
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Surg. , 09 December 2024
Sec. Colorectal and Proctological Surgery
Volume 11 - 2024 | https://doi.org/10.3389/fsurg.2024.1450434
This article is part of the Research Topic Advances in Proctology and Colorectal Surgery Volume II View all 8 articles
 Carlos Darcy Alves Bersot1,2
Carlos Darcy Alves Bersot1,2 Lucas Ferreira Gomes Pereira1,3
Lucas Ferreira Gomes Pereira1,3 Victor Gabriel Vieira Goncho1,2
Victor Gabriel Vieira Goncho1,2 José Eduardo Guimarães Pereira4Luiz Fernando dos Reis Falcão1,5*
José Eduardo Guimarães Pereira4Luiz Fernando dos Reis Falcão1,5*
Introduction: The relationship between the Enhanced Recovery After Surgery (ERAS) guidelines and inflammatory markers in laparoscopic surgery has garnered increasing attention. These recommendations are designed to minimize surgical stress and potentially improve recovery outcomes by modifying perioperative care.
Objective: This scoping review aims to evaluate the impact of ERAS recommendations on inflammatory markers in patients undergoing laparoscopic surgeries, identifying current research gaps and consolidating findings from existing studies.
Methods: Guided by the Cochrane Handbook for Systematic Reviews and adhering to the PRISMA-ScR guidelines, this review analyzed studies from databases like PubMed, Scopus, and Cochrane Library. We included both randomized controlled trials and observational studies that assessed inflammatory markers such as C-reactive protein (CRP), white blood cells (WBC), and Interleukin-6 (IL-6) in laparoscopic surgery patients managed with ERAS recommendations.
Results: Out of 64 initial studies, 7 met the inclusion criteria, involving a total of 2,047 patients. Most of the studies focused on laparoscopic colorectal surgeries. Commonly assessed markers were CRP and WBC. The findings consistently showed that ERAS guideline could mitigate the inflammatory response, evidenced by reduced levels of CRP and IL-6, which correlated with fewer postoperative complications and expedited recovery.
Conclusion: ERAS recommendations appear to beneficially modulate inflammatory responses in laparoscopic surgery, which suggests a potential for enhanced recovery outcomes. However, the evidence is currently limited by the small number of studies and inherent methodological biases. Further robust RCTs are required to strengthen the evidence base and refine these protocols for broader clinical application.
Systematic Review Registration: https://osf.io/tj8mw/
The association between inflammation and cancer has been extensively discussed since 1,863, when Virchow observed that tumors frequently develop at sites of chronic inflammation (1). Research has consistently demonstrated that inflammation contributes to tumor growth and aggressiveness; both preoperative and early postoperative inflammatory responses can foster a micrometastatic environment and adversely affect cancer prognosis (1–4).
The initiative to reduce recovery times after surgery was pioneered in the USA under the concept of “fast-track” surgery, particularly aimed at expediting recovery following cardiac procedures (5). Kehlet et al. further advanced this concept by developing a multimodal rehabilitation program focused on colorectal surgeries, which was successful in reducing hospital stay durations (6). The Enhanced Recovery After Surgery (ERAS) programs have refined these preliminary concepts into a standardized, evidence-based approach that enhances surgical outcomes across various disciplines. Originating in Europe, ERAS Society unites diverse surgical teams dedicated to fostering comprehensive, multi-professional patient care (7).
The cellular response to surgical tissue damage triggers the activation of macrophages and neutrophils within the innate immune system via the production of inflammatory cytokines, such as tumor necrosis factor (TNF) alpha, interleukin (IL)-1, and IL-6. These pro-inflammatory cytokines modify the levels of circulating acute-phase proteins, including C-reactive protein (CRP), albumin, ferritin, transferrin, and fibrinogen (8). However, the pathophysiology of post-surgical recovery is not solely a consequence of tissue injury but is inherently multifactorial, encompassing elements such as anxiety, pain, coagulation disorders, hemodynamic changes, and hypoxia. Given the multitude of factors that promote inflammation during the surgical stress response, interventions proposed by the ERAS guidelines address these various components comprehensively (9).
This scoping review aims to provide a descriptive summary of the studies included and to identify potential gaps in the literature regarding the impact of the ERAS guidelines on the inflammatory response following laparoscopic surgery. The guiding question for this review is: “What research has been conducted on the impact of the ERAS recommendations on inflammatory markers in laparoscopic surgery, and what evidence is available regarding its effects on the immune system?”
This scoping review was guided by the Cochrane Handbook for Intervention Reviews (10) and conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extensions for Scoping Reviews (PRISMA-ScR) (11). The research protocol was registered on the Open Science Framework (https://osf.io/tj8mw/).
