 Zhenya Zou
Zhenya Zou Shijiao Lv2
Shijiao Lv2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 04 January 2024
Sec. Visceral Surgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1308181
This article is part of the Research Topic Innovation in Surgery and Surgical Education View all 11 articles
Aim: To compile the awareness and implementation status of patients with intraoperative acquired pressure injuries prevention by operating room nurses and to test its reliability and validity.
Design: This is an equipment development research based on recommendations for developing a reliable and valid questionnaire.
Methods: The research was carried out in two phases from February to November 2022. Through a panel discussion, expert consultation, and literature review, the questionnaire for operating room nurses on the current status of awareness and implementation of the prevention of intraoperative acquired pressure injuries was preliminarily formulated. The formal questionnaire was developed through validity analysis, reliability analysis and item analysis, and reliability and validity tests were conducted. Moreover, according to the questionnaire survey results, confirmatory factor analysis was carried out to construct the structural equation model.
Results: The initial questionnaire consisted of five dimensions with 48 items, which was finalized to five dimensions with 38 items after reliability and validity testing and analysis. The five dimensions included implementation of intraoperative acquired pressure injuries prevention, intraoperative acquired pressure injuries preventing cognitive conditions, preoperative intraoperative acquired pressure injuries preventing cognitive conditions, basic knowledge of pressure injuries, and implementation of intraoperative acquired pressure injuries prevention in special patients. Cronbach's α of the overall questionnaire was 0.969 while that of each dimension was 0.846–0.959. The KMO value of structural validity was 0.945 (P < 0.001), and the contribution rate of cumulative variance was 70.694%. The fitting of confirmatory factor analysis was found to be generally ideal: χ2/df = 2.382, RMR = 0.027, TLI = 0.894, RMSEA = 0.072, IFI = 0.905, CFI = 0.904.
Conclusions: The study and design of the questionnaire for operating room nurses on the current status of awareness and implementation of the prevention of intraoperative acquired pressure injuries are scientific and rational, providing a scientific basis for the standardized reform of hospitals and the optimization of the intraoperative acquired pressure injuries management system of the operating room.
The prevention of intraoperative acquired pressure injuries (IAPI) is an important part of operating room care, which is also a global health issue of great concern. Several objective factors, such as the position during operation, the methods of anesthesia; and patient factors, such as individual tolerance capacity (1). It may cause a range of psychological problems and prolonged hospitalization (2, 3). In addition, it will increase the cost burden of patients and healthcare systems to some extent (4). Combine risk assessment prevention and prevention strategies to increase the nurses' awareness of pressure injuries (PI), thereby reducing the incidence of PI (5). This study intended to design a questionnaire for nurses in the operating room on the cognitive and operational status of IAPI, investigate the current status of IAPI prevention, and provide specific assessment tools for further optimizing prevention and management.
IAPI often occurs within 48 to 72 h after operation, which is characterized by acupressure pale erythema, purple skin, and blistering (6). Factors such as intraoperative hypothermia and long surgical immobilization time increase the incidence of IAPI. Studies have shown that most patients with PI of varying degrees will occur after the operation time is greater than 4 h, and the risk of PI increases by 33% for every 0.5 h increase (7).
The first staging system was recognized by Shea in 1975. Subsequently, in 1991, the International Association of Enterostomal Therapists (IAET) simplified and refined the system of Shea (8), however, PI is divided into four stages as before: ruddy bruising, inflammatory infiltrates, superficial ulcers, and deep ulcers. In addition, the National Pressure Ulcer Advisory Panel (NPUAP) staging system is the most widely used staging scale for PI, which was last revised in 2016 (9). Depending on the current understanding of the etiology of PI and the recent release of ICD-11 by the World Health Organization (WHO) in 2018, PI is classified into six stages in NPUAP: nonblanchable erythema of intact skin, partial skin defects with the exposed dermis, full skin defects, full skin, and tissue defects, obscured full skin and tissue defects and persistent nonblanchable erythema of deep tissue (10).
At present, the most widely used pressure injury risk assessment scales include the Braden scale, the Norton scale, and the Waterlow scale. Although these scales have a good effect on the application process, there are also some disadvantages. The Braden scale is currently the most widely used pressure injury risk assessment scale in the world, and although it is good for predicting pressure injury, it is not suitable for surgical patients (11). In contrast, the Norton scale and the Waterlow scale are more suitable for use in the operating room, and the Waterlow scale is more comprehensive and requires higher expertise from the evaluator (12). Moreover, the CORN-IAPI scale evaluates surgical patients from three aspects: preoperative, intraoperative and postoperative, including 2 dimensions and 10 factors, which are defined by anesthesia risk classification, body mass index (BMI), skin condition of the pressure site, preoperative limb activity, planned operation time, high-risk diseases, factors of body temperature loss, brought in PI, surgical blood loss, pressure shear force change, actual operation time, and postoperative skin results, and the scale is being promoted for use in China and has been shown to be effective in the prevention of IAPI (13).
With the improvement of measures to prevent IAPI, it is significant to discuss the understanding and implementation of operating room nurses on the prevention of IAPI in patients. A review of the literature revealed that most of the current studies have focused mainly on IAPI preventive measures or IAPI treatment strategies, ignoring the importance of the operating room nurse in the process of preventing or treating IAPI (14). Although some studies have investigated the awareness of IAPI among OR nurses, there is no specific research instrument to measure it (15). Scholars have developed IAPI-related test papers to determine OR nurses' IAPI knowledge through the scores of the test paper, which is very limited. Firstly, the content of the test papers produced by different scholars is not the same, and the test papers have not been developed through scientific and standardized methods, which lacks reliability and validity. On the other hand, there is a lack of specific tools to measure the current status of IAPI implementation among OR nurses.
The aim of this study was to develop a questionnaire for operating room nurses on the current status of awareness and implementation of the prevention of IAPI. Moreover, it provides a reference for further improving the preventive measures of IAPI.
This was a methodological study of scales conducted in a multi-centre (China) between February and November 2022. The study was conducted in two phases, the first involving the design and commissioning of the questionnaire, and the second phase including a formal validation process.
In both phases, the subjects involved a sample of 530 operating room nurses from three 3-A-class hospitals in Shandong Province, which are regional hospitals that can provide high-level specialized medical and health services and perform higher education and scientific research tasks. Inclusion criteria were as follows: ① have a nurse qualification certificate; ② voluntary participation in this study; ③ professional nursing in the operating room. Exclusion criteria were as follows: ① unable to attend on time due to further education or vacation.
