 A. Tsoposidis1
A. Tsoposidis1 A. Thorell2,3H. Axelsson4
A. Thorell2,3H. Axelsson4 M. Reuterwall Hansson2,3*†L. Lundell5,6V. Wallenius4
M. Reuterwall Hansson2,3*†L. Lundell5,6V. Wallenius4 S. Kostic4B. Håkanson2,3
S. Kostic4B. Håkanson2,3
- 1Department of Surgery, Institute of Clinical Sciences, Sahlgrenska Academy, Sahlgrenska University Hospital, University of Gothenburg, Gothenburg, Sweden
- 2Department of Clinical Sciences, Danderyds Hospital, Karolinska Institutet, Stockholm, Sweden
- 3Department of Surgery, Ersta Hospital, Stockholm, Sweden
- 4Department of Surgery, Institute of Clinical Sciences, Sahlgrenska Academy, Sahlgrenska University Hospital Östra, University of Gothenburg, Gothenburg, Sweden
- 5Division of Surgery and Oncology CLINTEC, Karolinska Institutet, Stockholm, Sweden
- 6Department of Surgery, Odense University Hospital, Odense, Denmark
Background: Surgical repair of paraesophageal hernias (PEHs) is burdened with high recurrence rates, and hitherto various techniques explored to enforce the traditional crural repair have not been successful. The hiatal reconstruction in PEH is exposed to significant tension, which may be minimized by adding a diaphragmatic relaxing incision to enhance the durability of the crural repair.
Patients and methods: All individuals undergoing elective laparoscopic repair of a large PEH, irrespective of age, were considered eligible. PEHs were classified into types II–IV. The preoperative work-up program included multidetector computed tomography and symptom assessment questionnaires, which will be repeated during the postoperative follow-up. Patients were randomly divided into a control group with crural repair alone and an intervention group with the addition of a left-sided diaphragmatic relaxing incision at the edge of the upper pole of the spleen. The diaphragmatic defect was then covered by a synthetic mesh.
Results: The primary endpoint of this trial was the rate of anatomical PEH recurrence at 1 year. Secondary endpoints included symptomatic gastroesophageal reflux disease, dysphagia, odynophagia, gas bloat, regurgitation, chest pain, abdominal pain, nausea, vomiting, postprandial pain, cardiovascular and pulmonary symptoms, and patient satisfaction in the immediate postoperative course (3 months) and at 1 year. Postoperative complications, morbidity, and disease burden were recorded for each patient. This was a double-blind study, meaning that the operation report was filed in a locked archive to keep the patient, staff, and clinical assessors blinded to the study group allocation. Blinding must not be broken during the follow-up unless required by any emergencies in the clinical management of the patient. Likewise, the patients must not be informed about the details of the operation.
Trial Registration: ClinicalTrials.gov, identification number NCT04179578.
Introduction
Paraesophageal hernias (PEHs) are rare, accounting for less than 5% of all hiatus hernias (HHs) (1), and occur most commonly in older people. A PEH is characterized by a herniation of the gastric fundus and sometimes the entire stomach (with or without additional viscera) through a widened diaphragmatic hiatus. The indications for surgical repair are controversial but must balance the patient's fitness for surgery and respective symptom burden (2–6). Surgical repair traditionally includes dissection of the hernia sac from the mediastinum, reduction of herniated intra-abdominal organs, posterior repair of the crura (with or without mesh), and a fundoplication to control reflux.
