
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 16 March 2023
Sec. Neurosurgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1152316
This article is part of the Research Topic Surgical Treatment Of Spinal Infections: Management of Spondylodiscitis and Implant-Associated Vertebral Osteomyelitis View all 9 articles
 Maximilian Schwendner1,2
Maximilian Schwendner1,2 Raimunde Liang1
Raimunde Liang1 Vicki M. Butenschön1
Vicki M. Butenschön1 Bernhard Meyer1
Bernhard Meyer1 Sebastian Ille1,2
Sebastian Ille1,2 Sandro M. Krieg1,2*
Sandro M. Krieg1,2*
Objective: Treatment strategies of patients suffering from pyogenic spondylodiscitis are a controverse topic. Percutaneous dorsal instrumentation followed by surgical debridement and fusion of the infectious vertebral disc spaces is a common approach for surgical treatment. Technical advances enable spinal navigation for dorsal and lateral instrumentation. This report investigates combined navigated dorsal and lateral instrumentation in a single surgery and positioning for lumbar spondylodiscitis in a pilot series.
Methods: Patients diagnosed with 1- or 2-level discitis were prospectively enrolled. To enable posterior navigated pedicle screw placement and lateral interbody fusion (LLIF) patients were positioned semi-prone in 45-degree fashion. For spinal referencing, a registration array was attached to the pelvic or spinal process. 3D scans were acquired intraoperatively for registration and implant control.
Results: 27 patients suffering from 1- or 2-level spondylodiscitis with a median ASA of 3 (1–4) and a mean BMI of 27.9 ± 4.9 kg/m2 were included. Mean duration of surgery was 146 ± 49 min. Mean blood loss was 367 ± 307 ml. A median of 4 (4–8) pedicle screws were placed for dorsal percutaneous instrumentation with an intraoperative revision rate of 4.0%. LLIF was performed on 31 levels with an intraoperative cage revision rate of 9.7%.
Conclusions: Navigated lumbar dorsal and lateral instrumentation in a single operation and positioning is feasible and safe. It enables rapid 360-degree instrumentation in these critically ill patients and potentially reduces overall intraoperative radiation exposure for patient and staff. Compared to purely dorsal approaches it allows for optimal discectomy and fusion while overall incisions and wound size are minimized. Compared to prone LLIF procedures, semi-prone in 45-degree positioning allows for a steep learning curve due to minor changes of familiar anatomy.
Pyogenic spondylodiscitis (PS) is a potentially life-threatening bacterial infection, that represents 3%–5% of all cases of osteomyelitis (1, 2). Incidence rates in Europe are reported ranging from 0.4 to 5.8 /100,000 persons every year, while data from the German Federal Statistical Office reported rates above 10/100,000 persons every year (1–3). Magnetic resonance imaging (MRI) remains the most important method of imaging for spondylodiscitis, while new imaging methods such as 18F-fluorodeoxiglucose positron emission tomography (FDG-PET) are frequently used in patients with contraindications for MRI, for the differentiation between spondylodiscitis and severe degenerative changes as well as to exclude metastatic infections (4–6).
Treatment strategies regarding PS vary widely. The primary indications for surgery include progressive neurological impairment, epidural abscess, pain caused by spinal instability, progressive deformity, or failure to respond to conservative treatment (7–10). However, in the last years there is an increasing trend towards surgical treatment of newly diagnosed PS as an initial treatment strategy due to early mobilization and reduced medical complications (11). Minimally invasive surgery (MIS) including percutaneous pedicle screw placement was shown to provide superior surgical outcomes such as significantly shorter durations of surgery, a lower perioperative need for blood products and a shorter hospital stays for multiple indications including pyogenic spondylodiscitis, traumatic fractures and spinal metastases (12–14).
At our institution surgical treatment of PS of the thoracolumbar spine is mostly performed via dorsal instrumentation by percutaneous pedicle screw placement and debridement of the disc space and cage placement via lateral lumbar interbody fusion (LLIF) in a second surgery. A surgical approach to perform dorsal and lateral instrumentation in one single positioning surgery under fluoroscopic control was reported by Drazin et al. in 2015 in cohort of patients with degenerative spinal disease (15).
With this study we report our initial experience with a combined navigated 360-degree instrumentation by dorsal percutaneous pedicle screw placement and LLIF procedure in a semi-prone 45-degree position. Clinical and radiological outcome of patients diagnosed with single or two-level spondylodiscitis of the lumbar spine treated are analyzed.
Our hypothesis is that combined 360-degree instrumentation by dorsal percutaneous pedicle screw placement and debridement of the intervertebral disc space and cage placement via LLIF performed in a single positioning under guidance of spinal navigation offers a safe and accurate treatment strategy for the surgical treatment of patients suffering from PS of the lumbar spine. Due to the quick and straightforward procedure including extensive discectomy, multimorbid PS patients can be treated safe and without recurrence.
