 Wei-Shang Li
Wei-Shang Li Qi Yan2
Qi Yan2 Lin Cong
Lin Cong- 1Department of Orthopedic Surgery, The First Hospital of China Medical University, Shenyang, China
- 2Department of Surgery, University of Texas Health San Antonio, San Antonio, TX, United States
- 3Department of Obstetrics and Gynecology, Shengjing Hospital of China Medical University, Shenyang, China
- 4Disease Control and Prevention Center of China Railway Shenyang Bureau Group Corporation, Shenyang, China
Objective: To evaluate the global research productivity in the field of discectomy for lumbar disc herniation (LDH) through bibliometric analysis and mapping knowledge domains.
Methods: A systematic literature search was performed on the Web of Science (WoS), including the Science Citation Index Expanded (SCIE) database and PubMed. The number of publications, countries of publications, journals of publications, total citation frequency, impact factors of journals, and Institutional sources were analyzed by Microsoft Excel 2019, the Online Analysis Platform of Bibliometrics, and VOSviewer. Hotspots were also analyzed and visualized based on VOSviewer.
Results: A total of 2,066 papers were identified. The United States ranked first in the number of total citations (7,970). China ranked first in the number of publications (556, 26.9%), which has surpassed the United States in terms of the number of publications published annually since 2016. Wooridul Spine Hospital published the most papers (43). For journals, Spine has published the largest number of papers (289) in this field with the most citation frequencies (6,607). Hotspots could be divided into three clusters: surgery, lumbar disc herniation, and diagnoses. The most recent topic that appeared was symptomatic re-herniation.
Conclusions: The United States is the most significant contributor to the development of discectomy for LDH. The current research focus of discectomy on LDH was the comparison between surgical approaches and evaluation of current minimally invasive discectomy. At present, minimally invasive techniques, such as endoscopic discectomy, cannot completely replace non-endoscopic discectomy (open discectomy and microdiscectomy) through bibliometric analysis and mapping knowledge domains.
Introduction
Sciatica in adults is mostly caused by lumbar disc herniation (LDH) (1), leading to significant physical disabilities and global health costs (2). Symptomatic LDH is a pathological process that requires surgical intervention after the failure of conservative treatment. In 1934, Mixter and Barr reported the first surgical intervention for symptomatic LDH, namely, open discectomy (3). With the continuous improvement of surgical techniques and instruments, many types of minimally invasive procedures have been developed. Moreover, the application of endoscopy is an innovation for the surgical treatment of symptomatic LDH. Minimally invasive discectomy could be classified into microdiscectomy (MD), microendoscopic discectomy (MED), percutaneous endoscopic lumbar discectomy (PELD), and full-endoscopic discectomy (FED). Both PELD and FED contain two different surgical approaches: transforaminal approach or interlaminar approach (4, 5), whereas these endoscopic procedures do not present a trend of iterative replacement (6–9). At present, the gold standard treatment for symptomatic LDH is still microdiscectomy.
Bibliometrics is a method to assess the trends in global research productivity based on literature databases and literature metrology characteristics. Moreover, its application has become more and more mature in various medical disciplines in recent years, including spinal surgery (10–17). Based on literature data and visualization technology, bibliometrics could be used to display the interaction, crossover, evolution, and derivation among information groups in a certain discipline. Moreover, bibliometrics could provide researchers with a new way to understand the connection between scientific issues and assist them to make superior decisions in either clinical practice or basic medical research. As far as we know, the bibliometric analysis of treatment for LDH has not been reported yet. Therefore, the objective of this study was to evaluate the global research productivity in discectomy on LDH through bibliometric analysis and mapping knowledge domains. The current research status in discectomy on LDH could be explained through the time and spatial distribution of scientific research as well as the analysis of literature topics. Moreover, the future research trend for the treatment of LDH could be predicted reasonably.
Materials and methods
Data source and search strategy
A systematic literature search was performed on PubMed, Web of Science (WoS), and the Science Citation Index Expanded (SCIE) database. The search terms were as follows: theme = ((discectomy) AND (lumbar disc herniation or lumbar disk herniation OR LDH)) AND publishing year = (all time) based on MeSH on PubMed. Original articles and reviews were identified.
Information extraction
Two researchers extracted the data from databases and imported it into Microsoft Excel 2019 independently. The data were imported as follows: number of publications, countries of publications, journals of publications, authors of publications, total citations, impact factors of journals, and institution sources. Disagreements between the two researchers were resolved by consensus after discussion.
Statistical analysis
The number of publications, contributive countries of publications, contributive journals of publications, total citation frequency, and impact factors of journals and institution sources were analyzed by Microsoft Excel 2019 (Microsoft Corporation, Santa Rosa, CA, United States), which were visualized by GraphPad Prism 8 (GraphPad Software Inc., CA, United States). VOSviewer (Leiden University, Leiden, The Netherlands) is used for visualizing the bibliometric mapping, including literature coupling, co-citation, collaboration, and co-word analysis (18). VOSviewer can also be used to create a map based on text data to mine the themes of articles, which allowed us to analyze the hot spots in certain fields visualized as clusters of masterpieces. The online analysis platform of bibliometrics (http://bibliometric.com/) was also used for analyzing and visualizing the data extracted from databases as a complement.
