 Gustavo Rassier Isolan1,2,3*
Gustavo Rassier Isolan1,2,3* Samir Ale Bark1,3
Samir Ale Bark1,3 Jander Moreira Monteiro1,3
Jander Moreira Monteiro1,3 Tobias A. Mattei4
Tobias A. Mattei4 Kaan Yağmurlu5
Kaan Yağmurlu5 Rafaela Fernandes Gonçalves1,3
Rafaela Fernandes Gonçalves1,3 Osvaldo Malafaia3
Osvaldo Malafaia3 Rafael Roesler2,6,7Jurandir Marcondes Ribas Filho3
Rafael Roesler2,6,7Jurandir Marcondes Ribas Filho3
- 1Graduate Program in Principles of Surgery, Mackenzie Evangelical University, Curitiba, Brazil
- 2National Science and Technology Institute for Children's Cancer Biology and Pediatric Oncology—INCT BioOncoPed, Porto Alegre, Brazil
- 3The Center for Advanced Neurology and Neurosurgery (CEANNE), Porto Alegre, Brazil
- 4Division of Neurological Surgery, St. Louis University, St. Louis, MO, United States
- 5Department of Neurosurgery, University of Virginia, Charlottesville, VA, United States
- 6Department of Pharmacology, Institute for Basic Health Sciences, Federal University of Rio Grande do Sul, Porto Alegre, Brazil
- 7Cancer and Neurobiology Laboratory, Experimental Research Center, Clinical Hospital (CPE-HCPA), Federal University of Rio Grande do Sul, Porto Alegre, Brazil
Object: In insular glioma surgery, lenticulostriate arteries (LSTa) tumoral encasement increases neurological deficits risk despite intensive efforts to preserve the internal capsule's integrity. In this study, we focus on the LSTa relationships with the medial aspect of the insular tumors. We propose a new non-invasive method for LSTa involvement prediction in preoperative MRI (Porto Alegre Line). We compare it with direct intraoperative encased LSTa visualization.
Methods: A retrospective review of our database of 52 patients of insular glioma was performed. In cases with no tumor located medial to Porto Alegre line, our medial resection limit, mainly for the tumor part located next to the limen insula, was the inferior fronto-occipital fasciculus (IFOF), identified through altered speech patterns during electric subcortical stimulation. In cases with no assumed LSTa involvement, the parameter used to stop resection was the confirmation of the corticospinal tract with 10-mA stimulus. The resection limit of tumors placed medially to the Porto Alegre line was intraoperative direct LSTa visualization.
Results: The LSTa involvement was the most critical medial limiting factor in more aggressive tumor resection and an excellent overall survival (P = 0.022). In cases in which there were direct intraoperative LSTa encasement visualization, Porto Alegre Line was employed as an MRI preoperative landmark for prediction of LSTa involvement in those patients with Sensitivity, Specificity, Positive Predictive Values of 1, 0.975 and 0.923, respectively.
Conclusion: We have found that LSTa encasement is a limiting factor to reach a satisfactory extent of resection and that Porto Alegre Line can predict it.
Introduction
Insular gliomas (1–6) are of challenging surgical management because of the complex anatomy of the insula and their proximity to several functional structures such as basal ganglia, internal capsule, speech and language processing cortex and subcortex, as well as the middle cerebral artery and lenticulostriate arteries (LSTa). Gross total resection of these tumors have been shown to impact progression-free survival as well as to contribute to function preservation and quality of life (1–3). Such results can only be obtained through a thorough understanding of the underlying microsurgical anatomy, accurate imaging analysis, language evaluation, and specific brain map techniques (2, 3). Historically, advances in cortical localization were achieved through intraoperative mapping by pioneer neurosurgeons (4, 7–12). Such type of functional mapping, which considers inter-individual variations, has inaugurated the era of surgical brain mapping, which, nowadays, is a sine qua non for ensuring safety during surgical resection of such lesions (13). The main advantage of awake brain surgery is the capacity of identifying eloquent brain areas, thereby possibly decreasing postoperative neurological deficits and enabling maximal extent of resection, even with supramaximal resection in some cases (5, 6, 14, 15).
However, brain mapping is quite challenging when the medial aspect of insular tumors does not displace but involves the LSTa. In these cases, even with intensive efforts to preserve the integrity of the internal capsule based on subcortical mapping, there is no assurance that the patient will not experience a new motor or sensory deficit in the postoperative period. This is the main reason why studying the relation of the LSTa with the medial aspect of the insular tumors pre and intraoperatively is of paramount importance. Although the location and deviation of the LSTa on preoperative angiography has already been elegantly shown in a previous study (16), there is still a lack of practical MRI criteria that can predict the involvement of these arteries.
The study aims to describe the current state-of-art for functional mapping during resection of insular gliomas, focusing on the underlying microsurgical anatomy, and the impact of the relationship between the LSTa and the tumor based on the extent of resection, overall survival, and functional outcomes after surgery for insular gliomas. Finally, we describe the “Optic Chiasm - Insular Recess line” (OC-IR line) and Porto Alegre Line on preoperative MRI as an important surrogate marker for prediction of the involvement of the LSTa.
Materials and methods
A retrospective review of our database of 52 patients of insular glioma operated on by the senior author (GRI) between 2007 and 2018 was performed. Insular gliomas were classified according to Yaşargil (17) and Berger-Sanai classifications (18, 19).
The histological tumor type was defined according to the 2016 World Health Organization (WHO) classification (20). Handedness and language dominance were evaluated employing the Portuguese Edinburgh Handedness Inventory (21, 22). For this study, drug-resistant epilepsy (DRE) was considered a failure of two or more drug therapies in patients with glioma and having at least one epileptic seizure per month. In all cases, we also ran tests at pre and postoperative (one day, three months, and six months) period as follows: Test of Picture Naming (D80 test) and Boston Diagnostic Aphasia Examination (23), and Karnofsky Performance Status (KPS) scale (24).
The Research Ethics Committee of the FEMPAR (FAculdade Evangélica Mackenzie do Paraná) approved this study. Informed consent was obtained from all patients. This study adheres to the principles outlined in the US Code of Federal Regulations, Title 45, Part 46, Protection of Human Subjects, revised January 15, 2009 (25) and the World Medical Association Declaration of Helsinki (26). Microsurgical anatomy was studied and photographed in 5 human cadaveric heads that were prepared in a manner described elsewhere (27, 28).
Surgical technique
All patients undergoing awake surgery were submitted to a preoperative simulation of the clinical environment's surgical process. During the actual surgery, the patient's head was fixed in a Mayfield frame. Operating microscope and ultrasonic surgical aspirator with a low setting were used in most patients.
Over the years, our technique for resecting the insular tumors has evolved from an approach focused purely on the underlying microsurgical anatomy to a combination of anatomy and functional brain mapping. The first patient of this series, who presented a left insular low-grade glioma (LGG), was operated via transsylvian approach without any type of intraoperative neurophysiological monitoring in 2007 (29).
From 2008 to 2009, we have used a transsylvian approach for all insular tumors with the aid of intraoperative neurophysiological monitoring (including somatosensory and motor evoked potential) (30) with subcortical electric stimulation under general anesthesia to define the medial limit of the resection. We considered a positive electromyographic response in the contralateral body at 10 mA of subcortical stimulation sign of proximity to the motor tract to use this limit parameter as resection limit (31). From 2010 to 2014, for purely insular tumors located in the dominant hemisphere, awake surgery with a transsylvian approach was employed. For insular tumors extended beyond the insula into the frontal and temporal lobes, we used the transcortical approach in those cases in which silent mapping was obtained. During manipulation of the M2 segment of the middle cerebral artery, an intense headache occurred in two patients. Based on this experience, over the years, we have evolved to a transcortical-transopercular approach with subpial resection for all insular tumors in the dominant hemisphere, avoiding direct arterial wall manipulation and manipulation-induced headache (32).
At the beginning of this series, we employed image guidance with navigation in four patients. We have observed that, mainly in larger tumors, the localization parameters were significantly affected after the beginning of the tumor resection due to brain shift. Therefore, in such patients, we currently take the accuracy of navigation with some reluctance. We have not used intraoperative MRI, due to the fact that we identify the resection borders based on function rather than anatomy. On the other hand, we employed intraoperative ultrasound to determine the tumor's position with sulci and gyri. In the past, we used to use intraoperative electrocorticography to evaluate the after-discharge phenomenon during cortical mapping stimulation, but we have recently abandoned it (33). Our parameters of intraoperative cortical and subcortical electrical stimulation have been described elsewhere in the literature (34, 35).
Identification of the lenticulostriate arteries
We presume that identifying early and pre-operatively the anterior perforated substance via MRI as well as its proximity to the tumor could help ascertain the path of the LSTa across the medial tumor boundaries. The anterior perforated substance can be found in coronal T2-weighted MRI by examining a plane which cuts through the optic chiasm. The optic chiasm in this case is the medial reference, and the insular recess at the anteroinferior aspect of the insular pole is the lateral limit (Optic Chiasm - Insular Recess line - OC- IR line).