The study was approved by the local ethics board (registration number: 2022-22_1-S-KH). We performed the study in accordance with the Declaration of Helsinki and in accordance to the STROBE statement.
Patients diagnosed with single- or two-level PS of the lumbar spine who were surgically treated by a combined navigated lumbar 360-degree instrumentation in a single positioning at our institution. between June 2021 and October 2022 were prospectively enrolled. Subsequently, patients undergoing conservative treatment or instrumentation in a staged approached were excluded. Perioperative complications as well as the clinical and radiographic outcome were further analyzed.
All patients underwent preoperative MRI and CT-imaging to diagnose PS. Indication for surgery was an infectious alteration of the intervertebral discs and anterior longitudinal ligament combined with a bony destruction of the adjacent vertebral body endplates. Patients suffering from low-back pain, sciatica or neurological deficits were scheduled for surgical treatment.
For spinal navigation, a mobile navigation system (Medtronic Stealth™ S7, Medtronic, Minneapolis, Minnesota, USA) or operating room-installed ceiling-mounted navigation system (Curve, Brainlab, Munich, Germany) was used in all cases. For the registration of the spinal navigation system, an intraoperative 3D-imaging scan using a mobile cone-beam computed tomography scanner (CT) (O-arm II, Medtronic, Minneapolis, Minnesota, USA) or operating room-installed CT (Brilliance CT Big Bore, Philips, Amsterdam, Netherlands) covering all planned vertebral bodies was performed accordingly. For referencing during surgery, a registration array equipped with reflective sphere markers was attached to a pelvic or spinal process.
The patient was positioned semi-prone in a 45-degree right-sided positioning on the operation table during the whole procedure (Figure 1). For referencing during surgery, a registration array was attached to a pelvic or spinal process. For the registration of the navigation system, an intraoperative 3D-imaging scan covering all planned vertebral bodies was performed. The first surgical step was bilateral dorsal instrumentation by navigated percutaneous pedicle screw placement (CD Horizon Solera, Medtronic, Minneapolis, Minnesota, USA) (Figure 1) using a navigated drill-guide and Kirschner wires. Starting the procedure with pedicle screw placement is crucial for an optimal accuracy of the spinal navigation. Next, lateral instrumentation was performed using a left-sided retroperitoneal approach by a tubular retractor (Clydesdale Spinal System, Medtronic, Minneapolis, Minnesota, USA) (Figure 1). In terms of total navigation, this procedure was performed under guidance of the spinal navigation as well, allowing for constant image referencing during all surgical steps (skin incision, preparation, implant placement). For planning of the skin incision and surgical preparation a navigated pointer was used. The infectious vertebral discs were resected using a navigated chisel, and anterior decompression was performed in case of spinal canal stenosis. Titanium cages (Juliet LL, Spineart, Plan-Les-Ouates, Switzerland) prepared with topic gentamicin or vancomycin were implanted into the disc spaces. Positioning was reviewed using the navigated pointer. After completing cage placement, a second intraoperative 3D imaging set including updated spinal navigation was performed for implant control. In case of implant revision, a second control scan was acquired. Afterwards, rods were implanted bilaterally and a stepwise wound closure was performed.
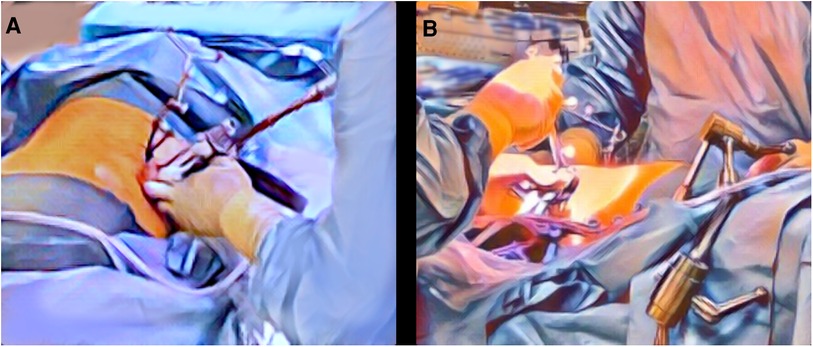
Figure 1. Patient positioning and setup. The patient is positioned semi-prone in a 45-degree right-sided positioning to enable sufficient surgical access for both surgical steps—navigated pedicle screw placement (A) and lateral discectomy and fusion (B). For referencing during surgery, a registration array is attached to a pelvic or spinal process. The surgical sites for pedicle screw placement (A) and lateral interbody fusion (B) are illustrated.
