
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Surg. , 08 November 2022
Sec. Neurosurgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.971066
This article is part of the Research Topic Chronic Carotid Artery Occlusion: Surgical Techniques, Screening modalities, Evaluation Scale, Prescription, and Beyond View all 8 articles
 Junnan Wu1,†
Junnan Wu1,† Chaoyou Fang2,†Lingying Wei1Yibo Liu3,4
Chaoyou Fang2,†Lingying Wei1Yibo Liu3,4 Houshi Xu2
Houshi Xu2 Xiaoyu Wang3,4Ling Yuan2Xiaoya Wu1*
Xiaoyu Wang3,4Ling Yuan2Xiaoya Wu1* Yuanzhi Xu5*
Yuanzhi Xu5* Anke Zhang3,4*
Anke Zhang3,4*
Chronic internal carotid artery occlusion (CICAO) has high prevalence and incidence rates, and patients with CICAO can be completely asymptomatic, experience a devastating stroke or die. It is important to note that CICAO causes cerebrovascular accidents. Currently, the external carotid-internal carotid (EC-IC) bypass technique is used to treat CICAO. However, many clinical studies showed that EC-IC bypass was not beneficial for many patients with CICAO. Meanwhile, endovascular intervention treatment options for CICAO are evolving, and an increasing number of patients are undergoing endovascular intervention therapy. Accordingly, a review comparing both techniques is warranted. For this review, we searched PubMed and collected relevant case study reports comparing endovascular interventional therapy and internal and external cervical bypass surgeries to provide strategies for clinical treatment.
Internal carotid artery occlusion (ICAO) can be classified as acute internal carotid artery occlusion (AICAO) and CICAO (1–4). Normally, complete internal carotid occlusion that lasts more than 4 weeks is considered CICAO (5). The main causes of CICAO include carotid atherosclerotic disease, heart-derived thrombosis, and carotid artery dissection (6, 7). Previous studies revealed that CICAO is usually a result of complex hemodynamics, such as low shear stress, blood flow stasis, and blood flow separation (8, 9). In addition, radiation therapy may cause chronic occlusion of the carotid artery (10). Of note, occlusion caused by carotid dissection mainly occurs in young individuals, and the pathogenic site is often at the entrance of hard vessels (11). In elderly individuals, occlusion is usually caused by atherosclerosis, which generally occurs proximal to the internal carotid artery. Additionally, CICAO caused by atherosclerotic plaque of the stenotic carotid artery is the underlying cause of major ischemic strokes (12).
Antiplatelet aggregation therapy is currently the basic treatment for secondary prevention of ischemic cerebrovascular disease. Low-dose aspirin (75–150 mg) is effective for secondary prevention of minor stroke or TIA episodes and can significantly reduce the risk of vascular events (13). However, healthy lifestyle changes, including healthy diet and appropriate exercising can reduce the risk of stroke with no need for additional medical intervention in partial patients with CICAO. Most symptomatic patients require an urgent visit to the hospital for treatment (14). In terms of drug treatment, if there are no contraindications, it is recommended to take double antibody within 3 months after the onset, and then long-term monoclonal antibody platelet aggregation treatment (13). A previous study showed that patients receiving conservative treatment for CICAO-induced stroke had poor outcomes (15). In addition, Robert et al. also mentioned that with medical treatment alone, the risk of ipsilateral ischemic stroke 2 years after carotid occlusion is still 5%–8% per year (16). Therefore, while medication can reduce the risk of stroke, it does not eliminate the risk entirely (17). The combination of conservative treatment and surgical intervention may be an effective approach for patients with CICAO. With the development of clinical management, there are various approaches to treat symptomatic patients with CICAO, such as conservative treatment, surgical EC-IC bypass, endovascular interventional therapy, carotid endarterectomy, and hybrid surgery (14, 18).
Currently, surgical revascularization (EC-IC bypass) improves cerebral hemodynamics and oxygen extraction fraction and is used as a primary treatment option for patients with CICAO (19, 20). However, a large-scale cohort study showed that most patients with CICAO are not suitable for EC-IC bypass (21, 22). In addition, several studies of patients treated with endovascular or hybrid therapy have shown positive outcomes, which reflects the clinical value of either treatment. In this review, we summarize these treatment modalities based on the current data and evidence, compare the treatment effects of EC-IC bypass and endovascular treatment, and provide a reference for the choice of clinical treatment modalities.