We included randomized controlled trials and observational studies assessing the impact of the Enhanced Recovery After Surgery (ERAS) recommendations on inflammatory markers in patients undergoing laparoscopic surgery. Eligible participants were adults aged 18 years or older who underwent any type of laparoscopic surgery and had one or more of the following inflammatory biomarkers measured: C-reactive protein (CRP), white blood cell count (WBC), immunoglobulins (IgG and IgA), tumor necrosis factor (TNF), total protein (TP), cortisol, among others.
The intervention study groups will be considered those adopting any series of measures aimed at optimizing and accelerating recovery in the perioperative period, while the control group will be considered the population with traditional perioperative care. Both nomenclatures will be considered for the intervention group, both ERAS and Fast-track will be accepted.
The literature search was conducted using PubMed (MEDLINE), Scopus, Embase, Web of Science, and the Cochrane Controlled Register of Trials (CENTRAL). We also searched for unpublished studies and gray literature through manual searches of reference lists of included articles. The initial search was performed in January 2024, with a follow-up search in February 2024. Searches employed combinations of MeSH terms and their synonyms including “Enhanced Recovery After Surgery,” “Inflammation,” and “Laparoscopy.” Our search strategies, adapted for each database, are detailed in Appendices I and II. No restrictions were placed on language or publication date.
Three reviewers (VGVG, LFGP, CDAB) independently screened titles and abstracts using a standardized screening protocol. Full texts of potentially relevant studies were retrieved, and their details uploaded into Rayyan® (Qatar Computing Research Institute, Doha, Qatar) (12). Disagreements among reviewers were resolved through discussion or consultation with a third party (JEGP, LFRF).
Data were extracted independently by the same four reviewers using a specially developed form. Extracted information included publication year, country, study type, surgical type, population characteristics, ERAS recommendations details, inflammatory markers, and pertinent findings. Authors were contacted to resolve data discrepancies or clarify missing details.
Risk of bias was assessed using the Guyatt-modified Cochrane approach for randomized trials (13, 14) and the Morgan approach for non-randomized studies (15). The criteria for randomized trials included adequacy of random sequence generation, allocation concealment, blinding (of investigators, patients, data collectors, statisticians, outcome assessors), completeness of outcome data, and absence of selective reporting. A threshold of less than 10% total loss to follow-up was considered low risk. Non-randomized studies were assessed for eligibility criteria, outcome and exposure measurement accuracy, confounder control, and follow-up adequacy.
Data were synthesized and displayed in two tables highlighting the characteristics of the ERAS recommendations and the inflammatory markers assessed. Details such as publication year, country, study type, surgical type, ERAS details, and outcomes were tabulated. If the outcomes found and summarized in the results are amenable to quantitative analysis, they will be analyzed by means of a meta-analysis, divided into different outcomes.
Our systematic database search initially identified 64 studies. After removing 9 duplicates, 55 records were screened by title and abstract, with 43 subsequently excluded. Full texts of the remaining 12 studies were evaluated for eligibility, resulting in 5 further exclusions. Ultimately, 7 studies met our inclusion criteria. The selection process is depicted in the PRISMA flowchart (Figure 1).
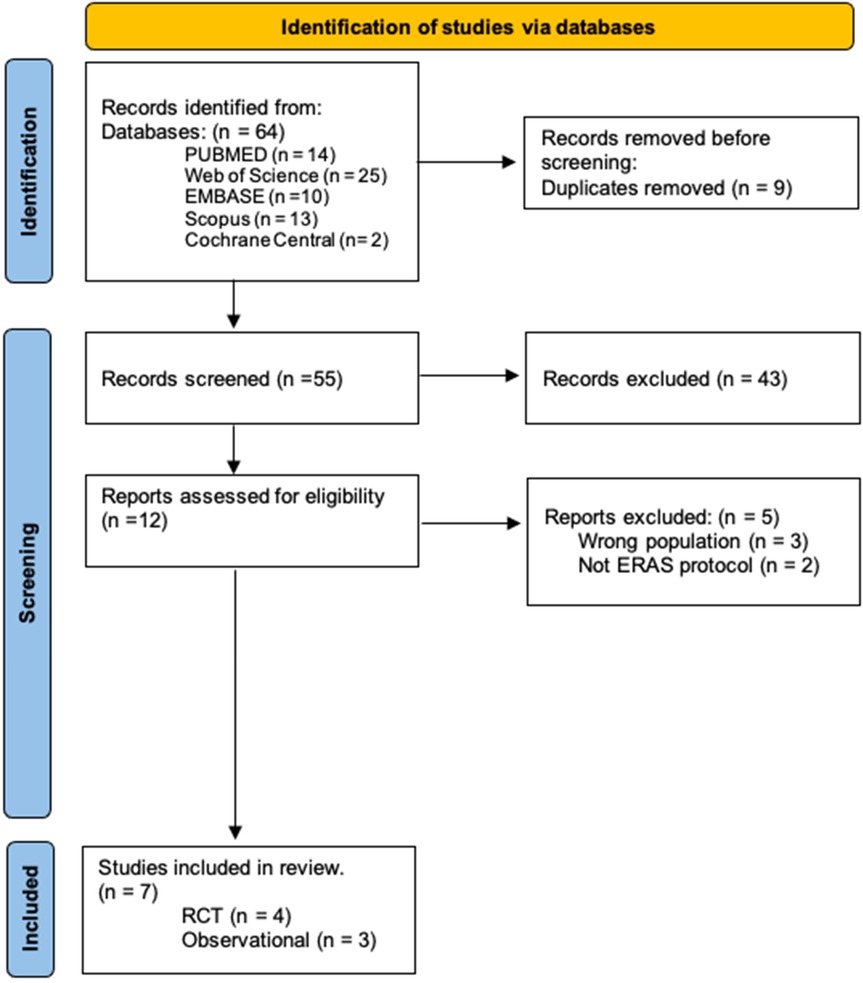
Figure 1. PRISMA flowchart.
