 László Libor
László Libor Balázs Pécsy1
Balázs Pécsy1 Judit Lantos
Judit Lantos József Furák
József Furák
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Surg. , 01 July 2024
Sec. Thoracic Surgery
Volume 11 - 2024 | https://doi.org/10.3389/fsurg.2024.1430100
This article is part of the Research Topic Near-Infrared Fluorescence Guided Surgery: State of the evidence from a health technology assessment perspective View all 10 articles
For early-stage non-small cell lung cancer, surgical resection remains the best treatment option. Currently, sublobar resection, including segmentectomy, is recommended in these cases, as it provides a better quality of life with the same oncological outcomes; however, is requires adequate resection margins. Accurate preoperative planning and proper identification of the intersegmental planes during thoracic surgery are crucial for ensuring precise surgical management and adequate resection margins. Three dimensional computed tomography reconstruction and near-infrared-guided intersegmental plane identification can greatly facilitate the surgical procedures. Three-dimensional computed tomography reconstruction can simulate both the resection and resection margins. Indocyanine green is one of the most frequently used and affordable fluorophores. There are two ways to identify the intersegmental planes using indocyanine green: intravenous and transbronchial administration. Intravenous application is simple; however, its effectiveness may be affected by underlying lung disease, and it requires the isolation of segmental structures before administration. Transbronchial use requires appropriate bronchoscopic skills and preoperative planning; however, it also allows for delineation deep in the parenchyma and can be used for complex segmentectomies. Both methods can be used to ensure adequate resection margins and, therefore, achieve the correct oncological radicality of the surgical procedure. Here, we summarise these applications and provide an overview of their different possibilities.
Surgical resection remains one of the best therapeutic options for the long-term survival of patients with early stage non-small cell lung cancer (NSCLC) (1). Multicentre trials have shown that there is no significant difference in 5-year survival between lobectomy and segmentectomy or sublobar resection in early-stage (Stage IA) NSCLC, where the tumour size is ≤2 cm. In the JCOG0802/WJOG4607l trial, the 5-year relapse-free survival rates were 87.9% and 88.0%, respectively, while the 5-year overall survival rates were 91.1% and 94.3%, respectively, for lobectomy and segmentectomy. In the CALGB clinical trial, the 5-year disease-free survival rates were 64.1% and 63.6%, and the 5-year overall survival rates were 78.9% and 80.3%, respectively (lobectomy vs. sublobar resection). Notably, the proportion of anatomical segmentectomies among sublobar resections in this study was 37.9% compared to 59.1% for wedge resections. However, the incidence of locoregional recurrence was significantly higher in patients who underwent segmentectomy (11% vs. 5%, segmentectomy vs. lobectomy P = 0.0018) in the JCOG0802/WJOG4607l trial. Similarly, in the CALGB trial, locoregional recurrence was observed in 10.0% of the lobectomies and 13.4% of the sublobar resections (2, 3). Importantly, tumours located in the periphery of the lungs (an indication for segmentectomy) may have a higher locoregional recurrence rate (4).
Due to the development of a variety of national screening programs and sensitive diagnostics, an increasing number of early stage lung cancers are being detected (5). With the increase in minimally invasive surgical procedures, video-assisted thoracic surgery (VATS) (6, 7) and robot-assisted thoracic surgery (8) have emerged and are now the preferred procedures for early stage lung cancer surgery, providing better perioperative outcomes with reduced postoperative pain, improved quality of life, and equivalent oncological outcomes compared to open surgery.
Despite the use of more complex surgical techniques, such as the identification of intersegmental planes (ISP), the complication rate was comparable between VATS segmentectomies and lobectomies, and the length of stay and drainage time were reduced for segmentectomies (9). Patients with early stage NSCLC (≤2 cm) localised in the outer third of the parenchyma are candidates for segmentectomy. Accordingly, the European Society of Thoracic Surgeons has formulated recommendations for segmentectomy for early NSCLC (10).
Inadequate resection margins and lymph node removal are the main causes of locoregional recurrence. Therefore, ensuring and defining adequate margins and lymph node status are crucial for reducing local recurrence rates in segmentectomies (2, 3). To ensure adequate resection margins, it is important to identify the ISP.
The standard approach for segmentectomy is to perform vascular and bronchial transections, and then divide the ISPs. There are different preoperative and intraoperative methods for tumour localisation and identification of the ISPs. Chest computed tomography (CT) and its three-dimensional (3D) reconstruction are important in preoperative planning. A virtual bronchogram and accurate identification of vascular structures, segments, or planes can make the procedure safer and allow for complete resection (11). Near-infrared (NIR)-guided surgery is a relatively new technique that makes it easier to identify the ISPs. Indocyanine green (ICG) can be used to visualise segmental boundaries, eliminating the need for traditional inflation or deflation methods, and can be administered intravenously or via endobronchial injections (12, 13).
Using fluorophores, the localisation of lesions and their intraoperative visualisation can be used to determine the proper resection margins. Pafolacianine is a novel fluorophore used for intraoperative molecular imaging (IMI) (14). In this narrative review, we discuss the advantages and disadvantages of ICG administration methods by comparing the characteristics of different applications, and the role of preoperative 3D CT reconstruction.