The clinical manifestations of CICAO vary widely; patients may be completely asymptomatic, experience a devastating stroke or die (23). An epidemiological study based on Americans showed that the incidence of ICAO is approximately 6 per 100,000, and approximately 60,000 cases of first stroke are diagnosed as ICAO (24, 25). The severity of the disease depends on the collateral circulation status, and well-compensated patients may be asymptomatic. Nevertheless, approximately 2%–8% of patients progress from asymptomatic occlusion to symptomatic occlusion every year, with an annual stroke rate of 4.4% and an annual transient ischemic attack (TIA) rate of 3.2% (26, 27). In addition, the annual stroke rate of symptomatic carotid artery obstruction is 6%–20% (28, 29), and of course, spontaneous re-channeling of the blood vessels may occur in some patients, accounting for approximately 2.3%–10.3% of patients (26).
Intravascular hemodynamics depend largely on the anatomy of the vessel wall. The involvement of vessel wall mechanics and hemodynamics in atherosclerosis has been amply demonstrated (30). The vascular intimal layer, which is composed of endothelial cells, an internal elastic layer and fibrous collagen tissue, plays a key role in preventing platelet aggregation and antithrombosis (31, 32). Disruption of the endothelium is a key factor in the initial development of atherosclerotic disease within the vessel wall (33). After the endothelial layer is damaged, endothelial function is damaged, which promotes platelet adhesion and endothelial cell proliferation by releasing cytokines, which leads to hardened intima in the vascular lumen and causes the occurrence of atherosclerotic disease (34, 35). In addition, damage to the endothelium also causes structural changes to the media layer. Structural changes to the media layer occur through inflammatory stress and smooth muscle hyperplasia, thus causing fat stripes to form and ultimately leading to atherosclerosis (36–38). Over time, these changes and developments will gradually cause vascular lumen stenosis or even occlusion.
Different blood vessel diameters, endothelial thicknesses and blood vessel bifurcations easily cause blood turbulence. The uneven distribution of blood flow can easily cause local thrombosis, which is another cause of vascular occlusion (39). Therefore, additional carotid artery lesions are better developed at the carotid artery bifurcation (40). In summary, the pathogenesis of CICAO can be summarized in two aspects: the destruction of vascular endothelial cells causes local or other sources of thrombosis caused by atherosclerosis and blood turbulence.
The clinical symptoms of CICAO vary widely (41–44). If the collateral circulation is good, then the patient may have no clinical symptoms after ICAO (45). However, CICAO can also present as a transient ischemic attack, a focal stroke, or a massive cerebral infarction that results in patient death. Most patients with CICAO do not have any clinical symptoms (27). When intracranial hemodynamic changes induced by events, including postural transient ischemic attack, postprandial hypotension, heart failure, allergy, blood loss, dehydration, exercise and other factors, that lead to a decrease in cerebral perfusion pressure, then transient neurological deficiency symptoms will appear, and furthermore, a decrease in cerebral perfusion pressure may promote the occurrence of ischemic stroke symptoms. Very few patients with CICAO exhibit episodic involuntary movements of the ipsilateral limb and are often misdiagnosed as partial epilepsy. An electroencephalogram (EEG) is usually normal in such patients and a thermal conductivity detector (TCD) shows decreased cerebral blood flow. Patients with extremely rare CICAO present with decreased monocular vision under light variations ranging from dark to high light, possibly with increased retinal metabolic activity under light variations ranging from dark to high light, and no corresponding increase in cerebral blood flow, thus resulting in retinal ischemia. Paroxysmal involuntary movement of the ipsilateral limb or transient decline in monocular vision was highly suggestive of CICAO (23).
Patients with partial chronic occlusion of the internal carotid artery present with an unusual headache, due to compensation from the external carotid artery collateral circulation of the mandibular angle, eyebrow arch and buccal artery stroke, which is called ABC beating (41). With compensation from Willis' circle, no ABC pulsation was observed. The most common symptom of acute retinal ischemia is amaurosis fugax, and the most common cause of acute retinal ischemia is the loss of the embolus in the internal carotid artery. Chronic ocular ischemia syndrome with the clinical manifestations of a progressive decline in visual acuity is likely to develop in 4%–18% of patients with severe stenosis or occlusion of the internal carotid artery (42). Fundoscopy showed patchy retinal hemorrhage, arterial stenosis, and venous dilatation, and the late manifestations were flocculated exudation and angiogenesis. Some patients with CICAO present with transient syncope (43). Hypoperfusion associated with CICAO can even lead to vascular dementia (44). Some patients with chronic internal carotid artery occlusion (ICAO) develop neurological deficits in the future (46).
