 Daniel S. J. Pang
Daniel S. J. Pang Frédérik Rousseau-Blass
Frédérik Rousseau-Blass- Department of Clinical Sciences, Faculty of Veterinary Medicine, Université de Montréal, Saint-Hyacinthe, QC, Canada
This mini review presents current knowledge on the role of morbidity and mortality conferences (M&MCs) as a powerful educational tool and driver to improve patient care. Although M&MCs have existed since the early twentieth century, formal evaluation of their impact on education and patient care is relatively recent. Over time, M&MCs have evolved from single discipline discussions with a tendency to focus on individual errors and assign blame, to multidisciplinary, standardized presentations incorporating error analysis techniques, and educational theory. Current evidence shows that M&MCs can provide a valuable educational experience and have the potential to generate measurable improvements in patient care.
Introduction
Adverse events, defined as a complication caused by medical management and resulting in patient harm, are an unfortunately common occurrence in hospitalized human patients (1–5). While estimates vary depending on the outcome(s) used to define adverse events, up to 4% of all hospitalized human patients will experience a serious negative outcome (prolonged hospital stay, disability at discharge, or death) (1, 2). Importantly, half of all adverse events are preventable (1, 2, 4, 5). As a result, there is room for substantial improvement in patient outcomes through better care (2–5).
The potential for adverse events to drive improved patient care and safety, and serve as a valuable educational resource, has long been recognized in human medicine (6–9). Since their inception in the first half of the twentieth century, morbidity and mortality conferences (M&MCs, also known as M&M rounds and reviews) have been the mechanism to achieve these outcomes, and they are implemented in a wide range of medical specialties, most notably surgery and anesthesia (7, 9). Their use is now mandated by the Accreditation Council for Graduate Medical Education in human medicine and is part of the Practice Standards Scheme of the Royal College of Veterinary Surgeons (10, 11).
Fittingly described as familiar yet lacking a clear definition, at a fundamental level M&MCs comprise of caregivers gathering to review adverse events, with the goals of education and improving care (7). In principle, M&MCs should provide an open forum for the collaborative review of adverse events without fear of retribution or blame. The primary goals should be improving patient care and maximizing the educational benefits of a shared experience (6, 12–14). These can be achieved through: presentation and acknowledgment of error(s) [defined as performance that deviates from the ideal; failure to carry out a planned action as intended (error of execution), or the use of an incorrect or inappropriate plan (error of planning)], analysis and discussion of adverse events and contributing factor(s), identification of means for improvement, dissemination of information, and reinforcement of responsibility to provide best practice standard of care (7, 15–17). In practice, however, M&MCs are often poorly defined in terms of format, goals, and outcomes (7, 18, 19). Learning from errors through reflection and discussion is essential to improve practice, though where this is done ineffectually, or with the emphasis on assigning blame, M&MCs fail to be productive (7, 13, 20).
While there is a large body of literature supporting and advocating the use of M&MCs, their efficacy in terms of measurable outcomes has, until recently, been largely untested. Increasing evidence suggests that a structured, transparent approach to M&MCs results in measurable gains in user satisfaction and participation, education, patient safety, quality of care, and mortality (13, 15, 21–25). This mini review will discuss the demonstrated benefits of M&MCs and available evidence on their optimal format.
Benefits
Education
Despite their long history, it has only been relatively recently that prospective trials have been conducted to evaluate the educational contribution of M&MCs (15, 19, 21, 24, 26). These studies have developed and tested structured approaches to M&MCs, encompassing case reporting and selection, analysis of adverse events, presentation, participation, and learning outcomes.
Implementation of a standardized presentation format significantly improved the number of correct responses to multiple choice questions completed at the end of each M&MC and presentation quality (15). The same group had previously developed an M&MC presentation assessment tool using psychometric principles that was feasible (taking <10 min to complete), reliable (high-internal consistency and inter-rater agreement), and valid (construct validity), thus allowing presenters and presentation content to be objectively evaluated (21).