For radiographic analysis, intraoperative 3D-imaging and postoperative imaging was analyzed. Pedicle screw positioning was evaluated on intraoperative 3D-scans according to the Gertzbein and Robbins scale (GRS) (16). Cage placement was evaluated in relation to the center of the intervertebral disc space and limits of the upper and lower endplate of the adjacent vertebral bodies (Figure 2).
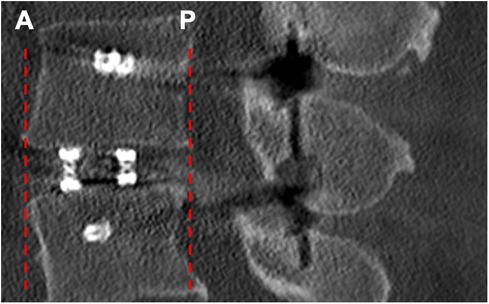
Figure 2. Radiographic evaluation of cage placement. Figure 2 shows an intraoperative CT-scan after 360-degree instrumentation of the lumbar spine in a sagittal view. Cage placement was evaluated in anterior (A) and posterior (P) orientation in relation to the limits of the upper and lower endplate of the adjacent vertebrae.
Statistical analyses were performed using Prism (version 9.1.1, GraphPad Software, La Jolla, CA, USA). Descriptive statistics including mean, median, minimum, maximum, and standard deviation were calculated for patient characteristics as well as radiographic measurements. For statistical testing between groups, Mann–Whitney U tests for unpaired samples as well as Fisher's exact tests with a level of significance set at p < 0.05 were performed. Figures were created using Prism (version 9.1.1, GraphPad Software, La Jolla, CA, USA).
A consecutive series of 27 patients (8 women, 19 men) with 32 levels of spondylodiscitis of the lumbar spine was analyzed (Table 1). All patients underwent 360-degree instrumentation of the lumbar spine in a single surgery. No access surgeon was used. Mean age was 68.5 ± 13.7 (31.9–86.4) years, with 20 patients (74.1%) aged 65 years or above. Mean BMI was 27.9 ± 4.9 (21.3–38.7) and the median ASA-PS (American Society of Anaesthesiologists physical status) class was 3 (1–4) (Table 1). One patient showed a hip flexor weakness preoperatively due to a psoas abscess, while all other patients showed no sensory or motor deficit related to the spinal infection.
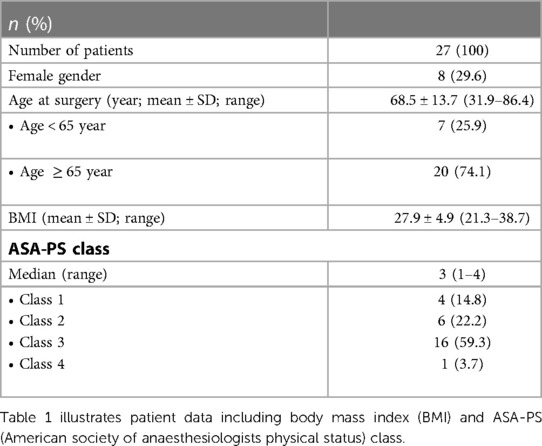
Table 1. Patient data.
Duration of surgery was 146 ± 49 min (69–233) minutes (Figure 3). Estimated intraoperative blood loss was 367 ± 307 (50–1300) ml.
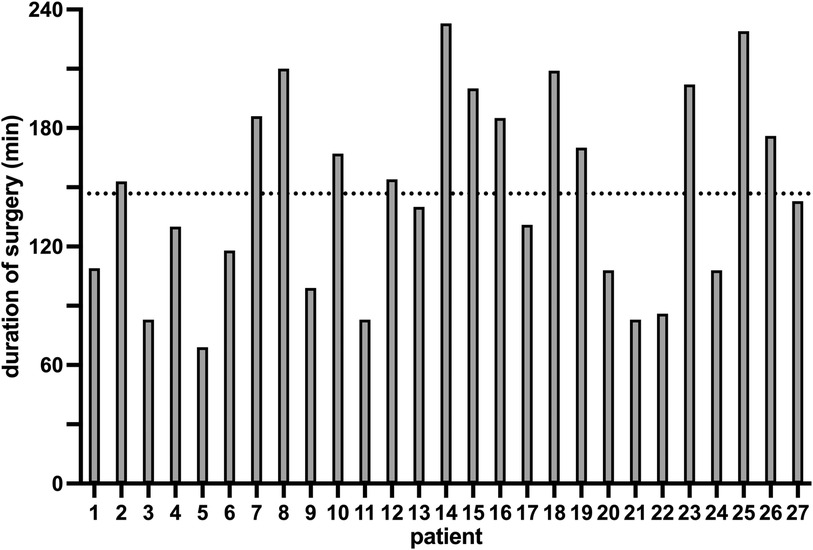
Figure 3. Duration of surgery. The duration of surgery of all 27 patients with an average duration of 147 min (ticked line), a minimum duration of 69 min (patient 5) and a maximum duration of 233 min (patient 14) is illustrated in this figure.