Although good clinical outcomes have been reported with direct suturing of the hiatus, clinical and/or radiological recurrences have been described in up to 60% of patients (7–12). The use of mesh to reinforce the crura has been suggested to reduce the recurrence of PEH based on the same principles that have been successfully used in groin hernia repair. However, although the use of mesh in laparoscopic surgery of hiatus hernia has increased, the indications for mesh reinforcement can be seriously questioned. The primary concern regarding the use of mesh is the long-term risk of mesh erosion into the esophagus and other adjacent vital structures. To avoid or reduce this risk, the synthetic mesh has been abandoned in favor of biological meshes (6, 13–18). However, results from more recent reports suggest that the long-term durability of mesh (irrespective of type) and suture cruroplasty did not differ. Indeed, the same high recurrence rates have been reported during the first 3–5 years postoperatively in patients with smaller hiatus hernias, including the traditional sliding hernias (type I HH) (6, 19–24). Accordingly, novel approaches must be explored to enable more durable reconstructions in HH repair.
One possible explanation behind the high recurrence rates can be found in the three-dimensional structures of the hiatus, which are in constant motion. In addition, the counteracting pressures prevailing in the abdominal and chest cavities create a situation where the experiences from other types of hernia repair do not apply (10, 24–26). However, a complementary explanation is that during laparoscopic repair there may be an underappreciation of the tension applied to the repair. This tension comes from two major directions: axial tension related to esophageal shortening and lateral tension related to the widely separated crura that must be reapproximated as part of the repair. The pathogenetic relevance of this lateral tension can conceptually be addressed by adding diaphragmatic relaxing incisions to enhance the durability of the crural repair (27, 28). Until now, this concept has not been evaluated in the randomized clinical trial setting.
Objectives
In this trial, we compared the rates of anatomical PEH recurrence at 1 year in patients allocated to diaphragmatic relaxing incisions to those with a crural repair alone.
Secondary objectives included rates of symptomatic gastroesophageal reflux disease (GERD), dysphagia, odynophagia, gas bloat, regurgitation, chest pain, abdominal pain, nausea, vomiting, postprandial pain, cardiovascular and pulmonary symptoms, and patient satisfaction in the immediate postoperative course (3 months) and at 1 year. The Clavien–Dindo classification and the comprehensive complication index were also used to measure postoperative complications, morbidity, and disease burden for each patient (29, 30).
Patients and methods
The trial occurred at two high-volume centers, one in Stockholm and one in Göteborg, Sweden. All operations were performed by or directly supervised by one experienced upper gastrointestinal surgeon, and all procedures were completed within a university teaching hospital setting. All individuals undergoing elective laparoscopic repair of a PEH, irrespective of age, were considered eligible. PEHs were classified into type II (pure paraesophageal), type III (combined sliding and paraesophageal), and type IV (combined with other hernia sac contents than the stomach). Patients who have undergone previous surgery involving the stomach or the esophagogastric junction or who require any additional procedure affecting the hiatal hernia (HH) repair were excluded.
Pre- and postoperative investigations included esophagogastroduodenoscopy, multidetector computed tomography (MDCT), and symptom assessment questionnaires. Esophageal high-resolution manometry and pH monitoring were used selectively in patients with significant reflux symptoms but most often omitted in patients in whom the indication for surgery is mechanical symptoms emanating from the hernia.
Trial group allocation
Patients were asked to sign an informed consent before surgery and were randomly divided into one of the two groups in a 1:1 ratio during surgery, after the induction of the anesthesia:
Group 1 (control group) patients had a crural repair using sutures alone (control) + a total fundoplication.
Group 2 (intervention group) was the same as group 1 but before adapting the crura, a left-sided 5–6-cm-long diaphragmatic relaxing incision was added at the edge of the upper pole of the spleen (Figure 1).
