 Marco Battistelli
Marco Battistelli Manuela D’Ercole
Manuela D’Ercole Quintino Giorgio D’Alessandris
Quintino Giorgio D’Alessandris Nicola Montano
Nicola Montano
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Surg., 16 November 2023
Sec. Neurosurgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1310414
This article is part of the Research TopicFunctional Approach To Neurosurgery: Current Research and Future PerspectivesView all 8 articles
Trigeminal neuralgia (TN) is the most frequent facial pain. It is difficult to treat pharmacologically and a significant amount of patients can become drug-resistant requiring surgical intervention. From an etiologically point of view TN can be distinguished in a classic form, usually due to a neurovascular conflict, a secondary form (for example related to multiple sclerosis or a cerebello-pontine angle tumor) and an idiopathic form in which no anatomical cause is identifiable. Despite numerous efforts to treat TN, many patients experience recurrence after multiple operations. This fact reflects our incomplete understanding of TN pathogenesis. Artificial intelligence (AI) uses computer technology to develop systems for extension of human intelligence. In the last few years, it has been a widespread of AI in different areas of medicine to implement diagnostic accuracy, treatment selection and even drug production. The aim of this mini-review is to provide an up to date of the state-of-art of AI applications in TN diagnosis and management.
Trigeminal neuralgia (TN) is a form of neuropathic facial pain which significantly impacts quality-of-life of affected patients (1). Typical TN presents as relapse-remitting pain, whereas in atypical TN a continuous component of pain is present (2). Etiologically, it can be divided in primary and secondary TN, the latter one due to cerebellopontine-angle tumors or multiple sclerosis. Primary TN is further divided in classic, due to a neurovascular conflict (NVC), and idiopathic, where a clear anatomical cause is missing. In a recent umbrella review microvascular decompression (MVD) emerged as the most effective treatment for classic TN (3). Even if there are continuous innovations in the field of TN, such as the understanding of the role of some biomarkers (4) and the use of morphometric magnetic resonance imaging (MRI) (5), it is not always easy to determine the etiology, and consequentially the appropriate treatment, in each patient. Artificial intelligence (AI) uses computer technology to develop systems for extension of human intelligence. It is emerging as a increasingly widespread tool in medicine to implement diagnostic accuracy, treatment selection and even drug production (6). The aim of this mini-review is to provide an up to date of the state-of-art of AI applications in TN management.
Two medical databases (PubMed and Scopus) were screened for eligible scientific reports. The key words “deep learning”, “machine learning”, “artificial intelligence”, “trigeminal neuralgia”, “tic douloureux” (MeSH) have been used in any possible combination. The last search was launched in August 2023. Two reviewers (M.B., A.I.) independently screened the abstracts and the references list. Any difference was solved by consensus with a third senior author (N.M.) A total of 26 articles were identified and reviewed and finally, 17 studies were included in the present mini-review (Figure 1).
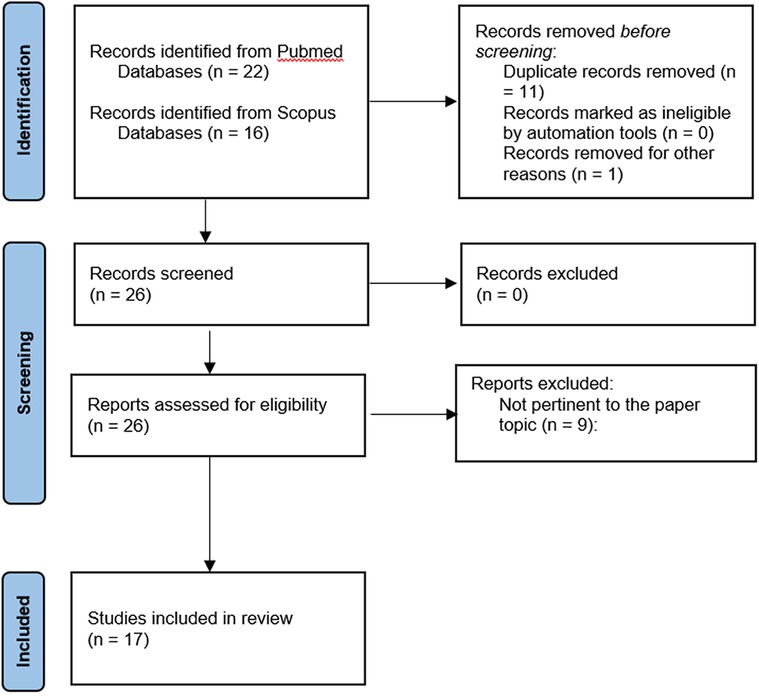
Figure 1. Flowchart of study selection.