With the development of clinical management, there are various surgical approaches to treat symptomatic patients with CICAO, such as EC-IC bypass, endovascular interventional therapy, carotid endarterectomy, and hybrid surgery (47, 48).
In the 1960s, the benefits of EC-IC bypass began to be recognized (49). At the same time, it is widely believed that EC-IC bypass can successfully treat ICAO to prevent cerebrovascular ischemia. Therefore, efforts to develop and improve some bypass techniques can lead to a sharp increase in the number of surgeries performed using the new and improved techniques. However, several research studies published in 1985 showed that there was no significant difference between EC-IC bypass surgery combined with drug therapy and optimal drug therapy alone in terms of reducing the risk of long-term stroke (21). However, this procedure continues to be reported and is beneficial in patients with a specific carotid or middle cerebral artery occlusion (50).
At present, the surgical methods are divided into high flow and low flow, and the main difference lies in the choice of the blood vessels that will receive surgical intervention (51). Low-flow surgery was performed on the superficial temporal artery-middle cerebral artery (STA-MCA), superficial temporal artery-superior cerebellar artery (STA-SCA), and ophthalmic artery-posterior inferior cerebellar artery (OA-PICA). However, STA-MCA, as the basic bypass for low-flow revascularization in neurosurgery, can only provide up to 1/4—1/3 of the normal MCA blood flow (52). STA-MCA provides an average blood flow of 30 ml/min shortly after the start of surgery, which can then gradually increase but can rarely reach the blood supply of the MCA (53, 54). Sometimes, to increase the blood supply, double bypass surgery is performed in the anterior temporal artery and the MCA (54). High-flow surgical methods include large saphenous vein transplantation and ulnar artery transplantation. Although high-flow surgical techniques can provide more blood flow, these methods are mostly used to treat a brain tumor or brain aneurysm, and few cases of carotid artery occlusion treated with these techniques have been reported.
EC-IC bypass is a new procedure to prevent and treat cerebral ischemia. At that time, blood vessels were reconstructed to treat cerebral ischemic diseases caused by vascular stenosis or occlusion. When the results of the EC-IC research group were published in 1985, the number of EC-IC bypass operations performed worldwide plummeted to only a few a year. However, some cerebrovascular surgeons have questioned the rationality, rigor, and statistical method of the study (55, 56) and have been using this surgery to prevent the occurrence of stroke. The controversies are as follows: (1) The inclusion criteria for the patients are controversial. The selected patients did not strictly regulate the compensation of the circulation after the evaluation of vertebral artery angiography, the intracranial collateral circulation before the selection, the cerebrovascular reserve capacity (CVR), or the decline in cerebral blood flow and metabolic disorders in the corresponding area. It is impossible to distinguish whether it is caused by embolus distal blood vessel embolization or cerebral blood supply disorder caused by hemodynamic reasons. Embolization was painful for patients undergoing cooperative EC-IC bypass (55, 56). (2) The number of patients selected is also controversial. The research team includes professionals from more than 100 medical centers in North America, Europe and Asia Pacific, and patients are prospectively randomized to internal medicine (714 for aspirin) and surgical treatment (663). However, the survey found that a large number of qualified patients in the surgical group were not included, which is likely to affect the accuracy of the study (55, 56).
Studies on EC-IC bypass are still ongoing in the 21st century. In 2006, the Japanese EC-IC Trial (JET) Study Group designed a pilot trial to evaluate the role of EC-IC bypass in preventing ischemic stroke recurrence in patients with major cerebral artery occlusive disease and hemodynamic cerebral ischemia (57). The trial randomly evaluated 196 patients (98 receiving maximal drug treatment; 98 undergoing EC-IC bypass + maximal drug treatment) who were followed up for 2 years. Preliminary data showed that the incidence of stroke recurrence in the surgical treatment group was significantly lower than that in the medical group (5% vs. 14%, p-value = 0.046). In 2011, the Carotid Occlusion Surgery Study (COSS) conducted a prospective, randomized trial that divided patients into groups A and B. Group A underwent STA-MCA bypass surgery combined with drug therapy, and Group B received the best drug therapy. However, the trial was terminated early because previous data showed no significant difference in the recurrence rate between groups A and B (58). Later, the Cerebrovascular Section of the American Association of Neurological Surgeons (AANS) and the Congress of Neurological Surgeons (CNS) reported that the COSS was flawed. Thus, the findings of the COSS are also controversial. They believe that EC-IC bypass surgery is still feasible for specific patients in technologically advanced medical centers (59). A similar assessment was published by the European Association of Neurological Surgeons (60).
