 Arnaud Daché1Richard Fatica2Brian R. Herts2Gordon McLennan2Erick M. Remer2Georges-Pascal Haber2
Arnaud Daché1Richard Fatica2Brian R. Herts2Gordon McLennan2Erick M. Remer2Georges-Pascal Haber2 Idir Ouzaid1*
Idir Ouzaid1*
- 1Department of Urology, Bichat Claude Bernard Hospital, University Paris-Cité, Paris, France
- 2Cleveland Clinic, Glickman Urological and Kidney Institute, Cleveland, OH, United States
Introduction and objective: This study aimed to identify clinical features representing predictive factors of active treatment (AT) compared to active surveillance (AS) for renal angiomyolipoma (AML).
Patients and methods: From 1990 to 2020, patients referred to two institutions for a renal mass and diagnosed with an AML based on typical features on CT were included in the analysis. The study population was divided into two groups based on the treatment received: active surveillance (AS) or active treatment (AT). Age, gender, tuberous sclerosis syndrome, tumor size, contralateral kidney disease, renal function, year of diagnosis, and symptoms at presentation were assessed as potential predictive factors of active treatment using a logistic regression model in univariate and multivariate analyses.
Results: In total, 253 patients (mean age 52.3 ± 15.7 years; 70% women; 70.9% incidentally diagnosed) were included in the analysis. One hundred and nine (43%) received AS, whereas 144 (57%) were actively treated. For univariate analysis, age, tuberous sclerosis complex syndrome, tumor size, symptoms at presentation, and contralateral kidney disease were found to be predictors of AT. Only tumor size (p < 0.001) and the year of diagnosis (p < 0.001) remained significant for multivariable analyses. The likelihood of being managed with AS evolved over the study period and was 50% and 75% when diagnosed before and after 2010, respectively. With respect to size, 4-cm and 6-cm tumors had a probability of 50% and 75% of being treated with AS, respectively.
Conclusion: The present analysis from a high-volume institution provides evidence that the management of renal masses with typical radiological features of AML has markedly changed over the last three decades with a trend toward AS over AT. Tumor size and the year of diagnosis were significant factors for the treatment strategies.
Introduction
Angiomyolipoma (AML) is the only benign renal tumor that can be confidently diagnosed by cross-sectional imaging, with fat density within a lesion as a diagnostic hallmark (1, 2). Regions with Hounsfield unit densities of −80 or less are diagnostic of gross fat within a lesion and considered diagnostic of AML. Diagnosis is more difficult for the less common variant of AML with minimal fat at imaging. For these lesions, findings of more than 20 pixels with attenuation less than −20 HU or more than 5 pixels with attenuation less than −30 HU, when present, were shown to have a positive predictive value of 100% but are not sensitive for a diagnosis of minimal-fat AML (3).
As a nonmalignant tumor, its prognosis is related to potential bulking effect symptoms including flank pain, hematuria, and hemorrhage. Spontaneous renal hemorrhage, also known as Wunderlich's syndrome, is a rare but potentially life-threatening complication that occurs in up to 10% of patients, especially in the setting of larger tumors (4–6).
As a result, surgical excision was considered the main treatment option in young patients with large and/or symptomatic diseases (7). Recently, minimally invasive treatment options have been described including cryoablation and angioembolization (2, 8, 9). The obvious benefits of active surveillance (AS) include maximum preservation of normal functional renal parenchyma and avoidance of the morbidity associated with active treatment (AT).
Most practice guidelines for AML are empirically derived upon outcomes of retrospective studies, with a limited sample size over a short period. Moreover, given disease incidence and prognosis, randomized trials are not likely to be conducted. Consequently, evidence is lacking on whether these tumors should be treated pre-emptively or treatment be deferred until the patient becomes symptomatic.
High-volume referrals to our institutions have allowed for the acquisition of a large data set on AML. This study aimed to review our institutional 30 years’ experience in the management of these tumors and identify clinical drivers for AT as opposed to AS.
