 Marlene Davis Ekpo1
Marlene Davis Ekpo1 George Frimpong Boafo1Suleiman Shafiu Gambo2Yuying Hu1Xiangjian Liu1Jingxian Xie1
George Frimpong Boafo1Suleiman Shafiu Gambo2Yuying Hu1Xiangjian Liu1Jingxian Xie1 Songwen Tan1*
Songwen Tan1*- 1Xiangya School of Pharmaceutical Sciences, Central South University, Changsha, China
- 2Department of Orthopedic Surgery, The Second Xiangya Hospital of Central South University, Central South University, Changsha, China
The basis of cryonics or medical cryopreservation is to safely store a legally dead subject until a time in the future when technology and medicine will permit reanimation after eliminating the disease or cause of death. Death has been debunked as an event occurring after cardiac arrest to a process where interjecting its progression can allow for reversal when feasible. Cryonics technology artificially halts further damages and injury by restoring respiration and blood circulation, and rapidly reducing temperature. The body can then be preserved at this extremely low temperature until the need for reanimation. Presently, the area has attracted numerous scientific contributions and advancement but the practice is still flooded with challenges. This paper presents the current progression in cryonics research. We also discuss obstacles to success in the field, and identify the possible solutions and future research directions.
Introduction
In an era of limitless scientific possibilities, humans are continually pushing boundaries to bring to reality the seemingly unimaginable. A perfect example of such innovation is the preservation of whole animals and humans at cryogenic temperature with the intention of restoring good health and resurrection in the future (1). Cryopreserving animals especially endangered species can be applicable to preventing extinction. Cryonicists hold the opinion that the pronouncement of legal death does not infer an irreversible event and that the medical technology required to initiate this reverse is presently unlocked (2).
Some proven fundamental principles of cryopreservation and cryobiology govern the practice of cryonics (2). These principles include: (A) Hypothermia can reduce or pause metabolism and other biochemical reactions while offering protection against ischemic injury. This is a natural occurrence for the northern wood frog (Rana sylvatica), which adapts to subzero temperatures (−3 to −6°C) for prolonged durations by transitioning into a semi-frozen phase devoid of cardiac function (3). Clinically, cryopreservation technology is applied extensively to extend the survival time of different cells, tissues and organs which would naturally lose viability if left unpreserved. Also, several research studies are presently being conducted to optimize cryopreservation of different materials (4, 5). (B) Cryoprotectants otherwise called cryoprotective agents (CPAs) can reduce or inhibit ice formation and nucleation (6). The effective application of cryoprotectants has been in existence as far back as the 1960's when glycerol was used by a Japanese scientist for the cryopreservation of cat brain at −20°C. Upon thawing after 45 days and electroencephalogram examinations, the brain displayed normal activity (7). Cryopreservation is performed either through programmable slow freezing, vitrification or low-CPA vitrification (ultra-rapid cooling) with vitrification being is the preferred technique in cryonics because it prevents/reduces the formation of damaging ice crystals within the cryopreserved subject (8).
To carry out cryonics presently, the candidate must be declared legally dead and consent must have been obtained prior because the procedure is yet to obtain medical recognition and approval (9). As shown in Figure 1, the cryopreservation procedure should commence ideally within 1–2 min post-mortem.
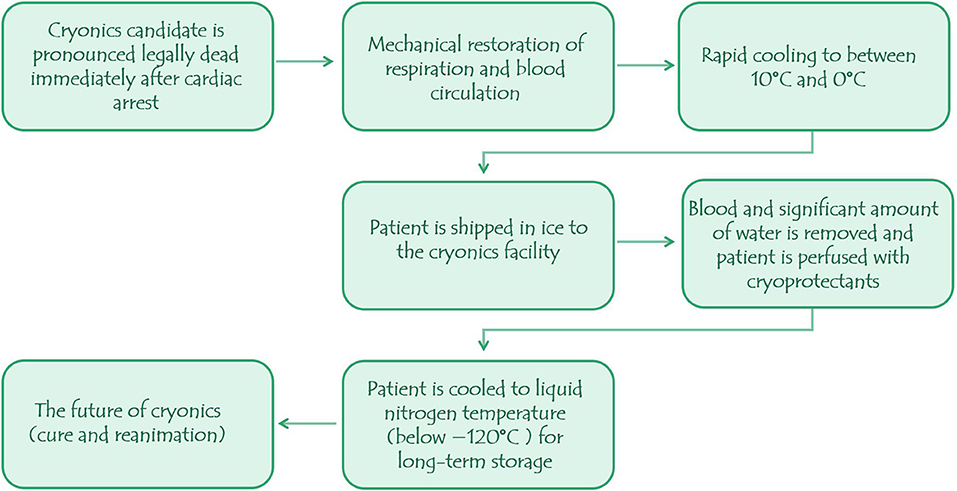
Figure 1. The procedure in cryonics.
The initial cooling of the subject to below 10°C is a crucial step required to cease biochemical and metabolic processes. It is usually carried out in a bath containing ice water and the cooling transfer is mainly controlled by convection, fluid motion and conduction mechanisms. The assisted blood circulation induced by cardiopulmonary support also facilitates cooling by promoting heat transfer (9). Each step leading to the final placement of the vitrified subject in liquid nitrogen (usually at −196°C) is performed with utmost precision to minimize or prevent further injury to tissues and depending on the cryonics facility, the protocol may vary slightly. For instance, the Alcor cryonics facility; after artificially restoring cardiopulmonary activity infuse intravenous protective medications into the subject in the hope for better outcome (10).