The included studies were published between 2012 and 2022. Four of these were randomized clinical trials, and three were non-randomized observational studies (Table 1). The studies involved both male and female participants, with the ERAS group having a mean age of 59.7 years-old compared to 49.7 years-old in the control group. Geographically, four studies were conducted in China (16–19), one in Italy (20), and one in South Korea (21) (Tables 2, 3). The surgical interventions examined included colorectal surgeries (16–18, 20, 21), gastrectomy (19), and gynecological oncological surgery (22).

Table 1. Study characteristics according to population and type of publication.
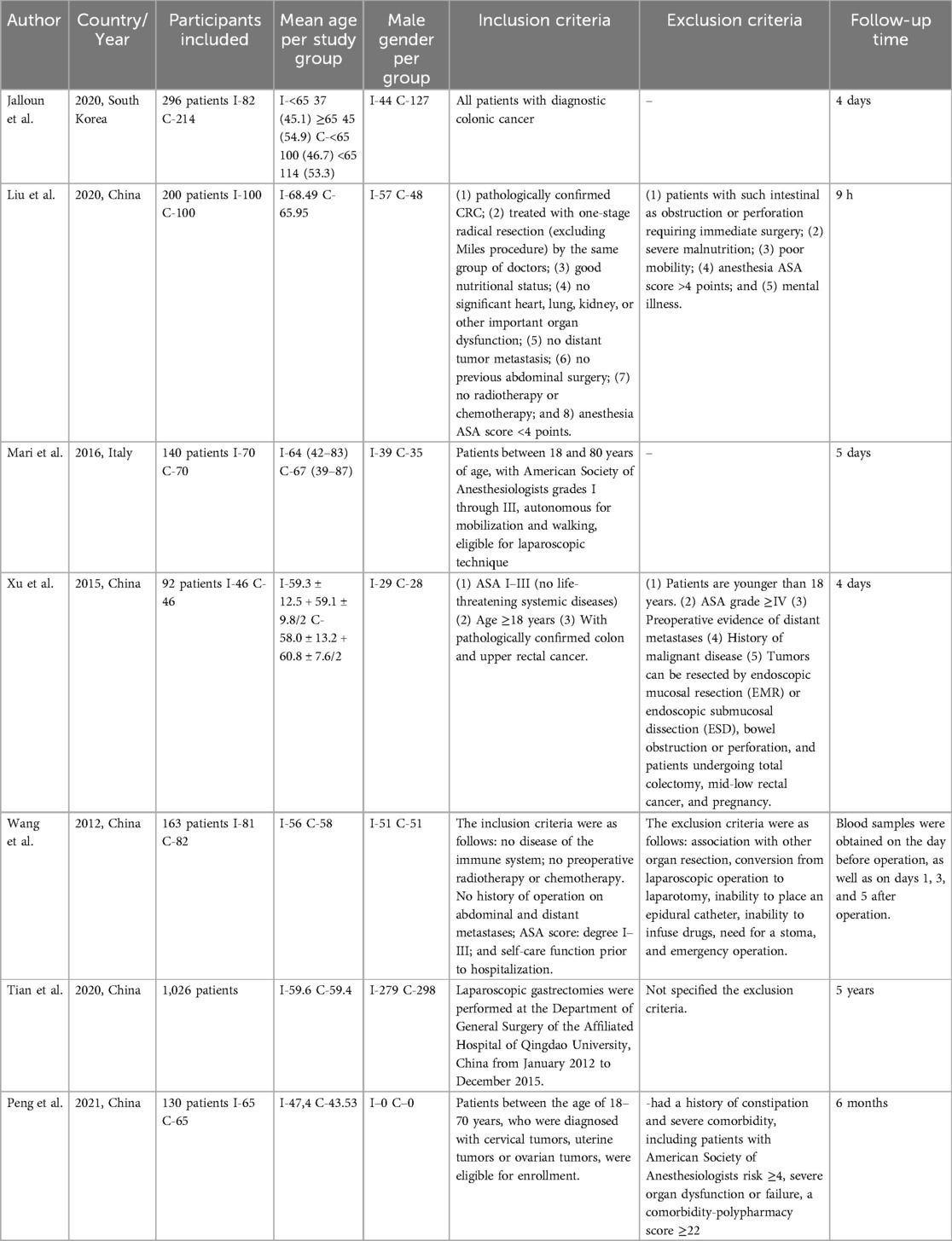
Table 2. Study characteristics related to population and setting.