Regarding dorsal instrumentation, 124 screws were implanted in total. In 20 patients, single segment instrumentation was performed, while in five (18.5%) patients two segments and in two (7.4%) patients three segments were instrumented (Table 2). Overall, five (4.0%) pedicle screws were revised in two patients, in one case an intraoperative revision of two screws and a postoperative revision of another screw was performed.
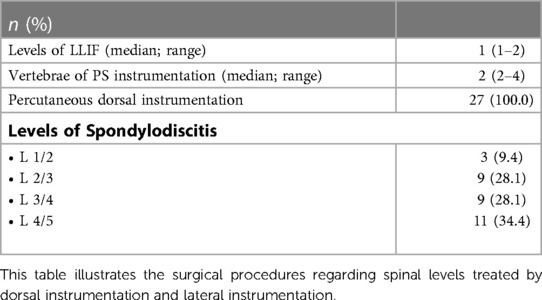
Table 2. Surgical data.
Regarding lateral instrumentation, 30 cages including one expandable cage due to severe end plate osteolysis (Obelisc, Ulrich Medical, Ulm, Germany) were implanted. Intraoperative cage revision was performed in three cases, and in two cases the cage was further inserted in the intervertebral disc space after the control scan. In one case no cage was implanted as reduced height of the intervertebral disc space did not allow for cage placement.
Pedicle screw placement was reviewed on initial intraoperative imaging instrumentation according to GRS. Screw positioning rated GRS A and B was achieved in 111 screws (89.5%) (Figure 4).

Figure 4. Accuracy of pedicle screw placement. Figure 4 illustrates the accuracy of pedicle screw placement regarding the radiographic evaluation according to the Gertzbein and Robbins scale (GRS) and revision rates of the pedicle screws.
Regarding cage placement in sagittal plane—cages showed contact to the anterior border of the upper and lower endplates of the adjacent vertebral bodies in nine (30.0%) cases with the cage exceeding the endplates in two cases (6.7%), and contact to the posterior border in two (6.7%) cases (Figure 2).
All patients were treated with intravenous antibiotics for a minimum of 14 d, followed by 10 weeks of oral antibiosis. Treatment schemes were individually adapted and discussed during interdisciplinary ward rounds lead by the department of microbiology. Three patients (11.1%) required ICU treatment, with a mean ICU stay of 13.3 (3–28) days. Mean hospital stay was 18.5 ± 12.2 (4–64) days, and 11 patients were referred to a secondary care hospital for further intravenous antibiosis and rehabilitation.
Regarding surgery-related neurological deficits persisting at the time of discharge one patient showed postoperative deterioration of motor function related to an intraoperative nerve-root injury. Atrophic wound healing disorders requiring local surgical wound revision occurred in five cases (18.5%) with one patient aged under 65 years (14.2%) and four patients (20%) over 65 years.
Follow-up examinations were available on 25 patients on 129 ± 111 (22–484) d postoperatively. One patient had to undergo a second surgery due to ongoing bony destruction of the vertebral body leading to cage subsidence requiring a complete vertebral body replacement using an expandable cage. Two multimorbid patients died due to cardiac complications induced by the systemic infection. Another patient suffered a severe acute respiratory syndrome coronavirus 2-infection four weeks postoperatively and was subsequently treated with best supportive care due to multiple comorbidities and advanced age. Two patients had to be re-hospitalized due to persistent infection parameters in blood testing. Further diagnostics ruled out persistent spondylodiscitis—both patients were effectively treated by a prolongated scheme of intravenous antibiotics followed by oral antibiosis. All six patients younger than 65 years with follow-up data available showed regular healing.
Treatment strategies regarding PS vary widely amongst centers worldwide. However, in the last years there is an increasing trend towards surgical treatment of newly diagnosed spondylodiscitis as an initial treatment strategy (17–19). Regarding surgical treatment strategies of PS of the thoracolumbar spine, dorsal percutaneous pedicle screw instrumentation with additional surgical debridement of the intervertebral disc space via posterior discectomy or LLIF including cage implantation has been proven to show most favorable outcomes, especially regarding long-term fusion rates (17, 20–22). For the choice of implants, titanium implants should be favored over polyetheretherketone (PEEK) as higher rates of implant loosening were reported for PEEK in patients treated for spondylodiscitis (22–24). A significant rate of postoperative wound healing disorders of 18.5%, which was similar in patients below and over the age of 65 years, was observed in this study. In previous studies, rates of wound healing disorders greatly vary between 2.4% and 12.3% (20, 22). The definition of a wound healing disorder might vary between studies—in this study all patients requiring surgical revision under general and local anesthesia were considered.