Results
Global publications
A total of 2,066 papers were identified in this analysis. An overview of global publications in discectomy on LDH over the past 20 years is shown in Figure 1. The total number of publications was on the increase over the years (Figure 1A). The research of China in this field was relatively late, and China has surpassed the United States in terms of the number of publications published annually since 2016 (Figure 1B).
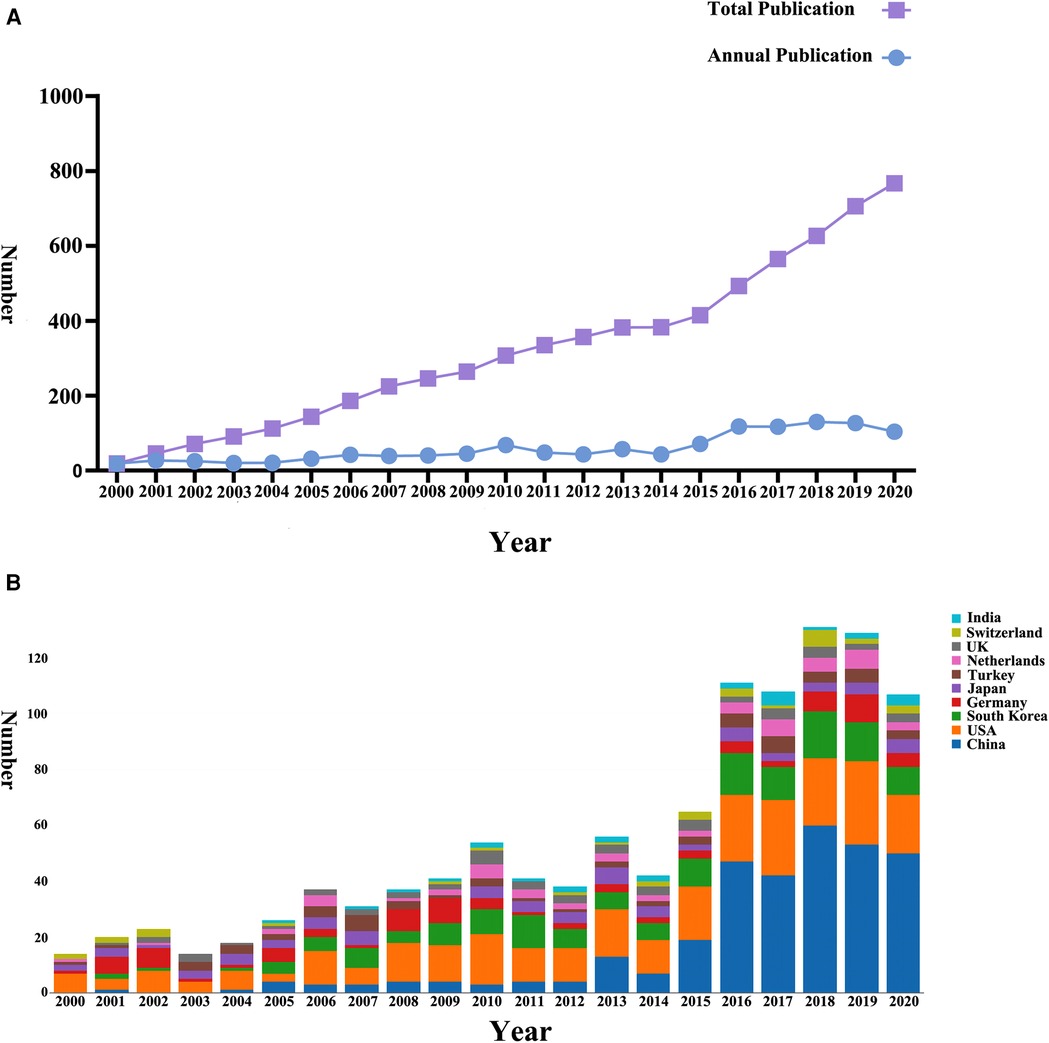
Figure 1. Global trends in research on discectomy from 2000 to 2020. (A) The number of publications on discectomy worldwide. (B) The number of publications on discectomy worldwide classified by country.
Highly contributive country, institutions and journals
The top 10 contributing countries, institutions, and journals by the number of publications are shown in Figure 2 and Table 1. China ranked first in the number of publications (556, 26.9%), followed by the United States (526, 25.5%). The United States ranked first in the number of total citations (7,970), followed by South Korea (3,471). As for institutions, Wooridul Spine Hospital published the most papers (43) and Tongji University ranked second in the number of publications (19). For journals, Spine has published the largest number of papers (289) in discectomy on LDH with the most citation frequencies (6,607). World Neurosurgery ranked second in the number of publications (163). European Spine Journal ranked second in citation frequencies (2586).

Figure 2. (A) The sum number and citation frequency of publications on discectomy from the top 10 contributing countries/regions. (B) The sum number and citation frequency of publications on discectomy from the top 10 contributing institutions. (C) The sum number and citation frequency of publications on discectomy from the top 10 contributing journals. (D) The top 20 keywords of occurrence frequency on discectomy.