Fiedler et al. showed a significant improvement in some neurocognitive function in 30 patients at 12 months before and after EC-IC bypass surgery (61). With the results of the randomized evaluation of Carotid Occlusion and Neurocognition (RECON) trial published, the effect of recovery of cognitive function has again been controversial. They showed no difference in the 2-year follow-up of neurocognitive function between the 13 EC-IC bypass surgery groups and the 16 drug treatment groups (62). However, the small sample size of the trial limits the reliability of the conclusions. At present, EC-IC bypass surgery is still considered the first treatment option for CICAO (19). However, large-scale cohort studies revealed the limited benefit of the EC-IC bypass procedure for patients with CICAO (21, 22). Therefore, there is an urgent need to investigate novel therapeutics with better outcomes for CICAO.
Endovascular treatment is also considered to be effective for patients with CICAO. Endovascular treatment includes carotid stenting (CAS) alone or the combination of carotid endarterectomy (CEA) and CAS (63–66). According to previous studies, the assessment of revascularization is mainly done by imaging, for example, high-resolution magnetic resonance vessel wall imaging (MR-VWI) and hemodynamic evaluation (67). Occlusion with the residual lumen and shorter occlusion length on high-resolution MR-VWI were identified as predictors of technical success of endovascular recanalization for nonacute ICAO (68). In addition, the evaluation of cerebral hemodynamics following recanalization therapy can also help identify patients at high risk for complications associated with reperfusion. CAS refers to the use of a micro guide wire to place a stent at the stenosis or occlusion site, which then expands through the stent to support the vessel and recanalize the blood flow. In hybrid surgery, CEA is performed at the initial site of the ICA and then at the distal end of the ICA, which is where the micro guide wire and micro guide catheter are placed. Hybrid surgery is relatively safe because by cutting the blood vessel, the thrombus debris of the neck blood vessels can be effectively removed, thus helping to prevent distal embolization accidents. Through these techniques, revascularization can be achieved through various degrees of vascular remodeling. According to some previous literature reviews, successful recanalization was defined as final residual diameter stenosis ≤20%. And the rate of successful recanalization varied from 60% to 100% according to previous literature (69).
We can adopt different endovascular treatment modalities depending on the location of the occluded vessels (70). If the occluded vessel is located in the skull, then the blood flow can be restored with an endovascular stent, which is the goal of treatment. If the occluded vessel is located in the neck, then the intima can be removed to restore the blood flow. Of course, some patients have occlusion vessels with long lengths that involve the neck and intracranial areas, and the guidewire may not successfully cross the occlusion site. At this time, we can choose hybrid surgery to achieve the purpose of treatment. In addition, the disadvantage of endovascular intervention is that the thrombus may be shed during balloon dilation or stent release, going distal to the blood flow, thereby blocking the intracranial artery (71, 72). Thus, experienced clinicians will protect the common and external carotid arteries in some cases (73, 74). Some doctors currently use the Parodi embolic protection system (75–77), but this method still has limitations. For example, if the thrombus aggressively occupies the blocked vessels, then the proximal occlusion may not necessarily provide additional protection (78).
In 2005, Terada introduced a new treatment method for CICAO patients, which uses the vascular recanalization technique (73). As interventional materials and technology advance, it has become more feasible and safer to open the occluded internal carotid artery. Patients with cervical ICA stenosis who undergo carotid endarterectomy (CEA) are protected against ischemic stroke, but not those with occlusions. However, when a patient is at high surgical risk and does not want to undergo CEA, endovascular carotid artery stenting (CAS) can be an alternative (79). Piotr's study also proposed that endovascular treatment for CICAO is safe and feasible, with a technical success rate of 67% and a low incidence of early and late neurological complications (80, 81). In recent years, an increasing number of research findings have been reported regarding the endovascular treatment of CICAO. In 2014, Fan et al. (82) conducted a prospective controlled study in which 40 patients were divided into two groups: A and B. Group A will receive endovascular treatment, and Group B will receive conservative treatment. The results showed that 16 of the 18 patients in group A had successful flow recanalization and no cerebrovascular events. Improvement in cerebral perfusion was observed in 12 patients according to single-photon emission computed tomography scans. At the 1-month, 3-month, and 6-month follow-ups, the Montreal Cognitive Assessment in Group A significantly outperformed Group B. Moreover, Xia et al. (83) also designed a controlled study of endovascular treatment and optimal drug treatment in the two groups, indicating that endovascular surgery had a good outcome in terms of neurological function. However, after two years of follow-up, there was no significant difference in the incidence of cerebrovascular accidents or mortality between the two groups. In the study by Lin et al., cases of stroke recurrence and death persisted after endovascular therapy (84). Therefore, whether endovascular therapy can be used as an effective treatment method still needs to be further proved by comparison.