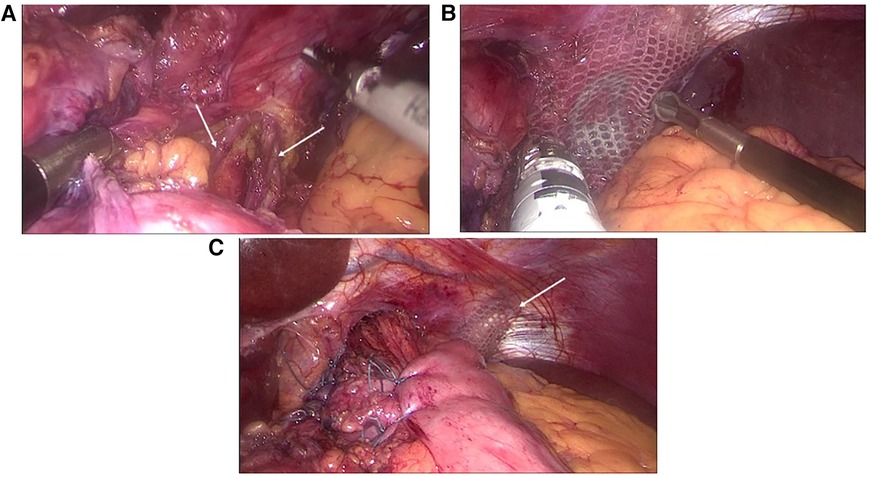
Figure 1. Intraoperative images demonstrating (A) the left-sided lateral diaphragmatic incision (also marked by the arrows) originating from the costal area close to the pole of the spleen, (B) the application of the mesh to cover the diaphragmatic defect, and (C) an overview of the end result including the total fundoplication.
Randomization and blinding
Randomization was performed during the operation by opening a sealed envelope. The envelopes were prepared before the start of the trial and shuffled independently by research nurses. More envelopes were prepared than needed to ensure that the operating surgeon cannot anticipate the randomization. A computer-generated randomization list in blocks of eight was used. The subsequent operation report, with information on the specific type of repair performed, was not included in the digital patient chart. Instead, a hard copy was created and kept in a sealed envelope, which is filed in a locked archive to keep the patient, staff, and clinical assessors blinded to the study group allocation. Blinding must not be broken during the follow-up unless required by any emergencies in the clinical management of the patient. Likewise the patients will not be informed about the details of the operation. The same is true for the clinical follow-up investigators.
Operating technique
Before commencing the trial, surgical techniques were standardized and harmonized across the two sites after a consensus meeting between the participating surgeons and an exchange of videos of the standard operating techniques.
The initial steps entailed full dissection and resection of the hiatus hernia sac from the mediastinum, and complete reduction of the sac's contents into the abdomen. An esophageal lengthening procedure was not added. Five trocars were utilized. Ultracision (Ethicon Endo-Surgery) was used for dissection. After completing the hernia sac resection, the anatomical preparation of both crural muscles followed. Mobilization of the mediastinal esophagus was completed to allow at least 3 cm of the lower esophagus to rest without tension below the hiatus. The posterior and anterior branches of the vagal nerve were identified and kept within the wrap. The gastric fundus was mobilized as judged necessary to complete a floppy full wrap, with a wrap length of 2 cm by three interrupted non-absorbable sutures (GORE-TEX or Ethibond), all anchored to the esophageal muscular wall. No formal bougie was used in the esophagus during the procedure. In the suture-alone group, the right and left crura were approximated posteriorly to the esophagus using at least three continuous stitches with non-absorbable sutures (GORE-TEX or Ethibond) and a suture-to-suture distance of 5–8 mm, leaving an appropriate remaining opening for the esophagus.
In the intervention group, a left-sided diaphragmatic relaxing incision was added at the edge of the upper pool of the spleen before adapting the crura (Figure 1). The length of this incision was 5–6 cm. After the completion of the crural sutures, the gap in the diaphragm was covered by a synthetic mesh, which was anchored to the remaining diaphragm by staples.