The principle of determining the sample size of this study was as follows: the number of nurses included is 5–10 times the number of survey items and the sample number is ≥100 cases; The sample size taken by the structural equation model is at least 200 cases, and for each additional variable, the sample size increases by 5–10 times on the basis of the independent variable.
This study combined expert consultation method, literature analysis method and group discussion method to compile a questionnaire for operating room nurses on the cognition and implementation status of prevention of patient's acquired pressure injury. Through reviewing relevant literature at home and abroad, after intensive discussion by members of the research group, and combined with clinical post management measures, a questionnaire entry pool of 48 items in five dimensions including IAPI prevention implementation, IAPI preventive cognition, preoperative IAPI preventive cognition, basic knowledge of pressure injury, and special patient IAPI prevention implementation was preliminarily formed.
The expert consultation method was used to conduct 2 rounds of expert consultation for 10 experts, and the questionnaire on the cognition and implementation status of the nurses in the operating room on the prevention of patient's acquired PI was revised, and the expert inclusion criteria were as follows: ① engaged in clinical nursing or nursing management in the operating room; ② voluntary and guaranteed continuous participation in the subject; ③ have more than 10 years of clinical work experience; ④ intermediate or above professional title; ⑤ bachelor's degree or above. The experts were contacted before issuing the letter inquiry form through e-mail or on-site distribution to obtain their advice, and eventually, a questionnaire of prevention of IAPI containing 45 items in five dimensions for the cognition and implementation status of operating room nurses was developed.
The questionnaire of prevention of IAPI with five dimensions and 45 items to the cognition and implementation status of operating room nurses was verified through two stages. The first stage was as follows: operating room nurses from three 3-A-class hospitals in Shandong Province were selected to fill in the questionnaire for project analysis, reliability analysis and validity analysis. The questionnaire consisted of three parts: ① general profile of the study subject; ② purpose and description of the survey; ③ the main part of the questionnaire consists of 45 entries. A 5-point Likert scale was adopted for the 45 items. The higher the score, the clearer the understanding of the operating room nurse in the prevention of patient-acquired PI and the better able to implement it. Before the questionnaire is distributed, the research purpose and precautions were explained to the research objects. After the questionnaire was collected, the contents were carefully verified and incomplete questionnaires were eliminated. Based on the results of the initial questionnaire data analysis, the questionnaire was revised and entered the second stage. The second phase was as follows: operating room nurses from three 3-A-class general hospitals in Shandong Province were selected for the confirmatory factor analysis and structural equation construction. Nurses who had participated in the previous phase were excluded. Based on the research results, the questionnaire was revised, revealing a questionnaire of the prevention of patient's IAPI composed of five dimensions and 38 items that can be applied to the the operating room nurse's awareness and implementation status.
The data used are entered and proofread through Microsoft Excel. Demographic characteristics are described through descriptive statistics, such as the average of continuous variables and the frequency of category variables. Date analysis was performed using IBM SPSS software version 26.0, such as project analysis and reliability analysis, with a significance value of p set at <0.05. In addition, AMOS 24.0 statistical software was used to validate factor analysis and construct structural equation.
The questionnaire was revised in two stages and 530 valid questionnaires were received. Table 1 shows general information about participants in both phases.
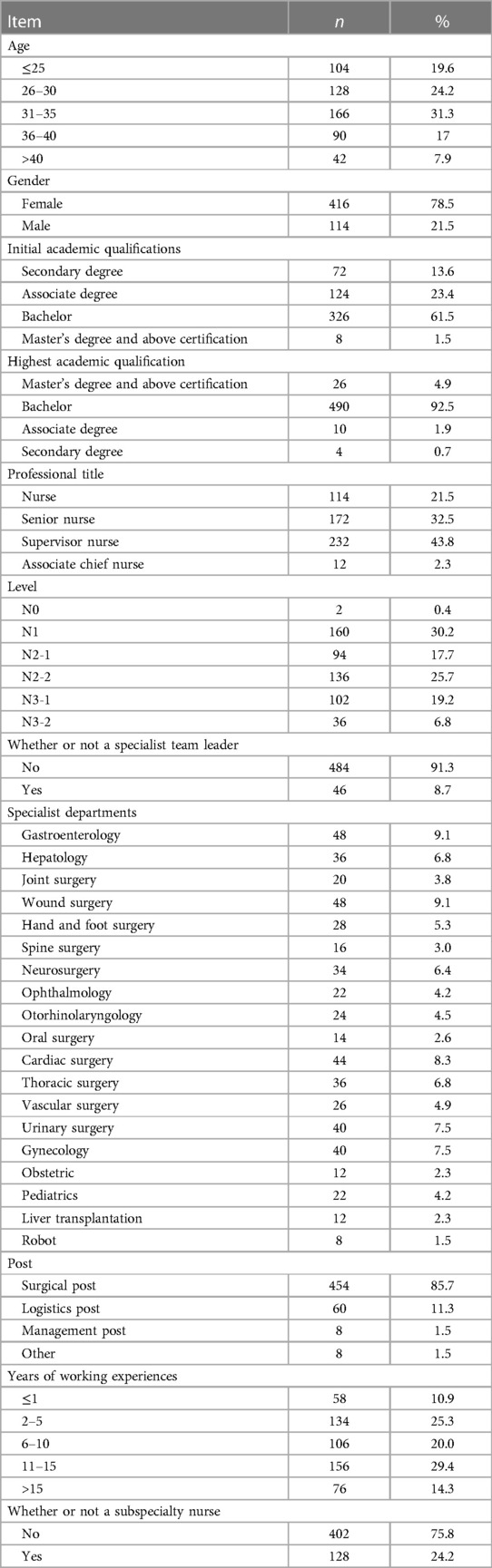
Table 1. Characteristics of the participants [phase 1 & phase 2; (n = 530)].
Project analysis is used to assess the effectiveness and applicability of questionnaire items. The principle is to summarize the conditions first, with the first 27% of subjects recorded as high and the second 73% as low. The T-test is then used to compare the difference between high and low-score groups. If there is a difference, the design of the scale item is appropriate. Otherwise, the scale item is indistinguishable from the information and the design is unreasonable. It should be deleted (16).
As can be seen from Table 2, high and low scores showed significance for Q1 to Q45 items (p < 0.05), indicating that all 45 projects were well differentiated and did not require the deletion of the analysis items.