AI has become increasingly involved in various aspects of TN diagnosis. It plays a pivotal role in identifying signature patterns within the cortical and subcortical regions, delineating the surgical anatomy of the cerebello-pontine angle, and distinguishing different types of facial pain. Liang et al. explored the capabilities of correlation and machine learning (ML) analysis methods in detecting activated cortical centers in TN patients. Interestingly, they found that certain cortical areas were only activated by conventional correlation methods, while others were detected by convolutional neural networks (CNN) and graph convolutional neural networks (GCNN). Their suggestion to combine these methods aims to achieve a more comprehensive understanding of the neural structures underlying TN pain perception (7). Zhong et al. utilized ML for the automated segmentation of white matter connectivity, comparing it with conventional analysis methods to identify alterations that could distinguish TN from healthy control subjects. Achieving a 0.96 AUC, they concluded that ML exhibits high reliability in discerning connectivity patterns between affected and non-affected groups (8). Mo et al. constructed a support vector machine (SVM) model based on T1-weighted and T2-weighted MRI data regarding cortical and subcortical morphological characteristics to diagnose TN patients. This model displayed high specificity, effectively distinguishing healthy patients from those afflicted by TN (9). Chen et al. used ML to analyze white matter fractional anisotropy differences between the affected and unaffected sides and healthy controls in both the trigeminalpontothalamic (TPT) and thalamocortical white matter (S1), achieving an 85% accuracy for TPT and 76% for S1 (10). Ge et al. used ML to extract V nerve radiomic features from 89 patients with unilateral idiopathic TN (UC-ITN), 55 of whom had NVC on the unaffected side. Small Area Low Gray Level Emphasis (SALGLE), Coarsenss, Minor Axis Length (MAL) Dependence Variance (DV), Maximum MALDV, Correlation and Offending Vessel were identified as texture features relevant to pain occurrence (11). AI also proves valuable in differentiating between various facial pain syndromes through radiographic and clinical questionnaires. Latypov et al. demonstrated 95% prediction accuracy using Random Forest (RF) supervised learning to distinguish classic TN from healthy controls based on T1-weighted and DTI MRI features. However, when attempting to differentiate between classic TN and trigeminal neuropathic pain (TNP), the accuracy dropped to 51% (12). Limonadi et al., as early as 2006, trained an Artificial Neural Network (ANN) to recognize facial pain syndrome patterns based on an 18-binomial response questionnaire. While high accuracy was achieved for classic TN assessment, the sensitivity was 50% for atypical TN and 33% for TNP (13). In a more recent study, McCartney et al. developed an ANN model based on a 22-question binomial questionnaire for distinguishing facial pain syndromes. This approach yielded high sensitivity and specificity for classic TN (92.5% and 87.8%, respectively). Remarkably, unlike Limonadi et al., they achieved high sensitivity and specificity for TNP (86.7% and 95.2%, respectively) (14). AI is also finding utility in examining peripheral V nerve characteristics. Mulford et al. employed a deep learning network to segment and extract radiomic features from the pre-ganglionic V nerve to distinguish affected from non-affected sides. Their method achieved an accuracy of 78%, specificity of 76%, sensitivity of 82%, and an AUC of 0.83, enabling reliable differentiation of TN-afflicted and pain-free nerves (15). Additionally, Lin et al. utilized an AI network to develop a V nerve and surrounding vascular structures segmentation network, aiding surgeons in planning surgery by creating a 3D model based on Magnetic Resonance Angiography (MRA). Their segmentation approach exhibited higher accuracy for V nerve segmentation (Dice similarity coefficient 0.8645, Hausdorff distance 0.2414, and average surface distance error 0.4296) compared to cerebrovascular structures segmentation (16).