In a large pediatric anesthesia service (approximately 18,000 anesthetics per year), McDonnell et al. sought to improve an overburdened and inefficient M&M system that was associated with a culture of blame and lost educational opportunities (19). M&MCs held following restructuring of the reporting mechanism and focusing case selection on educational potential identified multiple areas for improvement, including situations more commonly associated with adverse events (e.g., fluid management and transfusion, emergent exploratory laparotomies), equipment contributions to error, and wider dissemination of information. These were addressed with targeted educational sessions, equipment changes (e.g., replacement of inaccurate atomizers for local anesthetic delivery with syringes and compatible catheters), and presentation of cases at national meetings and as published case reports, respectively (19).
Similarly, as a result of improved case selection and error analysis, Calder et al. showed that succinct recommendations (“M&M Bottom Lines”) could be generated from M&MCs, providing participants with a memorable message that could improve personal practice and be easily disseminated (e.g., “Find one fracture, look for the next one”) (24).
Satisfaction and Participation
Mandatory attendance of M&MCs is commonly reported in the literature as a requirement of training (6, 7, 12, 15, 19, 27, 28). In moving to a mandatory M&MC system, McDonnell et al. increased M&MC attendance fivefold (19). Interestingly, this action built the habit of attendance, so that when M&MCs were eventually separated in to their own regular schedule, attendance rates were maintained. Mitchell et al. (15) showed that the adoption of a structured presentation [situation, background, assessment, recommendations (SBAR), presented in detail below] was associated in increased user satisfaction, compared with variable presentation formats decided by individual presenters (17).
Patient Safety
Several studies have reported improvements in patient safety following the presentation of cases at M&MCs and subsequent changes in patient care and management (12, 13, 22, 25, 26, 29, 30). A common theme of these reports is the clear structure to the M&MC process, though the degree and extent of standardization varied. Some studies focused on identifying and enacting mechanisms for improvement coupled with continuous monitoring of progress (12, 13, 20, 25, 29), while others focused on the care pathway (12, 29), standardized presentation, and error analysis (12, 13).
These varied approaches have resulted in a 50% reduction in malpractice claims (20), improved safety culture and quality of care (20, 25, 29, 30), and reductions in mortality of up to 40% (12, 13, 29). Data should be collected prospectively before as well as after implemented changes in management to properly establish the relationship between enacted changes and outcome. Clinical audit, a core element of clinical governance, is an invaluable tool to monitor adherence to changes in practice and related outcomes (31–34). Furthermore, standardization of data collection is a prerequisite for collaborative efforts to assess the impact of proposed changes in care (35).
Within the broader context of patient safety, M&MCs can be viewed as one of a suite of techniques and tools to report, analyze, and prevent errors (36–39). As such, M&MCs should not be applied in isolation but be included in an organizational approach to error management. It is interesting to note that well-managed M&MCs have the potential to encompass several of the key components of improving patient safety: a reporting system, error analysis using a human factors approach, education, and risk reduction. A discussion of error and patient safety is beyond the scope of this Mini Review. Interested readers are referred to reference texts (36, 38, 40, 41).
M&MC Format
Publicly disclosing and discussing an adverse event is a difficult process. All M&MCs comprise components that can be optimized to yield the greatest benefit from such a process. The general structure described in this section follows that of two models whose performance has been evaluated prospectively and shown to be effective: the Ottawa M&M model (OM3) and the SBAR model (15, 21, 24). A fictionalized account of a clinical case is used to illustrate the individual components.
Case Reporting and Selection
Under-reporting of adverse events can stem from lack of awareness of an available reporting system, be it formal or informal, or the inability to submit an anonymous report. Educating new staff members to the existence and use of a reporting system and requiring all submissions be through a single hospital-wide database improves the capture of adverse events, with an increase in the total number of reports and self-reports (19).