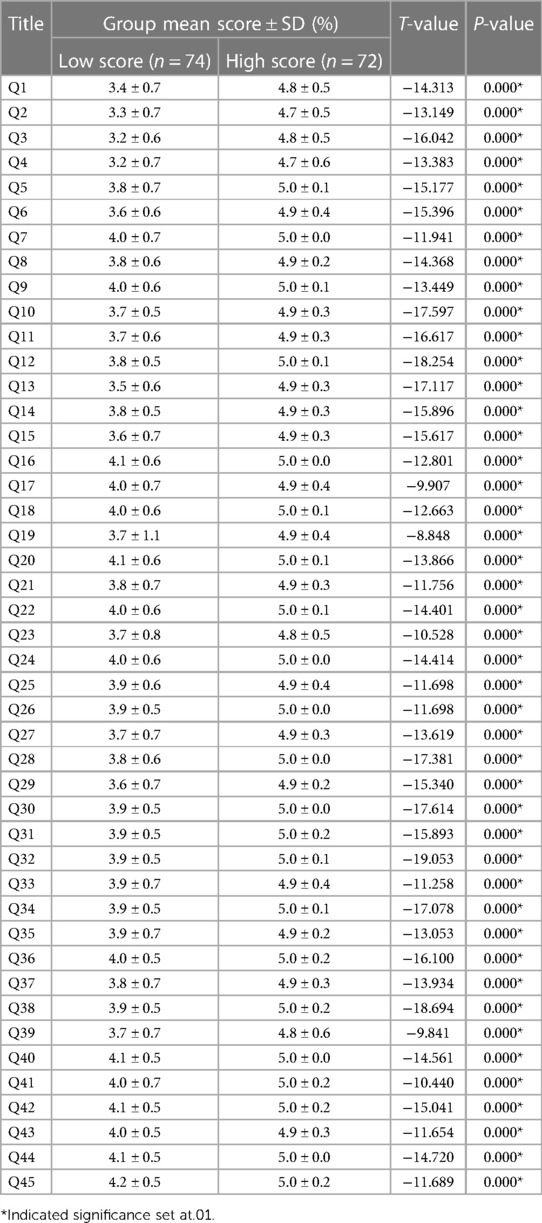
Table 2. The analysis results of the project analysis.
Reliability analysis, which is primarily used to evaluate the reliability and accuracy of quantitative data answers, should be guided by the following principles: (1) the Cronbach α coefficient ≥0.8, indicating high reliability; (2) if Corrected Item-Total Correlation (CITC) ≤0.3, consider deleting the item; and (3) if the “deleted α coefficient” is significantly higher than the α coefficient, consider deleting the item and re-analyzing it. Details are shown in Table 3.
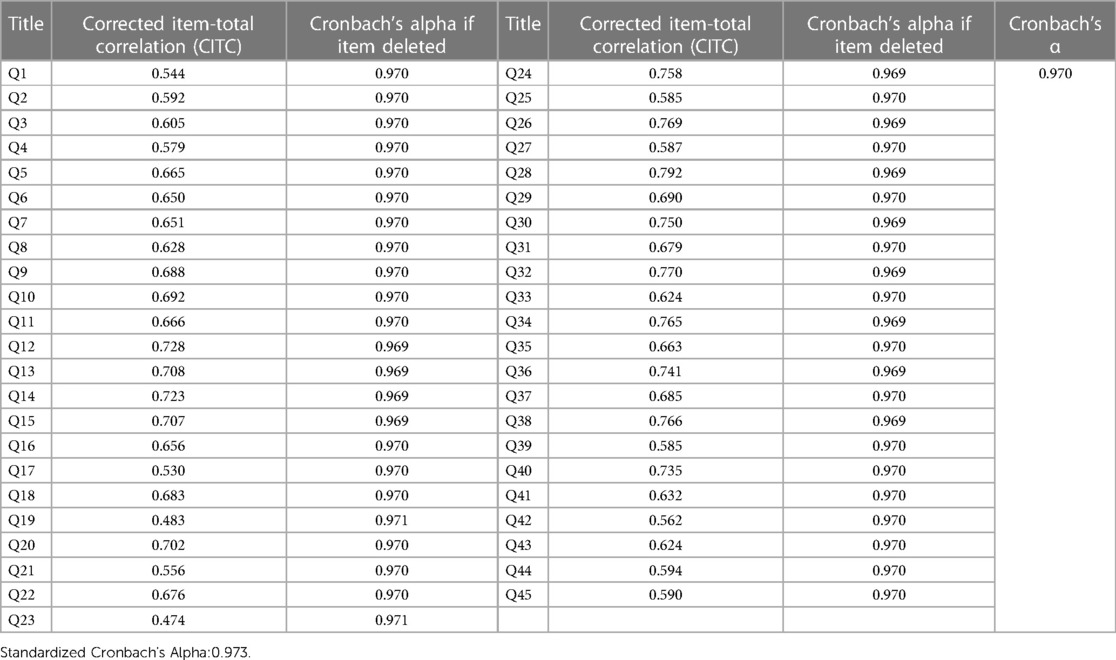
Table 3. Reliability analysis.
As can be seen from Table 3, the reliability coefficient value is 0.970, as it is greater than 0.9, indicating a very high reliability quality of the study data. For the “deleted item alpha factor”, the reliability coefficient would increase significantly if Q19 and Q23 were deleted, so consider correcting or deleting them. For the “CITC value”, all items meet the standard.
In summary, consider deleting Q19 and Q23.
Validity analysis is used to determine the relevance of tool items to the concepts being assessed (17). Content validity and structural validity are selected for analysis in this study.
The average content validity index (S-CVI) of the questionnaire was 0.926, and the content validity index (I-CVI) of the entry level was 0.821∼1.000.
The validity analysis of the data was verified by a comprehensive analysis of KMO, commonality, variance explanation rate, and factor loading coefficient.
The KMO test and the Bartlett test allow for assessing the applicability factor analysis for a particular data or the adequacy of sampling (18). Common values are used to eliminate irrational research projects; variance explanation rates are used to illustrate the level of information extraction; and the factor loading coefficients are used to measure the correlation between factors and problems.
