
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Surg. , 13 June 2023
Sec. Visceral Surgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1142585
 Anas Taha1*†
Anas Taha1*† Stephanie Taha-Mehlitz2,†Niklas Ortlieb3Vincent Ochs1Michael Drew Honaker4Robert Rosenberg5Johan F. Lock6Martin Bolli2,‡
Stephanie Taha-Mehlitz2,†Niklas Ortlieb3Vincent Ochs1Michael Drew Honaker4Robert Rosenberg5Johan F. Lock6Martin Bolli2,‡ Philippe C. Cattin1,‡
Philippe C. Cattin1,‡
Background: Machine learning (ML) is an inquiry domain that aims to establish methodologies that leverage information to enhance performance of various applications. In the healthcare domain, the ML concept has gained prominence over the years. As a result, the adoption of ML algorithms has become expansive. The aim of this scoping review is to evaluate the application of ML in pancreatic surgery.
Methods: We integrated the preferred reporting items for systematic reviews and meta-analyses for scoping reviews. Articles that contained relevant data specializing in ML in pancreas surgery were included.
Results: A search of the following four databases PubMed, Cochrane, EMBASE, and IEEE and files adopted from Google and Google Scholar was 21. The main features of included studies revolved around the year of publication, the country, and the type of article. Additionally, all the included articles were published within January 2019 to May 2022.
Conclusion: The integration of ML in pancreas surgery has gained much attention in previous years. The outcomes derived from this study indicate an extensive literature gap on the topic despite efforts by various researchers. Hence, future studies exploring how pancreas surgeons can apply different learning algorithms to perform essential practices may ultimately improve patient outcomes.
Machine learning (ML) is an inquiry domain that aims to establish methodologies that leverage information to enhance performance on various applications. ML is an essential branch of artificial intelligence that helps in solving traditionally-complex challenges (1). In the healthcare domain, the ML concept has gained a lot of prominence over the years. The adoption of ML algorithms has become numerous. Qayyum et al. claimed that healthcare professionals could use ML in prognosis, diagnosis, treatment, and clinical workflows (2). Pancreatic surgery represents a field of surgery whose primary purpose is to resect malignant tumors in an effort to improve patient survival. Thus, the analysis of ML's contribution to pancreatic surgery is vital to understanding the algorithm's various benefits, shortcomings, and future expectations. The aim of the study is to provide additional information concerning the utilization of ML in pancreatic surgery, facilitating the development of more algorithms in the field.
Previous researchers in the field have found a positive association between the application of machine learning algorithms and success in pancreatic surgery. For example, Dalal et al. revealed that radiomics demonstrated promising outcomes in the diagnosis and prognosis of pancreatic cystic lesions (3). From a similar perspective, Zhou et al. indicated that ML-based approaches had a higher prediction capacity to the point of outperforming other conventional models used in predicting acute pancreatitis (4). Additional studies have shown that machine learning supported decision derivation in the personalized oversight of pancreatic cancer (5). Furthermore, Palumbo et al. established that ML algorithms was a significant prediction tool for probability of recurrence in pancreatic adenocarcinoma (6). This study offers a scoping review of the relevant publications in the field of pancreatic surgery to aid in developing sound conclusions.
The primary goal of this scoping review is to evaluate the application of ML in pancreatic surgery. The following objectives were adopted to fullfil this aim:
• Evaluating the current application of machine learning in pancreatic surgery
• Analyzing the benefits of integrating machine learning in pancreatic surgery.
• Examining the future of the application of machine learning in pancreatic surgery.
This study followed the Preferred Reporting Itens for Systematic Reviews and Meta-Analysis Extension for Scopic Reviews (PRISMA-ScR) guidelines (7). The technique has twenty compulsory features and two optional elements that are utilized in scoping reviews to ensure quality results. PRISMA-ScR was applied as it will allow assessment of the pros and cons of the study to take place. Also, the process will facilitate the duplication of review techniques used in future studies when analyzing the topic. More importantly, the PRISMA-ScR technique will ensure transparency and fairness in the current study (8, 9). According to Sarkis-Onofre et al., the process facilitates the amplification of the methods researchers use in their studies, airing the results and developing research strategies (10). As a result, the PRISMA-ScR principle assists in presenting the techniques used to acquire outcomes.
The relevancy of the study determined the type of eligibility criteria implemented articles published between 2019 and May 2022 containing relevant data specializing in ML in pancreas surgery and those with original study design undertaken on human participates were included This timeframe was used to guarantee gathering of recent, updated information concerning the application of ML in pancreas surgery. Articles specializing in other forms of surgery were excluded.
