 Dengchen Li
Dengchen Li Xiaolin Li1,2,4*
Xiaolin Li1,2,4*
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg., 15 March 2023
Sec. Orthopedic Surgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1120030
This article is part of the Research TopicEquity and Bias in SurgeryView all 5 articles
Purpose: This study sought to conduct several three-dimensional measurements of the distal ulna in healthy Han Chinese, providing the anatomical basis for the diagnosis and treatment of hand trauma, distal ulnar disorders, and the design of wrist prostheses.
Methods: 50 Han Chinese men and women that underwent computed tomography (CT) scans of the distal ulnar carpus were included in the present study. A three-dimensional digital model of the distal ulna was reconstructed using Mimics software. Moreover, the anatomical data of 10 indicators were measured using MIMICS software. Each index data was measured by 2 investigators independently, and the average value was taken. The data were stratified and compared between left and right sides and men and women.
Results: A 3D digital model of the distal ulnar bone with a realistic shape was reconstructed. The 10 anatomical parameters measured are as follows: The length of the ulnar styloid process (posterior anterior), The length of the ulnar styloid process(anterior and posterior); the transverse diameter of the ulnar head; the anteroposterior diameter of the ulnar head. The radial inclination angle of the ulna; the ulnar inclination angle; the distal space between the ulna and radius; the ulnar notch angle of the lower radius. The anterior and posterior diameters of the ulnar notch of the lower radius, and the superior and inferior diameters of the ulnar notch of the lower radius. Statistical analysis showed no significant difference after stratification by laterality and gender.
Conclusion: our findings can providing the anatomical basis for the diagnosis and treatment of hand trauma, distal ulnar disorders and further improve currently available wrist joint prostheses.
Type of Study: Observational, Cross-sectional study, LOE: Level II
The wrist joint is a complex and delicate joint composed of the distal ulnar radius, eight carpal bones and the proximal end of the metacarpal bone, which is used most frequently in daily life and work and is, therefore, prone to injury. Although the radius dominates the proximal end, the ulna also plays an important role in the movement of the entire wrist joint. It has long been controversial whether to operate on the distal ulna in patients with distal radius fractures combined with distal ulnar fractures, but an increasing body of evidence from domestic and western studies suggests that operating on distal ulna fractures combined with distal radius fractures can reduce the incidence of complications, promote fracture healing, and significantly improve the wrist joint function (1–6). This finding proves that the distal ulna is a very important part of the wrist joint for normal functional activity, and the importance of the distal ulna in the wrist joint is increasingly appreciated. In severe wrist injuries, late wrist replacement is an effective way to save the function of the patient's hand, but the wrist joint prosthesis is not as good as it should be, resulting in a poor outcome of wrist joint replacement. The diagnosis and treatment of wrist disorders and the design of wrist prostheses require detailed knowledge of the anatomy of the bones that make up the wrist joint. In this respect, Moore Douglas C et al. have started to establish a database of carpal anatomy and wrist motion (7). Mona Hassan Mohammed Ali et al. (8) used 300 normal radiographs for posterior-anterior anatomical data of the wrist joint to establish a database of normal carpal anatomy in Egyptians. A domestic team represented by Professor Xu Yongqing used cadaveric specimens to measure and analyze the bones in wrist joints (9–12), yielding bony anatomical data of the carpal bones such as the lunar bone, the hook bone, the cephalic bone, and the large and small polygonal bones. Ryan Lohre (13) used x-rays to photograph the wrist joint in 60 patients and measured the distal ulnar Diaphyseal angle, but the x-rays were less accurate than CT and the study's measurements were not comprehensive enough. Due to the potential influence of different ethnic groups, data from western studies cannot be applied to the Chinese population. To our knowledge, no studies have hitherto been reported on the distal ulna abroad and in China.
