 Anne K. Ebelt
Anne K. Ebelt Sonja Fuchs1
Sonja Fuchs1 Corinna Weber
Corinna Weber Urs Giger
Urs Giger- 1Laboklin GmbH&Co KG, Kissingen, Germany
- 2PennGen Laboratory, University of Pennsylvania, Philadelphia, PA, United States
More than twelve blood group systems have been described in dogs, but little is known about their distribution frequencies within breed populations. Here, we report on an extensive typing survey carried out using available reagents and either established or new clinical kits in purebred dogs from Germany. Leftover anticoagulated blood samples were examined using an immunochromatographic strip method for DEA 1, a gel column technique for Dal and Kai 1/2, and new card agglutination tests for DEA 4 and DEA 5 (which were partially compared with the gel column technique). Monoclonal antibodies were used for DEA 1 and Kai 1/2 typing, and polyclonal antibodies were used for all other types. Among the 206 dogs, 59.2% were DEA 1+, 100% DEA 4+, 9% (Card)/11% (Gel) DEA 5+, 89.3% Dal+, 96.6% Kai 1+, and 2.9% Kai 2+. None of the dogs were Kai 1+/2+, and only one was Kai 1–/2–. Dal– dogs were found in several breeds. Erythrocytes from most DEA 1+ dogs bound strongly on the strips. The agglutination reactions for DEA 5 on the new card tests were generally less than those on the gel column. The blood group pattern DEA 4+, DEA 5–, Dal+, Kai 1+/2– and either DEA 1+ or DEA 1– was found among 80% of the dogs. In this first extensive blood typing survey of purebred dogs from Europe, the proportions of positive and negative blood types were similar to those found in the United States and, for DEA 1, were also similar to those from other European countries, with considerable breed variation in blood types. The newer typing techniques seem to work well and will likely be useful for detecting and preventing specific blood type incompatibilities in the clinic.
Introduction
Canine blood group systems are defined by the expression of various antigens on the surface of red blood cells (RBCs), with different individuals either missing a specific antigen (negative blood type) or expressing it to varying degrees (positive blood type) (1, 2). Because individuals lacking the expression of a certain antigen may develop transfusion reactions following subsequent transfusions due to naturally occurring or induced alloantibodies, accurate typing of canine blood types is essential to prevent potentially fatal blood incompatibility reactions in clinics (3–6).
While canine blood groups have been studied for more than half a century (7, 8), none have been characterized at the biochemical and/or molecular genetic level. Instead, canine blood group systems, which now number more than a dozen, have been identified utilizing antisera from previously transfused dogs and/or the specifically generated monoclonal antibodies (1, 9). An international committee meeting in the 1970s designated the initially identified blood group systems as Dog Erythrocyte Antigen—DEA (10). Since then, additional blood group systems have been proposed, including Dal (11), Kai 1 and Kai 2 (12), and other currently unclassified blood groups (9). Moreover, additional blood group systems are suspected to exist based upon incompatible major crossmatch test results observed in previously transfused dogs (13).
While some blood group systems are well accepted, there is still some controversy regarding the presence of clinically important naturally occurring alloantibodies against DEA 3, DEA 5, and DEA 7 (2, 7, 14, 15). However, there have been no acute hemolytic transfusion reactions reported in dogs in clinical settings, and similarly, no neonatal isoerythrolysis has been reported in puppies unless the dogs have been previously transfused (16, 17). Therefore, the presence and clinical importance of any naturally occurring alloantibodies are questioned.
The blood group system DEA 1 is clinically considered most important due to the strong DEA 1 antigenicity and the fact that DEA 1+ and DEA 1– dogs are found in relatively equal proportions (14, 18). The DEA 1 blood group system was originally proposed to have several subtypes: DEA 1.1 (A1), DEA 1.2 (A2), and DEA 1.3 (A3) (7, 8). However, recent studies indicate that the DEA 1 antigen(s) can be recognized by a single monoclonal antibody, with the antigen(s) variably expressed from weakly to moderately to strongly positive (19). The level of expression of DEA 1 antigen(s) is genetically determined and does not change over time or during storage of blood (19, 20).
Blood typing methods have evolved from tube and card tests to immunochromatographic strip, cartridge, and flow cytometry assays, but additional typing kits for other blood types would be desirable (1, 21–24). Several limited surveys have been performed for DEA 1, and a few have assessed other blood types in North America and Europe (25–35), but there have been no comprehensive surveys carried out on a canine population typing for many blood groups.
The purpose of this study was to determine the prevalence of several blood types in dogs using available reagents and kits at a diagnostic reference laboratory in Germany. We also determined the degree of DEA 1 antigen expression and introduced two novel typing kits, i.e., agglutination cards for DEA 4 and DEA 5. Finally, we compared our typing results with studies from the USA and other countries. This represents the first extended blood typing survey in purebred dogs from Europe.
Materials and Methods
Dogs and Blood Samples
Leftover ethylene-diaminetetraacetic acid (EDTA)-anticoagulated blood samples from purebred dogs that had been submitted for routine diagnostic work to Laboklin GmbH& Co KG, Kissingen, Germany between December 2018 and October 2019 were used for this survey. Of a total of 206 samples, the majority (188) originated from Germany, with 18 samples from neighboring or other European countries (Czech Republic, Denmark, Finland, Italy, Luxembourg, Sweden, and Norway). The approval to use leftover samples for research was received from the Government IACUC in Bayern, Germany. Only leftover samples with of least 1 ml EDTA blood that was less than 1 week old and had been stored at 4–8°C prior to analysis were included. Samples from several dog breeds, classified based on the Fédération Cynologique Internationale (FCI1), were selected based upon prior studies (11, 12, 27, 29, 36, 37) and our own early results of their varied blood group antigen expression. Samples from known related dogs or repeat samples from the same dog were excluded. Data on breed, gender, and age as well as geographic region were obtained. None of the samples showed any auto-agglutination in card and gel tests. All results were photographically captured.
Blood Typing Assays
DEA 1 Typing by Immunochromatographic Strip
An immunochromatographic strip test (Strip, Lab Test DEA 1, Alvedia, Limonest, France) with a murine monoclonal anti-DEA 1 alloantibody was used according to the manufacturer's instructions and as previously described (19, 27). The strength of the DEA 1 band was semi-quantitatively assessed by visually comparing the control (anti-glycophorin antibody) band to the DEA 1 band and grading it from – to 4+ (Figure 1), as previously described (27, 38).
