 Giorgio Bianchi1,2,3
Giorgio Bianchi1,2,3 Paschalis Gavriilidis4
Paschalis Gavriilidis4 Aleix Martínez-Pérez5,6Gian Luigi de’Angelis3*Mathieu Uzzan7
Aleix Martínez-Pérez5,6Gian Luigi de’Angelis3*Mathieu Uzzan7 Iradj Sobhani7,8Federico Coccolini9
Iradj Sobhani7,8Federico Coccolini9 Carlo Alberto Schena1
Carlo Alberto Schena1 Maria Clotilde Carra10Giuseppe Spinoglio11Nicola de’Angelis1,8,12
Maria Clotilde Carra10Giuseppe Spinoglio11Nicola de’Angelis1,8,12
- 1Unit of general surgery, CARE Department, Henri Mondor University Hospital, Créteil, France
- 2Department of medicine and surgery, University of Parma, Parma, Italy
- 3Gastroenterology and Endoscopy Unit, Department of Medicine and Surgery, University Hospital of Parma, Parma, Italy
- 4Department of surgery, University Hospitals Coventry and Warwickshire NHS Trust, Coventry, United Kingdom
- 5Faculty of Health Sciences, Valencian International University, Valencia, Spain
- 6Department of General and Digestive Surgery, Hospital Universitario Doctor Peset, Valencia, Spain
- 7Department of Gastroenterology, APHP-Henri Mondor University Hospital, Creteil, France
- 8EC2M-EA7375 Research Team, Henri Modor Campus, Paris East University, Creteil, France
- 9General, Emergency and Trauma Department, Pisa University Hospital, Pisa, Italy
- 10Rothschild Hospital, AP-HP, Université de Paris, Paris, France.
- 11IRCAD Faculty Member Robotic and Colorectal Surgery-IRCAD, Strasbourg, France
- 12University Paris-Est, UPEC, Créteil, France
Purpose: Robotic surgery has been progressively implemented for colorectal procedures but is still limited for multiquadrant abdominal resections. The present study aims to describe our experience in robotic multiquadrant colorectal surgeries and provide a systematic review and meta-analysis of the literature investigating the outcomes of robotic total proctocolectomy (TPC), total colectomy (TC), subtotal colectomy (STC), or completion proctectomy (CP) compared to laparoscopy.
Methods: At our institution 16 consecutive patients underwent a 2- or 3-stage totally robotic total proctocolectomy (TPC) with ileal pouch-anal anastomosis. A systematic review of the literature was performed to select studies on robotic and laparoscopic multiquadrant colorectal procedures. Meta-analyses were used to compare the two approaches.
Results: In our case series, 14/16 patients underwent a 2-stage robotic TPC for ulcerative colitis with a mean operative time of 271.42 (SD:37.95) minutes. No conversion occurred. Two patients developed postoperative complications. The mean hospital stay was 8.28 (SD:1.47) days with no readmissions. Mortality was nil. All patients underwent loop-ileostomy closure, and functional outcomes were satisfactory. The literature appraisal was based on 23 retrospective studies, including 736 robotic and 9,904 laparoscopic multiquadrant surgeries. In the robotic group, 36 patients underwent STC, 371 TC, 166 TPC, and 163 CP. Pooled data analysis showed that robotic TC and STC had a lower conversion rate (OR = 0.17;95% CI, 0.04–0.82; p = 0.03) than laparoscopic TC and STC. The robotic approach was associated with longer operative time for TC and STC (MD = 104.64;95% CI, 18.42–190.87; p = 0.02) and TPC and CP (MD = 38.8;95% CI, 18.7–59.06; p = 0.0002), with no differences for postoperative complications and hospital stay. Reports on urological outcomes, sexual dysfunction, and quality of life were missing.
Conclusions: Our experience and the literature suggest that robotic multiquadrant colorectal surgery is safe and effective, with low morbidity and mortality rates. Nevertheless, the overall level of evidence is low, and functional outcomes of robotic approach remain largely unknown.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier: CRD42022303016.
1. Introduction
In the last two decades, robotic surgery has been progressively implemented as a minimally invasive approach for colorectal procedures (1, 2). Nowadays, robotic colorectal surgery is widely used, and evidence supports its safety and efficacy compared to laparoscopic surgery (3, 4). Despite its large applications (5, 6), there is limited data on the use of robotic surgical platforms for extended colorectal resections requiring access in all four quadrants of the abdomen (7) mainly because, to achieve this by robotics, a repositioning of the patient-side robotic cart is needed, leading to an increased operative time and workload (7, 8). The last generation of robotic platforms allows the rotation of the robotic cart without the need for robot repositioning, and thus it may favor the performance of multiquadrant procedures (7, 9).
Four colorectal procedures require a multiquadrant approach, including subtotal colectomy (STC) (10), total colectomy (TC) (11), total proctocolectomy (TPC) (12), and completion proctectomy (CP) (11), performed in a staged multiquadrant surgery. TPC with ileal pouch-anal anastomosis (IPAA) (11, 13), which avoids permanent stoma (12), can be performed in one- (11), two- (11, 14), or three- (11, 14) stage surgery, depending on the extent of the resection and the performance of a loop ileostomy, which will finally require a reversal procedure.
The present study aims to describe our experience in robotic multiquadrant colorectal surgeries (particularly TPC and CP) using the da Vinci Xi (Intuitive Surgical Inc, Sunnyvale CA, USA) robotic platform. In addition, we conducted a systematic review and meta-analysis of the literature to investigate the outcomes of robotic multiquadrant colorectal surgeries and compare them with those associated with laparoscopy.
2. Material and methods
2.1. Single-center experience
2.1.1. Study population
We identified consecutive adult patients who underwent a 2- or 3-stage robotic TPC with IPAA between January 2014 and December 2021 in elective settings in a prospectively maintained database at a tertiary care center (Henri Mondor University Hospital of Creteil, France).
A robotic TPC was defined as all procedural stages performed robotically using da Vinci Xi (Intuitive Surgical Inc, Sunnyvale CA, USA).
Indication for surgery was established in the institutional multidisciplinary meeting discussion for all patients.
The patient is placed in a modified lithotomy position with the legs in Allen stirrups. The robotic cart is placed between the patient's legs on the median axis. This positioning allows the rotation of the boom in all necessary positions as well as an easy access for the surgeon for the introduction of circular stapler. Only the robotic boom is rotated and manually adjusted in two different positions according to the operational steps: (1) right colectomy and transverse colon mobilization; (2) left colectomy and rectal resection with total mesorectal excision (TME) and IPAA. In total, 4 robotic (three 8-mm ports and one 12-mm port) and 2 laparoscopic (5-mm) ports are used. The 4 robotic ports are placed on a diagonal line drawn from the right femoral head (lateral border of the inguinal triangle) to where the left mid clavicular line (MCL) crosses over the left subcostal margin. The two laparoscopic ports are placed 2 cm laterally of the MCL at the level of the left and right subcostal margin.
In the two-stage procedure, the TPC is performed following a medial-to-lateral approach. The procedure starts from the right side; a complete mobilization of right and transverse colon, and the splenic flexure is performed with the proximal ligation of the ileo-colic, right and middle colic pedicles. After rotation of the robotic boom, the left colectomy is performed with a medial-to-lateral approach with the ligation of the inferior mesenteric artery and vein. Last step of the dissection consists of a sphincter-preserving low rectum resection with TME. The rectal transection is achieved with Endo-Wrist 45-mm stapler. The surgical specimen is extracted by a 3 cm incision right to the umbilicus. A 20-cm ileal J pouch is done extracorporeally using GIA 80-mm stapler, the anvil of circular 29-mm stapler is fixed with purse-string suture in the distal angle of the J pouch and an ileo-anal end-to-end anastomosis is constructed with a circular 29-mm stapler introduced transanally. A protective loop ileostomy is exteriorized using the incision close to the umbilicus.
In the first part of the three-stage procedure, the total colectomy is performed with the same technique. Once the colon is totally mobilized, following exsufflation, an incision is made 3 cm left to the umbilicus; this incision is used for extracting the colon, the ileum is dissected using GIA 80-mm stapler 5 cm proximally from the ileo-cecal valve; the sigmoid colon is dissected proximal to the sacral promontory. A double-barreled ileo-sigmoid ostomy (15–17) is created.
In the second operation, the ileo-sigmoid ostomy is dissected, the robotic cart is placed on the left side of the patient and the rectal resection with TME and IPAA are performed using the same technique of the two-stage technique. A protective loop ileostomy is exteriorized using the incision close to the umbilicus.
A more detailed description of the surgical procedures and operative techniques is provided as Supplementary Material.
Data collected included patient demographics (age, sex), previous abdominal surgery, indication for operation, American Society of Anesthesiologists (ASA) score, operative clinical variables (operative time, blood loss, conversion to laparoscopy or open surgery), postoperative outcomes (postoperative complications, 90-days morbidity and mortality, hospital stay, rate of stoma closure), and assessment of fecal incontinence, using the Wexner score (18). The Dindo-Clavien classification was used to define and grade postoperative complications (19).
Data are presented as frequencies and percentages for categorical variables and mean and standard deviation for continuous variables. This retrospective study exclusively used clinical record data routinely collected in health databases (MR004 regulation) and declared to the National Commission for Data Protection and Liberties (CNIL: 2210699). All personal data were collected after obtaining informed consent, and patients received treatment following the ethical standards of the Helsinki Declaration.
2.2. Systematic review
A systematic review of the literature was performed following the Cochrane Collaboration specific protocol (20) and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (21) (Additional Tables 1, 2). The protocol was registered in PROSPERO, University of York (Id: CRD42022303016)
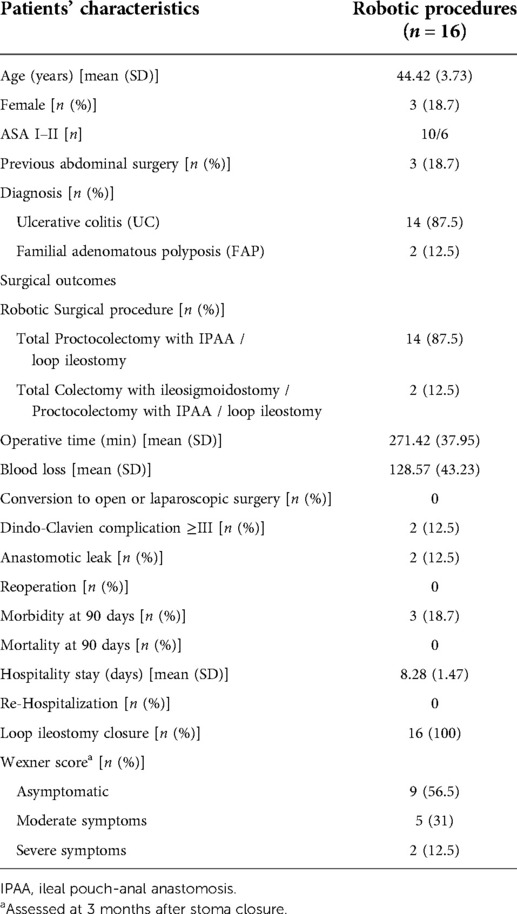
Table 1. Patients’ characteristics and surgical outcomes.