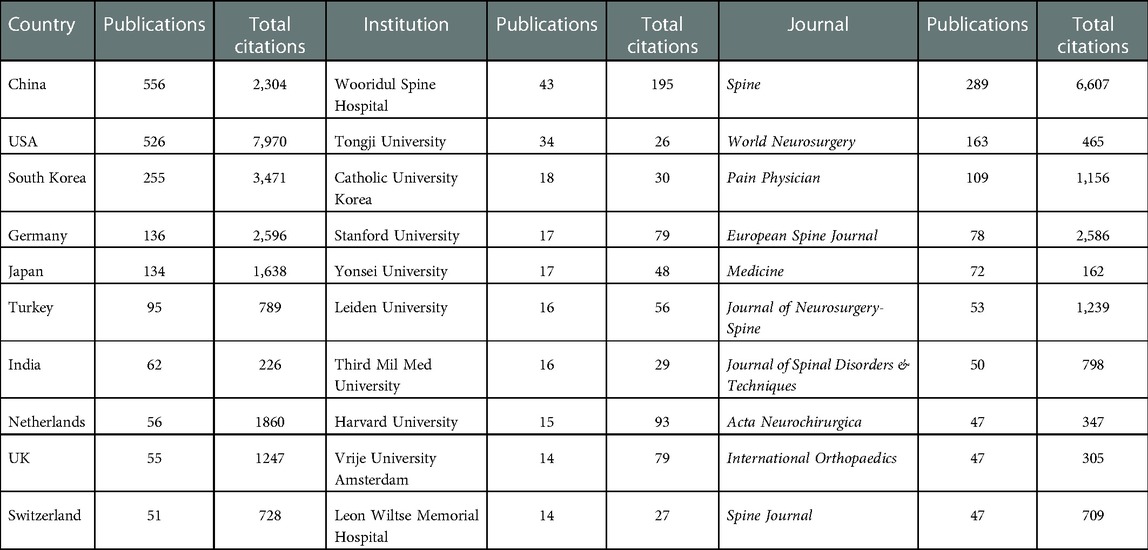
Table 1. The top 10 countries/regions, institutions, and journals contributing to publications in discectomy.
Analysis of keywords and hotspot
The top 20 keywords sorted by frequency of occurrence are shown in Figure 2D. A bibliometric map based on text data Generated by VOSviewer shown the themes of papers in discectomy on LDH classified according to four different colored clusters in Figure 3A. The size of each node represented its weight in the graph. Among the four-color clusters, surgery was the hotspot of papers in the red and yellow clusters on the upper left corner (Clusters 1 and 4); lumbar disc herniation was the hotspot of papers in green clusters on the right (Cluster 2) and those diagnoses of LDH were the hotspot of papers in blue clusters at the bottom (Cluster 3). A chronological distribution of the topics of papers in discectomy on LDH is shown in Figure 3B. According to the average publication year, the most recent topic to appear was symptomatic re-herniation, which occurred 27 times in cluster 2. The earliest topic was chemonucleolysis, which occurred 63 times in cluster 4. The 10 most recent hotspots according to the average publication year are shown in Table 2.
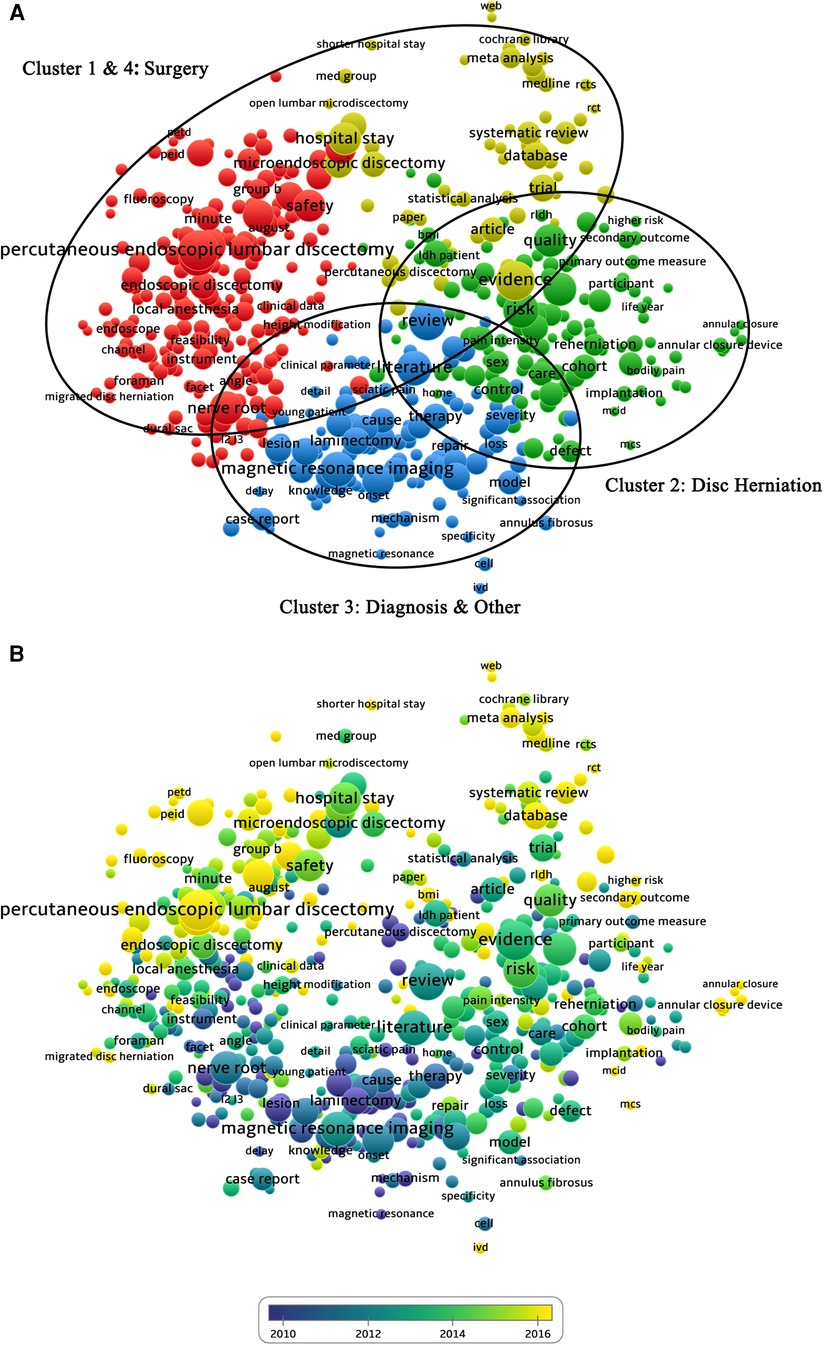
Figure 3. (A) Mapping of hotspots in the research on discectomy; the size of the points represents the frequency, and the hotspots are divided into four clusters: surgery (red and yellow clusters in the upper left corner), lumbar disc herniation (green clusters on the right), and diagnoses (blue clusters at the bottom). (B) Distribution of hotspots according to the appearance for the average time; hotspots in blue appeared earlier than those in yellow.