In general, all cases of mortality should be reviewed with an M&MC, though this is not always the case (42). In some centers, deaths resulting from the natural progression of a condition are not reviewed (30). In cases where morbidity has occurred as a result of an adverse event, not all cases may progress to an M&MC or meet the threshold for review at an M&MC (7, 19, 24). In large centers, the number of reported cases can outstrip the time and resources available to hold M&MCs. There are several possibilities for handling these cases:
1. Include such cases in the institutional reporting system, where they can serve to highlight a trend of complications or collected by theme (e.g., drug calculation errors) and presented as a group.
2. Hold a smaller M&MC restricted to the discipline in which the error occurred.
3. Address failures in individual performance with the appropriate supervisor. When an error has occurred as a result of a deviation from a well-established procedure and has not resulted in an adverse event, the case may not meet the criteria for presentation at an M&MC. An example is provided below:
A dog was given a 10x intravenous overdose of the alpha-adrenergic agonist dexmedetomidine as a result of a drug calculation error by a veterinary student. Standard practice at the clinic was for all student drug calculations (and injectate volumes) to be checked by a veterinary technician before injection. In this case, the error occurred as standard practice was circumvented with the intention to save time. The error was realized within 3 minutes of the injection occurring, the dog was immediately examined, atipamezole was given and the dog was placed under clinical observation for 6 hours. The case was reviewed the same day with the individuals directly involved and the supervising anesthetist.
Such a near-miss incident (no harm resulted as a result of timely intervention or chance) may not proceed to an M&MC but should be recorded in case a pattern of similar events is occurring and to reinforce individual accountability.
Where case selection is necessary, it should be based on the greatest benefit to future patient safety and educational value (19, 24). Cases should be presented and discussed soon after they occur. There is no evidence in support of a specific time frame, but early presentation reinforces the importance of timely acknowledgment of an adverse event (7, 29). In large centers, the establishment of an M&M committee and coordinators facilitates efficient handling of reports and cases are typically presented within 4–8 weeks of reporting (19, 24, 29).
If there is reluctance to participate in, or convene M&MCs, an option to encourage participation is to initially select cases of near-miss incidents. Selecting such a case is still valuable in terms of improving care and providing education by allowing participants to analyze the factors contributing to the event (see root cause analysis, below), make recommendations to avoid similar incidents and learn from the experience.
M&MC Duration and Frequency
The duration of M&MCs is often unreported though is likely to be a function of available time (e.g., over lunch) and the number of cases to be discussed. Reported durations have ranged from 20 min (15 min presentation plus 5 min discussion) to over an hour (6, 15, 21, 28, 30, 42, 43). The OM3 and SBAR models last 1 h and 20 min, respectively.
Similarly, frequency of M&MCs is highly variable, with a monthly interval being a common frequency reported in the literature (3, 7, 12, 18–20, 23–25, 28–30, 42, 43).
Moderator
The moderator should be familiar with the M&MC format, principles of error analysis and have sufficient content expertise to guide the presenter during preparation and the audience in participation and have the authority to establish the desired tone, creating an open, collaborative, and supportive discussion without minimizing or magnifying the error (14, 24, 44).
Presenter
Typically, M&MCs are presented by a clinician directly involved in the case, though whether this is a trainee or senior clinician may vary depending on the complexity of the case and frequency of presentations (18, 24). In programs where presentations are given by trainees, it is important that senior personnel show support in the form of attendance, setting the appropriate tone for discussion, and sharing their experiences (7). Cases may be presented by someone external to the case though those involved with the case should have the option to present (7, 18). If the responsible clinicians are unable to attend, the tone of the M&MC should be the same as though they were present (7).
Attendees/Audience
Audience composition is highly variable, though a multidisciplinary approach is strongly favored, as this enriches the discussion and maximizes dissemination of information (7, 18, 28–30, 42, 44). An inclusive approach has been advocated to include care staff, having the added benefit of fostering an open safety culture (12, 29, 30, 45).