We thus trace a vertical line from the lateral limit of the OC-IR line parallel to the median sagittal plane as the probable lateral LSTa trajectory (Porto Alegre Line) (Figure 1).
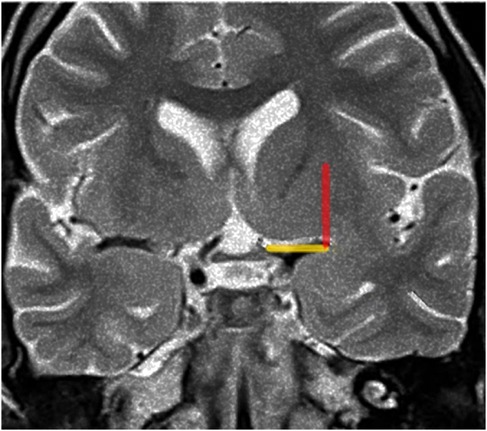
Figure 1. Porto alegre line (red) on coronal T2-weighted MRI reflects indirectaly the lateral limit of the anterior perforated substance, the OC-IR line (yellow). Figure from Isolan et al. (36).
Coronal T2-weighted MRI at the level of the optic chiasm as an imaging parameter of the anterior perforated substance. The imaginary line (the Optic Chiasm – Insular Recess line) extends from the optic chiasm medially to the insular recess laterally. It is used to locate the anterior perforated substance (Yellow line). The ascending red line which we call The Porto Alegre Line extends from the lateral end of the OC-IR line and defines the lateral limit of the lateral LSTa within the central core. In cases which the medial border of insular tumor cross this line medially there is a high probability that LSTa will participate in the tumor's evolution.
Medial limit of tumor resection
With insular glioma patients who had undergone awake surgery, our medial limit of resection (the part of the tumor next to the limen insula) was determined mostly by way of altered speech (paraphasia, etc.) under administration of electric subcortical stimulation to the inferior fronto-occipital fasciculus (IFOF). In order to examine the possibility of LSTa being involved at the medial aspect of the tumor, we conducted a careful analysis of coronal and axial T2 and T1-weighted because we understood that the tumors entangling these vessels could not be entirely resected (16, 37–43). In cases in which LSTa involvement was likely, the limiting factor for resection of the medial portion of the tumor was established as the direct intraoperative view of the LSTa. When LSTa within the tumor could be seen, resection was immediately stopped. In patients in which it was assumed that LSTa was not involved, the factor limiting the medial portion resection was the establishment of the corticospinal tract with a 10-mA probe (Figure 2) or paraphasia due to IFOF stimulation in the anterior and inferior part of the tumor.
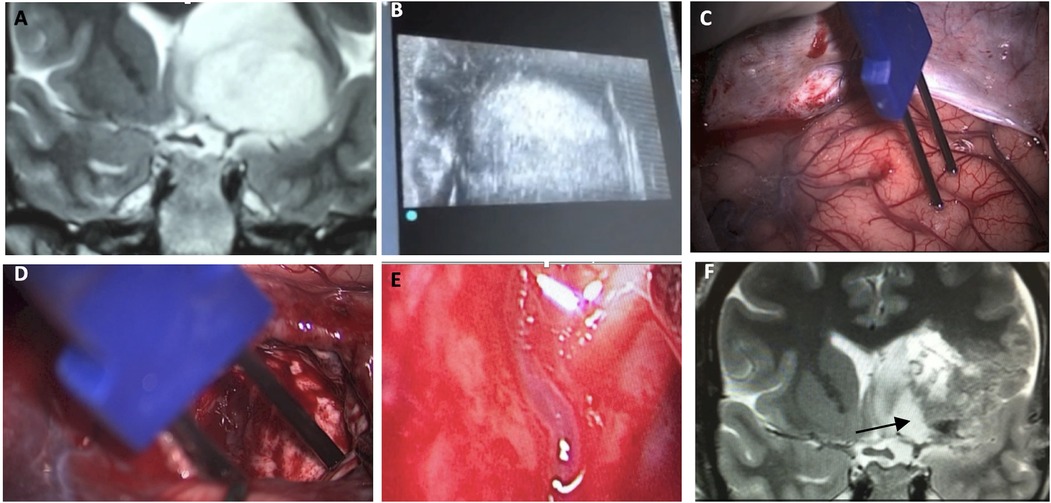
Figure 2. A microsurgical resection of a left insular glioma with LSTa encasement. (A) Coronal T2-weighted MRI showing left-sided insular glioma suggesting crossing over the Porto Alegre indicating high probability of LSTa tumoral encasement; (B) intraoperative echography; (C) cortical brain mapping was silent on the so called “Braca's area”; (D) subcortical brain (day 1) showing residual tumor medial to the Porto Alegre line, as it was the medial resection limit. (E) Intraoperative view of the LSTa. (F) Part of the tumor medial to the Porto Alegre line was not resected (arrow). Figure from Isolan et al. (36).
Volumetric analysis
Up to 2013, we calculated tumor volume using three largest diameters (D1, D2, and D3) of the tumor taken from T2-weighted MR images along the three principal anatomical planes. Then, we estimated tumor volume using the formula D1 × D2 × D3/2 (44). Since 2014, we have used OsiriX (Pixmeo SARL, Geneva, Switzerland) via stored MR image files in DICOM format (Digital Imaging and Communications in Medicine) (45).
Statistical analysis
Categorical variables were represented by absolute and relative frequency. Quantitative variables were defined by the median and interquartile range according to the distribution verified by the Shapiro-Wilk normality test.
The proportions of the immediate postoperative deficits and late postoperative deficits (6 months) were compared between the general mapping categories and discriminated by the chi-square test.
For asymmetric variables, we compared the distribution of the extent of resection (EOR) between the categories of LSTa involvement and surgical techniques using the Mann-Whitney and Kruskal-Wallis tests, respectively. Spearman's correlation was performed to verify the degree of relationship between the survival time and the score of the degree of resection (EOR).
Kaplan-Meier analysis was used to describe the mean or median variability and probability at specific survival time points. This description was stratified by symptoms, by Yaşargil's and Berger-Sanai's classifications, and by time ranges from symptoms to diagnosis. Through the Kaplan-Meier analysis, we compared the estimated time distributions using the Log-Rank test. The analysis was performed using the SPSS software (v.25). The classification level used was p value < 0.05.
Results
Patient demographics
The clinical features of the patient enrolled in this retrospective study are summarized in Table 1. Among 52 patients studied, 30 were male. Most of the tumors were situated on the left side (29 subjects). The most frequent symptom was complex partial seizure.

Table 1. Patient's clinical features.
Histological findings
A total of 52 patients were enrolled in this study. The histologic analysis was stratified as follows: patients of diffuse astrocytoma (30 subjects) and patients of anaplastic astrocytoma or glioblastoma (22 subjects), 61% and 39% respectively. The mean age for high-grade tumors was 41 (range of 19–68 years), and for low-grade tumors, the mean age was 32 (range of 13–53 years).
Surgical results and overall survival analysis
According to Berger-Sinai's classification, the tumor was found in one zone in 7 cases (13.5%), two zones in 30 cases (57.7%), and 15 giant tumor cases (28.8%). Considering Yaşargil's classification of insular tumors, 28 patients were classified as type 3 (A or B) and 24 as type 5 (A or B).
When analyzing the survival odds according to the Yaşargil's classification, patients classified as type 3 (A or B) demonstrated a longer survival rate, mean of 121.6 months, and patients of type 5 (A or B) have shown shorter survival rate, mean of 59.1 months (Log-Rank test p = 0.008).
According to Berger-Sanai's classification, the survival odds in this series were: when the tumor was found in one zone, mean survival was 98.7 months; whenever the tumor was more invasive and situated in two zones, the mean survival rate was 101.4 months. If the tumor involved more than two zones, the mean survival obtained was 67.9 months.
Regarding extent of resection, we found under the Spearman correlation longer overall survival in the population submitted to more than 90% resection (R = −0.037 in low-grade tumors and R = −0.169 in high-grade tumors (Table 2).
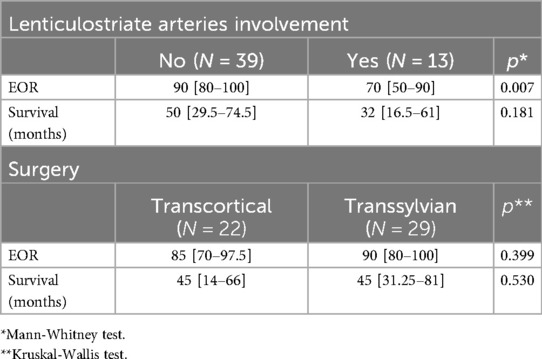
Table 2. The correlation of LSTa involvement with the extent of resection (EOR) and survival and the correlation of EOR via the transsylvian or transcortical and survival rates.