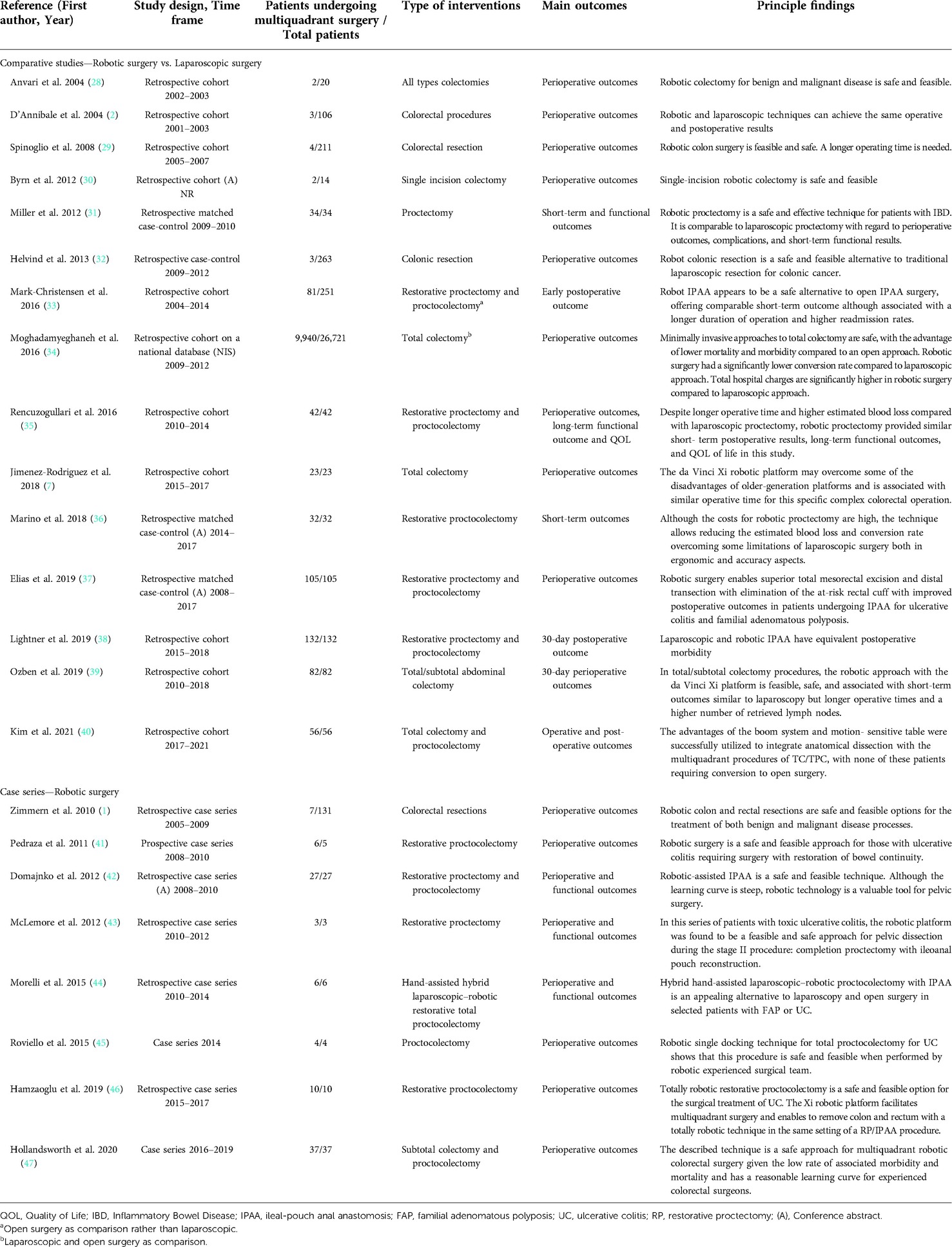
Table 2. Overview of the included studies.
2.2.1. Study selection criteria
We defined the study selection criteria before data collection to identify eligible studies. All publications describing the efficacy, safety, complications, and outcomes of robotic multiquadrant colorectal procedures were retrieved and analyzed. Due to the expected paucity of studies in the literature, comparative and non-comparative studies (case series) were both considered.
The research equations were built according to the following PICOS format:
P, population: patients who required multiquadrant colorectal procedures.
I, intervention: robotic or robot-assisted TC, STC, TPC, CP performed as one-, two- or three-stage procedures.
C, comparisons: laparoscopic multiquadrant colorectal procedures, or no comparison.
O, outcome(s): operative, postoperative, and long-term surgical outcomes, including functional outcomes.
S, study design: comparative studies (e.g., case-control) and case series. Published articles and conference abstracts were eligible for inclusion.
Single case reports and review articles were excluded. Studies on open surgery procedures may be eligible if separated outcomes of interest were reported for the robotic or the laparoscopic approaches.
No trial duration limitation was set. No publication date restriction was applied but only English literature was considered.
2.2.2. Literature search strategy
A literature search was performed using the following online databases up to January 2022: Medline (through PubMed), Embase, and Cochrane Library. A specific research query was formulated for each database, using the following keywords and MeSH terms: robotic surgery; robotics; robot-assisted; minimally invasive surgery; colectomy; total colectomy; subtotal colectomy; proctocolectomy; completion proctectomy; large bowel resection; total proctocolectomy; restorative proctocolectomy; completion proctocolectomy; ileal pouch-anal anastomosis; IPAA.
We cross-checked reference lists from eligible studies and relevant review articles to identify additional publications.
2.2.3. Article selection and quality assessment
The literature search and selection were performed by two independent reviewers (GB and NdeA). First, all records from the merged searches were reviewed for relevance on title and abstract. Records excluded by both reviewers were removed; any disagreement was resolved by discussion or the intervention of a tiebreaker (GS). Both reviewers performed an independent full-text analysis for the final inclusion or exclusion of pre-selected articles.
The reviewers independently assessed the risk of bias using appropriate tools according to the study design. The Newcastle–Ottawa Scale (NOS) (22) was used for case-control and cohort studies. The case series studies were evaluated using the tool described by Murad et al (23). The Grading of Recommendations Assessment Development and Evaluation (GRADE) system was used to grade the “body of evidence” arising from this review (24).
2.2.4. Data extraction and data analysis
Data from the included studies were processed for qualitative and quantitative analysis. Outcome measures (percentages, mean/median values with standard deviations/ranges) were extracted for each surgical approach. Mean values or standard deviation (SD) values (if not reported) were estimated from the median, ranges, inter-quartile ranges (IQR), or p-values, whenever possible (25, 26). Whenever a meta-analysis was possible to compare robotic multiquadrant procedures vs. laparoscopic procedures, the odds ratio (OR) and 95% CI were estimated using the Mantel–Haenszel method for binary outcome data. The mean differences (MD) and 95% CIs were estimated using inverse variance weighting for continuous data. Heterogeneity was assessed using the I2 statistic, and values of 25%, 50%, and 75% were considered low, moderate, and high, respectively (25, 27). Random-effects models were used to explore potential inter-study heterogeneity. The effect was considered significant at p < 0.05. The meta-analysis was performed using RevMan software (version 5.4; Cochrane Collaboration 2020, Copenhagen, Denmark).
3. Results
3.1. Single center experience
Between January 2014 and December 2021, 16 consecutive patients underwent robotic TPC with IPAA. The clinical and surgical characteristics of the series are described in Table 1. Patients were relatively young (mean age: 44.42 (SD: 3.37) years) and predominantly male. The most frequent indication for surgery was ulcerative colitis (UC).
Fourteen patients underwent a totally robotic two-stage TPC with IPAA, and 2 underwent a totally robotic three-stage procedure with a TC and a double-barreled ileo-sigmoido ostomy (first step), a CP with IPAA and a loop ileostomy (second step), followed by an ileostomy reversal (third step). The mean operative time was approximately 271 min with no conversions to laparoscopy or open approach. Two patients (12.5%) with a Dindo-Clavien ≥ III complication (i.e., anastomotic leak) were treated with percutaneous drainage and intravenous antibiotics in the postoperative period. The mean hospital stay was >8 days. Mortality was nil. The last surgical stage (loop ileostomy closure) was completed in all patients. The Wexner score for fecal incontinence was assessed at 3 months after ileostomy closure: 9 (56.5%) patients were asymptomatic (0–4), 5 (31%) had moderate symptoms (5–9), and 2 (12.5%) had severe symptoms.
3.2. Systematic review and meta-analysis
3.2.1. Literature search and selection
After removing duplicates, the literature search yielded 172 articles for screening on title and abstract. Of these, 31 were selected for a full-text evaluation and 7 additional studies were identified by crosschecking reference lists. A total of 23 studies (including 4 conference abstracts) fulfilled the selection criteria and were finally included in this systematic review (Figure 1).