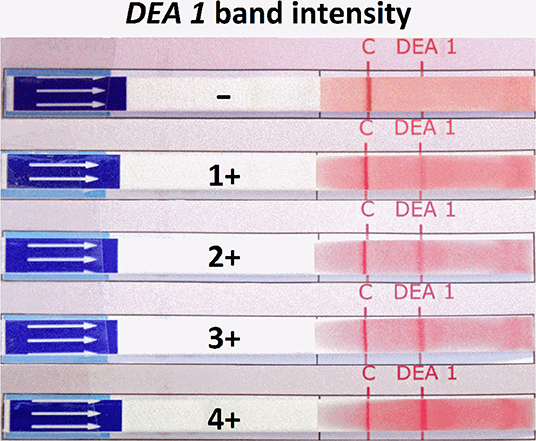
Figure 1. DEA 1 typing results on immunochromatographic strips from 206 dogs. The varied binding intensities to a monoclonal anti-DEA 1 antibody at the DEA 1 position on the strip were graded from – (no band, negative) to 1+ to 4+ (band, positive). Red blood cells in suspension migrated in the membrane; the C (control) band had to show for it to be a valid test, while a variably strong DEA 1 band was visible in some cases.
DEA 4 and DEA 5 Typing by Agglutination Cards
Newly introduced agglutination cards (Card, RapidVet-H DEA 4 Agglutination Card Test, and DEA 5 Card RapidVet- H DEA 5 Agglutination Card Test, DMS, Flemington, NJ, USA) with polyclonal anti-DEA 4 or anti-DEA 5 typing reagents (antisera) were used for this survey according to the manufacturer's instructions, with minor modifications. Prior to utilizing these cards in this survey, they were validated with DEA 4+ and DEA 4– RBCs as well as with DEA 5+ and DEA 5– RBCs, respectively, by the manufacturer.
While the manufacturer's instructions suggested the use of 40 μl of diluent for DEA 4 typing, very weak resulting agglutination reactions prompted us to add an additional 40 μl of diluent after the initial reading to achieve a total of 80 μl of diluent (identical to the volume in the protocol for DEA 5 typing). This was routinely performed for 191 of 206 samples after the occurrence of weak agglutination reactions was observed with some of the first blood samples. The lack of and degree of an agglutination reaction was recorded from – to 4+ (Figure 2A).
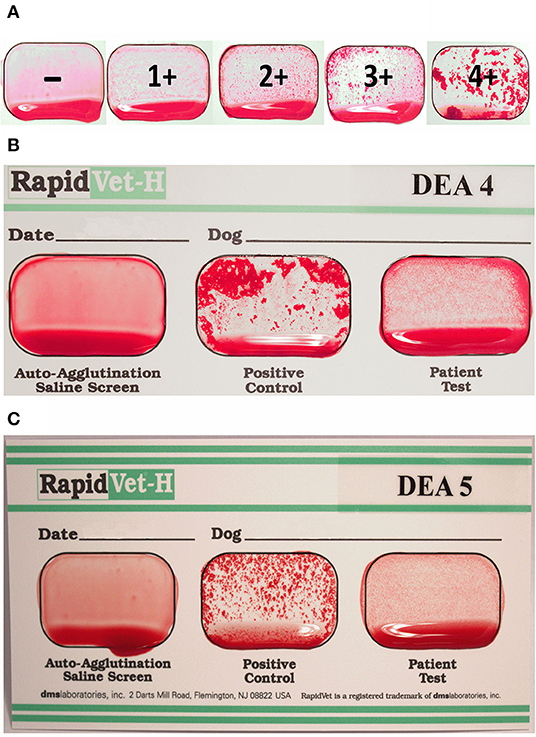
Figure 2. New agglutination cards for DEA 4 and DEA 5 typing of dogs. (A) Grading of the agglutination reaction strength from – to 4+. (B) DEA 4+ and (C) DEA 5+ showing weak agglutination reactions (1+). In each of the three wells of a card, 40 μl (DEA 4) or 80 μl (DEA 5) of buffer and 50 μl of EDTA blood from one dog was added and gently mixed. The well for “Auto-Agglutination-Saline Screen” and “Positive Control” must be negative and positive, respectively, to interpret the typing results. Depending on whether there is agglutination in the “Patient Test” well, the dog is considered positive or negative.
Briefly, 50 μl of EDTA blood was added to 40 μl of diluent for DEA 4 typing or 80 μl of diluent for DEA 5 typing in each of the three wells on one card. Using the wooden stirrer provided, the reagents adhering to both the positive control and the patient well surface were rubbed off (no reagent in auto-agglutination control) and mixed to cover the entire well. The cards were gently rocked for 30 s and then examined for agglutination reactions, first while still rocking and once again after slightly tilting the card to allow excess blood to run to the bottom of each well.
If there were no visible agglutinations in the auto-agglutination well and a visible agglutination reaction in the positive control well, the assay was considered valid. Depending on the presence or absence of an agglutination reaction in the patient test well, the dog is considered weakly (1+) to strongly positive (3+/4+) or negative (–) for the respective blood group (Figures 2B,C).
Any degree of agglutination was considered a positive typing result. While the agglutination card testing was performed with all samples, gel column assay (see below) was also performed on some samples (n = 158) using the same anti-DEA 4 and anti-DEA 5 alloantibodies.
DEA 4 and DEA 5, Dal, Kai 1, and Kai 2 Typing by a Gel Column Technique
A gel column technique (Gel, using BioRad ID-Cards, NaCl, Enzyme Test and Cold Agglutinins, DiaMed, Cressier, Switzerland) was used for DEA 4 and DEA 5, Dal, Kai 1, and Kai 2 typing, similar to our previous studies (24, 27, 29, 39). Briefly, EDTA blood samples were washed three times and diluted to a 2% RBC suspension using phosphate-buffered saline. Canine antisera containing anti-DEA 4 or anti-DEA 5 polyclonal alloantibodies from previously sensitized dogs (Animal Blood Resources International, Michigan, USA, provided by DMS Laboratories Inc.) were diluted at 1:32 and 1:10 with Blood Bank Saline, respectively. The anti-Dal alloantibody was from a previously sensitized dog [University of Pennsylvania (11)], and monoclonal alloantibodies against Kai 1 and Kai 2 [Dr. He Young Kim, South Korea (12)] were used undiluted. We added 25 μl of the 2% RBC suspension and 25 μl of alloantibody reagent on top of the gel column. The mixture was incubated for 15 min at room temperature (~23°C), and then the gel column cards were centrifuged for 10 min at 85 x g in an ID-Centrifuge 6 S (DiaMed-ID, Microtyping System, DiaMed, Cressier, Switzerland). The results were then visually analyzed, and the results were graded from – to 4+ (Figure 3) depending on the location of the majority of RBCs within the gel column, as described (27, 29, 30).