Choosing the suitable files for the research topic entailed performing a comprehensive literature scan of different databases and search engines. Databases utilized included PubMed, Cochrane, EMBASE, and IEEE, while search engines included Google and Google Scholar. We explicitly searched for articles printed from 2019 to 2022. The literature search was performed in May 2022. Two team members with experience in the techniques utilized took part in refining the adopted search strategies. An equal chance to voice opinions in a group discussion was undertaken. Subsequently, we evaluated the references of relevant journals to access different properties that were fit for inclusion. We also conducted a search of appropriate journals to add to the study, utilizing Google and Google Scholar search engines. The amalgamation of this approach endorsed a broad literature search, thereby ensuring the gathering of additional supporting information on the study topic.
The search strategy used in the study entailed keying in specific terms in the relevant search engines and databases. On the PubMed, Cochrane, EMBASE, and IEEE databases, the words used included “machine learning in pancreas surgery,” “benefits of machine learning in pancreas surgery,” “definition of machine learning,” and “disadvantages of machine learning in pancreas surgery.” Filters used on PubMed were “best match” and “2019 to 2022.” On Cochrane, we used the date filter to certify that the articles gathered were published from 2019 to 2022 and the trials filter to guarantee acquired publications were original studies. On EMBASE, the researchers integrated the “study type” and “publication year” filters to gather relevant documents used in the research. We used the “2019–2022” filter on IEEE to gather relevant documents. On Google and Google Scholar search engines, phrases used included “machine learning in pancreas surgery,” “benefits of machine learning in pancreas surgery,” and “definition of machine learning”. We did not incorporate any filters on Google, though, on Google Scholar, the filters incorporated included “2019 to 2022,” “sort by relevance,” and “any type.” A librarian was in charge of the oversight search method as well as enlisting the search strategy. The additional team members counter-checked the process to guarantee validity and reliability by implementing the Peer Review of Electronic Search Strategies (PRESS) checklist. According to Bramer et al., the PRESS agenda directs researchers to check the search strategies included in the study (11). As a result, this method enabled us to show that the foundations attained echoed a precise understanding of the research question.
Choosing sources of extracting evidence necessitated focusing on the screening process. All publications were screened to guarantee that they were complete scripts and had the necessary information to qualify for inclusion. We matched the abstracts and complete texts to make sure they fitted. We exluded cases of an included article lacking complete scripts as it would be challenging to establish reliable conclusions. Workload was reduced during screening by first assessing files from all platforms before the process.
We created a data charting form and outlined aspects to be observed when gathering information. The form emphasized elements such as ML in pancreas surgery.
Acquisition of information was based on various backgrounds of articles. For example, the papers addressed the medical field and emphasized spreading awareness of ML in pancreas surgery.
For this research, we arranged the journals according to their primary area of concentration. The identified category was ML in pancreas surgery.
We used the Measurement Tool to Assess Systematic Reviews (AMSTAR) technique to analyze the operational quality used in the incorporated studies that facilitated settlement of any disagreements among the authors. Moreover, the tool guarantees reliable satisfaction of different systematic reviews and randomized controlled treatment trials (12). Furthermore, there are eleven items in the tool the researcher should use to know the quality of the articles. The technique ensured the implemented studies fulfilled and met the needs of the criterion.
The search on the four databases adopted (PubMed, Cochrane, EMBASE, and IEEE) yielded 117 results. The number of files acquired from Google and Google Scholar was twenty. Out of the included articles, there were seventy-five duplicate documents. The screening process identified fifty-three articles eligible for inclusion. After seeking retrieval and assessing eligibility, only twenty-one articles were deemed appropriate for inclusion Figure 1. The main themes of the included studies revolved around ML integration in pancreas surgery. Most studies tested machine learning's prediction abilities in the sector (Table 1).
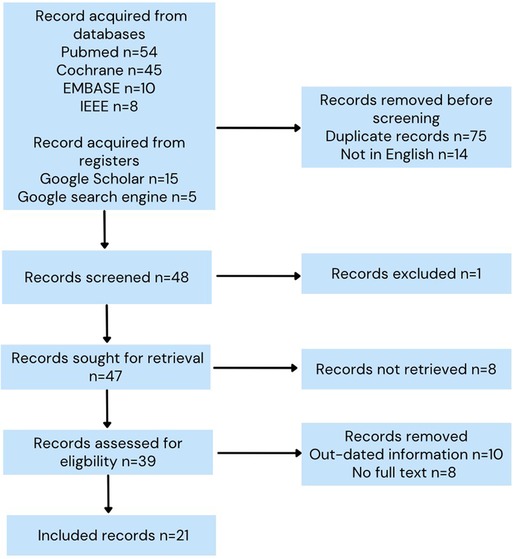
Figure 1. Prisma flowchart.