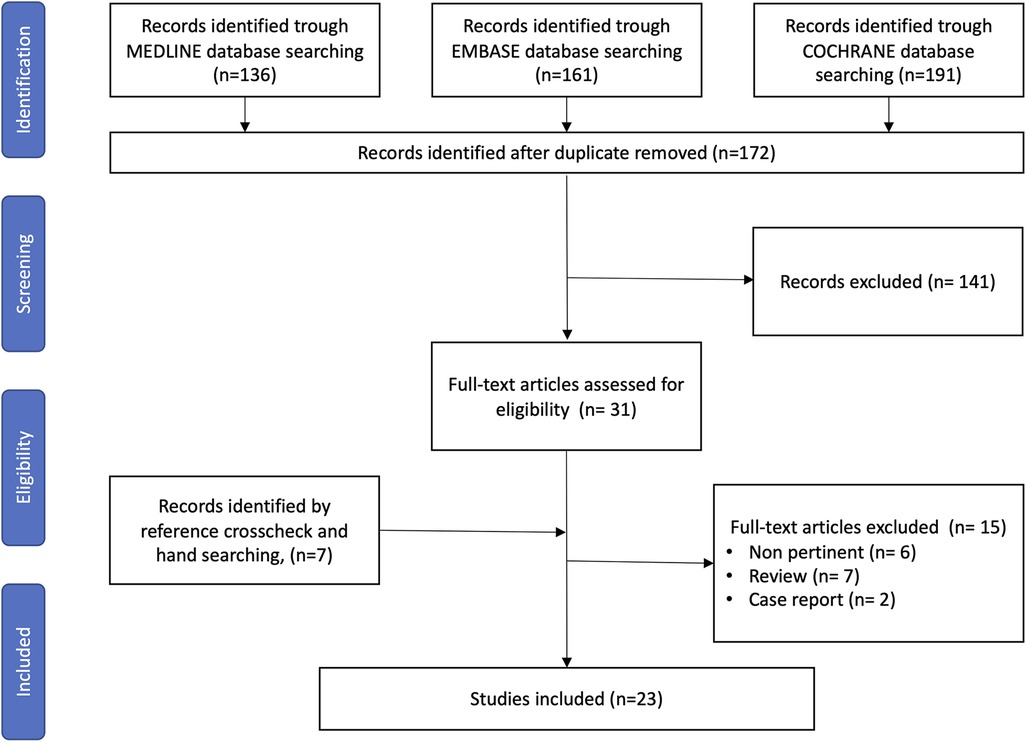
Figure 1. PRISMA flow diagram for study search, selection, inclusion, and exclusion. Example of the research strategy: ((robotic[Title/Abstract])) OR (robotic surgery[Title/Abstract])) OR (robotics[Title/Abstract])) OR (robotic procedure[Title/Abstract])) OR (minimally-invasive surgery[Title/Abstract]))) AND ((((((((((((((((total proctocolectomy[Title/Abstract]) OR (subtotal colectomy[Title/Abstract])) OR (total colectomy[Title/Abstract])) OR (completion proctectomies[Title/Abstract])) OR (completion proctectomy[Title/Abstract])) OR (ileal pouch-anal anastomosis[Title/Abstract])) OR (multiquadrant surgery[Title/Abstract])) OR (multiquadrant abdominal surgery[Title/Abstract])) OR (loop ileostomy[Title/Abstract])) OR (restorative proctocolectomy[Title/Abstract])) OR (restorative coloproctectomy[Title/Abstract])) OR (proctocolectomy[Title/Abstract])) OR (Coloproctectomy[Title/Abstract]))).
3.2.2. Study characteristics
The 23 selected studies were published between 2004 and 2021; they consisted of 15 cohort studies (2, 7, 28–40) and 8 case series (1, 41–47). All had a retrospective design. One study was based on data from nationwide databases (NIS) (34), and all the others were based on single-center experience. The characteristics of the selected studies are summarized in Table 2.
Of the comparative studies, ten papers and three conference abstracts compared robotic and laparoscopic procedures; three papers were matched case-control studies (31, 36, 37), and ten were cohort studies (2, 7, 28–30, 32–35, 38–40). One cohort study compared robotic to open procedures (33), and another compared robotic with laparoscopic and open procedures (34).
For comparatives and case series studies, we considered short-term postoperative outcomes and observed a 30-day postoperative period of follow-up in all studies. Two cohort studies (31, 35) and two case series (42, 44) reported functional outcomes. Only one cohort study described the quality of life in patients (35).
Overall, the included studies analyzed a total of 28,315 patients undergoing colorectal surgical procedures between 2001 and 2020; of these, 10,640 patients underwent a multiquadrant surgery (736 by robotic and 9,904 by laparoscopy).
In the robotic group, 36 patients underwent an STC, 371 a TC, 166 a TPC, and 163 a CP. The main surgical indication for robotic surgery was UC, concerning more than 50% of the patients; other indications included colorectal cancers and benign tumors in 18.6% and 8%, respectively. The main indications for laparoscopy were UC, colorectal cancers, and functional disorders in 31.8, 18.9 and 14.3% of patients, respectively (Table 3).
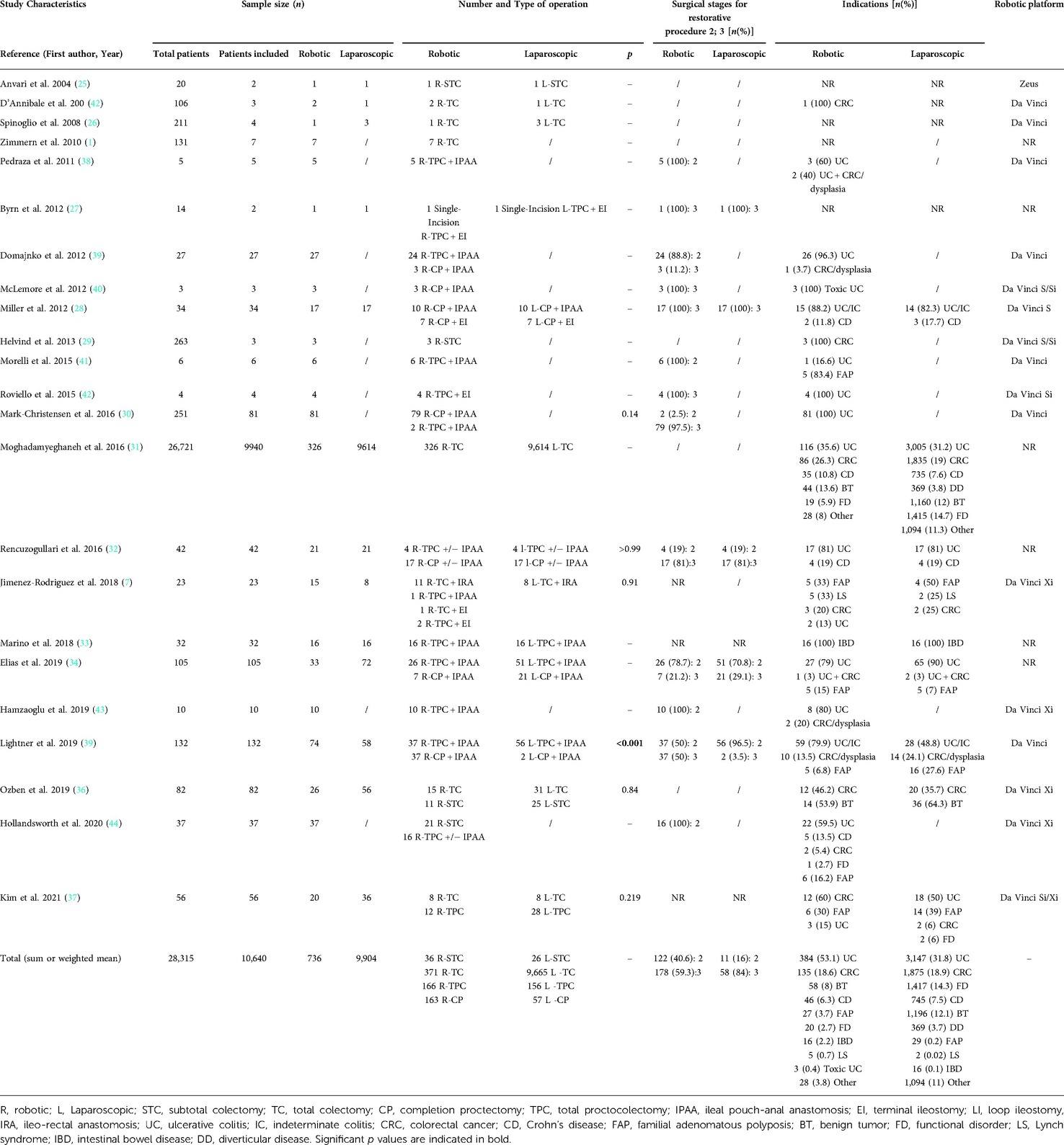
Table 3. Included study characteristics.
3.2.3. Robotic surgical approach
3.2.3.1. Subtotal colectomy
Four studies reported the outcomes of 36 patients who underwent STC (28, 32, 39, 47) (Table 4). The first literature report of a robotic-assisted STC was published by Anvari et al. in 2004 (28), performed by using the Zeus Microwrist System (Computer Motion, Santa Barbara, CA) with a robotic/laparoscopic hybrid approach. Most other cases (32 interventions; 88.8%) were performed with a totally robotic technique and operated with the Da Vinci Xi robotic platform with a single docking approach and two boom placements.
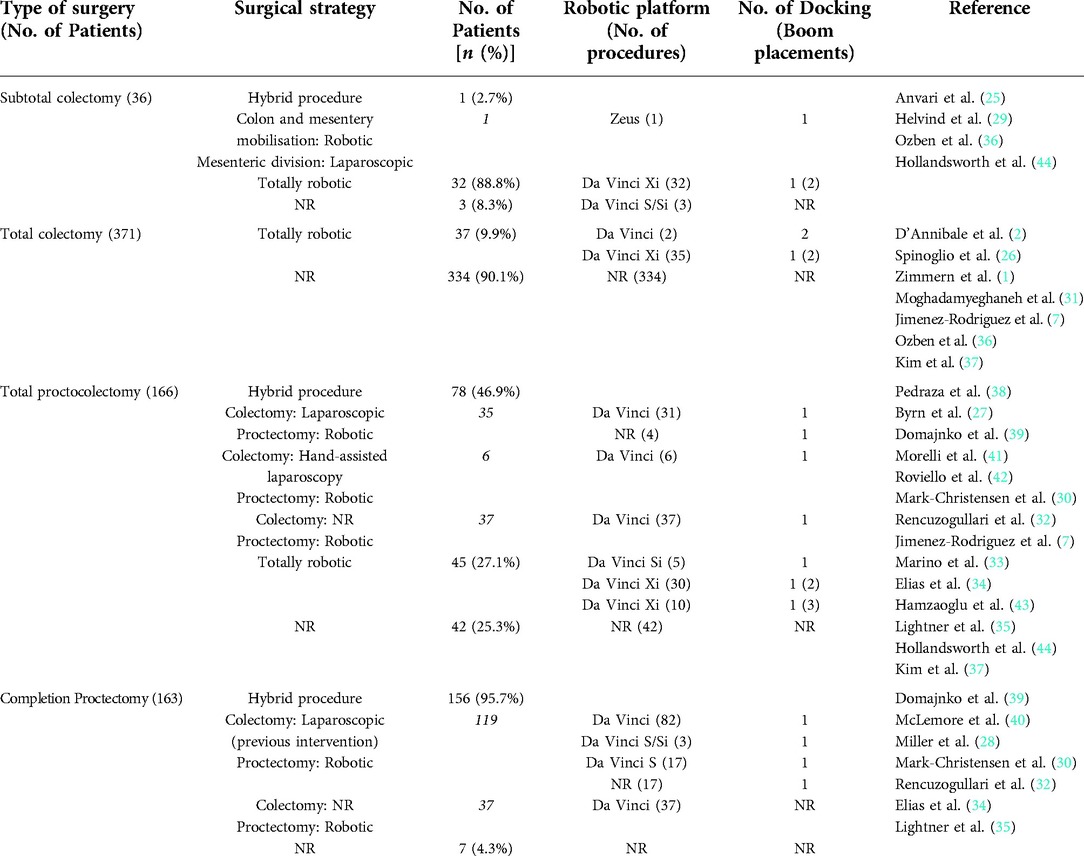
Table 4. Robotic multiquadrant surgery type.
