 Ping Li1,2,3,†
Ping Li1,2,3,† Pingming Fan
Pingming Fan Peng-fei Lyu
Peng-fei Lyu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg., 27 April 2023
Sec. Otorhinolaryngology - Head and Neck Surgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1120442
Purpose: In this study, the aim was to comprehensively analyze the current status, hotspots, and trends of trans-oral endoscopic thyroidectomy (TOET) through bibliometric analysis and by presenting the field atlas.
Methods: Web of Science Core Collection database was adopted to screen studies regarding TOET published between January 1, 2008 and August 1, 2022. The evaluation covered the criteria total number of studies, keywords, and contributions from countries/regions, institutions, journals, and authors.
Results: A total of 229 studies were covered. SURGICAL ENDOSCOPY AND OTHER INTERVENTIONAL TECHNIQUES is the largest publication in the field of TOET. The three countries that contributed the most studies were Korea, China, and the USA. The most frequently occurring core keywords in the field of TOET are vestibular approach, outcomes, experience, safety, robotic thyroidectomy, scar, video-assisted thyroidectomy and quality-of-life. The seven clusters were generated in this study: intraoperative monitoring of the laryngeal return nerve (# 0), learning curve (# 1), postoperative quality of life (# 2), central lymph node dissection and safety (# 3), complications (# 4), minimally invasive surgery (# 5), and robotic surgery (# 6).
Conclusion: The main research topics in the field of TOET place focuses on learning curves, laryngeal nerve monitoring, carbon dioxide gas bolus, chin nerve injury, surgical complications, and surgical safety. In the future, more academics will focus on the safety of the procedure and reducing complications..
There are 586,000 cases of thyroid cancer around the world, and the incidence of thyroid cancer ranked 9th in 2020 (1). Papillary thyroid carcinoma (PTC) has been confirmed as a highly common endocrine malignancy in the world. Existing studies have suggested that the global incidence of thyroid cancer has been rising over the past two decades (2). Surgery has been most frequently used to treat thyroid cancer. However, it is inevitable that conventional open thyroidectomy (COT) will leave visible scars on the neck, such that COT is not preferred widely, in particular young females. Patients with a high expectation of cosmetic results, in particular Asian patients having pronounced scars, cannot accept any small surgical scar left on or near their neck (3). In the last century, minimally invasive and remote access surgical technologies emerged and have been applied to numerous surgical specialties (e.g., thoracic, abdominal, pelvic surgery, as well as head and neck surgery in recent years). A wide variety of scar-free surgical approaches had been developed (e.g., total endoscopic thyroidectomy via trans-axillary approach and the areola approach (ETA), as well as the transoral endoscopic thyroidectomy vestibular approach (TOETVA) (4–6). TOETVA, a type of natural orifice translumenal endoscopic surgery (NOTES), has been the most used process in transoral thyroidectomy. Its superiorities involve good function short-term voice outcomes, advantages of central lymph nodes dissection, scar free approaches and low surgical morbidity (7).
Bibliometric research is often adopted to evaluate published research, analyze the characteristics of disciplinary developments, and predict future trends in scientific research. The above research has combined mathematical and statistical methods to identify research areas and then visualized and analyzed the number of publications, authors, institutional countries/regions, journals, themes, and so forth. Network research between some of the research indicators forms a relational network diagram and improve the knowledge structure established on subject clusters. The researcher or practitioner can employ the study to gain valuable insights into the lineage, current characteristics, and future trends in the development of the subject area.
TOET refers to an emerging surgical procedure that is rapidly used by surgeons with good results. In this study, bibliometrics is adopted to present comprehensive assessment of global scientific research in TOET, analyzing TOET's disciplinary characteristics, current hotspots, and future trends. On that basis, enthusiasts and practitioners can gain a quick and in-depth understanding of TOET and more effectively identify hotspots of relevant studies.
The WoSCC database was searched for studies published in a range from January 1, 2008 to August 1, 2022. The keywords employed in the database to be used to search the database comprised (transoral OR vestibular OR oral OR mouth OR transorally OR trans-oral OR “vestibule of the mouth” OR TOET OR TOT OR TOETVA) AND (thyroidectomy OR thyroidectomies OR “thyroid lobectomy”) AND (endoscopic OR endoscopy OR video endoscopic). Two authors evaluated the retrieved studies to exclude irrelevant literature. Areas of disagreement were assessed by the corresponding author. All covered studies were downloaded as plain text files and software analysis was performed for reference, keyword, fundings, abstracts, author, titles, and other research indicators.
A total of 285 English-language document records were achieved for transoral thyroidectomy. Duplicates were removed, and document types (original studies and reviews) were selected. Lastly, 229 articles were retained for the bibliometric analysis through manual review and confirmation by two authors.
Bibliometric tools [e.g., CiteSpace, Vosviewer, Rstudio (bibliometric package), and gCLUTO software] were adopted to analyze the covered studies for institution, country, journal, author, keywords, as well as references. A bibliographic coupling network was established, and a visual network analysis was conducted on the content of the study.
The time span for TOETVA technology to be applied to people is from 2009 to 2022. 72 journals published studies in the field; and each study was cited an average of 17.28 times per year. In terms of study type, there were 202 original researches and 27 reviews. The number of studies per year is shown in Figure 1.