Finally, the patient is preserved in cryostasis in a vacuum-insulated liquid nitrogen vessel awaiting when research answers the question of how to cure and rejuvenate the subject. In this review we contribute toward the way forward in cryonics by presenting current progress and findings in cryonics research like the techniques employed to enhance the neuroprotective effect of hypothermia, restore functioning of the brain and other organs, reduce cryoinjury, extend survival after delayed time to cardiopulmonary resuscitation and minimize perfusion injury. Furthermore, we highlight the challenges encountered and discuss possible research directions.
Cryonics: From Conception Till Date
Cryonicists share ideologies with anti-aging scientists who propose that aging is a disease treatable with foreseeable medicine after the biomolecular and cellular mechanism of its pathology has been deciphered (11). Human cryostasis was proposed by Robert Ettinger “the father of cryonics” in the 1960s as a means to prevent the brain from deteriorating after legal death (12). The first cryonics patient; Prof. James Bedford remains cryopreserved in the United States of America (USA) (13) and Ettinger became a cryonic patient following his passing in 2011. Some operational cryonics facilities in the world include Alcor Life Extension Foundation (founded 1972) and the Cryonics Institute (founded 1976) both in USA, KrioRus (founded 2005) in Russia and the Shandong Yinfeng Life Science Research Institute (founded 2015) in China.
In 2014, the Alcor Life Extension Foundation claimed to have up to 300 cryonics patients held in their USA facility with more than 1,200 people signing up for the procedure after their demise (2). A recent survey that assessed the knowledge, perception and interest of internet users in the USA on “medical cryopreservation” after death has revealed the propensity of cryonics to gain more recognition (14). A 14-year-old patient who passed away from cancer in 2016 believed cryonics hold the key for her resurrection and cure in the future. Her case was legally upheld and her body is currently cryogenically preserved (15). Nonetheless, while some are still skeptical regarding the success of cryonics, a mean time of 82 years until the revival of cryopreserved bodies has been projected (14).
Challenges in Cryonics and Cryopreservation of Animals
Cost
Predictably, cryonics would be expensive because of the large amounts of resources required for prolonged preservation and the scarcity of expertise in the practice. In 2018, affording the procedure was valued at US$28,000 to $200,000 (16) which is significantly high especially for a clinically unproven theory that depends presently on inexistent technology. Notwithstanding, cryonics might be worth the cost should reanimation be achieved in the future.
Legal Consequences
There is currently no unified global perspective on cryonics. Countries like France and British Columbia have reservations (17) concerning the practice while some others (Germany, Russia and USA) are less stringent (18). Regardless of the technological advancements, cryonics raise some ethical and legal arguments that must be explored. For example, some believe it to be unethical while others think that employing cryonics is justifiable and humane. Other intriguing questions are the legal status of cryopreserved people and if cryothanasia is a feasible option to increase the chances of revival (1).
Feasibility of Revival
Proving the revival of cryopatients is the most daring obstacle because there are currently no proven interventions that can extend human lifespan (19) talk more of resurrection after legal death. Revival would involve repairing damage caused by freezing (in unvitrified tissues), hypoxia, cryoprotectant toxicity, thermal stress, then cure and possibly tissue regeneration if necessary but valid questions to consider in this regard would be: what does it really entail to be alive? would reversing the cause of death guarantee resurrection or a “healthy corpse”? Presently, research has revealed that different cells, tissues and organs require specifically tailored cryopreservation protocols to promote survival of the cryopreserved material. This requirement would pose a serious challenge to cryonics because the whole body is subjected to the same cryopreservation procedure which may not guarantee revival. Also, a revival protocol would have to be designed for every cryonic patient because people die of innumerable causes.
Cryopreservation Damage
Increasing the survival of complex tissues and organs remains a difficulty in cryopreservation. Considering the complexity of the human body, recovery from cryoinjury in cryonics would be even more challenging because prolonged vitrification at extremely low temperatures predisposes huge organs to rupture (20, 21). Ice crystals also damage intercellular junctions required for organ functioning (22) and without safe/effective cryoprotectants, cell survival is diminished by dehydration, high salt concentrations and cryoprotectant induced toxicity (23).
Limited Pro-cryonic Research
Although cryobiology research especially those on cryopreservation of more complex tissues and organs forms the core of cryonics, they cannot count as cryonics studies. According to Alcor, “THE SOCIETY FOR CRIOBIOLOGY has discouraged scientist from doing work that could advance cryonics ….” (24). The predictable outcome of this stance is minor research contributions as seen in Table 1, and slow scientific progress which could be improved upon by encouraging specialization of pro-cryonic scientists and research.