In contrast to Lin et al., Bai et al. introduced MVDNet, a deep learning network focused on real-time blood vessel and cranial nerve segmentation during MVD procedures for facial and trigeminal nerve disorders. MVDNet achieved impressive precision, with a 76.59% Intersection-over-Union (mIoU) accuracy and a rapid 137.6 fps speed, surpassing other real-time models (17). AI has brought about predictive models for postoperative outcomes. Hao et al. developed an ANN which forecasted long-term Barrow Neurological Institute (BNI) Scores after MVD with an accuracy rate of 95.2% and area under the curve of 0.862 (18). Goyal et al. evaluated an ANN model, trained on 16 variables, to predict post-operative outcomes following Gamma Knife Radiosurgery (GKRS). The ANN exhibited 90.9% accuracy in predicting treatment responses (19). Ertiaei et al. created a multidimensional ANN model for post-GKRS predictions, including pain reduction and hypoesthesia, achieving accuracy rates of 91.5% and 76.8%, respectively (20). Hung et al. used SVM and sequential backward selection (SBS) models with MRI data on cortical thickness and regional surface area. These models showed predictive capabilities for one-year GKRS responses, with regional surface area at 96.7% accuracy and regional cortical thickness at 90.5% accuracy (21). The same team used Gaussian Process Regression (GPR) on T1-weighted MRI data to assess brain-predicted age (Brain-AGE) differences between TN patients and healthy controls, finding a significant correlation with radiosurgery response (21). Willsey et al. employed an SVM model to predict TN recurrence post-MVD surgery, considering factors like normalized radial diffusivity (PRD) and symptom duration. The SVM model reached an 85% accuracy, 83% sensitivity, and 86% specificity (22).
TN affects about 15,000 people per year in the US (23). Classic TN is the most common type with with MVD as a specific etiological treatment (24). NVC identification is crucial for surgical success, but it's not always evident pre-surgery. A recent study by Jani et al. identified neurovascular compression in 18 out of 27 patients on T2-weighted FIESTA thin-cut sequence performed with a 3 T scanner (25). However, Deep et al. reported up to 53% NCV in asymptomatic patients using high-resolution MRI on 200 examined nerves (26). Different pathophysiological theories such as bioresonance hypothesis and ignition hypothesis have been developed to explain the TN pathogenesis (27). Given the crucial role of identifying NVC before MVD procedures, Lin et al. introduced trigeminal nerve segmentation method from MRA based on 3D convolutional neural network using CS2Net for tubular structure segmentation (23). The proposed method outperformed other models in segmenting the trigeminal nerve and surrounding vascular structures near the REZ, enabling accurate NVC identification, severity assessment, and surgical simulation. This is enhanced by 3D rendering, enabling direct visualization of NVC from various perspectives and zoom levels. With advancements in neuronavigation reducing bone flaps during MVD (28), AI intraoperative segmentation protocols, like Bai et al. innovative encoder-decoder structure, become invaluable for identifying vessels and nerves in tight surgical spaces (17). It is worth noting the protocol's impressive speed and accuracy, providing real-time assistance to surgeons during procedures. This was made possible by an extensive dataset comprising 3,087 MVD images labeled by experts, with 1,806 used for training. However, it is important to note that the protocol's accuracy decreased notably when applied to elderly patients (age 40–50 PICA mIoU: 74.08% vs. age 60–70: 70.33%; age 40–50 AICA mIoU: 71.43% vs. age 60–70: 68.43%), likely due to a tortuous anatomy of intracranial vessels. Limonadi et al. and McCartney et al., despite focusing on different aspects of TN management, also observed reduced accuracy in their ANN predictive models when assessing rarer pathologies [sensitivity for TN type 2 and TNP was 50% and 33%, respectively (13); sensitivity for TN type 2 and TDP was 62.5% and 0%, respectively (14)]. These reports raise concerns about AI's precision with non-linear and limited datasets, emphasizing its limited ability to draw reliable