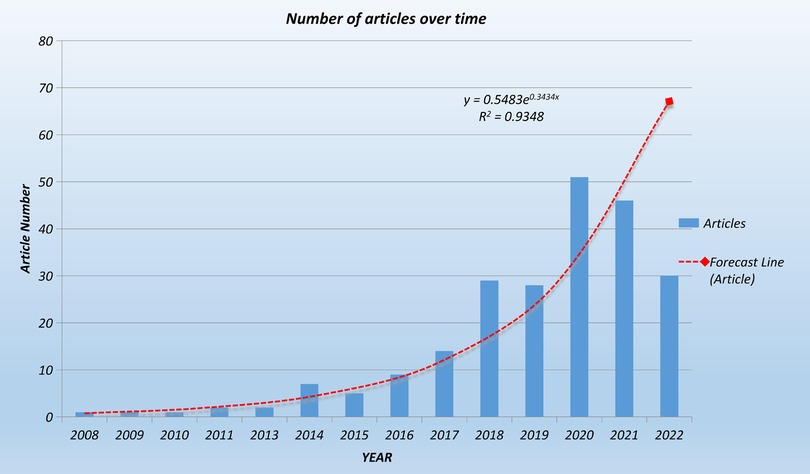
Figure 1. Changes in the number of articles linked to TOET over time. The red dotted line is the forecast line, and the red square represents the forecast document volume in 2022. From 2008 to 2016, the number of studies per year was below 10. Rapid growth from 2017 onward, the number of studies published per year is above 28, reaching 51 in 2020. Based on the prediction curve (red dashed line), it is predicted that 68 studies may come out in 2022.
Korea, China, and the United States have outstanding contributions to the development of trans-oral thyroid surgery with 68, 66, and 61 published studies, respectively. Together, the above three countries account for 85.15% of all study publications. Figure 2A shows a map of TOET's national collaboration network with frequent international collaborations.
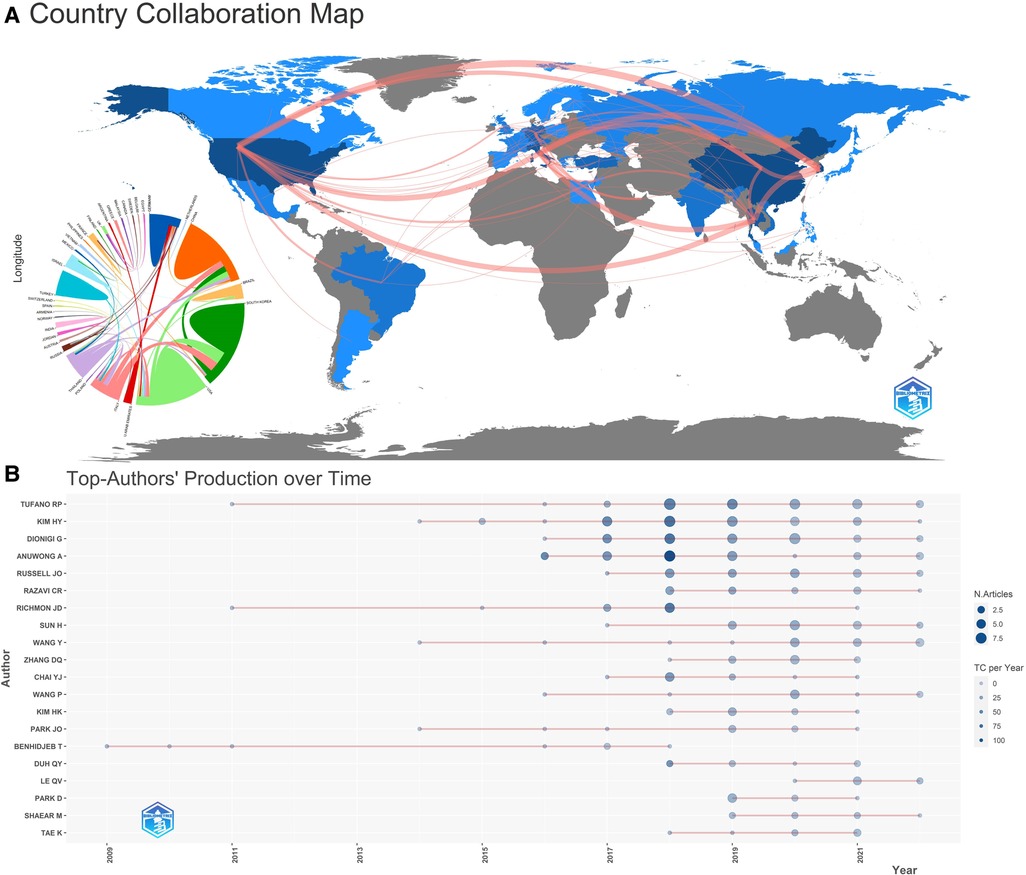
Figure 2. (A) national cooperation map. The connection represents the cooperation between countries. The darker the color, the greater the number of articles. (B) Top-author's production over time. TC, total citation.
There are 766 authors from 35 countries contributing to TOETVA. The top 3 most productive authors are Tufano RP, Kim HY and Dionigi G. Tufano RP from the USA published 36 studies, accounting for 15.7% of the total. Kim HY from Thailand published 35 studies (15.2%). Dionigi G from Italy published 32 studies (13.98%). Anuwong A has published 29 studies (12.66%) and is ranked fourth. The top 20 authors' production over time is shown in Figure 2B. The above authors have a high number of studies published and cited after 2017.
In term of TOETVA-related institutions, KOREA UNIV, UNIV MESSINA, Johns Hopkins Univ and POLICE GEN HOSP contribute significantly to TOETVA. Figure 3A is a map of co-occurrence between institutions, with some inter-institutional collaboration. 41 studies were from Johns Hopkins Univ, of which 13 were first author; the most cited institution was Korea Univ with 615 citations. The top 10 contributing institutions to the study about TOETVA is in Table 1.