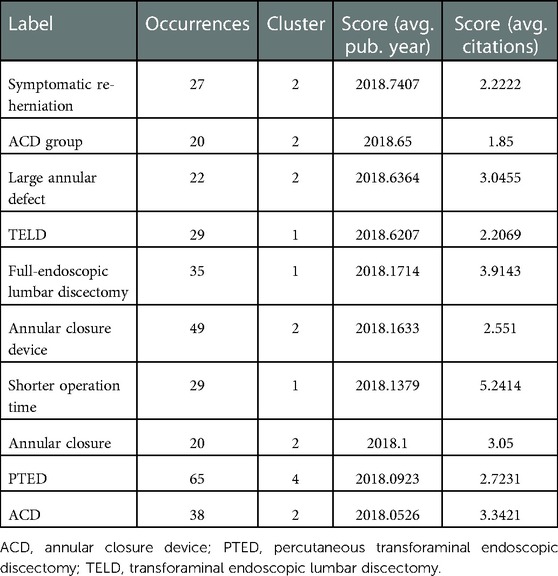
Table 2. The 10 most recent hotspots according to the average publication year.
Analysis of citation situation
The citation status of papers in discectomy on LDH is shown in Figure 4, which could be divided into four different-color clusters. The connection represented the degree of connection between each node in this graph. The left red cluster represented the references of open lumbar discectomy (Cluster 1), the middle blue cluster represented the references of microdiscectomy (Cluster 2), and the right green cluster represented the references of endoscopic discectomy (Cluster 3). The yellow cluster in the upper left corner represented references to recurrent lumbar disc herniation (Cluster 4).
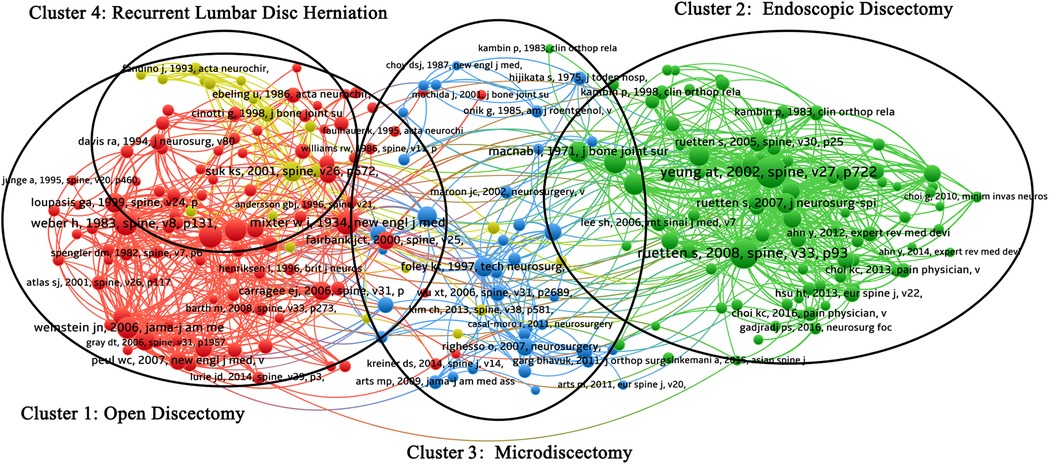
Figure 4. Mapping of citation network related to discectomy. Given the large number of cited references, this study only selected papers cited more than 20 times for analysis and a total 240 papers were included. A line between two points means that both were cited in one paper. Points are divided into four clusters: clusters one (red) are papers related to open lumbar discectomy; clusters two (green) are papers related to endoscopic discectomy; cluster three (blue) contains papers related to microdiscectomy and microendoscopic discectomy; and cluster four (yellow) contains papers related to recurrent lumbar disc herniation.