The KMO value is 0.946 with a result greater than 0.8, indicating good validity of the study data. As can be seen from Table 4, two factors in Q8, Q10, Q42, and Q44 load simultaneously >0.5, while factors in Q17 load less than 0.5, so the five items with invalid headings should be deleted. In addition, the variance interpretation rate values of the six factors were 18.29%, 14.88%, 13.95%, 12.51%, 6.21%, and 5.26%, respectively. The cumulative variance explanation rate after rotation is 71.10% > 60%. This means that the amount of information on the research item can be extracted efficiently.
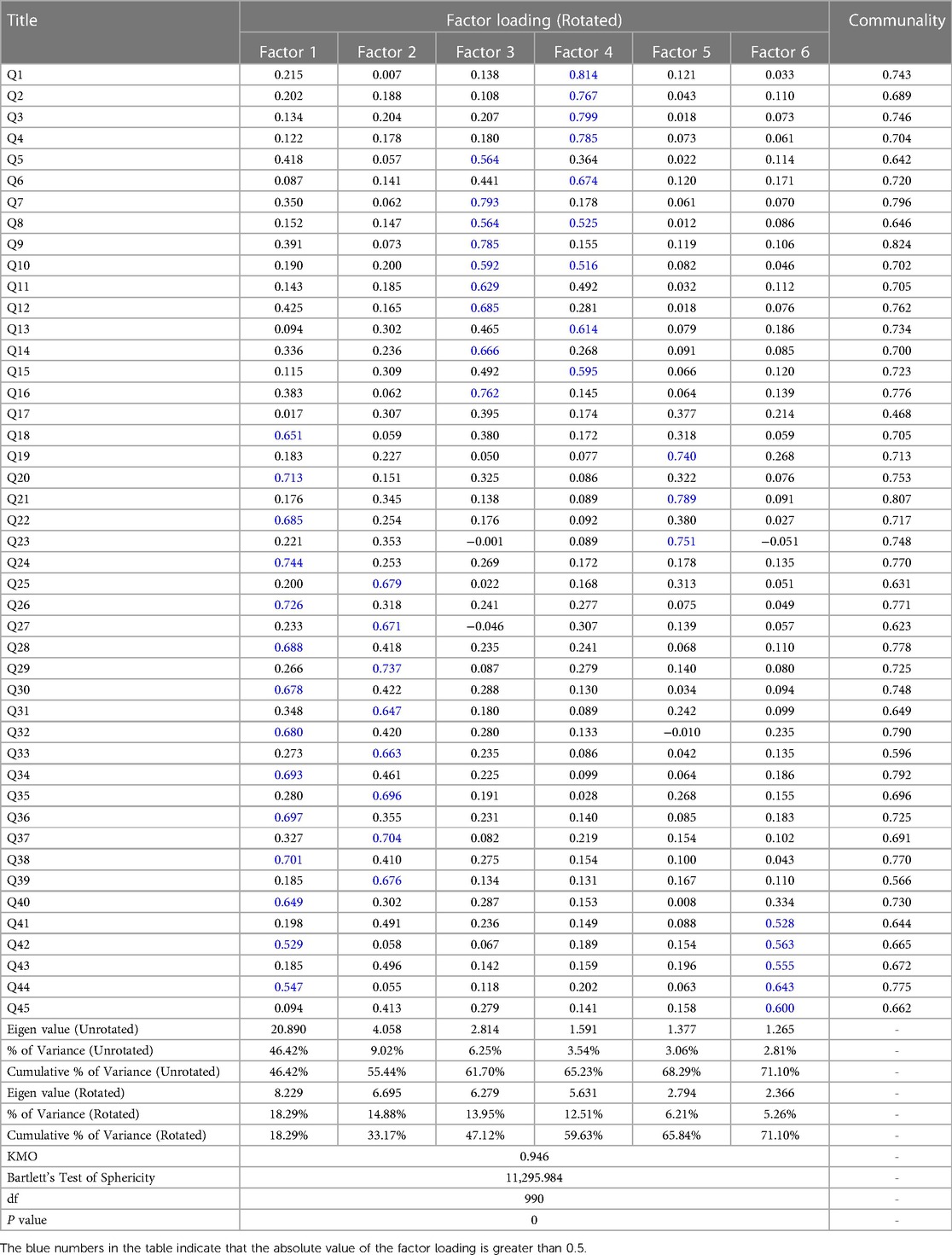
Table 4. Results of validity analysis.
In summary, seven questions were excluded from the analysis of the initial questionnaire: Q8, Q10, Q17, Q19, Q23, Q42, and Q44. At the same time, the remaining questions were adjusted and the questionnaire was sent out again for hypothesis verification.
After the reliability analysis of the revised questionnaire, the overall Cronbach's α coefficient was 0.969. Moreover, Cronbach's alpha coefficients for each dimension were as follows: implementation of IAPI prevention, 0.927; IAPI prevents cognitive conditions, 0.959; preoperative IAPI to prevent cognitive conditions, 0.939; basic knowledge of PI, 0.926; implementation of IAPI prevention in special patients, 0.846. All indicators were above 0.7, indicating good reliability value of the questionnaire.
Principal component analysis was performed on the revised questionnaire data to test the validity of the variables. Before factor analysis, each variable was tested for the KMO test and Bartlett's test of sphericity to determine if factor analysis is possible.
The KMO value is 0.945 > 0.6, and the significance value of the Bartlett sphericity test is <0.05, indicating that there are common factors and are suitable for factor analysis.
A total of 5 factors were extracted using principal component analysis, with a cumulative variance interpreted as 0.71, indicating that of all variables, 71% of variable information could be aggregated by extracting 5 factors, as detailed in Table 5. By factor rotation, the maximum variance method is used and the factor load of each component was greater than 0.5, as shown in Table 6. A total of five components were identified, which is in line with the revised questionnaire. In conclusion, the structure of this survey questionnaire is reasonable.