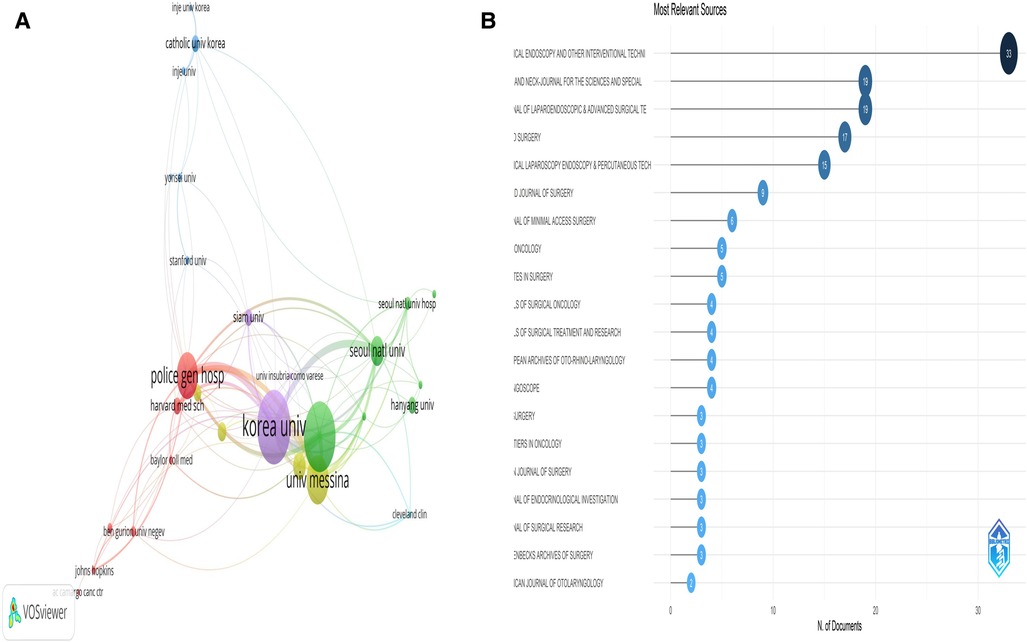
Figure 3. (A) organization co-occurrence network diagram. The size of the circle represents the number of documents issued by the organization, and the connection represents the connection between organizations. (B) Publications of top 20 related magazines.
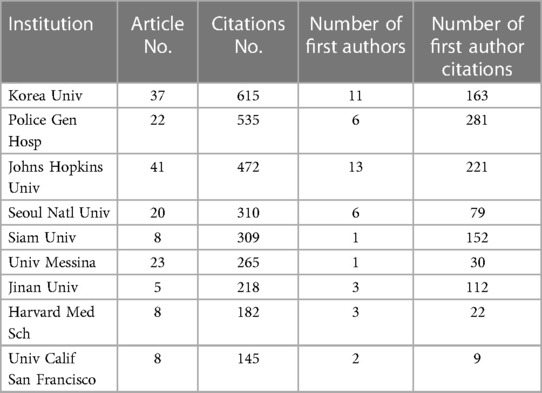
Table 1. Top 10 contributing institutions to the article about TOETVA.
SURGICAL ENDOSCOPY AND OTHER INTERVENTIONAL TECHNIQUES was the most published journal (n = 33), followed by HEAD AND NECK—JOURNAL FOR THE SCIENCES AND SPECIALTIES OF THE NECK and JOURNAL OF LAPAROENDOSCOPIC & ADVANCED SURGICAL TECHNIQUES (n = 19). Figure 3B lists the 20 journals with the highest number of publications.
The most cited study is by Anuwong A from Thailand with 264 citations. Table 2 lists the 10 most cited studies in the field of TOETVA. Among the above 10 studies, 3 studies from Anuwong A with a total of 596 citations are the most cited authors. In addition, four of the 10 most cited studies are from the journal SURGICAL ENDOSCOPY AND OTHER INTERVENTIONAL TECHNIQUES, with a total of 463 citations.
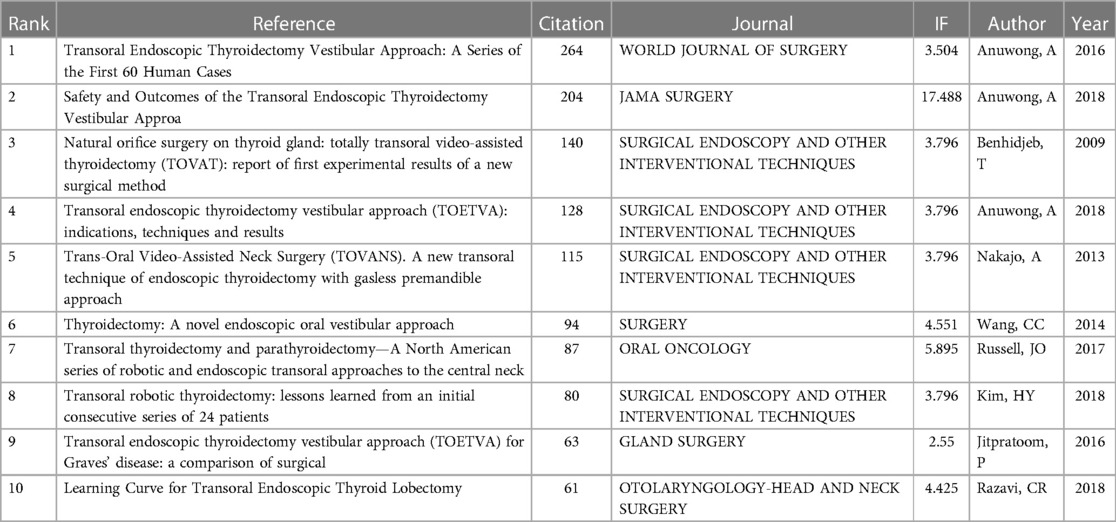
Table 2. The top 10 most cited articles in TOETVA field.