Discussion
With the improvement of patients' requirements for prognosis, discectomy continued to improve as the treatment for symptomatic LDH under the general trend of minimally invasive surgery. By 2020, China ranked the first in the number of publications in the field of discectomy in worldwide (556, 26.9%), followed by the United States (526, 25.5%). However, the citation frequency of Chinese articles was less than that of the United States. In terms of time, China has surpassed the United States in terms of the number of publications published annually since 2016. China started to get involved in the research of discectomy on LDH relatively late, whereas the incidence rate and absolute value of LDH are relatively high in China based on great population, which could provide great number of clinical data. China has considerable experience in the application of various discectomy approaches to LDH. However, none of these surgical approaches to discectomy was invented by the Chinese. China was not as contributive as other countries such as the United States and South Korea, when it came to the creation or renewal of surgical techniques. Similar situations existed in the research institutions. Among the top 10 institutions that contributed the most publications, the number of citations from Chinese institutions was relatively small compared with institutions in other countries. These findings in this study suggest that the United States is the most significant contributor to the development of discectomy in LDH. China developed rapidly in discectomy on LDH but lack of research depth and citation.
For the analysis of the citation situation, Clusters 1–3 were classified according to surgical techniques. Cluster 1 mainly focused on open discectomy, and the representative highly cited articles are published by Weber et al. in Spine (118 citations) (20), Carragee et al. in Journal of Bone and Joint Surgery (116 citations) (21), and Mixter and Barr in New England Journal of Medicine (116 citations) (3). Cluster 2 mainly focused on endoscopic discectomy, and the representative highly cited articles are published by Yeung and Tsou in Spine (198 citations) (22), Ruetten et al. in Spine (172 citations) (5), and Mayer and Brock in Journal of Neurosurgery (101 citations) (4). Cluster 3 focused on microdiscectomy and microendoscopic discectomy, and the representative highly cited articles are published by Caspar et al. in Advances in Neurosurgery (81 citations) (23), Maurice et al. in Techniques in Neurosurgery (80 citations) (24), and Perez-Cruet et al. in Neurosurgery (65 citations) (25). Cluster 4 mainly focused on recurrent lumbar disc herniation, and the representative highly cited articles are published by Suk et al. in Spine (87 citations) (26), Cinotti et al. in Journal of Bone and Joint Surgery (55 citations) (27), and Swartz and Trost in Neurosurgical Focus (47 citations) (19). We found that there were miscellaneous interactions between clusters 1 and 4. The main reason for this finding could be that the researchers found that the surgical intervention was not associated with well-controlled postoperative recurrence in the early stages of discectomy development. Therefore, the papers focusing on recurrent lumbar disc herniation after surgery were performed greatly, which interacted with the papers on open surgery. These papers also prompted researchers and clinicians to improve the approaches of discectomy. With the further development of surgical techniques, the recurrence rate has been controlled and is now in a stable state (6, 28–30). Whereas symptomatic recurrence was still a research hotspot and regarded as one aspect of evaluating surgery in papers at present. Moreover, we found that the highly cited literature studies in each cluster were the first reports or randomized controlled trials of a certain surgical technique. Although systematic reviews and meta-analyses based on the data extracted from these clinical studies were also hotspots, the frequency of citations of these systematic reviews and meta-analyses was lower, which may indicate that the evaluation of different surgical procedures in the field of discectomy on LDH was still not uniform.
In the top 20 keywords sorted by frequency of occurrence, half were associated with surgical techniques and the research of minimally invasive surgery occupied a quite dominant position. In the bibliometric map generated by VOSviewer, clusters 1 and 4 mainly focus on surgical techniques and postoperative clinical outcomes in Figure 3A. The node of “percutaneous endoscopic lumbar discectomy” in cluster 1 ranked first in occurrence. The hotspots of papers in discectomy on LDH were mainly on the evaluation of surgical techniques and the comparison of different surgical techniques. The nodes of “Trial,” “meta-analysis,” and “systemic review” in Cluster 4 indicated that the evaluation of surgical techniques has mostly relied on clinical controlled studies, and different surgical techniques were compared through meta-analysis or systematic review. According to the time-sequence analysis, the early research of discectomy on LDH mainly focused on the pathogenesis of LDH, sciatica, lower back pain, basic surgical procedures, and postoperative failure syndrome. And most recent research focused on minimally invasive surgery and the evaluation of postoperative clinical outcomes. In this bibliometric analysis, the research chronology of discectomy on LDH was consistent with the general law of occurrence and development in modern medicine. Minimally invasive surgery is the inevitable trend of surgery development. However, the real problem is to prove that a newly invented minimally invasive surgery can actually achieve the desired effect, which is equal to microincision. In the current evaluation system, surgical damage is evaluated by a number of indicators, such as operation time, length of hospital stay, intraoperative blood loss, and complications (intraoperative or postoperative). Some studies suggested that the reoperation rate of endoscopic discectomy was higher than that of non-endoscopic discectomy due to the steep learning curve and the limited operative field (22, 31–33). Moreover, the anatomical structure and technique during some endoscopic discectomy (such as percutaneous endoscopic transforaminal discectomy) are not similar to traditional non-endoscopic discectomy. The surgeons not adapt to this approach very quickly, which makes the introduction of the endoscope relatively difficult in the early stages. In addition, for complicated situations such as malformations and degeneration, non-endoscopic discectomy can achieve better clinical results and ensure safety. From the findings in this study, the current research focus of discectomy on LDH was the comparison between surgical approaches and evaluation of current minimally invasive discectomy. At present, minimally invasive techniques such as endoscopic discectomy cannot completely replace non-endoscopic discectomy (open discectomy and microdiscectomy) through bibliometric analysis and mapping knowledge domains.