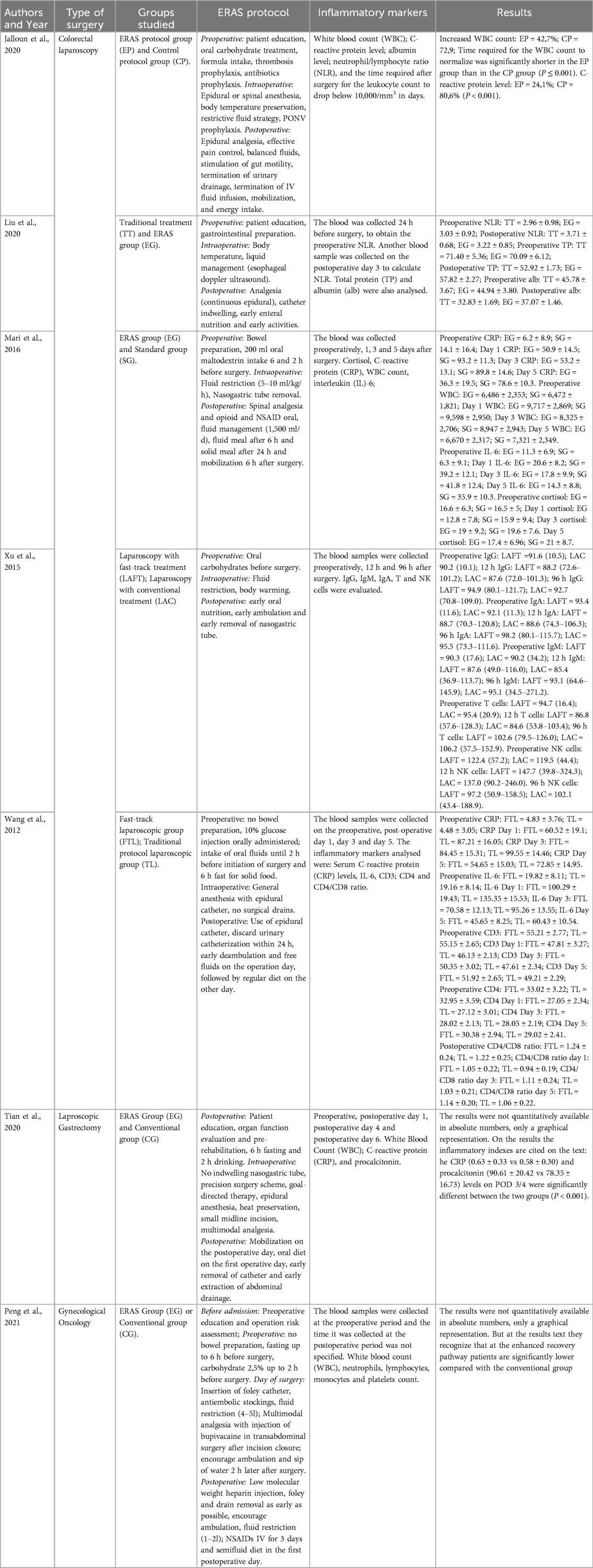
Table 3. Assessment of the ERAS protocol and the inflammatory markers analyzed.
The ERAS recommendations varied but commonly included preoperative patient education, a 6 h fasting period, and carbohydrate-rich liquids up to 2 h before surgery. Intraoperative measures focused on fluid restriction, body temperature maintenance, and multimodal anesthetic strategies, including epidural anesthesia in four studies. Postoperative care emphasized early mobilization across all studies.