The high frequency keywords reveal the research focus of scholars in a field. The top 20 high-frequency words from Figure 4A (density plot of keywords) are elucidated as follows: surgery, series, vestibular approach, endoscopic thyroidectomy, outcomes, experience, safety, robotic thyroidectomy, scar, breast approach, video-assisted thyroidectomy, cancer, quality-of-life, approach TOETVA assisted thyroidectomy, initial-experience, parathyroid surgery parathyroid surgery, as well as parathyroidectomy. Figure 4B shows a heat map of the matrix visualization after keyword clustering divided into seven broad clusters: intraoperative monitoring of the laryngeal return nerve (# 0), learning curve (# 1), postoperative quality of life (# 2), central lymph node dissection and safety (# 3), complications (# 4), transoral vestibular pathway is minimally invasive surgery (# 5), and robotic surgery (# 6). Figure 4C shows the visual mountain maps of the seven clusters. After trying different combinations of clusters, it was determined that the 7 clusters had the optimal clustering of the mountain maps, with the peaks being independent of each other and the peaks being brightly colored. Figure 4D provides a graph of TOETVA's theme bubbles. The lower right quadrant is the base theme with a good degree of low centrality development, and themes in this quadrant are currently more maturely researched. The largest number of bubbles in the lower right quadrant reveals that the technology is mature. As depicted in Figure 4A, the themes in the upper right quadrant are the motor themes, i.e., the safety of TOET. This theme is highly central and has a good degree of development, and more scholars will continuously optimize intraoperative and postoperative safety in the future.
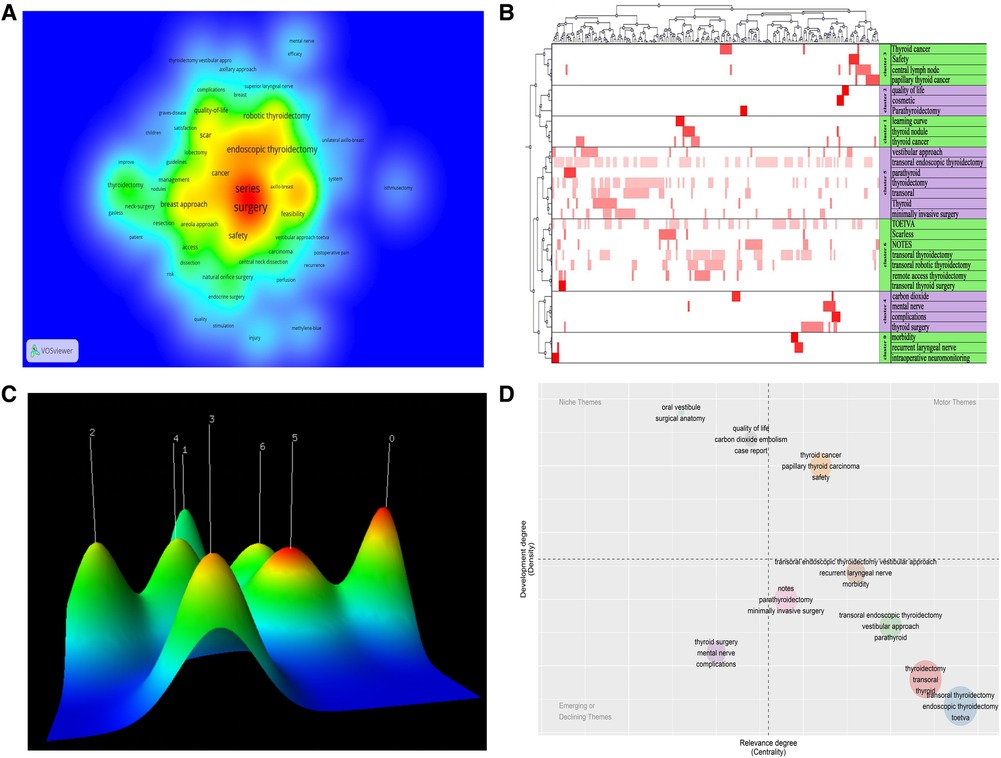
Figure 4. (A) the density map of keywords; (B) the visualized heat map linked to data matrix of keywords; (C) the visualized mountain map of theme clustering; (D) the thematic map of keywords (bubble chart).
The field of TOET has developed significantly over the last decade, especially after 2017 when it entered a rapid development phase and became a popular technology. It has been widely favored by doctors and patients. Accordingly, the hotspots and trends of TOET should be summarized through bibliometrics. This study can provide head and neck surgeons with research highlights and hotspots in the field of TOET. Keeping abreast of developments in relevant studies will be conducive to identifying hotspots for this research and guiding further developments in this field.
Sublingual transoral access for thyroid surgery was first proposed by Entezami P et al. (8). The first application of complete trans-oral video-assisted thyroidectomy (TOVT) to humans was reported by Benhidjeb T in Germany (9). Thomas from Germany reported cases where the use of sublingual transoral access hindered surgical manipulation due to narrow access (10) and increased risk of infection.
Afterward, Wang et al. first reported TOETVA in human patients in 2014 (11). The oral vestibular approach is capable of avoiding damage to the floor of the oral cavity. Moreover, it reduces postoperative damage to the floor of the oral cavity, and it can improve the safety of the procedure. This approach became widespread after Anuwong's 2016 study of 60 patients who underwent the transoral endoscopic thyroidectomy vestibular approach (12), which rank first in the top 10 most cited studies. Subsequently, Anuwong A summarized the postoperative results and surgical indications of TOETVA (13), assessed the safety (6), and significantly optimized the technique. The work of this scholar has been the most cited. Among the top 10 cited studies, except for three highly cited studies by Anuwong, the remaining seven presented TOETVA experience sharing (9, 14), learning curve (15), robotic surgery (16, 17), and inflation-free methods (18). The above 10 highly cited studies have contributed to the development of TOETVA.
In the field of TEOT, there have been frequent exchanges and cooperation between countries. Korea, China and the United States have made outstanding contributions, as manifested by the number of publications and the number of important authors, institutions and journals from the above three countries. Table 3 lists the top ten projects funded by the fund, and they all come from the above three countries. Accordingly, the development of TEOT requires the support of national government funds. Hot topics and future trends in the TOET field can be concluded (e.g., learning curves, surgical points, and complication prevention and management) through clustering analysis of keywords and topics. Considerable studies have indicated the advantages of TOETVA and how to prevent against complications.