Most patients diagnosed with PS are of higher age and suffer multiple comorbidities. Therefore, the total duration of surgery and blood loss should be kept as low as possible, intraoperative stress minimized and early mobilization and rehabilitation should be facilitated. A study by Tong et al. in 2019 successfully combined dorsal and lateral instrumentation in a single surgery with an intraoperative switch from prone positioning to lateral positioning in patients with single-level PS (25). In terms of intraoperative patient positioning in general, the conventional prone position bears the risk of cardiovascular complications including cardiac arrest as well as the risk of hypovolemia, reduced pulmonary compliance, and postoperative vision loss (26, 27). A lateral positioning helps to partially reduce these complications. Furthermore, combining lateral and dorsal instrumentation in one single positioning helps to reduce the overall time of the patient under general anesthesia, especially when compared to two separate surgeries but also compared to two patient positionings in one surgery (28). A large meta-analysis published by Mills et al. in 2021 compared single position lumbar fusion surgery in both lateral and prone positioning for patients with lumbar degenerative disease, spondylolisthesis, or radiculopathy to surgery in a staged approach, demonstrating overall significantly reduced durations of surgery and a reduced length of hospitalization (29). Nevertheless, higher complication rates regarding pedicle screw placement in a lateral positioning were reported for this approach (29).
Navigated pedicle screw placement has been proven to be advantageous over conventional screw placement, especially when performing percutaneous transmuscular instrumentation (30, 31). Though, applying spinal navigation has proved to be advantageous also in lateral instrumentation in terms of constant image referencing during all surgical steps (skin incision, preparation, implant placement) and for minimizing radiation exposure to the staff. In patients with PS, debridement of the disc space and cage placement is performed to reduce bacterial load quickly and to facilitate fusion without the intention to perform major corrections by multi-level instrumentation. Otherwise, the accuracy of spinal navigation might be impaired during cage placement.
When applying spinal navigation for both—dorsal and lateral instrumentation—another registration scan is warranted when repositioning the patient. Sellin et al. applied CT-guided navigation for simultaneous lateral interbody fusion and pedicle screw placement in lateral positioning showing reduced radiation exposure and reduced duration of surgery, especially as intraoperative navigation replaced intraoperative fluoroscopy and therefore allowed the parallel execution of both procedures (32). Ikuma et al. compared single-positioning surgery in a right lateral decubitus positioning for cases with and without spinal navigation, showing a significantly reduced duration of surgery for cases with spinal navigation as spinal navigation partially enabled simultaneous anterior and posterior instrumentation (33).
Regarding the application of robot-assisted navigated pedicle screw placement for 360-degree surgeries in a single positioning, Sinkov et al. reported limitations regarding contralateral pedicle screw placement due to problems accessing the surgical site in lateral decubitus positioning (34).
In our study, patients were positioned semi-prone in a 45-degree right-sided positioning on the operation table during the whole procedure (Figure 1). Compared to conventional 90°-lateral decubitus positioning, the accessibility of the surgical site especially for pedicle screw placement is improved. Dorsal and lateral instrumentation were performed under spinal navigation to enable continuous 3D visualization during all surgical steps, which helps to adapt to the modified patient positioning. In our experience, semi-prone 45-degree positioning allows for a steep learning curve due to minor changes of familiar anatomy, especially compared to prone LLIF and procedures like pedicle screw placement in a lateral decubitus position. When compared to purely dorsal approaches, this combined surgical approach allows for optimal discectomy and fusion. In addition, overall incisions and wound sizes are minimized by MIS, as percutaneous pedicle screw placement can be performed without the necessity of additional dorsal decompression. The spinal canal remains untouched.
Regarding the accuracy of pedicle screw placement in our study, two patients (7.4%) were reported with pedicle screw revision in this study, resulting in a total screw revision rate of 4.0%, which is comparable to previous studies in patient positioning in prone position (35, 36).
This study was performed as a pilot study to confirm the feasibility and safety of this surgical approach. Therefore, no control group was included. In this study, patients with single or two-level PS of the lumbar spine were treated. In more extensive cases of PS including patients requiring multi-level instrumentation or instrumentation of the middle and upper thoracic spine a staged approach should be favored. When applying a modified patient positioning, the potential time benefit should be weighed against potential limitations and impairments regarding the surgical field and safety. In all cases in this study, dorsal instrumentation was performed via percutaneous pedicle screw placement.