This narrative review aims to discuss the relevant literature regarding the different applications of ICG, and the impact of NIR-guided surgery on the resection margins during thoracoscopic segmentectomy in early-stage NSCLC. We searched the literature on PubMed. The search was narrowed to articles between 2017 and 2023. The keywords used in the search were “thoracoscopic segmentectomy”, “near-infrared fluorescence”, “indocyanine green”, “resection margin”, “transbronchial”, “endobronchial” and “intravenous”. Eventually, after reviewing the abstracts, 8 articles were selected for analysis. The following questions were investigated in the articles we reviewed. What are the advantages and disadvantages of different applications of ICG in NIR-guided lung surgery? How does NIR fluorescence imaging help to achieve adequate resection margins in early-stage NSCLCs? How does preoperative 3D CT reconstruction facilitate surgical planning? After reviewing the articles, we summarized the information that we found relevant in the form of text and tables.
To perform lung segmentectomy, the surgeon must be familiar with the radiologic segmental anatomy. Preoperative review of chest CT scans helps to localise the nodule and determine the anatomy of the segment, mapping the bronchi and blood vessels. High-resolution CT scans provide an accurate picture of the segmental anatomy and 3D reconstructions help to accurately define the tumour and segmental structures and visualise bronchovascular variations. It is essential to identify the arteries and bronchi of the target segment, as well as the intrasegmental veins, and to preserve the intersegmental veins as a prerequisite for identifying the intersegmental planes. This is greatly facilitated by appropriate 3D reconstruction (15). Additionally, segmentectomies can be simulated using virtually defined intersegmental planes and resection margins. Together, these methods facilitate surgical planning and help to prevent locoregional recurrence by aiding in defining the resection margins (2, 16).
Most authors use thin-slice (1 mm) chest CT with intravenous contrast. For 3D reconstruction, the two software packages “Synapse Vincent” (Fujifilm, Tokyo, Japan) and “Ziostation2” (Ziosoft, Inc., Tokyo, Japan) are often used. These scans are used to automatically reconstruct the vasculature, bronchial tree, and parenchyma. In addition, tumour localisation, adjacent anatomical structures, virtual intersegmental planes, resection margins, and segment volumes can be determined in collaboration with the surgeon. One of the most important applications of CT is planning the resection margin. The shortest distance between the tumour and planned resection line was determined using reconstruction software. The nearest resection margin was defined as being at least 2 cm from the tumour or greater than its diameter. Resection distances were defined according to the recommendations of Sawabata et al. (17). If this was less, the planned resection was extended to the adjacent segments. Thus, complex or multiple segmentectomies can be planned. The concordance rate between the simulated and specimen resection margins and between segmental structures was 90% or above (18–20).
Chang et al. performed intraoperative cone-beam CT in addition to preoperative 3D CT planning. This rare procedure requires a hybrid operating room. During NIR guidance (intravenously administered ICG), the defined intersegmental planes were marked with metal clips and verified during the CT scan and 3D reconstruction. The resection margins were then calculated. Intraoperative CT scan was performed under bilateral ventilation. The planned resection margins were determined by the distance between the tumour, the intersegmental planes marked with metal clips, and the planned stapler line. If the calculated resection margin was less than 2 cm, the resection was extended to adjacent segments. The median time of the intraoperative CT scan was 10.5 min despite the complexity of the procedure. The concordance rate between intraoperatively reconstructed 3D CT scans and preoperatively simulated scans was 97.1% (21). The correlation and/or difference between the calculated preoperative and intraoperative resection margins and the resection margins measured on the specimens are shown in Table 1.
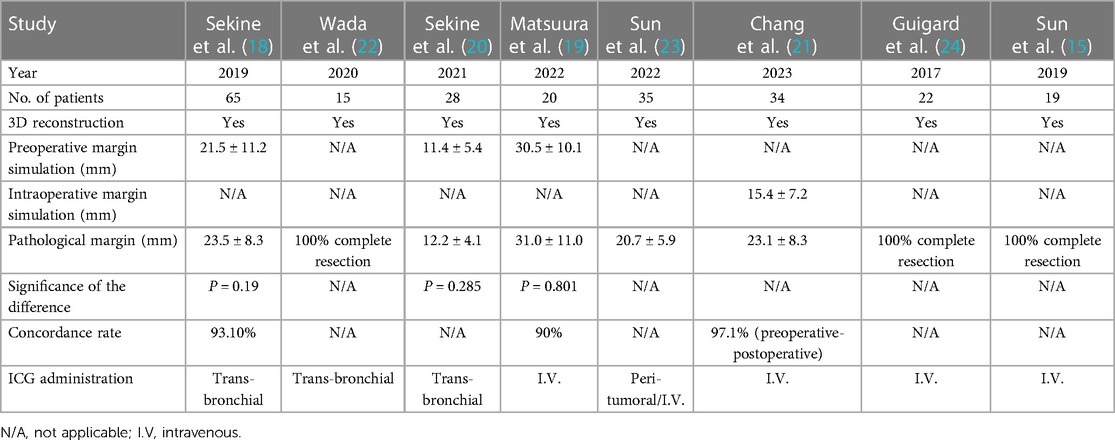
Table 1 Characteristics of the preoperative computed tomography reconstruction and simulation.
Wada et al. performed preoperative volume measurements during 3D CT reconstruction. The entire lung was scanned during a single breath hold at the end of inspiration. The volume of the ICG injected endobronchially was calculated after determining the volume of the target segment. The ICG volumes were then used during NIR-guided surgery; no adverse events were recorded (section 3.4). The volume of the ICG administered endobronchially was at least 0.04 of the target segment volume. Virtual bronchoscopy performed during reconstruction also supported the selection of bronchi for ICG administration in the segment of interest (22).