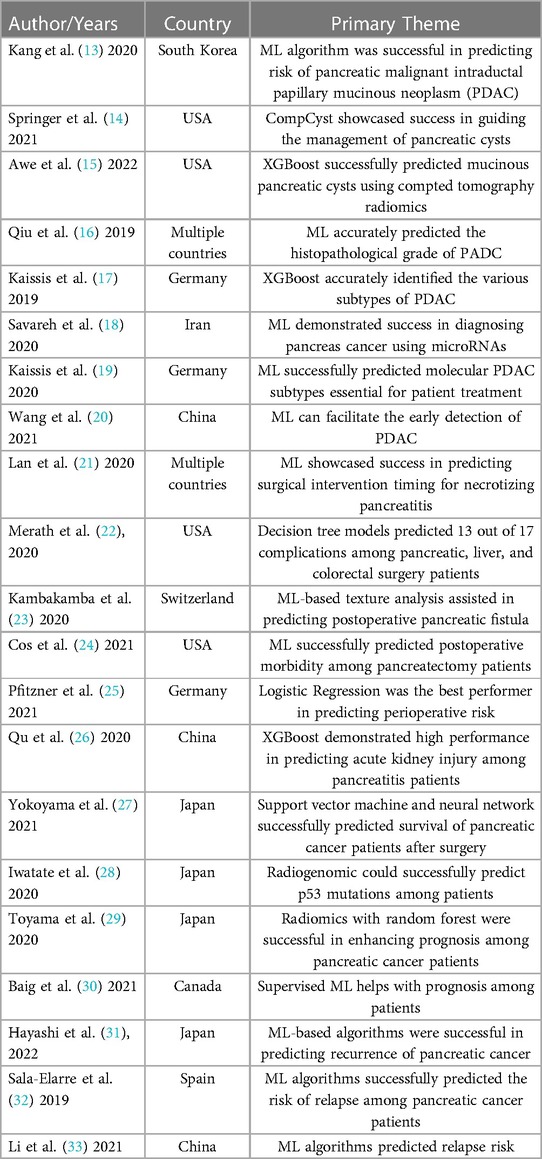
Table 1. Main themes of included studies and characteristics.
The main features of included studies revolved around the year of publication, the country, and the type of article. The majority of articles incorporated into this study were journal articles (n = 21). Only one conference proceedings paper was included. Additionally, the publication of all included articles occurred between 2019 to May 2022. Articles selected discussed various ML algorithms, including linear regression, support vector machine, and extreme gradient boosting (XGBoost). Details of included articles are displayed in Table 2.
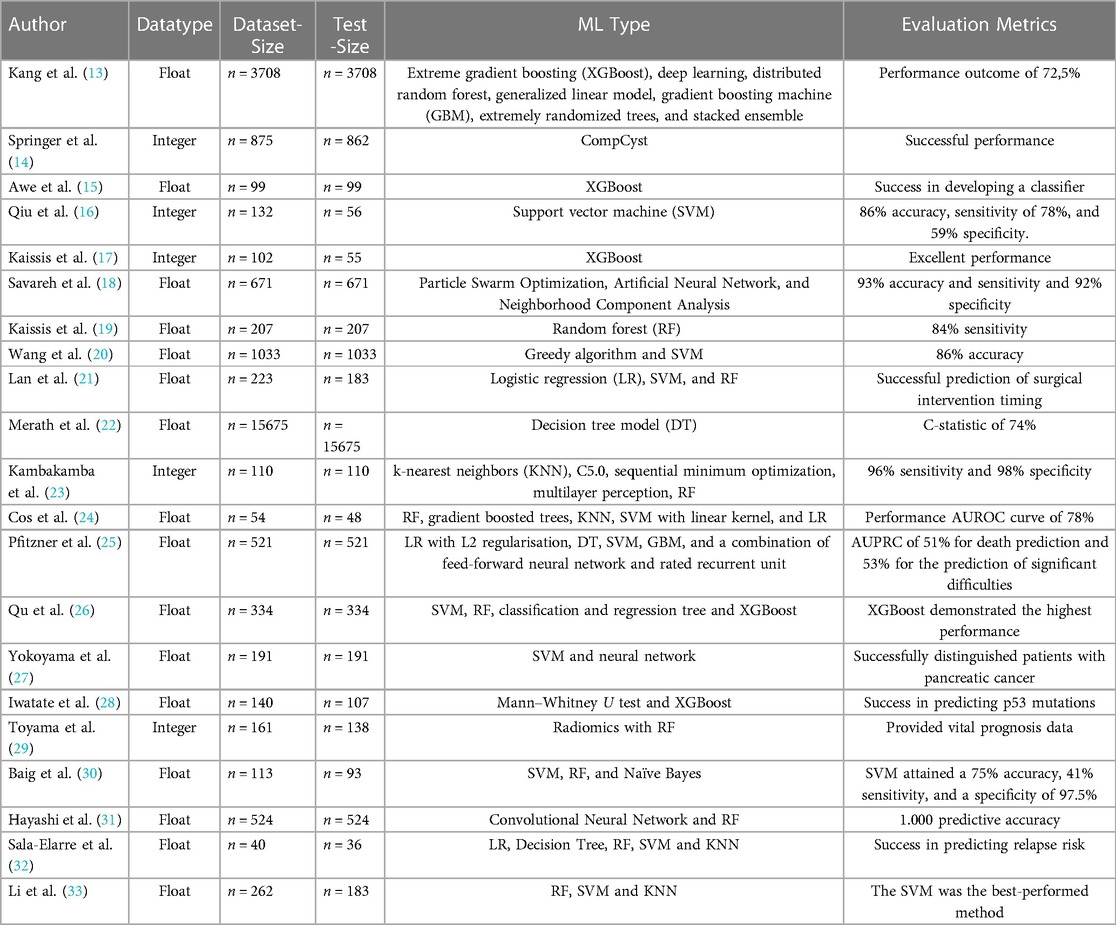
Table 2. Data types, sizes, and evaluation metrics of included articles.
