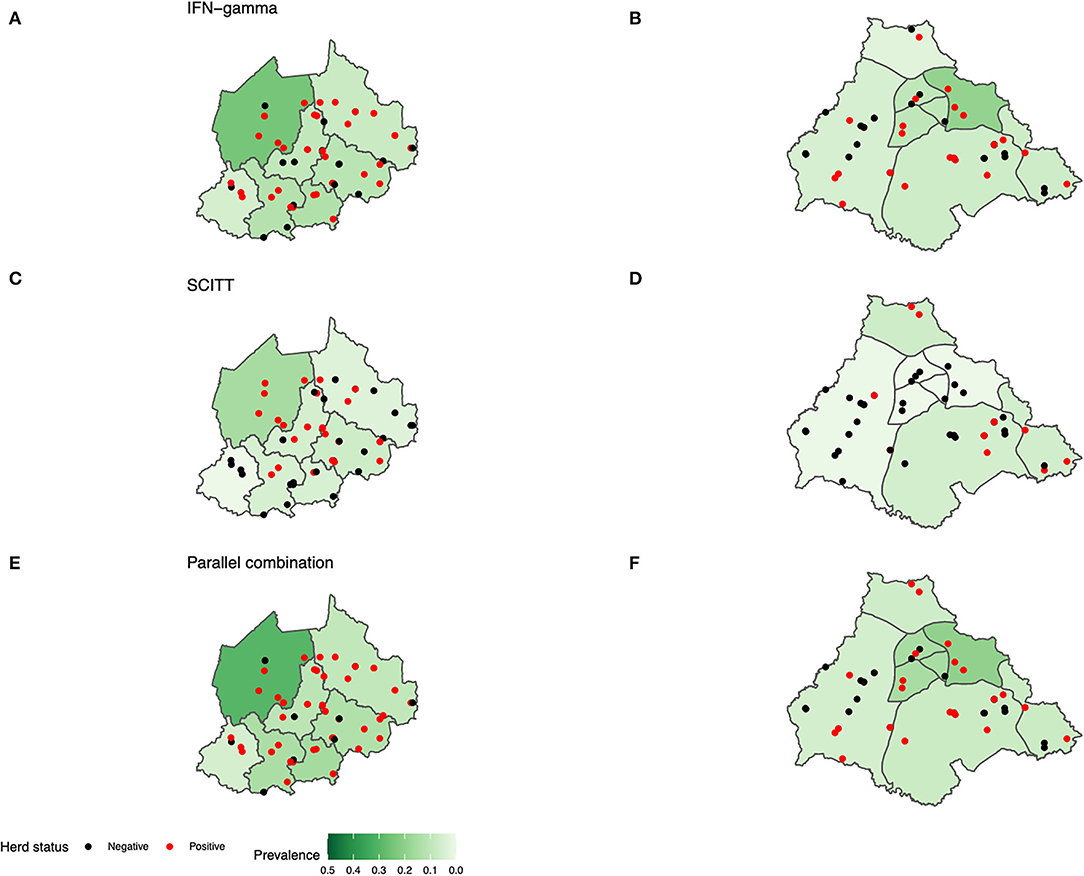
Figure 5. Map study site by sublocation prevalence for pastoral cattle. (A,B) IFN-γ assay (≥0.1), (C,D) SCITT (>2 mm) and (E,F) Parallel combination [subfigure (A,C,E) NWR n = 750. (B) VIN n = 748. (D,F) VIN n = 741]. Positive herds have at least one infected animal per herd.
Results from sampled cattle were subsetted to investigate diagnostic disagreement for being IFN-γ assay-positive and SCITT-negative using two methods to produce two final models (Figures 2A,B described the disagreement investigated using the models outlined Table 2). The final models are presented in Table 2. Model a looked at animals that were IFN-γ-positive and then looked at factors associated with testing SCITT-negative (n = 133). Only age was strongly associated with disagreement. In other words, older animals were more likely to test negative on the SCITT test given they were IFN-γ-positive. Model b looked at the reverse and looked at SCITT-negative animals and factors associated with them being positive for the IFN-γ (n = 1422). Here, female animals were less likely to be IFN-γ-positive compared to males, and also interestingly, animals having had exposure to BLV or paraTB were more likely to be in disagreement. The area under the ROC curve for the final averaged models was 0.94 (95% CI: 0.90–0.97) and 0.87 (95% CI: 0.85–0.91) for models a and b, respectively. This was an indicative of good model performance in relation to classifying the disagreements.