Patients and methods
In this HIPAA-compliant retrospective study, we reviewed the charts of patients referred to our institution from 1990 to 2020 for renal mass, with a radiological diagnosis of AML based on CT findings (identification of fat-containing mass). Patients were grouped, according to their treatment, into either AS or AT. AS consisted of 6-month, 12-month, and then yearly monitoring, which consisted of a physical exam and one of the following imaging modalities: ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI). AT included open, laparoscopic, and robotic partial or radical nephrectomy, angioembolization, and cryoablation. The diagnosis of AML was confirmed at final pathology only for patients who underwent surgery or percutaneous biopsy.
Then, clinical features predicting the likelihood of one treatment option over the other were assessed. Age, gender, tuberous sclerosis complex syndrome, tumor size, year of diagnosis, contralateral kidney disease, chronic kidney disease (CKD) stage, and clinical presentation were assessed as potential factors associated with a higher likelihood of AT.
Statistical analyses
Data are presented as means ± standard deviations (SDs) or proportions when appropriate. Categorical and continuous variables were assessed using χ2 and Student’s t tests, as appropriate. Univariable and multivariable cox regression models were used to determine the association between active treatment and the clinical features of AML. Logistic fit and inverse prediction of AS by significant factors on the multivariable analysis were plotted. All p-values were two-sided, and statistical significance was defined as a p < 0.05. Statistical analyses were performed using SPSS (IBM SPSS Statistics for Windows, Version 24.0, IBM Corp., Armonk, NY, USA).
Results
In total, 253 patients met the inclusion criteria and were included in the analysis. The mean age of the study population was 52.3 ± 15.7 years. Seventy-seven percent of patients were women. At presentation, 70.9% were asymptomatic. Hematuria (14.1%) and flank pain (9.7%) were the most commonly reported symptoms. Table 1 summarizes the baseline patient characteristics.
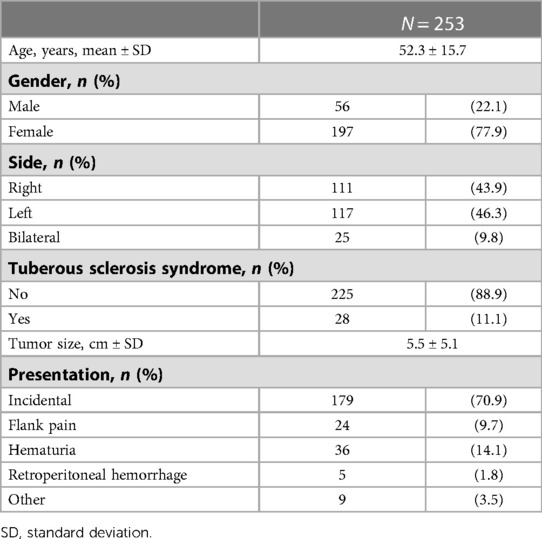
Table 1. Patients’ characteristics.
Of the selected patients, 109 (43%) and 144 (57%) underwent AS and AT, respectively. Surgical excision was the most frequent treatment option (88%), followed by angioembolization (9%) and cryoablation (3%). Figure 1 details the different treatment options.

Figure 1. Active treatment options. OPN, open partial nephrectomy; LPN, laparoscopic partial nephrectomy; RALPN, robot-assisted laparoscopic partial nephrectomy ORN, open radical nephrectomy; LRN, laparoscopic radical nephrectomy; RALRN, robot-assisted laparoscopic radical nephrectomy.
On univariate analyses, age at diagnosis, TSC, tumor size, symptoms at presentation, contralateral kidney disease, and year of diagnosis were all associated with AT (Table 2). All of these factors, except tumor size and year of diagnosis, were not significant in multivariate analysis (Table 3).