Invisible NIR fluorescence imaging has been used over the last two decades to assist with intraoperative findings. Since this technique does not require ionising radiation, it is safe (25). Further, because NIR light is invisible to the human eye, it does not affect the surgeon's vision. NIR fluorescence imaging systems are based on the detection of infrared light emitted by fluorescent dyes. A special camera is used for this purpose after the tissues are excited by a specific infrared light. All of these systems can be integrated into cameras used in open and mostly laparoscopic or robotic surgeries. NIR imaging systems offer several advantages. While visible light can penetrate only a few micrometres into tissues, NIR light (700–900 nm) can penetrate centimetres through different tissues (26).
Several NIR systems can detect infrared light. These systems are affordable and simple to use and can be used as alternatives to conventional, complicated, and expensive intraoperative imaging techniques. Fluorophores are required in addition to NIR light detectors. The most commonly used fluorophore is ICG, a water-soluble, amphiphilic tricarbocyanine fluorophore. It has a molecular weight of 775 D and it fluoresces and absorbs the NIR spectrum. ICG binds rapidly to plasma proteins and lipoproteins. It is secreted through the liver into bile in an unconjugated form, is not metabolized, and has a half-life of 120–240 s (27).
ICG is safe for systemic use up to a dose of 5 mg/kg. The excitation and emission wavelengths are approximately 805 and 830 nm, respectively. With an emission spectrum at 830 nm, the tissue penetration of ICG is up to 15 mm. Owing to its amphiphilic and protein-binding characteristics, it can migrate through lymphatic vessels. ICG is relatively inexpensive, nontoxic, and approved by the Food and Drug Administration. It is affordable, making it an optimal fluorophore for NIR-guided surgery. ICG has long been used in cardiac function tests, functional liver examinations, and ophthalmic angiography (28, 29).
However, ICG has some disadvantages, such as moderate photostability, a relatively narrow fluorescence quantum yield, high propensity for binding to plasma proteins, and aggregation in aqueous solutions (12). Some cases of anaphylaxis have also been reported during its use and it is not recommended for patients with iodine allergy or thyreotoxicosis (30, 31).
Pafolacianine, also known as OTL38, is a newly developed ICG-like folate analogue. Binding to the folate receptor alpha can be used to mark folate receptor-positive tumours. It is eliminated relatively quickly from receptor-negative tissues, with a half-life of <30 min (32, 33). NIR-guided lung surgery is suitable for localising lesions, considering that 85% of lung tumours express folate receptors (34, 35) that are unaffected by chemotherapy (36). Besides rapid plasma clearance, it also has several additional benefits, such as a long residence time in the tumour, which allows it to be administered on the day of surgery in cases of active tumour targeting. Furthermore, pafolacianine has a better penetration depth and signal-to-background ratio and was approved by the Food and Drug Administration in late 2022 (14, 36).
Delineation and division of the intersegmental planes are critical in segmentectomy. These steps ensure appropriate oncological radicality by securing the resection margins but can also lead to a decision to extend the resection if necessary. One method often used to determine the ISPs is the inflation-deflation technique or it's modification. This technique involves re-ventilating the lungs after clamping the target bronchus and this is performed as described below: After identification and ligation of the targeted segmental bronchus, artery and intrasegmental vein, the collapsed lung is fully re-expanded with controlled airway pressure below 20 cmH2O, opening the bronchus on the operated side to the atmosphere while continuing the ventilation of the contralateral lung. Five to twelve minutes later, a demarcation forms between the inflated target segment and adjacent deflated segments, representing the ISP (37). However, it is often inaccurate due to collateral ventilation and is difficult to use in patients with underlying lung diseases such as emphysema. In addition, during VATS, the surgeon's vision is disturbed by the inflated lungs. Selective ventilation of the target bronchus can also be performed, although it is a relatively complicated procedure (38).
In 2009, a new method was introduced to identify ISPs. In this method, an NIR thoracoscope is used after the intravenous administration of ICG (12, 39). Using the surface blood flow of the lung, the segments can be visualised after the bronchi, and the vessels of the targeted segment are clamped. This method is currently widely accepted (40).
Endobronchial administration is another option for the use of ICG. This is a relatively complex bronchoscopic procedure. These methods allow for the delineation of target segments based on the distribution of ICG in the lungs. These application methods have advantages and disadvantages, as explained below (13).
Many factors can influence the delineation of ISPs. Therefore, a delineation score is sometimes used to describe the degree of ISP identification. In general, the detectability of ISP is at least 90% with the use of ICG (18, 19).
Since 2009, when Misaki et al. reported the benefits of intravenously administered ICG during thoracoscopic surgery, this method has been widely used (39). In general, ICG is administered intravenously after the identification and division of the bronchi and vessels of the targeted segment or segments previously identified during 3D CT reconstruction and simulation. Staining usually takes 200–400 s after injection. Using an NIR thoracoscope, the visceral pleura shows fluorescence, except in the affected segment. This method is referred to as negative staining.
After 3D CT reconstruction and planning, Matsuura et al. used ICG at a dose of 0.3 mg/kg/10 ml administered at a rate of 300 ml/h. The demarcation was evaluated by two authors, and each intersegmental plane was scored as follows: clear visualisation without interruption (3 points, excellent), partially unclear visualisation but can be identified (2 points, fair), and difficult to identify (1 point, poor). The demarcation was marked with electrocautery and divided using staplers. In total, 92.2% of the 64 ISPs examined were visualised. All the tumours were completely removed. This method is now considered the standard for intravenously administered ICG (19), including the use of staplers for division of the parenchyma (41).
