 Polán Ordás1,†,§
Polán Ordás1,†,§ Emanuela Spagnolo1,†*§
Emanuela Spagnolo1,†*§ Lucía Gómez-Lavín Fernández2María Dolores Diestro Tejeda1,§Pilar Lafuente1,§Patricia Salas1Ana Lopez Carrasco1,§María Carbonell1,§
Lucía Gómez-Lavín Fernández2María Dolores Diestro Tejeda1,§Pilar Lafuente1,§Patricia Salas1Ana Lopez Carrasco1,§María Carbonell1,§ Alicia Hernández1,3
Alicia Hernández1,3
- 1Department of Obstetrics and Gynecology, La Paz University Hospital, Madrid, Spain
- 2Department of Obstetrics and Gynecology, Consorci Sanitari Parc Taulí, Hospital de Sabadell, Barcelona, Spain
- 3Department of Obstetrics and Gynecology, Faculty of Medicine, Universidad Autónoma de Madrid, Madrid, Spain
Our aim was to study the advantages, complications and obstetrical outcomes of laparoscopic myomectomy (LM) compared with abdominal myomectomy (AM). We conducted a retrospective cohort study at La Paz University Hospital that included LMs and AMs performed between 2012 and 2018, analyzing 254 myomectomies (142 AMs [55.7%] and 112 LMs [43.9%]). The mean number of fibroids was 1.8 ± 1.5 and 3 ± 2.9 for the LM and AM groups, respectively (p < 0.006). The mean size of the largest myoma was 7.6 cm ± 2.7 cm and 10.2 cm ± 5.4 cm for the LM and AM groups, respectively (p < 0.001). LMs were associated with longer surgical times (p < 0.001) and shorter hospitalizations (p = 0.001). There were no significant differences in the intraoperative and postoperative complication rates (p = 0.075 and p = 0.285 for LM and AM, respectively). The subsequent pregnancy rate was higher for the LM group (30.8% vs. 16.8%, p = 0.009), with a vaginal delivery rate of 69% and no cases of uterine rupture.
Introduction
Uterine fibroids, or leiomyomas, are benign uterine neoplasms that arise from smooth-muscle tissue and are present in 20%–40% of women of reproductive age (1–3) and 70%–80% of women older than 50 years (4, 5). In most cases, however, uterine fibroids go unnoticed, with only 40% of cases presenting symptoms. The most frequent symptoms are severe vaginal bleeding (and consequent anemia), pelvic pain, dysmenorrhea, worsening quality of life and reproductive dysfunction (6–9). The symptoms will depend basically on the composition, size, location and number of myomas (4–6, 9).
The classical treatment for uterine fibroids has been open abdominal hysterectomy. Cultural and social developments, as well as delayed conception age, have led to the development and improvement of myomectomy, which was first described in the 1970s. For those patients who wish to retain their reproductive ability, myomectomy is an alternative to hysterectomy (3).
The advent of minimally invasive techniques has significantly improved the short-term outcomes of major gynecologic surgery, including myomectomy, by enhancing recovery and decreasing pain and postoperative complications (10, 11). However, the current criteria for selecting patients and deciding on the surgical approach are still a matter of debate (10, 12).
The presence of leiomyomas can affect obstetrical outcomes, causing decreased fertility, increased pregnancy loss and complications during pregnancy (13–15). The delivery mode for these patients is controversial, given that many obstetricians recommend elective caesarean delivery for most patients with a previous history of myomectomy (mainly if the uterine cavity was entered at the time of surgery), despite a lack of strong supporting evidence (15).
Therefore, this study's main objective was to compare the surgical and obstetrical outcomes of laparoscopic myomectomy (LM) vs. open abdominal myomectomy (AM), thereby establishing selection criteria for the most appropriate surgical approach.
Materials and methods
After institutional review board approval (PI-3661), this retrospective cohort study included all patients who underwent LM or open AM at the Department of Gynecology of La Paz University Hospital between May 2012 and December 2018. The study included patients aged 18–50 years, with an ultrasound diagnosis of at least 1 myoma with a mean diameter ≥3 cm and presenting heavy menstrual bleeding or infertility, pelvic pain or suspicious ultrasound findings (16) as the main indications for myomectomy. The exclusion criteria were a postmenopausal state, history of primary ovarian insufficiency or tubal factor infertility and the presence of uterine mass suspicious for malignancy. Patients were grouped according to the surgical approach: LM group and AM group.
We collected preoperative data that included age, body mass index, indication for surgery, preoperative hemoglobin levels, previous myomectomy, previous use of ulipristal acetate (5 mg daily for 3–6 months), total number of myomas and the diameter and location of the largest myoma as determined by ultrasound. A preoperative systematic ultrasound examination was conducted in all cases, classifying the fibroids according to the International Federation of Gynecology and Obstetrics classification (17). We analyzed the details of the surgery, hospital stay and histology and described and compared the intraoperative and postoperative complications according to the Clavien-Dindo classification (18), as well as the recurrence rates. Lastly, we investigated the pregnancy rates, conception method, delivery type and delivery outcomes.