Lenticulostriate arteries
The anterior perforated substance is bordered by medial and lateral olfactory striae, optic tract, and limen recess. The LSTa pass through the anterior perforated substance (APS) to supply the caudate nucleus, thalamus, globus pallidus, putamen, anterior limb, genu and posterior limb of the internal capsule. LSTa subdivided into the medial, intermediate, and lateral groups. The medial LSTa arise mainly from anterior cerebral artery, and both intermediate and lateral LSTa arise mainly from the middle cerebral artery. Microanatomical knowledge of the region and its vascular supply emphasizes the neuroradiological and clinical relation (Figure 3).
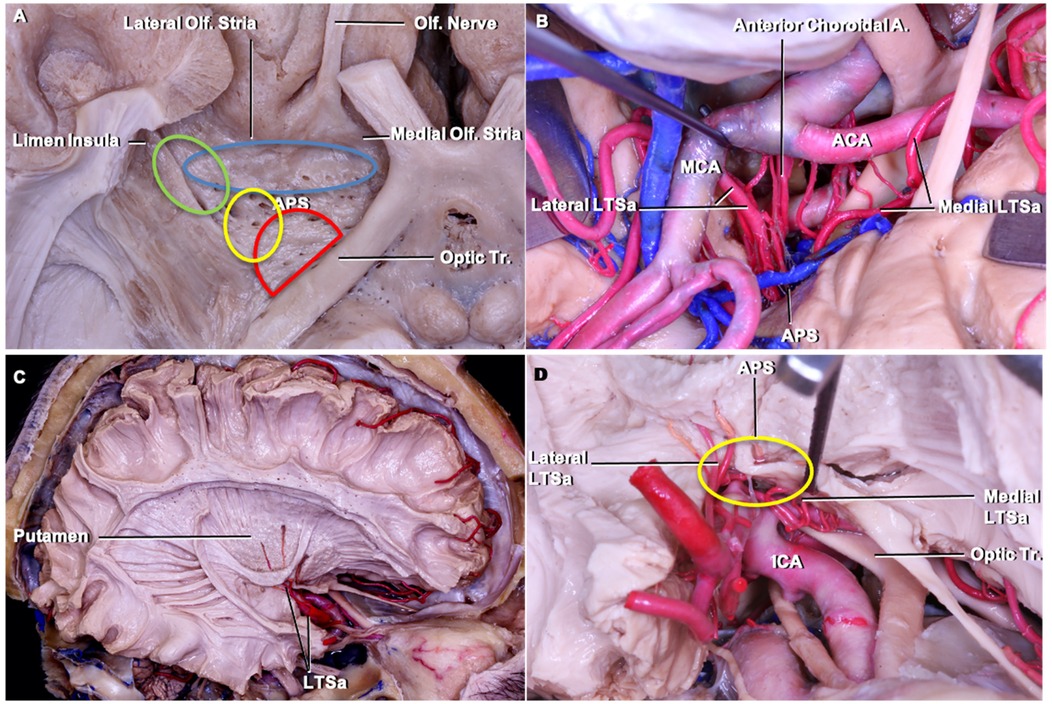
Figure 3. Cadaveric dissection pictures. (A) An inferior view of the anterior perforated substance (APS) and LSTa territories. The APS is bordered by medial and lateral olfactory striae, optic tract, and limen (insular) recess. In the APS, the green circle indicates the lateral LSTa, yellow circle indicates the medial LSTa, red circle indicates the branches of the anterior choroidal artery, and blue circle stands for the medial LSTa. The OC-IR is drawn between the optic tract and recess of the limen insula; (B) the surgical view of LSTa on the left side. The medial LSTa arises from anterior cerebral artery, and the lateral LSTa arises from the middle cerebral artery; (C) white fiber dissection showing the LSTa passing through the APS to supply the basal ganglia; (D) enlarged view of C. ACA, anterior cerebral artery; APS, anterior perforated substance; ICA, internal carotid artery; LSTa, lenticulostriate arteries; Tr, tract.
LSTa involvement was determined through preoperative MRI and intraoperative methods, as described above. In 13 patients, LSTa were founded to be involved by the tumor. In 39 patients, there were no involvement of the LSTa, which allowed a more aggressive resection. These findings suggest that tumors with a invasion medially to the anterior perforated substance, that mean's Porto Alegre Line, cannot be submitted to a total resection without causing a severe neurological deficit. Most of these patients have a subtotal resection regardless of the surgical approach (transsylvian or transcortical). The LSTa involvement is probably the most critical medial limiting factor to obtain a more aggressive tumor resection and an excellent overall survival (p = 0.022) (Figures 4–6).
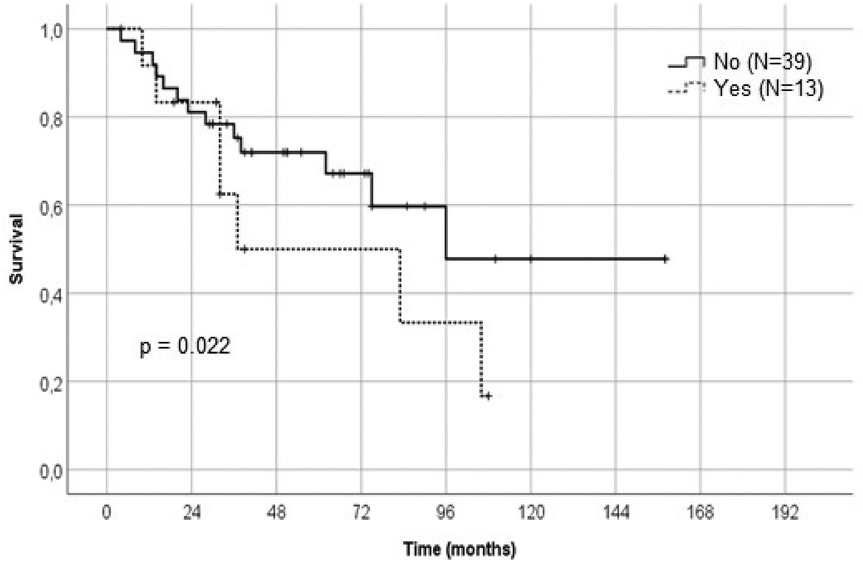
Figure 4. Kaplan-Meier graph showing the relation of the lenticulostriate arteries involvement and survival rate.
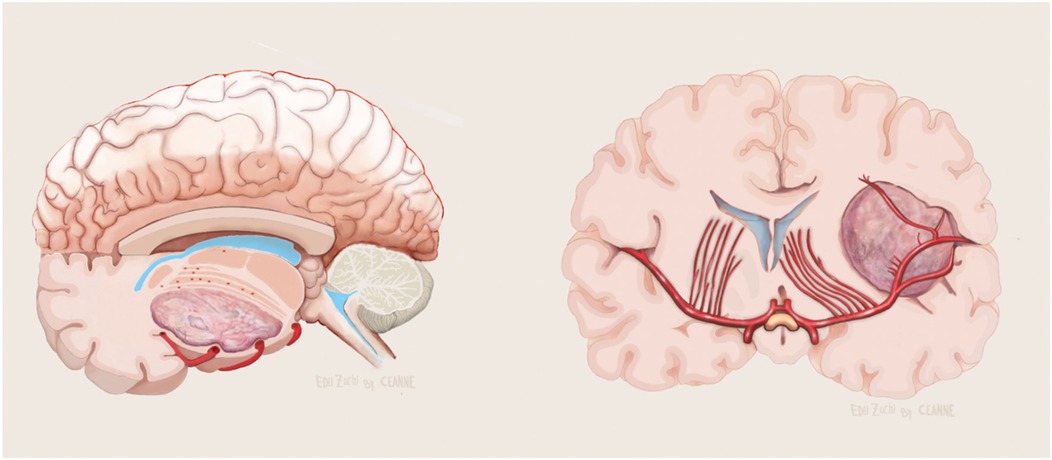
Figure 5. Illustration showing no evolvement of the LSTa by the tumor in axial (left) and coronal (right) view. Figure from Isolan et al. (36).
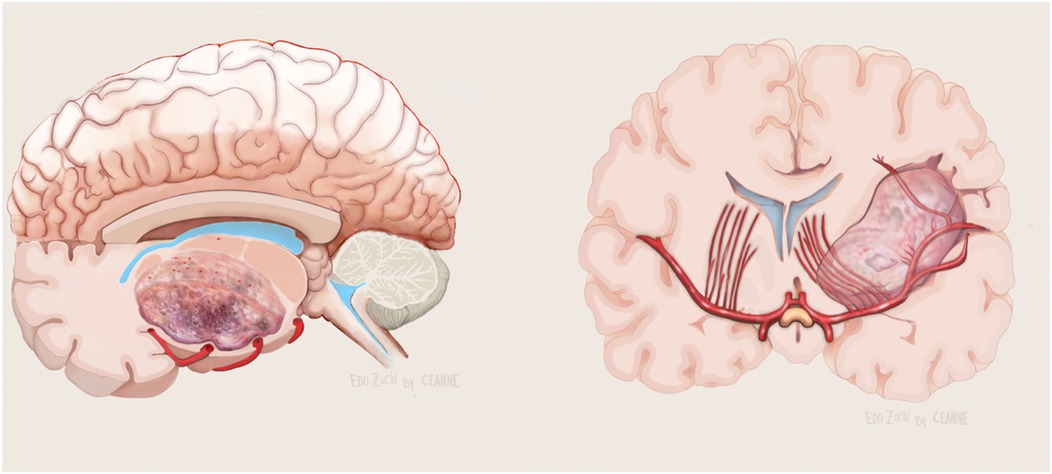
Figure 6. Illustration showing evolvement of the LSTa by the tumor in axial (left) and coronal (right) view. Figure from Isolan et al. (36).