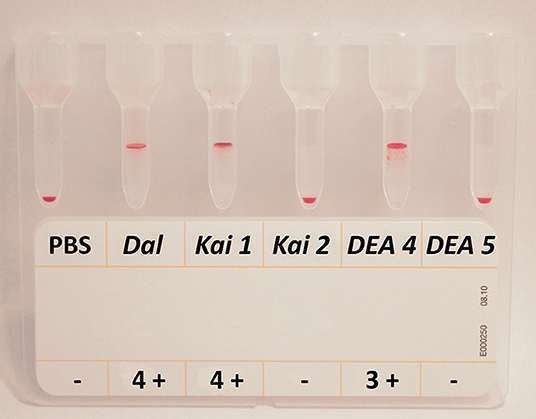
Figure 3. Gel column typing results for Dal, Kai 1, Kai 2, DEA 4, and DEA 5 from one dog. The blood sample from this dog shows a typical typing pattern: 4+ agglutination reactions for Dal and Kai 1, no agglutination for Kai 2, a 3+ agglutination reaction for DEA 4, and no agglutination for DEA 5. Red blood cells at the top (4+) to within the gel mean positive agglutination reactions. PBS, phosphate-buffered saline, serves as auto-agglutination control.
Statistical Analysis
Python v. 3.5.2 using Scipy2 v. 0.17.0 and Numpy v. 1.11.0 were used for statistical analyses. Chi-square test was done using Scipy's Chi-square implementation. Results were considered significant when p < 0.05. Additionally, Cohen's Kappa Test in Scikit v. 0.17.0 was used for comparison of DEA 4 and DEA 5 Card and Gel Tests.
Results
In this survey, we screened 206 dogs from 18 breeds of six FCI groups, with ≥10 dogs for nine breeds (Table 1 and Supplement Table 1). They were 53.9% males and 43.7% females (2.4% unknown). The ages of the dogs ranged between 0.4 and 17 years (age unknown for nine dogs). Of the 64 (26) possible blood type combinations, 14 different patterns were found, with two predominant patterns that only differed by DEA 1 type; 47% of the dogs were DEA 4+, DEA 5–, Dal+, Kai 1+, Kai 2–, or DEA 1+, and 33% were DEA 4+, DEA 5–, Dal+, Kai 1+, Kai 2–, or DEA 1–; thus, 80% only differed by their DEA 1 type. The other 12 observed blood type patterns were seen in only 0.5–5% of the dogs, without any specific breed association (patterns shown in Supplement Table 2).
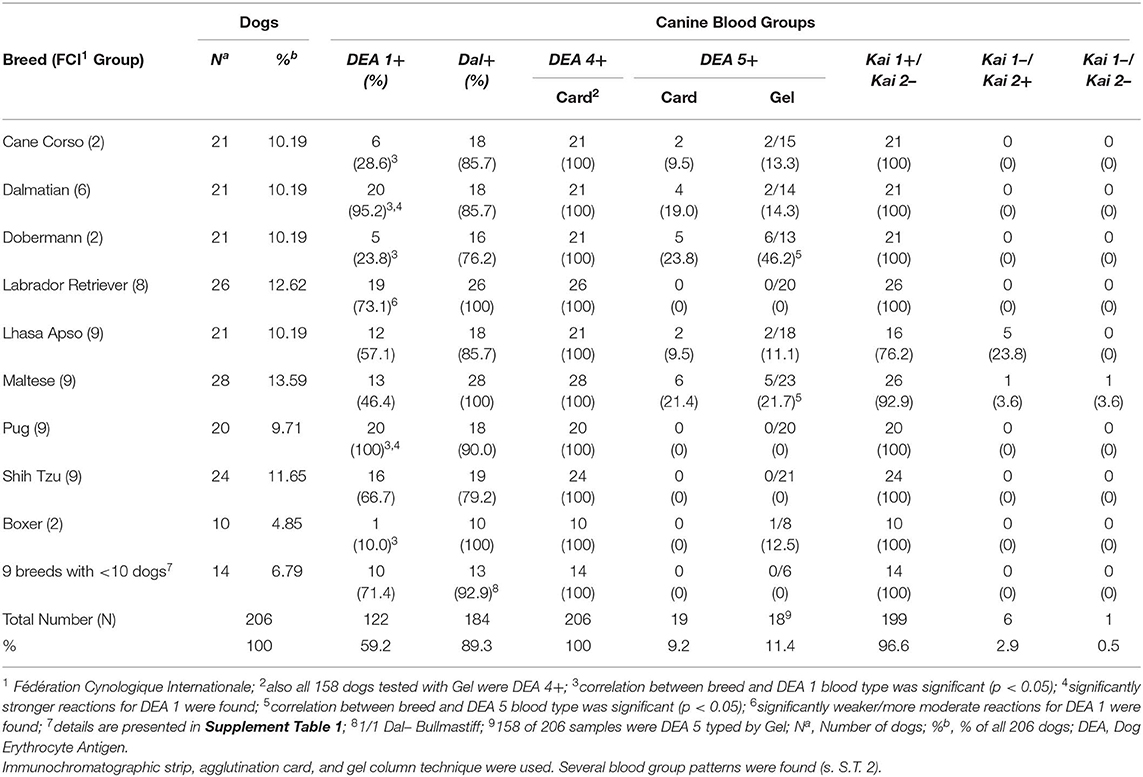
Table 1. Typing results for blood groups DEA 1, Dal, DEA 4, DEA 5, Kai 1, and Kai 2 in 206 dogs from Germany including breed and FCI1 group.
DEA 1 Typing Results
Utilizing the Strip with a monoclonal anti-DEA 1 alloantibody, we were able to identify dogs with no reactivity, and thus DEA 1–, as well as dogs that were strongly positive, with DEA 1 bands comparable to the positive control band. Of the 206 dogs, an equal proportion was either graded as DEA 1– (40.8%) or strongly DEA 1+ (40.3%) with a smaller proportion (18.9%) of weak to moderate DEA 1+ band reactions (Figure 1). Strong reactions (3+ and 4+) for DEA 1 were found significantly more often in Dalmatians (p = 0.0003) and Pugs (p = 0.0003), and weak/moderate (1+/2+) reactions were significantly more common in Labrador Retrievers (p = 0.001). All Pugs and Dalmatians except for one Dalmatian were DEA 1+, and more Labrador retrievers and Shih Tzus were DEA 1+ than were other breeds (Table 1).
In contrast, less than a quarter of Cane Corsos and Doberman Pinschers were DEA 1+, and all but one Boxer was DEA 1– (Table 1). These breeds belong to the FCI group 2. A significant dependency between breed and DEA 1 type was found for Cane Corso (p = 0.004), Dalmatian (p = 0.001), Doberman Pinscher (p = 0.001), Pug (p = 0.0002), and Boxer (p = 0.002).