Surgical technique
Myomectomy was performed in both groups using the intracapsular technique with pseudocapsule preservation, as previously described (19). The surgeries were performed by an expert (more than 10 years of experience) minimally invasive gynecologic surgeon (Table 1) or training surgeon. To reduce intraoperative bleeding during the laparoscopic myomectomy, the patients were administered an intramyometrial injection of dilute vasopressin (20 IU/100 ml normal saline), or a temporary uterine artery occlusion was performed using vascular clips (10-mm Hem-o-lok clip or medium titanium clip). LM was performed using a 10-mm trocar for the camera (placed at or above the umbilicus, depending on the size of the uterus). Two ancillary 5-mm trocars were inserted in each iliac fossa, and one ancillary 10–12 mm trocar was inserted in the suprapubic area. For the LM group, a RUMI® II System uterine manipulator (Cooper Surgical, Inc, Trumbull, United States) was employed. The surgeon therefore performed the following steps: transversal or oblique hysterotomy using a crochet needle electrode, enucleation of the myoma (by traction and counter-traction movements using a strong grasper and an irrigator cannula inserted in the space under the myoma pseudocapsule and fibroid) and suture of the uterine defect. A bipolar clamp was used for selected hemostasis. The myoma was finally extracted from the abdominal cavity using manual morcellation through the umbilical incision in endobag. The uterine walls were sutured in 1 or 2 layers, according to the depth of the hysterotomy, with a continuous suture. For the uterine suture, the surgeon employed a size 0 barbed suture (VLock, Covidien) or an absorbable monofilament thread 1/0 (Biosyn, Covidien).
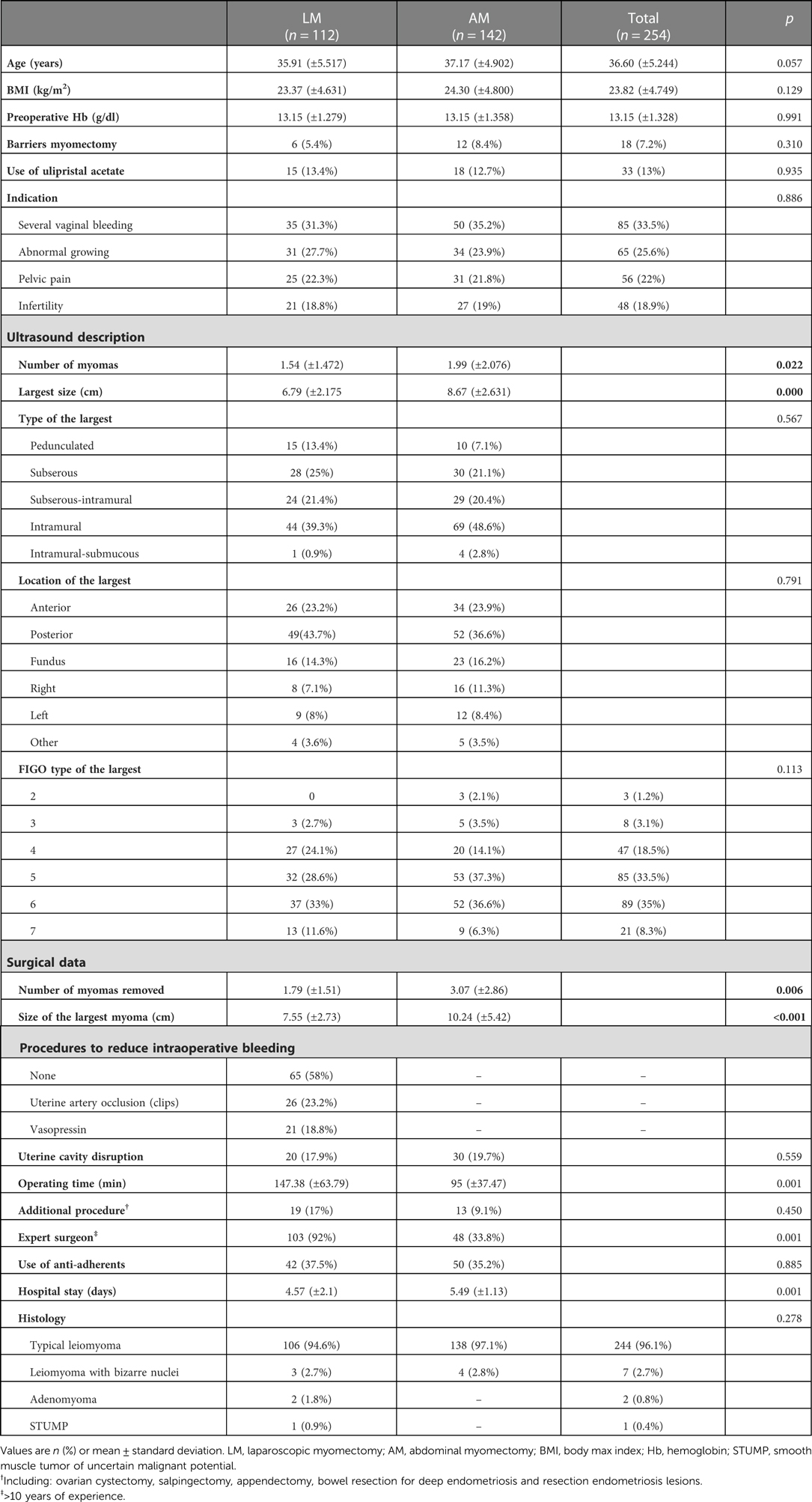
Table 1. Patient characteristics of the two groups (laparoscopic myomectomy versus abdominal myomectomy).