We used brain mapping as a parameter to compare immediate and late postoperative neurological deficits. When no mapping was used, 15 patients (40%) developed some immediate neurological deficits, and 6 (16.2%) developed a late deficit. In patients whose motor evoked potentials (MEPs) and somatosensory evoked potentials (SSEPs) were available, 18.2% developed a transient immediate neurological deficit with complete recovery at 3 months. In the awake group, 50% developed immediate motor deficit and none late neurological deficit (total recovery despite the extent of resection) (Table 3).
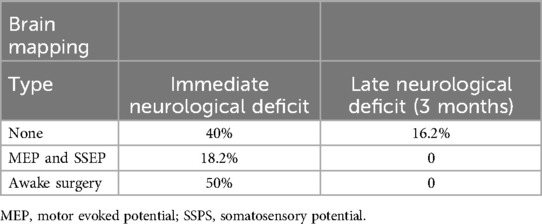
Table 3. Relation of intraoperative brain mapping and neurological deficits.
Fourteen patients had refractory epilepsy (46). All of them improved their seizures after surgery, being then categorized as Engel I and II.
Considering that the LSTa were involved in 13 patients (intraoperative visualization in its superior part with no IFOF distuption), the coronal T2-weighted MRI showed that, using the Porto Alegre Line, as a parameter, the involvement of these arteries could be predicted in all MRIs with tumor located medial to the Porto Alegre Line (Figures 1, 7, 8). In cases in which we did not see the LSTa intraoperatively, the medial limit of resection was based on subcortical mapping and most of these tumors were lateral of the Porto Alegre Line, being a total resection feasable Based on these results, we calculated the Sensitivity, Specificity, Positive Predictive Values of the Porto Alegre Line in predict LSTa encasement by the tumor. Our results were 1, 0.975 and 0.923, respectively.
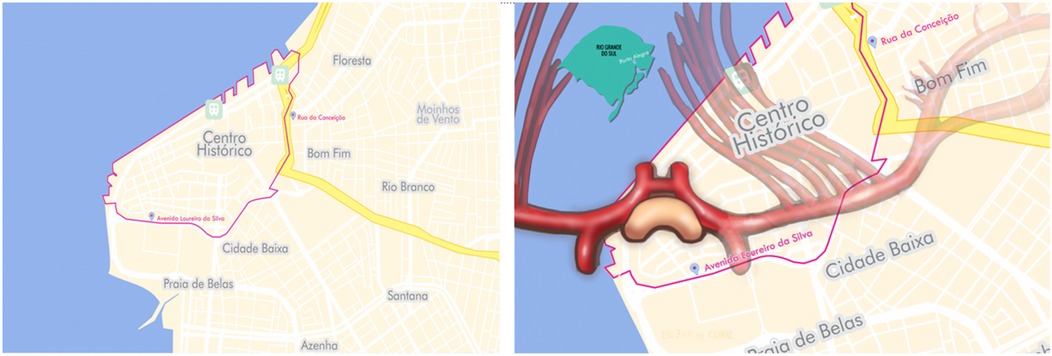
Figure 7. Porto alegrès historic city center (“Centro Histórico”) is one of its busiest neighborhoods and also sees the highest number of muggings. The neighborhood is bounded by Sarmento Leite Street to the east and by the Guaíba River to the west (left). Crossing into the city center runs the risk of falling victim to a crime, much as intruding on insula gliomas can run the risk of injuring the lenticulostriate arteries and causing neurological deficits (right) Figure from Isolan et al. (36).
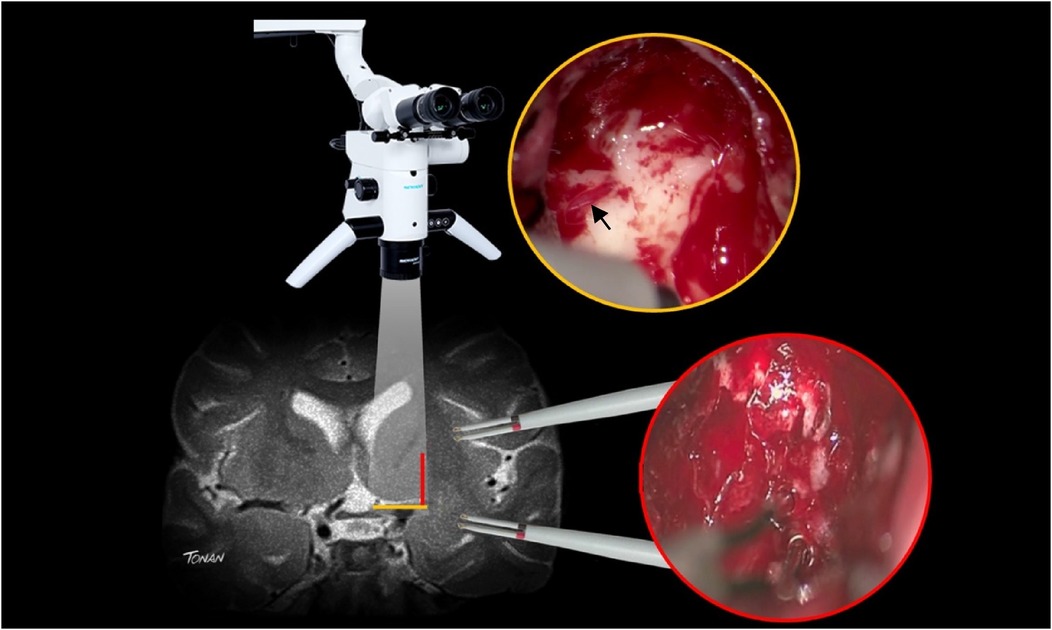
Figure 8. In order to avoid postoperative neurological deficit after insular glioma resection, surgeons have to use subcortical mapping for safe resection of the tumor located lateral to the porto alegre line and microscopic direct visualization of the lenticulostriate arteries (arrow) for safe resection of the tumor located medial to the porto alegre line (red line).
Discussion
Microsurgical resection is the gold standard for the treatment of high-grade gliomas. Low-grade gliomas are diffusely infiltrative tumors that generally manifest with seizures in young and professionally active patients. Although surgery of low-grade gliomas has been a controversial subject for decades, it is now also considered the gold-standard therapy (1, 12, 47–52), even in asymptomatic patients (1–3).
Insular gliomas migrate along white matter tracts, progressively invading the surrounding structures. Inevitably, low-grade tumor progresses to high-grade malignancy. A significant delay of malignant transformation of low grades and death can be achieved by appropriate and timely treatment. According to current guidelines, an aggressive protocol with a maximum safe resection, when feasible, is the first line treatment (53–59).
Thus, the management of patients with insular tumors has been dramatically changing during the last two decades, mainly due to technological developments in neuroimaging and the available surgical armamentarium. The benefits provided by these technical advances have generally improved the decision-making process involved in the management of intrinsic brain tumors (60–68).
Awake craniotomy with intraoperative mapping by cortical and axonal stimulation allows minimizing the risk of neurological dysfunction by sparing eloquent surrounding brain structures while improving the resection extent. Cortical and subcortical brain mapping have become a standard of care across multiple subspecialties within Neurosurgery. It is therefore a reliable method in the treatment of insular gliomas.
The technique of intraoperative direct electrical stimulation has been previously described as a safe, precise and reliable method of detection of functional cortical areas (37, 69–72) as well as subcortical supra-tentorial (73), infra-tentorial (74) and spinal pathways (75). Essentially, we began our experience with direct cortical/subcortical electrical stimulation in 2012. From this year on, we were able to obtain a greater extent of resection with simultaneous preservation of functional areas at the same time. We have found, analyzing our cases submitted to the awaked protocol, that all the patients operated with gross total resection philosophy were functionally preserved at six months postoperatively.