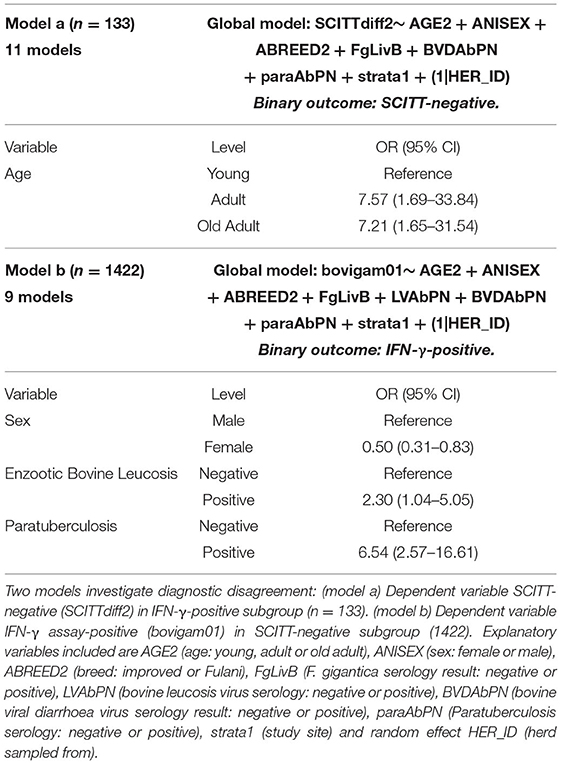
Table 2. Final models to investigate risk factors for pastoral cattle testing IFN-γ assay-positive and SCITT-negative.
Cattle were also subsetted to investigate diagnostic test disagreement for being SCITT-positive and IFN-γ assay-negative using two methods (Figures 2C,D described the disagreement investigated using the models outlined Table 3). The final models are presented in Table 3; model c looked at animals that were IFN-γ-negative and then looked at factors associated with testing SCITT-positive (n = 1,364). Only age was strongly associated with disagreement, where animal that has tested negative on the IFN-γ it is more likely to be SCITT-positive if it is an older animal (adult or older adult) compared to the young animal. For model d, using the subset of animals testing SCITT-positive, there were no factors strongly associated with animals testing IFN-γ-negative (disagreement), but the sample size for this subset was very small (n = 68). The area under the ROC curve for the final averaged models was 0.90 (95% CI: 0.83–0.96) and 0.99 (95% CI: 0.97–1.00) and for models c and d, respectively. These results indicate that the models correctly classified the disagreements.
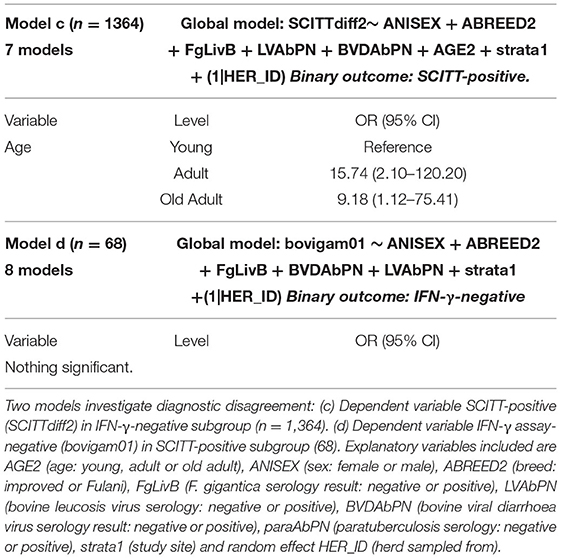
Table 3. Final models to investigate risk factors for pastoral cattle testing IFN-γ assay-negative and SCITT-positive.
In this study, we highlight that the use of the IFN-γ assay, SCITT, and parallel combination tests can give a quite different impression of the overall magnitude of bTB prevalence in a naturally infected cattle population. Although individual or combined test prevalence estimates overlapped in the two localities, the lowest and highest estimates in each locality differed by multiples of ~2–3. Internationally, the individual and combined use of IFN-γ assay and SCITT are used to estimate prevalence to prioritise local resources in bTB surveillance and control programmes (2, 3). Inaccurate estimates of bTB prevalence will likely have a detrimental public health impact where resources for control are limited. This is of particular concern in SSA contexts where M. bovis is undoubtedly a public health issue, due to a close interaction between cattle and humans, and disease surveillance is infrequent. Understanding the level of agreement and host factors associated with disagreement will improve interpretation of future bTB prevalence estimates in SSA cattle populations.