A consensus has been reached that the operation for re-herniation is associated with more cost and is less effective (34–37). Hence, reducing the re-herniation rate has always been one of the topics in the field of discectomy. Studies suggested that the rate of re-herniation after lumbar discectomy has decreased to approximately 3% in 2017 (38), whereas some recent studies reported that patients with large postoperative annular defects (≥6 mm width) had a 2.5-fold higher rate of recurrence, compared with patients who had small annular defects (<6 mm width) (39, 40). In recent years, a method for repairing an annular defect to control the re-herniation rate has been proposed, which includes the implantation of an annular closure device (ACD). Through bibliometric analysis and mapping knowledge domains in this study, the recent appeared topic included symptomatic re-herniation, large annular defect and annular closure device shown in Figure 3B and Table 2. By combining bibliometrics analysis with clinical practice, we predict that one of the research hotspots in the future could be the control of recurrence rate and the solution of symptomatic re-herniation after lumbar discectomy.
The objective of this study was to evaluate the global research productivity in the field of discectomy on LDH through bibliometric analysis and mapping knowledge domains. Previous published studies have investigated the quantity and quality of articles in the field of full-endoscopic spine surgery (15). The advantage of this study was that we focused on a specific surgical intervention, namely, discectomy for lumber disc herniation, which narrowed the scope of research and improved its depth, but there were still several limitations in this study. First, the databases that we indicated mainly contain publications in English, which lacked non-English literature. Second, differences may exist between the real research situation and the bibliometric analysis findings because of the calculation load of the algorithm. Some recently published high-quality papers were removed because the number of citations did not reach the set threshold. Third, some of the latest articles may not be included in the databases yet.
Conclusions
The United States is the most significant contributor to the development of discectomy for LDH. Some countries developed rapidly in the number of publications but lacked research depth and citations, such as China. The current research focus of discectomy on LDH was the comparison between surgical approaches and evaluation of current minimally invasive discectomy. At present, minimally invasive techniques such as endoscopic discectomy cannot completely replace non-endoscopic discectomy (open discectomy and microdiscectomy) through bibliometric analysis and mapping knowledge domains. One of the research hotspots in the future is the control of the recurrence rate and the solution of symptomatic re-herniation after lumbar discectomy.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical review and approval was not required for this study in accordance with the local legislation and institutional requirements.
Author contributions
W-SL: study concept and design, data acquisition and interpretation, and drafted the manuscript. QY: data acquisition, data interpretation, and language editing. G-YL: data interpretation and language editing. W-TC: data acquisition and data proofreading. LC: study concept and design, study supervision, and critical review of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the National Natural Science Foundation of China (No: 81871803). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ACD, annular closure device; FED, full-endoscopic discectomy; LDH, lumbar disc herniation; MD, microdiscectomy; MED, microendoscopic discectomy; PELD, percutaneous endoscopic lumbar discectomy; PTED, percutaneous transforaminal endoscopic discectomy; SCIE, Science Citation Index Expanded; TELD, transforaminal endoscopic lumbar discectomy; WoS, Web of Science.