Table 3. Top 10 funding agencies.
Intraoperative neuromonitoring (IONM) is considered an important accessory to protect the nerves during conventional radical thyroidectomy (19). Given the high sensitivity and specificity, IONM should be considered a useful tool for thyroid surgery and its use should be suggested for patients undergoing planned total thyroidectomy. Its right application may cancel the risk of bilateral paralysis (20). Memeh K et al. used a doubly robust (DR) estimator in the form of an inverse probability weighted regression adjustment model to estimate the effect of using IONM on the risk of RLN injury and found that the use of IONM was associated with a reduction in RLN injury (21). In a retrospective study by Fei Y et al. divided into IONM and non-IONM groups, the time required to identify the recurrent laryngeal nerve (RLN) was shorter in the IONM group (3.05 ± 1.58 vs. 9.36 ± 4.82 min, p < 0.01); the RLN identification rate was much higher in the IONM group than in the non-IONM group (100.00% vs. 88.52%, p = 0.01) (22). In our experience, IONM is not only necessary in finding RLN but, at the same time, can help to change some operating habits, such as keeping energy devices away from RLN and using scissors to remove lymph nodes if necessary.
Regarding the learning curve of TORT, many scholars have made studies in this area. Many studies show that intraoperative neuromonitoring help decreased learning curve (23–25), because nerve monitoring can assist in the exploration of the recurrent laryngeal nerve. The learning curve revealed two phases, an initial and a mature phase, for initial phase its range from 15 to 35 cases (26). Chai YJ et al. used cumulative summation (CUSUM) analysis of TOETVA learning curves for glandular lobectomy in 58 cases (27). The learning curves for trans-oral robotic thyroidectomy (TORT) was 25 cases, having a shorter learning curve (28). Meanwhile, in vitro simulation training and animal experiments would notably decrease learning curve. Case series from the initial TOETVA operations of four surgeons at three different hospitals were tested over the past few years. Binary logistic regression showed a negative correlation of complication rate and case number (p < 0.001, Odds Ratio: 0.91) (29).
Numerous studies have confirmed that TOET can achieve the same effect with open thyroidectomy (OT) in VI and VII neck nodes dissection (5, 30, 31). A recent study indicated that TOETVA outperformed endoscopic thyroidectomy via areola approach (ETA) on total central lymph nodes (7.82 ± 3.35 vs. 5.26 ± 2.45, p < 0.05) (32). Under the TOETVA viewer, innominate artery can be easily exposed for VII dissection compares to ETA. Zheng, GB et al. also noted that the TOETVA group achieved a higher number of central lymph nodes than the endoscopic thyroidectomy transaxillary approach (ETTA) group (7.2 ± 4.6 vs. 3.9 ± 3.0, p < 0.001) (33).
Existing research has initially reported that there was no difference in the number of lymph nodes between the transoral and non-transoral routes, i.e., a result that may have been due to the limited number of studies covered in the early meta-analysis (34). In the latest meta-analysis conducted by Dabsha A et al., trans-oral endoscopic trans-vestibular thyroidectomy (TOT) had an advantage in terms of the number of lymph nodes harvested compared with the trans-axillary route (35). The possible reason for different results of the two meta-analyses is that fewer studies were covered earlier. TOETVA has some advantages in central regional lymph node dissection, because which is a natural route.
Numerous studies have suggested that TOETVA has high safety (36), the amplified visual field has easy to identify recurrent laryngeal nerve and blood vessel, thus improving the safety of the procedure (7, 37). Trans-oral endoscopic treatment can achieve better cosmetic results and a higher quality of life, as compared with the trans-areolar path (38). In our center, no drainage was placed in unilateral thyroidectomy combined with central lymph nodes dissection in common. All those patients recover quickly, and the neck was scarless without swelling. Furthermore, the quality of life related to neck appearance after transoral robotic thyroidectomy is higher than that of conventional open thyroidectomy was verified using 2 questionnaires as follows: the University of Washington QOL questionnaire and the thyroid cancer-specific Quality of Life questionnaire (Thyroid Version) (39). Transoral robotic thyroidectomy is likely to be used by more physicians in the future.
Injury of mental nerve was a relative common complication in TOETVA, which can be avoided by preoperative elevation (40, 41). Our experience is that to place the operating TROCA between 3 and 4 teeth firstly and then to place the observe TROCA to prevent mental nerve shift and had accidental injury.
Carbon dioxide (CO2) embolism refers to a rare but potentially devastating complication of in endoscopy surgery. CO2 embolism, characterized by a decrease in end-tidal CO2 and oxygen saturation, can cause rapid intraoperative hypotension and cardiovascular collapse (42). Some reports regarding CO2 embolism in TOETVA, as gas pressure 6 mmhg, this complication would notably decrease. When a CO2 embolism is encountered, my recommendation is to quickly shut off the CO2 and place the patient in a foot-high, head-low position, which will help stabilize the patient's vital signs.
In the early exploration of TOVETA, there were concerns of postoperative infection. As the technology matures, strict oral sterilization or antisepsis can prevent infection after surgery. Previous studies have shown that although TOETVA is technically mature, its learning curve is significantly longer than that of ETA and open surgery, and some complications, such as carbon dioxide embolism, mental nerve injury, infection, skin burn, recurrent laryngeal nerve injury, etc., can be well prevented by skilled surgeons during the operation. Regression analysis of TOETVA complications by Fernandez-Ranvier G et al. showed the most significant reduction in complications in case 12, with the risk and severity of complications decreasing significantly as the number of cases increased (23). In addition, delayed tracheal rupture was reported after 1 week of TOETVA treatment (43). Previous studies have shown judicious use of energy instruments and a safe distance from the windpipe can avoid tracheal damage..