Navigated lumbar dorsal and lateral instrumentation in a single operation and 45-degree positioning is feasible and safe. It enables rapid 360-degree instrumentation in these critically ill patients and potentially reduces overall intraoperative radiation exposure for patient and staff. Compared to purely dorsal approaches it allows for optimal discectomy and fusion while overall incisions and wound size are minimized. Compared to prone LLIF procedures, semi-prone in 45-degree positioning allows for a steep learning curve due to minor changes of familiar anatomy.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by The study was approved by the local ethics board (registration number: 2022-22_1-S-KH). We performed the study in accordance with the Declaration of Helsinki and in accordance to the STROBE statement. Ethikkommission der Technischen Universität München Grillparzerstraße 16, 3. Stock, Raum 3.46 81,675 MünchenZXRoaWtrb21taXNzaW9uQG1yaS50dW0uZGU=. The patients/participants provided their written informed consent to participate in this study.
MS, RL, VB, BM, SI and SK: designed the study. MS, RL, VB, SI, BM, and SK: coordinated subject inclusion, data handling, and data storage. MS and RL: were responsible for data analysis and performed statistics. MS, VB, SI and SK: were involved in literature research. MS, RL, VB, BM, SI and SK: drafted the manuscript. The study was supervised by BM, SI, and SK. All authors contributed to the article and approved the submitted version..
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors. This trial was funded entirely by institutional grants from the Department of Neurosurgery, Technical University of Munich, Germany, School of Medicine, Klinikum rechts der Isar.
BM received honoraria, consulting fees, and research grants from Medtronic (Meerbusch, Germany), Icotec AG (Altstätten, Switzerland), and Relievant Medsystems Inc., (Sunnyvale, CA, USA); honoraria and research grants from Ulrich Medical (Ulm, Germany); honoraria and consulting fees from Spineart Deutschland GmbH (Frankfurt, Germany) and DePuy Synthes (West Chester, PA, USA); royalties from Spineart Deutschland GmbH (Frankfurt, Germany) and is a consultant for Medacta International (Castel San Pietro, Switzerland). SK is a consultant for Ulrich Medical (Ulm, Germany) and Need Inc. (Santa Monica, CA, USA). He received honoraria from Nexstim Plc (Helsinki, Finland), Spineart Deutschland GmbH (Frankfurt, Germany), Medtronic (Meerbusch, Germany), and Carl Zeiss Meditec (Oberkochen, Germany). SK, SI, VB and BM received research grants, and are consultants for Brainlab AG (Munich, Germany). However, all authors declare that they have no conflict of interest regarding the materials used or the results presented in this study.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ASA-PS, American society of anaesthesiologists physical status; CT, computed tomography scanner; FDG-PET, 18F-fluorodeoxiglucose positron emission tomography; GRS, Gertzbein and Robbins scale; LLIF, lateral lumbar interbody fusion; MRI, magnetic resonance imaging; PEEK, polyetheretherketone; PS, pyogenic spondylodiscitis; MIS, minimal invasive surgery.
1. Fantoni M, Trecarichi EM, Rossi B, Mazzotta V, Di Giacomo G, Nasto LA, et al. Epidemiological and clinical features of pyogenic spondylodiscitis. Eur Rev Med Pharmacol Sci. (2012) 16(Suppl 2):2–7.22655478
2. Herren C, Jung N, Pishnamaz M, Breuninger M, Siewe J, Sobottke R. Spondylodiscitis: diagnosis and treatment options. Dtsch Arztebl Int. (2017) 114(51–52):875–82. doi: 10.3238/arztebl.2017.0875
3. des Bundes G. Diagnosedaten der Krankenhäuser ab 2000. Available at: www gbe-bund de/078 068 083. 2017;3(0.78):0.41.