The role of the distal ulna in the overall wrist joint has received increasing attention over the years, while the fine anatomy of the distal ulna has been understudied. Basic research is urgently needed to further improve the diagnosis and treatment of distal ulnar disorders and to design safer and more effective wrist prostheses. A comprehensive study of the distal ulna anatomy in normal Han Chinese is an important part of the relevant basic research. In this paper, we applied CT scan data of the wrist joint, including the distal ulna, in a normal Han Chinese population to reconstruct a 3D digital model of the wrist joint including the distal ulna, to provide a more comprehensive set of anatomical data of the distal ulna by performing 3D stereoscopic measurements of the structures related to the distal ulna.
Based on previous literature research, Combined with statistical calculation, The specimens for our study was 100, Fifty Han Chinese normal males and 50 females each,selected by random sampling (provided informed consent and approved by the ethics committee of the university), with a mean age of 37.5 (20–50 years), mean height of 168.4 (145–190 cm) and weight of 42–80 kg, with no deformity and fracture of the bilateral wrist joints, were included in this study. Anterior, oblique and lateral radiographs of bilateral wrist joints were obtained to confirm that no bone abnormalities were found in the selected volunteers.
64-row slice spiral CT (GE Healthcare, USA), MIMICS 10.0 software (Materialise, Belgium).
CT scans were performed in the Department of Radiology of the First People's Hospital affiliated with our hospital, and fine-cut uninterrupted CT scans were performed on each volunteer's bilateral wrist joints, with a scanning range of 10.0 cm above the distal radial ulnar joint to the end of the fingers, The scan parameters included: selection of bone tissue window, voltage 120 kV, 65 Ma, pixel size 0.43 mm, layer thickness 0.625 mm, matrix 512 × 512, and the scanned images were saved in DICOM format on disk.
The CT data of patients were input into the MIMICS software. After determining the orientation, the bone threshold was defined between 226-1950HU. The distal ulnar and radius were selected as the modeling range and underwent regional enhancement. Noise reduction was conducted to remove redundant data, and 3D calculations were conducted to generate the 3D model of the distal ulnar radius and hand.
Based on previous literature research, combined with our clinical experience, 10 bony anatomical datas of distal ulna were measured. (1) ulnar styloid length (posterior-anterior position) (2) ulnar styloid length (anterior-posterior position) (3) transverse ulnar head diameter (4) anterior-posterior ulnar head diameter (5) ulnar radial tilt angle (6) ulnar ulnar tilt angle (7) distal ulnar radial gap (8) ulnar notch angle of the lower radius (9) anterior-posterior radial notch diameter (10) upper and lower ulnar notch diameter of the lower radius. More details on the positioning are shown in Table 1.
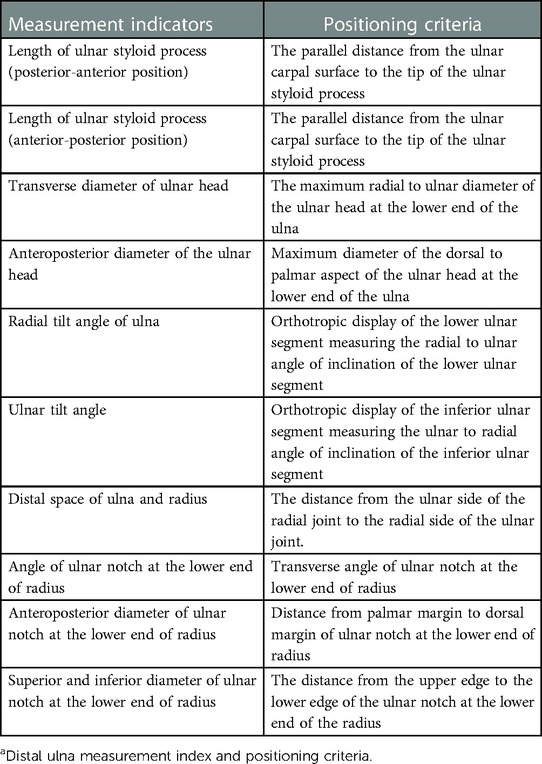
Table 1. Distal ulna measurement index and positioning criteria.a
MIMICS software was used to measure the distance or angle using the measure 3D distance or measure 3D angle tools, respectively. The measurement method is shown in Figure 1. To minimize the measurement errors caused by human factors, Each index data was measured by 2 people independently, the computer automatically generated the measurements.the average value was taken, and the results were approximated to an accuracy of 0.01. The measurement fixing points and methods are shown in Figure 1.