References
1. Kerr D, Zhao W, Lurie JD. What are long-term predictors of outcomes for lumbar disc herniation? A randomized and observational study. Clin Orthop Relat Res. (2015) 473:1920–30. doi: 10.1007/s11999-014-3803-7
2. Gadjradj PS, Arts MP, Van Tulder MW, Rietdijk WJR, Peul WC, Harhangi BS. Management of symptomatic lumbar disk herniation: an international perspective. Spine. (2017) 42:1826–34. doi: 10.1097/BRS.0000000000002294
3. Mixter WJ, Barr JS. Rupture of the intervertebral disc with involvement of the spinal canal. N Engl J Med. (1934) 211:210–5. doi: 10.1056/NEJM193408022110506
4. Mayer HM, Brock M. Percutaneous endoscopic discectomy: surgical technique and preliminary results compared to microsurgical discectomy. J Neurosurg. (1993) 78:216–25. doi: 10.3171/jns.1993.78.2.0216
5. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective, randomized, controlled study. Spine. (2008) 33:931–9. doi: 10.1097/BRS.0b013e31816c8af7
6. Alvi MA, Kerezoudis P, Wahood W, Goyal A, Bydon M. Operative approaches for lumbar disc herniation: a systematic review and multiple treatment meta-analysis of conventional and minimally invasive surgeries. World Neurosurg. (2018) 114:391–407.e2. doi: 10.1016/j.wneu.2018.02.156
7. Phan K, Xu J, Schultz K, Alvi MA, Lu VM, Kerezoudis P, et al. Full-endoscopic versus micro-endoscopic and open discectomy: a systematic review and meta-analysis of outcomes and complications. Clin Neurol Neurosurg. (2017) 154:1–12. doi: 10.1016/j.clineuro.2017.01.003
8. Ruan W, Feng F, Liu Z, Xie J, Cai L, Ping A. Comparison of percutaneous endoscopic lumbar discectomy versus open lumbar microdiscectomy for lumbar disc herniation: a meta-analysis. Int J Surg. (2016) 31:86–92. doi: 10.1016/j.ijsu.2016.05.061
9. Zhang B, Liu S, Liu J, Yu B, Guo W, Li Y, et al. Transforaminal endoscopic discectomy versus conventional microdiscectomy for lumbar disc herniation: a systematic review and meta-analysis. J Orthop Surg Res. (2018) 13:169. doi: 10.1186/s13018-018-0868-0
10. Chen YC, Kuo CH, Cheng CM, Wu JC. Recent advances in the management of cervical spondylotic myelopathy: bibliometric analysis and surgical perspectives. J Neurosurg Spine. (2019) 31:299–309. doi: 10.3171/2019.5.SPINE18769
11. Das JP, Aherne E, Kavanagh E. Imaging of the spine: a bibliometric analysis of the 100 most-cited articles. Spine. (2019) 44:1593–8. doi: 10.1097/BRS.0000000000003131
12. Fan G, Han R, Zhang H, He S, Chen Z. Worldwide research productivity in the field of minimally invasive spine surgery: a 20-year survey of publication activities. Spine. (2017) 42:1717–22. doi: 10.1097/BRS.0000000000001393
13. Huang T, Wu H, Yang S, Su B, Tang K, Quan Z, et al. Global trends of researches on sacral fracture surgery: a bibliometric study based on VOSviewer. Spine. (2020) 45:E721–8. doi: 10.1097/BRS.0000000000003381
14. Huang Y, Zhao T, Reidler JS, Chen X, Zhang H, Shao H, et al. The top 100 most-cited articles on kyphoplasty and vertebroplasty. World Neurosurg. (2020) 135:e435–46. doi: 10.1016/j.wneu.2019.12.014
15. Lin GX, Kotheeranurak V, Mahatthanatrakul A, Ruetten S, Yeung A, Lee SH, et al. Worldwide research productivity in the field of full-endoscopic spine surgery: a bibliometric study. Eur Spine J. (2020) 29:153–60. doi: 10.1007/s00586-019-06171-2
16. Zhai X, Cui J, Shao J, Wang Q, Chen X, Wei X, et al. Global research trends in spinal ultrasound: a systematic bibliometric analysis. BMJ Open. (2017) 7:e015317. doi: 10.1136/bmjopen-2016-015317
17. Zhou JJ, Koltz MT, Agarwal N, Tempel ZJ, Kanter AS, Okonkwo DO, et al. 100 most influential publications in scoliosis surgery. Spine. (2017) 42:336–44. doi: 10.1097/BRS.0000000000001860
18. Synnestvedt MB, Chen C, Holmes JH. Citespace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc. (2005) 2005:724–8.16779135
19. Swartz KR, Trost GR. Recurrent lumbar disc herniation. Neurosurg Focus. (2003) 15:E10. doi: 10.3171/foc.2003.15.3.10
20. Weber H. Lumbar disc herniation. A controlled, prospective study with ten years of observation. Spine. (1983) 8:131–40. doi: 10.1097/00007632-198303000-00003
21. Carragee EJ, Han MY, Suen PW, Kim D. Clinical outcomes after lumbar discectomy for sciatica: the effects of fragment type and anular competence. J Bone Joint Surg Am. (2003) 85:102–8. doi: 10.2106/00004623-200301000-00016
22. Yeung AT, Tsou PM. Posterolateral endoscopic excision for lumbar disc herniation: surgical technique, outcome, and complications in 307 consecutive cases. Spine. (2002) 27:722–31. doi: 10.1097/00007632-200204010-00009
23. Caspar W. A new surgical procedure for lumbar disc herniation causing less tissue damage through a microsurgical approach. Adv Neurosurg. (1977) 4:74–80. doi: 10.1007/978-3-642-66578-3_15
24. Maurice MS, Kevin TF, Semmes-Murphey C. Microendoscopic discectomy: surgical technique and initial clinical results. Tech Neurosurg. (1997) 3:301.