DEA 4 Typing Results
When using the Card newly developed for DEA 4 typing according to manufacturer's instructions, 9.2% of 206 dogs showed an extremely weak and thus questionable 1+ agglutination reaction, and 67.0% produced only weakly positive (1+/2+) results. However, when adding an additional 40 μl of diluent, all 191 tested dogs produced ≥1+ and clearly visible agglutination reactions, supportive of a DEA 4+ blood type. When comparing the results between the two diluent concentrations, 72% of the reactions stayed the same, 18% strengthened, and 10% became weaker (never weakening by more than one degree, e.g., 2+ became 1+), but none of the positive agglutination reactions turned negative (Supplement Table 3). Based on these results, the manufacturer's instructions have been changed to indicate that if the results using the initial 40 μl are unclear, another 40 μl of diluent should be added.
To further evaluate the results obtained by the new DEA 4 typing card, we also applied the Gel using commercially available anti-DEA 4 alloantibodies (antiserum; same as for the Card). As all dogs tested were DEA 4+ with the Card and Gel, we had perfect agreement (Kappa = 1) between the tests. Of the 158 dogs tested, all reacted strongly positively (3+/4+) and, therefore, were considered to have blood type DEA 4+ (Figure 3). While all agglutination reactions observed by the Gel were 3+ to 4+, such strong reactions (3+ to 4+) using Cards were only seen in 23.8 and 15.7% using 40 and 80 μl of diluent, respectively. While the regression of DEA 4 agglutination strength with 40 μl and 80 μl in the 191 tested dogs showed a good correlation (r = 0.8999), there was no significant correlation of strength between the Gel and Card (r = 0.0754). Also, the degree of DEA 4 positivity did not appear to be associated with any particular breed.
DEA 5 Typing Results
When using the new DEA 5 typing card according to the manufacturer's instructions, 90.8% of 206 dogs did not show any RBC-agglutination reactions. Weak agglutination reactions (1+ or 2+) were seen in 19 dogs, and they were thus considered DEA 5+ (Table 1). The manufacturer states that the DEA 5 agglutination is “finer and less plentiful than that observed in a DEA 1 dog run on a DEA 1 test card” (DMS) and we also found the DEA 5+ card agglutination results to be consistently less intense than the DEA 4+ card results. Utilizing the Gel with the same polyclonal DEA 5 antibody used for the Card, 11.4% of the 158 dogs typed DEA 5+. With the Gel, six (33.3%) of the DEA 5+ dogs reacted only weakly/moderately positive, while the other 12 DEA 5+ dogs reacted strongly (3+/4+).
When comparing the Card and Gel methods, 97% of the DEA 5 results were concordant; in four of five discordant results, the Gel test indicated DEA 5+ (Table 2). The regression of DEA 5 Gel and Card strength in all 158 tested dogs showed a good correlation (r = 0.8329), and the two methods showed almost perfect agreement (Kappa = 0.831). For the Doberman Pinscher (p = 0.02) and Maltese (p = 0.03), the DEA 5+ blood type was significantly associated with the breed.
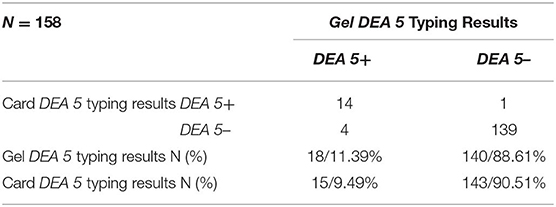
Table 2. Comparison and results for DEA 5 Card and Gel for 158 dogs typed by both methods.
Using the Card, 9% of all 206 dogs and also 9% of the 158 dogs that were typed by both Card and Gel were DEA 5+, while 11% of those 158 dogs were DEA 5+ using the Gel. DEA 5+ dogs were found by the Card and Gel in Cane Corso, Dalmatian, Doberman, Lhasa Apso, and Maltese, and by the Gel also in one Boxer (Table 1).
Dal Typing Results
Strong (3+/4+) agglutination reactions for Dal using a polyclonal anti-Dal antiserum in a Gel assay were observed in 183 of the Dal+ dogs, and a 2+ reaction was seen in one Shih Tzu that was on immunosuppressive therapy. In addition to the previously reported breeds with Dal– dogs, we found 22 Dal– dogs also in the breeds Cane Corso, Pug, and Mastiff (Table 1). We did not find any significant association between breed and Dal type, but the number of dogs per breed is small.
Kai 1 and Kai 2 Typing Results
Utilization of the Gel and specific monoclonal antibodies against Kai 1 and Kai 2 resulted in either very strong agglutination reactions or completely negative test results (Figure 4). Overall, 96.6% of all dogs were Kai 1+/Kai 2– (Table 3). There were only five Lhasa Apsos and one Maltese that were Kai 1–/Kai 2+. Furthermore, only a single Maltese dog was found to be Kai 1–/Kai 2– in this survey (Table 1).
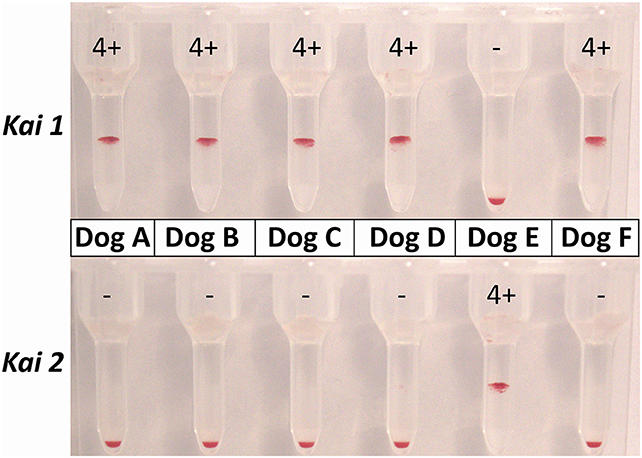
Figure 4. Gel column typing results for the same six dogs for Kai 1 and Kai 2. Dogs A–D and F are showing the most common Kai 1+/Kai 2– typing pattern, while Dog E has a Kai 1–/Kai 2+ pattern.
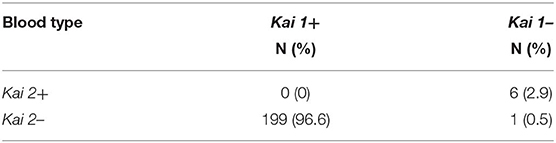
Table 3. Results for Kai 1 and Kai 2 typing of 206 dogs typed by the gel column method.
Discussion
Blood transfusions are pivotal in the supportive care of anemic and bleeding dogs, but the recruitment of blood donors and assuring blood type compatibility pose challenges. While DEA 1 typing is well established, limited availability of other typing reagents, in-practice kits, and laboratory methods have hampered the extended blood typing of dogs. In this comprehensive blood typing survey of 206 dogs from Germany, we used established and introduced new typing methods for several canine blood types and found significant differences in the prevalence of specific blood types among certain breeds. Overall, 80% of all dogs were DEA 4+, DEA 5–, Dal+, and Kai 1+/2– but could be either DEA 1+ or DEA 1–. While the Gel and Strip are the most accurate standardized methods, the new DEA 4 and DEA 5 typing cards are welcome diagnostic kits to extend the typing repertoire in clinical practice and assist with the investigation and prevention of blood incompatibilities.