Blood samples were collected at various times: six studies (16–20, 22) during the intraoperative period, one study (17) 12 h post-surgery, 4 studies (18–21) collected on the first postoperative day, 3 studies (16, 18, 20) collected on the 3rd postoperative day, 2 studies (17, 19) collected on the 4th postoperative day and 2 studies (18, 20) on the 5th postoperative day, and Tian et al. (19) was the only study to analyze samples on the 6th postoperative day. Inflammatory markers analyzed included white blood count (WBC) (19–22), C-reactive protein (CRP) (18–21), albumin (16, 21), neutrophil/lymphocyte ratio (NLR) (16, 21, 22), total protein (TP) (16), cortisol (20), interleukin-6 (IL-6) (18, 20), immunoglobulin (Ig) G, IgM, IgA (17), T lymphocytes (17, 18), natural killer (NK) cells (17), procalcitonin (19), and platelet count (22) (Table 3).
Randomized studies showed adequate random sequence generation and allocation concealment. Blinding of participants was achieved, but not for surgical staff due to the nature of the procedures. We did not consider this at high risk of bias because those outcomes cannot be influenced by the participants. Blinding of caregivers was considered at high risk due to the impossibility to hide surgical technique from them. Blinding of data collectors, statisticians, and outcome assessors were considered at low risk of bias in all studies. There were no studies reporting total loss to follow-up above the 10% threshold nor above 5% between groups. Therefore, loss to follow-up was considered as low risk of bias (Table 4).

Table 4. Risk of bias randomized studies.
Non-randomized studies showed critical. Bias due to confounding was considered critical in two studies (19, 21), and considered to be serious in one study (19), because they did not correct the adequate non-exposed cohort groups for confounding factors. Bias in selection of participants was considered to be serious in all observational studies (16, 19, 21), because selection was offered, and not encompassing all the patients. Bias in classification of exposures was considered moderate in three studies (16, 19, 21) because information was self-reported. Bias due to missing data was considered serious in all studies (16, 19, 21) due to the design of the studies (Tables 5, 6).

Table 5. Risk of bias non-randomized studies.
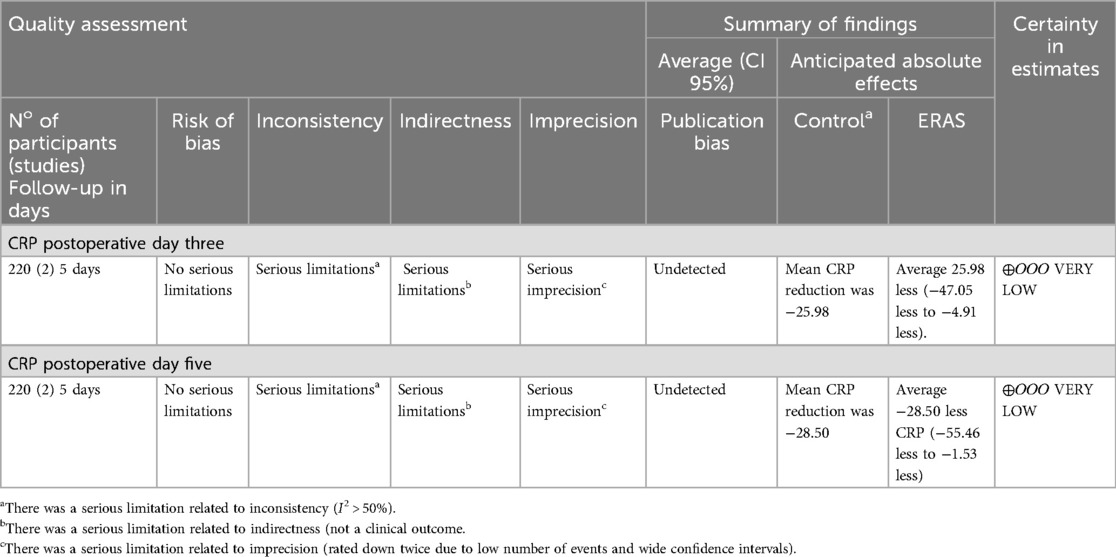
Table 6. Assessment of GRADE.
C-reactive protein (CRP): has been investigated in two observational studies (19, 21) and two RCTs (18, 20). The studies included 1,322 patients in the retrospective cohorts (19, 21) and 303 patients in two RCTs (18, 20). It found significantly lower levels of CRP in ERAS group when compared with standard on postoperative day (POD) 1, 3, and 5. All retrospective studies found lower plasma concentrations of CRP after laparoscopy when compared to open surgery. Jelloun et al. (21), 2020, including 296 patients, found an increase in CPR count of 24.1% in the ERAS group and an increase of 80.6% in the control group (p < 0.001). Tian et al. (19), 2020, including 1,026 patients, found no significant reduction of CRP in the ERAS group compared to the control group. Mari et al. (20), 2016, including 140 patients, found that ERAS protocol significantly reduced the rise slope of CRP on postoperative days, 1, 3, and 5 (p < 0,05) compared to the control group. Results from two RCTs, including 220 participants, found a significant reduction on the rising slope of C-reactive protein on postoperative day three in the ERAS group compared to the control group (MD: −25.98, 95% CI: −47.05, −4.91; p = 0.02; I2 = 96%). Certainty of evidence was considered very low due to imprecision (wide confidence interval and low number of patients), inconsistency (from high heterogeneity) and indirectness (Figure 2).