Although the antemortem tests measure the CMI response to M. bovis infection (56), and a degree of agreement is likely, agreement between the two tests was only “moderate” [κ = 0.42 (moderate agreement: 0.41–0.60)] at best when using positive cut-off values of ≥0.1 and >2 mm positive cut-offs for the IFN-γ assay and SCITT, respectively. Even lower agreement was noted between the IFN-γ assay and the SCITT was reported at >4 mm, defined as poor [κ = 0.13 (poor agreement: 0.01–0.2)]. Poor agreement has also been reported between the two assays in Ethiopia where the >4 mm cut-off was used for the SCITT and ≥0.1 for the IFN-γ assay (57). Other studies in SSA, including Cameroon, reported that bTB-positive B. indicus cattle respond differently to M. bovis PPD, when compared to B. taurus cattle, with improved agreement when using the >2 mm cut-off for the SCITT (58–60). Suggesting that use of a lower >2 mm cut-off for the SCITT could be more appropriate in cattle populations in SSA. The IFN-γ assay and the SCITT also do not identify the same bTB positive population of cattle, possibly because the two tests are measuring different aspects of the CMI response (15, 61). Sampled cattle were from a naturally infected population, where M. bovis infected cattle are likely infected at different time points, likely to be at different stages in pathogenesis and consequently have marked variation in their host immune responses at the time of sampling. The IFN-γ assay is considered to be more sensitive than the SCITT and can detect M. bovis infection weeks–months earlier than the SCITT test (10, 62), which could explain why in our study, the IFN-γ assay consistently detecting more positives than the SCITT (at either study site). This suggests that potentially, the IFN-γ assay may be more suitable for highlighting the potential magnitude of prevalence in resource-limited settings, by detecting animals earlier post-infection. Further work is required to understand the diagnostic performance of the IFN-γ assay compared to the SCITT to improve the accuracy of prevalence estimates in naturally infected cattle populations.
Using subsets of the complete dataset, of test positive and negative animals, we were able to explore host-related factors for disagreement. Being IFN-γ assay-positive and SCITT-negative was a far more common form of disagreement and, as reported in other studies (16, 63–66), potentially associated with the low sensitivity of the SCITT, although reasons for reported lower sensitivity of the SCITT are poorly eluded. The impact of co-infections is likely to depend on pathogen or subtype exposed to, burden and timing of exposure (7, 18, 67). Bovine leucosis virus and paratuberculosis positivity were reported to increase the risk of this form of disagreement. As in our study, animals sampled from naturally infected populations may be co-infected with immunosuppressing or modulating infections and have been reported to influence CMI immune responses (7). Exposure to bovine leucosis virus can result in a persistent immunosuppression which may lead to depression in CMI responses, although its less clear why one CMI diagnostic may be affected more than another. Non-tuberculous mycobacteria have been shown to infect Cameroonian cattle (34) yet as both CMI diagnostic tests included a control avian PPD in their protocols, and the impact of non-tuberculous mycobacteria is likely to vary (68–70). Other researchers have identified that the performance of both the SCITT and the IFN-γ assay can be affected by paratuberculosis (Mycobacterium avium subspecies paratuberculosis) positivity in experimental infections (28, 71–73) specifically with increased reactivity to avian PPD. Although it is currently unclear why the IFN-γ-positive/ SCITT-negative disagreement was predominant in our study, this might be related to younger animals being less impacted by MAP immunosuppressive responses than older animals (>1 year of age) (74). Although frequency of avian PPD and paratuberculosis positives was low in this study, the addition of mitogen to IFN-γ assay may be helpful to improve diagnostic sensitivity (13, 75) when testing Cameroon or similar SSA cattle populations. Interestingly, F. gigantica exposure was not associated with increased risk of disagreement between the CMI diagnostics. This is contra to an abattoir study, also conducted by authors, which demonstrated that F. gigantica was associated with decreased IFN-γ positivity and larger bTB lesions (23). Although it is unclear why a similar relationship was not also noted in this field study, multiple parasite and host factors are likely to affect the interaction between M. bovis and F. gigantica at any given time point. For example, experimental studies have demonstrated that a related Fasciola species, Fasciola hepatica, has been associated with decreases in diagnostic sensitivity for IFN-γ and SCITT when compared to detection of bTB lesions postmortem (76), but the extent of the effect on bTB diagnosis is determined by the order of infection of the two organisms (76). In our study, fluctuations in exposure or burden are not captured by the F. gigantica antibody ELISA (35) as the test detects exposure to infection at some point in an animal's lifetime. Future work should focus on investigating the variation in the bovine immune response to M. bovis in naturally infected cattle beyond singular time points and the dynamic impact of co-infections on bTB diagnostic test performance.
Advanced age was reported to be associated with both types of disagreement (IFN-γ-positive/ SCITT-negative and IFN-γ-negative/ SCITT-positive). In later stages of infection, IFN-γ responses can fluctuate throughout the course of M. bovis infection and may lead to IFN-γ assay false negatives (56, 65) when SCITT is positive. Furthermore, IFN-γ responses become anergic in chronic M. bovis infections (56), and advanced age of cattle could be a proxy for chronicity when investigating disagreement. IFN-γ assay-negative and SCITT- positive disagreement were less frequently reported which is potentially due to the higher specificity of the SCITT (16, 63–65). Cattle with chronic M. bovis infections are thought to be more likely to become SCITT-positive if they initially start out as IFN-γ-positive (12, 77), which may partly explain why this form of disagreement occurred less frequently.