Multiple articles have explored the integration of ML in pancreatic surgery. One of the main domains of ML is prediction, which studies implemented in diagnostics for pancreatic diseases. Kang et al., found that the pancreatic surgery domain applies ML techniques after comparing the performance of ML and logistic regression in predicting the risk for pancreatic malignant intraductal papillary mucinous neoplasm using preoperative clinical data and radiological features (13). In this international multicenter study, patient variables of 3708 subjects were included. The ML method developed consisted of a combination of numerous algorithms such as XGBoost, deep learning, distributed random forest, generalized linear model, gradient boosting machine, randomized trees, and stacked ensemble. The results indicated that both models, logistic regression and ML models, demonstrated similar performance outcomes. The authors asserted that logistic regresion demonstrated higher practicability and interpretability than the ML algorithm (13).
Springer et al. demonstrated the benefits of applying a ML algorithm in pancreas surgery by demonstrating its capability to improve the management of patients with pancreatic cysts (14). The researchers established the CompCyst classifier to suggest various approaches to managing cysts. The study's outcome indicated that the ML algorithm prompted the sparing of surgery among half of the patients who had undergone unnecessary cyst resection. Surgeons can use such machine algorithms to minimize morbidity and the extensive economic expenses of current management practices (14). From a synonymous perspective, Awe et al. examined the integration of ML in pancreatic surgery to predict the occurrence of mucinous pancreatic cysts through the integration of computed tomography (CT) radiomics (15). The specific ML algorithm implemented was XGBoost, which facilitated the generation of mucinous classifiers via texture characteristics or radiological and clinical combined models. The results indicated that ML could aid in pancreatic cyst identifiecation by enabling the creation of suitable classifiers (15). These arguments insinuate that many researchers will continue to explore ways to exploit ML techniques to their advantage.
Moreover, further research spearheaded by Qiu et al. revealed that ML was applicable in the pancreatic surgery domain in predicting the histopathological grade of pancreatic ductal adenocarcinoma (PDAC) among patients using preoperative CT scans (16). The tested data size was 56 patients, whereas the adopted ML algorithm was the support vector machine. After a thorough texture analysis, the ML technique achieved an accuracy of 86%, a sensitivity of 78%, and a specificity of 95% (16). Hence, the success of the support vector machine in making predictions about histopathological subtypes among PDACs indicates that the application of ML algorithms will benefit medical practitioners in individualizing treatment options for patients undergoing pancreas surgery. Kaissis et al. also showed the that ML radiomics could facilitate the prediction of molecular subtypes in PDAC (17). The authors aimed to establish a supervised ML approach for predicting the subtypes using diffusion-weighted-imaging-derived radiomic feature characteristics. The ML model used was XGBoost, and it demonstrated success in predicting the various subtypes of PDAC (17). Accordingly, ML integration and consideration into pancreas surgery are likely to increase since knowing the multiple subtypes of PDAC is vital to predict patient survival, response to chemotherapy, and recurrence-free survival.