During the procedure, the esophageal length was measured endoscopically before hernia sac reduction and esophageal mobilization and at the time point after completion of the hiatal reconstruction. The length from the incisors to the GEJ was recorded in centimeters. The hiatal area was calculated before reconstruction by measuring (a) the length of the right crus and (b) the distance between the base of the left crus and the base of the right crus. The following formula was used for the calculation of the hiatal area (A, in cm2):
Statistics and sample size
Based on the assumption that the 12-month CT detected recurrence rate is at least 30%, it can be estimated that, by the effect of the intervention, these figures were reduced by 50%–15%. Accordingly, by enrolling 35 patients into each group, such a difference can be detected at a probability of 5% and a power of 80%. To compensate for the loss of follow-up and early exit of patients, 80 patients were enrolled.
All data were entered into a computerized database. Analyses were performed on an intention-to-treat basis with patients analyzed according to randomization. The two groups were compared separately. The χ2 test was used to evaluate 3 × 2 contingency tables. Comparison of continuous data sets was completed using one-way analysis of variance. A p-value of <0.05 was considered statistically significant. The statistical analyses were performed using the statistical software package SPSS, version 26.0 (SPSS, Inc., Chicago, IL, USA).
Follow-up assessment
After discharge, the patients were followed up at 3 and 12 months. The Swedish version of the validated Short Form-36 (SF-36) questionnaire was used for global QoL assessment, and data were then presented as physical and mental component scores (PCS and MCS). For each subscale score (0–100), higher values reflect improved health status. The gastrointestinal symptom rating scale (GSRS) is a validated questionnaire containing five dimensions of abdominal symptoms (gastroesophageal reflux, abdominal pain, indigestion, obstipation, and diarrhea). The subscales were presented according to a seven-point Likert scale, and the mean item scores of the respective domain were used throughout the study. Higher values represent more severe symptoms. For these two questionnaires, comparative values for the adult normal population were available. In addition, a standardized specific questionnaire was used, which includes a four-graded scale to describe any dysphagia for solid and liquid food components (31). The MDCT was done only at 12 months postoperatively.
Discussion
The number of PEH repairs has increased significantly over the last three decades, but the optimal technique for hiatal closure, either sutured or mesh-augmented (absorbable or non-absorbable), remains controversial. In the 1990s, the standard laparoscopic approach was developed to include PEH repair: during these operations, the need to dissect the entire hernia sac from the mediastinum and restore the anatomy in the GEJ was emphasized. Despite these many precautions, at least a third of these patients develop a radiological hernia recurrence by 5 years postsurgery, albeit most patients probably remain asymptomatic (8, 24). To address the problem of high recurrence rates, tension-free mesh-augmented hernioplasty, analogous to that used to repair groin and abdominal wall hernias, has been proposed. Synthetic absorbable and non-absorbable meshes for hiatal closure have now been evaluated in randomized controlled trials. Data from recent meta-analyses concluded that using mesh in HH repair does not offer any advantage over sutured hiatal closure alone (23). As both techniques deliver good and comparable clinical outcomes, a suture-only technique remains an appropriate standard of care surgical approach.
Nevertheless, hernia recurrence remains the Achilles’ heel of PEH repair. Recurrence after laparoscopic repair seems to be higher than in previous reports on open repairs (1, 10, 24). The explanation for the higher recurrence rate with laparoscopic repair remains unclear, but explanatory factors may include the lack of deep bites during crural closure, with the use of laparoscopic suturing devices, and fewer adhesions associated with laparoscopy compared with an open procedure. However, an alternative explanation may be that during laparoscopic repair, the applied tension may be underappreciated during the repair. The consequences of tension on hernia recurrence are well documented in other settings, including inguinal and ventral hernia repair (32). To reduce tension and improve outcomes with laparoscopic HH repair, adjunct techniques have been adopted. These include a diaphragm relaxing incision, esophageal lengthening wedge-fundectomy, or traditional Collis gastroplasty (1, 4, 27, 28). A diaphragmatic relaxing incision has rarely been tested and, when so, most commonly executed on the right side. This is the easiest approach for the diaphragmatic relaxing incision. However, the right-sided relaxing incision may often be inadequate since the right crus might be frail and phylogenetically only a part of the left. Therefore, a left-sided diaphragmatic relaxing incision carries potential advantages and can almost always be employed. A phrenic nerve injury must be avoided when carrying out a left-sided incision. Large openings (5–6 cm) between the abdomen and thorax are well tolerated during laparoscopic surgery, and in the absence of an injury to lung parenchyma, no chest tube or pleural drainage catheter is routinely placed at the end of the procedure. The follow-up MDCT investigation at 12 months was conducted to determine whether any local complications can be detected at the incision site covered by a synthetic mesh placed at a safe distance from the hiatal region.