In several studies, 100% successful ISP delineation has been achieved with intravenous administration of ICG (15, 20, 23, 24), although the lack of emphysema may facilitate this success rate. In the study by Sun et al., the ISPs determined by ICG was fully consistent with those determined by the modified inflation-deflation method. At the same time, ICG application saves the waiting time required for the modified inflation-deflation method, and also avoids complications associated with the procedure, such as pressure trauma (15). Intravenous ICG may affect the extent of the resection. Thus the preoperatively planned anatomical resection can be modified during NIR angiography. Dividing the intersegmental planes determined by the vasculature would prevent retention of devascularized parenchyma. Adequate management of vascular variations detected in the background of inappropriate delineation, can avoid devitalisation of adjacent segments, or can ensure adequate resection margins by extending the resection if necessary. During surgery, we can freely choose pulmonary artery branches, which can be clamped to change the extent of the resection. Accordingly, we have the possibility to modify the resection margin during surgery if it is considered insufficient. In this way, oncological safety can be increased. The repeatability and quickness of intravenous administration is a real advantage in this case (19, 24). In the study by Guigard et al., the use of intravenously administered ICG changed the progress of segmentectomy in three of the 22 cases (24).
However, assessment of the ISPs delineated after ICG administration is not always straightforward and can be influenced by a number of factors. In approximately 10% or less of the cases, the ISPs cannot be visualised (39, 42). In patients with severe chronic obstructive pulmonary disease, emphysematous lungs, or anthracosis, the possibility of identifying the intersegmental line could be reduced (43). This implies that insufficient resection margins may be achieved during surgery under certain circumstances. Therefore, it is necessary for surgeons to confirm that the ISP to be drawn matches the actual anatomical or simulated line during preoperative planning. Intraoperative CT scanning and 3D reconstruction may be potential solutions to this problem. Chang et al. used this method. After intravenous ICG administration (5 mg/patient) followed by bronchovascular clamping and delineation, the intersegmental planes were marked with metal clips, and intraoperative cone beam CT 3D reconstruction was performed to verify the relationship between the ISP and the tumour. The intersegmental planes were well defined by ICG in 91.2% of the cases. The concordance between CT reconstructions was similarly high. This intervention provided confirmation to the surgeon or provoked extension of the surgery when needed. Intraoperative CT was performed under bilateral ventilation, and the median time required for intraoperative CT imaging was 10.5 min (21).
Marking methods are another option for intraoperatively identifying tumours and ensuring proper radical resection. CT-guided hook-wire markings (44), coil markings (45), transbronchial fiducial markers, and dye injections may all be suitable for this purpose (46).
Sun et al. used CT-guided percutaneous ICG injection paratumorally immediately before surgery to localise nodules intraoperatively. A 0.1 ml dose (2.5 mg/ml concentration) was injected into the medial border of the tumour. The average time to nodulus localisation was 15.48 ± 5.13 min. Otherwise, intravenous ICG was administered and negative staining was performed intraoperatively. As a result, dual visualisation was achieved, which allowed for real-time monitoring of the tumour-ISP relationship. This ensured an adequate resection margin. However, this method is not suitable for marking deep nodules owing to its NIR penetration abilities. It is an invasive procedure that must be closely synchronised with the timing of surgery (23). Further characteristics of the applications are shown in Table 2.
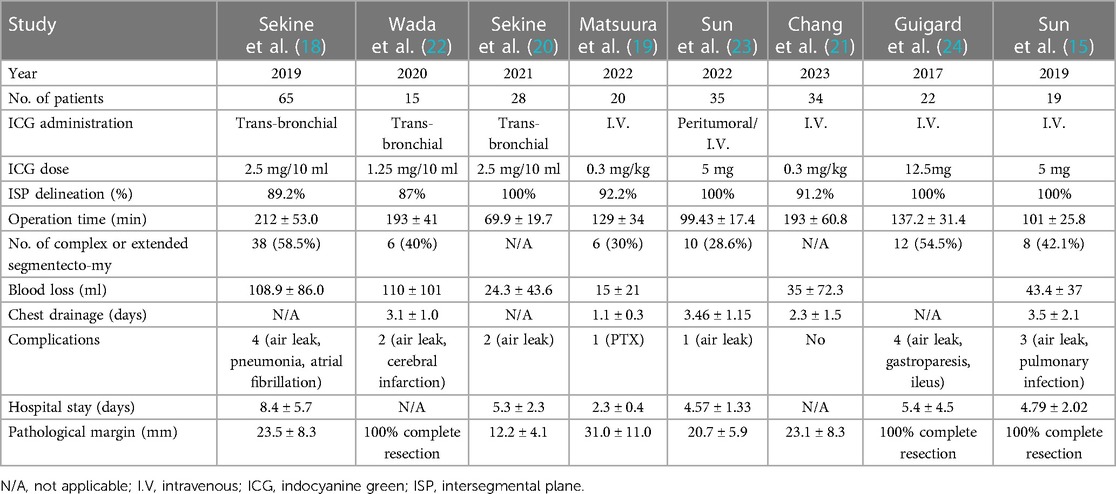
Table 2 Characteristics of ICG administration and postoperative outcomes.