conclusions. Limonadi et al. observed improved diagnostic performance in the second set of patients, as evidenced by decreasing mean square errors during network simulations, highlighting the importance of robust training and ample data for AI model effectiveness. However, sensitivity in TN type 2 diagnosis remained unsatisfactory in the second set. The Authors attributed this to initial symptom onset resembling TN type 1, evolving into the continuous pain typical of TN type 2. This underscores the importance of initial input from experienced clinicians to determine essential diagnostic variables, as also emphasized by Mulford et al. (10) and Chen et al. (15). While ML accuracy improves with repeated calculations, manual data input can introduce bias into dataset analyses. AI can be valuable in preoperative outcome assessment and patient selection. Hao et al. identified four factors affecting ANN model performance in long-term MVD prognostication: correspondence of the neurovascular offending site with facial pain region, immediate postoperative pain remission, degree of nerve compression by culprit vessels, and culprit vessel type, while age seems to not affect long-term outcome. Recent meta-analyses highlighted predictors like isolated venous conflict (p < 0.01), absence of immediate postoperative pain remission (29), arterial conflict (p < 0.01) (30), symptom duration less than 5 years, SCA involvement, and paroxysmal pain (31). A prospective non-randomized trial documented severity of NVC (grade 2–3) as a positive predictor (p = 0.003) (32) and a retrospective study documented the non-inferiority of MVD in elderly people (33). Regarding GKRS long-term outcome prediction, ANN models and conventional analyses evaluated similar factors, including prior treatment, involved dermatomes, post-GKRS numbness, pain type, radiosurgery dosage, and age (19, 20, 34, 35). In summary, AI's contribution is not significantly superior to conventional statistical analyses. However, its primary advantage in routine clinical use lies in enhancing accuracy and providing real-time assistance during outpatient assessments, compensating for the limitations of empirical judgment derived from traditional statistical analyses. AI's role in TN management extends to research. Ge et al. found that 61.80% of patients analyzed had NVC on the unaffected V nerve, highlighting predictive radiomics features for symptomatic TN (11). Chen et al. observed bilateral radial diffusivity changes, even on the unaffected side of unilateral TN, differing from healthy controls (10). Microscopic degeneration in TN patients may affect not only the affected nerve but also the contralateral side, potentially contributing to chronic pain and warranting further research. While AI exhibits remarkable performance in aiding clinical practice, its seamless integration poses significant challenges. Ethical concerns, encompassing data privacy, informed consent, and patient autonomy, must be addressed. Despite its potential drawbacks, AI is an integral part of modern healthcare. Collaborative efforts between governments and clinicians are essential to establish robust regulations. In conclusion, this review highlights AI's diverse applications in TN management, showcasing its pivotal role in precise diagnosis, individualized treatment, and advancing our understanding of the condition's pathophysiology. The future holds promise for AI-driven research and enhanced patient care.
MB: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. AI: Data curation, Investigation, Methodology, Validation, Writing – original draft. MD: Data curation, Methodology, Validation, Visualization, Writing – original draft. QD: Supervision, Validation, Visualization, Writing – review & editing. NM: Conceptualization, Data curation, Supervision, Writing – original draft, Writing – review & editing.
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rapisarda A, Baroni S, Gentili V, Moretti G, Burattini B, Sarlo F, et al. The role of biomarkers in drug-resistant trigeminal neuralgia: a prospective study in patients submitted to surgical treatment. Neurol Sci. (2022) 43:4425–30. doi: 10.1007/s10072-022-05971-7