In the absence of a gold-standard diagnostic for bTB, we were unable to fully explore the diagnostic performance of animals sampled using antemortem diagnostic tests. However, we were able to explore the associations with host factors that may account for diagnostic disagreement, using multivariable mixed-effects logistic regression modelling and a model averaging selection method. Compared to traditional methods of model selection, model averaging techniques allowed us to better identify the factors associated with the disagreements and the risk factors through a better estimation of the coefficients. Similar to Bayesian approaches, several models can be ranked and weighted to provide a quantitative measure of relative support for each competing hypothesis (51). By comparison, more traditional approaches such as stepwise methods, although also resulting in a final model, completely ignore model uncertainty (78). It is clear that co-infections can have complex impacts on bTB test diagnostics performance, and this may have important implications for bTB prevalence estimates along with future surveillance and control programmes in SSA. Although we did not test for every co-infection possible, our study has highlighted the need to consider animal level factors when interpretating bTB diagnostic test results to develop accurate prevalence estimates in cattle populations of interest.
Inaccuracies in local prevalence estimates hinder the progress of bTB surveillance and control programmes. In this study, we demonstrated that individual or combined use of the IFN-γ assay and SCITT can lead to a large variation in bTB prevalence estimates. Animal-level factors may impact on the agreement between CMI diagnostics and could limit our understanding of bTB epidemiology in endemic settings, where animals of various disease states exist. Quantifying the impact of factors, such as co-infections, should be prioritised to improve the accuracy of diagnosis and understanding of bTB epidemiology across cattle populations in SSA as well as other LMICs.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study was reviewed and approved by the University of Edinburgh Ethics Committee, UK (ERC No: OS02-13) and by the Institute of Research and Development (IRAD), Cameroon. All participants gave informed verbal consent to the translator before participating and could opt out at any stage. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
BB, LN, and VT conceived the original project. BB, RK, KM, LN, VT, MS, and NE designed the field study, the databases, and the survey instrument. RK, NE, VN, VT, KM, and BB developed the field SOPs and collected the data. RK, EF, and LG conducted laboratory work. RK and BB cleaned the initial dataset. RK, LG, BB, and IH contributed to the analysis. RK was responsible for writing the initial drafts. All authors contributed comments for the final draft. All authors contributed to the article and approved the submitted version.
This work was funded by the Wellcome Trust (WT094945).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Importantly, we would like to thank all the cattle keepers, MINEPIA veterinary centre staff, delegates, and our diligent translator Saidou M. Hamman whom without this study would not possible.
1. O'Reilly LM, Daborn CJ. The epidemiology of Mycobacterium bovis infections in animals and man: a review. Tuber Lung Dis. (1995) 76 (Suppl. 1):1–46.
2. Schiller I, Oesch B, Vordermeier HM, Palmer MV, Harris BN, Orloski KA, et al. Bovine tuberculosis: a review of current and emerging diagnostic techniques in view of their relevance for disease control and eradication. Transbound Emerg Dis. (2010) 57:205–20. doi: 10.1111/j.1865-1682.2010.01148.x
3. OIE. Bovine tuberculosis. In: OIE Manual for Diagnostic Tests and Vaccines for Terrestrial Animals. (2009). p. 1–16.
4. Corner LA. Post mortem diagnosis of Mycobacterium bovis infection in cattle. Vet Microbiol. (1994) 40:53–63.
5. Corner L, Melville L, McCubbin K, Small KJ, McCormick BS, Wood PR, et al. Efficiency of inspection procedures for the detection of tuberculous lesions in cattle. Aust Vet J. (1990) 67:389–92.
6. Bezos J, Casal C, Romero B, Schroeder B, Hardegger R, Raeber AJ, et al. Current ante-mortem techniques for diagnosis of bovine tuberculosis. Res Vet Sci. (2014) 97 S44–52. doi: 10.1016/j.rvsc.2014.04.002
7. de la Rua-Domenech R, Goodchild AT, Vordermeier HM, Hewinson RG, Christiansen KH, Clifton-Hadley RS. Ante mortem diagnosis of tuberculosis in cattle: a review of the tuberculin tests, gamma-interferon assay and other ancillary diagnostic techniques. Res Vet Sci. (2006) 81:190–210. doi: 10.1016/j.rvsc.2005.11.005
8. Rhodes SG, Buddle BM, Hewinson RG, Vordermeier HM. Bovine tuberculosis: immune responses in the peripheral blood and at the site of active disease. Immunology. (2000) 99:195–202.