DEA 1 Typing
Overall, 40.8 % of all dogs in our survey were DEA 1–, which is very similar to recent surveys from USA, France, India, and Italy that also utilized the same immunochromatographic method and monoclonal anti-DEA 1 alloantibody (25, 27, 31, 37, 40). Comparison to prior studies is complicated, because these studies utilized polyclonal alloantibodies against DEA 1.1 and DEA 1.2 (7). However, recent studies clearly showed a close association between DEA 1 typing and DEA 1.1 typing results (19). In fact, the original monoclonal anti-DEA 1.1 alloantibodies used in DEA 1 typing kits were later renamed as DEA 1 by the manufacturers. The relationship between DEA 1 and DEA 1.2 is less clear, but it is likely that DEA 1.2 is a weaker DEA 1 antigen (20). No laboratories currently offer DEA 1.2 typing or any reagents for DEA 1.2 typing. Nevertheless, prior surveys using polyclonal anti-DEA 1.1 and anti-DEA 1.2 antisera also showed a predominance of DEA 1+ dogs (Table 4). A comparative overview of prior DEA 1 typing surveys is shown in Table 4.
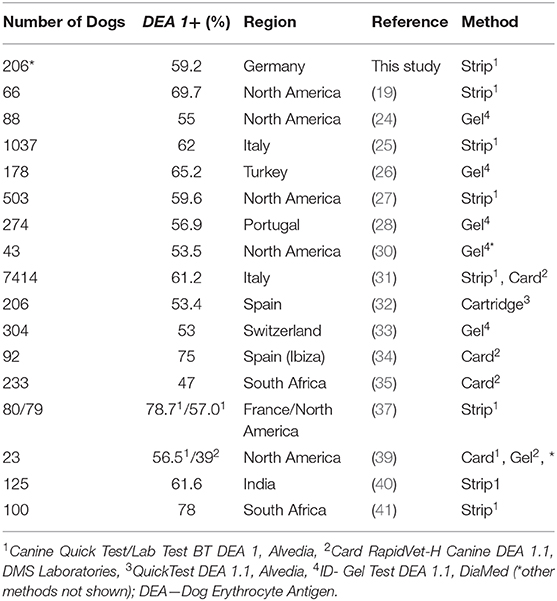
Table 4. Comparative table for the current survey and previously reported DEA 1 blood type prevalence per region.
Far more (71–90%) of the tested Cane Corsos, Doberman Pinschers, and Boxers were DEA 1–. Interestingly, these breeds belong to the FCI group 2, while other breeds studied were in other groups. Boxers and Cane Corso from various other European countries and South Africa were also mostly DEA 1– in prior surveys (details in Supplement Table 4). Thus, these breeds may be preferentially considered when recruiting blood donors to increase the DEA 1– donor pool, as suggested previously (25, 42)
In contrast, the Dalmatians and Pugs in our survey were all DEA 1+, except for one Dalmatian. Also, the Labrador Retriever and Shih Tzu breeds had mostly DEA 1+ dogs. The predominance of DEA 1+ dogs in these breeds was also observed in recent surveys from Switzerland, South Africa, Portugal, and India (details in Supplement Table 4). Finally, the Maltese breed had a near equal proportion of DEA 1+ and DEA 1– dogs, as previously reported from another survey in Italy (31). Thus, these DEA 1 typing surveys show similar proportions of DEA 1+ and DEA 1– dogs in each breed worldwide, which is not surprising considering their common ancestors and international breeding practices within breeds.
The strength of DEA 1 expression in DEA 1+ dogs is similar to a prior survey from the USA (27). Equal proportions are either strongly DEA 1+ or DEA 1–. Only a fifth of dogs show weak or moderate DEA 1 expression, an important observation for clinical practice, as the latter may lead to difficulties in interpretation and, potentially, in sensitizing dogs. Indeed, even blood from a weakly DEA 1+ donor given to a DEA 1– dog can elicit the sustained production of anti-DEA 1 alloantibodies (38), and sensitized dogs may develop an acute hemolytic transfusion reactions when again transfused (14).
DEA 4 Typing
All dogs in this survey were typed as DEA 4+ by the Gel and Card. Only a few prior typing surveys included DEA 4 typing, and these studies also revealed that almost all dogs are DEA 4+, as DEA 4– dogs are extremely rarely observed (7, 16, 27, 30, 37, 39). Thus, while DEA 4 is known as a blood group system, it should be considered a high-frequency antigen, as less than 1% of dogs are DEA 4– (14, 43).
The new DEA 4 typing card test was easy to perform, but some results were challenging to interpret. Agglutination reactions on the Card were weaker than those observed with the Control on the Card or with the Gel. The addition of another 40 μl diluent enhanced the weak agglutination reactions, and this phenomenon might be caused by a Prozone-like effect, though this was not further studied. The varying degrees of agglutination reactions observed with the Cards remain unexplained but are likely technical, as all 158 dogs tested produced strongly positive (3+ to 4+) results by the Gel method. Optimization of the Card to increase agglutination reactions would enhance the reliability of this assay. In the meantime, the manufacturer has independently adjusted the protocol based upon our observations.
Because the instructions are identical to DEA 1 typing cards, the DEA 4 cards can be readily added to the typing repertoire in clinical practice. The DEA 4 typing cards may be particularly useful for clinical diagnostics of incompatibility reactions in previously transfused DEA 4– dogs and for identifying DEA 4– donors. Indeed, early experimental studies (8) reported blood incompatibilities caused by DEA 4+ alloantibodies, and there is one clinical case report of an acute hemolytic transfusion reaction after the dog had been sensitized by a prior DEA 4+ transfusion (4). Thus, identifying DEA 4– donors could be very valuable when facing broad blood incompatibilities in previously transfused dogs potentially caused by DEA 4 sensitization.
DEA 5 Typing
In this survey from Germany, we found 9 and 11% DEA 5+ dogs with the Card and Gel, respectively. Similarly, a limited survey from the Netherlands identified 17% DEA 5+ (44), and other surveys from North America found 12–25% DEA 5+ dogs (14, 16). Although DEA 5 has been associated with blood type incompatibilities and reduced RBC lifespan experimentally (8), there are no clinical reports of any acute hemolytic transfusion reactions related to DEA 5. The new DEA 5 typing cards will be useful in the practical diagnostic examination of blood type incompatibilities and acute hemolytic transfusion reactions in previously transfused dogs.
Finally, the new commercially available DEA 4 and DEA 5 typing cards used in this survey produced similar but weaker agglutination results to the gel column method. Moreover, the agglutinations were weaker than seen with the commonly used DEA 1 cards. Nevertheless, there was a strong correlation between the two methods, with only five discordant DEA 5 typing results, supporting their use in clinical settings.