Presentation Format
There are few formats for M&MCs presented in the literature and this has been cited as a limiting factor in maximizing the educational opportunity and unbiased case analysis (7, 15, 18, 21). Consequently, recent work has focused on developing and assessing a standardized M&MC presentation format, the SBAR model (Table 1) (21, 25). Communication using SBAR is an example of situational briefing, to efficiently transfer critical information between team members who may occupy different levels in organization hierarchy (46, 47). As described earlier, the SBAR format has educational benefits for attendees and presenters (15, 21).
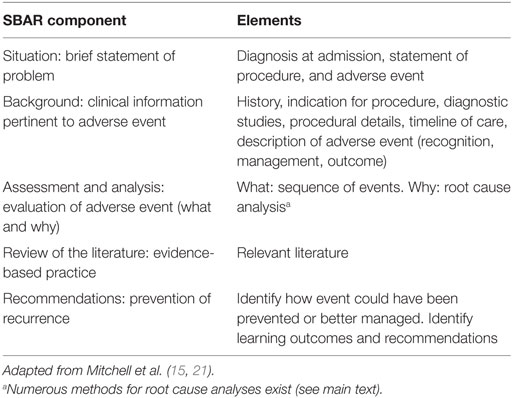
Table 1. The situation, background, assessment, recommendations (SBAR) presentation format for morbidity and mortality conferences.
Root Cause Analysis
The objective of root cause analysis is to identify factors contributing to an adverse event. Several methods have been reported in the M&MC literature, with the common goal of gaining a deeper understanding of the circumstances surrounding an adverse event (13, 15, 21, 25, 43, 45, 48, 49). The method presented here is the fishbone diagram (also known as, cause and effect, Ishikawa, or Fishikawa diagram). It is recommended for process improvement as it provides a visual framework for analysis and discussion and is one of the seven basic quality control tools (Figure 1) (50). The adverse event represents the “head” of the fish and each bone represents a potential contributing factor. The example included in Presentations S1 and S2 in Supplementary Material is based on the work of reason (40, 41) though other, more detailed approaches exist (39). The order and position of individual factors is unrelated to any priority; it may be that a sub-factor is a major contributing factor. A small group discussion may be helpful to determine the role, if any, of each factor, with the group formed by the individual(s) most closely involved with the adverse event and a senior team member with understanding of error analysis. In making these determinations questioning why things occurred, using a “five whys” approach, can be useful (50):
1. Describe the problem.
2. Ask “why” it happened.
3. Continue to ask “why” until the root cause is identified (may take more or less than five “whys”).
4. Maintain a focus on the process and not the personalities.
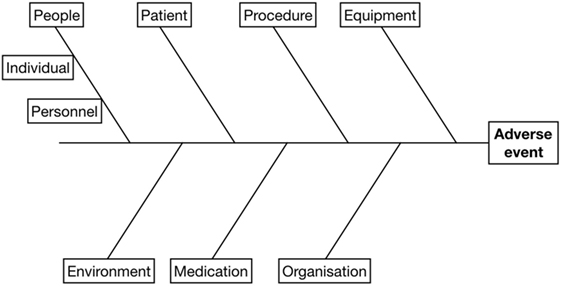
Figure 1. Fishbone diagram used to facilitate root cause analysis. The adverse event is listed at the “head” and potential contributory factors are examined to establish a cause and effect relationship. See Presentations S1 and S2 in Supplementary Material for an example.
In maintaining a non-punitive environment for M&MCs, it is critical that causes are based on fact (and evidence) rather than opinion. As illustrated with the sample case (below), there are likely to be multiple factors contributing to an adverse event. Identifying these factors facilitates a complete discussion and identifies potential solutions.
Follow-up
Where recommendations have resulted in changes in practice, relevant outcomes should be tracked to ensure that changes are beneficial and do not lead to unexpected negative consequences. Tracking has been successfully employed to identify improvements in mortality rates and patient care (as described earlier) (12, 13, 20, 25, 29, 30). Clinical audit is a suitable method for tracking performance that is easy to institute (51). Where a system or infrastructure deficit has been identified as a major contributing factor to the adverse event, the appropriate member of leadership (e.g., hospital director) should be notified so the deficit(s) can be addressed. A recent survey of surgical residency programs registered with the American College of Veterinary Surgeons suggests that in the majority of cases (26/35 programs, survey response rate 32%), discussions do not translate in to implemented changes in practice or changes are not tracked to assess outcome (42).