3.2.3.2. Total colectomy
Seven studies analyzed 371 robotic TC procedures (1, 2, 7, 29, 34, 39, 40) (Table 4). Most interventions (334; 92%) were described in a retrospective study based on a national database with little information on the technique and the surgical platform. The remaining 37 procedures were performed using a fully robotic approach: 2 with a non-specified da Vinci platform with 2 dockings and 37 with the da Vinci Xi platform with a single docking and two boom placements.
3.2.3.3. Total proctocolectomy
Overall, 166 TPC were described in 14 studies (7, 30, 33, 35–38, 40–42, 44–47) (Table 4). A hybrid approach was defined as a laparoscopically performed colectomy and a robotic proctectomy for half the cases (78; 46.9%). When reported, the da Vinci robotic platform was used for the hybrid technique. In 45 (27.1%) patients, a totally robotic technique for TPC was described, 40 procedures were performed using the da Vinci Xi platform with a single docking and two or three boom placements in 30 and 10 patients, respectively. In two series, 5 patients underwent a totally robotic TPC with a da Vinci Si platform with a single docking approach (40, 45). The technique used to perform the colectomy in hybrid procedure TPC was laparoscopy in 35 patients and hand-assisted laparoscopy in 6 patients; the technique was unreported in the remaining 37 procedures.
3.2.3.4. Completion proctectomy
In all described cases (156 patients) reported in 7 studies (31, 33, 35, 37, 38, 42, 43) (Table 4), the robotic CP was part of a hybrid approach preceded by a colectomy performed laparoscopically (119 patients) or an undescribed technique (37 patients). In none of the reported cases, the colectomy was performed with a robotic approach. Da Vinci S and Si robotic platforms were used in the reported cases.
Only two studies included CP exclusively (20 patients) (31, 43). All other cases were a part of a series of TPC and CP.
3.2.4. Total and subtotal colectomy
3.2.4.1. Operative outcomes
Six cohort studies (2, 7, 28, 29, 34, 39, 40) and 3 case series were considered (1, 32, 47) in the subgroup of the TC and STC. All cohort studies compared robotic and laparoscopic procedures. Only one study compared the robotic surgical outcome with laparoscopic and open procedures (34). In total, 407 robotic procedures (36 STC and 371 TC) were compared with 9,691 laparoscopic (26 STC and 9,665 TC) procedures.
Weighted mean operative time was 331.5 min for the robotic approach and 251.1 for the laparoscopic approach. The MD was 104.64 min in favor of laparoscopy (95% CI, 18.42, 190.87; p = 0.02; I2 = 58%). Conversion to open surgery was reported in 1.7% of patients who underwent robotic surgery and 13.8% in the laparoscopic procedure. The overall OR for conversion in TC and STC was 0.17 (95% CI, 0.04–0.82; p = 0.03) in favor of robotic with moderate heterogeneity (I2 = 38%). Anastomosis was fashioned in 37 out of 40 patients in the robotic group and all 38 patients in the laparoscopic group. In the robotic procedures, all anastomoses were stapled, while in laparoscopic procedures, 12.8% were hand-sewn. The intraoperative complication rate was 6.25% in the laparoscopic approach, whereas no intraoperative complication occurred for the robotic approach (Tables 5, Figure 2).
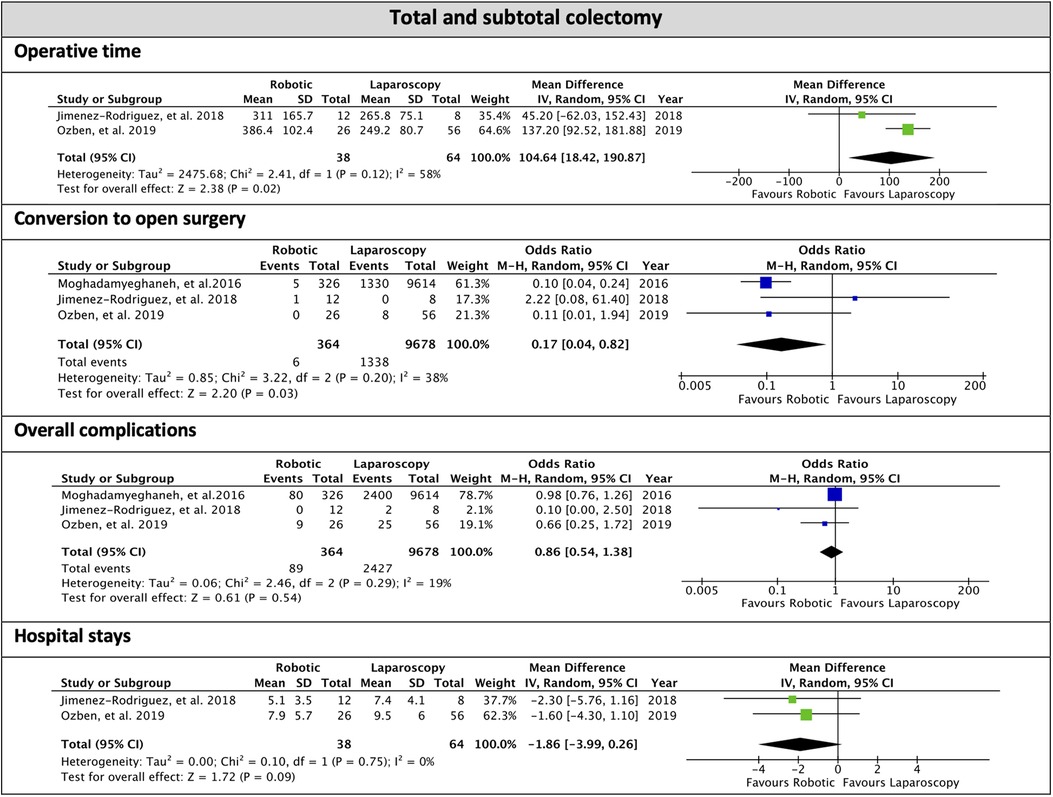
Figure 2. Subgroup of total and subtotal colectomy, forest plots of the overall analysis.
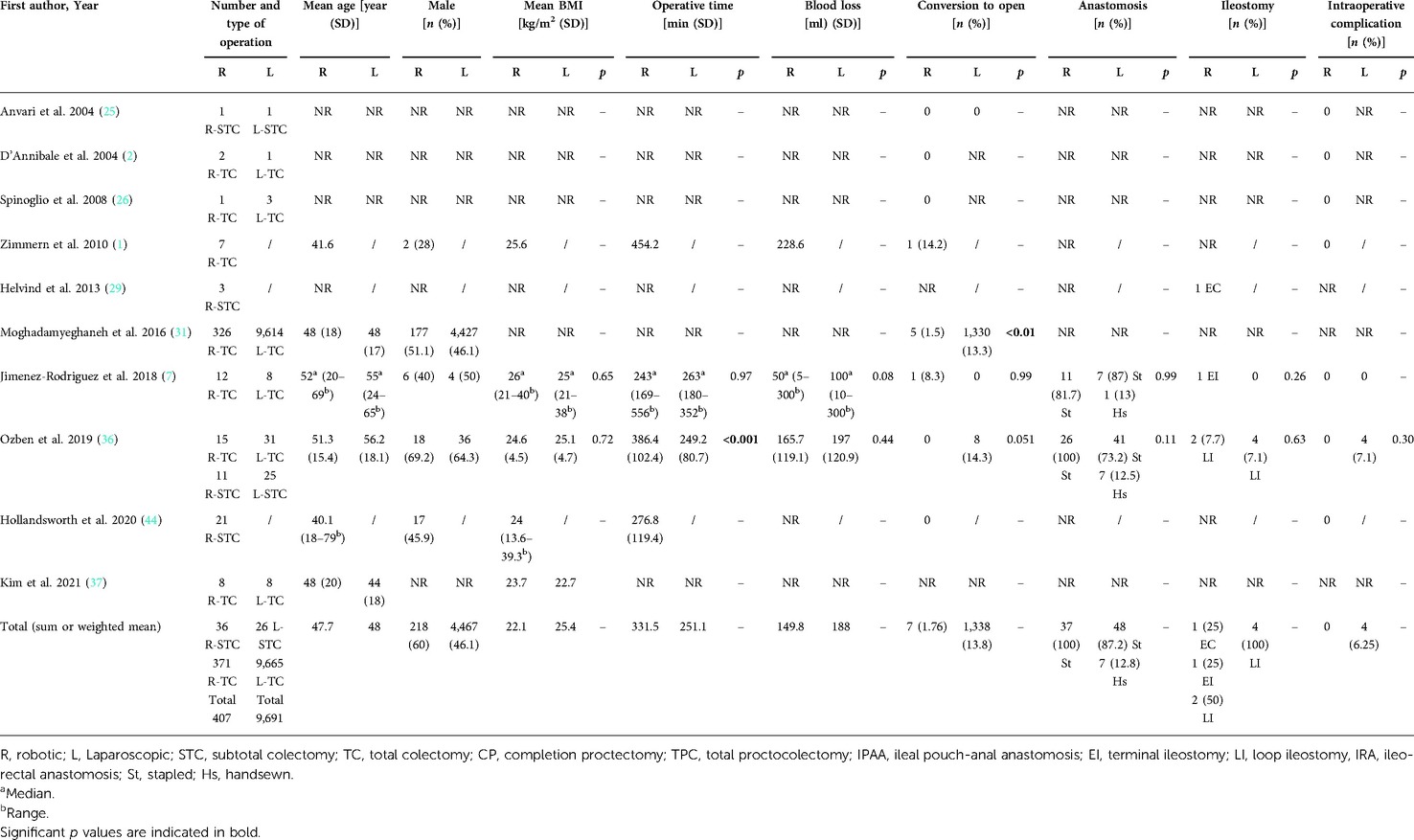
Table 5. Total and subtotal colectomy—operative outcomes.