The results from the very few retrospective studies that have explored the options offered by these approaches (i.e., either esophageal lengthening or diaphragm relaxing incision) addressing the two major tension forces operating on the crural repair do not offer much guidance in the clinical decision-making process to minimize the risk for recurrent HH. Well-designed, separate RCTs with simple crural closure as reference/control must be completed before alternative recommendations can be made in the surgical management of PEH.
Ethics statement
The studies involving humans were approved by the Human Research Ethics Committee and the Clinical Research Ethics Committees (reference number 2019-02801). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
ATs: Data curation, Investigation, Writing – original draft. ATh: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing. HA: Methodology, Writing – original draft, Writing – review & editing. MR: Methodology, Software, Writing – original draft, Writing – review & editing. LL: Conceptualization, Resources, Supervision, Writing – original draft, Writing – review & editing. VW: Conceptualization, Supervision, Writing – review & editing. SK: Conceptualization, Supervision, Writing – review & editing. BH: Conceptualization, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article.
This study was supported by Stockholm City Council, and Ehrling-Persson Foundation. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Landreneau RJ, Del Pino M, Santos R. Management of paraesophageal hernias. Surg Clin North Am. (2005) 85(3):411–32. doi: 10.1016/j.suc.2005.01.006
2. Clapp B, Hamdan M, Mandania R, Kim J, Gamez J, Hornock S, et al. Is fundoplication necessary after paraesophageal hernia repair? A meta-analysis and systematic review. Surg Endosc. (2022) 36(8):6300–11. doi: 10.1007/s00464-022-09024-0
3. Edye M, Salky B, Posner A, Fierer A. Sac excision is essential to adequate laparoscopic repair of paraesophageal hernia. Surg Endosc. (1998) 12(10):1259–63. doi: 10.1007/s004649900832
4. Watson DI. Current state of repair of large hiatal hernia. Int J Abdom Wall Hernia Surg. (2019) 2(2):39–43. doi: 10.4103/ijawhs.ijawhs_12_19
5. Watson DI, Davies N, Devitt PG, Jamieson GG. Importance of dissection of the hernial sac in laparoscopic surgery for large hiatal hernias. Arch Surg. (1999) 134(10):1069–73. doi: 10.1001/archsurg.134.10.1069
6. Hunter JG, Smith CD, Branum GD, Waring JP, Trus TL, Cornwell M, et al. Laparoscopic fundoplication failures—patterns of failure and response to fundoplication revision. Ann Surg. (1999) 230(4):595–604. doi: 10.1097/00000658-199910000-00015
7. Aly A, Munt J, Jamieson GG, Ludemann R, Devitt PG, Watson DI. Laparoscopic repair of large hiatal hernias. Br J Surg. (2005) 92(5):648–53. doi: 10.1002/bjs.4916
8. Dallemagne B, Kohnen L, Perretta S, Weerts J, Markiewicz S, Jehaes C. Laparoscopic repair of paraesophageal hernia. Long-term follow-up reveals good clinical outcome despite high radiological recurrence rate. Ann Surg. (2011) 253(2):291–6. doi: 10.1097/SLA.0b013e3181ff44c0