Conclusion
Current evidence shows that a structured M&MC with a standardized presentation format and root cause analysis, and tracking of outcomes, serves as a valuable educational experience with the greatest potential to improve patient safety and quality of care. The described approaches can easily be adopted and applied in veterinary medicine.
Sample Case
Case Selection
A 10-year old, warmblood mare experienced pronounced acute hypoxemia during recovery from general anesthesia for bilateral thoracic limb magnetic resonance imaging (MRI). This case was selected for presentation at an M&MC as it contained multiple factors contributing to an adverse event and illustrated an important perturbation of normal physiology during anesthesia. Case selection was made following an initial case review between an anesthesia resident and supervisor.
Presenter and Moderator
The presenter (first year anesthesia resident) was directly involved in the case. The moderator was a senior anesthetist with detailed knowledge of the case.
Audience
The invited audience included equine interns (mandatory participation), residents (mandatory participation), clinicians, and faculty. All final year veterinary students rotating through the equine hospital and student members of the faculty equine club were also invited. The audience included board-certified internists, theriogenologists, surgeons, and anesthesiologists, and a representative anesthesia technician. Approximately 30 people attended.
Presentation
The SBAR presentation format was used (Presentations S1 and S2 in Supplementary Material). Educational components were provided by presentation and discussion of the adverse event alongside a brief review of relevant respiratory physiology. Duration was set by the context of inclusion in a weekly graduate trainee seminar series and limited to 15 min presentation followed by 10 min discussion. The proportion of time allocated to the discussion was helpful to explore the contributing factors identified and generate recommendations. To set the tone for the presentation and discussion, the opening and closing presentation slides included a statement of the goal of the M&MC (Presentations S1 and S2 in Supplementary Material).
Root Cause Analysis (Contributing Factors Corresponding to the Fishbone Diagram Are Italicized)
Specific problem—horse became hypoxemic during recovery (confirmed with arterial blood gas analysis), which potentially began during transfer from MRI.
1. Why? Body position was changed from left to right lateral for transfer to recovery (procedure) and ventilation was inadequate (procedure or equipment) during transfer.
2. Why? There was confusion and unclear communication between different teams (anesthesia, radiology, animal handlers—people-personnel) and the endotracheal tube cuff was prematurely deflated limiting efficacy of positive pressure ventilation (people-individual).
3. Why? One anesthetist was managing multiple cases on both sides of the hospital (small and large animal, organization) and the anesthetist was not present at the start of transfer (people-individual & personnel).
4. Why? A second anesthetist was unavailable that morning (organization).
5. Why? This was a planned absence with an email circulated to service chiefs notifying them of short-staffing in anesthesia (organization).
Identified contributing factors were added to a fishbone diagram in Presentations S1 and S2 in Supplementary Material.
Follow-up
The equine hospital chief attends all equine M&MCs. Each of the fishbone factors was discussed. The role and responsibilities of different personnel were clarified. Recommendations: (1) A leader is designated to manage transfer. The senior anesthetist is ultimately responsible, but has power to delegate leadership if someone with specific expertise is present, such as senior animal handler. (2) Cases should not be transferred without permission of senior anesthetist. (3) Senior anesthetist has the right to delay or turn away elective cases, and cases may be stopped prematurely in the interests of patient safety. (4) A wider discussion of case transfer, with the potential to introduce a checklist or standard operating protocol, was planned.
Author Contributions
DP, FR-B, and JP concept and design, drafting and revising, final approval, and accountability for all aspects of the work.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors wish to acknowledge Dr. Jean-Pierre Lavoie’s championing of M&MCs at the equine hospital of the Centre Hospitalier Universitaire Vétérinaire, Université de Montréal.