The safety of the procedure was the motor theme from the topic map analysis (Figure 4B), and it is believed that this topic will continue to be a hot topic of research in the future. Transoral robotic thyroidectomy has become popular with a wide range of surgeons over the last three years, and its safety, quality of life and effectiveness have aroused much scholarly attention (28, 44).
A transoral endoscopic thyroidectomy transmandibular approach has recently been reported to be effective and safe, avoiding skin numbness in the central mandibular region and reducing the difficulty of establishing a surgical space (45). In addition, some studies have reported good results with inflation-free TOETVA, such as clear visual fields and no CO2 gas embolism complications (18, 33, 46, 47). As the technology develops, several studies suggest TOETVA may be a feasible and safe thyroidectomy for children (48). The above new findings and perspectives make TOETVA very promising for the future.
First, studies from WoS-indexed journals were only analyzed; thus, some novel studies regarding TOET may have been overlooked and excluded from this study. Second, since the classification of studies is based on the number of citations reported, some of the best recently published studies in the field failed to attract our attention due to the low number of citations; therefore, regular bibliometric updates of the study are required. Third, only original published studies were analyzed in this study, and other forms of research (e.g., proposals, conferences, and materials) may not be covered, and new insights may be missed. Although there may be shortcomings, they do not affect TOETVA's comprehensive and exhaustive analysis of the literature in our study.
This study is dedicated to exploring hot topics and developing features in the field of TOET through a visual bibliometric analysis. TOET's topics primarily focus on learning curves, recurrent laryngeal nerve monitoring, carbon dioxide gas embolism, mental nerve injury, surgical complications, and surgical safety. In the future, more academics will place a focus on the safety of the procedure and reduce the number of complications. Furthermore, more updates may be reported on TOETVA technology and optimization of the safety of the procedure.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
PL, HQ, and P-fL participated in the conception and formulation. PF and RJ collected and analyzed the data. PL and RJ drew and wrote the first draft. WZ helped revise the manuscript. P-fL, PF, and WZ were responsible for supervision. All authors contributed to the article and approved the submitted version.
This research was supported by the Excellent Young Talents Fund Program of TJMUCH (Grant No. 2019-1-11) and Tianjin Key Medical Discipline (Secialty) Construction Project (TJYXZDXK-009A).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. La Vecchia C, Malvezzi M, Bosetti C, Garavello W, Bertuccio P, Levi F, et al. Thyroid cancer mortality and incidence: a global overview. Int J Cancer. (2015) 136(9):2187–95. doi: 10.1002/ijc.29251
3. Wang C, Feng Z, Li J, Yang W, Zhai H, Choi N, et al. Endoscopic thyroidectomy via areola approach: summary of 1,250 cases in a single institution. Surg Endosc. (2015) 29(1):192–201. doi: 10.1007/s00464-014-3658-8
4. Yang JG, Wang CC, Li JY, Yang W, Cao G, Wong HM, et al. Complete endoscopic thyroidectomy via oral vestibular approach versus areola approach for treatment of thyroid diseases. J Laparoendosc Adv Surg Tech. (2015) 25(6):470–6. doi: 10.1089/lap.2015.0026
5. Liu ZD, Li YJ, Wang Y, Xiang C, Yu X, Zhang ML, et al. Comparison of the transoral endoscopic thyroidectomy vestibular approach and open thyroidectomy: a propensity score-matched analysis of surgical outcomes and safety in the treatment of papillary thyroid carcinoma. Surgery. (2021) 170(6):1680–6. doi: 10.1016/j.surg.2021.06.032
6. Anuwong A, Ketwong K, Jitpratoom P, Sasanakietkul T, Duh QY. Safety and outcomes of the transoral endoscopic thyroidectomy vestibular approach. JAMA Surg. (2018) 153(1):21–7. doi: 10.1001/jamasurg.2017.3366
7. Tae K. Complications of transoral thyroidectomy: overview and update. Clin Exp Otorhinolaryngol. (2021) 14(2):169–78. doi: 10.21053/ceo.2020.02110
8. Witzel K, von Rahden BH, Kaminski C, J H. Stein: transoral access for endoscopic thyroid resection. Surg Endosc. (2008) 22(8):1871–5. doi: 10.1007/s00464-007-9734-6
9. Benhidjeb T, Wilhelm T, Harlaar J, Kleinrensink GJ, Schneider TAJ, Stark M. Natural orifice surgery on thyroid gland: totally transoral video-assisted thyroidectomy (tovat): report of first experimental results of a new surgical method. Surg Endosc. (2009) 23(5):1119–20. doi: 10.1007/s00464-009-0347-0
10. Wilhelm T, Metzig A. Endoscopic minimally invasive thyroidectomy (emit): a prospective proof-of-concept study in humans. World JSurg. (2011) 35(3):543–51. doi: 10.1007/s00268-010-0846-0
11. Wang CC, Zhai HN, Liu WJ, Li JY, Yang JG, Hu YZ, et al. Thyroidectomy: a novel endoscopic oral vestibular approach. Surgery. (2014) 155(1):33–8. doi: 10.1016/j.surg.2013.06.010