2. Cruccu G, Gronseth G, Alksne J, Argoff C, Brainin M, Burchiel K, et al. AAN-EFNS guidelines on trigeminal neuralgia management: trigeminal neuralgia management. Eur J Neurol. (2008) 15:1013–28. doi: 10.1111/j.1468-1331.2008.02185.x
3. Rapisarda A, Battistelli M, Izzo A, D’Ercole M, D’Alessandris QG, Polli FM, et al. Outcome comparison of drug-resistant trigeminal neuralgia surgical treatments—an umbrella review of meta-analyses and systematic reviews. Brain Sci. (2023) 13:530. doi: 10.3390/brainsci13040530
4. Baroni S, Rapisarda A, Gentili V, Burattini B, Moretti G, Sarlo F, et al. CSF neuron-specific enolase as a biomarker of neurovascular conflict severity in drug-resistant trigeminal neuralgia: a prospective study in patients submitted to microvascular decompression. Neurol Sci. (2023) 44:1319–25. doi: 10.1007/s10072-022-06573-z
5. Montano N, Gaudino S, Giordano C, Pignotti F, Ioannoni E, Rapisarda A, et al. Possible prognostic role of magnetic resonance imaging findings in patients with trigeminal neuralgia and multiple sclerosis who underwent percutaneous balloon compression: report of our series and literature review. World Neurosurg. (2019) 125:e575–81. doi: 10.1016/j.wneu.2019.01.134
6. Liu P-R, Lu L, Zhang J-Y, Huo T-T, Liu S-X, Ye Z-W. Application of artificial intelligence in medicine: an overview. Curr Med Sci. (2021) 41:1105–15. doi: 10.1007/s11596-021-2474-3
7. Liang Y, Zhao Q, Hu Z, Bo K, Meyyappan S, Neubert JK, et al. Imaging the neural substrate of trigeminal neuralgia pain using deep learning. Front Hum Neurosci. (2023) 17:1144159. doi: 10.3389/fnhum.2023.1144159
8. Zhong J, Chen DQ, Hung PSP, Hayes DJ, Liang KE, Davis KD, et al. Multivariate pattern classification of brain white matter connectivity predicts classic trigeminal neuralgia. Pain. (2018) 159:2076–87. doi: 10.1097/j.pain.0000000000001312
9. Mo J, Zhang J, Hu W, Luo F, Zhang K. Whole-brain morphological alterations associated with trigeminal neuralgia. J Headache Pain. (2021) 22:95. doi: 10.1186/s10194-021-01308-5
10. Chen DQ, Zhong J, Chu PPW, Fei Li CM, Hodaie M. Trigeminal neuralgia diffusivities using gaussian process classification and merged group tractography. Pain. (2021) 162:361–71. doi: 10.1097/j.pain.0000000000002023
11. Ge X, Wang L, Pan L, Ye H, Zhu X, Feng Q, et al. Risk factors for unilateral trigeminal neuralgia based on machine learning. Front Neurol. (2022) 13:862973. doi: 10.3389/fneur.2022.862973
12. Latypov TH, So MC, Hung PSP, Tsai P, Walker MR, Tohyama S, et al. Brain imaging signatures of neuropathic facial pain derived by artificial intelligence. Sci Rep. (2023) 13:10699. doi: 10.1038/s41598-023-37034-y
13. Limonadi FM, McCartney S, Burchiel KJ. Design of an artificial neural network for diagnosis of facial pain syndromes. Stereotact Funct Neurosurg. (2006) 84:212–20. doi: 10.1159/000095167
14. McCartney S, Weltin M, Burchiel KJ. Use of an artificial neural network for diagnosis of facial pain syndromes: an update. Stereotact Funct Neurosurg. (2014) 92:44–52. doi: 10.1159/000353188
15. Mulford KL, Moen SL, Grande AW, Nixdorf DR, Van De Moortele PF. Identifying symptomatic trigeminal nerves from MRI in a cohort of trigeminal neuralgia patients using radiomics. Neuroradiology. (2022) 64:603–9. doi: 10.1007/s00234-022-02900-5
16. Lin J, Mou L, Yan Q, Ma S, Yue X, Zhou S, et al. Automated segmentation of trigeminal nerve and cerebrovasculature in MR-angiography images by deep learning. Front Neurosci. (2021) 15:744967. doi: 10.3389/fnins.2021.744967
17. Bai R, Liu X, Jiang S, Sun H. Deep learning based real-time semantic segmentation of cerebral vessels and cranial nerves in microvascular decompression scenes. Cells. (2022) 11:1830. doi: 10.3390/cells11111830
18. Hao W, Cong C, Yuanfeng D, Ding W, Li J, Yongfeng S, et al. Multidata analysis based on an artificial neural network model for long-term pain outcome and key predictors of microvascular decompression in trigeminal neuralgia. World Neurosurg. (2022) 164:e271–9. doi: 10.1016/j.wneu.2022.04.089
19. Goyal S, Kedia S, Kumar R, Bisht RK, Agarwal D, Singh M, et al. Role of gamma knife radiosurgery in trigeminal neuralgia—its long term outcome and prediction using artificial neural network model. J Clin Neurosci. (2021) 92:61–6. doi: 10.1016/j.jocn.2021.07.017