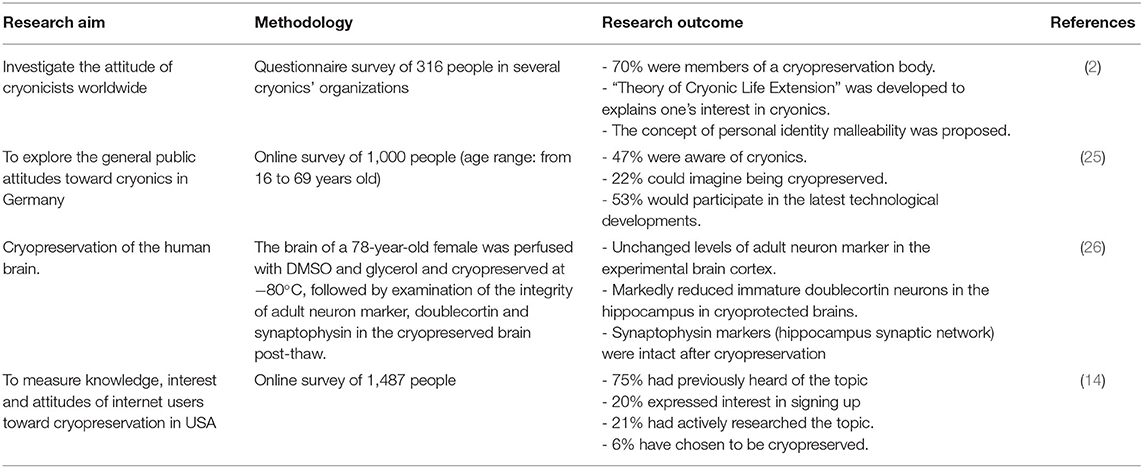
Table 1. Summary of original research on cryonics.
Technical Progress and Possible Research Directions in Cryonics
Some view cryonics as fictional. Singh in 2016 states “It appears man is trying to play god, but these attempts are most likely to prove futile. Instead of prolonging human life, it is more important to improve the vitality of health and quality of life throughout the life span of a person” (27). Notwithstanding this notion, researchers are making technical contributions to the field. These studies were mostly not aimed at cryonics but they have contributed substantially and can be considered as research directions in cryonics specialized studies.
Evaluating the Neuroprotective Effect of Hypothermia
Hypothermia considerably extends tolerance to irreversible ischemic injury (28–30) and many clinical reports, especially pediatrics', exist to support this cerebroprotective property of low temperatures (31). Research with animal models have also confirmed the potential benefits of hypothermia following cardiac arrest (32–34) with most of the neuroprotection attributable to the suppression of neuronal injury (35). Techniques to induce quicker hypothermia are being researched and developed such as cold saline aortic flush tested in pigs (36) and the invention of transnasal high flow dry air (37, 38). Furthermore, candidates like vasopressin (39), dihydrocapsaicin (DHC) (40, 41) and mesenchymal stem cell (MSC) (42) have been evaluated for their neuroprotective enhancing properties.
Restoring Functioning of the Brain and Other Organs
The closest procedure to cryonics and cryopreservation of whole animals is the cryopreservation of tissues and more complex organs including ovarian tissue (43), bones (44), bone marrow (45), skin grafts (46), pancreatic islet grafts (46), hearts (47), and lungs (48) with some of them being clinically applied during organ transplantation. Several studies are presently geared at improving extending cryopreservation time using suitable techniques and cryoprotectants and concomitantly preserving quality of the cryopreserved material. These studies can serve as insights toward the precise conditions necessary for effective long-term preservation and suggest to cryonics whether to review cryopreservation strategies for increased chances of reanimation.
The brain is highly complex in anatomy and function (49) therefore more difficult to recover after cryopreservation. Anoxia, reperfusion injury, oedema, and metabolic alterations could challenge the integrity of the brain after cryonics exposure and averting them is the aim of some research. Some neuroscientists suggest that memory retention is encoded in the physical structures of the brain, particularly neuropil connectivity and long-term retention of synaptic strengths (50) and possibly within individual neurons through DNA modifications (51). Vrselja et al. developed a cytoprotective and pulsatile-perfusion system that restored brain circulation and cellular functions up to 4 h post-mortem in the pig model (52).
Humans have been subjected to deep hypothermic (16, 24°C) cardiac arrest lasting more than 1 h without gross neurological deficits (53) confirming that for as much as the anatomy is untampered, the brains' electrical activity can be lost and fully recovered (9, 54). Also, the brain has been found intrinsically capable of resisting structural alterations for some time after death. 70–90% of Neurons from autopsied geriatric humans obtained approximately 2.6 h post-mortem remained viable after two (2) weeks in vitro (55). Theses research discoveries provide evidence that cryonically preserved subjects might have the chance to recover from ischemia and cryopreservation injury. Neural stem cell therapy (56), digital neural and soma reconstruction (57, 58) using bioabsorbable materials, e.g., polyglycolic acid conduit (59) nanobot cellular repair (60) and neural prosthesis (61) are under investigation as means to improve on restoring brain function. The other less complex organs can be replaced artificially, by tissue engineering (62) or stem cell based regenerative medicine. Regeneration of limbs in salamanders (63) and the use of lab-grown artificial ears (64) are green lights in this direction. Soon, organ replacement by 3D Tissue printing (65) and construction from biodegradable materials, e.g., ligaments with silk collagen scaffold (66) might be put to clinical application.
Minimizing Cryoinjury and Cryoprotectant Toxicity
A very critical stage in preparing patients for cryostasis is the replacement of body fluids (blood and water) with CPAs which are additives used to minimize ice induced injury to cryopreserved materials and support their post-thaw recovery. Different classes of CPAs exist, each functioning by one or more mechanisms including the induction of thermal hysteresis, ice nucleation and recrystallization inhibition and ice shaping. The most commonly used CPAs in cryobiology are dimethylsulfoxide (DMSO), glycerol, and different polyols like propylene glycol. Vitrification is the preferred cooling method in cryonics as the body is preserved in a stable glassy state (8, 67) but achieving this requires high CPA concentrations which can be damaging and toxic. As the future of cryonics is reanimation, a significant amount of research is currently focused on developing safer and effective CPA options including antifreeze proteins (AFPs) (68), trehalose (69), DP6 (70), nanotechnology engineered cryoprotectants (71), neutral amino acids (6). A major milestone was recorded in 2007 when major cryonics organizations claimed to have successfully vitrified the brain without ice formation (9), still post-thaw recovery not being promised drove the award-winning research of G. Fahy and R. McIntyre in 2015 (72). They infused rabbit brain with glutaraldehyde before vitrification allowing for recovery of an almost perfect brain post-thaw (73).