Regarding diagnostics, Savareh et al. demonstrated that ML could aid in diagnosis of pancreatic cancer via circulating microRNA signatures (18). The ML algorithms used in this study were Particle Swarm Optimization, Artificial Neural Network, and Neighborhood Component Analysis. The outcomes illustrated that the developed algorithm showcased 93% accuracy and sensitivity and a 92% specificity (18). This factor implies that the future application of ML in the field is inevitable. In a different study, Kaissis et al. evaluated how pancreas surgeons can apply ML and radiomics to develop a non-invasive approach for facilitating clinical imaging (19). The authors combined features from CT imaging with random forest. The results found that the ML algorithm was influential in predicting the histological phenotyping of PDAC with a sensitivity of 84% (19). Another study by Wang et al. supported this argument highlighting the effectiveness of the greedy algorithm and support vector machine in early detection of PDAC using a combination of metabolomic features. Their approach yielded an 86.74% accuracy and AUC of 0.9351 in the validation cohort of 1,003 patients. Furthermore, in the added prospective collected data of 300 patients, the approach performed with an 85% accuracy and 0.9389 AUC (20). Hence, the approaches were deemed successful in detecting and analyzing the metabolism and systems of PDAC. ML methods may facilitate diagnosis and prediction of malignant pancreatic lesions and even their molecular features. Thus, ML's future application in diagnostics related to pancreas surgery will likely increase in the coming years.
The efficacy of ML models in prediction is also demonstated by the approaches to evaluate the ideal timepoint for surgical intervention. For example, a study conducted by Lan et al. revealed that ML approaches could assist in predicting the timing of surgical intervention among individuals with necrotizing pancreatitis (21). Three ML classifiers were used: logistic regression, support vector machine, and random forest. The results generated via the study indicated that ML could be beneficial in predicting the critical features related to surgical timing.
Moreover, the advantages of ML in pancreas surgery are highlighted by studies evaluating postoperative outcomes. Merath et al. assessed how ML algorithms could help predict complications after pancreatic, liver, and colorectal surgeries (22). The researchers used the decision tree models, which accurately forecasted 13 out of 17 complications evaluated. The model demonstrated a significant predictive capability and superiority over previously developed methods. Kambakamba et al. found that ML-based tissue analysis in CT could predict the occurrence of pancreatic fistula preoperatively (23). The pilot study involved 110 patients who had undergone pancreatoduodenectomy from 2008 to 2018. The results reveiled that CT had a sensitivity of 96% and a specificity of 98% in predicting pancreatic fistula after pancreatoduodenectomy (23).
Another study conducted by Cos et al. provides more evidence of ML applications in pancreatic surgery, by predicting postoperative morbidity outcomes among individuals undergoing pancreatectomy through ML and wearable devices (24). The study consisted of 48 patients, using ML methods of random forest, gradient boosted trees, k-nearest neighbors, support vector machine with linear kernel, and logistic regression with L1 penalty. The integrated ML approach utilized patient clinical features and patient activity information to develop the model. The outcomes indicated that the adopted ML algorithm attained the highest performance after scoring an AUROC curve of 0.7875 (24). Further, Pfitzner et al. showed that ML effectively predicts perioperative morbidity and mortality among patients with pancreatic cancer (25). The specific algorithms used were logistic regression, decision tree, support vector machine, gradient boosting machine, and a mixture of feed-forward neural network and rated recurrent unit. The best performing algorithm was logistic regression (25). The results indicated that more interest into ML in pancreas surgery is unavoidable. Furthermore, Qu et al. presented a synonymous argument by stating that pancreas surgeons could integrate ML algorithms to facilitate the prediction of severe kidney injury among individuals with acute pancreatitis (26). The ML model used consisted of a support vector machine, random forest, classification and
regression tree, and XGBoost. Out of all the approaches, the XGBoost demonstrated the best performance in making appropriate predictions after demonstrating an accuracy of 91.93% (26). Thus, it remains evident that machine learning integration into pancreatic surgery could also aid in predicting clinical outcomes.
Yokoyama et al. claimed that ML application in pancreatic surgery could assist in predicting oncological outcomes after resection in patients with pancreatic carcinoma (27). The authors proposed to use tissue samples from individuals with pancreatic neoplasms to assess whether they could act as predictive biomarkers for patients` 5-year overall survival. The integrated ML algorithm was a prognostic classifier formed after integrating support vector technologies, a neural network, and multinomial-based approaches (27). The results supported the approach's success in predicting survival prognosis in their cohort of patients. Different research initiated by Iwatate et al. revealed that ML via CT could predict the genetic data for pancreatic tumors in an easy, economical, and non-invasive method via cancer imaging analysis (28). The results demonstrated radiogenomic's success in predicting p53 mutations and the consequent prognosis of PDAC patients. Long-term, this could assist in establishing personalized precision treatment by gathering information from CT scans (28). Toyama et al. found that ML algorithms can help in estimating prognosis among pancreatic cancer patients (29). By using radiological features from F-fluorodeoxyglucose-positron emission tomography prior to treatment from 138 patients, results indicated that the ML algorithm adopted provided essential prognostic data by using radiomics only. Similarly, Baig et al. found that ML algorithms could help with outcome prognosis among individuals with cancer of the pancreatic head (30). Their main aim was to analyze whether the ML algorithm developed could successfully predict the survival chances of patients. The authors adopted a supervised ML algorithm which attained a 75% accuracy, 41.9% sensitivity, and 97.5% specificity (30). These studies indicate that ML adoption in pancreatic surgery can lead to multiple positive advantages and the implication has already been broad with oncological outcome prediction in pancreas surgery potentially becoming a domain of ML algorithms.