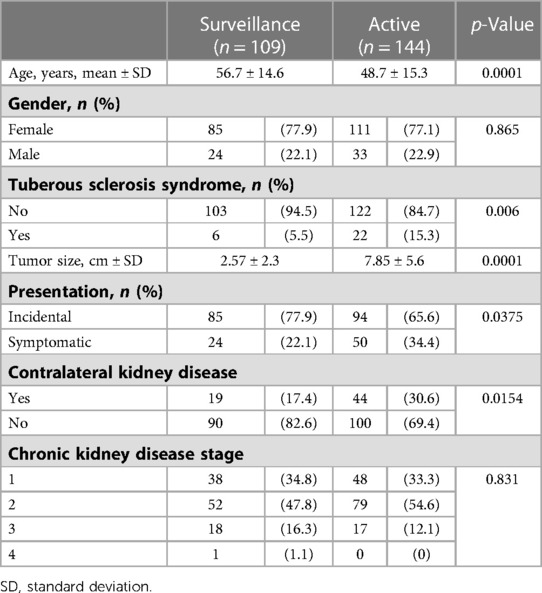
Table 2. Univariable analysis of the likelihood of active treatment vs. surveillance.
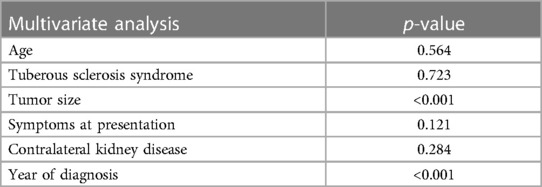
Table 3. Multivariable analysis of factors predicting active treatment.
Based on the logistic fit plot analyses, recent tumors were more likely to be treated with AS. For example, the probability of being managed with AS was 50% and 75% before and after 2010, respectively. The probability of being treated with AS was also inversely proportional to tumor size. A patient diagnosed with 4-cm and 6-cm tumors had a probability of 50% and 25% of being treated with AS, respectively (Figure 2).
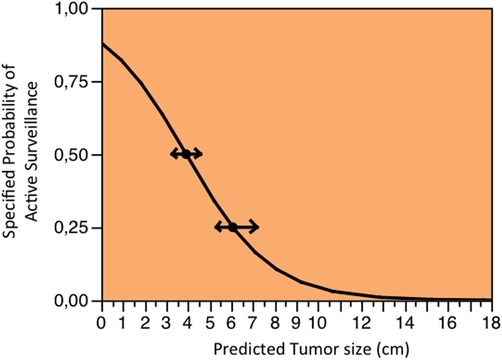
Figure 2. Specific probability of being treated with active surveillance according to the tumor size. A patient diagnosed with 4-cm and 6-cm tumors had a probability of 50% and 25% (arrows) of being treated with active surveillance, respectively.
Discussion
According to current guidelines (Level C recommendation), primary indications for intervention for patients with an AML include symptoms such as pain, bleeding, or suspected malignancy (7). Thus, prophylactic intervention seems justifiable for large tumors (the recommended threshold of intervention is >4 cm), women of childbearing age, or patients in whom follow-up or access to emergency care may be inadequate (7, 10).
With respect to these guidelines, our results suggest that only tumor size was associated with AT on multivariate analysis. In addition, the year of diagnosis was also highly predictive of AT. Conversely, gender, age, and symptoms were not associated with AS.
Mues and colleagues investigated factors predicting surgical intervention or embolization in a series of 91 AMLs (11). They used a regression model to assess predictors of AT in patients treated initially with AS. However, only three patients failed AS in the analysis, which might have undermined the power of their statistical model. We found that size coded as a continuous variable is strongly associated with AT, as outlined by Rosales and colleagues, who assessed factors predictive of AT in a cohort of patients with cortical renal tumors and treated with AS (12).
The radiologic appearance of the tumor is an important feature in the decision-making process and inpatient counseling. In fact, typical fatty masses are more likely to be watched, whereas fat-poor AMLs are resected because of suspicion of renal cell carcinoma (RCC). Selecting only typical AMLs on CT offsets this important confounding factor.