Figure 2. Comparison of CRP on postoperative days three between ERAS and control groups.
Results from two RCTs (18, 20), including 220 participants, found a significant reduction on the rising slope of C-reactive protein on postoperative day five in the ERAS group compared to the control group (MD: −28.50 95% CI: −55.46, −1.53; p = 0.04; I2 = 98%). Certainty of evidence was considered very low due to imprecision (wide confidence interval and low number of patients), inconsistency (from high heterogeneity) and indirectness (Figure 3).

Figure 3. Comparison of CRP on postoperative days five between ERAS and control groups.
White blood cell count (WBC): two observational (19, 21) and two RCT (20, 22) analyzed this inflammatory marker. They found significant reduction of WBC in the ERAS group compared to control on POD 1, 3, and 5. Jaloun et al. (21), 2020, including 296 patients, found an increase on WBC count of 42.7% in the ERAS group and an increase of 72.9% in the control group. Time required for the WBC count to normalize was significantly shorter in the ERAS group than in the control group (p ≤ 0.001). Tian et al. (19), 2020, including 1,026 patients. Although results were not quantitatively available in absolute numbers, a graphic representation suggests that WBC did not increase as much in the ERAS group as it did in the control. Both randomized control trials by Peng et al. (22), including 130 patients, and Mari et al. (20), including 140 patients, found no significant reduction of WBC in the ERAS group compared to the control group.
Interleukin-6 (IL-6): Two RCTs (18, 20) evaluated the impact of the ERAS protocol on patients undergoing laparoscopic surgery and the IL-6 marker. A total population of 303 patients, both studies found significantly lower levels of IL-6 on POD 3 after ERAS protocol groups vs. standard groups.
This scoping review evaluates the impact of Enhanced Recovery After Surgery (ERAS) recommendation measures during the perioperative period on inflammatory markers in patients undergoing laparoscopic surgery. It aims to elucidate consistent findings, recognize knowledge gaps, and suggest directions for future research on both existing and novel inflammatory markers.
The initial studies following the conceptualization of ERAS by Kehlet et al. (6) focused predominantly on morbidity, mortality, and surgical complications, rather than on the quantitative assessment of inflammatory markers. It took 13 years from the inception of this concept for the first study analyzing the influence of ERAS on inflammatory markers in laparoscopic surgeries to be published.
According to literature, open surgery, amongst several other factors, such as age >70 years, BMI ≥30 kg/m2, ASA score >2, dirty/contaminated surgery, as well as comorbidities (diabetes and chronic steroid use) were associated with significantly higher incidence of surgical site infection (SSI) (23, 24).
Results from literature regarding index admission and total expenses, including 30-day readmissions, demonstrated that laparoscopic approach is less expensive than open surgery and with shorter hospital length of stay (25).
Laparoscopic colorectal surgery was the most examined procedure, covered in five of the seven included studies. These studies collectively analyzed a total of 2,047 patients, with 891 undergoing colorectal procedures. The largest study, by Tian et al. (19), involved 1,026 patients and examined laparoscopic gastrectomy.
White blood cell count, and C-reactive protein were the most frequently assessed markers, each studied in four investigations. Notably, critical inflammatory markers such as tumor necrosis factor-alpha and alpha 1-acid glycoprotein were absent from the studies reviewed, representing a significant gap in the literature. Markers such as neutrophil gelatinase-associated lipocalin (NGAL) and N-terminal pro B-type natriuretic peptide (NT-proBNP), which indicate organ damage, were also not evaluated.
An innovative strategy that can be incorporated into perioperative optimization protocols is the adoption of probiotics in the perioperative period, a topic that was studied by Xiong et al. (26) In the 2023 (27) and 2024 study (26), patients undergoing radical distal gastrectomy were divided into two groups, probiotics vs. placebo. The group administered probiotics reduced the post-operative inflammatory response, accelerated the fall in the neutrophil-lymphocyte ratio (NLR), and promoted a faster increase in serum albumin concentration, further studies should be conducted to possibly add another tool to ERAS.
Inflammatory markers can also be useful for predicting postoperative complications, which can delay early discharge, one of the pillars of the perioperative optimization scenario. The study by Van Daele et al. (28) analyzed the diagnostic accuracy of biomarkers for anastomotic fistula in patients undergoing esophagectomy. When analyzing 5,348 patients (28), C-reactive protein was found to be a reliable negative predictor, indicating a low probability of fistula and supporting safe early discharge in the ERAS protocol.