The AM procedure was performed by a mini-Pfannenstiel incision. The surgeon attempted to remove all visible myomas by using a minimum number of incisions. The uterine defect was repaired using an absorbable multifilament thread 1/0 (Vicryl, Ethicon; Johnson & Johnson) or an absorbable monofilament thread 1/0 (Biosyn, Covidien). As previously described for the LM group, the uterus was sutured in 1 or 2 layers, according to the depth of the hysterotomy, with a continuous suture.
In both surgical techniques, the pelvis was irrigated with saline solution at the end of the procedure. For both groups, the use of absorbable adhesion barrier (oxidized regenerated cellulose; Surgicel, Ethicon) and drain was not standardized, and they were placed only if the surgeon considered them necessary.
Statistical analysis
The statistical analysis was performed using SPSS version 24.0 for Windows (IBM Corp., Armonk, NY, United States). The quantitative variables are expressed as mean and standard deviation, and the qualitative variables are expressed as absolute numbers and percentages. The quantitative variables were analyzed between the two groups using Student's t-test, whereas the qualitative variables were analyzed using the chi-squared test and Fisher's exact test. To assess the significance of the individual parameters, we performed a bivariate logistic regression analysis. To investigate the combination of predictors for the myomectomy route, we conducted a multiple regression analysis. To assess the degree of agreement between the ultrasound examination and the surgery evaluation, we calculated the intraclass correlation coefficient (ICC). A p-value <0.05 was considered statistically significant for all variables.
Results
Surgical outcomes
From May 2012 to December 2018, a total of 254 myomectomies were performed (112 [43.9%] LMs and 142 [55.7%] AMs). In 4 (3.6%) cases, the surgery started by laparoscopy and then converted to open surgery; these cases were therefore assigned to the AM group. In 2 of these cases, the conversion was due to the enormous size of the myoma (>15 cm), and in the other 2 cases, the conversion was due to massive blood loss.
Table 1 summarizes the patients' preoperative characteristics and surgical data, while Table 2 summarizes the intraoperative and postoperative complications, the latter of which were mostly minor and controllable with no invasive procedures. In contrast, 1 patient of the AM group (Table 2) underwent emergency abdominal hysterectomy due to uncontrolled intraoperative blood loss (>1000 ml). One (0.9%) case in the LM group and 5 (3.6%) cases in the AM group experienced recurrence and required reintervention, a difference that was not statistically significant (p = 0.285).
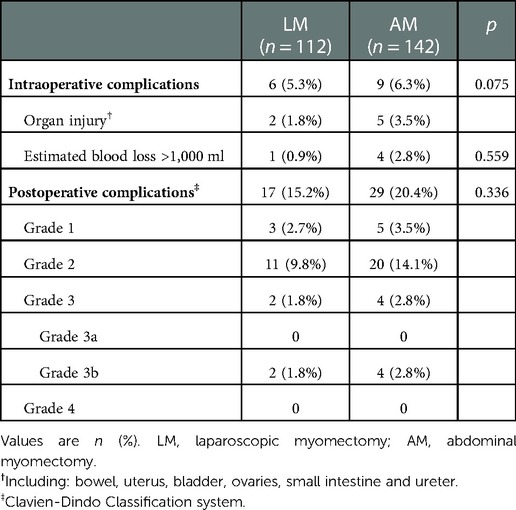
Table 2. Comparison of the intraoperative and postoperative complications between laparoscopic myomectomy and abdominal myomectomy.
The logistic regression analysis demonstrated that the number of enucleated myomas, the size of the largest myoma and the surgeon's experience were related to the outcomes and could predict the success of the surgical approach. Our results showed that having more than 3 myomas reduced the probability of a successful LM by 69.3% (p = 0.001), which also applied to the size of the largest enucleated myoma. The probability of successful enucleation was 3-fold higher with laparotomic access than with laparoscopic access for myomas measuring >9 cm [odds ratio 3.24, 95% confidence interval (CI) 1.865–5.656] (p < 0.001). Moreover, the surgeon with more than 10 years of experience in laparoscopic surgery increased the chances of a successful minimally invasive surgery of uterine fibroids by 20,431 fold (95% CI 8704–47,956; p < 0.001).
Lastly, we calculated the ICC to determine whether there was a correlation between the number of myomas observed by ultrasound and the number of myomas observed during the surgical procedure. We obtained an ICC of 0.729 (95% CI: 0.591–0.812; p < 0.001), which indicated “high similarity”. The dimensions of the major myoma observed in the preoperative ultrasound showed moderate agreement with those ultimately observed during surgery (ICC: 0.686; 95% CI: 0.597–0.756; p < 0.001).
Obstetric outcomes
Table 3 shows the obstetric outcomes of the 2 groups, and Figure 1 summarizes the pregnancy and delivery outcomes. The overall pregnancy rate (pregnancies with evidence of a viable fetus) for the patients whose indication for surgery was infertility was 40% (23 patients), compared with the other indications: 16.9% (10 patients) for vaginal bleeding, 25.4% (15 patients) for suspicious ultrasound findings and 18.6% (11 patients) for pelvic pain (p < 0.001). Moreover, in the patients whose indication for surgery was infertility, a higher pregnancy rate was maintained in the LM group than in the AM group (61.9% [13/21 patients] vs. 37% [10/27 patients]); however, the difference was not statistically significant (p = 0.087). There was an increase in the overall pregnancy rate (33%) for the patients whose largest enucleated myoma was <8 cm compared with those whose largest myoma was ≥8 cm (20%) (p = 0.022), regardless of surgical approach. There were no cases of major maternal or obstetric complications such as preterm delivery, placental abnormalities or placental abruption in either group.