ICG can also be used transbronchially to identify intersegmental planes. This technique is less common than intravenous application. Transbronchial injection of ICG can be performed intraoperatively following ligation of the segmental vessels and bronchi. This method was described by Oh et al., who used a generally open approach during video-assisted surgery. This manoeuvre allowed for the visualisation of the ISP; however, in contrast to intravenous application, it was not only delineated on the surface, but also deeply in the parenchyma. This is one advantage of the proposed method. However, this technique has not become popular because it requires the separation of hilar structures prior to administration and can be difficult to perform during thoracoscopic surgery (47).
Another common transbronchial method is bronchoscopic administration. This procedure is typically performed using an ultrathin bronchoscope. Thus, it is possible to administer the ICG to both the segmental and subsegmental bronchi. In all cases, precise 3D CT reconstruction and virtual bronchoscopy were used to simulate the planned resection. Reconstruction was performed up to 4th to 6th levels of the bronchi. This allowed for the accurate planning of bronchoscopic administration. In some cases, the volume of the lung segment was calculated to determine the amount of the ICG solution administered (22).
After the induction of general anaesthesia, bronchoscopy was performed through a single-lumen endotracheal tube or laryngeal mask. An ultrathin bronchoscope was used to identify the target bronchus or bronchi, followed by a bronchial catheter with a balloon to deliver the ICG solution and 50–400 ml of air into the segment. In this step, it is crucial to prevent ICG leakage as it can lead to false results if transferred to other bronchi. Positive end-expiratory pressure ventilation was initiated. As ICG binds rapidly to plasma proteins, it is dissolved in saline and autologous blood, and this solution is injected into the bronchi. On average, ICG administration took 5–22 min, and it took 15–30 min until the start of surgery (20, 22).
During VATS segmentectomy, an NIR thoracoscope was used to visualise the resection borders. The visceral pleura was marked with diathermy. The intersegmental planes were separated using electrocautery and/or a stapler. After the resection, an NIR thoracoscope was used to identify the residual tissues that should be resected. This is one of the advantages of this method because fluorescence can be observed deep in the parenchyma. The types of resection include subsegmental resection, simple segmentectomy, complex segmentectomy, and extended segmentectomy (18, 20, 22).
The concentration of the injected ICG solution was between 1.25 mg/10 ml and 2.5 mg/10 ml. The injected volume depended on the calculated segmental volume or 10 ml per subsegmental bronchi. The corresponding demarcation rate shown by ICG was 87%–100%. Sekine et al. used a four-degree scoring system to describe the degree of delineation. Complete resection was achieved in all cases, and no ICG-induced adverse reactions were reported (18, 20, 22).
Sekine et al. analysed the residual segmental structure 6 months later during a control CT scan and reconstruction and found 93.1% concordance with the preoperative simulation. Furthermore, a comparison with a traditional segmentectomy control group was performed to assess the efficacy of ICG. Complicated sublobar resection was performed more often in the ICG group (P < 0.0001) and the operative time was longer. However, after propensity score matching, the results were similar (18). Additional characteristics of the interventions are presented in Table 2.
Aside from ICG, other options are emerging for intraoperative imaging. In ELUCIDATE, a multicentre phase 3 trial, intravenous pafolacanine was used for active tumour targeting using IMI. Thus, it is possible to localise non-palpable tumours and detect additional lesions, metastases, and positive lymph nodes. As it is a preoperative intravenous injection, there is no need for the isolation of segmental structures prior to application or for complex additional procedures such as bronchoscopy. In the trial, after visualising the tumour using NIR imaging, it was possible to measure the resection margins in situ or on the back table. The IMI group comprised 100 patients. Overall, IMI with pafolacianine changed the scope of the surgical procedure in 29% of cases. A total of 65 clinically significant events occurred in 53 patients during the trial. Of these, 38 events affected the resection margins. This represents, that the most common clinically significant event was the identification of close margins. The sensitivity for detecting cancerous tissues was 76.9%. No serious adverse drug-related effects were reported (48).
NIR-guided surgery is a relatively new technique that has been rapidly adopted in the field of thoracic surgery. The most commonly used fluorophore is ICG (25, 28, 29). Achieving adequate resection margins is one of the most crucial factors in preventing local recurrence (2, 3); this can be facilitated by the combination of three-dimensional CT reconstruction and NIR-guided surgery. Reliable visualisation of the ISP is crucial for accurate single or complex segmentectomy. In this regard, there are two ways to use ICG: intravenous, and trans-, or endobronchially. The advantages of intravenous ICG include easy and quick application and repeatability. Thus, NIR angiography can be used to modify the extent of the resection during surgery (24). Therefore, it is widely accepted. The disadvantages include a relatively short duration of fluorescence and the need to separate the vessels and bronchi of the target segment prior to administration (19, 21, 24). Furthermore, underlying lung diseases (e.g., emphysema and chronic obstructive pulmonary disease) affect the applicability of intravenous ICG (43).
In contrast, after transbronchial administration of ICG, fluorescence can be observed for a long time and detected deep in the parenchyma. Complex sublobar resections are more feasible when using virtual bronchial maps. Delineation of the ISP can be observed at the beginning of surgery, and there is no need for dissection of segmental structures before surgery (20). Disadvantages include the complexity of bronchoscopic application, which requires advanced skills and must be synchronised with the timing of the surgery. Furthermore, the ICG solution that leaks during injection may provide a false result if it is transferred into the adjacent bronchi (22).