Dal Typing
While original reports suggested that the Dal– blood type was exclusive to Dalmatians (11), recent studies from North America also found Dal– dogs in other breeds (27, 29, 36). Similarly, our survey from Germany found 10.7% Dal– dogs. This includes dogs from breeds with previously described Dal– dogs like Dalmatians, Dobermans, Shih Tzu, and Lhasa Apso (27, 29, 36), and also, for the first time, in Cane Corsos, Pugs, and a Mastiff. The prevalence of Dal– dogs in specific breeds is difficult to compare, because of the small numbers of dogs in each breed typed and reported geographical differences in the prevalence of Dal (29). Clearly, Dal typing is warranted for those breeds as well as for additional breeds, as Dal type blood incompatibility could potentially lead to an acute hemolytic transfusion reaction (29). Thus, it would be beneficial to identify Dal– donors for use in Dal– patients. Unfortunately, at this point, there is no commercial Dal typing kit available.
While the Gel uniformly showed strong (3+/4+) agglutination reactions with Dal+ blood, there was one dog that was receiving long-term treatment with immunosuppressives that had only a 2+ reaction. It may be possible that immunosuppression reduces the expression of the Dal antigen or the binding with the antibody. Differences in antigen expression have been shown in humans with illnesses (45) and were suspected in FeLV+ cats (46).
Kai 1 and Kai 2 Typing
Utilizing the Gel, the agglutination reactions were very strong for Kai 1 and Kai 2. In this survey, 96.6% of all dogs were Kai 1+/Kai 2–, and few dogs were Kai 1– and Kai 2+ or Kai 2–. Thus, our results for the Kai 1 /Kai 2 blood type pattern distribution were similar to a prior survey from North America, which found 94% Kai 1+/Kai 2–, 5% Kai 1–/Kai 2–, and 1% Kai 1–/Kai 2+ (27). In a recent survey using the conventional tube agglutination assay with 203 mostly Mastiff dogs from South Korea, the proportion of Kai 1+/Kai 2– was only 42%, with the proportion of Kai 1–/Kai 2+ being 37% and that of Kai 1–/Kai 2– being 20% (12). The large group of Kai 1–/Kai 2+ Mastiffs seen in Korea could not be substantiated here and in the survey from North America because of a lack of samples received from this breed. Noteworthy, however, is the absence of dogs that were Kai 1+ as well as Kai 2+. While the Kai 1 and Kai 2 antigens appear to be very different based on protein size (12), it cannot be excluded that these two antigens are genetically related.
Finally, several Lhasa Apsos were found to be Kai 1– /Kai 2+ in the United Kingdom (Watson et al., personal communication). Because the only other Kai 1–/Kai 2+ dog was a Maltese and another Maltese was Kai 1–/Kai 2–, it is possible that these two related breeds of the FCI Group 9 are unique regarding their Kai antigen expressions.
However, the clinical importance of the Kai 1 and Kai 2 blood groups needs to be further investigated, especially since the development of alloantibodies against Kai 1 and Kai 2 in previously transfused dogs has been reported (12).
Limitations
Although this is the first published survey for Dal, Kai 1, and Kai 2 in Europe, it was primarily limited to Germany geographically. While over 200 dogs were typed for many blood types, the reported blood type prevalences for each breed are still limited by sample size. The prevalences could well be impacted if more dogs are typed and/or if dogs from other geographic regions are included. Because several reagents for typing are not readily available, and the clinical importance of some of the blood types tested has not been established, larger surveys are unlikely to be done.
This study was performed under strict laboratory conditions in a reference diagnostic laboratory, with the same trained personnel (AE, SF) performing all the tests and with appropriate control samples. Typing conditions in private practice are likely to be less favorable, and weak agglutination and binding reactions will be difficult to interpret. When uncertain, blood samples should be sent to a reference laboratory for retyping and potentially back-typing if possible.
Notably, this study did not evaluate the presence of naturally occurring alloantibodies in any dogs. However, the presence of naturally occurring alloantibodies has been evaluated in prior studies (12, 15, 16, 27, 29, 30), and they do not appear to cause acute hemolytic transfusion reactions when transfusing a dog for the first time (1, 8). Specific alloantibody studies of plasma or serum from previously transfused dogs, which were extensively typed as in this survey, would be of interest, although only rarely is a known RBC antigen identified to cause a hemolytic transfusion reaction (3, 4, 14).
This study excluded typing for DEA 7, because commercial reagents were not available at the time this survey was performed, and in the past, the available typing reagents have given DEA 7 typing and alloantibody results that have been difficult to reproduce (27). Therefore, the presence of naturally occurring anti-DEA 7 alloantibodies and their importance in eliciting an acute hemolytic transfusion reaction independent of whether a dog was previously transfused or not remains unclear (7, 8, 14, 15, 42, 43).
Conclusions
The options for extended in-house typing, including the two now commercially available DEA 4 and DEA 5 cards, may be especially useful in previously transfused dogs, as well as in blood incompatibility work-up in a practice setting. While in-house typing reduces the turnaround time, tests should always be performed by trained personnel and, in the case of uncertain results, retyping and back-typing should be performed in a reference laboratory. Additional typing for Dal and Kai 1/2 with the Gel method should remain restricted to reference laboratories for now.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
Ethical review and approval was not required for the animal study because only leftover EDTA blood samples sent for routine diagnostic work were used. Approval for further use of surplus material is given when submitting to Laboklin as stated in the Laboklin policy.
Author Contributions
AE performed typing, data analysis, and manuscript writing. SF performed tests and sample preparation. CW gathered samples, provided demographic data, and reviewed the manuscript. EM contributed to the concept, funding, material acquisition, and manuscript review. UG contributed to the concept of the study, material acquisition, data analysis, and manuscript writing.
Funding
The authors declare that this study received funding from Alvedia, Limonest, France, and DMS Laboratories Inc., Flemington, NJ, USA, as well as the National Institutes of Health OD010939 (UG): Alvedia and DMS provided reagents for this study, and NIH supported in part UG. None of these funders were involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of Interest
The authors declare that they are associated with either the Laboklin GmbH ' Co KG, Kissingen, Germany or PennGen Laboratory, University of Pennsylvania, Philadelphia, PA, USA. Both offer blood typing services. This survey is part of AE's doctoral thesis at the University of Zürich, Switzerland, with UG being her mentor. Laboklin provided the workplace and doctoral fellowship of AE and was involved in the study; the study received funding from Laboklin and was executed at Laboklin GmbH ' Co KG, Kissingen and Radolfzell, Germany, but was performed independently from Laboklin's routine laboratory work.