3.2.4.2. Post-operative outcomes
Postoperative complications occurred in 28.4% of the robotic and 25.7% of laparoscopic procedures. The overall OR for postoperative complications was 0.86 (95% CI, 0.54, 1.38; p = 0.54) with low heterogeneity (I2 = 19%).
Anastomotic leakage was reported only in 2 cohort studies (7, 39) and one case series (47); it occurred in 1.6% of robotic and 6.2% of laparoscopic procedures. Intrabdominal abscess followed 2.0% of robotic, 1.89% of laparoscopic interventions. Reoperation was necessary in 4.2% of robotic and 10.9% of laparoscopic procedures.
Hospital stay was reported in 4 studies on the robotic (1, 7, 39, 47) and only 2 studies on the laparoscopic approach (7, 39). The meta-analysis showed an overall MD of 1.86 days between robotic and laparoscopic surgery (95% CI, −3.99, 0.26; p = 0.09) with moderate heterogeneity (I2 = 38%).
Overall, the readmission rate was 30.3% and 10.9% in robotic and laparoscopic surgery, respectively.
No postoperative mortality was reported after robotic procedures, whereas an overall postoperative mortality rate of 0.85% was described for laparoscopic surgery (Table 6, Figure 2).
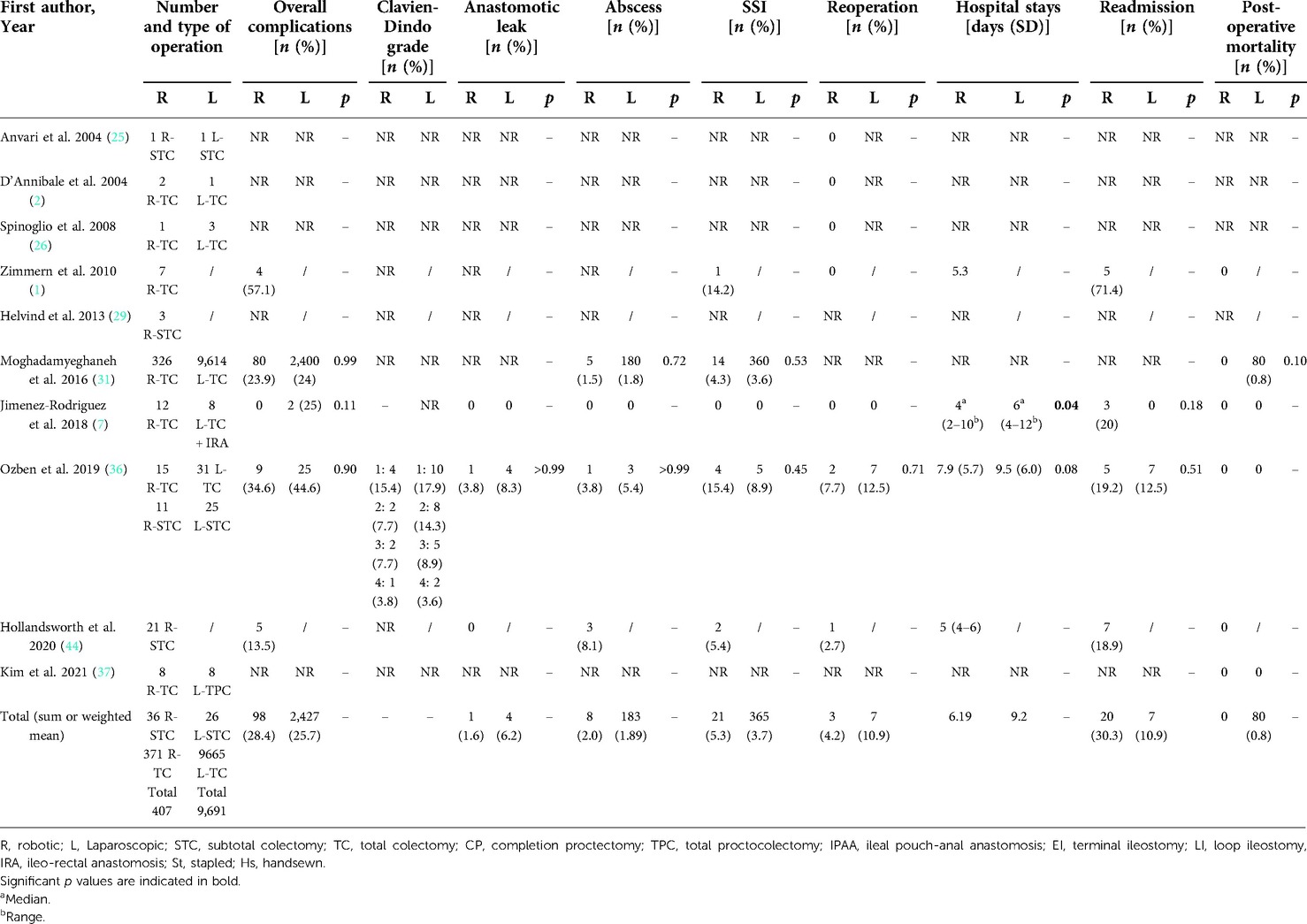
Table 6. Total and subtotal colectomy—post-operative outcomes.
3.2.5. Total proctocolectomy and completion proctectomy
3.2.5.1. Operative outcomes
In the subgroup of TPC and CP, 8 cohort studies (30, 31, 33, 35–38, 40) and 8 case series were considered (7, 41–47). One cohort study used a series of open procedures (33), whereas all the others used laparoscopic series to compare the outcomes of robotic surgery.
In total, 329 robotic procedures (166 TPC and 163 CP) were compared with 213 laparoscopic (156 TPC and 57 CP) procedures.
In 59.3% of the robotic and 63.3% of the laparoscopic procedures, a 3-stage strategy was adopted (Table 3).
No differences were found in the surgical strategy; 59.3% of patients in the robotic group had a three-stage strategy versus 63.4% in the laparoscopic group (Table 3). The overall OR to perform a three-stage procedure was 2.55 (95% CI, 0.24, 27.60; p = 0.44; I2 = 90%) with no differences between robotic and laparoscopy. In the robotic surgery group, restorative IPAA was performed in 94.8% of patients; in the remaining patients, an ileorectal anastomosis and an end-ileostomy were performed in 0.9% and 3.7%, respectively. In the laparoscopic group, an IPAA was fashioned in 94.8% of patients and an end-ileostomy in 5.5%. Operative time was prolonged in robotic compared to laparoscopic interventions (MD 38.8; 95% CI, 18.7, 59.06; p = 0.0002; I2 = 36%). Blood loss did not significantly differ between the two surgical methods (MD 57.99; 95% CI, −65.2, 181.17; p = 0.36; I2 = 81%). The anastomosis was stapled in 95.7% of the robotic and 98.8% of the laparoscopic group. A loop ileostomy was performed in 92.7% of robotic and 88.6% of laparoscopic patients.
Conversion to open surgery during TPC and CP occurred in 3.4% of the robotic and 4.4% of the laparoscopic group. The overall OR for conversion was 0.45 (95% CI, 0.09, 2.26; p = 0.33; I2 = 0%)showing no differences between the approaches.
Intraoperative complications occurred in 2% and 2.6% of the robotic and laparoscopic groups, respectively (Table 7, Figure 3).
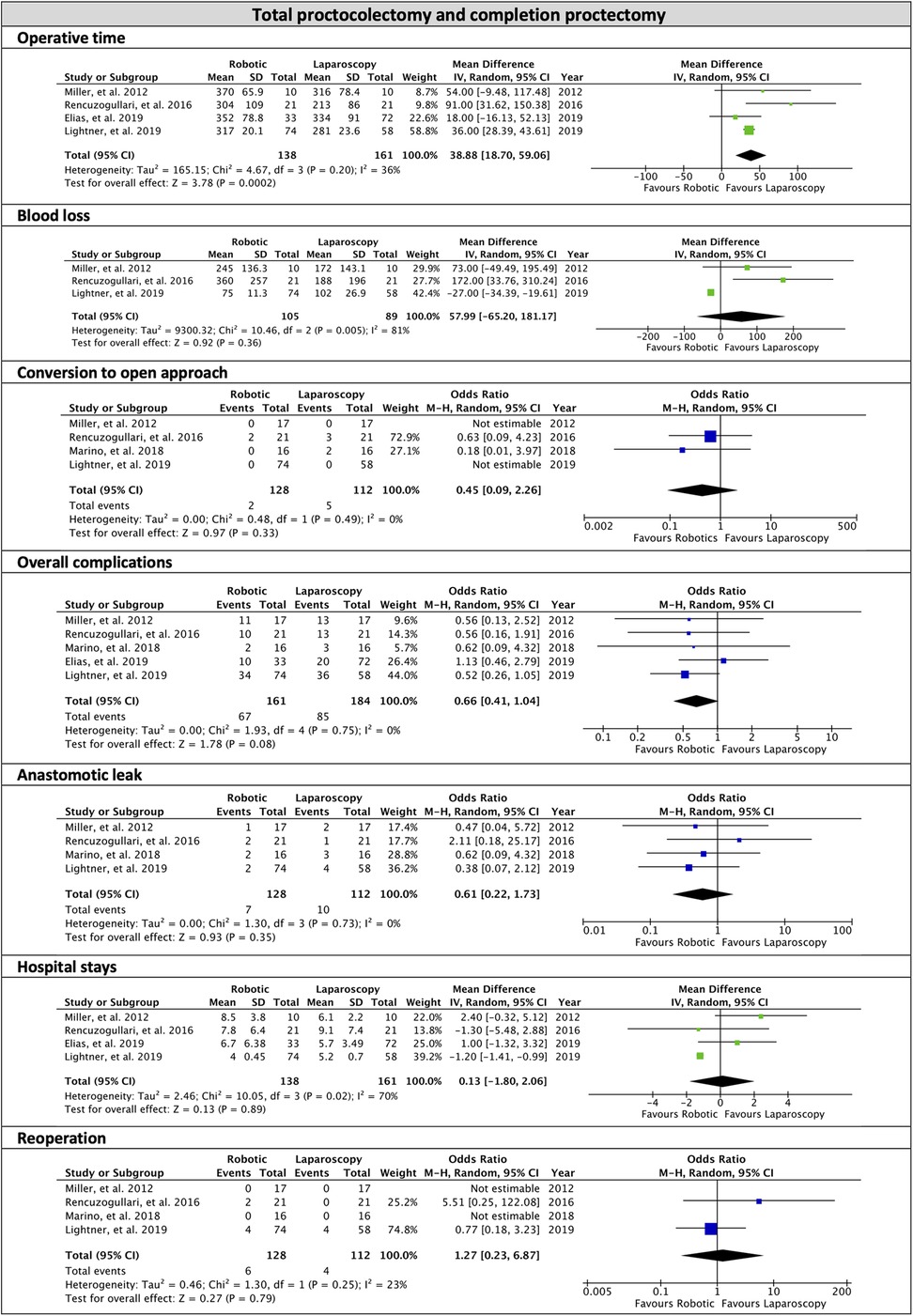
Figure 3. Subgroup of total proctocolectomy and completion proctectomy, forest plots of the overall analysis.