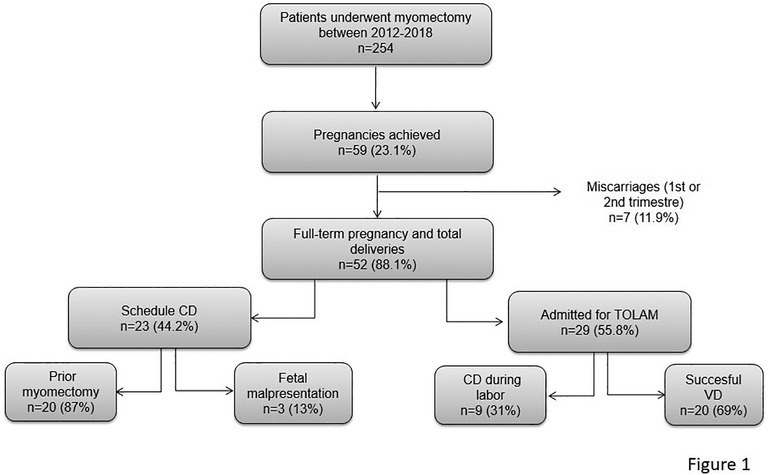
Figure 1. Flow diagram of study population: pregnancy and delivery outcomes in patients who underwent laparoscopic and abdominal myomectomy. CD, cesarean delivery; TOLAM, trial of labor after myomectomy; VD, vaginal delivery.
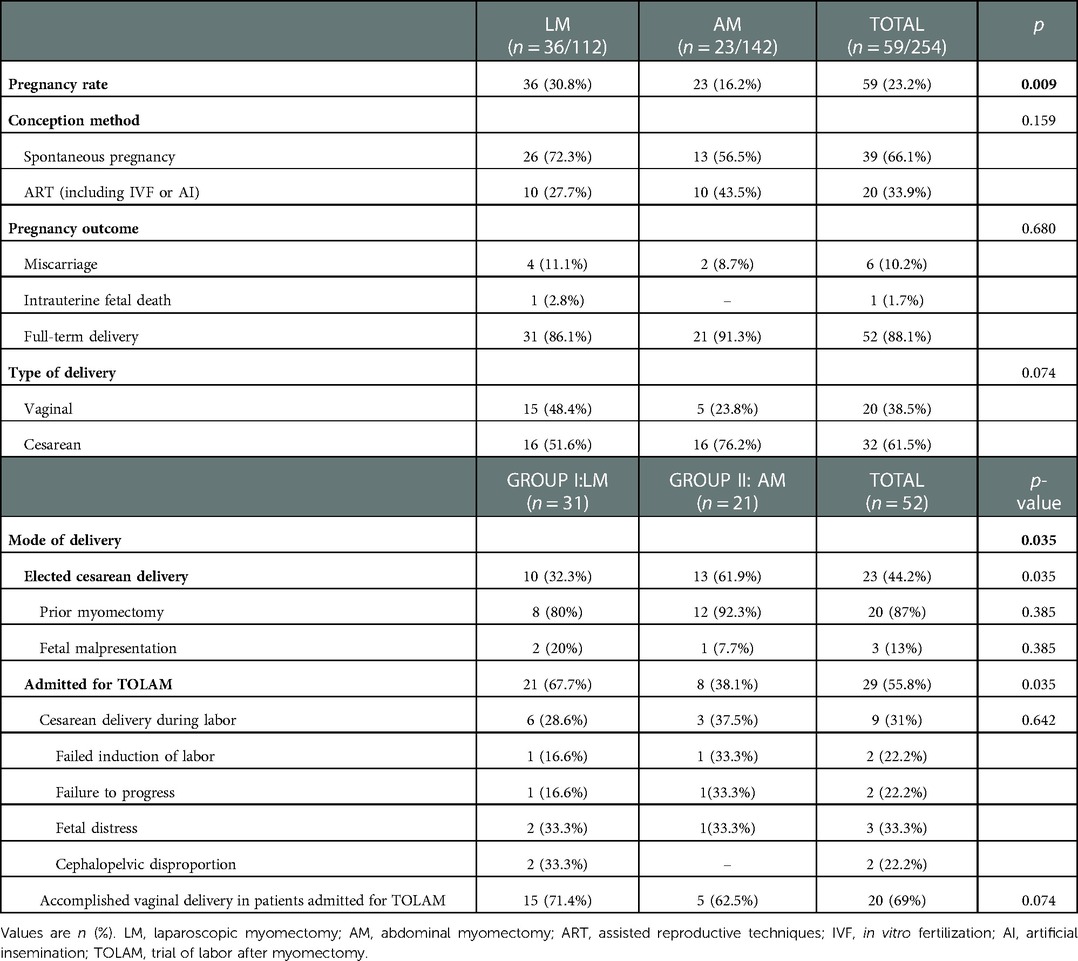
Table 3. Obstetrics and delivery outcomes according surgical approach.