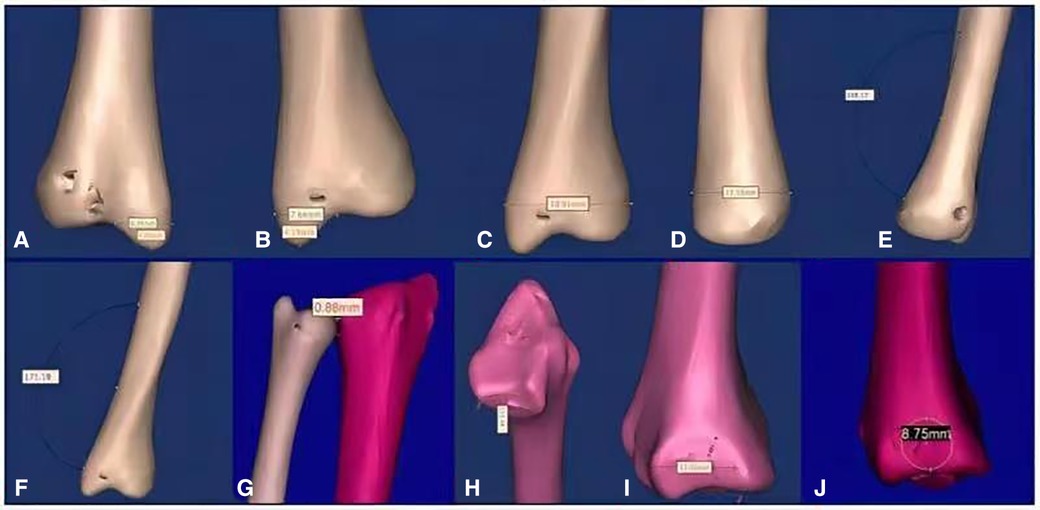
Figure 1. Measurement chart ((A) ulnar styloid length (posterior-anterior position), (B) ulnar styloid length (anterior-posterior position), (C) transverse ulnar head diameter, (D) anterior-posterior ulnar head diameter, (E) ulnar radial inclination angle, (F) ulnar ulnar inclination angle, (G) distal ulnar radial clearance, (H) inferior radial ulnar notch angle, (I) inferior radial ulnar notch anterior-posterior diameter, (J) inferior radial ulnar notch superior-inferior diameter).
Statistical Package for Social Sciences (SPSS 20.0 statistical package) was used for analysis, and data were expressed as mean ± standard deviation. Data from each group were stratified according to laterality (left vs. right side) and gender (men vs. women) and compared using an independent sample t-test. A P-value <0.05 was statistically significant.
A more comprehensive 3D reconstruction model of the whole wrist joint of a healthy Han Chinese was obtained, including the distal ulnar radius, carpal bones, metacarpals and all phalanges (Figure 2).
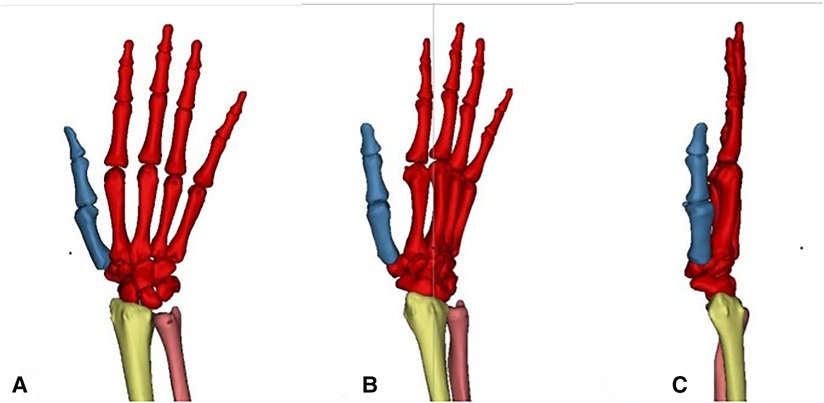
Figure 2. 3d view of the whole wrist joint [(A) positive phase (B) oblique 45° phase (C) side phase].