12. Anuwong A. Transoral endoscopic thyroidectomy vestibular approach: a series of the first 60 human cases. World JSurg. (2016) 40(3):491–7. doi: 10.1007/s00268-015-3320-1
13. Anuwong A, Sasanakietkul T, Jitpratoom P, Ketwong K, Kim HY, Dionigi G, et al. Transoral endoscopic thyroidectomy vestibular approach (Toetva): indications, techniques and results. Surg Endosc. (2018) 32(1):456–65. doi: 10.1007/s00464-017-5705-8
14. Jitpratoom P, Ketwong K, Sasanakietkul T, Anuwong A. Transoral endoscopic thyroidectomy vestibular approach (Toetva) for Graves’ disease: a comparison of surgical results with open thyroidectomy. Gland Surg. (2016) 5(6):546–52. doi: 10.21037/gs.2016.11.04
15. Razavi CR, Vasiliou E, Tufano RP, Russell JO. Learning curve for transoral endoscopic thyroid lobectomy. Otol Head Neck Surg. (2018) 159(4):625–9. doi: 10.1177/0194599818795881
16. Kim HY, Chai YJ, Dionigi G, Anuwong A, Richmon JD. Transoral robotic thyroidectomy: lessons learned from an initial consecutive series of 24 patients. Surg Endosc. (2018) 32(2):688–94. doi: 10.1007/s00464-017-5724-5
17. Russell JO, Clark J, Noureldine SI, Anuwong A, Al Khadem MG, Kim HY, et al. Transoral thyroidectomy and parathyroidectomy—a North American series of robotic and endoscopic transoral approaches to the central neck. Oral Oncol. (2017) 71:75–80. doi: 10.1016/j.oraloncology.2017.06.001
18. Nakajo A, Arima H, Hirata M, Mizoguchi T, Kijima Y, Mori S, et al. Trans-oral video-assisted neck surgery (tovans). A new transoral technique of endoscopic thyroidectomy with gasless premandible approach. Surg Endosc. (2013) 27(4):1105–10. doi: 10.1007/s00464-012-2588-6
19. Barczynski M, Konturek A, Stopa M, Hubalewska-Dydejczyk A, Richter P, Nowak W. Clinical value of intraoperative neuromonitoring of the recurrent laryngeal nerves in improving outcomes of surgery for well-differentiated thyroid cancer. Pol Przegl Chir. (2011) 83(4):196–203. doi: 10.2478/v10035-011-0030-8
20. Rossini M, Cozzani F, Loderer T, Bonati E, Giuffrida M, Del Rio P. Intraoperative neuromonitoring, nerves at risk and staged thyroidectomy, our experience on 377 consecutive cases. Acta Biomed Atenei Parm. (2022) 93(2):e2022040. doi: 10.23750/abm.v93i2.11178
21. Memeh K, Vaghaiwalla T, Keutgen X, Angelos P. Effect of intraoperative neuromonitoring on the risks of recurrent laryngeal nerve injury during thyroidectomy: a doubly robust approach. Ann Surg. (2022) 276(4):684–93. doi: 10.1097/SLA.0000000000005588
22. Fei Y, Li Y, Chen F, Tian W. Intraoperative neuromonitoring of the recurrent laryngeal nerve is indispensable during complete endoscopic radical resection of thyroid cancer: a retrospective study. Laryngoscope Investig Otol. (2022) 7(4):1217–23. doi: 10.1002/lio2.822
23. Malik R, Linos D. Intraoperative neuromonitoring in thyroid surgery: a systematic review. World J Surg. (2016) 40(8):2051–8 doi: 10.1007/s00268-016-3594-y
24. Sun H, Tian W, Jiang K, Chiang F, Wang P, Huang T, et al. Clinical guidelines on intraoperative neuromonitoring during thyroid and parathyroid surgery. Ann Transl Med. (2015) 3(15):213 doi: 10.3978/j.issn.2305-5839.2015.08.21
25. Kuo TC, Duh QY, Wang YC, Lai CW, Chen KY, Lin MT, et al. Practice patterns and learning curve in transoral endoscopic thyroidectomy vestibular approach with neuromonitoring. Front Endocrinol. (2021) 12:8. doi: 10.3389/fendo.2021.744359
26. Lira RB, Ramos AT, Nogueira RMR, de Carvalho GB, Russell JO, Tufano RP, et al. Transoral thyroidectomy (Toetva): complications, surgical time and learning curve. Oral Oncol. (2020) 110:104871. doi: 10.1016/j.oraloncology.2020.104871
27. Chai YJ, Chae S, Oh MY, Kwon H, Park WS. Transoral endoscopic thyroidectomy vestibular approach (Toetva): surgical outcomes and learning curve. J Clin Med. (2021) 10(4):14. doi: 10.3390/jcm10040863
28. Lee MJ, Oh MY, Lee JM, Sun J, Chai YJ. Comparative surgical outcomes of transoral endoscopic and robotic thyroidectomy for thyroid carcinoma: a propensity score-matched analysis. Surg Endosc. (2023) 37(2):1132–9. doi: 10.1007/s00464-022-09636-6
29. Fernandez-Ranvier G, Lieberman B, Guevara D, Voogd A, Matsuda ME, Eck K, et al. Transoral endoscopic thyroidectomy vestibular approach (Toetva) learning curve: a regression analysis of complication rates and severity. Surg Endosc. (2022) 36(7):4839–44. doi: 10.1007/s00464-021-08832-0
30. Sun HQ, Wang XJ, Zheng GB, Wu GC, Zeng QD, Zheng HT. Comparison between transoral endoscopic thyroidectomy vestibular approach (Toetva) and conventional open thyroidectomy for patients undergoing total thyroidectomy and central neck dissection: a propensity score-matching analysis. Front Oncol. (2022) 12:8. doi: 10.3389/fonc.2022.856021
31. Sun HQ, Zheng HT, Wang XJ, Zeng QD, Wang P, Wang Y. Comparison of transoral endoscopic thyroidectomy vestibular approach, total endoscopic thyroidectomy via areola approach, and conventional open thyroidectomy: a retrospective analysis of safety, trauma, and feasibility of central neck dissection in the treatment of papillary thyroid carcinoma. Surg Endosc. (2020) 34(1):268–74. doi: 10.1007/s00464-019-06762-6