Our findings revealed that ISP identification has similar efficacy for both methods, and overall, there were no significant differences in the duration of surgery. Complete resection was achieved in all studies, independent of the ICG application method. Limitations of the studies included a limited number of cases and short follow-up period (19, 21). Sekine et al. noted that one patient died of multiple distant metastases one year after surgery. No local recurrences were reported (20). Transbronchial administration may be advantageous in the management of complex segmentectomies. However, intravenous administration is simple and widespread.
Overall, both methods (intravenosus and transbronchial administration) can help to ensure adequate resection margins for segmentectomy in patients with early stage NSCLC. However, owing to the emergence of new fluorophores, such as pafolacianine, for active tumour targeting and IMI, the localisation of lesions can be more easily performed to provide sufficient resection margins independent of ISP determination (48). However, this requires further investigation.
LL: Conceptualization, Data curation, Formal Analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. BP: Data curation, Writing – original draft. ES: Data curation, Writing – original draft. JL: Data curation, Writing – original draft. AB: Data curation, Writing – original draft. GL: Conceptualization, Writing – original draft. JF: Conceptualization, Formal Analysis, Methodology, Project administration, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We would like to thank Editage (www.editage.com) for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ICG, indocyanine green; IMI, intraoperative molecular imaging; ISP, intersegmental plane; NIR, near-infrared; NSCLC, non-small cell lung cancer; RATS, robot-assisted thoracic surgery; VATS, video-assisted thoracic surgery.
1. Wolf AS, Richards WG, Jaklitsch MT, Gill R, Chirieac LR, Colson YL, et al. Lobectomy versus sublobar resection for small (2 cm or less) non–small cell lung cancers. Ann Thorac Surg. (2011) 92:1819–23. discussion 1824. doi: 10.1016/j.athoracsur.2011.06.099
2. Saji H, Okada M, Tsuboi M, Nakajima R, Suzuki K, Aokage K, et al. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607l): a multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial. Lancet. (2022) 399:1607–17. doi: 10.1016/S0140-6736(21)02333-3
3. Altorki N, Wang X, Kozono D, Watt C, Landrenau R, Wigle D, et al. Lobar or sublobar resection for peripheral stage IA non-small-cell lung cancer. N Engl J Med. (2023) 388:489–98. doi: 10.1056/NEJMoa2212083
4. Fourdrain A, Anastay V, Pauly V, Braggio C, D’Journo XB, Boulate D, et al. Peripheral location of lung cancer is associated with higher local disease recurrence. Eur J Cardiothorac Surg. (2023) 63:ezad130. doi: 10.1093/ejcts/ezad130
5. De Koning HJ, Van Der Aalst CM, De Jong PA, Scholten ET, Nackaerts K, Heuvelmans MA, et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N Engl J Med. (2020) 382:503–13. doi: 10.1056/NEJMoa1911793
6. Lim E, Harris RA, McKeon HE, Batchelor TJ, Dunning J, Shackcloth M, et al. Impact of video-assisted thoracoscopic lobectomy versus open lobectomy for lung cancer on recovery assessed using self-reported physical function: violet RCT. Health Technol Assess. (2022) 26:1–162. doi: 10.3310/THBQ1793
7. Bendixen M, Jørgensen OD, Kronborg C, Andersen C, Licht PB. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol. (2016) 17:836–44. doi: 10.1016/S1470-2045(16)00173-X
8. Veronesi G, Abbas AES, Muriana P, Lembo R, Bottoni E, Perroni G, et al. Perioperative outcome of robotic approach versus manual videothoracoscopic major resection in patients affected by early lung cancer: results of a randomized multicentric study (ROMAN study). Front Oncol. (2021) 11:726408. doi: 10.3389/fonc.2021.726408
9. Bédat B, Abdelnour-Berchtold E, Perneger T, Licker MJ, Stefani A, Krull M, et al. Comparison of postoperative complications between segmentectomy and lobectomy by video-assisted thoracic surgery: a multicenter study. J Cardiothorac Surg. (2019) 14:189. doi: 10.1186/s13019-019-1021-9
10. Brunelli A, Decaluwe H, Gonzalez M, Gossot D, Petersen RH, Augustin F, et al. European Society of Thoracic Surgeons expert consensus recommendations on technical standards of segmentectomy for primary lung cancer. Eur J Cardiothorac Surg. (2023) 63:ezad224. doi: 10.1093/ejcts/ezad224
11. Kato H, Oizumi H, Suzuki J, Hamada A, Watarai H, Sadahiro M. Thoracoscopic anatomical lung segmentectomy using 3D computed tomography simulation without tumour markings for non-palpable and non-visualized small lung nodules. Interact Cardiovasc Thorac Surg. (2017) 25:434–41. doi: 10.1093/icvts/ivx113