Acknowledgments
We thank the team in Radolfzell and Bad Kissingen, Germany for their assistance, Dr. He Young Kim, South Korea for gifting the anti-Kai 1 and anti-Kai 2 alloantibodies, and Alvedia, Limonest, France for kindly providing DEA 1 kits and DMS, Flemington, New Jersey, USA for kindly providing DEA 4 and DEA 5 kits and alloantibody reagents.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fvets.2020.00085/full#supplementary-material
Abbreviations
Card, agglutination card (RapidVet-H DEA 4 Agglutination Card Test and DEA 5 Card RapidVet-H DEA 5 Agglutination Card Test, DMS, Flemington, NJ, US); DEA, dog erythrocyte antigen; EDTA, ethylene-diaminetetraacetic acid; FCI, Federation Cynologique Internationale; Gel, gel column method (BioRad ID-Cards, NaCl, Enzyme Test and Cold Agglutinins, DiaMed); RBC, red blood cell; Strip, immunochromatographic strip technique (Alvedia, Lab Test DEA 1, Limonest, France).
Footnotes
References
1. Giger U. Blood typing and crossmatching to ensure blood compatibility. In: Bonagura JD, Twedt DC editors. Kirk's Current Veterinary Therapy, 15th Ed. St. Louis, MO: WB Saunders (2014). Web Chapter 26:143.
2. Hohenhaus AE. Importance of blood groups and blood group antibodies in companion animals. Transfus Med Rev. (2004) 18:117–26. doi: 10.1016/j.tmrv.2003.12.003
3. Callan MB, Jones LT, Giger U. Hemolytic transfusion reactions in a dog with an alloantibody to a common antigen. J Vet Intern Med. (1995) 9:277–9. doi: 10.1111/j.1939-1676.1995.tb01080.x
4. Melzer KJ, Wardrop KJ, Hale AS, Wong VM. A hemolytic transfusion reaction due to DEA 4 alloantibodies in a dog. J Vet Intern Med. (2003) 17:931–3. doi: 10.1111/j.1939-1676.2003.tb02536.x
5. Ottenberg R, Kaliski DJ, Friedman SS. Experimental agglutinative and hemolytic Transfusions. J Med Res. (1913) 28:141–63.
6. Tocci LJ, Ewing PJ. Increasing patient safety in veterinary transfusion medicine: an overview of pretransfusion testing. J Vet Emerg Crit Care. (2009) 19:66–73. doi: 10.1111/j.1476-4431.2009.00387.x
7. Hale AS. Canine blood groups and their importance in veterinary transfusion medicine. Vet Clin North Am Small Anim Pract. (1995) 25:1323–32.
8. Swisher SN, Young LE. The blood grouping systems of dogs. Physiol Rev. (1961) 41:495–520. doi: 10.1152/physrev.1961.41.3.495
9. Symons M, Bell K. Expansion of the canine A blood group system. Anim Genet. (1991) 22:227–35. doi: 10.1111/j.1365-2052.1991.tb00672.x
10. Vriesendorp HM, Albert ED, Templeton JW, Belotsky S, Taylor B, Blumenstock DA, et al. Joint report of the second international workshop on canine immunogenetics. Transplant Proc. (1976) 8:289–314.
11. Blais MC, Berman L, Oakley DA, Giger U. Canine Dal blood type: a red cell antigen lacking in some Dalmatians. J Vet Intern Med. (2007) 21:281–6. doi: 10.1892/0891-6640(2007)21[281:cdbtar]2.0.co;2
12. Lee JH, Giger U, Kim HY. Kai 1 and Kai 2: Characterization of these dog erythrocyte antigens by monoclonal antibodies. PLoS ONE. (2017) 12:e0179932. doi: 10.1371/journal.pone.0179932
13. Wardrop KJ. New red blood cell antigens in dogs and cats–a welcome discovery. J Vet Intern Med. (2007) 21:205–6. doi: 10.1111/j.1939-1676.2007.tb02949.x
14. Giger U, Gelens CJ, Callan MB, Oakley DA. An acute hemolytic transfusion reaction caused by dog erythrocyte antigen 1.1 incompatibility in a previously sensitized dog. J Am Vet Med Assoc. (1995) 206:1358–62.
15. Spada E, Proverbio D, Baggiani L, Canzi I, Perego R. Activity, specificity, and titer of naturally occurring canine anti-DEA 7 antibodies. J Vet Diagn Invest. (2016) 28:705–8. doi: 10.1177/1040638716668626
16. Blais MC, Rozanski EA, Hale AS, Shaw SP, Cotter SM. Lack of evidence of pregnancy-induced alloantibodies in dogs. J Vet Intern Med. (2009) 23:462–5. doi: 10.1111/j.1939-1676.2009.0286.x
17. Young LE, Christian RM, Ervin DM, Davis RW, O'Brien WA, Swisher SN, et al. Hemolytic disease in newborn dogs. Blood. (1951) 6:291–313.
18. Corato A, Mazza G, Hale AS, Barker RN, Day MJ. Biochemical characterization of canine blood group antigens: immunoprecipitation of DEA 1.2, 4 and 7 and identification of a dog erythrocyte membrane antigen homologous to human Rhesus. Vet Immunol Immunopathol. (1997) 59:213–23.