Additionally, the integration of ML in pancreatic surgery remains evident through the series of publications released on the topic. ML techniques may also be beneficial in forecasting cancer recurrence. For instance, Hayashi et al. aimed to establish and forecast patients undergoing pancreatic surgery initial and late cancer recurrence patterns and matestasis sites using a histology-based ML technique (31). The ML method consisted of a convolutional neural network and random forest combination. The sample involved 524 who had undergone pancreatic cancer surgery between 2001 and 2014. The results indicated that the model had a predictive capacity of 1,000 for nonrecurrence in both the training and test data (31). Moreover, Sala-Elarre et al., claimed that the pancreatic surgery domain could apply ML algorithms in pre-treated patients with pancreatic cancer to help in predicting their risk of developing a recurrence (32). The algorithm developed by the researchers entailed the combination of an intensified induction polychemotherapy with chemoradiation. The results of logistic regression indicated that the algorithm had the potential to predict long-term outcomes and could be a vital tool for predicting the threats of patients relapsing (32). Similarly, a study by Li et al. revealed that ML approaches like random forest, support vector machine and k-neighbor algorithms demonstrated success in predicting the relapse among PDAC patients within a one-year and two-year range using patient-related and histopathological features (33). The results indicated that support vector machine (SVM) had the most accurate approach for predicting relapse among patients who had undergone radical resection (33). Based on these results, it remains evident that pancreatic surgeons are likely to know the various advantages of incorporating ML into the field. Hence, future applications are broad since the algorithms can help guide the establishment of personalized observation systems after surgery.
The increasing integration of ML in pancreas surgery is inevitable due to the efficacy of the models in prediction. Thus, it remains evident that ML integration into pancreatic surgery could help with multiple activities, mainly aiding in diagnostics and prediction of postoperative complications and oncological outcomes.
The study's primary limitation is the paucity of information on the research topic. However, the probable cause for the research gap is the focus on recent articles released from 2019 to 2022. Also, the study exclusively included studies in English, implying that there is a possibility of excluding relevant studies published in other languages.
This research's outcomes are essential as they will improve care of pantients with undergoing pancreatic surgery by suggesting various diagnosis and outcome prediction approaches. Nevertheless, more research into the sector is necessary to ensure recent and accurate information concerning ML incorporation in pancreas surgery.
The integration of ML in pancreas surgery has gained much attention in previous years. However, the outcomes derived from this study indicate an extensive literature gap on the topic despite efforts by various researchers. Hence, future research should explore how pancreas surgeons can apply different learning algorithms to perform essential practices that ultimately improve patient outcomes. Future studies should also conduct original studies that test ML algorithms' performance using factual data from human participants. This will facilitate increased supporting information that can help delineate the future of ML in pancreas surgery. Further, researchers should explore the various shortcomings associated with ML in pancreas surgery. Mastering the limitations will be essential to developing relevant solutions to the issues. Increased evidence will ensure that surgeons can use ML techniques to make their work easier and guarantee enhanced prediction and diagnosis for pancreatic surgery complications.