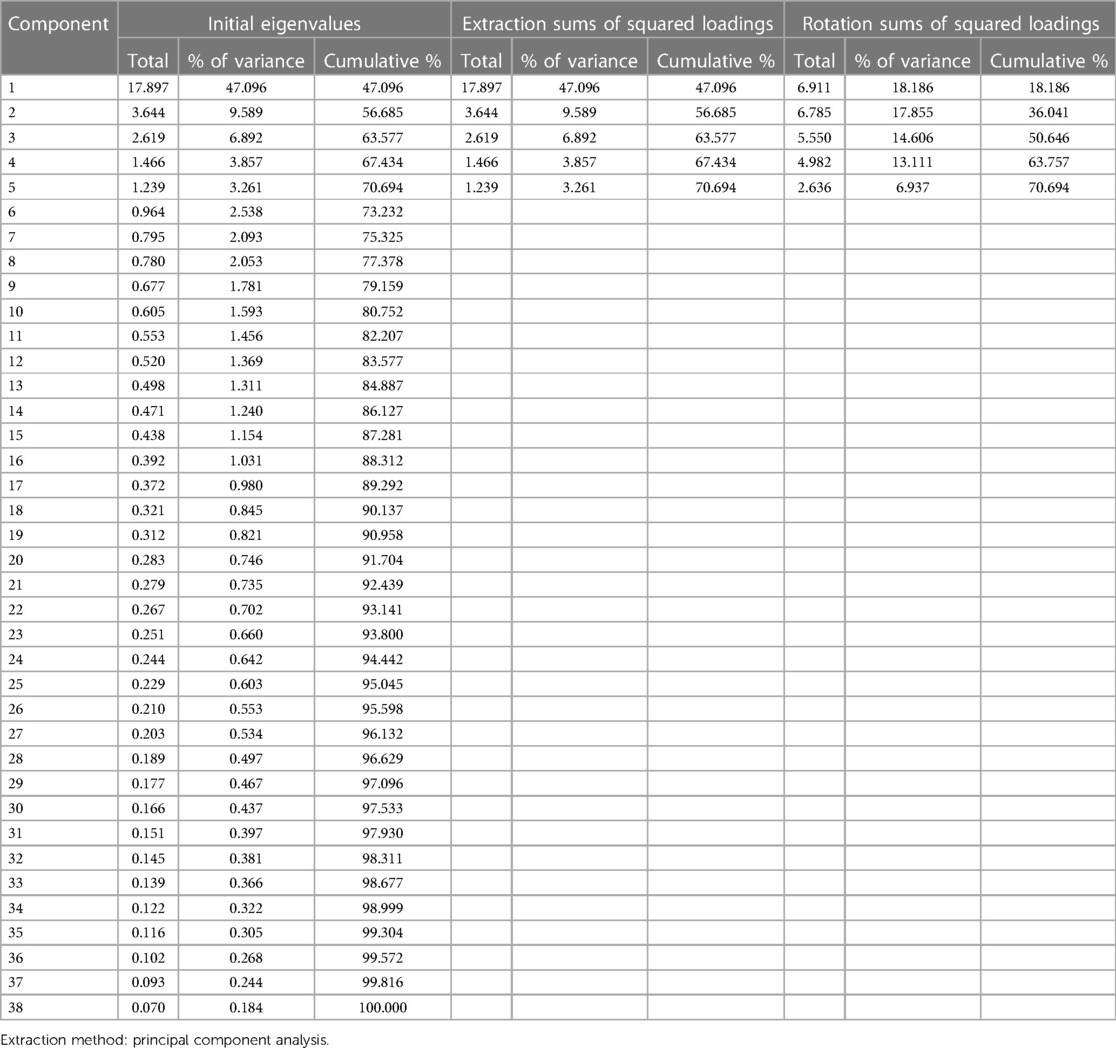
Table 5. Total variance explained.
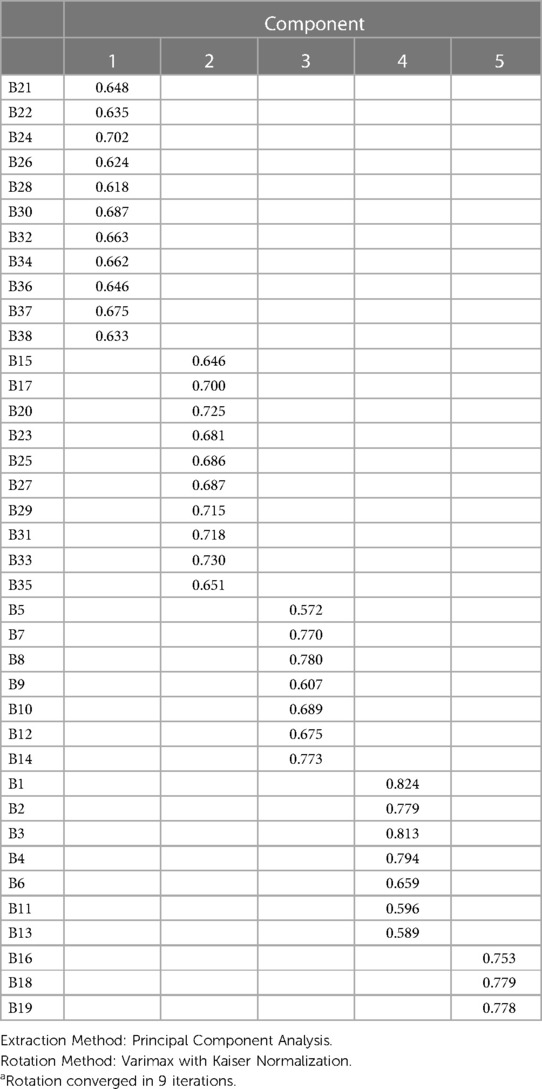
Table 6. Rotated component matrixa.
In this study, we performed a validation factor analysis using AMOS 24.0 software for a questionnaire on the patients’ cognition and implementation status of surgical acquired pressure injury among operating room nurses. Key indications included: Root Mean Square Residual (RMR), Tucker-Lewis Index (TLI), Incremental Fit Index (IFI), Comparative Fit Index (CFI), and Root-Mean-Square Error of Approximation (RMSEA). By testing the goodness-of-fit coefficient of the model, the results show that all indicators are within a reasonable range. The model path is significantly tested, the model factor load is greater than 0.5, and the path is significant, which proves once again that the model has good structural validity. The AMOS verification model is shown in Figure 1, and the path fit and path coefficient are shown in Tables 7, 8.