20. Ertiaei A, Ataeinezhad Z, Bitaraf M, Sheikhrezaei A, Saberi H. Application of an artificial neural network model for early outcome prediction of gamma knife radiosurgery in patients with trigeminal neuralgia and determining the relative importance of risk factors. Clin Neurol Neurosurg. (2019) 179:47–52. doi: 10.1016/j.clineuro.2018.11.007
21. Hung PSP, Noorani A, Zhang JY, Tohyama S, Laperriere N, Davis KD, et al. Regional brain morphology predicts pain relief in trigeminal neuralgia. NeuroImage: Clinical. (2021) 31:102706. doi: 10.1016/j.nicl.2021.102706
22. Willsey MS, Mossner JM, Chestek CA, Sagher O, Patil PG. Classifier using pontine radial diffusivity and symptom duration accurately predicts recurrence of trigeminal neuralgia after microvascular decompression: a pilot study and algorithm description. Neurosurg. (2021) 89:777–83. doi: 10.1093/neuros/nyab292
23. Araya EI, Claudino RF, Piovesan EJ, Chichorro JG. Trigeminal neuralgia: basic and clinical aspects. CN. (2020) 18(2):109–19. doi: 10.2174/1570159X17666191010094350
24. Jannetta PJ. Arterial compression of the trigeminal nerve at the pons in patients with trigeminal neuralgia. J Neurosurg. (1967) 26(1part2):159–62. doi: 10.3171/jns.1967.26.1part2.0159
25. Jani RH, Hughes MA, Gold MS, Branstetter BF, Ligus ZE, Sekula RF. Trigeminal nerve compression without trigeminal neuralgia: intraoperative vs imaging evidence. Neurosurgery. (2019) 84:60–5. doi: 10.1093/neuros/nyx636
26. Deep N, Fletcher G, Nelson K, Patel A, Barrs D, Bendok B, et al. Magnetic resonance imaging assessment of vascular contact of the facial nerve in the asymptomatic patient. J Neurol Surg B. (2016) 77(06):503–9. doi: 10.1055/s-0036-1584196
27. Montano N, Conforti G, Di Bonaventura R, Meglio M, Fernandez E, Papacci F. Advances in diagnosis and treatment of trigeminal neuralgia. TCRM. (2015) 11:289–99. doi: 10.2147/TCRM.S37592
28. Legninda Sop FY, D’Ercole M, Izzo A, Rapisarda A, Ioannoni E, Caricato A, et al. The impact of neuronavigation on the surgical outcome of microvascular decompression for trigeminal neuralgia. World Neurosurg. (2021) 149:80–5. doi: 10.1016/j.wneu.2021.02.063
29. Sarsam Z, Garcia-Fiñana M, Nurmikko TJ, Varma TRK, Eldridge P. The long-term outcome of microvascular decompression for trigeminal neuralgia. Br J Neurosurg. (2010) 24:18–25. doi: 10.3109/02688690903370289
30. Di Carlo DT, Benedetto N, Perrini P. Clinical outcome after microvascular decompression for trigeminal neuralgia: a systematic review and meta-analysis. Neurosurg Rev. (2022) 46:8. doi: 10.1007/s10143-022-01922-0
31. Holste K, Chan AY, Rolston JD, Englot DJ. Pain outcomes following microvascular decompression for drug-resistant trigeminal neuralgia: a systematic review and meta-analysis. Neurosurg. (2020) 86:182–90. doi: 10.1093/neuros/nyz075
32. Loayza R, Wikström J, Grabowska A, Semnic R, Ericson H, Abu Hamdeh S. Outcome after microvascular decompression for trigeminal neuralgia in a single center-relation to sex and severity of neurovascular conflict. Acta Neurochir (Wien). (2023) 165:1955–62. doi: 10.1007/s00701-023-05642-2
33. Menna G, Rapisarda A, Izzo A, D’Ercole M, D’Alessandris QG, Olivi A, et al. Surgical and clinical outcomes of microvascular decompression: a comparative study between young and elderly patients. Brain Sci. (2022) 12:1216. doi: 10.3390/brainsci12091216
34. Shaya M, Jawahar A, Caldito G, Sin A, Willis BK, Nanda A. Gamma knife radiosurgery for trigeminal neuralgia: a study of predictors of success, efficacy, safety, and outcome at LSUHSC. Surg Neurol. (2004) 61:529–34; discussion 534–5. doi: 10.1016/j.surneu.2003.11.027
Keywords: trigeminal neuralgia, neurovascular conflict, neuroanatomy, microvascular decompression, artificial intelligence, magnetic resonance imaging
Citation: Battistelli M, Izzo A, D’Ercole M, D’Alessandris QG and Montano N (2023) The role of artificial intelligence in the management of trigeminal neuralgia. Front. Surg. 10:1310414. doi: 10.3389/fsurg.2023.1310414
Received: 9 October 2023; Accepted: 1 November 2023;
Published: 16 November 2023.
Edited by:
Gianluca Trevisi, G d'Annunzio University, ItalyReviewed by:
Artur Xhumari, University of Medicine, Albania© 2023 Battistelli, Izzo, D’Ercole, D'Alessandris and Montano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicola Montano bmljb2xhbW9udGFub21kQHlhaG9vLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.