Prolonging Survival and Revival After Delayed Time to Cardiopulmonary Resuscitation
Some researchers have suggested that cryothanasia (subjecting a terminally ill patient to cryopreservation prior to legal death) might increase the chances of reanimation (74) but this concept is also hindered by lack of proof and ethical restraints. Experimenting on the concept of cryothanasia might hold the required breakthrough in cryonics but suitable live models have to be used and proven in studies prior to application in humans. In marine and aquatic science, several animals are naturally capable of adapting and surviving hypothermia for prolonged periods during overwintering. This act shares some similarities with cold preserving bodies before death and simulating the natural mechanisms that occur in overwintering animal models may make significant contributions to cryonics.
For instance, ranid frogs are highly sensitive to anoxia and during hypothermia, they maintain normal oxygen uptake and circulation at low oxygen partial pressures by cutaneous gas exchange and diverse physiological changes while energy is supplied by reserves in adipose tissues, liver and muscles (75). This example shows the significance of oxygenation, and justifies the artificial restoration of respiration and blood circulation performed in cryonics. It also reveals that it may be more beneficial to continue the supply of oxygen and energy to the cryopreserved subject throughout the entire cryopreservation process thereby reducing damage induced by hypoxia.
Similarly, Ultsch in 2006 studied different species of turtles undergoing overwintering where it was discovered that most of the marine species respond by migrating to avoid the negative effects of extensive exposure to cold (76). The Terrapene turtle adapts by freeze tolerance while some non-marine aquatic turtles are anoxia-tolerant (76). Mimicking the freeze tolerance and anoxia tolerance mechanisms could be advantageous to improving cryopreservation results.
Furthermore, a strain of Gibel Carp (Carassius gibelio) has been discovered to possess genetic resistance to overwintering starvation with less apoptosis (77), pointing to fact that certain genetic manipulations might confer resistance to tissue damage on cryopreserved subjects.
Cardiopulmonary resuscitation (CPR) combined with external defibrillation has restored life to many declared clinically dead from cardiac arrest (78) however, studies have suggested that delayed defibrillation is associated with lower survival rates (79, 80). This poses a serious challenge to cryonics and prolonging survival after delayed time to CPR is therefore critical in reanimating cryonics patients. In a related study using cats, brain activity was restored in a significant population after an hour of global cerebral ischemia and administration of norepinephrine/dopamine, heparin, insulin, and acidosis buffers (81). These agents are potentially applicable in increasing the chances of survival.
Minimizing Reperfusion Injury
Reperfusion injury is a term used to describe damage to tissues incurred from inflammatory responses and oxidation by toxic free radicals when blood circulation returns following ischemia lasting more than approximately 20 min (82, 83). In order to prevent reperfusion injury, different interventions have been employed. For example, microcirculation remodeling (84), administration of alpha-tocopherol (vitamin E) (85) and cilostazol (86) have been found beneficial against reperfusion injury in the spinal cord of rats. Pretreatment of cryonics subjects with vitamin E could be of added advantage as it reduces blood clotting and lacks the risk of gastric bleeding associated with aspirin (9) and administration of iptakalim has been found to improve cerebral microcirculation in mice (87). At Alcor, drugs including excitotoxicity inhibitors, nitric oxide synthase inhibitors and Poly ADP-ribose polymerase inhibitors are administered against reperfusion injury with further resistance conferred on the brain by anesthesia (10).
Conclusion
The ultimate expectation of animal cryopreservation and cryonics is that the subject will be revived after re-warming, removal of cryoprotectant, tissue repair, and cure. Whether or not this goal comes to fruition in the nearest future is widely dependent on the extent of research and scientific contributions. From this review, it is evident that scientific studies in cryonics and cryopreservation of animals are limited. The major challenges in cryonics have been identified as cost, ethical issues, cryodamage and revival with the most problematic being revival as its possibility is hanging on hope. Cryodamage can be overcome with the use of effective and safe cryoprotectants. At the same time, the cost of cryonics and ethical constrains might be lessened if there is proof of the concept of revival. Currently, no studies have attempted to cryopreserve and revive whole animals because of legal issues, pessimism surrounding the practice and shortage of cryonics expertise. Approval and funding of more pro-cryonics studies will lead to several serendipitous discoveries that could be advantageous to cryomedicine and cryobiology even though reanimation is not achieved.
Author Contributions
All the authors contributed significantly to the writing of the manuscript. ME, GB, and SG: writing—original draft preparation. ME, YH, XL, JX, and ST: writing—review and editing. ST: supervision and approval.
Funding
This research was supported by Central South University.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank Bo Li, Anjie Wang, and Chuanbao Zang from Yinfeng Biological Group., Ltd, and Baoqing Wang, Yuhang Luo, and Guang Zhao from Hunan Shengbao Biotechnology Co., Ltd (Yinfeng Group) for their research support and sharing their ideas in the field of cryopreservation of animals and cryonics. The cryonics centre in Yinfeng Biological Group., Ltd at Shandong, China is very inspiring.