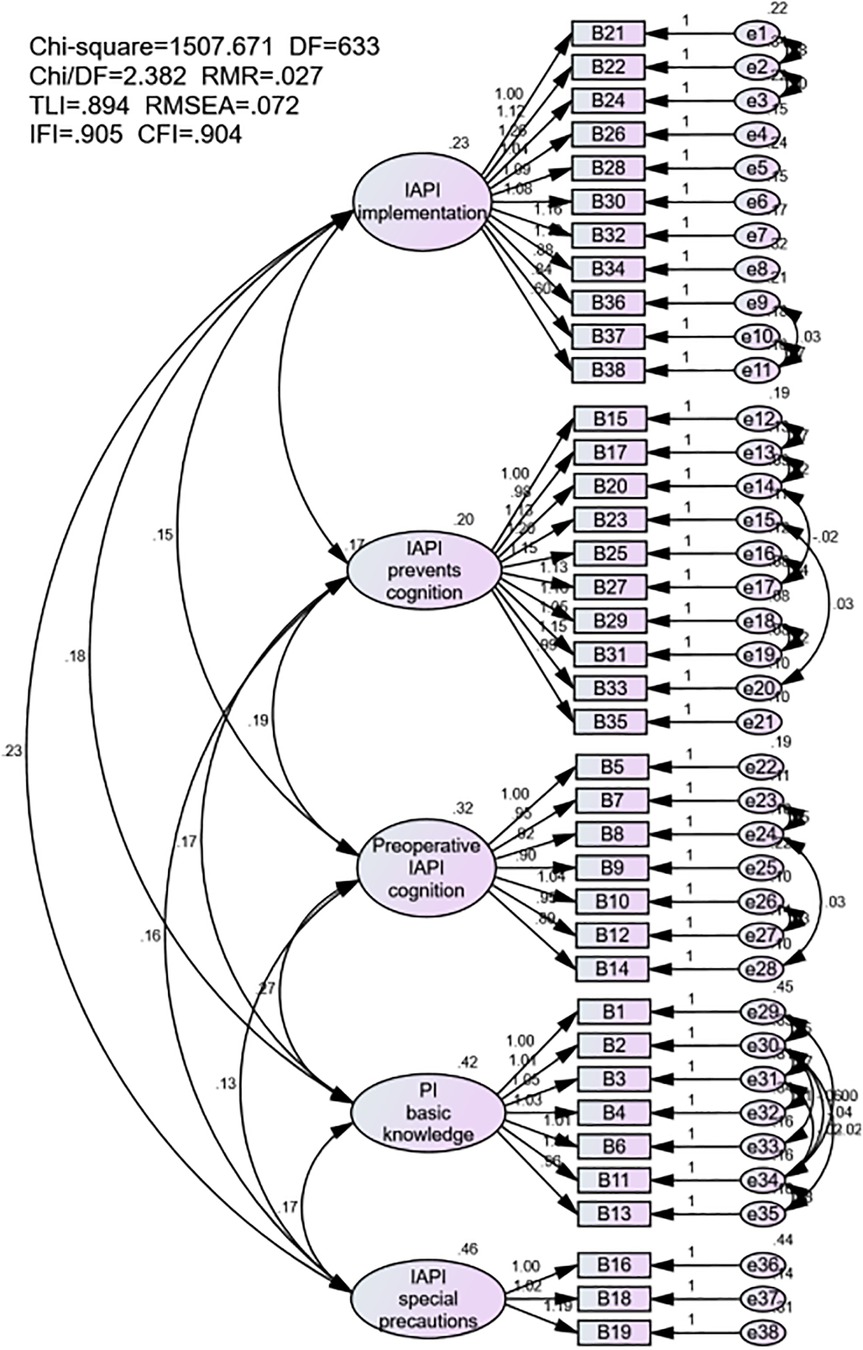
Figure 1. Model of structural equations.

Table 7. Model fit summary.
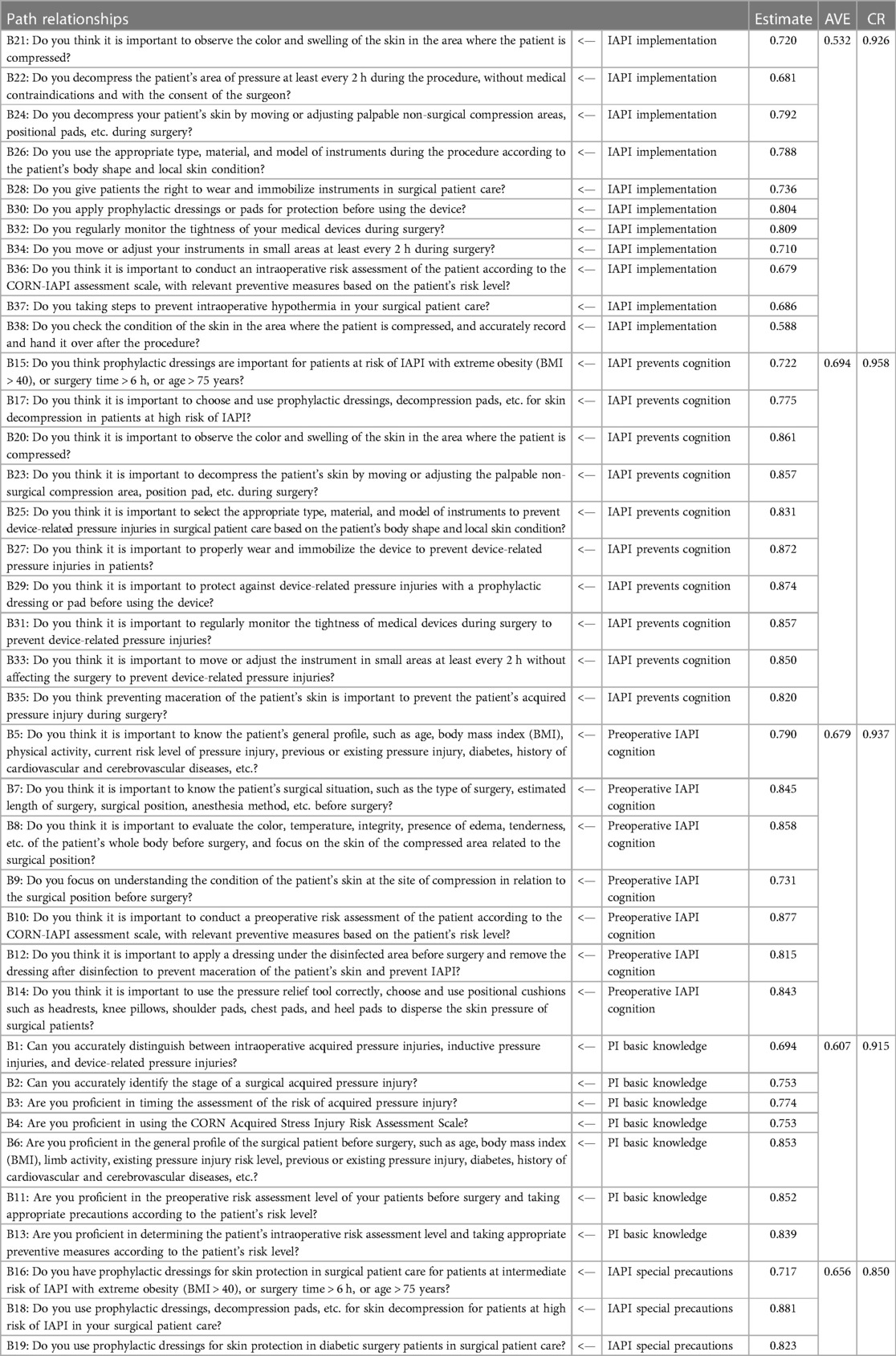
Table 8. Path coefficient analysis.