4. Modic MT, Feiglin DH, Piraino DW, Boumphrey F, Weinstein MA, Duchesneau PM, et al. Vertebral osteomyelitis: assessment using MR. Radiology. (1985) 157(1):157–66. doi: 10.1148/radiology.157.1.3875878
5. Salaffi F, Ceccarelli L, Carotti M, Di Carlo M, Polonara G, Facchini G, et al. Differentiation between infectious spondylodiscitis versus inflammatory or degenerative spinal changes: how can magnetic resonance imaging help the clinician? Radiol Med. (2021) 126(6):843–59. doi: 10.1007/s11547-021-01347-7
6. Smids C, Kouijzer IJ, Vos FJ, Sprong T, Hosman AJ, de Rooy JW, et al. A comparison of the diagnostic value of MRI and (18)F-FDG-PET/CT in suspected spondylodiscitis. Infection. (2017) 45(1):41–9. doi: 10.1007/s15010-016-0914-y
7. Duarte RM, Vaccaro AR. Spinal infection: state of the art and management algorithm. Eur Spine J. (2013) 22(12):2787–99. doi: 10.1007/s00586-013-2850-1
8. Ryang YM, Akbar M. Pyogenic spondylodiscitis: symptoms, diagnostics and therapeutic strategies. Orthopade. (2020) 49(8):691–701. doi: 10.1007/s00132-020-03945-1
9. Tsantes AG, Papadopoulos DV, Vrioni G, Sioutis S, Sapkas G, Benzakour A, et al. Spinal infections: an update. Microorganisms. (2020) 8(4). doi: 10.3390/microorganisms8040476
10. Gregori F, Grasso G, Iaiani G, Marotta N, Torregrossa F, Landi A. Treatment algorithm for spontaneous spinal infections: a review of the literature. J Craniovertebr Junction Spine. (2019) 10(1):3–9. doi: 10.4103/jcvjs.JCVJS_115_18
11. Segreto FA, Beyer GA, Grieco P, Horn SR, Bortz CA, Jalai CM, et al. Vertebral osteomyelitis: a comparison of associated outcomes in early versus delayed surgical treatment. Int J Spine Surg. (2018) 12(6):703–12. doi: 10.14444/5088
12. Viezens L, Schaefer C, Helmers R, Vettorazzi E, Schroeder M, Hansen-Algenstaedt N. Spontaneous pyogenic spondylodiscitis in the thoracic or lumbar spine: a retrospective cohort study comparing the safety and efficacy of minimally invasive and open surgery over a nine-year period. World Neurosurg. (2017) 102:18–27. doi: 10.1016/j.wneu.2017.02.129
13. Perna A, Smakaj A, Vitiello R, Velluto C, Proietti L, Tamburrelli FC, et al. Posterior percutaneous pedicle screws fixation versus open surgical instrumented fusion for thoraco-lumbar spinal metastases palliative management: a systematic review and meta-analysis. Front Oncol. (2022) 12:884928. doi: 10.3389/fonc.2022.884928
14. Phan K, Rao PJ, Mobbs RJ. Percutaneous versus open pedicle screw fixation for treatment of thoracolumbar fractures: systematic review and meta-analysis of comparative studies. Clin Neurol Neurosurg. (2015) 135:85–92. doi: 10.1016/j.clineuro.2015.05.016
15. Drazin D, Kim TT, Johnson JP. Simultaneous lateral interbody fusion and posterior percutaneous instrumentation: early experience and technical considerations. Biomed Res Int. (2015) 2015:458284. doi: 10.1155/2015/458284
16. Gertzbein SD, Robbins SE. Accuracy of pedicular screw placement in vivo. Spine. (1990) 15(1):11–4. doi: 10.1097/00007632-199001000-00004
17. Shiban E, Janssen I, Wostrack M, Krieg SM, Ringel F, Meyer B, et al. A retrospective study of 113 consecutive cases of surgically treated spondylodiscitis patients. A single-center experience. Acta Neurochir. (2014) 156(6):1189–96. doi: 10.1007/s00701-014-2058-0
18. Pluemer J, Freyvert Y, Pratt N, Robinson JE, Cooke JA, Tataryn ZL, et al. An assessment of the safety of surgery and hardware placement in de-novo spinal infections. A systematic review and meta-analysis of the literature. Global Spine J. (2022):21925682221145603. doi: 10.1177/21925682221145603 [Online ahead of print]36510352
19. Behmanesh B, Gessler F, Duetzmann S, Seifert V, Weise L, Setzer M. Quality of life following surgical and conservative therapy of pyogenic spinal infection: a study of long-term outcome in 210 patients. J Neurol Surg A Cent Eur Neurosurg. (2023) 84(1):14–20. doi: 10.1055/s-0041-1722965.33690878
20. Sommer B, Babbe-Pekol T, Feulner J, Richter RH, Buchfelder M, Shiban E, et al. Long-term clinical and radiologic outcome following surgical treatment of lumbar spondylodiscitis: a retrospective bicenter study. J Neurol Surg A Cent Eur Neurosurg. (2023) 84(1):44–51. doi: 10.1055/s-0042-1748767
21. Schatlo B, Rohde V, Abboud T, Janssen I, Melich P, Meyer B, et al. The role of discectomy in reducing infectious complications after surgery for lumbar spondylodiscitis. J Neurol Surg A Cent Eur Neurosurg. (2023) 84(1):3–7. doi: 10.1055/a-1832-9092