References
1. Moen OM. The case for cryonics. J Med Ethics. (2015) 41:677–81. doi: 10.1136/medethics-2015-102715
2. Swan M. Worldwide cryonics attitudes about the body, cryopreservation, and revival: Personal identity malleability and a theory of cryonic life extension. SOPHIA. (2019) 58:699–735. doi: 10.1007/s11841-019-0727-4
3. Storey KB, Storey JM. Mitochondria, metabolic control and microRNA: advances in understanding amphibian freeze tolerance. Biofactors. (2020) 46:220–8. doi: 10.1002/biof.1511
4. Dou M, Lu C, Rao W. Bioinspired materials and technology for advanced cryopreservation. Trends Biotechnol. (2021) 40:93–106. doi: 10.1016/j.tibtech.2021.06.004
5. Taylor MJ, Weegman BP, Baicu SC, Giwa SE. New approaches to cryopreservation of cells, tissues, and organs. Transfus Med Hemother. (2019) 46:197–215. doi: 10.1159/000499453
6. Sui X, Chen P, Wen C, Yang J, Li Q, Zhang L. Exploring novel cell cryoprotectants based on neutral amino acids. Chin J Chem Eng. (2020) 28:2640–9. doi: 10.1016/j.cjche.2020.07.009
7. Suda I, Kito K, Adachi C. Viability of long term frozen cat brain in vitro. Nature. (1966) 212:268–70. doi: 10.1038/212268a0
8. Finger EB, Bischof JC. Cryopreservation by vitrification: a promising approach for transplant organ banking. Curr Opin Organ Transplant. (2018) 23:353–60. doi: 10.1097/MOT.0000000000000534
9. Best BP. Scientific justification of cryonics practice. Rejuven Res. (2008) 11:493–503. doi: 10.1089/rej.2008.0661
10. ALCOR. Introduction to Alcor Procedures. (2020). Available online at: https://www.alcor.org/library/introduction-to-alcor-procedures/
11. De Winter G. Aging as disease. Med Health Care Philos. (2015) 18:237–43. doi: 10.1007/s11019-014-9600-y
12. The Cryonics Institute. Human Cryostasis: Realizing The Prospect of Immortality. (2022). Available online at: https://www.cryonics.org/ci-landing/human-cryostasis
13. Darwin M. Dear Dr. Bedford-open letter to the first frozen man. In: Alcor Life Extension Foundation. (1991). Available online at: https://alcor.org/Library/html/BedfordLetter.htm
14. Gillett CR, Brame T, Kendiorra EF. Comprehensive survey of United States internet users' sentiments towards cryopreservation. PLoS ONE. (2021) 16:e0244980. doi: 10.1371/journal.pone.0244980
15. Huxtable R. Cryonics in the courtroom: which interests? Whose interests? Med Law Rev. (2017) 26:476–99. doi: 10.1093/medlaw/fwx045
16. Human Tissue Authority,. Things to Consider When Making Your Decision on Cryonics. (2018). Available online at: https://www.hta.gov.uk/things-consider-when-making-your-decision-cryonics
17. CRYONICS Magazine,. British Columbia's Anti-Cryonics Law. (1991). Available online at: http://www.cryocdn.org/law57.html
18. Erte LA, Efimkova KS. Cryonics: legal and ethical aspects. Bioethics. (2019) 24:30–6. doi: 10.19163/2070-1586-2019-2(24)-30-36
19. Underwood M, Bartlett HP, Partridge B, Lucke J, Hall WD. Community perceptions on the significant extension of life: an exploratory study among urban adults in Brisbane, Australia. Soc Sci Med. (2009) 68:496–503. doi: 10.1016/j.socscimed.2008.11.002
20. Fahy GM, Saur J, Williams RJ. Physical problems with the vitrification of large biological systems. Cryobiology. (1990) 27:492–510. doi: 10.1016/0011-2240(90)90038-6
21. Alcor Life Extension F. Alcor: reaching for tomorrow: a publication of the Alcor Life Extension Foundation. Scottsdale, AZ: Alcor Life Extension Foundation (2001).