Our series presented a miscarriage rate of 10.2% and an overall full-term delivery rate of 88.1%. All deliveries resulted in live births, and there were no cases of uterine rupture or postpartum hemorrhaging in our series. The pregnancy outcomes of the 2 groups are summarized in Table 3.
Discussion
Myomas are the most common female benign tumors and frequently require surgery. Although there are no universally accepted selection criteria for the surgical approach, based on our results, women with 3 or more fibroids and whose largest myoma is ≤9 cm can be successfully treated through laparoscopy. Our results agree with those of previous studies that showed that the number of complications, surgical difficulties and risk of laparoconversion increase if LM is performed in patients with these characteristics (11, 20–22).
A preoperative ultrasound evaluation should be systematically performed to select the most appropriate surgical approach because ultrasound provides information on the number, size, type and location of the fibroids (14, 21). Frascà et al. (2018) (23) concluded that preoperative ultrasound can correctly identify the number, type, size and locations of myomas with an accuracy >72%. Our results showed that there was a high correlation between the number and size of the largest myoma observed by ultrasound and those identified during surgery.
Does LM improve surgical outcomes compared with AM?
In our series, the women who underwent LM and open AM were comparable in their preoperative characteristics. The association between the surgeon's experience and the laparoscopic approach was statistically significant (p < 0.001), with 92% of the laparoscopies performed by expert surgeons and 66% performed by training surgeons. The surgeon's experience continues to be decisive for successful LM (20, 21). We therefore found no association between the type of myoma and the surgical approach (p = 0.767), given the expert surgeon's skill in managing different types of myomas. For the same reason, there was no significant difference in the estimated blood loss between the groups (p = 0.559). Despite the surgeon's experience, LM required longer surgical times (p < 0.001), as previously reported (13, 22).
With regard to intraoperative and postoperative complications, we found no statistical differences between the 2 groups, as reported in the literature (13). In our study, the mean hospital stay was shorter for the LM group than for the AM group, corroborating the reports of previous studies (13, 24, 25), thereby confirming the major advantage of the laparoscopic approach. Furthermore, a recent meta-analysis (26) which compared transvaginal retrieval and port-site specimen retrieval after LM showed comparable results in terms of intraoperative complications, hospital stay and operative time. Concerning transvaginal extraction of the surgical specimen after LM, a large case series by Laganá et al. (27) demonstrated a significant increase in operative time, intraoperative blood loss and hospital stay with increasing weight of removed fibroid.
One of the limitations of the laparoscopic approach is the inability to palpate the uterus during the intervention, which can result in persistence of intramural fibroids (22). However, this limitation could be overcome by performing an intra-operative vaginal ultrasound to confirm the presence of any intramural fibroids prior to completing the surgery (23). Studies have established that the recurrence rates for patients who undergo LM are 167% higher than for those who undergo AM, with a cumulative 5-year recurrence rate of 57.3%–62.1% for the LM group and 15.4%–62% for the AM group (13, 28). Recent studies have reported that although recurrence rates after LM might be high, the number of patients who require re-operation is low (2.4%) (29, 30). Our study showed different results, given that 5 (3.62%) patients underwent re-operation after AM vs. only 1 after LM (0.9%), although there were no significant differences, and the reintervention rates were low in both cases. Lastly, it is important to highlight the effect of additional procedures such as endometriosis on the operative time. Although there were no statistical differences in operative times between the 2 groups, the association between endometriosis and myomas is very common. In particular, eradication of deep endometriosis could affect surgical times and could represent a selection bias in our study.
Do obstetric outcomes improve after LM compared with AM?
Numerous studies have indicated that the cumulative pregnancy rate and cumulative live birth rate are similar between women treated by LM and those treated with AM (30, 31). Our study showed a higher pregnancy rate after LM (30.8% vs. 16.8%), which was statistically significant (p = 0.009). Our results agree with those of other studies that found that patients who underwent LM had a higher pregnancy rate than those who underwent AM, possibly due to a reduced occurrence of postoperative adhesions (14, 21). In our study, anti-adherent barriers were employed in 37.5% of the LM procedures and in 36.2% of the AM procedures. Although these differences are not statistically significant, we can speculate that their use in LM might prevent adhesions. In a recent review (32), oxidized regenerated cellulose was found to be effective in reducing the total adhesion score during second-look surgery. Laganá et al. (33) showed that the opening of uterine cavity and the laparotomic approach represented independent risk factors for developing intrauterine adhesions, after 3 months from surgery.
Unfortunately, it is difficult to speculate on the relationship between increased pregnancy rates among patients who underwent LM and those who underwent AM.
Numerous studies have shown that pregnancy rates increased up to 70% after myomectomy (14) due to various mechanisms, such as distortion of the uterine cavity, alteration of myometrial contractility and alteration of the tube-ovary anatomic relationship (34). Our data showed a higher pregnancy rate for the patients whose indication for surgery was sterility compared with the other indications (40% vs. <25.4%, respectively; p < 0.001), Furthermore, the gestational rate was higher for the LM group than for the AM group (61.9% vs. 37%), although these clinical differences were not statistically significant (p = 0.087). Our results showed a higher pregnancy rate (33% vs. 20%) among the patients whose main excised myoma measured <8 cm (p = 0.020), regardless of the surgical approach. Similar results were reported by Kundu et al. (2018) (14), who indicated a pregnancy rate of nearly 50% in the group with removed myomas <8 cm in diameter, dropping to ≤30% when the myomas measured ≥8 cm in diameter.