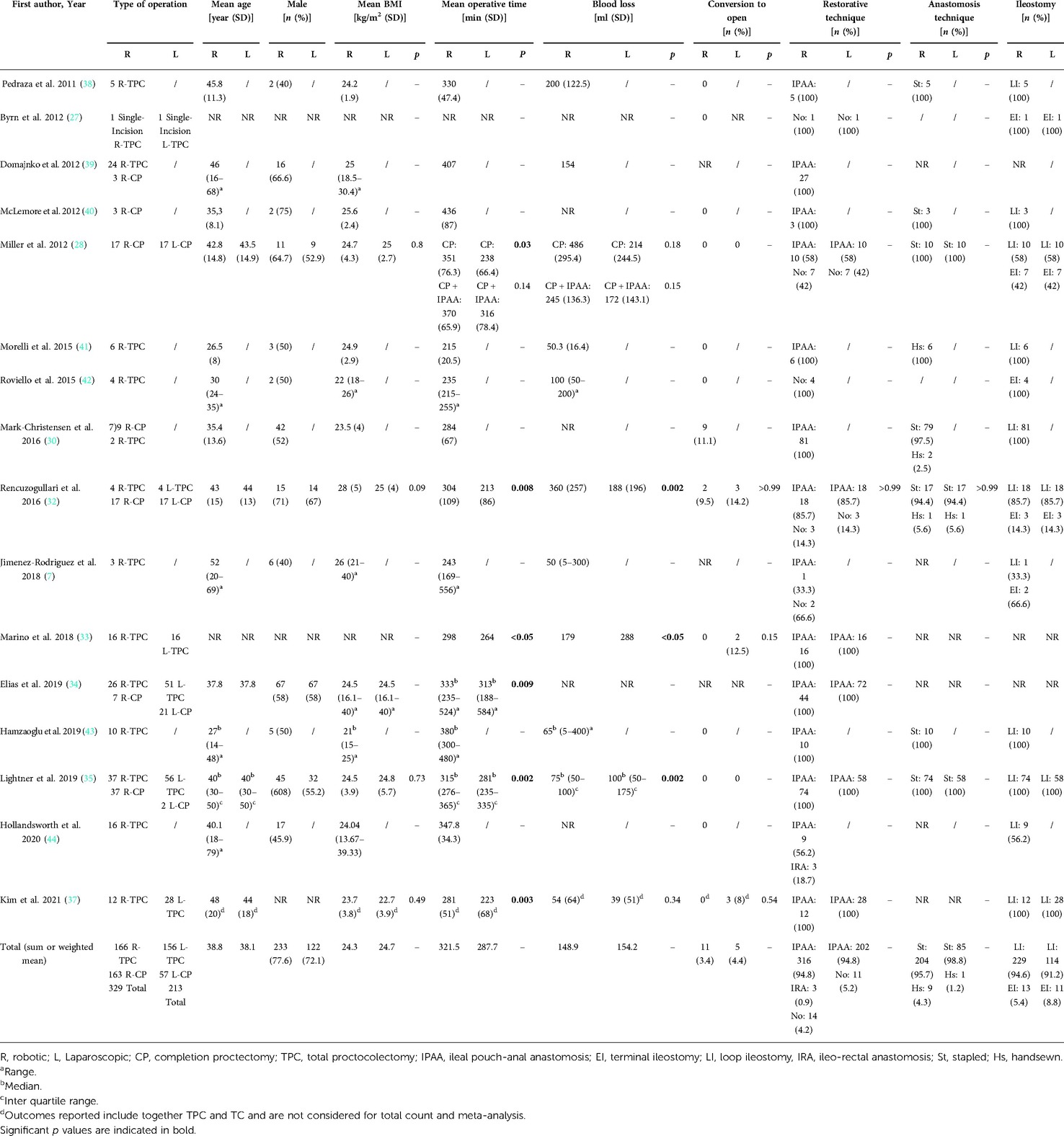
Table 7. Total proctocolectomy and completion proctectomy—operative outcomes.
3.2.5.2. Post-operative outcomes
Overall postoperative complications occurred in 47.4% of the robotic and in 46.1% of laparoscopic procedures during TPC and CP, with an OR of 0.66 (95% CI, 0.41, 1.04; p = 0.08) and no heterogeneity (I2 = 0%). Clavien-Dindo grading system was reported in 4 series of robotic surgery (33, 37, 43, 45) and only one of laparoscopy surgery (33, 37); in the robotic group, 72.6% of the complications were classified as grade I–II, and 27.4% were grade III–IV. Anastomotic leakage occurred in 4.9% of robotic and 8.9% of laparoscopic procedures, with an OR of 0.61 (95% CI, 0.22, 1.73; p = 0.35) and no heterogeneity (I2 = 0%). Reoperation was necessary for 6.7% of robotic and 3.5% of laparoscopic interventions (OR: 1.27; 95% CI, 0.23, 6.87; p = 0.79; I2 = 23%). The MD for hospital stay was 0.13 days (95% CI, −1.80, 2.06; p = 0.89) with high heterogeneity (I2 = 70%). No postoperative mortality was reported in both groups. Readmission was reported in 22% of robotic and 17.8% of laparoscopic patients (Table 8, Figure 3).
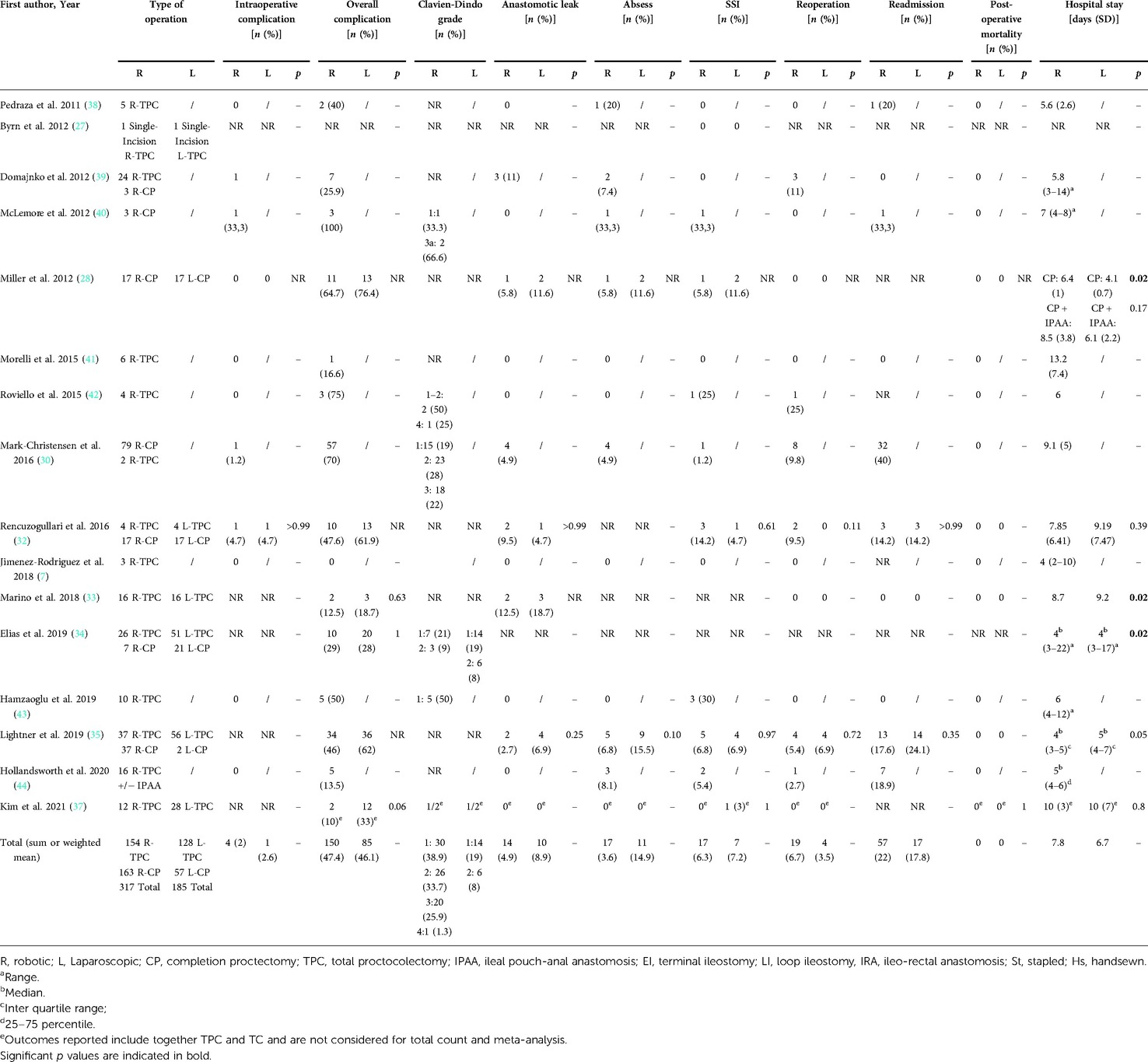
Table 8. Total proctocolectomy and completion proctectomy—operative and post-operative outcomes.