12. Misaki N, Chang SS, Gotoh M, Yamamoto Y, Satoh K, Yokomise H. A novel method for determining adjacent lung segments with infrared thoracoscopy. J Thorac Cardiovasc Surg. (2009) 138:613–8. doi: 10.1016/j.jtcvs.2009.01.003
13. Sekine Y, Ko E, Oishi H, Miwa M. A simple and effective technique for identification of intersegmental planes by infrared thoracoscopy after transbronchial injection of indocyanine green. J Thorac Cardiovasc Surg. (2012) 143:1330–5. doi: 10.1016/j.jtcvs.2012.01.079
14. Wong LY, Lui NS. Intraoperative molecular imaging of lung cancer. Thorac Surg Clin. (2023) 33:227–32. doi: 10.1016/j.thorsurg.2023.04.013
15. Sun Y, Zhang Q, Wang Z, Shao F, Yang R. Is the near-infrared fluorescence imaging with intravenous indocyanine green method for identifying the intersegmental plane concordant with the modified inflation-deflation method in lung segmentectomy? Thorac Cancer. (2019) 10(10):2013–21. doi: 10.1111/1759-7714.13192
16. Ji Y, Zhang T, Yang L, Wang X, Qi L, Tan F, et al. The effectiveness of three-dimensional reconstruction in the localization of multiple nodules in lung specimens: a prospective cohort study. Transl Lung Cancer Res. (2021) 10:1474–83. doi: 10.21037/tlcr-21-202
17. Sawabata N, Ohta M, Matsumura A, Nakagawa K, Hirano H, Maeda H, et al. Optimal distance of malignant negative margin in excision of nonsmall cell lung cancer: a multicenter prospective study. Ann Thorac Surg. (2004) 77:415–20. doi: 10.1016/S0003-4975(03)01511-X
18. Sekine Y, Itoh T, Toyoda T, Kaiho T, Koh E, Kamata T, et al. Precise anatomical sublobar resection using a 3D medical image analyzer and fluorescence-guided surgery with transbronchial instillation of indocyanine green. Semin Thorac Cardiovasc Surg. (2019) 31:595–602. doi: 10.1053/j.semtcvs.2019.01.004
19. Matsuura N, Igai H, Ohsawa F, Numajiri K, Kamiyoshihara M. Novel thoracoscopic segmentectomy combining preoperative three-dimensional image simulation and intravenous administration of indocyanine green. Interact Cardiovasc Thorac Surg. (2022) 35:ivac064. doi: 10.1093/icvts/ivac064
20. Sekine Y, Koh E, Hoshino H. The efficacy of transbronchial indocyanine green instillation for fluorescent-guided wedge resection. Interact Cardiovasc Thorac Surg. (2021) 33:51–9. doi: 10.1093/icvts/ivab054
21. Chang SS, Yokomise H, Yokota N, Yoshida C, Katoh A, Misaki N, et al. Dual image navigation to secure surgical margins in thoracoscopic segmentectomy. Ann Surg Oncol. (2023) 30:843–9. doi: 10.1245/s10434-022-12615-9
22. Wada H, Yamamoto T, Morimoto J, Sakairi Y, Suzuki H, Nakajima T, et al. Near-infrared-guided pulmonary segmentectomy after endobronchial indocyanine green injection. Ann Thorac Surg. (2020) 109:396–403. doi: 10.1016/j.athoracsur.2019.08.083
23. Sun Y, Zhang Q, Wang Z, Shao F. Real-time image-guided indocyanine green fluorescence dual-visualization technique to measure the intraoperative resection margin during thoracoscopic segmentectomy. Asia Pac J Clin Oncol. (2023) 19:e39–44. doi: 10.1111/ajco.13771
24. Guigard S, Triponez F, Bédat B, Vidal-Fortuny J, Licker M, Karenovics W. Usefulness of near-infrared angiography for identifying the intersegmental plane and vascular supply during video-assisted thoracoscopic segmentectomy. Interact Cardiovasc Thorac Surg. (2017) 25(5):703–9. doi: 10.1093/icvts/ivx225
25. Schaafsma BE, Mieog JSD, Hutteman M, van der Vorst JR, Kuppen PJK, Löwik CWGM, et al. The clinical use of indocyanine green as a near-infrared fluorescent contrast agent for image-guided oncologic surgery. J Surg Oncol. (2011) 104:323–32. doi: 10.1002/jso.21943
26. Chance B. Near-infrared images using continuous, phase-modulated, and pulsed light with quantitation of blood and blood oxygenation. Ann N Y Acad Sci. (1998) 838:29–45. doi: 10.1111/j.1749-6632.1998.tb08185.x
27. Moody ED, Viskari PJ, Colyer CL. Non-covalent labeling of human serum albumin with indocyanine green: a study by capillary electrophoresis with diode laser-induced fluorescence detection. J Chromatogr B Biomed Sci Appl. (1999) 729:55–64. doi: 10.1016/s0378-4347(99)00121-8
28. Okusanya OT, Hess NR, Luketich JD, Sarkaria IS. Infrared intraoperative fluorescence imaging using indocyanine green in thoracic surgery. Eur J Cardiothorac Surg. (2018) 53:512–8. doi: 10.1093/ejcts/ezx352
29. De Grand AM, Lomnes SJ, Lee DS, Pietrzykowski M, Ohnishi S, Morgan TG, et al. Tissue-like phantoms for near-infrared fluorescence imaging system assessment and the training of surgeons. J Biomed Opt. (2006) 11:014007. doi: 10.1117/1.2170579
30. Luo S, Zhang E, Su Y, Cheng T, Shi C. A review of NIR dyes in cancer targeting and imaging. Biomaterials. (2011) 32:7127–38. doi: 10.1016/j.biomaterials.2011.06.024
31. Hope-Ross M, Yannuzzi LA, Gragoudas ES, Guyer DR, Slakter JS, Sorenson JA, et al. Adverse reactions due to indocyanine green. Ophthalmology. (1994) 101:529–33. doi: 10.1016/s0161-6420(94)31303-0