When targeting insular tumors, some neurosurgeons advocate the traditional transsylvian approach. After the opercular split and exposing the middle cerebral artery, frontal and temporal branches, superior and inferior circular sulci, limen insulae, and anterior perforated substance, the tumor was resected in-between MCA branches. Other neurosurgeons advocate a transcortical approach. In a transcortical approach, after cortical mapping, one or more delicate and limited subpial dissection is carried out until the superior or inferior circular insular sulcus, exposing the superior or inferior insular surface. In our series, twenty-nine patients were operated on with the transsylvian route and twenty-two patients with the transcortical route. We could not find a statistical significance to establish a clear correlation between surgical approaches and long-term survival or extent of resection. In theory, transcortical approach is a tumor-directed approach but has the disadvantage of a poor arterial control, especially the lateral lenticulostriate group. In our surgeries, we noted that this was not a problem because we could predict the LSTa encasement using the Porto Alegre Line. In the transsylvian approach, most of the vessels are directly seen but, just because of that, vascular injury may be a possible associated complication. Another disadvantage of this approach is that sometimes the posterior third of sylvian fissure cannot be appropriately split while preserving the superficial sylvian vein and its anastomosis with Labbé or Trolard veins. This is especially true in a tumor located in zone 2 of Berger-Sanai's classification.
Especially in awaked surgery, vascular manipulation in transsylvian approach has produced severe headache in two of our patients, as mentioned before. This was one of the reasons we switched to the transcortical approach in awake patients. It is significant to note that surgery in the insula may induce postoperative hemiparesis and speech impairment after dominant insula infarction or aggressive resection, and mutism and apraxia after non-dominant insula damage (76, 77).
Insular glioma classification
There are two main classifications for insular gliomas. Yaşargil's first extended series of limbic and paralimbic tumors included 57 insular and parainsular tumors (17). After the advent of microsurgical techniques, these first encouraging results convinced many neurosurgeons to take a renewed interest in insular tumor surgery. Yaşargil et al. proposed a classification system based on whether a tumor was restricted to the insula (type 3), was part of the insula (type 3A), or was included in the adjacent operculum (type 3B). Tumors Type 5A and 5B were those involving one or both of the paralimbic orbitofrontal and temporopolar areas, respectively.
Berger and Sanai have developed a quadrangular system to classify tumors in zone I to IV according to their major locations (51). The system considered a plane traced over the sylvian fissure where the insula straddle intersected by a perpendicular plane through a projection of the foramen of Monro. This classification is essential because the tumor in zone 2 (superior and posterior part of the insula) is better resect with transcortical approach in order to avoid brain retraction and possible venous infarction of posterior third of the superficial sylvian veins and its anastomosis.
In our series, we observed that type 3 tumors in Yaşargil classification could be resected with a transinsular approach. Notable, despite the decision making of surgical approaches (transcortical or transsylvian), survival rate was affected by the LSTa encasement.
Arterial relationships
A few key factors significantly impact the extent of resection at the medial boundary of insular tumors. The insular cortex is oriented laterally and acts as the medial wall of the operculoinsular compartment. The gray matter that lies medially to the insular cortex contains claustrum and the putamen; the internal capsule also lies medially, and is quite visible in MRIs of healthy subjects. When a tumor is present, the claustrum is difficult to identify because of its narrow form and flimsy structure. The putamen is more rigid than the insular cortex and can usually resist glioma's spread (38). Even though some insular tumors have obvious limits when viewed in MRIs, others appear to intrude on the putamen and at times the internal capsule. The MCA's branches (M2) can normally be found laterally to the insular surface. Tiny M2 branches penetrate the lateral surface in order to serve the insular cortex, the claustrum, and the external capsule. The lenticulostriate arteries (lateral group) are branches of the M1 (sphenoidal) segment and they cross superiorly, penetrating the anterior perforated substance to supply blood to the substantia innominata, putamen, globus pallidus, head and body of the caudate nucleus, internal capsule as well as the adjacent corona radiata, and the lateral portion of the anterior commissure (44, 78, 79). These number 1–15 per hemisphere, with an average of 7.75. The diameter of LSTa ranges from 0.1 to 1.5 mm (78, 80, 81). There is normally no anastomosis between any LSTa. The lateral view of LSTa appears fan-shaped and covers the lateral face of the internal capsule.
The sylvian fissure has to be opened, otherwise a trans-opercular access has to be performed, to reach the insular glioma. While tumor removal advances medially, the LSTa can become compromised and lead to ischemia of the basal ganglia and internal capsule (45). For this reason, preserving the LSTa is of primary importance. Some tumors may grow and infiltrate medial structures including the LSTa. If this occurs, stopping resection is recommended and the LSTa can be regarded as the primary limiting factor. In the part of the insula near to insular recess (inferior and anterior) identification of the IFOF provides the medial limit of the resection. On the other hand, on the superior and posterior parts of the tumor in order to perform an uneventful insular tumor resection, the vertical plane of the intraparenchymal course of the LSTa should define the medial limit of resection (30, 44, 82, 83).
In Moshel series, the location of the displaced LSTa on preoperative angiograms was employed to locate tumors extending medially into the putamen and globus pallidus, and thus amplifying the risk of postoperative deficit. This was found to be highly correlated when the medial tumor boundaries were established through MRIs superimposed on stereotactic cerebral arteriograms. In a series of 38 insular glioma patients, gross total resection was achieved more often when tumors were lateral to the LSAs, when they medially shifted the LSAs, and when they had well-defined tumor borders on T2-weighted MRIs. In cases in which tumors extended medially to the LSTa, EOR was subtotal (16).
Identifying the LSTa intraoperatively within the sylvian vallecula does not necessarily indicate their intraparenchymal route as the tumor can medially displace arteries here. Yaşargil found that low-grade gliomas initially extended within the confines of the anatomical limbic system's, which suggests that resection will be complete when LSTa are observed intra-operatively or when the common white matter is found covering the putamen (84). The problem of this technique is to disrupt the IFOF before see the LSTa, which can happen in the inferior and anterior part of the tumor and cause language deficit, mainly in the dominant hemisphere.
These are our images and anatomical brief for LSTa during resection of insular gliomas. Detailed knowledge of LSTa's origin, path, and spread is essential to successful resection, particularly the lateral group. Their identification or, at least, anatomical knowledge of their path has a direct effect on the limits of tumor resection and on preservation of function. Starting from the dorsal aspect of the M1 segment of the middle cerebral artery, the LSTa enter the lateral two-thirds of the anterior perforated substance of the basal forebrain, a quadrilateral area of grey matter located anterolateral to the optic tract and posterior to the gyrus rectus and olfactory trigone. It is medially limited by the optic chiasm and laterally by the lateral olfactory striae. After going across the anterior perforated substance, the LSTa extend into the lateral thirds of the anterior commissure, the lateral portion of the globus pallidus, the superolateral two-thirds of the head and whole body of the caudate nucleus, and most of the putamen, then outward towards and including the external capsule, the superior portion of the whole anterior limb and superior portion of the posterior limb of the internal capsule and periventricular white matter (corona radiata) at the angle of the lateral ventricle. Isolated tumor cells in insular gliomas can penetrate intact parenchyma and generate tumor tissue encasing the LSTa.
Certain clinicians advocate stereoscopic angiography and computerized tumor reconstruction, MR angiography, and CT angiography to estimate the position of the LSTa (16). In spite of the soundness of these studies, we have demonstrated that coronal T2-weighted MRIs Porto Alegre Line can predict the LSTa's location and route to great utility. This method was able to anatomically locate LSTa medially encased by tumors in 13 subjects, or 25% of cases. In 75%, the medial tumor border was confined to the normal white matter lateral to the putamen. Over 90% the tumors were resected from the latter patients. The presence of LSTa was a limiting factor to a reasonable extent of resection and we recommend that tumors encasing these arteries must be left intact due to the high risk of permanent postoperative functional deficit.
Another possible etiology of internal capsule and corona radiata infarction could be, at least theoretically, lesion or coagulation of the long perforating arteries (LPra) (85). The LPra originate in the M2 segment of the MCA vascularizing the insular cortex. A majority of these are short, however, the LPra, most commonly located in the posterior half of the central insular sulcus and the long gyri, can reach the corona radiata and/or more deeply in 36% of cases. Some pass through the fibers of the corona radiata and reach the lateral ventricular body's ependyma. In our experience, we coagulated long perforating arteries (LPra) in the posterior part of the insula without any postoperative stroke observed.
The external capsule is the limit of the regions supplied by the short insular arteries. No anastomosis occurs among the insular and lenticulostriate arteries. Although the LPra could be the reason for a postoperative motor deficit after insular glioma resectoin involving LSTa preservation,. Again, we did not find this to be the case with any of our patients, even after coagulating all insular perforator arteries using the transsylvian approach.
The city of Porto Alegre and the meaning of the Porto Alegre Line
Porto Alegre anchors Brazil`s fifth-largest metropolitan region of 4.4 million inhabitants and is the capital of its southernmost state, Rio Grande do Sul. This multicultural city sits at the junction of five rivers and has become a significant port in one of the country`s chief industrial and commercial regions. It contains several public and private universities as well as renowned public and private hospitals. In the 2010s, Porto Alegre suffered a growing wave of violence and in 2017 was ranked the world`s 39th most violent city (86). Fortunately, the incidence of violent crime has been dropping steadily since then (87, 88).