Conceptualization: AT, PCC; data collection: AT, NO; visualization: AT, JFL; writing—original draft preparation: AT, ST-M, NO; writing—review and editing: VO, RR, MDH, MB, and PCC. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ye H, Liang L, Li GY, Kim J, Lu L, Wu M. Machine learning for vehicular networks: recent advances and application examples. IEEE vehicular Technology Magazine. (2018) 13(2):94–101. doi: 10.1109/MVT.2018.2811185
2. Qayyum A, Qadir J, Bilal M, Al-Fuqaha A. Secure and robust machine learning for healthcare: a survey. IEEE Rev Biomed Eng. (2020) 14:156–80. doi: 10.1109/RBME.2020.3013489
3. Dalal V, Carmicheal J, Dhaliwal A, Jain M, Kaur S, Batra SK. Radiomics in stratification of pancreatic cystic lesions: machine learning in action. Cancer Lett. (2020) 469:228–37. doi: 10.1016/j.canlet.2019.10.023
4. Zhou Y, Ge YT, Shi XL, Wu KY, Chen WW, Ding YB, et al. Machine learning predictive models for acute pancreatitis: a systematic review. Int J Med Inf. (2022) 157:104641. doi: 10.1016/j.ijmedinf.2021.104641
5. Bradley A, Van Der Meer R, McKay C. Personalized pancreatic cancer management: a systematic review of how machine learning is supporting decision-making. Pancreas. (2019) 48(5):598–604. doi: 10.1097/MPA.0000000000001312
6. Palumbo D, Mori M, Prato F, Crippa S, Belfiori G, Reni M, et al. Prediction of early distant recurrence in upfront resectable pancreatic adenocarcinoma: a multidisciplinary, machine learning-based approach. Cancers (Basel). (2021) 13(19):4938. doi: 10.3390/cancers13194938
7. Thongsalab J, Yunibhand J, Uthis P. Conceptualisation and definition of personal recovery among people with schizophrenia: additionally review. Open Nurs J. (2023) 17(1). doi: 10.2174/18744346-v17-e230403-2023-17
8. Stewart LA, Clarke M, Rovers M, Riley RD, Simmonds M, Stewart G, et al. Preferred reporting items for a systematic review and meta-analysis of individual participant data: the PRISMA-IPD statement. Jama. (2015) 313(16):1657–65. doi: 10.1001/jama.2015.3656
9. McInnes MD, Moher D, Thombs BD, McGrath TA, Bossuyt PM, Clifford T, et al. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: the PRISMA-DTA statement. Jama. (2018) 319(4):388–96. doi: 10.1001/jama.2017.19163
10. Sarkis-Onofre R, Catalá-López F, Aromataris E, Lockwood C. How to properly use the PRISMA statement. Syst Rev. (2021) 10(1):1–3. doi: 10.1186/s13643-021-01671-z
11. Bramer WM, de Jonge GB, Rethlefsen ML, Mast F, Kleijnen J. A systematic approach to searching: an efficient and complete method to develop literature searches. J Med Library Assoc: JMLA. (2018) 106(4):531. doi: 10.5195/jmla.2018.283
12. Burda BU, Holmer HK, Norris SL. Limitations of A measurement tool to assess systematic reviews (AMSTAR) and suggestions for improvement. Syst Rev. (2016) 5(1):1–0. doi: 10.1186/s13643-016-0237-1
13. Kang JS, Lee C, Song W, Choo W, Lee S, Lee S, et al. Risk prediction for malignant intraductal papillary mucinous neoplasm of the pancreas: logistic regression versus machine learning. Sci Rep. (2020) 10(1):1–8. doi: 10.1038/s41598-019-56847-4
14. Springer S, Masica DL, Dal Molin M, Douville C, Thoburn CJ, Afsari B, et al. A multimodality test to guide the management of patients with a pancreatic cyst. Sci Transl Med. (2019) 11(501):eaav4772. doi: 10.1126/scitranslmed.aav4772
15. Awe AM, Vanden Heuvel MM, Yuan T, Rendell VR, Shen M, Kampani A, et al. Machine learning principles applied to CT radiomics to predict mucinous pancreatic cysts. Abdominal Radiol. (2022) 47(1):221–31. doi: 10.1007/s00261-021-03289-0
16. Qiu W, Duan N, Chen X, Ren S, Zhang Y, Wang Z, et al. Pancreatic ductal adenocarcinoma: machine learning–based quantitative computed tomography texture analysis for prediction of histopathological grade. Cancer Manag Res. (2019) 11:9253. doi: 10.2147/CMAR.S218414
17. Kaissis G, Ziegelmayer S, Lohöfer F, Steiger K, Algül H, Muckenhuber A, et al. A machine learning algorithm predicts molecular subtypes in pancreatic ductal adenocarcinoma with differential response to gemcitabine-based versus FOLFIRINOX chemotherapy. PloS one. (2019) 14(10):e0218642. doi: 10.1371/journal.pone.0218642
18. Savareh BA, Aghdaie HA, Behmanesh A, Bashiri A, Sadeghi A, Zali M, et al. A machine learning approach identified a diagnostic model for pancreatic cancer through using circulating microRNA signatures. Pancreatology. (2020) 20(6):1195–204. doi: 10.1016/j.pan.2020.07.399