With regard to delivery outcomes, the elective caesarean rate was 44.2% in our series, with a higher rate of scheduled caesareans in the AM group than the LM group (69.1% vs. 32.3%; p = 0.035). The main indication for scheduling a caesarean in our study was opening the uterine cavity and performing multiple myomectomy (85% of cases) to prevent uterine rupture during labor. Our results agree with those of Gambacorti-Passerini et al. (2018) (15), who also reported a higher rate of scheduled caesareans in their AM group (75% vs. 46.7% in the LM group), with the main indication for caesarean being a previous myomectomy. The authors compared the operative findings of the women admitted for trial of labor after myomectomy (TOLAM) with those who were scheduled for caesareans and found no significant differences apart from the incidence of entering the uterine cavity (33.3%) in the caesarean group compared with the patients admitted for TOLAM (1.4%; p < 0.01).
Surprisingly, a recent meta-analysis by Claeys et al. (2014) (35) demonstrated that LM is associated with a higher rate of elective caesareans (p = 0.001), which contrasts with our results and those of previous studies. The authors attributed the higher rate in the LM group to the surgeon's concerns that this type of myomectomy has a higher risk of rupture during subsequent pregnancies and labor compared with the open technique. Interestingly, the URIDA (uterine rupture international data acquisition) study (19), did not showed any association between the incidence of uterine rupture and the number and type of previous uterine surgeries. This study evaluated 224 patients with previous uterine operations (cesarean section, LM, AM, hysteroscopic myomectomy). In these patients, the mean gestational age at which the uterine rupture was 37.32 ± 5.09 weeks.
In our study, 21 (67.7%) patients in the LM group and 8 (38.1%) patients in the AM group (p = 0.035) were admitted for TOLAM. Fifteen (71.4%) patients achieved a successful vaginal delivery after LM, and 5 (62.5%) patients achieved it after AM (p = 0.074). Gambacorti-Passerini et al. (2018) (15) and Claeys et al. (2014) (35) showed similar results, with a vaginal delivery rate of 91.5% for the patients admitted for TOLAM, 93% after LM and 88% after AM, with no statistically significant difference between the two surgical approaches. Although our findings showed a lower percentage of vaginal delivery by the patients admitted for TOLAM in both types of myomectomy than in prior studies, we had no cases of intrapartum complications and a lower rate of caesarean deliveries. Our results are therefore encouraging. Considering the aforementioned data, we believe TOLAM should be considered a feasible and safe option in tertiary level hospitals for patients with a history of myomectomy.
We had no cases of uterine rupture in our series, a complication that represents the main obstetrical risk for women with a previous myomectomy. Uterine rupture is rare (0.47%–1%) and difficult to predict (15, 20, 36).
The strength of our study was its large patient cohort and the analysis of numerous factors in addition to surgical variables. Our study is limited by the retrospective data collection, which might have prevented us from collecting more exact data on cofactors that might have influenced the attitude of obstetricians in determining the delivery mode.
Conclusion
As an alternative to AM, LM can be considered a safe and suitable surgical technique for women of childbearing age, although LM requires longer surgical times and should be performed by surgical teams with a high degree of expertise and experience. A preoperative ultrasound evaluation of the size and number of myomas should be performed for careful patient selection. In our practice, LM was successfully performed in cases with ≤3 fibroids in which the largest measured ≤9 cm. The delivery mode for patients with a prior myomectomy should be individually established; however, vaginal delivery after LM should be considered a safe option for these patients, with uterine rupture an extremely rare complication.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by PI-3661 Hospital la Paz. The patients/participants provided their written informed consent to participate in this study.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This work has been supported by the Carlos III Health Institute and the European Regional Development Fund (ERDF) “European Union, A way to make Europe” (PI20/01368).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Donnez J, Bouchard P, Zakharenko NF, Ugocsai G, Bestel E, Loumaye E. Ulipristal acetate versus placebo for fibroid treatment before surgery. N Engl J Med. (2012) 366(5):409–20. doi: 10.1056/NEJMoa1103182