Like all renal masses, the trend in the management of AMLs is moving toward nephron-sparing strategies (13). Our study observed an increase in the adoption of AS since 2008. This increase can be intuitively attributed to the increased incidence of small renal masses due to the widespread use of cross-sectional imaging (14). Also, data from observational studies on RCC highlighted the potential benefits of nephron-sparing strategies on long-term cardiovascular morbidity and renal function (15). This practice can be extrapolated to all renal masses.
Our study carries some limitations. First, while it is notable that our analysis was conducted over a 30-year period, technical advances have occurred over this time that have impacted the management of AMLs. These advances have occurred not only in the fields of minimally invasive urologic surgery and minimally invasive radiological procedures but also in medical imaging. It can be estimated that CT diagnosis yields improved by 10% over the last decade (16–19). Consequently, AMLs were more likely to be treated with AT during the first period of this study, regardless of clinical presentation and size. Second, despite the high diagnostic accuracy of current cross-sectional imaging, the diagnosis of AMLs could not be confirmed in most of our AS patients since they have not systematically undergone a percutaneous renal biopsy. Also, we are cautious that some masses treated with AS without prior percutaneous biopsy might be malignant in nature since fat-containing RCC has already been reported (20). Finally, due to the retrospective design of this study, the superiority of one treatment vs. the other cannot adequately be compared because AT precedes the AS period, ultimately introducing bias. Ideally, a prospective randomized study would compare both treatment options with respect to subsequent cost and morbidity. Such a study is difficult to design due to the low incidence of AMLs and the high proportion of incidentally diagnosed AMLs. Nevertheless, it is noteworthy to assess whether the current threshold (4 cm) for AT should be revised and a larger-size threshold should be established.
Conclusion
Our high-volume, single-institution analysis provides evidence that managing renal masses with typical radiological features of AML has changed markedly over the last three decades toward AS over AT. Tumor size and year of diagnosis were the identified significant factors in the choice of intervention or surveillance at diagnosis. Additional research areas need to address whether prophylactic intervention in patients with large asymptomatic AML is cost-effective.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Cleveland Clinic. Written informed consent for participation was not required for this study in accordance with national legislation and institutional requirements.
Author contributions
AD: Manuscript drafting. RF: Data acquisition. BRH: Data acquisition. GM: Data acquisition. EMR: Data acquisition. G-PH: Supervision. IO: Supervision and manuscript drafting. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Tamboli P, Ro JY, Amin MB, Ligato S, Ayala AG. Benign tumors and tumor-like lesions of the adult kidney. Part II: benign mesenchymal and mixed neoplasms, and tumor-like lesions. Adv Anat Pathol. (2000) 7:47–66. doi: 10.1097/00125480-200007010-00007
2. Sivalingam S, Nakada SY. Contemporary minimally invasive treatment options for renal angiomyolipomas. Curr Urol Rep. (2013) 14:147–53. doi: 10.1007/s11934-013-0311-3
3. Simpfendorfer C, Herts BR, Motta-Ramirez GA, Lockwood DS, Zhou M, Leiber M, et al. Angiomyolipoma with minimal fat on MDCT: can counts of negative-attenuation pixels aid diagnosis? AJR Am J Roentgenol. (2009) 192:438–43. doi: 10.2214/AJR.08.1180