More detailed anatomical data of the distal ulna were obtained, as shown in Table 2.
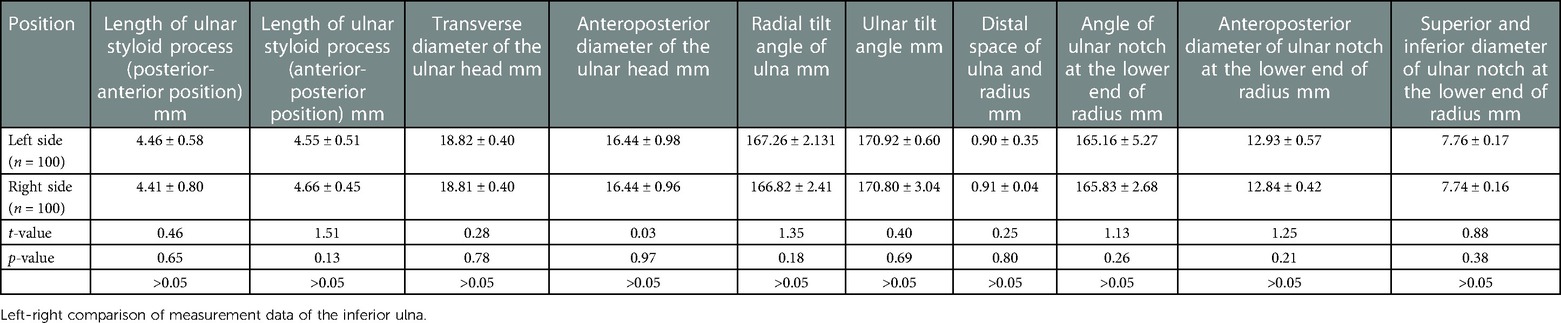
Table 2. Left-right comparison of measurement data of the inferior ulna.
Statistical analysis revealed no significant differences between the left and right sides in ulna-related indexes (Table 2). There was no statistically significant difference between men and women (Table 3).
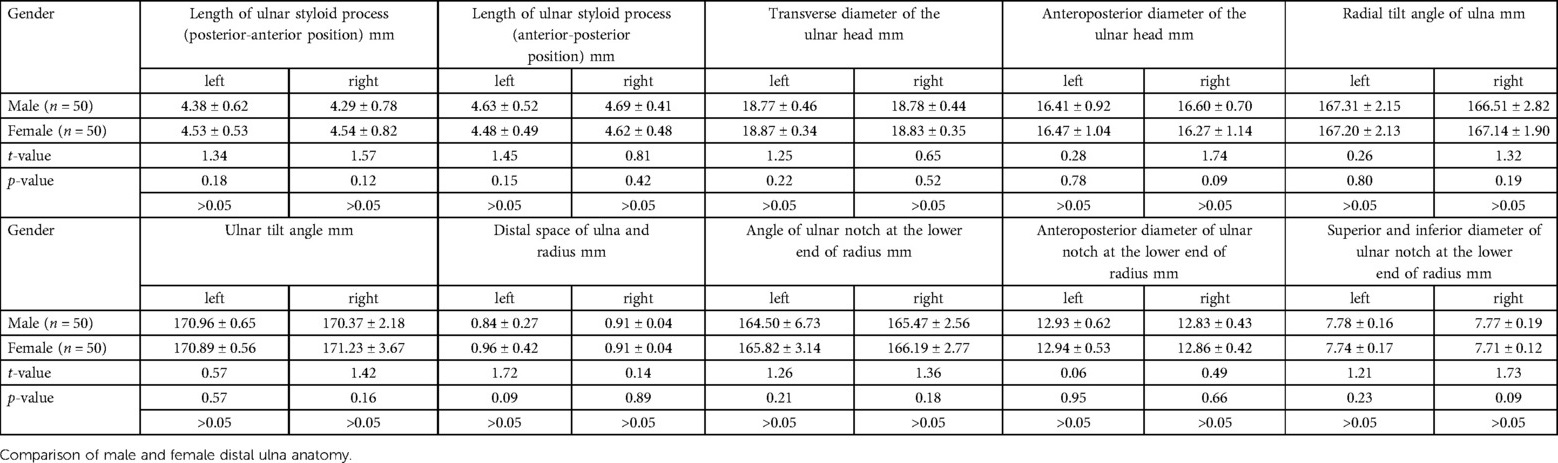
Table 3. Comparison of male and female distal ulna anatomy.