Porto Alegrès Historic City Center is one of its busiest neighborhoods and also sees the highest number of muggings. The neighborhood is bounded by Sarmento Leite Street to the east and by the Guaíba River to the west (36). Crossing into the city center runs the risk of falling victim to a crime, much as intruding on insula gliomas can run the risk of injuring the lenticulostriate arteries and causing neurological deficits.
Our study has some intrinsic limitations, such as the small number of cases with awake surgery. To the small number of patients, as expected in dealing with rare diseases, we have not performed multivariate analysis. In the near future we consider exploring the integration of the Porto Alegre Line with other advanced imaging modalities or machine learning algorithms to enhance predictive accuracy.
Conclusion
Adding cortical and subcortical mapping to microsurgical anatomy x-ray view knowledge is paramount to face insular glioma surgery in the modern era and to not put the patient on jeopardy (36, 89–91). We have found that LSTa encasement is a limiting factor which impacts the EOR of insular gliomas. Thus, future attempts to classify such lesions should consider the encasement of the LSTa among its prognostic factors for overall survival and EOR of these tumors, possibly enabling the surgeon to anticipate a subtotal resection. The preliminary data obtained in this study is expected to provide a foundation for future studies on the significance of the LSTa in insular glioma surgery.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The Research Ethics Committee of the FEMPAR (Faculdade Evangélica Mackenzie do Paraná) approved this study. Informed consent was obtained from all patients. This study adheres to the principles outlined in the US Code of Federal Regulations, Title 45, Part 46, Protection of Human Subjects, revised January 15, 200925 and the World Medical Association Declaration of Helsinki.2.
Author contributions
GI: Writing – original draft. SB: Writing – review & editing. JM: Writing – review & editing. TM: Writing – review & editing. KY: Writing – review & editing. RG: Writing – review & editing. OM: Writing – review & editing. RR: Writing – review & editing. JF: Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by the National Council for Scientific and Technological Development (CNPq, MCTI, Brazil) grant 406484/2022-8 (INCT BioOncoPed) to R.R.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
LSTa, lenticulostriate arteries; MRI, magnetic resonance imaging; OC-IR line, Optic Chiasm - Insular Recess line; GRI, Gustavo Rassier Isolan (author); WHO, World Health Organization; DRE, drug-resistant epilepsy; KPS, Karnofsky Performance Status; LGG, low-grade glioma; IFOF, inferior fronto-occipital fasciculus; DICOM, Digital Imaging and Communications in Medicine; EOR, extent of resection; APS, anterior perforated substance; MEP, motor evoked potential; SSEP, somatosensitive evoked potential; ACA, anterior cerebral artery; ICA, internal carotid artery; Tr, tract; LPra, long perforating arteries.
References
1. Hervey-Jumper SL, Berger MS. Insular glioma surgery: an evolution of thought and practice. J Neurosurg. (2019) 130(1):9–16. doi: 10.3171/2018.10.JNS181519
2. Duffau H. Surgery of low-grade gliomas: towards a ‘functional neurooncology’. Curr Opin Oncol. (2009) 21(6):543–9. doi: 10.1097/CCO.0b013e3283305996
3. Duffau H, Moritz-Gasser S, Gatignol P. Functional outcome after language mapping for insular world health organization grade II gliomas in the dominant hemisphere: experience with 24 patients. Neurosurg Focus. (2009) 27(2):E7. doi: 10.3171/2009.5.FOCUS0938
4. Folzenlogen Z, Ormond DR. A brief history of cortical functional localization and its relevance to neurosurgery. Neurosurg Focus. (2019) 47(3):E2. doi: 10.3171/2019.6.FOCUS19326
5. Ibrahim GM, Bernstein M. Awake craniotomy for supratentorial gliomas: why, when and how? CNS Oncol. (2012) 1(1):71–83. doi: 10.2217/cns.12.1
6. Chacko AG, Thomas SG, Babu KS, Daniel RT, Chacko G, Prabhu K, et al. Awake craniotomy and electrophysiological mapping for eloquent area tumours. Clin Neurol Neurosurg. (2013) 115(3):329–34. doi: 10.1016/j.clineuro.2012.10.022
7. Han SJ, Sughrue ME. The rise and fall of “biopsy and radiate": a history of surgical nihilism in glioma treatment. Neurosurg Clin N Am. (2012) 23(2):207–14, vii. doi: 10.1016/j.nec.2012.02.002
8. Whittle IR. The dilemma of low grade glioma. J Neurol Neurosurg Psychiatry. (2004) 75(Suppl 2):ii31–6. doi: 10.1136/jnnp.2004.040501
9. Wilson CB, Bramwell V, Bonfill X, Cuzick J, Grant R, Guthrie D, et al. Central nervous system tumours. In: Williams C, editor. Evidence-based Oncology. London: BMJ (2003). p. 561–4.
10. Wessels PH, Weber WE, Raven G, Ramaekers FC, Hopman AH, Twijnstra A. Supratentorial grade II astrocytoma: biological features and clinical course. Lancet Neurol. (2003) 2(7):395–403. doi: 10.1016/S1474-4422(03)00434-4
11. Feigenberg SJ, Amdur RJ, Morris CG, Mendenhall WM, Jr MR, Friedman WA. Oligodendroglioma: does deferring treatment compromise outcome? Am J Clin Oncol. (2003) 26(3):e60–6. doi: 10.1097/01.COC.0000072507.25834.D6
12. Jiang B, Chaichana K, Veeravagu A, Chang SD, Black KL, Patil CG. Biopsy versus resection for the management of low-grade gliomas. Cochrane Database Syst Rev. (2017) 4(4):CD009319. doi: 10.1002/14651858.CD009319.pub3
13. Sanai N, Mirzadeh Z, Berger MS. Functional outcome after language mapping for glioma resection. N Engl J Med. (2008) 358(1):18–27. doi: 10.1056/NEJMoa067819
14. Gravesteijn BY, Keizer ME, Vincent AJPE, Schouten JW, Stolker RJ, Klimek M. Awake craniotomy versus craniotomy under general anesthesia for the surgical treatment of insular glioma: choices and outcomes. Neurol Res. (2018) 40(2):87–96. doi: 10.1080/01616412.2017.1402147
15. Duffau H. Brain mapping in tumors: intraoperative or extraoperative? Epilepsia. (2013) 54:79–83. doi: 10.1111/epi.12449
16. Moshel YA, Marcus JD, Parker EC, Kelly PJ. Resection of insular gliomas: the importance of lenticulostriate artery position. J Neurosurg. (2008) 109(5):825–34. doi: 10.3171/JNS/2008/109/11/0825
17. Yaşargil MG, von Ammon K, Cavazos E, Doczi T, Reeves JD, Roth P. Tumours of the limbic and paralimbic systems. Acta Neurochir (Wien). (1992) 118(1–2):40–52. doi: 10.1007/BF01400725
18. Sanai N, Polley MY, Berger MS. Insular glioma resection: assessment of patient morbidity, survival, and tumor progression. J Neurosurg. (2010) 112(1):1–9. doi: 10.3171/2009.6.JNS0952
19. Hervey-Jumper SL, Li J, Osorio JA, Lau D, Molinaro AM, Benet A, et al. Surgical assessment of the insula. Part 2: validation of the Berger-Sanai zone classification system for predicting extent of glioma resection. J Neurosurg. (2016) 124(2):482–8. doi: 10.3171/2015.4.JNS1521
20. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 world health organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. (2016) 131(6):803–20. doi: 10.1007/s00401-016-1545-1
21. Espírito-Santo H, Pires CF, Garcia IQ, Daniel F, Silva AG, Fazio RL. Preliminary validation of the Portuguese Edinburgh handedness inventory in an adult sample. Appl Neuropsychol Adult. (2017) 24(3):275–87. doi: 10.1080/23279095.2017.1290636 Erratum in: Appl Neuropsychol Adult. 2017 Jul-Aug;24(4):394.
22. Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia. (1971) 9(1):97–113. doi: 10.1016/0028-3932(71)90067-4
23. Mansur LL, Radanovic M, Taquemori L, Greco L, Araújo GC. A study of the abilities in oral language comprehension of the Boston diagnostic aphasia examination – Portuguese version: a reference guide for the Brazilian population. Braz J Med Biol Res. (2005) 38(2):277–92. doi: 10.1590/S0100-879X2005000200017
24. Karnofsk DA, Burchenal JH. The clinical evaluation of hemotherapeutic agents in cancer. In: MacLeod CM, editor. Evaluation of Chemotherapeutic Agents. New York: Columbia University Press (1949). p. 191–205.
25. U.S. Department of Health and Human Services (HHS), Office for Human Research Protections (OHRP). CFR 46. HHS.gov (2021). Available online at: http://www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.html (cited June 18 2021).
26. World Medical Association. WMA - The World Medical Association-WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects. Wma.net (2021). Available online at: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (cited June 18 2021).