9. Ritacco V, Lopez B, DeKantor IN, Barrera L, Errico F. Nader A. Reciprocal cellular and humoral immune-responses in bovine tuberculosis. Res Vet Sci. (1991) 50:365–7.
10. McNair J, Welsh MD, Pollock JM. The immunology of bovine tuberculosis and progression toward improved disease control strategies. Vaccine. (2007) 25:5504–11. doi: 10.1016/j.vaccine.2007.02.037
11. Clegg TA, Duignan A, Whelan C, Gormley E, Good M, Clarke J, et al. Using latent class analysis to estimate the test characteristics of the γ-interferon test, the single intradermal comparative tuberculin test and a multiplex immunoassay under Irish conditions. Vet Microbiol. (2011) 151:68–76. doi: 10.1016/j.vetmic.2011.02.027
12. Álvarez J, Perez A, Marqués S, Bezos J, Grau A. de la Cruz ML, Romero B, et al. Risk factors associated with negative in-vivo diagnostic results in bovine tuberculosis-infected cattle in Spain. BMC Vet Res. (2014) 10:14. doi: 10.1186/1746-6148-10-14
13. Nuñez-Garcia J, Downs SH, Parry JE, Abernethy DA, Broughan JM, Cameron AR, et al. Meta-analyses of the sensitivity and specificity of ante-mortem and post-mortem diagnostic tests for bovine tuberculosis in the UK and Ireland. Prev Vet Med. (2018) 153:94–107. doi: 10.1016/J.PREVETMED.2017.02.017
14. Buddle BM, de Lisle GW, Pfeffer A, Aldwell FE. Immunological responses and protection against Mycobacterium bovis in calves vaccinated with a low dose of BCG. Vaccine. (1995) 13:1123–30.
15. Neill SD, Cassidy J, Hanna J, Mackie DP, Pollock JM, Clements A, et al. Detection of Mycobacterium bovis infection in skin test negative cattle with an assay for bovine interferon gamma. Vet Record. (1994) 135:134–5.
16. Wood P, Corner L. Field comparison of the interferon-gamma assay and the intradermal tuberculin test for the diagnosis of bovine tuberculosis. Aust Vet J. (1991) 68:286–90. doi: 10.1111/j.1751-0813.1991.tb03254.x
17. Buddle BM, de Lisle GW, Griffin JFT, Hutchings SA. Epidemiology, diagnostics and management of tuberculosis in domestic cattle and deer in New Zealand in the face of a wildlife reservoir. N Z Vet J. (2015) 63 (Suppl. 1):19–27. doi: 10.1080/00480169.2014.929518
18. Taylor P, Buddle BM, Livingstone PG, Lisle GW De. Advances in ante-mortem diagnosis of tuberculosis in cattle. N Z Vet J. (2011) 57:37–41.
19. Robinson PA. A history of bovine tuberculosis eradication policy in Northern Ireland. Epidemiol Infect. (2015) 143:1–14. doi: 10.1017/S0950268815000291
20. Wood PR, Jones SL. BOVIGAM an in vitro cellular diagnostic test for bovine tuberculosis. Tuberculosis (Edinb). (2001) 81:147–55. doi: 10.1054/tube.2000.0272
21. Palmer MV, Waters WR. Advances in bovine tuberculosis diagnosis and pathogenesis: what policy makers need to know. Vet Microbiol. (2006) 112:181–90. doi: 10.1016/j.vetmic.2005.11.028
22. Sinclair JA, Dawson KL, Buddle BM. The effectiveness of parallel gamma-interferon testing in New Zealand's bovine tuberculosis eradication programme. Prev Vet Med. (2016) 127:94–9. doi: 10.1016/j.prevetmed.2016.03.020
23. Kelly RF, Callaby R, Egbe NF, Williams DJL, Ngwa VN, Tanya VN, et al. Association of fasciola gigantica co-infection with bovine tuberculosis infection and diagnosis in a naturally infected cattle population in Africa. Front Vet Sci. (2018) 5:214. doi: 10.3389/fvets.2018.00214
24. Flynn RJ, Mulcahy G, Welsh M, Cassidy JP, Corbett D, Milligan C, et al. Co-Infection of cattle with Fasciola hepatica and Mycobacterium bovis- immunological consequences. Transbound Emerg Dis. (2009) 56:269–74. doi: 10.1111/j.1865-1682.2009.01075.x