Current evidence suggests that hand injuries remain highly in common worldwide, especially in China, where industrial automation is not very high. Moreover, the requirements for post-injury function following hand injuries have increased. Although hand surgeons in China have rich clinical experience, the functional recovery of patients with wrist diseases remains unsatisfactory because of the complex characteristics of anatomy, biomechanics and injury of the wrist (14–16). The clinical incidence of distal radius fracture is high, especially in postmenopausal women because of osteoporosis. Indeed, it has been established that in this patient population, distal radius fractures are rife and generally associated with ulnar styloid process fractures. Over the years, the treatment of this patient population has predominantly focused on the distal radius with little emphasis placed on the ulnar styloid process. In recent years, much emphasis has been placed on improving the function of the wrist joint. An increasing body of evidence suggests that treating the ulnar styloid process is very important to restore the function of the wrist joint (17–26). It has been established that the ulnar styloid process is relatively small, irrespective of the measurement approach, with a length of only about 4.5-inche. In such cases, internal fixation is often difficult and mastering the direction of the needle, and the size of the screw is often challenging. Indeed, the recovery of hand function following trauma and the treatment of the ulnar styloid process after distal radius fracture requires detailed anatomical knowledge of the wrist joint and ulna to provide the theoretical basis for clinical practice.
In this study, 10 anatomical parameters of the distal ulna, including the ulnar head, styloid process of ulna, inferior radioulnar joint and distal articular surface of ulna, were observed. Importantly, we found that the end of the ulna is not a straight tube but is tilted towards the radial and ulnar sides. The radial tilt angle of the ulna is about 166°, and the ulnar tilt angle is about 170°. Herein, we investigated the radial and ulnar tilt angles of the ulna, providing a reference for the reduction and fixation of distal ulnar fractures, especially for the pre-bending angle of the internal fixation plate. Moreover, the normal length of the styloid process of the ulna was measured from the anterior and posterior directions, and it was found that the length was the same in both positions, Its length is about 4.5 mm., which indicated that the styloid process of the ulna could be entered from the metacarpal or dorsal side when fixing the styloid process of the ulna. Clinically, distal ulnar variation is common. It is widely acknowledged that ulnar impingement syndrome occurs when there is a positive ulnar variance (the distal ulna is longer than the radius) (27). However, a negative ulnar variance (the ulna is shorter than the radius) can lead to ischemic necrosis of the lunate bone (28). Accordingly, during clinical diagnosis and orthopedic osteotomy, the tilt angle of the distal ulna, the transverse diameter of the ulnar head, and the anterior and posterior diameters should be considered; restoration to its normal anatomic position is the key to successful surgical treatment. Dislocation of the lower ulnar and radial joint is a common wrist injury complication. The distal space of the ulna and radius is an important index for diagnosing dislocation and judging reduction. Due to the lack of cartilage on the x-ray film, there is a certain gap between the distal end of the ulna and the radius during normal photography. According to the measurements of the present study, the gap will not exceed one inch. A dislocation should be strongly suspected if it exceeds one inch and is accompanied by clinical symptoms. Moreover, it can guide clinical treatment and evaluate the curative effect of lower radial and ulnar joint dislocation. The four anatomical variations of the distal sigmoid notch of the radius were correlated with the stability of the inferior radioulnar joint. The instability rate of the distal radioulnar joint is higher in the Flatt type, S type and Ski type sigmoid notch., with the lowest rates associated with the C type (29). In this study, the parameters such as the angle of the ulnar notch at the lower end of the radius, the anterior and posterior diameter of the ulnar notch at the lower end of the radius, and the upper and lower diameter of the ulnar notch at the lower end of the radius were measured, which provided an accurate anatomical basis for judging the anatomical variation and the degree of variation of the sigmoid notch.