25. Perez-Cruet MJ, Foley KT, Isaacs RE, Rice-Wyllie L, Wellington R, Smith MM, et al. Microendoscopic lumbar discectomy: technical note. Neurosurgery. (2002) 51:S129–36. doi: 10.1227/01.NEU.0000031004.69814.2D
26. Suk KS, Lee HM, Moon SH, Kim NH. Recurrent lumbar disc herniation: results of operative management. Spine. (2001) 26:672–6. doi: 10.1097/00007632-200103150-00024
27. Cinotti G, Roysam GS, Eisenstein SM, Postacchini F. Ipsilateral recurrent lumbar disc herniation. A prospective, controlled study. J Bone Joint Surg Br. (1998) 80:825–32. doi: 10.1302/0301-620X.80B5.0800825
28. Chen J, Jing X, Li C, Jiang Y, Cheng S, Ma J. Percutaneous endoscopic lumbar discectomy for L5S1 lumbar disc herniation using a transforaminal approach versus an interlaminar approach: a systematic review and meta-analysis. World Neurosurg. (2018) 116:412–20.e2. doi: 10.1016/j.wneu.2018.05.075
29. Chen X, Chamoli U, Lapkin S, Castillo JV, Diwan AD. Complication rates of different discectomy techniques for the treatment of lumbar disc herniation: a network meta-analysis. Eur Spine J. (2019) 28:2588–601. doi: 10.1007/s00586-019-06142-7
30. Cong L, Zhu Y, Tu G. A meta-analysis of endoscopic discectomy versus open discectomy for symptomatic lumbar disk herniation. Eur Spine J. (2016) 25:134–43. doi: 10.1007/s00586-015-3776-6
31. Kim MJ, Lee SH, Jung ES, Son BG, Choi ES, Shin JH, et al. Targeted percutaneous transforaminal endoscopic diskectomy in 295 patients: comparison with results of microscopic diskectomy. Surg Neurol. (2007) 68:623–31. doi: 10.1016/j.surneu.2006.12.051
32. Li WS, Yan Q, Cong L. Comparison of endoscopic discectomy versus non-endoscopic discectomy for symptomatic lumbar disc herniation: a systematic review and meta-analysis. Global Spine J. (2022) 12:1012–26. doi: 10.1177/21925682211020696
33. Schaffer JL, Kambin P. Percutaneous posterolateral lumbar discectomy and decompression with a 6.9-millimeter cannula. Analysis of operative failures and complications. J Bone Joint Surg Am. (1991) 73:822–31. doi: 10.2106/00004623-199173060-00005
34. Abdu RW, Abdu WA, Pearson AM, Zhao W, Lurie JD, Weinstein JN. Reoperation for recurrent intervertebral disc herniation in the spine patient outcomes research trial: analysis of rate, risk factors, and outcome. Spine. (2017) 42:1106–14. doi: 10.1097/BRS.0000000000002088
35. Adogwa O, Parker SL, Shau DN, Mendenhall SK, Aaronson O, Cheng JS, et al. Cost per quality-adjusted life year gained of revision neural decompression and instrumented fusion for same-level recurrent lumbar stenosis: defining the value of surgical intervention. J Neurosurg Spine. (2012) 16:135–40. doi: 10.3171/2011.9.SPINE11308
36. Ambrossi GL, Mcgirt MJ, Sciubba DM, Witham TF, Wolinsky JP, Gokaslan ZL, et al. Recurrent lumbar disc herniation after single-level lumbar discectomy: incidence and health care cost analysis. Neurosurgery. (2009) 65:574–8; discussion 578. doi: 10.1227/01.NEU.0000350224.36213.F9
37. O'donnell JA, Anderson JT, Haas AR, Percy R, Woods ST, Ahn UM, et al. Treatment of recurrent lumbar disc herniation with or without fusion in workers' compensation subjects. Spine. (2017) 42:E864–70. doi: 10.1097/BRS.0000000000002057
38. Heindel P, Tuchman A, Hsieh PC, Pham MH, D'oro A, Patel NN, et al. Reoperation rates after single-level lumbar discectomy. Spine. (2017) 42:E496–501. doi: 10.1097/BRS.0000000000001855
39. Ammerman J, Watters WC, Inzana JA, Carragee G, Groff MW. Closing the treatment gap for lumbar disc herniation patients with large annular defects: a systematic review of techniques and outcomes in this high-risk population. Cureus. (2019) 11:e4613. doi: 10.7759/cureus.4613
Keywords: discectomy, lumbar disc herniation (LDH), bibliometrics, research hotspots, keywords
Citation: Li W, Yan Q, Li G, Chen W and Cong L (2023) Global research productivity in the field of discectomy on lumbar disc herniation: A systematic bibliometric analysis. Front. Surg. 10:1046294. doi: 10.3389/fsurg.2023.1046294
Received: 27 September 2022; Accepted: 6 January 2023;
Published: 31 January 2023.
Edited by:
Panayiotis D. Megaloikonomos, McGill University, CanadaReviewed by:
Delia Cannizzaro, Humanitas Research Hospital, ItalySherwan Hamawandi, Hawler Medical University, Iraq
© 2023 Li, Yan, Li, Chen and Cong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lin Cong Y2hpbmFjb25nbGluQG91dGxvb2suY29t
Specialty Section: This article was submitted to Orthopedic Surgery, a section of the journal Frontiers in Surgery