The data after the correction of the model shows that: χ2/df = 2.382; RMR = 0.027; TLI = 0.894; RMSEA = 0.072; IFI = 0.905; CFI = 0.904. The overall display model structure is well valid, as shown in Figure 1. The final version of the questionnaire is shown in Table 9.
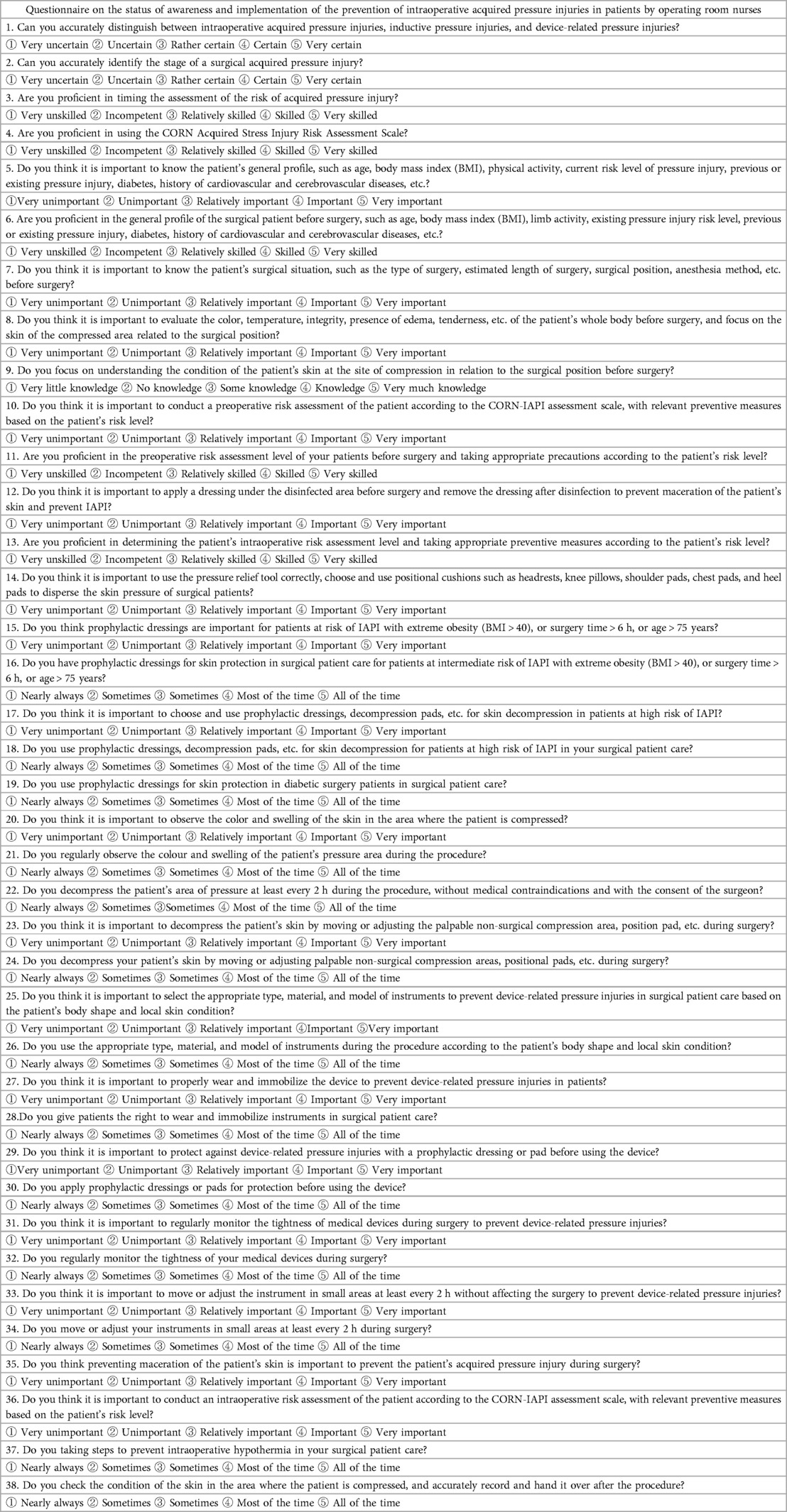
Table 9. The final version of the questionnaire.
The operating room is an important department that is independently managed in the operation of the hospital, and the patient's time in the operating room is usually an independent event during the hospitalization, and IAPI mostly occurs within hours to up to 5 days after surgery (19). Continuously refining the nursing management mode of the operating room and improving the prevention awareness of the nursing staff in the operating room is the key to strengthening standardized nursing.
At present, although there are relevant scales to assess IAPI, they are less involved in the cognition of prevention related to operating room nurses, and a systematic prevention management questionnaire has not been formed. This study conducted in-depth research on the cognition and implementation status of IAPI prevention in patients in operating room nurses, analyzed various influencing factors of IAPI prevention, understood the implementation status of preventive measures, and provided the reference for further optimizing the prevention and management of IAPI through scientific evaluation.
The overall Cronbach's alpha coefficient of the questionnaire was 0.969, whereas that of each dimension of the questionnaire was above 0.70, which is consistent with the criterion that the reliability coefficient should preferably be above 0.70. This indicated that the internal consistency of the questionnaire is great.
In this study, the questionnaire for operating room nurses on the current status of awareness and implementation of the prevention of IAPI was constructed using the expert consultation method, literature analysis method, and group discussion method. The scientific and reasonable verification of the entries through structural validity, exploratory factor analysis, and validation factor analysis confirmed that each dimension and item met the research theme. In the exploratory factor analysis, the principal component analysis method was used, and five principal components were obtained, which cumulatively explained 70.694% of the total variance. The factor load matrix of each factor is 0.572∼0.824, which met the requirements that the factor load should be greater than 0.400. Additionally, validation factor analysis showed that χ2/df = 2.382, RMR = 0.027, TLI = 0.894, RMSEA = 0.072, IFI = 0.905, CFI = 0.904 met the statistical criteria, which indicates that this model fits well and has a better simulation degree. Thus, the questionnaire structure has a great fit, and the structural validity of the questionnaire is excellent.