2. Jacques D, Janusz T, Francisco V, Philippe B, Boguslav L, Francesco B, et al. Ulipristal acetate versus leuprolide acetate for uterine fibroids. N Engl J Med. (2012) 366(5):421–32. doi: 10.1056/NEJMoa1103180
3. Sandberg EM, Tummers FHMP, Cohen SL, van den Haak L, Dekkers OM, Jansen FW. Reintervention risk and quality of life outcomes after uterine-sparing interventions for fibroids: a systematic review and meta-analysis. Fertil Steril. (2018) 109(4):698–707.e1. doi: 10.1016/j.fertnstert.2017.11.033
4. Cruz MSDDL, Buchanan EM. Uterine fibroids: diagnosis and treatment. Am Fam Physician. (2017) 95(2):100–7. PMID: 28084714.28084714
5. Laughlin-Tommaso SK, Jacoby VL, Myers ER. Disparities in fibroid incidence, prognosis, and management. Obstet Gynecol Clin North Am. (2017) 44(1):81–94. doi: 10.1016/j.ogc.2016.11.007
6. Kroon B, Johnson N, Chapman M, Yazdani A, Hart R. Fibroids in infertility – consensus statement from ACCEPT (australasian CREI consensus expert panel on trial evidence). Aust N Z J Obstet Gynaecol. (2011) 51(4):289–95. doi: 10.1111/j.1479-828X.2011.01300.x
7. Williams ARW, Bergeron C, Barlow DH, Ferenczy A. Endometrial morphology after treatment of uterine fibroids with the selective progesterone receptor modulator, ulipristal acetate. Int J Gynecol Pathol. (2012) 31(6):556–69. doi: 10.1097/PGP.0b013e318251035b
8. Donnez J, Vázquez F, Tomaszewski J, Nouri K, Bouchard P, Fauser BCJM, et al. Long-term treatment of uterine fibroids with ulipristal acetate⋆. Fertil Steril. (2014) 101(6):1565–1573.e18. doi: 10.1016/j.fertnstert.2014.02.008
9. Donnez J, Dolmans MM. Uterine fibroid management: from the present to the future. Hum Reprod Update. (2016) 22(6):665–86. doi: 10.1093/humupd/dmw023
10. Sandberg EM, Cohen SL, Jansen FW, Einarsson JI. Analysis of risk factors for intraoperative conversion of laparoscopic myomectomy. J Minim Invasive Gynecol. (2016) 23(3):352–7. doi: 10.1016/j.jmig.2015.10.017
11. Vargas MV, Larson KD, Sparks A, Margulies SL, Marfori CQ, Moawad G, et al. Association of operative time with outcomes in minimally invasive and abdominal myomectomy. Fertil Steril. (2019) 111(6):1252–1258.e1. doi: 10.1016/j.fertnstert.2019.02.020
12. Saccardi C, Gizzo S, Noventa M, Ancona E, Borghero A, Litta PS. Limits and complications of laparoscopic myomectomy: which are the best predictors? A large cohort single-center experience. Arch Gynecol Obstet. (2014) 290(5):951–6. doi: 10.1007/s00404-014-3289-2
13. Cezar C, Becker S, di Spiezio Sardo A, Herrmann A, Larbig A, Tanos V, et al. Laparoscopy or laparotomy as the way of entrance in myoma enucleation. Arch Gynecol Obstet. (2017) 296(4):709–20. doi: 10.1007/s00404-017-4490-x
14. Kundu S, Iwanuk C, Staboulidou I, Garcia-Rocha GJ, Soergel P, Hertel H, et al. Morbidity, fertility and pregnancy outcomes after myoma enucleation by laparoscopy versus laparotomy. Arch Gynecol Obstet. (2018) 297(4):969–76. doi: 10.1007/s00404-018-4697-5
15. Gambacorti-Passerini ZM, Penati C, Carli A, Accordino F, Ferrari L, Berghella V, et al. Vaginal birth after prior myomectomy. Eur J Obstet Gynecol Reprod Biol. (2018) 231:198–203. doi: 10.1016/j.ejogrb.2018.10.007
16. Van den Bosch T, Dueholm M, Leone FPG, Valentin L, Rasmussen CK, Votino A, et al. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: a consensus opinion from the morphological uterus sonographic assessment (MUSA) group. Ultrasound Obstet Gynecol. (2015) 46(3):284–98. doi: 10.1002/uog.14806
17. Munro MG, Critchley HOD, Broder MS, Fraser IS. FIGO Classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynecol Obstet. (2011) 113(1):3–13. doi: 10.1016/j.ijgo.2010.11.011
18. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. (2004) 240(2):205–13. doi: 10.1097/01.sla.0000133083.54934.ae
19. Tinelli A, Hurst BS, Hudelist G, Tsin DA, Stark M, Mettler L, et al. Laparoscopic myomectomy focusing on the myoma pseudocapsule: technical and outcome reports. Hum Reprod Oxf Engl. (2012) 27(2):427–35. doi: 10.1093/humrep/der369
20. Martinez MEG, Domingo MVC. Size, type, and location of myoma as predictors for successful laparoscopic myomectomy: a tertiary government hospital experience. Gynecol Minim Invasive Ther. (2018) 7(2):61–5. doi: 10.4103/GMIT.GMIT_12_18
21. Bean EMR, Cutner A, Holland T, Vashisht A, Jurkovic D, Saridogan E. Laparoscopic myomectomy: a single-center retrospective review of 514 patients. J Minim Invasive Gynecol. (2017) 24(3):485–93. doi: 10.1016/j.jmig.2017.01.008
22. Jansen LJ, Clark NV, Dmello M, Gu X, Einarsson JI, Cohen SL. Perioperative outcomes of myomectomy for extreme myoma burden: comparison of surgical approaches. J Minim Invasive Gynecol. (2019) 26(6):1095–103. doi: 10.1016/j.jmig.2018.10.022