22. Rodríguez-Fernández S, Álvarez-Portela M, Rendal-Vázquez E, Piñeiro-Ramil M, Sanjurjo-Rodríguez C, Castro-Viñuelas R, et al. Analysis of cryopreservation protocols and their harmful effects on the endothelial integrity of human corneas. Int J Mol Sci. (2021) 22:12564. doi: 10.3390/ijms222212564
23. Liu X, Pan Y, Liu F, He Y, Zhu Q, Liu Z, et al. A review of the material characteristics, antifreeze mechanisms, and applications of cryoprotectants (CPAs). J Nanomater. (2021) 2021:9990709. doi: 10.1155/2021/9990709
24. ALCOR. Problems Associated With Cryonics (and Some Possible Solutions). (2020). Available online at: https://www.alcor.org/library/problems-associated-with-cryonics/
25. Kaiser S, Gross D, Lohmeier J, Rosentreter M, Raschke J. Attitudes and acceptance toward the technology of cryonics in Germany. Int J Technol Assess Health Care. (2014) 30:98–104. doi: 10.1017/S0266462313000718
26. Canatelli-Mallat M, Lascaray F, Entraigues-Abramson M, Portiansky EL, Blamaceda N, Morel GR, et al. Cryopreservation of a human brain and its experimental correlate in rats. Rejuven Res. (2020) 23:516–25. doi: 10.1089/rej.2019.2245
27. Singh M. Pediatrics in 21(st) century and beyond. Indian J Pediatr. (2016) 83:1420–5. doi: 10.1007/s12098-016-2206-z
28. Jackson TC, Kochanek PM. A new vision for therapeutic hypothermia in the era of targeted temperature management: a speculative synthesis. Ther Hypothermia Temp Manag. (2019) 9:13–47. doi: 10.1089/ther.2019.0001
29. Sun YJ, Zhang ZY, Fan B, Li GY. Neuroprotection by therapeutic hypothermia. Front Neurosci. (2019) 13:586. doi: 10.3389/fnins.2019.00586
30. Mohiyaddin S, Nanjaiah P, Saad AO, Acharya MN, Khan TA, Davies RH, et al. Suspended animation: the past, present and future of major cardiothoracic trauma. ANZ J Surg. (2018) 88:678–82. doi: 10.1111/ans.14313
31. Eich C, Bräuer A, Kettler D. Recovery of a hypothermic drowned child after resuscitation with cardiopulmonary bypass followed by prolonged extracorporeal membrane oxygenation. Resuscitation. (2005) 67:145–8. doi: 10.1016/j.resuscitation.2005.05.002
32. Behringer W, Safar P, Wu X, Kentner R, Radovsky A, Kochanek PM, et al. Survival without brain damage after clinical death of 60-120 mins in dogs using suspended animation by profound hypothermia*. Crit Care Med. (2003) 31:1523–31. doi: 10.1097/01.CCM.0000063450.73967.40
33. Takata K, Takeda Y, Sato T, Nakatsuka H, Yokoyama M, Morita K. Effects of hypothermia for a short period on histologic outcome and extracellular glutamate concentration during and after cardiac arrest in rats*. Crit Care Med. (2005) 33:1340–5. doi: 10.1097/01.CCM.0000166351.19369.D3
34. Nozari A, Safar P, Stezoski SW, Wu X, Henchir J, Radovsky A, et al. Mild hypothermia during prolonged cardiopulmonary cerebral resuscitation increases conscious survival in dogs*. Crit Care Med. (2004) 32:2110–6. doi: 10.1097/01.CCM.0000142700.19377.AE
35. Takeda Y, Namba K, Higuchi T, Hagioka S, Takata K, Hirakawa M, et al. Quantitative evaluation of the neuroprotective effects of hypothermia ranging from 34°C to 31°C on brain ischemia in gerbils and determination of the mechanism of neuroprotection. Crit Care Med. (2003) 31:255–60. doi: 10.1097/00003246-200301000-00040
36. Janata A, Holzer M, Bayegan K, Frossard M, Sterz F, Losert UM, et al. Rapid induction of cerebral hypothermia by aortic flush during normovolemic cardiac arrest in pigs. Crit Care Med. (2006) 34:1769–74. doi: 10.1097/01.CCM.0000218816.30297.A2
37. Chava R, Zviman M, Raghavan MS, Halperin H, Maqbool F, Geocadin R, et al. Rapid induction of therapeutic hypothermia using Transnasal high flow dry air. Ther Hypothermia Temp Manag. (2017) 7:50–6. doi: 10.1089/ther.2016.0016
38. Assis FR, Narasimhan B, Ziai W, Tandri H. From systemic to selective brain cooling - methods in review. Brain Circ. (2019) 5:179–86. doi: 10.4103/bc.bc_23_19
39. Janata A, Weihs W, Schratter A, Bayegan K, Holzer M, Frossard M, et al. Cold aortic flush and chest compressions enable good neurologic outcome after 15 mins of ventricular fibrillation in cardiac arrest in pigs*. Crit Care Med. (2010) 38:1637–43. doi: 10.1097/CCM.0b013e3181e78b9a
40. Wu D, Shi J, Elmadhoun O, Duan Y, An H, Zhang J, et al. Dihydrocapsaicin (DHC) enhances the hypothermia-induced neuroprotection following ischemic stroke via PI3K/Akt regulation in rat. Brain Res. (2017) 1671:18–25. doi: 10.1016/j.brainres.2017.06.029
41. Wu D, Zhi X, Duan Y, Zhang M, An H, Wei W, et al. Inflammatory cytokines are involved in dihydrocapsaicin (DHC) and regional cooling infusion (RCI)-induced neuroprotection in ischemic rat. Brain Res. (2019) 1710:173–80. doi: 10.1016/j.brainres.2018.12.033
42. Wei W, Wu D, Duan Y, Elkin KB, Chandra A, Guan L, et al. Neuroprotection by mesenchymal stem cell (MSC) administration is enhanced by local cooling infusion (LCI) in ischemia. Brain Res. (2019) 1724:146406. doi: 10.1016/j.brainres.2019.146406