27. Yagmurlu K, Rhoton AL Jr, Tanriover N, Bennett JA. Three-dimensional microsurgical anatomy and the safe entry zones of the brainstem. Neurosurgery. (2014) 10 (Suppl 4):602–19; discussion 619–20. doi: 10.1227/NEU.0000000000000466
28. Yagmurlu K, Vlasak AL, Rhoton AL Jr. Three-dimensional topographic fiber tract anatomy of the cerebrum. Neurosurgery. (2015) 11(Suppl 2):274–305. discussion 305. doi: 10.1227/NEU.0000000000000704
29. Yaşargil MG, Krisht AF, Türe U, Al-Mefty O, Yasargil DCH. Microsurgery of insular gliomas: part II. Opening of the Sylvian fissure. Contemp Neurosurg. (2002) 24:1–5.
30. Neuloh G, Pechstein U, Schramm J. Motor tract monitoring during insular glioma surgery. J Neurosurg. (2007) 106(4):582–92. doi: 10.3171/jns.2007.106.4.582
31. Szelényi A, Bello L, Duffau H, Fava E, Feigl GC, Galanda M, et al. Intraoperative electrical stimulation in awake craniotomy: methodological aspects of current practice. Neurosurg Focus. (2010) 28(2):E7. doi: 10.3171/2009.12.FOCUS09237
32. Michaud K, Duffau H. Surgery of insular and paralimbic diffuse low-grade gliomas: technical considerations. J Neurooncol. (2016) 130(2):289–98. doi: 10.1007/s11060-016-2120-2
33. Boetto J, Bertram L, Moulinié G, Herbet G, Moritz-Gasser S, Duffau H. Electrocorticography is not necessary during awake brain surgery for gliomas. World Neurosurg. (2016) 91:656–7. doi: 10.1016/j.wneu.2016.03.030
34. Duffau H. Lessons from brain mapping in surgery for low-grade glioma: insights into associations between tumour and brain plasticity. Lancet Neurol. (2005) 4(8):476–86. doi: 10.1016/S1474-4422(05)70140-X
35. Ojemann G, Ojemann J, Lettich E, Berger M. Cortical language localization in left, dominant hemisphere. An electrical stimulation mapping investigation in 117 patients. J Neurosurg. (1989) 71(3):316–26. doi: 10.3171/jns.1989.71.3.0316
36. Isolan GR, Buffon V, Maldonado I, Monteiro JM, Yağmurlu K, Ribas CAPM, et al. Avoiding vascular complications in insular glioma surgery - a microsurgical anatomy study and critical reflections regarding intraoperative findings. Front Surg. (2022) 9:906466. doi: 10.3389/fsurg.2022.906466
37. Wang Y, Wang Y, Fan X, Li S, Liu X, Wang J, et al. Putamen involvement and survival outcomes in patients with insular low-grade gliomas. J Neurosurg. (2017) 126(6):1788–94. doi: 10.3171/2016.5.JNS1685
38. Ghali MGZ. Preservation of the lenticulostriate arteries during insular glioma resection. Asian J Neurosurg. (2020) 15(1):16–21. doi: 10.4103/ajns.AJNS_146_18
39. Gotoh K, Okada T, Satogami N, Yakami M, Takahashi JC, Yoshida K, et al. Evaluation of CT angiography for visualisation of the lenticulostriate artery: difference between normotensive and hypertensive patients. Br J Radiol. (2012) 85(1019):e1004–8. doi: 10.1259/bjr/67294268
40. Sen T, Esmer AF, Acar HI, Karahan ST, Tuccar E. Arterial vascularisation of the anterior perforated substance. Singapore Med J. (2011) 52(6):410–4.21731992
41. Okuchi S, Okada T, Ihara M, Gotoh K, Kido A, Fujimoto K, et al. Visualization of lenticulostriate arteries by flow-sensitive black-blood MR angiography on a 1.5 T MRI system: a comparative study between subjects with and without stroke. AJNR Am J Neuroradiol. (2013) 34(4):780–4. doi: 10.3174/ajnr.A3310
42. Šteňo A, Jezberová M, Hollý V, Timárová G, Šteňo J. Visualization of lenticulostriate arteries during insular low-grade glioma surgeries by navigated 3D ultrasound power Doppler: technical note. J Neurosurg. (2016) 125(4):1016–23. doi: 10.3171/2015.10.JNS151907
43. Lang FF, Olansen NE, DeMonte F, Gokaslan ZL, Holland EC, Kalhorn C, et al. Surgical resection of intrinsic insular tumors: complication avoidance. J Neurosurg. (2001) 95(4):638–50. doi: 10.3171/jns.2001.95.4.0638
44. Mandonnet E, Sarubbo S, Duffau H. Proposal of an optimized strategy for intraoperative testing of speech and language during awake mapping. Neurosurg Rev. (2017) 40(1):29–35. doi: 10.1007/s10143-016-0723-x
45. Rosset A, Spadola L, Ratib O. Osirix: an open-source software for navigating in multidimensional DICOM images. J Digit Imaging. (2004) 17(3):205–16. doi: 10.1007/s10278-004-1014-6
46. Fisher RS, Cross JH, French JA, Higurashi N, Hirsch E, Jansen FE, et al. Operational classification of seizure types by the international league against epilepsy: position paper of the ILAE commission for classification and terminology. Epilepsia. (2017) 58(4):522–30. doi: 10.1111/epi.13670
47. Duffau H, Capelle L, Lopes M, Faillot T, Sichez JP, Fohanno D. The insular lobe: physiopathological and surgical considerations. Neurosurgery. (2000) 47(4):801–10. discussion 810–1. doi: 10.1097/00006123-200010000-00001
48. Buckner JC. Factors influencing survival in high-grade gliomas. Semin Oncol. (2003) 30(6 Suppl 19):10–4. doi: 10.1053/j.seminoncol.2003.11.031
49. Hervey-Jumper SL, Berger MS. Role of surgical resection in low- and high-grade gliomas. Curr Treat Options Neurol. (2014) 16(4):284. doi: 10.1007/s11940-014-0284-7
50. Sanai N, Berger MS. Glioma extent of resection and its impact on patient outcome. Neurosurgery. (2008) 62(4):753–64. discussion 264–6. doi: 10.1227/01.neu.0000318159.21731.cf
51. McGirt MJ, Chaichana KL, Attenello FJ, Weingart JD, Than K, Burger PC, et al. Extent of surgical resection is independently associated with survival in patients with hemispheric infiltrating low-grade gliomas. Neurosurgery. (2008) 63(4):700–7. author reply 707–8. doi: 10.1227/01.NEU.0000325729.41085.73
52. Dehaene S, Dupoux E, Mehler J, Cohen L, Paulesu E, Perani D, et al. Anatomical variability in the cortical representation of first and second language. Neuroreport. (1997) 8(17):3809–15. doi: 10.1097/00001756-199712010-00030
53. Kreth FW, Thon N, Simon M, Westphal M, Schackert G, Nikkhah G, et al. Gross total but not incomplete resection of glioblastoma prolongs survival in the era of radiochemotherapy. Ann Oncol. (2013) 24(12):3117–23. doi: 10.1093/annonc/mdt388
54. Grabowski MM, Recinos PF, Nowacki AS, Schroeder JL, Angelov L, Barnett GH, et al. Residual tumor volume versus extent of resection: predictors of survival after surgery for glioblastoma. J Neurosurg. (2014) 121(5):1115–23. doi: 10.3171/2014.7.JNS132449
55. Cordova JS, Schreibmann E, Hadjipanayis CG, Guo Y, Shu HK, Shim H, et al. Quantitative tumor segmentation for evaluation of extent of glioblastoma resection to facilitate multisite clinical trials. Transl Oncol. (2014) 7(1):40–7. doi: 10.1593/tlo.13835
56. Kramm CM, Wagner S, Van Gool S, Schmid H, Sträter R, Gnekow A, et al. Improved survival after gross total resection of malignant gliomas in pediatric patients from the HIT-GBM studies. Anticancer Res. (2006) 26(5B):3773–9.17094400
57. Ausman JI. Gross total resection: do we want survival statistics or quality of life measurements. Surg Neurol Int. (2014) 5:77. doi: 10.4103/2152-7806.133200
58. Esquenazi Y, Friedman E, Liu Z, Zhu JJ, Hsu S, Tandon N. The survival advantage of “supratotal” resection of glioblastoma using selective cortical mapping and the subpial technique. Neurosurgery. (2017) 81(2):275–88. doi: 10.1093/neuros/nyw174 Erratum in: Neurosurgery. 2017 August 1;81(2):404. Erratum in: Neurosurgery. 2017;81(6):1047.28368547
59. Keles GE, Anderson B, Berger MS. The effect of extent of resection on time to tumor progression and survival in patients with glioblastoma multiforme of the cerebral hemisphere. Surg Neurol. (1999) 52(4):371–9. doi: 10.1016/S0090-3019(99)00103-2
60. Büchel C, Morris J, Dolan RJ, Friston KJ. Brain systems mediating aversive conditioning: an event-related fMRI study. Neuron. (1998) 20(5):947–57. doi: 10.1016/S0896-6273(00)80476-6