The questionnaire for operating room nurses on the current status of awareness and implementation of the prevention of IAPI is beneficial for nursing managers to understand the current mastery of IAPI prevention knowledge and the implementation of nursing measures by operating room nurses, and to investigate the areas in which IAPI preventive management can be improved in operating room nursing management. Thereby, this study provides a reference basis for the optimization of scientific preventive management in the operating room.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Ethics Committee of Provincial Hospital of Shandong First Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
ZZ: Conceptualization, Data curation, Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing. SL: Data curation, Investigation, Writing – review & editing. QG: Conceptualization, Investigation, Supervision, Writing – review & editing. XZ: Investigation, Supervision, Writing – review & editing. JM: Investigation, Resources, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Scott EM, Buckland R. Pressure ulcer risk in the peri-operative environment. Nurs Stand. (2005) 20(7):74–81. doi: 10.7748/ns2005.10.20.7.74.c3989
2. Jackson DE, Durrant LA, Hutchinson M, Ballard CA, Neville S, Usher K. Living with multiple losses: insights from patients living with pressure injury. Collegian. (2018) 25(4):409–14. doi: 10.1016/j.colegn.2017.10.008
3. Obagi Z, Damiani G, Grada A, Falanga V. Principles of wound dressings: a review. Surg Technol Int. (2019) 35:50–7.31480092
4. Demarré L, Verhaeghe S, Annemans L, Van Hecke A, Grypdonck M, Beeckman D. The cost of pressure ulcer prevention and treatment in hospitals and nursing homes in Flanders: a cost-of-illness study. Int J Nurs Stud. (2015) 52(7):1166–79. doi: 10.1016/j.ijnurstu.2015.03.005
5. Cebeci F, Senol Celik S. Knowledge and practices of operating room nurses in the prevention of pressure injuries. J Tissue Viability. (2022) 31(1):38–45. doi: 10.1016/j.jtv.2021.07.007
6. Burlingame BL. Guideline implementation: positioning the patient. AORN J. (2017) 106(3):227–37. doi: 10.1016/j.aorn.2017.07.010
7. Shi G, Jiang L, Liu P, Xu X, Wu Q, Zhang P. Using a decision tree approach to analyze key factors influencing intraoperative-acquired pressure injury. Adv Skin Wound Care. (2023) 36(11):591–7. doi: 10.1097/ASW.0000000000000003
8. Doughty D, Ramundo J, Bonham P, Beitz J, Erwin-Toth P, Anderson R, et al. Issues and challenges in staging of pressure ulcers. J Wound Ostomy Continence Nurs. (2006) 33(2):125–30. doi: 10.1097/00152192-200603000-00004
9. Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieggreen M. Revised national pressure ulcer advisory panel pressure injury staging system: revised pressure injury staging system. J Wound Ostomy Continence Nurs. (2016) 43(6):585–97. doi: 10.1097/WON.0000000000000281
10. Mervis JS, Phillips TJ. Pressure ulcers: pathophysiology, epidemiology, risk factors, and presentation. J Am Acad Dermatol. (2019) 81(4):881–90. doi: 10.1016/j.jaad.2018.12.069
11. Neves RC, Pinheiro Santos M, Oliveira dos Santos C. Escalas utilizadas para prevenir Úlceras por pressÃo em pacientes crÍticos. Revista Enfermagem Contemporânea. (2013) 2(1):19–31. doi: 10.17267/2317-3378rec.v2i1.185
12. Gurkan A, Kirtil I, Aydin YD, Kutuk G. Pressure injuries in surgical patients: a comparison of Norton, Braden and Waterlow risk assessment scales. J Wound Care. (2022) 31(2):170–7. doi: 10.12968/jowc.2022.31.2.170
13. Chen Y, Wang W, Qian Q, Wu B. Comparison of four risk assessment scales in predicting the risk of intraoperative acquired pressure injury in adult surgical patients: a prospective study. J Int Med Res. (2023) 51(10):3000605231207530. doi: 10.1177/03000605231207530
14. Choi S, Kim YJ, Oh H, Yuh WT, Lee CH, Yang SH, et al. Factors associated with perioperative hospital acquired pressure injury in patients undergoing spine surgery in the prone position: a prospective observational study. J Neurosurg Anesthesiol. (2024) 36(1):45–52. doi: 10.1097/ANA.0000000000000867
15. Gao L, Yang L, Li X, Chen J, Du J, Bai X, et al. The use of a logistic regression model to develop a risk assessment of intraoperatively acquired pressure ulcer. J Clin Nurs. (2018) 27(15-16):2984–92. doi: 10.1111/jocn.14491
16. Hou J, Zhu Y, Tong J, Ndasauka Y, Fang X. Preparation of multi-motive grid questionnaire for social networking sites use. PLoS One. (2020) 15(5):e0233205. doi: 10.1371/journal.pone.0233205
17. Park DI. Development and validation of a knowledge, attitudes and practices questionnaire on COVID-19 (KAP COVID-19). Int J Environ Res Public Health. (2021) 18(14):7493. doi: 10.3390/ijerph18147493
18. Polit DF, Beck CT. Nursing research: generating and assessing evidence for nursing practice. Lippincott Williams Wilkins. (2008).
Keywords: intraoperative acquired pressure injuries, operating room nursing, cognitive conditions, status of implementation, instrument development, surveys and questionnaires, validation study
Citation: Zou Z, Lv S, Gao Q, Zhou X and Mao J (2024) Operating room nurse's awareness and implementation status of the prevention of patient's intraoperative acquired pressure injuries: design and validation of a questionnaire. Front. Surg. 10:1308181. doi: 10.3389/fsurg.2023.1308181
Received: 6 October 2023; Accepted: 11 December 2023;
Published: 4 January 2024.
Edited by:
Marina Yiasemidou, Hull York Medical School, United KingdomReviewed by:
Manuela Mastronardi, University of Trieste, Italy© 2024 Zou, Lv, Gao, Zhou and Mao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinbao Mao bWFvamluYmFvQDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.