Moreover, 10 parameters were measured, no significant difference was found between the right and left sides and males and females, suggesting that laterality and gender are irrelevant during diagnosing and treating diseases related to the distal ulna. For serious wrist diseases such as wrist injury, suppurative arthritis and rheumatoid arthritis, compared with wrist fusion and proximal row carpectomy, wrist replacement brings many advantages, including better pain relief and maximum preservation of wrist function (30). However, it is not widely used in the clinic since it is prone to complications such as joint prosthesis loosening, sinking, dislocation and periprosthetic fracture (31,32). In addition to the complex structure of the wrist, the lack of joint prosthesis design is also an important reason. More anatomical studies are warranted to design a more suitable prosthesis, especially for Chinese patients. The measurement and study of the relevant parameters of the bony structure of the distal ulna, combined with the anatomical data of other bones of the wrist, can provide a bony structural basis for designing a prosthesis that is adequate for Chinese patients.
In the present study, based on the original CT scan data of normal healthy subjects, the digital visual model of the distal ulna of normal adults was established using the MIMICS 3D modeling software; the relevant anatomical datas were measured by the two-dimensional and three-dimensional measurement functions of MIMICS software. During measuring it was only necessary for the researcher to determine the starting and ending points, the computer generated the measurements automatically. The study of anatomical measurement was carried out using digital software based on the original datas of the normal human body. Compared with the traditional autopsy measurement, this method is more reproducible, the data is closer to the truth, and the fineness and credibility are improved. At the same time, a wider data source is available, and a large sample study can be carried out. In this study, a three-dimensional model of the whole wrist joint was established, and on this basis, 10 bone anatomical parameters of the distal ulna were measured, which is more comprehensive in previous studies, and the anatomical data obtained were relatively more detailed. Moreover, the number of selected specimens was small, emphasizing the need for more studies.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by the ethics committee of the yangtze university. The patients/participants provided their written informed consent to participate in this study.
This study Supported by the Teaching and Research Program of Yangtze University (JY2017016) and supported by the Innovation and Entrepreneurship training Program of Yangtze University (2019388). XL: Preside over the overall work of the project. DL: Responsible for experimental process and data measurement, and writing papers. ZH: data measurement. FP: data measurement. All authors contributed to the article and approved the submitted version.
Supported by the Teaching and Research Program of Yangtze University (JY2017016) and supported by the Innovation and Entrepreneurship training Program of Yangtze University (2019388)
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Youting D, Honghao D, Fei X, Wang Q, Zhou Y, Wei D, et al. Study on the effect of ulnar styloid process fracture type on the treatment of distal radius fracture. Chin J Orthop Trauma. (2022) 24(2):168–72. doi: 10.3760/cma.j.cn115530-20210430-00213
2. Hong Y, Yunfei H. Effect of ulnar styloid process and sigmoid notch fracture on wrist joint function in patients with distal radius fracture. Chin J Burn Wounds Ulcers. (2021) 33(1):51–4. doi: 10.3969/j.issn.1001-0726.2021.01.012
3. Peng Z, Bo J, Xiaoyi C, Wang Y, Huang W, Lai R, et al. Effect of ulnar styloid process and sigmoid notch fracture on wrist joint function in patients with distal radius fracture. J Peking Univ Med Ed. (2020) 552(3):578–81. doi: 10.19723/j.issn.1671-167X.2020.03.027