23. Frascà C, Tuzzato G, Arena A, Degli Esposti E, Zanello M, Raimondo D, et al. The role of pelvic ultrasound in preoperative evaluation for laparoscopic myomectomy. J Minim Invasive Gynecol. (2018) 25(4):679–83. doi: 10.1016/j.jmig.2017.08.661
24. Cicinelli E, Tinelli R, Colafiglio G, Saliani N. Laparoscopy vs minilaparotomy in women with symptomatic uterine myomas: a prospective randomized study. J Minim Invasive Gynecol. (2009) 16(4):422–6. doi: 10.1016/j.jmig.2009.03.011
25. Kim H, Shim S, Hwang Y, Kim M, Hwang H, Chung Y, et al. Is robot-assisted laparoscopic myomectomy limited in multiple myomas?: a feasibility for ten or more myomas. Obstet Gynecol Sci. (2018) 61(1):135–41. doi: 10.5468/ogs.2018.61.1.135
26. Laganà AS, Vitagliano A, Casarin J, Garzon S, Uccella S, Franchi M, et al. Transvaginal versus port-site specimen retrieval after laparoscopic myomectomy: a systematic review and meta-analysis. Gynecol Obstet Invest. (2022) 87(3–4):177–83. doi: 10.1159/000525624
27. Laganà AS, Casarin J, Uccella S, Garzon S, Cromi A, Guerrisi R, et al. Outcomes of in-bag transvaginal extraction in a series of 692 laparoscopic myomectomies: results from a large retrospective analysis. J Minim Invasive Gynecol. (2022) 29(12):1331–38. doi: 10.1016/j.jmig.2022.09.009
28. Kotani Y, Tobiume T, Fujishima R, Shigeta M, Takaya H, Nakai H, et al. Recurrence of uterine myoma after myomectomy: open myomectomy versus laparoscopic myomectomy. J Obstet Gynaecol Res. (2018) 44(2):298–302. doi: 10.1111/jog.13519
29. Shiota M, Kotani Y, Umemoto M, Tobiume T, Hoshiai H. Recurrence of uterine myoma after laparoscopic myomectomy: what are the risk factors? Gynecol Minim Invasive Ther. (2012) 1(1):34–6. doi: 10.1016/j.gmit.2012.08.003
30. Malzoni M, Tinelli R, Cosentino F, Iuzzolino D, Surico D, Reich H. Laparoscopy versus minilaparotomy in women with symptomatic uterine myomas: short-term and fertility results. Fertil Steril. (2010) 93(7):2368–73. doi: 10.1016/j.fertnstert.2008.12.127
31. Flyckt R, Soto E, Nutter B, Falcone T. Comparison of long-term fertility and bleeding outcomes after robotic-assisted, laparoscopic, and abdominal myomectomy. Obstet Gynecol Int. (2016) 2016:2789201. doi: 10.1155/2016/2789201
32. Borghese G, Raffone A, Raimondo D, Saccone G, Travaglino A, Degli Esposti E, et al. Adhesion barriers in laparoscopic myomectomy: evidence from randomized clinical trials. Int J Gynecol Obstet. (2021) 152(3):308–20. doi: 10.1002/ijgo.13495
33. Laganà AS, Garzon S, Dababou S, Uccella S, Medvediev M, Pokrovenko D, et al. Prevalence of intrauterine adhesions after myomectomy: a prospective multicenter observational study. Gynecol Obstet Invest. (2022) 87(1):62–9. doi: 10.1159/000522583
34. Milazzo GN, Catalano A, Badia V, Mallozzi M, Caserta D. Myoma and myomectomy: poor evidence concern in pregnancy: myoma and myomectomy in pregnancy. J Obstet Gynaecol Res. (2017) 43(12):1789–804. doi: 10.1111/jog.13437
35. Claeys J, Hellendoorn I, Hamerlynck T, Bosteels J, Weyers S. The risk of uterine rupture after myomectomy: a systematic review of the literature and meta-analysis. Gynecol Surg. (2014) 11(3):197–206. doi: 10.1007/s10397-014-0842-8
Keywords: uterine leiomyoma, laparoscopy, myomectomy, obstetric outcome, uterine rupture
Citation: Ordás P, Spagnolo E, Fernández LG, Diestro Tejeda MD, Lafuente P, Salas P, Lopez Carrasco A, Carbonell M and Hernández A (2022) Comparison of surgical and obstetric outcomes in women with uterine leiomyomas after laparoscopic vs. abdominal myomectomy: A single-center cohort study. Front. Surg. 9:997078. doi: 10.3389/fsurg.2022.997078
Received: 18 July 2022; Accepted: 8 December 2022;
Published: 26 December 2022.
Edited by:
Tai-Ho Hung, Taipei Chang Gung Memorial Hospital, TaiwanReviewed by:
Kelly Wright, Cedars Sinai Medical Center, United StatesAntonio Simone Laganà, University of Palermo, Italy
© 2022 Ordás, Spagnolo, Fernández, Diestro Tejeda, Lafuente, Salas, Lopez Carrasco, Carbonell and Hernández. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emanuela Spagnolo ZW1hLnNwYWdub2xvQGxpYmVyby5pdA==
†These authors have contributed equally to this work and share first authorship
§ORCID Polán Ordás orcid.org/0000-0002-5686-2131 Emanuela Spagnolo orcid.org/0000-0001-5566-8479 María Dolores Diestro Tejeda orcid.org/0000-0002-2935-7359 Pilar Lafuente orcid.org/0000-0001-8664-4971 Ana Lopez Carrasco orcid.org/0000-0002-1674-7585 María Carbonell orcid.org/0000-0001-9287-0182
Specialty Section: This article was submitted to Obstetrics and Gynecological Surgery, a section of the journal Frontiers in Surgery