25. Kao RR, Gravenor MB, Charleston B, Hope JC, Martin M, Howard CJ. Mycobacterium bovis shedding patterns from experimentally infected calves and the effect of concurrent infection with bovine viral diarrhoea virus. J R Soc Interface. (2007) 4:545–51. doi: 10.1098/rsif.2006.0190
26. Lützelschwab CM, Forletti A, Cepeda R, Esteban EN, Confalonieri O, Gutiérrez SE. Co-infection with Mycobacterium bovis does not alter the response to bovine leukemia virus in BoLA DRB3*0902, genetically resistant cattle. Res Vet Sci. (2016) 109:10–6. doi: 10.1016/J.RVSC.2016.09.002
28. Hope JC, Thom ML, Villarreal-Ramos B, Vordermeier HM, Hewinson RG, Howard CJ. Exposure to Mycobacterium avium induces low-level protection from Mycobacterium bovis infection but compromises diagnosis of disease in cattle. Clin Exp Immunol. (2005) 141:432–9. doi: 10.1111/j.1365-2249.2005.02882.x
29. Kelly RF, Hamman SM, Morgan KL, Nkongho EF, Ngwa VN, Tanya V, et al. Knowledge of bovine tuberculosis, cattle husbandry and dairy practices amongst pastoralists and small-scale dairy farmers in cameroon. PLoS ONE. (2016) 11:e0146538. doi: 10.1371/journal.pone.0146538
30. Awah-Ndukum J, Kudi AC, Bradley G, Ane-Anyangwe I, Titanji VPK, Fon-Tebug S, et al. Prevalence of bovine tuberculosis in cattle in the highlands of Cameroon based on the detection of lesions in slaughtered cattle and tuberculin skin tests of live cattle. Vet Med. (2012) 57:59–76.
31. Egbe NF, Muwonge A, Ndip L, Kelly RF, Sander M, Tanya V, et al. Molecular epidemiology of Mycobacterium bovis in Cameroon. Sci Rep. (2017) 7:4652. doi: 10.1038/s41598-017-04230-6
32. Cameroon National Statistics Department. Cameroon Culture Statistics. (2012). Available online at: http://www.statistics-cameroon.org/manager.php?id=11&id2=71&link=8 (accessed January 1, 2014).
33. Sergeant E. Epitools Epidemiological Calculators. AusVet Animal Health Services Australian Biosecurity Cooperative Research Centre for Emerging Infectious Disease (2013). Available online at: https://epitools.ausvet.com.au/
34. Egbe NF, Muwonge A, Ndip L, Kelly RF, Sander M, Tanya V, et al. Abattoir-based estimates of mycobacterial infections in Cameroon. Nat Sci Rep. (2016) 6:24320. doi: 10.1038/srep24320
35. Kelly RF, Mazeri S, Hartley C, Hamman SM, Ngu Ngwa V, Nkongho EF, et al. Assessing the performance of a Fasciola gigantica serum antibody ELISA to estimate prevalence in cattle in Cameroon. BMC Vet Res. (2019) 15:8. doi: 10.1186/s12917-018-1762-z
36. ID.Vet. ID Screen® Paratuberculosis Indirect. Available online at: https://www.id-vet.com/produit/id-screen-paratuberculosis-indirect/ (accessed November 1, 2021).
37. ID.Vet. ID Screen® BLV Competition - IDvet. Available online at: https://www.id-vet.com/produit/id-screen-blv-competition/ (accessed November 1, 2021).
38. ID.Vet. ID Screen® BVD p80 Antibody Competition - IDvet. Available online at: https://www.id-vet.com/produit/id-screen-bvd-p80-antibody-competition/ (accessed November 1, 2021).
39. RStudio. R Studio (Version 3.6.1). (2019). Available online at: http://www.rstudio.org/
41. Team QD. QGIS Geographic Information System (QGIS 3.16). (2009). Available online at: https://www.qgis.org/en/site/
42. Wickham H. tidyverse: Easily Install Load the “Tidyverse” (R package version 1.2.1). (2017). Available online at: https://www.tidyverse.org/
43. Dohoo I, Martin W, Stryhn H. Screening and diagnostic tests. In: McPike SM, editor. Veterinary Epidemiologic Research. 2nd ed. (2009). p. 91–134.