9. Rogers MP, Velanovich V, DuCoin C. Narrative review of management controversies for paraesophageal hernia. J Thorac Dis. (2021) 13(7):4476–83. doi: 10.21037/jtd-21-720
10. Zehetner J, Demeester SR, Ayazi S, Kilday P, Augustin F, Hagen JA, et al. Laparoscopic versus open repair of paraesophageal hernia: the second decade. J Am Coll Surg. (2011) 212(5):813–20. doi: 10.1016/j.jamcollsurg.2011.01.060
11. Draaisma WA, Gooszen HG, Tournoij E, Broeders I. Controversies in paraesophageal hernia repair—a review of literature. Surg Endosc. (2005) 19(10):1300–8. doi: 10.1007/s00464-004-2275-3
12. Braghetto I, Lanzarini E, Musleh M, Korn O, Lasnibat JP. Thinking about hiatal hernia recurrence after laparoscopic repair: when should it be considered a true recurrence? A different point of view. Int Surg. (2018) 103(1–2):105–15. doi: 10.9738/INTSURG-D-17-00123.1
13. Frantzides CT, Carlson MA, Loizides S, Papafili A, Luu M, Roberts J, et al. Hiatal hernia repair with mesh: a survey of SAGES members. Surg Endosc. (2010) 24(5):1017–24. doi: 10.1007/s00464-009-0718-6
14. Furnée E, Hazebroek E. Mesh in laparoscopic large hiatal hernia repair: a systematic review of the literature. Surg Endosc. (2013) 27(11):3998–4008. doi: 10.1007/s00464-013-3036-y
15. Edelman DS. Laparoscopic paraesophageal hernia repair with mesh. Surg Laparosc Endosc. (1995) 5(1):32–7. PMID: 7735538
16. Johnson JM, Carbonell AM, Carmody BJ, Jamal MK, Maher JW, Kellum JM, et al. Laparoscopic mesh hiatoplasty for paraesophageal hernias and fundoplications. Surg Endosc. (2006) 20(3):362–6. doi: 10.1007/s00464-005-0357-5
17. Oelschlager BK, Pellegrini CA, Hunter J, Soper N, Brunt M, Sheppard B, et al. Biologic prosthesis reduces recurrence after laparoscopic paraesophageal hernia repair—a multicenter, prospective, randomized trial. Ann Surg. (2006) 244(4):481–90. doi: 10.1097/01.sla.0000237759.42831.03
18. Braghetto I, Korn O, Csendes A, Burdiles P, Valladares H, Brunet L. Postoperative results after laparoscopic approach for treatment of large hiatal hernias: is mesh always needed? Is the addition of an antireflux procedure necessary? Int Surg. (2010) 95(1):80–7. PMID: 20480847
19. Analatos A, Håkanson BS, Lundell L, Lindblad M, Thorell A. Tension-free mesh versus suture-alone cruroplasty in antireflux surgery: a randomized, double-blind clinical trial. Br J Surg. (2020) 107(13):1731–40. doi: 10.1002/bjs.11917
20. Antoniou SA, Antoniou GA, Koch OO, Pointner R, Granderath FA. Lower recurrence rates after mesh-reinforced versus simple hiatal hernia repair: a meta-analysis of randomized trials. Surg Laparosc Endosc Percutan Tech. (2012) 22(6):498–502. doi: 10.1097/SLE.0b013e3182747ac2
21. Frantzides CT, Madan AK, Carlson MA, Stavropoulos GP. A prospective, randomized trial of laparoscopic polytetrafluoroethylene (PTFE) patch repair vs simple cruroplasty for large hiatal hernia. Arch Surg. (2002) 137(6):649–52. doi: 10.1001/archsurg.137.6.649
22. Memon MA, Memon B, Yunus RM, Khan S. Suture cruroplasty versus prosthetic hiatal herniorrhaphy for large hiatal hernia: a meta-analysis and systematic review of randomized controlled trials. Ann Surg. (2016) 263(2):258–66. doi: 10.1097/SLA.0000000000001267