Funding
DP receives funding from the Natural Sciences and Engineering Research Council of Canada Discovery Grant (424022-2013) and the Fondation J.-Louis Lévesque.
Supplementary Material
The Supplementary Material for this article can be found online at http://www.frontiersin.org/articles/10.3389/fvets.2018.00043/full#supplementary-material.
Presentation S1. Example of power point presentation given to accompany sample case (English).
Presentation S2. Example of power point presentation given to accompany sample case (Francais).
References
1. Gawande AA, Thomas EJ, Zinner MJ, Brennan TA. The incidence and nature of surgical adverse events in Colorado and Utah in 1992. Surgery (1999) 126:66–75. doi:10.1067/msy.1999.98664
2. Kohn LT, Corrigan JM, Donaldson MS, Committee on Quality of Health Care in America (Institute of Medicine). To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press (2000).
3. Ksouri H, Balanant PY, Tadié JM, Heraud G, Abboud I, Lerolle N, et al. Impact of morbidity and mortality conferences on analysis of mortality and critical events in intensive care practice. Am J Crit Care (2010) 19:135–45. quiz 146, doi:10.4037/ajcc2010590
4. Leape LL, Brennan TA, Laird N, Lawthers AG, Localio AR, Barnes BA, et al. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med (1991) 324:377–84. doi:10.1056/NEJM199102073240605
5. Vincent C, Moorthy K, Sarker SK, Chang A, Darzi AW. Systems approaches to surgical quality and safety: from concept to measurement. Ann Surg (2004) 239:475–82. doi:10.1097/01.sla.0000118753.22830.41
6. Higginson J, Walters R, Fulop N. Mortality and morbidity meetings: an untapped resource for improving the governance of patient safety. BMJ Qual Saf (2012) 21:576–85. doi:10.1136/bmjqs-2011-000603
7. Orlander JD, Barber TW, Fincke BG. The morbidity and mortality conference: the delicate nature of learning from error. Acad Med (2002) 77:1001–6. doi:10.1097/00001888-200210000-00011
8. Reverby S. Stealing the golden eggs: Ernest Amory Codman and the science and management of medicine. Bull Hist Med (1981) 55:156–71.
9. Ruth HS, Haugen FP, Grove DD. Anesthesia Study Commission; findings of 11 years’ activity. J Am Med Assoc (1947) 135:881–4. doi:10.1001/jama.1947.02890140001001
10. Accreditation Council for Graduate Medical Education. (2017). Available from: http://www.acgme.org/What-We-Do/Initiatives/Clinical-Learning-Environment-Review-CLER
11. Royal College of Veterinary Surgeons Practice Standards Scheme. (2017). Available from: https://www.rcvs.org.uk/setting-standards/practice-standards-scheme/
12. Kirschenbaum L, Kurtz S, Astiz M. Improved clinical outcomes combining house staff self-assessment with an audit-based quality improvement program. J Gen Intern Med (2010) 25:1078–82. doi:10.1007/s11606-010-1427-5
13. Antonacci AC, Lam S, Lavarias V, Homel P, Eavey RA. A report card system using error profile analysis and concurrent morbidity and mortality review: surgical outcome analysis, part II. J Surg Res (2009) 153:95–104. doi:10.1016/j.jss.2008.02.051
14. Joseph C, Garrubba M, Melder A, Loh E. Best practice for conducting morbidity and mortality reviews: a literature review. The Quaterly (2015).