44. Gamer M, Lemon J, Fellows I, Singh P. Irr: various coefficients of iterrater reliability and agreement. (2012).
46. Thrusfield M. Evaluation and interpretation of diagnostic tests. Veterinary Epidemiology. Oxford, UK: Blackwell publishing (2005). p. 313–28
47. Vach W. The dependence of Cohen's kappa on the prevalence does not matter. J Clin Epidemiol. (2005) 58:655–61. doi: 10.1016/j.jclinepi.2004.02.021
49. Stevenson M. epiR: Tools for the Analysis of Epidemiological Data. (2016). Available online at: http://cran.r-project.org/package=epiR/
50. Schenker N, Gentleman JF. On judging the significance of differences by examining the overlap between confidence intervals. Am Stat. (2001) 55:182–6. doi: 10.1198/000313001317097960
51. Grueber CE, Nakagawa S, Laws RJ, Jamieson IG. Multimodel inference in ecology and evolution: challenges and solutions. J Evol Biol. (2011) 24:699–711. doi: 10.1111/j.1420-9101.2010.02210.x
52. Barton K. MuMIn” Title Multi-Model Inference (1.43.17). R (2020). Available online at: https://cran.r-project.org/web/packages/MuMIn/index.html#:~:text=MuMIn%3AMultiModelInference&text=Automatedmodelselectionthroughsubsetting,orcustommodelweightingschemes
53. Akaike H. Information Theory and an Extension of the Maximum Likelihood Principle. New York, NY: Foundations and Basic Theory. (1992) 1:610–24.
54. Burnham KP, Anderson DR. Model Selection and Multimodel Inference: A Practical Information-Theoretic Approach. New York, NY: Springer (2004). p. 1–454.
55. Kelly RF, Jennings A, Hunt J, Hamman SM, Mazeri S, Nkongho EF, et al. The epidemiology of bacterial zoonoses in pastoral and dairy cattle in Cameroon, Central Africa. Zoonoses Public Health. (2021) 68:781–93. doi: 10.1111/ZPH.12865
56. Pollock JM, Welsh MD, McNair J. Immune responses in bovine tuberculosis: towards new strategies for the diagnosis and control of disease. Vet Immunol Immunopathol. (2005) 108:37–43. doi: 10.1016/j.vetimm.2005.08.012
57. Ameni G, Aseffa A, Hewinson G, Vordermeier M. Comparison of different testing schemes to increase the detection Mycobacterium bovis infection in Ethiopian cattle. Trop Anim Health Prod. (2010) 42:375–83. doi: 10.1007/s11250-009-9429-1
58. Ameni G, Miörner H, Roger F, Tibbo M. Comparison between comparative tuberculin and gamma-interferon tests for the diagnosis of bovine tuberculosis in Ethiopia. Trop Anim Health Prod. (2000) 32:267–76. doi: 10.1023/A:1005271421976
59. Ameni G, Hewinson G, Aseffa A, Young D, Vordermeier M. Appraisal of interpretation criteria for the comparative intradermal tuberculin test for diagnosis of tuberculosis in cattle in central Ethiopia. Clin Vaccine Immunol. (2008) 15:1272–6. doi: 10.1128/CVI.00114-08
60. Ngandolo BNR, Müller B, Diguimbaye-Djaïbe C, Schiller I, Marg-Haufe B, Cagiola M, et al. Comparative assessment of fluorescence polarization and tuberculin skin testing for the diagnosis of bovine tuberculosis in Chadian cattle. Prev Vet Med. (2009) 89:81–9. doi: 10.1016/j.prevetmed.2009.02.003
61. Vordermeier M, Goodchild A, Clifton-Hadley R. de la Rua R. The interferon-gamma field trial: background, principles and progresss. Vet Rec. (2004) 155:37–8.
62. Brooks-Pollock E, Conlan AJ, Mitchell AP, Blackwell R, McKinley TJ, Wood JL. Age-dependent patterns of bovine tuberculosis in cattle. Vet Res. (2013) 44:1–9. doi: 10.1186/1297-9716-44-97
63. Gormley E, Doyle M, Duignan A, Good M, More SJ, Clegg TA. Identification of risk factors associated with disclosure of false positive bovine tuberculosis reactors using the gamma-interferon (IFNγ) assay. Vet Res. (2013) 44:117. doi: 10.1186/1297-9716-44-117
64. Alvarez J, Perez A, Bezos J, Marqués S, Grau A, Saez JL, et al. Evaluation of the sensitivity and specificity of bovine tuberculosis diagnostic tests in naturally infected cattle herds using a Bayesian approach. Vet Microbiol. (2012) 155:38–43. doi: 10.1016/j.vetmic.2011.07.034
65. Lahuerta-Marin A, Gallagher M, McBride S, Skuce R, Menzies F, McNair J, et al. Should they stay, or should they go? relative future risk of bovine tuberculosis for interferon-gamma test-positive cattle left on farms. Vet Res. (2015) 46:90. doi: 10.1186/s13567-015-0242-8