23. Petric J, Bright T, Liu DS, Wee Yun M, Watson DI. Sutured versus mesh-augmented hiatus hernia repair: a systematic review and meta-analysis of randomized controlled trials. Ann Surg. (2022) 275(1):e45–51. doi: 10.1097/SLA.0000000000004902
24. Smith GS, Isaacson JR, Draganic BD, Baladas HG, Falk GL. Symptomatic and radiological follow-up after para-esophageal hernia repair. Dis Esophagus. (2004) 17(4):279–84. doi: 10.1111/j.1442-2050.2004.00426.x
25. Kim J, Hiura GT, Oelsner EC, Yin X, Barr RG, Smith BM, et al. Hiatal hernia prevalence and natural history on non-contrast CT in the multi-ethnic study of atherosclerosis (MESA). BMJ Open Gastroenterol. (2021) 8(1):1–9. doi: 10.1136/bmjgast-2020-000565
26. Watson DI, Thompson SK, Devitt PG, Smith L, Woods SD, Aly A, et al. Laparoscopic repair of very large hiatus hernia with sutures versus absorbable mesh versus nonabsorbable mesh a randomized controlled trial. Ann Surg. (2015) 261(2):282–9. doi: 10.1097/SLA.0000000000000842
27. Alicuben ET, Worrell SG, DeMeester SR. Impact of crural relaxing incisions, Collis gastroplasty, and non-cross-linked human dermal mesh crural reinforcement on early hiatal hernia recurrence rates. J Am Coll Surg. (2014) 219(5):988–92. doi: 10.1016/j.jamcollsurg.2014.07.937
28. Greene CL, DeMeester SR, Zehetner J, Worrell SG, Oh DS, Hagen JA. Diaphragmatic relaxing incisions during laparoscopic paraesophageal hernia repair. Surg Endosc. (2013) 27(12):4532–8. doi: 10.1007/s00464-013-3107-0
29. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. (2004) 240(2):205–13. doi: 10.1097/01.sla.0000133083.54934.ae
30. Slankamenac K, Nederlof N, Pessaux P, de Jonge J, Wijnhoven BP, Breitenstein S, et al. The comprehensive complication index: a novel and more sensitive endpoint for assessing outcome and reducing sample size in randomized controlled trials. Ann Surg. (2014) 260(5):757–62; discussion 762–3. doi: 10.1097/SLA.0000000000000948
31. Analatos A, Lindblad M, Ansorge C, Lundell L, Thorell A, Håkanson BS. Total versus partial posterior fundoplication in the surgical repair of para-oesophageal hernias: randomized clinical trial. BJS Open. (2022) 6(3):1–9. doi: 10.1093/bjsopen/zrac034
Keywords: paraesophageal hernia, crural repair, hernia recurrence, diaphragmatic relaxing incision, GERD, obstructive symptoms, quality of life
Citation: Tsoposidis A, Thorell A, Axelsson H, Reuterwall Hansson M, Lundell L, Wallenius V, Kostic S and Håkanson B (2023) The value of “diaphragmatic relaxing incision” for the durability of the crural repair in patients with paraesophageal hernia: a double blind randomized clinical trial. Front. Surg. 10:1265370. doi: 10.3389/fsurg.2023.1265370
Received: 22 July 2023; Accepted: 9 October 2023;
Published: 10 November 2023.
Edited by:
Peter C. Ambe, Witten/Herdecke University, GermanyReviewed by:
Italo Braghetto, University of Chile, ChileOwen Korn, University of Chile Clinical Hospital, Chile
© 2023 Tsoposidis, Thorell, Axelsson, Retuerwall Hansson, Lundell, Wallenius, Kostic and Håkanson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: M. Reuterwall Hansson bWFyY3VzLnJldXRlcndhbGwuaGFuc3NvbkBlcnN0YWRpYWtvbmkuc2U=
†ORCID M. Reuterwall Hansson orcid.org./0000-0002-4424-8847