3.2.6. Study quality assessments
According to the NOS, the quality of the retrospective cohort studies was 8/9 in 2 studies (33, 34), 7/9 in 7 studies (7, 31, 32, 35, 38–40), 6/9 in 4 studies (2, 28, 29, 37), 5/9 in one study (30) and 4/9 in one study (36).
Based on the quality assessment described by Murad (23), 3 series received a score of 6/8 (41, 43, 47) and 5 received a grade of 5/8 (1, 42, 44–46). Overall, the 23 studies were considered at high risk of bias.
Based on the GRADE system, the overall quality of evidence was rated as low. The study quality and risk of bias of the included studies are summarized in the additional file: Table Supplementary 3.
4. Discussion
Multiquadrant colorectal procedures represent challenging interventions performed with a totally robotic approach. However, our single-center experience and an appraisal of the literature support the safety and feasibility of robotic TPC, associated with satisfactory postoperative outcomes comparable to laparoscopy. Specifically, for STC and TC, the robotic approach appeared to be associated with a lower conversion rate than laparoscopy. We found a trend in favor of robotic surgery for the duration of hospital stay (for TC and STC procedures) and the overall rate of postoperative complications (for TPC and CP procedures). However, the operative time was longer for robotic procedures than laparoscopy.
Interest in robotic-assisted colorectal surgery has risen exponentially (48) in the last few years, with a consequent increase in the number of original articles and reviews published each year (49). There is a paucity of data on the application of robotic surgery for multiquadrant resections. A recent systematic review examined the outcomes of restorative proctocolectomy, limiting the analysis to robotic proctectomy or proctocolectomy with IPAA (50). Based on 6 comparative studies and 3 case series, the authors preferred the robotic platform for similar (or slightly better) outcomes than laparoscopy (50). The present systematic review updates these findings with the most recent evidence and considers TC and STC procedures performed robotically. Notably, staged procedures were often performed using a hybrid approach, implying that colectomy was often performed laparoscopically, whereas CP used a robotic platform. Even if only the proctectomy was performed with the help of the robotic platform, CP were included in this study as a part of staged multiquadrant robotic procedures. Concerning the small bowel mesentery mobilization in CP, only three studies described the technique used and in all of them the mobilization was performed laparoscopically (31, 33, 43). Interestingly, in the mentioned studies all the surgeries were performed with the old generation robotic platform that could not provide access to all four abdominal quadrants with a single cart positioning (7–9) and this could influence the choice in favor to the laparoscopic approach. This finding was also observed for TPC, which could lead to missing evidence on the potential advantages of an approach over the other because longer operative times may be necessary to allow the shift from laparoscopy to robotic surgery during the same procedure.
Despite this heterogeneity, the overall evidence is based on a not negligible sample, accounting for more than 10,600 patients who underwent a robotic or laparoscopic procedure, suggesting that minimally invasive surgery for multiquadrant colorectal resections is widespread and acceptable. This evolution may be also linked to the introduction of the da Vinci Xi surgical system, characterized by the boom-mounted arms and the ability of the boom to rotate and provide access to all four abdominal quadrants with a single cart positioning (7–9). Most totally robotic procedures used the da Vinci Xi system with a single docking approach. The only difference in the surgical technique was the number of boom placement, which varied from 2 to 3 on some occasions when proctectomy was needed. This strategy is in accordance with Protyniak et al. (8), who demonstrated that the Xi platform can be used for multiquadrant surgery without repositioning the patient-side surgical cart. Recently two comparative studies (7, 39) and two case series (46, 47) evaluated the da Vinci Xi surgical system and multiquadrant surgery for TC, STC, and restorative TPC, using a totally robotic approach. All authors agreed that the robotic platform offered a significant advantage over the previous generations. Likewise, we reported our experience with the technical note to perform totally robotic TPC, using the totally robotic approach (Supplementary material).
There is consistent literature indicating that the operative time for robotic multiquadrant procedures is longer than laparoscopy. Only one study showed no differences in the operative time between 15 robotic procedures (TC and TPC) and 8 laparoscopic TC (7). In this study, all the patients were operated using the da Vinci Xi system, and the authors justified these findings, attributing a major advantage of the robotic platform over the previous versions. Morelli et al. demonstrated evidence supporting the advantages of the da Vinci Xi over the da Vinci Si for multiquadrant and combined procedures (51, 52).
The present study findings are limited by the nature of the studies included. The available literature consists of retrospective case series or cohort studies. No RCT was found, and its performance would be extremely hazardous. A high degree of heterogeneity in the surgical techniques was noted, also regarding the different indications for surgery. We tried to overcome this bias by performing separated analysis for procedures including or not a proctectomy. Sensitivity analyses were not performed due to the paucity of data on the subgroups of patients and procedures. Similarly, it was not possible to analyze the outcomes of the alternative surgical strategies for TPC, comparing two- to three-stage surgeries, for example. Four comparative studies reported a combination of two- and three-stage procedures (33, 35, 37, 38), and only one cohort by Lightner et al. reported a significant difference between the procedures (38). However, the meta-analysis showed no differences in the surgical strategy adopted. Outcomes were limited to operative and postoperative variables. Patient-centered outcomes, including urological, sexual dysfunction, and quality of life, remain essentially unexplored (53).
Our experience and a systematic review of the literature suggest that robotic multiquadrant colorectal surgery is safe and effective, with low morbidity and mortality rates. The overall level of evidence merging from the present systematic review was judged as low. The functional outcomes associated with robotic TPC, TC, STC, or CP should be the focus for future studies.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author contributions
NdeA, GB and GS participated to study conception and design. GB, MCC and NdeA contributed to acquisition of data. NdeA, GB, AMP and PG contributed to analysis and interpretation of data. GB and NdeA participated to drafting of manuscript. GLdeA, AMP, GS, IS, MU, FC, CAS and PG contributed to the critical revision of manuscript. All authors contributed to the article and approved the submitted version.
Funding
G. Spinoglio received honoraria as proctor for Intuitive Surgical.
Conflict of interest
G. Spinoglio received honoraria as proctor for Intuitive Surgical. All other authors have no conflicts of interest to declare in relation to the matter of this publication.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2022.991704/full#supplementary-material.
References
1. Zimmern A, Prasad L, Desouza A, Marecik S, Park J, Abcarian H. Robotic colon and rectal surgery: a series of 131 cases. World J Surg. (2010) 34(8):1954–8. doi: 10.1007/s00268-010-0591-4
2. D’Annibale A, Morpurgo E, Fiscon V, Trevisan P, Sovernigo G, Orsini C, et al. Robotic and laparoscopic surgery for treatment of colorectal diseases. Dis Colon Rectum. (2004) 47(12):2162–8. doi: 10.1007/s10350-004-0711-z
3. Aly EH. Robotic colorectal surgery: summary of the current evidence. Int J Colorectal Dis. (2014) 29(1):1–8. doi: 10.1007/s00384-013-1764-z
4. Trinh BB, Jackson NR, Hauch AT, Hu T, Kandil E. Robotic versus laparoscopic colorectal surgery. JSLS. (2014) 18(4):e2014.00187, 1–11. doi: 10.4293/JSLS.2014.00187
5. Baik SH, Kwon HY, Kim JS, Hur H, Sohn SK, Cho CH, et al. Robotic versus laparoscopic low anterior resection of rectal cancer: short-term outcome of a prospective comparative study. Ann Surg Oncol. (2009) 16(6):1480–7. doi: 10.1245/s10434-009-0435-3
6. Kim JC, Lee JL, Yoon YS, Kim CW, Park IJ, Lim SB. Robotic left colectomy with complete mesocolectomy for splenic flexure and descending colon cancer, compared with a laparoscopic procedure. Int J Med Robot. (2018) 14(5):e1918. doi: 10.1002/rcs.1918
7. Jimenez-Rodriguez RM, Quezada-Diaz F, Tchack M, Pappou E, Wei IH, Smith JJ, et al. Use of the Xi robotic platform for total abdominal colectomy: a step forward in minimally invasive colorectal surgery. Surg Endosc. (2019) 33(3):966–71. doi: 10.1007/s00464-018-6529-x
8. Protyniak B, Jorden J, Farmer R. Multiquadrant robotic colorectal surgery: the Da Vinci Xi Vs Si comparison. J Robot Surg. (2018) 12(1):67–74. doi: 10.1007/s11701-017-0689-x
9. Ozben V, Cengiz TB, Atasoy D, Bayraktar O, Aghayeva A, Erguner I, et al. Is Da Vinci Xi better than Da Vinci Si in robotic rectal cancer surgery? Comparison of the 2 generations of Da Vinci systems. Surg Laparosc Endosc Percutan Tech. (2016) 26(5):417–23. doi: 10.1097/SLE.0000000000000320
10. Hennessy O, Egan L, Joyce M. Subtotal colectomy in ulcerative colitis-long term considerations for the rectal stump. World J Gastrointest Surg. (2021) 13(2):198–209. doi: 10.4240/wjgs.v13.i2.198