66. Praud A, Boschiroli ML, Meyer L, Garin-Bastuji B, Dufour B. Assessment of the sensitivity of the gamma-interferon test and the single intradermal comparative cervical test for the diagnosis of bovine tuberculosis under field conditions. Epidemiol Infect. (2015) 143:157–66. doi: 10.1017/S0950268814000338
67. Bezos J, Alvarez J, de Juan L, Romero B, Rodríguez S, Fernández-de-Mera IG, et al. Assessment of in vivo and in vitro tuberculosis diagnostic tests in Mycobacterium caprae naturally infected caprine flocks. Prev Vet Med. (2011) 100:187–92. doi: 10.1016/j.prevetmed.2011.03.012
68. Lilenbaum W, Marassi CD, Varges R, Medeiros L, Oelemann WMR, Fonseca LS. Occurrence of false-positive results in three paratuberculosis ELISAs performed in a tuberculous herd. Vet Res Commun. (2009) 33:693–9. doi: 10.1007/S11259-009-9218-3/TABLES/2
69. Raffo E, Steuer P, Monti G, Salgado M. Effect of Mycobacterium avium subsp. paratuberculosis (MAP) infection on the diagnostic accuracy for Mycobacterium bovis (M bovis) infection under field conditions in cattle belonging to low M bovis prevalence herds. Tropical Animal Health Prod. (2017) 49:771–5. doi: 10.1007/S11250-017-1259-Y/TABLES/1
70. Byrne AW, Graham J, Milne G, Guelbenzu-Gonzalo M, Strain S. Is there a relationship between bovine tuberculosis (bTB) herd breakdown risk and Mycobacterium avium subsp. paratuberculosis status? An investigation in bTB chronically and non-chronically infected herds. Front Vet Sci. (2019) 6:30. doi: 10.3389/FVETS.2019.00030/BIBTEX
71. Dunn JR, Kaneene JB, Grooms DL, Bolin SR, Bolin CA, Bruning-Fann CS. Effects of positive results for Mycobacterium avium subsp paratuberculosis as determined by microbial culture of feces or antibody ELISA on results of caudal fold tuberculin test and interferon-γ assay for tuberculosis in cattle. J Am Vet Med Assoc. (2005) 226:429–35. doi: 10.2460/JAVMA.2005.226.429
72. Álvarez J, de Juan L, Bezos J, Romero B, Sáez JL, Marqués S, et al. Effect of paratuberculosis on the diagnosis of bovine tuberculosis in a cattle herd with a mixed infection using interferon-gamma detection assay. Vet Microbiol. (2009) 135:389–93. doi: 10.1016/J.VETMIC.2008.09.060
73. Barry C, Corbett D, Bakker D, Andersen P, McNair J, Strain S. The effect of mycobacterium avium complex infections on routine mycobacterium bovis diagnostic tests. Vet Med Int. (2011) 2011:145092. doi: 10.4061/2011/145092
74. Koets AP, Eda S, Sreevatsan S. The within host dynamics of Mycobacterium avium ssp. paratuberculosis infection in cattle: where time and place matter. Vet Res. (2015) 46:61. doi: 10.1186/s13567-015-0185-0
75. Bass KE, Nonnecke BJ, Palmer M. v., Thacker TC, Hardegger R, Schroeder B, et al. Clinical and diagnostic developments of a gamma interferon release assay for use in bovine tuberculosis control programs. Clin Vaccine Immunol. (2013) 20:1827. doi: 10.1128/CVI.00519-13
76. Flynn RJ, Mannion C, Golden O, Hacariz O, Mulcahy G. Experimental Fasciola hepatica infection alters responses to tests used for diagnosis of bovine tuberculosis. Infect Immun. (2007) 75:1373–81. doi: 10.1128/IAI.01445-06
77. Gormley E, Doyle MB, Fitzsimons T, McGill K, Collins JD. Diagnosis of Mycobacterium bovis infection in cattle by use of the gamma-interferon (Bovigam) assay. Vet Microbiol. (2006) 112:171–9. doi: 10.1016/j.vetmic.2005.11.029
Keywords: bovine tuberculosis, diagnostic test performance, cattle, epidemiology, Africa, Mycobacterium bovis
Citation: Kelly RF, Gonzaléz Gordon L, Egbe NF, Freeman EJ, Mazeri S, Ngwa VN, Tanya V, Sander M, Ndip L, Muwonge A, Morgan KL, Handel IG and Bronsvoort BMdC (2022) Bovine Tuberculosis Antemortem Diagnostic Test Agreement and Disagreement in a Naturally Infected African Cattle Population. Front. Vet. Sci. 9:877534. doi: 10.3389/fvets.2022.877534
Received: 16 February 2022; Accepted: 09 May 2022;
Published: 07 July 2022.
Edited by:
Julio Alvarez, VISAVET Health Surveillance Centre (UCM), SpainReviewed by:
Anita Luise Michel, University of Pretoria, South AfricaCopyright © 2022 Kelly, Gonzaléz Gordon, Egbe, Freeman, Mazeri, Ngwa, Tanya, Sander, Ndip, Muwonge, Morgan, Handel and Bronsvoort. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robert F. Kelly, cm9iZXJ0LmtlbGx5QHJvc2xpbi5lZC5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.