All reviewed studies reported benefits of the ERAS recommendations over standard care, notably in reducing the surgical stress response, as evidenced by lower levels of IL-6, CRP, and WBCs. Moreover, a trend towards fewer postoperative complications was observed in ERAS patients, although statistical significance was achieved in only one study.
Our findings support the literature showing a beneficial impact of ERAS recommendations, particularly noted in significant reductions of CRP levels on postoperative days three and five (Figures 2, 3). However, the overall certainty of this evidence remains very low due to issues with precision, consistency, and directness.
This review's strengths lie in its methodical approach, including a comprehensive search, systematic selection, and rigorous bias assessment, independently replicated by multiple reviewers. Additionally, the GRADE approach was employed to enhance the reliability of evidence evaluation. Conversely, the primary limitations stem from high variability in study outcomes, insufficient blinding of surgical teams, and the reliance on a limited number of small-scale studies, which collectively restrict the precision and applicability of the findings.
This scoping review highlights the need for additional randomized controlled trials (RCTs) to more precisely determine the effects and validate the impact of Enhanced Recovery After Surgery (ERAS) recommendations on inflammatory markers in laparoscopic surgery. The preliminary findings suggest that the implementation of ERAS guidelines may significantly reduce inflammatory markers, potentially leading to enhanced recovery outcomes for patients undergoing laparoscopic procedures. However, due to the limited number of studies and their small sample sizes, the certainty of these findings remains very low, emphasizing the importance of further high-quality research to provide more definitive evidence and refine clinical practice guidelines.
CA: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. LF: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. VG: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JP: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. LF: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. (2008) 454(7203):436–44. doi: 10.1038/nature07205
2. Coussens LM, Werb Z. Inflammation and cancer. Nature. (2002) 420(6917):860–7. doi: 10.1038/nature01322
3. Lu H, Ouyang W, Huang C. Inflammation, a key event in cancer development. Mol Cancer Res. (2006) 4(4):221–33. doi: 10.1158/1541-7786.MCR-05-0261
4. Paik KY, Lee IK, Lee YS, Sung NY, Kwon TS. Clinical implications of systemic inflammatory response markers as independent prognostic factors in colorectal cancer patients. Cancer Res Treat. (2014) 46(1):65–73. doi: 10.4143/crt.2014.46.1.65
5. Engelman RM, Rousou JA, Flack JE III, Deaton DW, Humphrey CB, Ellison LH, et al. Fast-track recovery of the coronary bypass patient. Ann Thorac Surg. (1994) 58(6):1742–6. doi: 10.1016/0003-4975(94)91674-8
6. Kehlet H, Mogensen T. Hospital stay of 2 days after open sigmoidectomy with a multimodal rehabilitation programme. Br J Surg. (1999) 86(2):227–30. doi: 10.1046/j.1365-2168.1999.01023.x
7. Brindle M, Nelson G, Lobo DN, Ljungqvist O, Gustafsson UO. Recommendations from the ERAS® society for standards for the development of enhanced recovery after surgery guidelines. BJS Open. (2020) 4(1):157–63. doi: 10.1002/bjs5.50238
8. Lord JM, Midwinter MJ, Chen YF, Belli A, Brohi K, Kovacs EJ, et al. The systemic immune response to trauma: an overview of pathophysiology and treatment. Lancet. (2014) 384(9952):1455–65. doi: 10.1016/S0140-6736(14)60687-5
9. Carli F. Physiologic considerations of enhanced recovery after surgery (ERAS) programs: implications of the stress response. Can J Anaesth. (2015) 62(2):110–9. doi: 10.1007/s12630-014-0264-0
10. Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. (2019) 10:Ed000142. doi: 10.1002/14651858.ED000142
11. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169(7):467–73. doi: 10.7326/M18-0850
12. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5(1):210. doi: 10.1186/s13643-016-0384-4
13. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. Br Med J. (2011) 343:d5928. doi: 10.1136/bmj.d5928
14. Guyatt GH, Schünemann HJ, Djulbegovic B, Akl EA. Guideline panels should not GRADE good practice statements. J Clin Epidemiol. (2015) 68(5):597–600. doi: 10.1016/j.jclinepi.2014.12.011