61. Bucher SF, Dieterich M, Seelos KC, Brandt T. Sensorimotor cerebral activation during optokinetic nystagmus. A functional MRI study. Neurology. (1997) 49(5):1370–7. doi: 10.1212/WNL.49.5.1370
62. Burton H, Videen TO, Raichle ME. Tactile-vibration-activated foci in insular and parietal-opercular cortex studied with positron emission tomography: mapping the second somatosensory area in humans. Somatosens Mot Res. (1993) 10(3):297–308. doi: 10.3109/08990229309028839
63. Chollet F, DiPiero V, Wise RJ, Brooks DJ, Dolan RJ, Frackowiak RS. The functional anatomy of motor recovery after stroke in humans: a study with positron emission tomography. Ann Neurol. (1991) 29(1):63–71. doi: 10.1002/ana.410290112
64. Colebatch JG, Deiber MP, Passingham RE, Friston KJ, Frackowiak RS. Regional cerebral blood flow during voluntary arm and hand movements in human subjects. J Neurophysiol. (1991) 65(6):1392–401. doi: 10.1152/jn.1991.65.6.1392
65. Ghaem O, Mellet E, Crivello F, Tzourio N, Mazoyer B, Berthoz A, et al. Mental navigation along memorized routes activates the hippocampus, precuneus, and insula. Neuroreport. (1997) 8(3):739–44. doi: 10.1097/00001756-199702100-00032
66. Kettenmann B, Hummel C, Stefan H, Kobal G. Multiple olfactory activity in the human neocortex identified by magnetic source imaging. Chem Senses. (1997) 22(5):493–502. doi: 10.1093/chemse/22.5.493
67. Kobayakawa T, Endo H, Ayabe-Kanamura S, Kumagai T, Yamaguchi Y, Kikuchi Y, et al. The primary gustatory area in human cerebral cortex studied by magnetoencephalography. Neurosci Lett. (1996) 212(3):155–8. doi: 10.1016/0304-3940(96)12798-1
68. Kosslyn SM, DiGirolamo GJ, Thompson WL, Alpert NM. Mental rotation of objects versus hands: neural mechanisms revealed by positron emission tomography. Psychophysiology. (1998) 35(2):151–61. doi: 10.1111/1469-8986.3520151
69. Ebeling U, Schmid UD, Ying H, Reulen HJ. Safe surgery of lesions near the motor cortex using intra-operative mapping techniques: a report on 50 patients. Acta Neurochir (Wien). (1992) 119(1–4):23–8. doi: 10.1007/BF01541777
70. Haglund MM, Berger MS, Shamseldin M, Lettich E, Ojemann GA. Cortical localization of temporal lobe language sites in patients with gliomas. Neurosurgery. (1994) 34(4):567–76. discussion 576. doi: 10.1227/00006123-199404000-00001
71. Danks RA, Rogers M, Aglio LS, Gugino LD, Black PM. Patient tolerance of craniotomy performed with the patient under local anesthesia and monitored conscious sedation. Neurosurgery. (1998) 42(1):28–34. discussion 34–6. doi: 10.1097/00006123-199801000-00006
72. Taylor MD, Bernstein M. Awake craniotomy with brain mapping as the routine surgical approach to treating patients with supratentorial intraaxial tumors: a prospective trial of 200 cases. J Neurosurg. (1999) 90(1):35–41. doi: 10.3171/jns.1999.90.1.0035
73. Duffau H, Capelle L, Sichez N, Denvil D, Lopes M, Sichez JP, et al. Intraoperative mapping of the subcortical language pathways using direct stimulations. An anatomo-functional study. Brain. (2002) 125(Pt 1):199–214. doi: 10.1093/brain/awf016
74. Duffau H, Sichez JP. Intraoperative direct electrical stimulation of the lamina quadrigemina in a case of a deep tectal cavernoma. Acta Neurochir (Wien). (1998) 140(12):1309–12. doi: 10.1007/s007010050255
75. Duffau H, Capelle L, Sichez J. Direct spinal cord electrical stimulations during surgery of intramedullary tumoral and vascular lesions. Stereotact Funct Neurosurg. (1998) 71(4):180–9. doi: 10.1159/000029662
76. Fernández Coello A, Moritz-Gasser S, Martino J, Martinoni M, Matsuda R, Duffau H. Selection of intraoperative tasks for awake mapping based on relationships between tumor location and functional networks. J Neurosurg. (2013) 119(6):1380–94. doi: 10.3171/2013.6.JNS122470
77. Berger MS, Ojemann GA. Intraoperative brain mapping techniques in neuro-oncology. Stereotact Funct Neurosurg. (1992) 58(1–4):153–61. doi: 10.1159/000098989
78. Türe U, Yaşargil MG, Al-Mefty O, Yaşargil DC. Arteries of the insula. J Neurosurg. (2000) 92(4):676–87. doi: 10.3171/jns.2000.92.4.0676
79. Türe U, Yaşargil DC, Al-Mefty O, Yaşargil MG. Topographic anatomy of the insular region. J Neurosurg. (1999) 90(4):720–33. doi: 10.3171/jns.1999.90.4.0720
80. Rosner SS, Rhoton AL Jr, Ono M, Barry M. Microsurgical anatomy of the anterior perforating arteries. J Neurosurg. (1984) 61(3):468–85. doi: 10.3171/jns.1984.61.3.0468
81. Vincentelli F, Caruso G, Andriamamonjy C, Rabehanta P, Graziani N, Grisoli F, et al. Etude micro-anatomique des branches collatérales perforantes de l'artère cérébrale moyenne [micro-anatomy of collateral perforating branches of the middle cerebral artery]. Neurochirurgie. (1990) 36(1):3–14. discussion 14-5. French.2352590
82. Hentschel SJ, Lang FF. Surgical resection of intrinsic insular tumors. Neurosurgery. (2005) 57(1 Suppl):176–83. discussion 176–83. doi: 10.1227/01.neu.0000163603.70972.ab
83. Vanaclocha V, Sáiz-Sapena N, García-Casasola C. Surgical treatment of insular gliomas. Acta Neurochir (Wien). (1997) 139(12):1126–34. discussion 1134–5. doi: 10.1007/BF01410972
84. Zentner J, Meyer B, Stangl A, Schramm J. Intrinsic tumors of the insula: a prospective surgical study of 30 patients. J Neurosurg. (1996) 85(2):263–71. doi: 10.3171/jns.1996.85.2.0263
85. Delion M, Mercier P, Brassier G. Arteries and veins of the Sylvian fissure and insula: microsurgical anatomy. Adv Tech Stand Neurosurg. (2016) 43:185–216. doi: 10.1007/978-3-319-21359-0_7
86. Woody C. These were the 50 most violent cities in the world in 2017. Business Insider (2018). Available online at: https://www.businessinsider.com/most-violent-cities-in-the-world-2018-3?r=US&IR=T (retrieved January 28, 2022).
87. Working together to protect U.S. organizations overseas. OSAC (n.d.). Available online at: https://www.osac.gov/Country/Brazil/Content/Detail/Report/08a8af2f-06b2-4808-8692-15f4aecd6d7c (retrieved January 28, 2022).
88. Porto Alegre Registra Queda de 61,9% nos homicídios no mês de agosto. Portal do Estado do Rio Grande do Sul (2019). Available online at: https://estado.rs.gov.br/porto-alegre-tem-queda-de-61-9-nos-homicidios-em-agosto (retrieved January 28, 2022).
89. Krayenbühl N, Isolan GR, Hafez A, Yaşargil MG. The relationship of the fronto-temporal branches of the facial nerve to the fascias of the temporal region: a literature review applied to practical anatomical dissection. Neurosurg Rev. (2007) 30:8–15. doi: 10.1007/s10143-006-0053-5
90. Isolan GR, Campero A, Ajler P, Farina EM, Frigeri TM, Dini LI. Parte I: anatomía microquirúrgica tridimensional de la ínsula. Surg Neurol Int. (2020) 11:S21–36. doi: 10.25259/SNI_557_2020
Keywords: insular tumors, lenticulostriate arteries, Optic Chiasm - Insular Recess line, Porto Alegre Line, tumor resection
Citation: Isolan GR, Bark SA, Monteiro JM, Mattei TA, Yağmurlu K, Gonçalves RF, Malafaia O, Roesler R and Filho JMR (2025) Porto Alegre Line predicts lenticulostriate arteries encasement and extent of resection in insular gliomas. A preliminary study. Front. Surg. 12:1414302. doi: 10.3389/fsurg.2025.1414302
Received: 8 April 2024; Accepted: 7 January 2025;
Published: 10 February 2025.
Edited by:
Sabino Luzzi, University of Pavia, ItalyReviewed by:
Kuntal Kanti Das, Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGI), IndiaMuhammet Enes Gurses, University of Miami, United States
Copyright: © 2025 Isolan, Bark, Monteiro, Mattei, Yağmurlu, Gonçalves, Malafaia, Roesler and Filho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gustavo Rassier Isolan, Z3VzdGF2by5pc29sYW5AZmVtcGFyLmVkdS5icg==