43. Rivas Leonel EC, Lucci CM, Amorim CA. Cryopreservation of human ovarian tissue: a review. Transfus Med Hemother. (2019) 46:173–81. doi: 10.1159/000499054
44. Fan MC, Wang QL, Sun P, Zhan SH, Guo P, Deng WS, et al. Cryopreservation of autologous cranial bone flaps for cranioplasty: a large sample retrospective study. World Neurosurg. (2018) 109:e853–9. doi: 10.1016/j.wneu.2017.10.112
45. Bahsoun S, Coopman K, Akam EC. The impact of cryopreservation on bone marrow-derived mesenchymal stem cells: a systematic review. J Transl Med. (2019) 17:397. doi: 10.1186/s12967-019-02136-7
46. Dolezalova N, Gruszczyk A, Barkan K, Gamble JA, Galvin S, Moreth T, et al. Accelerating cryoprotectant diffusion kinetics improves cryopreservation of pancreatic islets. Sci Rep. (2021) 11:10418. doi: 10.1038/s41598-021-89853-6
47. Chiu-Lam A, Staples E, Pepine CJ, Rinaldi C. Perfusion, cryopreservation, and nanowarming of whole hearts using colloidally stable magnetic cryopreservation agent solutions. Sci Adv. (2021) 7:1–10. doi: 10.1126/sciadv.abe3005
48. Lautner LJ, Freed DH, Nagendran J, Acker JP. Current techniques and the future of lung preservation. Cryobiology. (2020) 94:1–8. doi: 10.1016/j.cryobiol.2020.04.009
49. Benito-Kwiecinski S, Lancaster MA. Brain organoids: human neurodevelopment in a dish. Cold Spring Harb Perspect Biol. (2020) 12:1–17. doi: 10.1101/cshperspect.a035709
50. Abraham WC, Robins A. Memory retention - the synaptic stability versus plasticity dilemma. Trends Neurosci. (2005) 28:73–8. doi: 10.1016/j.tins.2004.12.003
51. Arshavsky YI. “The seven sins” of the Hebbian synapse: can the hypothesis of synaptic plasticity explain long-term memory consolidation? Progress Neurobiol. (2006) 80:99–113. doi: 10.1016/j.pneurobio.2006.09.004
52. Vrselja Z, Daniele SG, Silbereis J, Talpo F, Morozov YM, Sousa AMM, et al. Restoration of brain circulation and cellular functions hours post-mortem. Nature. (2019) 568:336–43. doi: 10.1038/s41586-019-1099-1
53. Hayashida M, Sekiyama H, Orii R, Chinzei M, Ogawa M, Arita H, et al. Effects of deep hypothermic circulatory arrest with retrograde cerebral perfusion on electroencephalographic bispectral index and suppression ratio. J Cardiothoracic Vasc Anesthesia. (2007) 21:61–7. doi: 10.1053/j.jvca.2006.02.029
54. Rothstein TL. Recovery from near death following cerebral anoxia: a case report demonstrating superiority of median somatosensory evoked potentials over EEG in predicting a favorable outcome after cardiopulmonary resuscitation. Resuscitation. (2004) 60:335–41. doi: 10.1016/j.resuscitation.2003.10.007
55. Konishi Y, Lindholm K, Yang L-B, Li R, Shen Y. Isolation of living neurons from human elderly brains using the immunomagnetic sorting DNA-linker system. Am J Pathol. (2002) 161:1567–76. doi: 10.1016/S0002-9440(10)64435-5
56. Nalamolu KR, Chelluboina B, Fornal CA, Challa SR, Pinson DM, Wang DZ, et al. Stem cell treatment improves post stroke neurological outcomes: a comparative study in male and female rats. Stroke Vasc Neurol. (2021) 6:519–27. doi: 10.1136/svn-2020-000834
57. Li Q, Chen Z, He J-J, Hao S-Y, Wang R, Yang H-T, et al. Reconstructing the 3D digital core with a fully convolutional neural network. Appl Geophys. (2020) 17:401–10. doi: 10.1007/s11770-020-0822-x
58. Quan T, Li J, Zhou H, Li S, Zheng T, Yang Z, et al. Digital reconstruction of the cell body in dense neural circuits using a spherical-coordinated variational model. Sci Rep. (2014) 4:4970. doi: 10.1038/srep04970
59. Laroas G, Battiston B, Sard A, Ferrero M, Dellon AL. Digital nerve reconstruction with the bioabsorbable neurotube. Rivista Italiana di Chirurgia Plastica. (2003) 35:125–8.
60. Mitra M. Medical nanobot for cell and tissue repair. J Anal Pharm Res. (2017) 2:218–22. doi: 10.15406/iratj.2017.02.00038
61. Guggenmos DJ, Azin M, Barbay S, Mahnken JD, Dunham C, Mohseni P, et al. Restoration of function after brain damage using a neural prosthesis. Proc Natl Acad Sci USA. (2013) 110:21177–82. doi: 10.1073/pnas.1316885110
62. Zhu J, Wang Y, Zhong L, Pan F, Wang J. Advances in tissue engineering of vasculature through three-dimensional bioprinting. Dev Dyn. (2021) 250:1717–38. doi: 10.1002/dvdy.385
63. Brockes JP, Kumar A. Appendage regeneration in adult vertebrates and implications for regenerative medicine. Science. (2005) 310:1919–23. doi: 10.1126/science.1115200
64. BioMed Advances,. Children with Microtia Fitted with Lab-Grown Artificial Ears. (2018). Available online at: https://biomedadvances.com/children-microtia-fitted-lab-grown-artificial-ears/
65. Chen EP, Toksoy Z, Davis BA, Geibel JP. 3D bioprinting of vascularized tissues for in vitro and in vivo applications. Front Bioeng Biotechnol. (2021) 9:664188. doi: 10.3389/fbioe.2021.664188