15. Mitchell EL, Lee DY, Arora S, Kenney-Moore P, Liem TK, Landry GJ, et al. Improving the quality of the surgical morbidity and mortality conference: a prospective intervention study. Acad Med (2013) 88:824–30. doi:10.1097/ACM.0b013e31828f87fe
17. Leape LL. Reporting of adverse events. N Engl J Med (2002) 346:1633–8. doi:10.1056/NEJMNEJMhpr011493
18. Aboumatar HJ, Blackledge CG, Dickson C, Heitmiller E, Freischlag J, Pronovost PJ. A descriptive study of morbidity and mortality conferences and their conformity to medical incident analysis models: results of the morbidity and mortality conference improvement study, phase 1. Am J Med Qual (2007) 22:232–8. doi:10.1177/1062860607303292
19. McDonnell C, Laxer RM, Roy WL. Redesigning a morbidity and mortality program in a university-affiliated pediatric anesthesia department. Jt Comm J Qual Patient Saf (2010) 36:117–25. doi:10.1016/S1553-7250(10)36020-X
20. Chan LS, Elabiad M, Zheng L, Wagman B, Low G, Chang R, et al. A medical staff peer review system in a public teaching hospital—an internal quality improvement tool. J Healthc Qual (2014) 36:37–44. doi:10.1111/j.1945-1474.2012.00208.x
21. Mitchell EL, Lee DY, Arora S, Kwong KL, Liem TK, Landry GL, et al. SBAR M&M: a feasible, reliable, and valid tool to assess the quality of, surgical morbidity and mortality conference presentations. Am J Surg (2012) 203:26–31. doi:10.1016/j.amjsurg.2011.07.008
22. Nimptsch U, Mansky T. Quality measurement combined with peer review improved German in-hospital mortality rates for four diseases. Health Aff (Millwood) (2013) 32:1616–23. doi:10.1377/hlthaff.2012.0925
23. Szekendi MK, Barnard C, Creamer J, Noskin GA. Using patient safety morbidity and mortality conferences to promote transparency and a culture of safety. Jt Comm J Qual Patient Saf (2010) 36:3–9. doi:10.1016/S1553-7250(10)36001-6
24. Calder LA, Kwok ESH, Cwinn AA, Worthington J, Yelle JD, Waggott M, et al. Enhancing the quality of morbidity and mortality rounds: the Ottawa M&M model. Acad Emerg Med (2014) 21:314–21. doi:10.1111/acem.12330
25. Deis JN, Smith KM, Warren MD, Throop PG, Hickson GB, Joers BJ, et al. Transforming the morbidity and mortality conference into an instrument for systemwide improvement. In: Henriksen K, Battles JB, Keyes MA, Grady ML, editors. Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 2: Culture and Redesign). Rockville, MD: Agency for Healthcare Research and Quality (2008). 8 p.
26. Smaggus A, Mrkobrada M, Marson A, Appleton A. Effects of efforts to optimize morbidity and mortality rounds to serve contemporary quality improvement and educational goals: a systematic review. BMJ Qual Saf (2018) 27:74–84. doi:10.1136/bmjqs-2017-006632
27. Harbison SP, Regehr G. Faculty and resident opinions regarding the role of morbidity and mortality conference. Am J Surg (1999) 177:136–9. doi:10.1016/S0002-9610(98)00319-5
28. Xiong X, Johnson T, Jayaraman D, McDonald EG, Martel M, Barkun AN. At the crossroad with morbidity and mortality conferences: lessons learned through a narrative systematic review. Can J Gastroenterol Hepatol (2016) 2016:7679196. doi:10.1155/2016/7679196
29. Huddleston JM, Diedrich DA, Kinsey GC, Enzler MJ, Manning DM. Learning from every death. J Patient Saf (2014) 10:6–12. doi:10.1097/PTS.0000000000000053
30. Sellier E, David-Tchouda S, Bal G, François P. Morbidity and mortality conferences: their place in quality assessments. Int J Health Care Qual Assur (2012) 25:189–96. doi:10.1108/09526861211210411
31. Mair T. Clinical governance, clinical audit, and the potential value of a database of equine colic surgery. Vet Clin North Am Equine Pract (2009) 25:193–8. doi:10.1016/j.cveq.2009.04.009
32. Rose N, Toews L, Pang DS. A systematic review of clinical audit in companion animal veterinary medicine. BMC Vet Res (2016) 12:40. doi:10.1186/s12917-016-0661-4
33. Mosedale P. Introducing clinical audit to veterinary practice. In Pract (1998) 20:40–2. doi:10.1136/inpract.20.1.40
34. Viner BP, Jenner CS. Clinical audit—learning from the medical profession. Vet Rec (2005) 157:695–6. doi:10.1136/vr.157.22.695
35. Cummins RO. Moving toward uniform reporting and terminology. Ann Emerg Med (1993) 22:33–6. doi:10.1016/S0196-0644(05)80246-X
37. Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Breizat AHS, Dellinger EP, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med (2009) 360:491–9. doi:10.1056/NEJMsa0810119
38. Reason J. Human error: models and management. BMJ (2000) 320:768–70. doi:10.1136/bmj.320.7237.768
39. Wiegmann DA, Shappell SA. A Human Error Approach to Aviation Accident Analysis. Hampshire: Ashgate Publishing Limited (2003).