4. FranciscoRubio. Distal radioulnar joint, distal Ulna injury, and lunate facet considerations in distal radius fractures. J Orthop Trauma. (2021) 35(3):11–6. doi: 10.1097/BOT.0000000000002202
5. Suzuki T, Terasaka Y, Tomoyuki K, et al. Change of wrist motion before and after fixation of the distal radioulnar joint and resection of the distal ulna in a cadaveric model. Mod Rheumatol. (2022) 32(1):136–40. doi: 10.1080/14397595.2021.1910175
6. Rios-Russo JL, Lozada-Bado LS, de Mel S, et al. Ulnar-Sided wrist pain in the athlete: sport-specific demands, clinical presentation, and management options. Curr Sports Med Rep. (2021) 20(6):312–8. doi: 10.1249/JSR.0000000000000853
7. Moore DC, Crisco JJ, Trafton TG, et al. A digital database of wrist bone anatomy and carpal kinematics. J Biomech. (2007) 40(11):2537–42. doi: 10.1016/j.jbiomech.2006.10.041
8. Ali MM. A normal data-base of poster oanterior radiographic measurements of the wrist in healthy Egyptians. Surg Radiol Anat. (2009) 31(9):665–74. doi: 10.1007/s00276-009-0500-4
9. Wanqiu Z, Yongqing X. Clinical anatomy of Lunate bone and research progress of artificial prosthesis. Biol Orthop Mater Clin Res. (2020) 17(06):60–4. doi: 10.3969/j.issn.1672-5972.2020.06.015
10. Mingjie W, Yongqing X, Haotian L, Luo H, Wu Y, Wang Y, et al. Using mimics software to construct 3D visual anatomy of uncinate bone. Chin J Clin Anat. (2020) 38(06):652–6. doi: 10.13418/j.issn.1001-165x.2020.06.006
11. Huan W, Yongqing X, Haotian L, Fan X, He X, Zhang X, et al. Anatomical basis of cephalic bone morphology and blood supply. Chin J Clin Anat. (2020) 38(02):160–5. doi: 10.13418/j.issn.1001-165x.2020.02.012
12. Yakang W, Yongqing X, Libo Y, Zhang X, Xu Y, Luo H, et al. Anatomical study on the morphology and blood supply of large and small polygonal bone. J Clin Anat China. (2021) 39(2):134–9. doi: 10.13418/j.issn.1001-165x.2021.02.004
13. Ryan L, Parham D. Radiographic determination of the distal ulnar diaphyseal angle. J Hand Surg Am. (2022) 47(10):1015.e1–.e9. doi: 10.1016/j.jhsa.2021.08.003
14. Jin J. Analysis of related factors of postoperative functional recovery of distal radius fracture. Chin Med Innov. (2022) 19(23):168–71. doi: 10.3969/j.issn.1674-4985.2022.23.039
15. Qiang H. Influencing factors of postoperative wrist function recovery in patients with distal radius fracture. J Shandong Med Coll. (2021) 43(2):135–7. doi: 10.3969/j.issn.1674-0947.2021.02.031
16. Yongming Z, Xinjun G, Weiqiang Y, Yang W, Tian Z. Influencing factors of wrist function recovery in patients with distal radius fracture after internal fixation via brachioradialis tendon approach. Clin Medi. (2021) 41(8):69–71. doi: 10.19528/j.issn.1003-3548.2021.08.027
17. Tao W, Qinye W, Yaping L, Chang X, Xu Z. Comparison of two kinds of internal fixation in the treatment of distal radius fracture with ulnar styloid process base fracture. J Clin Orthop. (2021) 24(2):257–60. doi: 10.3969/j.issn.1008-0287.2021.02.032
18. Jihai X, Xiaofeng T, Libin C, Mao W, Wang X, Chen H, et al. Analysis of surgical effect of acute distal radioulnar joint instability caused by distal radius fracture combined with ulnar styloid process base fracture. Chin J Hand Surg. (2021) 37(02):102–5. doi: 10.3760/cma.j.cn311653-20200310-00115
19. Liuzhen X, Xuejian W, Peng X, Zhu X. Analysis of the effect of metacarpal plate combined with ulnar styloid process screw in the treatment of distal radius with ulnar styloid process fracture. Henan Med Res. (2019) 28(10):1782–4. doi: 10.3969/j.issn.1004-437X.2019.10.018
20. Zhijun L, Liangli C. Effect of surgical treatment of base fracture of ulnar styloid process on wrist function. China Med Innov. (2019) 16(10):1–5. doi: 10.3969/j.issn.1674-4985.2019.10.00
21. Jin C. Effect of surgical treatment of ulnar styloid process fracture on postoperative effect of type C distal radius fracture. Liaoning: Dalian Medical University (2021).