66. Ran J, Hu Y, Le H, Chen Y, Zheng Z, Chen X, et al. Ectopic tissue engineered ligament with silk collagen scaffold for ACL regeneration: a preliminary study. Acta Biomater. (2017) 53:307–17. doi: 10.1016/j.actbio.2017.02.027
67. Fahy GM, Wowk B. Principles of cryopreservation by vitrification. Methods Mol Biol. (2015) 1257:21–82. doi: 10.1007/978-1-4939-2193-5_2
68. Ekpo MD, Xie J, Hu Y, Liu X, Liu F, Xiang J, et al. Antifreeze proteins: novel applications and navigation towards their clinical application in cryobanking. Int J Mol Sci. (2022) 23:2639. doi: 10.3390/ijms23052639
69. Vasudevan B, Chang Q, Wang B, Huang S, Sui Y, Zhu W, et al. Effect of intracellular uptake of nanoparticle-encapsulated trehalose on the hemocompatibility of allogeneic valves in the VS83 vitrification protocol. Nanobiomedicine. (2020) 7:1849543520983173. doi: 10.1177/1849543520983173
70. Wowk B, Fahy GM, Ahmedyar S, Taylor MJ, Rabin Y. Vitrification tendency and stability of DP6-based vitrification solutions for complex tissue cryopreservation. Cryobiology. (2018) 82:70–7. doi: 10.1016/j.cryobiol.2018.04.006
71. Ehrlich LE, Gao Z, Bischof JC, Rabin Y. Thermal conductivity of cryoprotective agents loaded with nanoparticles, with application to recovery of preserved tissues and organs from cryogenic storage. PLoS ONE. (2020) 15:e0238941. doi: 10.1371/journal.pone.0238941
72. Thompson H,. Mammal Brain Frozen Thawed Out Perfectly for First Time: New Scientist. (2016). Available online at: https://www.newscientist.com/article/2077140-mammal-brain-frozen-and-thawed-out-perfectly-for-first-time/
73. McIntyre RL, Fahy GM. Aldehyde-stabilized cryopreservation. Cryobiology. (2015) 71:448–58. doi: 10.1016/j.cryobiol.2015.09.003
74. Minerva F, Sandberg A. Euthanasia and cryothanasia. Bioethics. (2017) 31:526–33. doi: 10.1111/bioe.12368
75. Tattersall GJ, Ultsch GR. Physiological ecology of aquatic overwintering in ranid frogs. Biol Rev Camb Philos Soc. (2008) 83:119–40. doi: 10.1111/j.1469-185X.2008.00035.x
76. Ultsch GR. The ecology of overwintering among turtles: where turtles overwinter and its consequences. Biol Rev Camb Philos Soc. (2006) 81:339–67. doi: 10.1017/S1464793106007032
77. Xu W, Li H, Wu L, Dong B, Jin J, Han D, et al. Genetically based physiological responses to overwinter starvation in Gibel Carp (Carassius gibelio). Front Endocrinol. (2020) 11:578777. doi: 10.3389/fendo.2020.578777
78. Page RL. The AED in resuscitation: it's not just about the shock. Trans Am Clin Climatol Assoc. (2011) 122:347–55.
79. Chan PS, Krumholz HM, Nichol G, Nallamothu BK. Delayed time to defibrillation after in-hospital cardiac arrest. N Engl J Med. (2008) 358:9–17. doi: 10.1056/NEJMoa0706467
80. Mhyre JM, Ramachandran SK, Kheterpal S, Morris M, Chan PS. Delayed time to defibrillation after intraoperative and periprocedural cardiac arrest. Anesthesiology. (2010) 113:782–93. doi: 10.1097/ALN.0b013e3181eaa74f
81. Hossmann K-A. Resuscitation potentials after prolonged global cerebral ischemia in cats. Crit Care Med. (1988) 16:964–71. doi: 10.1097/00003246-198810000-00007
82. Khalil AA, Aziz FA, Hall JC. Reperfusion injury. Plast Reconstr Surg. (2006) 117:1024–33. doi: 10.1097/01.prs.0000204766.17127.54
83. de Groot H, Rauen U. Ischemia-reperfusion injury: processes in pathogenetic networks: a review. Transplant Proc. (2007) 39:481–4. doi: 10.1016/j.transproceed.2006.12.012
84. Lapi D, Colantuoni A. Remodeling of cerebral microcirculation after ischemia-reperfusion. J Vasc Res. (2015) 52:22–31. doi: 10.1159/000381096
85. Morsy MD, Mostafa OA, Hassan WN. A potential protective effect of alpha-tocopherol on vascular complication in spinal cord reperfusion injury in rats. J Biomed Sci. (2010) 17:55. doi: 10.1186/1423-0127-17-55
86. Kurtoglu T, Basoglu H, Ozkisacik EA, Cetin NK, Tataroglu C, Yenisey C, et al. Effects of cilostazol on oxidative stress, systemic cytokine release, and spinal cord injury in a rat model of transient aortic occlusion. Ann Vasc Surg. (2014) 28:479–88. doi: 10.1016/j.avsg.2013.08.005
Keywords: cryonics, cryostasis, cryoprotectants, medical cryopreservation, cryopatient
Citation: Ekpo MD, Boafo GF, Gambo SS, Hu Y, Liu X, Xie J and Tan S (2022) Cryopreservation of Animals and Cryonics: Current Technical Progress, Difficulties and Possible Research Directions. Front. Vet. Sci. 9:877163. doi: 10.3389/fvets.2022.877163
Received: 16 February 2022; Accepted: 16 May 2022;
Published: 09 June 2022.
Edited by:
Mukesh Kumar Gupta, National Institute of Technology Rourkela, IndiaReviewed by:
Yan Zhang, Hunan Normal University, ChinaGuoxiang Tong, Changsha Medical University, China
Copyright © 2022 Ekpo, Boafo, Gambo, Hu, Liu, Xie and Tan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Songwen Tan, c29uZ3dlbi50YW5AY3N1LmVkdS5jbg==