11. Murphy B, Kavanagh DO, Winter DC. Modern surgery for ulcerative colitis. Updates Surg. (2020) 72(2):325–33. doi: 10.1007/s13304-020-00719-4
12. Fazio VW, Ziv Y, Church JM, Oakley JR, Lavery IC, Milsom JW, et al. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg. (1995) 222(2):120–7. doi: 10.1097/00000658-199508000-00003
13. Ali U A, Keus F, Heikens JT, Bemelman WA, Berdah SV, Gooszen HG, et al. Open versus laparoscopic (assisted) ileo pouch anal anastomosis for ulcerative colitis and familial adenomatous polyposis. Cochrane Database Syst Rev. (2009) 1:CD006267. doi: 10.1002/14651858.CD006267.pub2
14. Parks AG, Nicholls RJ. Proctocolectomy without ileostomy for ulcerative colitis. Br Med J. (1978) 2(6130):85–8. doi: 10.1136/bmj.2.6130.85
15. Felli E, Brunetti F, Disabato M, Salloum C, Azoulay D, De’angelis N. Robotic right colectomy for hemorrhagic right colon cancer: a case report and review of the literature of minimally invasive urgent colectomy. World J Emerg Surg. (2014) 9:32. doi: 10.1186/1749-7922-9-32
16. Beaugerie L, Blain A, Brazier F, Gornet JM, Parc Y. Traitement De La Rectocolite Ulcéro-Hémorragique Dans Sa Forme Étendue (Colite Grave Exclue). Gatroenterologie clinique et biologique. (2004) 28(10-c2):974–83. GCB-10-2004-28-10-C2-0399-8320-101019-ART9
17. Beaugerie L, Blain A, Brazier F, Gornet JM, Parc Y. [Treatment of extended ulcerative colitis (severe colitis excluded)]. Gastroenterol Clin Biol. (2004) 28(10 Pt 2):974–83. doi: 10.1016/s0399-8320(04)95175-5
18. Jorge JM, Wexner SD. Etiology and management of fecal incontinence. Dis Colon Rectum. (1993) 36(1):77–97. doi: 10.1007/BF02050307
19. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. (2004) 240(2):205–13. doi: 10.1097/01.sla.0000133083.54934.ae
20. Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. (2019) 10:ED000142. doi: 10.1002/14651858.ED000142
21. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. J Clin Epidemiol. (2009) 62(10):1006–12. doi: 10.1016/j.jclinepi.2009.06.005
22. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25(9):603–5. doi: 10.1007/s10654-010-9491-z
23. Murad MH, Sultan S, Haffar S, Bazerbachi F. Methodological quality and synthesis of case series and case reports. BMJ Evid Based Med. (2018) 23(2):60–3. doi: 10.1136/bmjebm-2017-110853
24. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. Grade: an emerging consensus on rating quality of evidence and strength of recommendations. Br Med J. (2008) 336(7650):924–6. doi: 10.1136/bmj.39489.470347.AD
25. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. Br Med J. (2011) 343:d5928. doi: 10.1136/bmj.d5928
26. Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. (2005) 5:13. doi: 10.1186/1471-2288-5-13
27. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Br Med J. (2003) 327(7414):557–60. doi: 10.1136/bmj.327.7414.557
28. Anvari M, Birch DW, Bamehriz F, Gryfe R, Chapman T. Robotic-assisted laparoscopic colorectal surgery. Surg Laparosc Endosc Percutan Tech. (2004) 14(6):311–5. doi: 10.1097/01.sle.0000148473.05042.8f
29. Spinoglio G, Summa M, Priora F, Quarati R, Testa S. Robotic colorectal surgery: first 50 cases experience. Dis Colon Rectum. (2008) 51(11):1627–32. doi: 10.1007/s10350-008-9334-0
30. Byrn J, Carroll S, Cromwell J. Single-incision robotic colectomy versus single-incision laparoscopic colectomy: an early experience. Dis Colon Rectum. (2012) 55(5):e269. doi: 10.1097/DCR.0b013e318256cadc
31. Miller AT, Berian JR, Rubin M, Hurst RD, Fichera A, Umanskiy K. Robotic-assisted proctectomy for inflammatory bowel disease: a case-matched comparison of laparoscopic and robotic technique. J Gastrointest Surg. (2012) 16(3):587–94. doi: 10.1007/s11605-011-1692-6
32. Helvind NM, Eriksen JR, Mogensen A, Tas B, Olsen J, Bundgaard M, et al. No differences in short-term morbidity and mortality after robot-assisted laparoscopic versus laparoscopic resection for colonic cancer: a case-control study of 263 patients. Surg Endosc. (2013) 27(7):2575–80. doi: 10.1007/s00464-013-2792-z
33. Mark-Christensen A, Pachler FR, Norager CB, Jepsen P, Laurberg S, Tottrup A. Short-term outcome of robot-assisted and open ipaa: an observational single-center study. Dis Colon Rectum. (2016) 59(3):201–7. doi: 10.1097/DCR.0000000000000540
34. Moghadamyeghaneh Z, Hanna MH, Carmichael JC, Pigazzi A, Stamos MJ, Mills S. Comparison of open, laparoscopic, and robotic approaches for total abdominal colectomy. Surg Endosc. (2016) 30(7):2792–8. doi: 10.1007/s00464-015-4552-8
35. Rencuzogullari A, Gorgun E, Costedio M, Aytac E, Kessler H, Abbas MA, et al. Case-matched comparison of robotic versus laparoscopic proctectomy for inflammatory bowel disease. Surg Laparosc Endosc Percutan Tech. (2016) 26(3):e37–40. doi: 10.1097/SLE.0000000000000269
36. Marino MV, Glagoleva A. <Marino_2018_Poster.Pdf>. J Crohn’s Colitis. (2018) 12(Suppl. 1):S322. doi: 10.1093/ecco-jcc/jjx180.556
37. Elias AW, Landmann RG. Tu1676 – chasing zero cuff: robotic distal dissection superior to laparoscopy in ileal pouch anal anastomosis. Gastroenterology. (2019) 156(6):S-1496. doi: 10.1016/s0016-5085(19)40818-4
38. Lightner AL, Grass F, McKenna NP, Tilman M, Alsughayer A, Kelley SR, et al. Short-term postoperative outcomes following robotic versus laparoscopic ileal pouch-anal anastomosis are equivalent. Tech Coloproctol. (2019) 23(3):259–66. doi: 10.1007/s10151-019-01953-8
39. Ozben V, de Muijnck C, Karabork M, Ozoran E, Zenger S, Bilgin IA, et al. The Da Vinci Xi system for robotic total/subtotal colectomy vs. Conventional laparoscopy: short-term outcomes. Tech Coloproctol. (2019) 23(9):861–8. doi: 10.1007/s10151-019-02066-y
40. Kim JC, Lee JL, Yoon YS, Kim HM, Kim CW, Park IJ, et al. Entirely robot-assisted total colectomy/total proctocolectomy compared with a laparoscopic approach. Surg Laparosc Endosc Percutan Tech. (2020) 31(4):428–33. doi: 10.1097/SLE.0000000000000883
41. Pedraza R, Patel CB, Ramos-Valadez DI, Haas EM. Robotic-Assisted laparoscopic surgery for restorative proctocolectomy with ileal J pouch-anal anastomosis. Minim Invasive Ther Allied Technol. (2011) 20(4):234–9. doi: 10.3109/13645706.2010.536355
42. Domajnko B, Ognibene S, Farid A, Rauh S. Robotic ileal pouh-anal anastomoses: the first 27 cases. Diseases of the Colon & Rectum. (2012) 55(5):e179–e80. doi: 10.1097/DCR.0b013e318256cadc
43. McLemore EC, Cullen J, Horgan S, Talamini MA, Ramamoorthy S. Robotic-Assisted laparoscopic stage ii restorative proctectomy for toxic ulcerative colitis. Int J Med Robot. (2012) 8(2):178–83. doi: 10.1002/rcs.445
44. Morelli L, Guadagni S, Mariniello MD, Furbetta N, Pisano R, D’Isidoro C, et al. Hand-assisted hybrid laparoscopic-robotic total proctocolectomy with ileal pouch–anal anastomosis. Langenbecks Arch Surg. (2015) 400(6):741–8. doi: 10.1007/s00423-015-1331-x
45. Roviello F, Piagnerelli R, Ferrara F, Scheiterle M, De Franco L, Marrelli D. Robotic single docking total colectomy for ulcerative colitis: first experience with a novel technique. Int J Surg. (2015) 21:63–7. doi: 10.1016/j.ijsu.2015.07.642
46. Hamzaoglu I, Baca B, Esen E, Aytac E, Ozben V, Aghayeva A, et al. Short-term results after totally robotic restorative total proctocolectomy with ileal pouch anal anas- tomosis for ulcerative colitis. Surg Laparosc Endosc Percutan Tech. (2020) 30(1):40–44. doi: 10.1097/SLE.0000000000000645
47. Hollandsworth HM, Stringfield S, Klepper K, Zhao B, Abbadessa B, Lopez NE, et al. Multiquadrant surgery in the robotic era: a technical description and outcomes for Da Vinci Xi robotic subtotal colectomy and total proctocolectomy. Surg Endosc. (2020) 34(11):5153–9. doi: 10.1007/s00464-020-07633-1
48. George EI, Brand TC, LaPorta A, Marescaux J, Satava RM. Origins of robotic surgery: from skepticism to standard of care. JSLS. (2018) 22(4):e2018.00039. doi: 10.4293/JSLS.2018.00039
49. Cuk P, Kjaer MD, Mogensen CB, Nielsen MF, Pedersen AK, Ellebaek MB. Short-term outcomes in robot-assisted compared to laparoscopic colon cancer resections: a systematic review and meta-analysis. Surg Endosc. (2022) 36(1):32–46. doi: 10.1007/s00464-021-08782-7
50. Flynn J, Larach JT, Kong JCH, Warrier SK, Heriot A. Robotic versus laparoscopic ileal pouch-anal anastomosis (IPAA): a systematic review and meta-analysis. Int J Colorectal Dis. (2021) 36(7):1345–56. doi: 10.1007/s00384-021-03868-z
51. Morelli L, Di Franco G, Guadagni S, Palmeri M, Gianardi D, Bianchini M, et al. Full robotic colorectal resections for cancer combined with other major surgical procedures: early experience with the Da Vinci Xi. Surg Innov. (2017) 24(4):321–7. doi: 10.1177/1553350617697183
52. Morelli L, Di Franco G, Guadagni S, Rossi L, Palmeri M, Furbetta N, et al. Robot-assisted total mesorectal excision for rectal cancer: case-matched comparison of short-term surgical and functional outcomes between the Da Vinci Xi and Si. Surg Endosc. (2018) 32(2):589–600. doi: 10.1007/s00464-017-5708-5
Keywords: total proctocolectomy, ileal pouch-anal anastomosis, total colectomy, robotic surgery, ulcerative colitis, familial adenomatous polyposis
Citation: Bianchi G, Gavriilidis P, Martínez-Pérez A, de’Angelis GL, Uzzan M, Sobhani I, Coccolini F, Schena CA, Carra MC, Spinoglio G and de’Angelis N (2022) Robotic multiquadrant colorectal procedures: A single-center experience and a systematic review of the literature. Front. Surg. 9:991704. doi: 10.3389/fsurg.2022.991704
Received: 11 July 2022; Accepted: 3 August 2022;
Published: 17 August 2022.
Edited by:
Gaetano Luglio, University of Naples Federico II, ItalyReviewed by:
Marco Frascio, University of Genoa, ItalySamuel Eisenstein, UC San Diego Health, University of California, United States
© 2022 Bianchi, Gavriilidis, Martínez-Pérez, de'Angelis, Uzzan, Sobhani, Coccolini, Schena, Carra, Spinoglio and de'Angelis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gian Luigi de'Angelis Z2lhbmx1aWdpLmRlYW5nZWxpc0B1bmlwci5pdA==
Specialty Section: This article was submitted to Visceral Surgery, a section of the journal Frontiers in Surgery