22. Chuanbin W. Clinical observation on the effect of type II ulnar styloid process fracture on wrist joint function after distal radius fracture. Liaoning: Dalian Medical University (2021).
23. Miyamura S, Shigi A, Kraisarin J, Omokawa S, Murase T, Yoshikawa H, et al. Impact of distal ulnar fracture malunion on distal radioulnar joint instability: a biomechanical study of the distal interosseous membrane using a cadaver model. J Hand Surg. (2017) 42(3):e185–91. doi: 10.1016/j.jhsa.2017.01.008
24. Daneshvar P, Chan R, MacDermid, Grewal R. The effects of ulnar styloid fractures on patients sustaining distal radius fractures. J Hand Surg. (2014) 39(10):1915–20. doi: 10.1016/j.jhsa.2014.05.032
25. Kim JY, Tae SK. Percutaneous distal radius–Ulna pinning of distal radius fractures to prevent settling. J Hand Surg. (2014) 39(10):1921–5. doi: 10.1016/j.jhsa.2014.07.008
26. Jorge O, Lauren V, Sophia P, Victor M, Richard C, Deana M. Effect of ulnar head offset on distal radioulnar joint stability. J Hand Surg Am. (2021) 46(9):816.e1–e7. doi: 10.1016/j.jhsa.2020.12.014
27. Wang G, Bin Z, Senhao J, Chang Z, Liang K, Li Y, et al. Progress in diagnosis and treatment of ulnar impingement syndrome. Int J Orthop. (2022) 43(2):75–8. doi: 10.3969/j.issn.1673-7083.2022.02.003
28. Chenlin L, Bin Z, Feng Z, Huang T, Wang J. Research progress on the effect of bony structural abnormality on the stability of inferior radioulnar joint. Chin Bone Trauma. (2020) 33(08):770–5. doi: 10.12200/j.issn.1003-0034.2020.08.017
29. Zijian S, Lin G, Zhi W, Meng X, Chen F, Zhang X, et al. CT Image evaluation of the effect of distal radius sigmoid notch on the stability of distal radioulnar joint. Tissue Eng Res China. (2023) 527(27):4357–61.
30. Yaqiang Z, Chengwei Y, Xianxia C, Guochao F, Xusheng L, Ping Z. One case of infection after artificial joint replacement for giant cell tumor of radius. Chin J Orthop. (2019) 27(21):2012–4. doi: 10.3977/j.issn.1005-8478.2019.21.22
31. Xingbo C, Jing D, Yongqing X. Research progress of artificial wrist prosthesis. Chin J Rehabil Reconstr Surg. (2018) 32(4):501–4. doi: 10.7507/1002-1892.201712031
Keywords: distal ulna, digital anatomy, mimics software, wrist, adult
Citation: Li D, Li X, Hou Z and Pan F (2023) Measurement of bony anatomical parameters of the distal ulna based on healthy adult data: A cross-sectional study. Front. Surg. 10:1120030. doi: 10.3389/fsurg.2023.1120030
Received: 9 December 2022; Accepted: 21 February 2023;
Published: 15 March 2023.
Edited by:
Hongyi Zhu, Shanghai Jiao Tong University, ChinaReviewed by:
Kiran Mahapure, KLE Society Hospital, India© 2023 Li, Li, Hou and Pan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaolin Li cGV0ZXJsZWU4NjlAMTYzLmNvbQ==
Specialty Section: This article was submitted to Orthopedic Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.