4. Oesterling JE, Fishman EK, Goldman SM, Marshall FF. The management of renal angiomyolipoma. J Urol. (1986) 135:1121–4. doi: 10.1016/S0022-5347(17)46013-7
6. Steiner MS, Goldman SM, Fishman EK, Marshall FF. The natural history of renal angiomyolipoma. J Urol. (1993) 150:1782–6. doi: 10.1016/S0022-5347(17)35895-0
7. Ljungberg B, Cowan NC, Hanbury DC, Hora M, Kuczyk MA, Axel S, Merseburger AS, et al. EAU guidelines on renal cell carcinoma: the 2010 update. Eur Urol. (2010) 58:398–406. doi: 10.1016/j.eururo.2010.06.032
8. Chan CK, Yu S, Yip S, Lee P. The efficacy, safety and durability of selective renal arterial embolization in treating symptomatic and asymptomatic renal angiomyolipoma. Urology. (2011) 77:642–8. doi: 10.1016/j.urology.2010.08.040
9. Ramon J, Rimon U, Garniek A, Golan G, Bensaid P, Kitrey ND, et al. Renal angiomyolipoma: long-term results following selective arterial embolization. Eur Urol. (2009) 55:1155–61. doi: 10.1016/j.eururo.2008.04.025
11. Mues AC, Palacios JM, Haramis G, Casazza C, Badani K, Gupta M, et al. Contemporary experience in the management of angiomyolipoma. J Endourol. (2010) 24:1883–6. doi: 10.1089/end.2010.0223
12. Rosales JC, Haramis G, Moreno J, Badani K, Mitchell C, Benson MC, et al. Active surveillance for renal cortical neoplasms. J Urol. (2010) 183:1698–702. doi: 10.1016/j.juro.2010.01.024
13. Sun M, Abdollah F, Bianchi M, Trinh QD, Jeldres C, Thuret R, et al. Treatment management of small renal masses in the 21st century: a paradigm shift. Ann Surg Oncol. (2012) 19:2380–7. doi: 10.1245/s10434-012-2247-0
14. Gupta K, Miller JD, Li JZ, Russell MW, Charbonneau C. Epidemiologic and socioeconomic burden of metastatic renal cell carcinoma (mRCC): a literature review. Cancer Treat Rev. (2008) 34:193–205. doi: 10.1016/j.ctrv.2007.12.001
15. Weight CJ, Larson BT, Fergany AF, Gao T, Lane BR, Campbell SC, et al. Nephrectomy induced chronic renal insufficiency is associated with increased risk of cardiovascular death and death from any cause in patients with localized cT1b renal masses. J Urol. (2010) 183:1317–23. doi: 10.1016/j.juro.2009.12.030
16. Bret PM, Bretagnolle M, Gaillard D, Plauchu H, Labadie M, Lapray JF, et al. Small, asymptomatic angiomyolipomas of the kidney. Radiology. (1985) 154:7–10. doi: 10.1148/radiology.154.1.3880613
17. Halpenny D, Snow A, McNeill G, Torreggiani WC. The radiological diagnosis and treatment of renal angiomyolipoma-current status. Clin Radiol. (2010) 65:99–108. doi: 10.1016/j.crad.2009.09.014
18. Kim JK, Park SY, Shon JH, Cho KS. Angiomyolipoma with minimal fat: differentiation from renal cell carcinoma at biphasic helical CT. Radiology. (2004) 230:677–84. doi: 10.1148/radiol.2303030003
19. Lemaitre L, Claudon M, Dubrulle F, Mazeman E. Imaging of angiomyolipomas. Semin Ultrasound CT MR. (1997) 18:100–14. doi: 10.1016/S0887-2171(97)90054-8
Keywords: angiomyolipomas, nephron-sparing surgery, angioembolization, active surveillance, renal tumors
Citation: Daché A, Fatica R, Herts BR, McLennan G, Remer EM, Haber G-P and Ouzaid I (2023) Factors predicting the active treatment of renal angiomyolipoma: 30 years of experience in two tertiary referral centers. Front. Surg. 10:1094806. doi: 10.3389/fsurg.2023.1094806
Received: 10 November 2022; Accepted: 27 March 2023;
Published: 11 May 2023.
Edited by:
Evanguelos Nicolas Xylinas, Hôpital Bichat-Claude-Bernard, FranceReviewed by:
Hanen Bouaziz, Salah Azaiez Institute, TunisiaMichael Kohrman, Northeast Ohio Medical University, United States
© 2023 Daché, Fatica, Herts, McLennan, Remer, Haber and Ouzaid. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Idir Ouzaid aWRpci5vdXphaWRAZnJlZS5mcg==
Specialty Section: This article was submitted to Genitourinary Surgery, a section of the journal Frontiers in Surgery