19. Kaissis GA, Ziegelmayer S, Lohöfer FK, Harder FN, Jungmann F, Sasse D, et al. Image-based molecular phenotyping of pancreatic ductal adenocarcinoma. J Clin Med. (2020) 9(3):724. doi: 10.3390/jcm9030724
20. Wang G, Yao H, Gong Y, Lu Z, Pang R, Li Y, et al. Metabolic detection and systems analyses of pancreatic ductal adenocarcinoma through machine learning, lipidomics, and multi-omics. Sci Adv. (2021) 7(52):eabh2724. doi: 10.1126/sciadv.abh2724
21. Lan L, Guo Q, Zhang Z, Zhao W, Yang X, Lu H, et al. Classification of infected necrotizing pancreatitis for surgery within or beyond 4 weeks using machine learning. Front Bioeng Biotechnol. (2020) 8:541. doi: 10.3389/fbioe.2020.00541
22. Merath K, Hyer J, Mehta R, Farooq A, Bagante F, Sahara K, et al. Use of machine learning for prediction of patient risk of postoperative complications after liver, pancreatic, and colorectal surgery. J Gastrointest Surg. (2020) 24(8):1843–51. doi: 10.1007/s11605-019-04338-2
23. Kambakamba P, Mannil M, Herrera PE, Müller PC, Kuemmerli C, Linecker M, et al. The potential of machine learning to predict postoperative pancreatic fistula based on pre-operative, non-contrast-enhanced CT: a proof-of-principle study. Surgery. (2020) 167(2):448–54. doi: 10.1016/j.surg.2019.09.019
24. Cos H, Li D, Williams G, Chininis J, Dai R, Zhang J, et al. Predicting outcomes in patients undergoing pancreatectomy using wearable technology and machine learning: prospective cohort study. J Med Internet Res. (2021) 23(3):e23595. doi: 10.2196/23595
25. Pfitzner B, Chromik J, Brabender R, Fischer E, Kromer A, Winter A, et al. Perioperative Risk Assessment in Pancreatic Surgery Using Machine Learning. In2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC) 2021 Nov 1 (pp. 2211-2214). IEEE.
26. Qu C, Gao L, Yu XQ, Wei M, Fang GQ, He J, et al. Machine learning models of acute kidney injury prediction in acute pancreatitis patients. Gastroenterol Res Pract. (2020) 2020:3431290. doi: 10.1155/2020/3431290
27. Yokoyama S, Hamada T, Higashi M, Matsuo K, Maemura K, Kurahara H, et al. Predicted prognosis of patients with pancreatic cancer by machine learning. Clin Cancer Res. (2020) 26(10):2411–21. doi: 10.1158/1078-0432.CCR-19-1247
28. Iwatate Y, Hoshino I, Yokota H, Ishige F, Itami M, Mori Y, et al. Radiogenomics for predicting p53 status, PD-L1 expression, and prognosis with machine learning in pancreatic cancer. Br J Cancer. (2020) 123(8):1253–61. doi: 10.1038/s41416-020-0997-1
29. Toyama Y, Hotta M, Motoi F, Takanami K, Minamimoto R, Takase K. Prognostic value of FDG-PET radiomics with machine learning in pancreatic cancer. Sci Rep. (2020) 10(1):1–8. doi: 10.1038/s41598-019-56847-4
30. Baig Z, Abu-Omar N, Khan R, Verdiales C, Frehlick R, Shaw J, et al. Prognosticating outcome in pancreatic head cancer with the use of a machine learning algorithm. Technol Cancer Res Treat. (2021) 20:15330338211050767. doi: 10.1177/15330338211050767
31. Hayashi K, Ono Y, Takamatsu M, Oba A, Ito H, Sato T, et al. Prediction of recurrence pattern of pancreatic cancer post-pancreatic surgery using histology-based supervised machine learning algorithms: a single-center retrospective study. Ann Surg Oncol. (2022) doi: 10.1245/s10434-022-11471-x. [Epub ahead of print]
32. Sala-Elarre P, Oyaga-Iriarte E, Yu KH, Baudin V, Arbea Moreno L, Carranza O, et al. Use of machine-learning algorithms in intensified pre-operative therapy of pancreatic cancer to predict individual risk of relapse. Cancers (Basel). (2019) 11(5):606. doi: 10.3390/cancers11050606
Keywords: machine learning, deep learning, pancreas surgery, scoping review, pancreas
Citation: Taha A, Taha-Mehlitz S, Ortlieb N, Ochs V, Honaker MD, Rosenberg R, Lock JF, Bolli M and Cattin PC (2023) Machine learning in pancreas surgery, what is new? literature review. Front. Surg. 10:1142585. doi: 10.3389/fsurg.2023.1142585
Received: 11 January 2023; Accepted: 19 May 2023;
Published: 13 June 2023.
Edited by:
Riccardo Casadei, University of Bologna, ItalyReviewed by:
Isabella Frigerio, Casa di cura Pederzoli, Italy© 2023 Taha, Taha-Mehlitz, Ortlieb, Ochs, Honaker, Rosenberg, Lock, Bolli and Cattin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anas Taha YW5hcy50YWhhQHVuaWJhcy5jaA==
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work, share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.