22. Shiban E, Janssen I, da Cunha PR, Rainer J, Stoffel M, Lehmberg J, et al. Safety and efficacy of polyetheretherketone (PEEK) cages in combination with posterior pedicel screw fixation in pyogenic spinal infection. Acta Neurochir. (2016) 158(10):1851–7. doi: 10.1007/s00701-016-2924-z
23. Joerger AK, Shiban E, Krieg SM, Meyer B. Carbon-fiber reinforced PEEK instrumentation for spondylodiscitis: a single center experience on safety and efficacy. Sci Rep. (2021) 11(1):2414. doi: 10.1038/s41598-021-81960-8
24. Burkhardt BW, Bullinger Y, Mueller SJ, Oertel JM. The surgical treatment of pyogenic spondylodiscitis using carbon-fiber-reinforced polyether ether ketone implants: personal experience of a series of 81 consecutive patients. World Neurosurg. (2021) 151:e495–506. doi: 10.1016/j.wneu.2021.04.064
25. Tong YJ, Liu JH, Fan SW, Zhao FD. One-stage debridement via oblique lateral interbody fusion corridor combined with posterior pedicle screw fixation in treating spontaneous lumbar infectious spondylodiscitis: a case series. Orthop Surg. (2019) 11(6):1109–19. doi: 10.1111/os.12562
26. Kwee MM, Ho YH, Rozen WM. The prone position during surgery and its complications: a systematic review and evidence-based guidelines. Int Surg. (2015) 100(2):292–303. doi: 10.9738/INTSURG-D-13-00256.1
27. Staartjes VE, Schillevoort SA, Blum PG, van Tintelen JP, Kok WE, Schroder ML. Cardiac arrest during spine surgery in the prone position: case report and review of the literature. World Neurosurg. (2018) 115:460–7.e1. doi: 10.1016/j.wneu.2018.04.116
28. Guiroy A, Carazzo C, Camino-Willhuber G, Gagliardi M, Fernandes-Joaquim A, Cabrera JP, et al. Single-position surgery versus lateral-then-prone-position circumferential lumbar interbody fusion: a systematic literature review. World Neurosurg. (2021) 151:e379–e86. doi: 10.1016/j.wneu.2021.04.039
29. Mills ES, Treloar J, Idowu O, Shelby T, Alluri RK, Hah RJ. Single position lumbar fusion: a systematic review and meta-analysis. Spine J. (2022) 22(3):429–43. doi: 10.1016/j.spinee.2021.10.012
30. Fichtner J, Hofmann N, Rienmuller A, Buchmann N, Gempt J, Kirschke JS, et al. Revision rate of misplaced pedicle screws of the thoracolumbar spine-comparison of three-dimensional fluoroscopy navigation with freehand placement: a systematic analysis and review of the literature. World Neurosurg. (2018) 109:e24–32. doi: 10.1016/j.wneu.2017.09.091
31. Shin BJ, James AR, Njoku IU, Hartl R. Pedicle screw navigation: a systematic review and meta-analysis of perforation risk for computer-navigated versus freehand insertion. J Neurosurg Spine. (2012) 17(2):113–22. doi: 10.3171/2012.5.SPINE11399
32. Sellin JN, Mayer RR, Hoffman M, Ropper AE. Simultaneous lateral interbody fusion and pedicle screws (SLIPS) with CT-guided navigation. Clin Neurol Neurosurg. (2018) 175:91–7. doi: 10.1016/j.clineuro.2018.10.013
33. Ikuma H, Hirose T, Takao S, Otsuka K, Kawasaki K. The usefulness and safety of the simultaneous parallel anterior and posterior combined lumbar spine surgery using intraoperative 3D fluoroscopy-based navigation (SPAPS). N Am Spine Soc J. (2021) 5:100047. doi: 10.1016/j.xnsj.2020.100047
34. Sinkov V, Lockey SD, Cunningham BW. Single position lateral lumbar interbody fusion with posterior instrumentation utilizing computer navigation and robotic assistance: retrospective case review and surgical technique considerations. Global Spine J. (2022) 12(2_suppl):75S–81S. doi: 10.1177/21925682221083909
35. Ille S, Baumgart L, Obermueller T, Meyer B, Krieg SM. Clinical efficiency of operating room-based sliding gantry CT as compared to mobile cone-beam CT-based navigated pedicle screw placement in 853 patients and 6733 screws. Eur Spine J. (2021) 30(12):3720–30. doi: 10.1007/s00586-021-06981-3
Keywords: one-stop shop, spinal navigation, lateral instrumentation, navigated pedicle screw placement, pyogenic spondylodiscitis
Citation: Schwendner M, Liang R, Butenschön VM, Meyer B, Ille S and Krieg SM (2023) The one-stop-shop approach: Navigating lumbar 360-degree instrumentation in a single position. Front. Surg. 10:1152316. doi: 10.3389/fsurg.2023.1152316
Received: 27 January 2023; Accepted: 27 February 2023;
Published: 16 March 2023.
Edited by:
Siegmund Lang, University Medical Center Regensburg, GermanyReviewed by:
Basem Ishak, Heidelberg University, Germany© 2023 Schwendner, Liang, Butenschön, Meyer, Ille and Krieg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sandro M. Krieg U2FuZHJvLktyaWVnQHR1bS5kZQ==
Specialty Section: This article was submitted to Neurosurgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.