15. Morgan RL, Thayer KA, Santesso N, Holloway AC, Blain R, Eftim SE, et al. A risk of bias instrument for non-randomized studies of exposures: a users’ guide to its application in the context of GRADE. Environ Int. (2019) 122:168–84. doi: 10.1016/j.envint.2018.11.004
16. Liu X, Wang Y, Fu Z. Impact of enhanced recovery after surgery on postoperative neutrophil-lymphocyte ratio in patients with colorectal cancer. J Int Med Res. (2020) 48(6):300060520925941. doi: 10.1177/0300060520925941
17. Xu D, Li J, Song Y, Zhou J, Sun F, Wang J, et al. Laparoscopic surgery contributes more to nutritional and immunologic recovery than fast-track care in colorectal cancer. World J Surg Oncol. (2015) 13:18. doi: 10.1186/s12957-015-0445-5
18. Wang G, Jiang Z, Zhao K, Li G, Liu F, Pan H, et al. Immunologic response after laparoscopic colon cancer operation within an enhanced recovery program. J Gastrointest Surg. (2012) 16(7):1379–88. doi: 10.1007/s11605-012-1880-z
19. Tian YL, Cao SG, Liu XD, Li ZQ, Liu G, Zhang XQ, et al. Short- and long-term outcomes associated with enhanced recovery after surgery protocol vs conventional management in patients undergoing laparoscopic gastrectomy. World J Gastroenterol. (2020) 26(37):5646–60. doi: 10.3748/wjg.v26.i37.5646
20. Mari G, Crippa J, Costanzi A, Mazzola M, Rossi M, Maggioni D. ERAS protocol reduces IL-6 secretion in colorectal laparoscopic surgery: results from a randomized clinical trial. Surg Laparosc Endosc Percutan Tech. (2016) 26(6):444–8. doi: 10.1097/SLE.0000000000000324
21. Jaloun HE, Lee IK, Kim MK, Sung NY, Turkistani SAA, Park SM, et al. Influence of the enhanced recovery after surgery protocol on postoperative inflammation and short-term postoperative surgical outcomes after colorectal cancer surgery. Ann Coloproctol. (2020) 36(4):264–72. doi: 10.3393/ac.2020.03.25
22. Peng J, Dong R, Jiao J, Liu M, Zhang X, Bu H, et al. Enhanced recovery after surgery impact on the systemic inflammatory response of patients following gynecological oncology surgery: a prospective randomized study. Cancer Manag Res. (2021) 13:4383–92. doi: 10.2147/CMAR.S294718
23. Panos G, Mulita F, Akinosoglou K, Liolis E, Kaplanis C, Tchabashvili L, et al. Risk of surgical site infections after colorectal surgery and the most frequent pathogens isolated: a prospective single-centre observational study. Med Glas (Zenica). (2021) 18(2):438–43. doi: 10.17392/1348-21
24. Mulita F, Liolis E, Akinosoglou K, Tchabashvili L, Maroulis I, Kaplanis C, et al. Postoperative sepsis after colorectal surgery: a prospective single-center observational study and review of the literature. Prz Gastroenterol. (2022) 17(1):47–51. doi: 10.5114/pg.2021.106083
25. Ribeiro U Jr, Tayar DO, Ribeiro RA, Andrade P, Junqueira SM Jr. Laparoscopic vs open colorectal surgery: economic and clinical outcomes in the Brazilian healthcare. Medicine (Baltimore). (2020) 99(42):e22718. doi: 10.1097/MD.0000000000022718
26. Xiong H, He Z, Wei Y, Li Q, Xiao Q, Yang L, et al. Probiotic compounds enhanced recovery after surgery for patients with distal gastric cancer: a prospective, controlled clinical trial. Ann Surg Oncol. (2024) 31(8):5240–51. doi: 10.1245/s10434-024-15394-7
27. Liu Z, Li N, Dang Q, Liu L, Wang L, Li H, et al. Exploring the roles of intestinal flora in enhanced recovery after surgery. iScience. (2023) 26(2):105959. doi: 10.1016/j.isci.2023.105959
28. Van Daele E, Vanommeslaeghe H, Peirsman L, Van Nieuwenhove Y, Ceelen W, Pattyn P. Early postoperative systemic inflammatory response as predictor of anastomotic leakage after esophagectomy: a systematic review and meta-analysis. J Gastrointest Surg. (2024) 28(5):757–65. doi: 10.1016/j.gassur.2024.02.003
Keywords: enhanced recovery after surgery, inflammation, laparoscopy, anesthesia, surgery
Citation: Alves Bersot CD, Ferreira Gomes Pereira L, Goncho VGV, Pereira JEG and Falcão LFdR (2024) Enhancing recovery and reducing inflammation: the impact of enhanced recovery after surgery recommendations on inflammatory markers in laparoscopic surgery—a scoping review. Front. Surg. 11:1450434. doi: 10.3389/fsurg.2024.1450434
Received: 17 June 2024; Accepted: 25 November 2024;
Published: 9 December 2024.
Edited by:
Vito D’Andrea, Sapienza University of Rome, ItalyReviewed by:
Theodoros Aslanidis, Agios Pavlos General Hospital, GreeceCopyright: © 2024 Alves Bersot, Ferreira Gomes Pereira, Goncho, Pereira and Falcão. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luiz Fernando dos Reis Falcão, ZmFsY2FvQHVuaWZlc3AuYnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.