32. Zhang WD, Dai L, Wang YC, Xie YY, Guo JY, Li JJ, et al. Transoral endoscopic thyroidectomy vestibular approach versus endoscopic thyroidectomy via areola approach for patients with unilateral papillary thyroid carcinoma: a retrospective study. Surg Laparosc Endosc Pct Tech. (2021) 31(5):550–3. doi: 10.1097/SLE.0000000000000932
33. Zheng GB, Xu JJ, Wu GC, Ma C, Sun HQ, Ge MH, et al. Transoral versus gasless transaxillary endoscopic thyroidectomy: a comparative study. Updates Surg. (2022) 74(1):295–302. doi: 10.1007/s13304-021-01062-y
34. Wang D, Wang YC, Zhou SL, Liu XT, Wei T, Zhu JQ, et al. Transoral thyroidectomy vestibular approach versus non-transoral endoscopic thyroidectomy: a comprehensive systematic review and meta-analysis. Surg Endosc. (2022) 36(3):1739–49. doi: 10.1007/s00464-021-08836-w
35. Dabsha A, Khairallah S, Elkharbotly I, Hossam E, Hanafy A, Kamel M, et al. Learning curve and volume outcome relationship of endoscopic trans-oral versus trans-axillary thyroidectomy; a systematic review and meta-analysis. Int J Surg. (2022) 104:9. doi: 10.1016/j.ijsu.2022.106739
36. Alnehlaoui F, Alsarraj MN, Malaki Z, Guraya SY. The effectiveness and quality of life outcomes by transoral endoscopic vestibular thyroidectomy using intraoperative indocyanin green fluorescence imaging and neuromonitoring-a cohort study. Healthcare. (2022) 10(5):13. doi: 10.3390/healthcare10050953
37. Tae K, Ji YB, Song CM, Ryu J. Robotic and endoscopic thyroid surgery: evolution and advances. Clin Exp Otorhinolaryngol. (2019) 12(1):1–11. doi: 10.21053/ceo.2018.00766
38. Shen S, Hu XC, Qu R, Guo YM, Luo LB, Chen X. Comparing quality of life between patients undergoing trans-areola endoscopic thyroid surgery and trans-oral endoscopic thyroid surgery. BMC Surg. (2021) 21(1):7. doi: 10.1186/s12893-021-01267-3
39. Song CM, Bang HS, Kim HG, Park HJ, Tae K. Health-related quality of life after transoral robotic thyroidectomy in papillary thyroid carcinoma. Surgery. (2021) 170(1):99–105. doi: 10.1016/j.surg.2021.02.042
40. Tae K, Lee DW, Bang HS, Ahn YH, Park JH, Kim DS. Sensory change in the chin and neck after transoral thyroidectomy: prospective study of mental nerve injury. Head Neck-J Sci Spec Head Neck. (2020) 42(11):3111–7. doi: 10.1002/hed.26351
41. Zhang D, Famá F, Caruso E, Pinto G, Pontin A, Pino A, et al. How to avoid and manage mental nerve injury in transoral thyroidectomy. Surg Technol Int. (2019) 35:101–6.31687788
42. Harnsberger CR, Alavi K, Davids JS, Sturrock PR, Zayaruzny M, Maykel JA. CO2 embolism can complicate transanal total mesorectal excision. Tech Coloproctol. (2018) 22(11):881–5. doi: 10.1007/s10151-018-1897-8
43. Weng YJ, Hu BL, Jiang J, Min L, Ai Q, Chen DB, et al. Delayed tracheal rupture following transoral endoscopic thyroidectomy vestibular approach: case report and review of the literature. Head Neck-J Sci Spec Head Neck. (2022) 44(11):E38–44. doi: 10.1002/hed.27180
44. Kang YJ, Cho JH, Stybayeva G, Hwang SH. Safety and efficacy of transoral robotic thyroidectomy for thyroid tumor: a systematic review and meta-analysis. Cancers (Basel). (2022) 14(17):18. doi: 10.3390/cancers14174230
45. Wang YY, Fu YL, Wu GY, Luo YZ, Yan CL, Fu JB, et al. Initial experience with transoral endoscopic thyroidectomy via the submental and vestibular approach for the treatment of thyroid cancer: a retrospective cohort study. Front Surg. (2022) 9:7. doi: 10.3389/fsurg.2022.882150
46. Lee MC, Ahn J, Choi IJ, Lee BC, Ryu J. Comparative study of gasless transaxillary, bilateral axillo-breast, unilateral axillo-breast with carbon dioxide insufflation, retroauricular, and transoral vestibular endoscopic thyroidectomy approaches at a single institution: a retrospective analysis and lessons learned. Clin Exp Otorhinolaryngol. (2022) 15(3):283–91. doi: 10.21053/ceo.2021.02285
47. Park YM, Kim DH, Moon YM, Lim JY, Choi EC, Kim SH, et al. Gasless transoral robotic thyroidectomy using the davinci Sp system: feasibility, safety, and operative technique. Oral Oncol. (2019) 95:136–42. doi: 10.1016/j.oraloncology.2019.06.003
Keywords: thyroidectomy, transoral, vestibular approach, research trends, TOET, bibliometrics
Citation: Li P, Qin H, Jin R, Zheng W, Fan P and Lyu P-f (2023) The global status and hotspots of research in the field of trans-oral endoscopic thyroidectomy (TOET) from 2008 to 2022. Front. Surg. 10:1120442. doi: 10.3389/fsurg.2023.1120442
Received: 10 December 2022; Accepted: 20 March 2023;
Published: 27 April 2023.
Edited by:
Flavio Hojaij, University of São Paulo, BrazilReviewed by:
Luiz Roberto Medina Dos Santos, Governador Celso Ramos Hospital, Brazil© 2023 Li, Qin, Jin, Zheng, Fan and Lyu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peng-fei Lyu c2t5MTI1NTg1MTE3QDE2My5jb20= Pingming Fan MTg5MDc1NzcxODBAMTYzLmNvbQ== Wuping Zheng aG56d3AyMDAwQDE2My5jb20=
†These authors have contributed equally to this work
Specialty Section: This article was submitted to Otorhinolaryngology—Head and Neck Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.