19. Acierno MM, Raj K, Giger U. DEA 1 expression on dog erythrocytes analyzed by immunochromatographic and flow cytometric techniques. J Vet Intern Med. (2014) 28:592–8. doi: 10.1111/jvim.12321
20. Polak K, Acierno MM, Raj K, Mizukami K, Siegel DL, Giger U. Dog erythrocyte antigen 1: mode of inheritance and initial characterization. Vet Clin Path. (2015) 44:369–79. doi: 10.1111/vcp.12284
21. Blois SL, Richardson DM, Abrams-Ogg AC. Comparison of a gel column blood typing method and a point-of-care cartridge for dog erythrocyte antigen 1.1. J Vet Emerg Crit Care. (2013) 23:340–3. doi: 10.1111/vec.12052
22. Davidow B. Transfusion medicine in small animals. Vet Clin North Am Small Anim Pract. (2013) 43:735–56. doi: 10.1016/j.cvsm.2013.03.007
23. Kohn B, Classe G, Weingart C. Clinical evaluation of the QuickVet/RapidVet canine dog erythrocyte antigen 1.1 blood-typing test. J Vet Diagn Invest. (2012) 24:539–45. doi: 10.1177/1040638712442880
24. Seth M, Jackson KV, Winzelberg S, Giger U. Comparison of gel column, card, and cartridge techniques for dog erythrocyte antigen 1.1 blood typing. Am J Vet Res. (2012) 73:213–9. doi: 10.2460/ajvr.73.2.213
25. Carli E, Carminato A, Ravagnan S, Capello K, Antognoni MT, Miglio A, et al. Frequency of DEA 1 antigen in 1037 mongrel and purebred dogs in Italy. BMC Vet Res. (2017) 13:364. doi: 10.1186/s12917-017-1286-y
26. Ergul Ekiz E, Arslan M, Ozcan M, Gultekin GI, Gulay OY, Kirmizibayrak T, et al. Frequency of dog erythrocyte antigen 1.1 in 4 breeds native to different areas in Turkey. Vet Clin Path. (2011) 40:518–23. doi: 10.1111/j.1939-165X.2011.00370.x
27. Euler CC, Lee JH, Kim HY, Raj K, Mizukami K, Giger U. Survey of two new (Kai 1 and Kai 2) and other blood groups in dogs of North America. J Vet Intern Med. (2016) 30:1642–7. doi: 10.1111/jvim.14572
28. Ferreira RR, Gopegui RR, Matos AJ. Frequency of dog erythrocyte antigen 1.1 expression in dogs from Portugal. Vet Clin Path. (2011) 40:198–201. doi: 10.1111/j.1939-165X.2011.00311.x
29. Goulet S, Giger U, Arsenault J, Abrams-Ogg A, Euler CC, Blais MC. Prevalence and mode of inheritance of the Dal blood group in dogs in North America. J Vet Intern Med. (2017) 31:751–8. doi: 10.1111/jvim.14693
30. Kessler RJ, Reese J, Chang D, Seth M, Hale AS, Giger U. Dog erythrocyte antigens 1.1, 1.2, 3, 4, 7, and Dal blood typing and cross-matching by gel column technique. Vet Clin Path. (2010) 39:306–16. doi: 10.1111/j.1939-165X.2010.00249.x
31. Medina Valentin AA, Gavazza A, Lubas G. Prevalence of dog erythrocyte antigen 1 in 7,414 dogs in Italy. Vet Med Int. (2017) 2017:5914629. doi: 10.1155/2017/5914629
32. Mesa-Sanchez I, Ruiz de Gopegui-Fernandez R, Granados-Machuca MM, Galan-Rodriguez A. Prevalence of dog erythrocyte antigen 1.1 in galgos (Spanish greyhounds). The Vet R. (2014) 174:351. doi: 10.1136/vr.102087
33. Riond B, Schuler E, Rogg E, Hofmann-Lehmann R, Lutz H. Prevalence of dog erythrocyte antigen 1.1 in dogs in Switzerland evaluated with the gel column technique. Schweiz Arch Tierheilkd. (2011) 153:369–74. doi: 10.1024/0036-7281/a000223
34. Spada E, Proverbio D, Vinals Florez LM, Serra Gomez de la Serna B, Del Rosario Perlado Chamizo M, Baggiani L, et al. Prevalence of dog erythrocyte antigens 1, 4, and 7 in Podenco Ibicenco (Ibizan Hounds) from Ibiza Island. Vet Med Int. (2016) 2016:1048257. doi: 10.1155/2016/1048257
35. van der Merwe LL, Jacobson LS, Pretorius GJ. The breed prevalence of dog erythrocyte antigen 1.1 in the Onderstepoort area of South Africa and its significance in selection of canine blood donors. J South Afri Vet Assoc. (2002) 73:53–6.
36. Goulet S, Blais MC. Characterization of anti- Dal alloantibodies following sensitization of two Dal-negative dogs. Vet P. (2018) 55:108–15. doi: 10.1177/0300985816688746
37. Goy-Thollot I, Giger U, Boisvineau C, Perrin R, Guidetti M, Chaprier B, et al. Pre- and post-transfusion alloimmunization in dogs characterized by 2 antiglobulin-enhanced cross-match tests. J Vet Intern Med. (2017) 31:1420–9. doi: 10.1111/jvim.14801
38. Guidetti M, Goy-Thollot I, Boisvineau C, Giger U. Alloimmunization of a dog erythrocyte antigen 1- dog transfused with weakly dog erythrocyte antigen 1+ blood. J Vet Intern Med. (2019) 33:2037–45. doi: 10.1111/jvim.15565
39. Giger U, Stieger K, Palos H. Comparison of various canine blood-typing methods. Am J Vet Res. (2005) 66:1386–92. doi: 10.2460/ajvr.2005.66.1386
40. Baranidharan G, Dhanan J, Prathaban S, Nambi A, Lubas G, Medina Valentin A. Prevalence of dog erythrocyte antigen (DEA) 1 amongst the dog blood donors at Tamil Nadu veterinary and animal sciences university animal blood bank (TABB), India. Hematol Transf Intern J. (2018) 6:47–49. doi: 10.15406/htij.2018.06.00151
41. Dhliwayo S, Makonese TA, Whittall B, Chikerema SM, Pfukenyi DM, Tivapasi MT. A study on the prevalence of dog erythrocyte antigen 1.1 and detection of canine Babesia by polymerase chain reaction from apparently healthy dogs in a selected rural community in Zimbabwe. J South Afric Vet Assoc. (2016) 87:e1–5. doi: 10.4102/jsava.v87i1.1409
42. Spada E, Proverbio D, Priolo V, Ippolito D, Baggiani L, Perego R, et al. Dog erythrocyte antigens (DEA) 1, 4, 7 and suspected naturally occurring anti-DEA 7 antibodies in Italian corso dogs. Vet J. (2017) 222:17–21. doi: 10.1016/j.tvjl.2017.02.008
43. Swisher SN, Young LE, Trabold N. In vitro and in vivo studies of the behavior of canine erythrocyte- isoantibody systems. Ann N Y Acad Sci. (1962) 97:15–25. doi: 10.1111/j.1749-6632.1962.tb34618.x
44. Vriesendorp HM, Westbroek DL, D'Amaro J, van der Does JA, van der Steen GJ, van Rood JJ, et al. Joint report of 1st international workshop on canine immunogenetics. Tissue Antigens. (1973) 3:145–63.
45. Nambiar RK, Narayanan G, Prakash NP, Vijayalakshmi K. Blood group change in acute myeloid leukemia. Bayl Univ Med Cent Proc. (2017) 30:74–5. doi: 10.1080/08998280.2017.11929536
Keywords: blood type, blood compatibility, transfusion reaction, polymorphism, alloantibodies, dog
Citation: Ebelt AK, Fuchs S, Weber C, Müller E and Giger U (2020) Survey of Blood Groups DEA 1, DEA 4, DEA 5, Dal, and Kai 1/Kai 2 in Different Canine Breeds From a Diagnostic Laboratory in Germany. Front. Vet. Sci. 7:85. doi: 10.3389/fvets.2020.00085
Received: 11 December 2019; Accepted: 04 February 2020;
Published: 28 February 2020.
Edited by:
Eva Spada, University of Milan, ItalyReviewed by:
Roberta Perego, University of Milan, ItalyAna Cristina Silvestre Ferreira, University of Trás-os-Montes and Alto Douro, Portugal
Copyright © 2020 Ebelt, Fuchs, Weber, Müller and Giger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Urs Giger, Z2lnZXJAdXBlbm4uZWR1