32. Mahalingam SM, Kularatne SA, Myers CH, Gagare P, Norshi M, Liu X, et al. Evaluation of novel tumor-targeted near-infrared probe for fluorescence-guided surgery of cancer. J Med Chem. (2018) 61:9637–46. doi: 10.1021/acs.jmedchem.8b01115
33. Shum CF, Bahler CD, Low PS, Ratliff TL, Kheyfets SV, Natarajan JP, et al. Novel use of folate-targeted intraoperative fluorescence, OTL38, in robot-assisted laparoscopic partial nephrectomy: report of the first three cases. J Endourol Case Rep. (2016) 2:189–97. doi: 10.1089/cren.2016.0104
34. Okusanya OT, Deshpande C, Barbosa EM, Aggarwal C, Simone CB, Jiang J, et al. Molecular imaging to identify tumor recurrence following chemoradiation in a hostile surgical environment. Mol Imaging. (2014) 13:1–6. doi: 10.2310/7290.2014.00051
35. Shen J, Putt KS, Visscher DW, Murphy L, Cohen C, Singhal S, et al. Assessment of folate receptor-β expression in human neoplastic tissues. Oncotarget. (2015) 6:14700–9. doi: 10.18632/oncotarget.3739
36. Kennedy GT, Azari FS, Chang A, Nadeem B, Bernstein E, Segil A, et al. Comparative experience of short-wavelength versus long-wavelength fluorophores for intraoperative molecular imaging of lung cancer. Ann Surg. (2022) 276:711–9. doi: 10.1097/SLA.0000000000005596
37. Wang J, Xu X, Wen W, Wu W, Zhu Q, Chen L. Modified method for distinguishing the intersegmental border for lung segmentectomy. Thorac Cancer. (2018) 9(2):330–3. doi: 10.1111/1759-7714.12540
38. Okada M, Mimura T, Ikegaki J, Katoh H, Itoh H, Tsubota N. A novel video-assisted anatomic segmentectomy technique: selective segmental inflation via bronchofiberoptic jet followed by cautery cutting. J Thorac Cardiovasc Surg. (2007) 133:753–8. doi: 10.1016/j.jtcvs.2006.11.005
39. Misaki N, Chang SS, Igai H, Tarumi S, Gotoh M, Yokomise H. New clinically applicable method for visualizing adjacent lung segments using an infrared thoracoscopy system. J Thorac Cardiovasc Surg. (2010) 140:752–6. doi: 10.1016/j.jtcvs.2010.07.020
40. Pardolesi A, Veronesi G, Solli P, Spaggiari L. Use of indocyanine green to facilitate intersegmental plane identification during robotic anatomic segmentectomy. J Thorac Cardiovasc Surg. (2014) 148:737–8. doi: 10.1016/j.jtcvs.2014.03.001
41. Miyasaka Y, Oh S, Takahashi N, Takamochi K, Suzuki K. Postoperative complications and respiratory function following segmentectomy of the lung – comparison of the methods of making an inter-segmental plane. Interact Cardiovasc Thorac Surg. (2011) 12:426–9. doi: 10.1510/icvts.2010.253989
42. Mehta K, Atak A, Sahu A, Srivastava S CMK. An early investigative serum Raman spectroscopy study of meningioma. Analyst. (2018) 143:1916–23. doi: 10.1039/c8an00224j
43. Iizuka S, Kuroda H, Yoshimura K, Dejima H, Seto K, Naomi A, et al. Predictors of indocyanine green visualization during fluorescence imaging for segmental plane formation in thoracoscopic anatomical segmentectomy. J Thorac Dis. (2016) 8:985–91. doi: 10.21037/jtd.2016.03.59
44. Ichinose J, Kohno T, Fujimori S, Harano T, Suzuki S. Efficacy and complications of computed tomography-guided hook wire localization. Ann Thorac Surg. (2013) 96:1203–8. doi: 10.1016/j.athoracsur.2013.05.026
45. Toba H, Kondo K, Miyoshi T, Kajiura K, Yoshida M, Kawakami Y, et al. Fluoroscopy-assisted thoracoscopic resection after computed tomography-guided bronchoscopic metallic coil marking for small peripheral pulmonary lesions. Eur J Cardiothorac Surg. (2013) 44:e126–32. doi: 10.1093/ejcts/ezt220
46. Sharma P. Value of liver function tests in cirrhosis. J Clin Exp Hepatol. (2022) 12:948–64. doi: 10.1016/j.jceh.2021.11.004
47. Oh S, Suzuki K, Miyasaka Y, Matsunaga T, Tsushima Y, Takamochi K. New technique for lung segmentectomy using indocyanine green injection. Ann Thorac Surg. (2013) 95:2188–90. doi: 10.1016/j.athoracsur.2012.12.068
Keywords: lung surgery, near-infrared fluorescence-guided surgery, indocyanine green, segmentectomy, VATS, resection margin, intersegmental plane
Citation: Libor László, Pécsy Balázs, Szűcs E, Lantos J, Bakos Annamária, Lázár György and Furák József (2024) Effect of transbronchial or intravenous administration of indocyanine green on resection margins during near-infrared-guided segmentectomy: a review. Front. Surg. 11:1430100. doi: 10.3389/fsurg.2024.1430100
Received: 9 May 2024; Accepted: 17 June 2024;
Published: 1 July 2024.
Edited by:
Luca Bertolaccini, European Institute of Oncology (IEO), ItalyReviewed by:
Michel Gonzalez, Centre Hospitalier Universitaire Vaudois (CHUV), Switzerland© 2024 Libor, Pécsy, Szűcs, Lantos, Bakos, Lázár and Furak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: László Libor, bGlib3JsYXN6QGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.