41. Reason J. Safety in the operating theatre—part 2: human error and organizational failure. Qual Saf Health Care (2005) 14:56–61.
42. Kieffer PJ, Mueller POE. A profile of morbidity and mortality rounds within resident training programs of the American College of Veterinary Surgeons. Vet Surg (2017). doi:10.1111/vsu.12765
43. Berenholtz SM, Hartsell TL, Pronovost PJ. Learning from defects to enhance morbidity and mortality conferences. Am J Med Qual (2009) 24:192–5. doi:10.1177/1062860609332370
44. Prince JM, Vallabhaneni R, Zenati MS, Hughes SJ, Harbrecht BG, Lee KK, et al. Increased interactive format for Morbidity & Mortality conference improves educational value and enhances confidence. J Surg Educ (2007) 64:266–72. doi:10.1016/j.jsurg.2007.06.007
45. Schwarz D, Schwarz R, Gauchan B, Andrews J, Sharma R, Karelas G, et al. Implementing a systems-oriented morbidity and mortality conference in remote rural Nepal for quality improvement. BMJ Qual Saf (2011) 20:1082–8. doi:10.1136/bmjqs-2011-000273
46. De Meester K, Verspuy M, Monsieurs KG, Van Bogaert P. SBAR improves nurse-physician communication and reduces unexpected death: a pre and post intervention study. Resuscitation (2013) 84:1192–6. doi:10.1016/j.resuscitation.2013.03.016
47. Leonard M, Graham S, Bonacum D. The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care (2004) 13(Suppl 1):i85–90. doi:10.1136/qshc.2004.010033
48. Pronovost PJ, Holzmueller CG, Martinez E, Cafeo CL, Hunt D, Dickson C, et al. A practical tool to learn from defects in patient care. Jt Comm J Qual Patient Saf (2006) 32:102–8. doi:10.1016/S1553-7250(06)32014-4
49. Mahajan RP. Critical incident reporting and learning. Br J Anaesth (2010) 105:69–75. doi:10.1093/bja/aeq133
50. Bauer JE, Duffy GL, Westcott RT, editors. Improvement Tools. Milwaukee, WI: ASQ Quality Press (2006).
Keywords: morbidity and mortality conference, rounds, meeting, errors, adverse events, complications
Citation: Pang DSJ, Rousseau-Blass F and Pang JM (2018) Morbidity and Mortality Conferences: A Mini Review and Illustrated Application in Veterinary Medicine. Front. Vet. Sci. 5:43. doi: 10.3389/fvets.2018.00043
Received: 29 November 2017; Accepted: 21 February 2018;
Published: 06 March 2018
Edited by:
Karine Portier, Université de Lyon, FranceReviewed by:
Rene Doerfelt, LMU Munich, GermanyJoost Jan Uilenreef, Academic Medical Center (AMC), Netherlands
Copyright: © 2018 Pang, Rousseau-Blass and Pang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel S. J. Pang, ZGFuaWVsLnBhbmdAdW1vbnRyZWFsLmNh