Additionally, hybrid surgery has been reported successively in recent years, thus improving the success rate of endovascular surgical treatment (18, 85, 86). Shih et al. reported in 2013 that the surgery was performed in three patients with a recurrent ischemic attack and the patients achieved complete recanalization of blood flow (87). Improved cerebral perfusion was shown on computed tomography angiography and perfusion imaging. After 6 months of follow-up, the ischemic symptoms did not recur. This is an earlier reported success, but with a small sample size. In 2018, Zhang et al. (88) divided 65 patients with long ICA occlusion into revascularization hybrid surgery (n = 30) and medication (n = 35) groups to analyze clinical and angiographic data. The vascular recanalization rate of the patients who underwent hybrid surgery was 100%, with 2 complications in the perioperative period. One patient had a recurrent laryngeal nerve injury, and the other patient had an intracranial hemorrhage, but none of the patients developed severe neurological deficits, therefore suggesting that hybrid surgery may be safe and effective in achieving revascularization of long segment occlusion of the internal carotid artery to prevent further ischemic events.
Patients with transient ischemic attacks (TIA) and ischemic strokes are at high risk for stroke recurrence, especially companied with symptomatic internal carotid artery stenosis (89). The latest data using modern DAPT poses an important baseline by which to compare results with both endovascular and surgical strategies. It has been illustrated that timely initiation of effective antithrombotic therapy and revascularization interventions are urgently required to prevent the recurrent events (90). Perioperative aspirin presents a better outcomes in patients with ICA occlusion. Additionally, application of single antiplatelet therapy (SAPT) in patients with symptomatic carotid stenosis (Class I, Level A) was recommend by the American Heart Association/American Stroke Association (AHA/ASA) guidelines (91). Although the dual antiplatelet therapy (DAPT) with aspirin and clopidogrel is a more effective strategy than monotherapy to alleviate emboli and neurological events, AHA/ASA guidelines do not discuss preoperative DAPT for ICA occlusion (92–94). The evaluation of the efficacy of preoperative antithrombotic therapies in reducing early recurrent ischemic events and whether promote the clinical outcomes of patients under endovascular intervention or bypass surgery will be an another worthwhile topic in the further studies.
In this review, we searched the PubMed database for “chronic internal carotid artery occlusion, endovascular intervention, and external Carotid-internal Carotid Bypass”. Nineteen studies were included, including seven studies on EC-IC bypass surgeries and twelve on endovascular treatments (consisting of six studies on CAS and six on hybrid surgeries). Although two earlier studies were released in 1985 and 1995, these studies were released after 2006. A total of eight studies were controlled studies, nine were single-arm studies and two were retrospective analysis studies. Among the eight controlled studies, endovascular treatment was performed in three studies (82, 83, 88) and EC-IC bypass was performed in five studies (21, 57, 58, 62, 95). Among the nine single-arm studies, endovascular treatment was performed in seven studies (14, 83, 86, 95–97) and EC-IC bypass was performed in two studies (61, 100). Endovascular treatment was performed in two retrospective analysis studies (101, 102) (See Table 1).

Table 1. Basic characteristics of included studies.
In two studies, EC-IC procedures reported a 96% recanalization rate. Possibly due to surgery to bypass diseased vessels and reconnect healthy ones without opening the occluded vessels (21, 62). Even if the vessel is completely occluded or if the calcification is very severe, postvascular flow is not affected. Five studies (82, 83, 96, 101, 102) on CAS reported the vascular recanalization rate. Compared with EC-IC, the recanalization rate of CAS is relatively low, possibly because the thrombus is hard and the micro guide wire cannot smoothly penetrate the thrombus. The recanalization rate of CAS may also be low because vascular calcification is severe, and the vascular stent cannot be successfully inserted. There was an increase in vascular recanalization rates with hybrid treatment. Six studies (14, 87, 88, 97–99) showed that vascular recanalization rates were increased when compared to that of CAS. Since carotid endarterectomy was performed prior to stent placement, most of the thrombus and atherosclerotic plaque were removed during carotid endarterectomy, thus allowing the guidewire to easily pass (See Table 2).
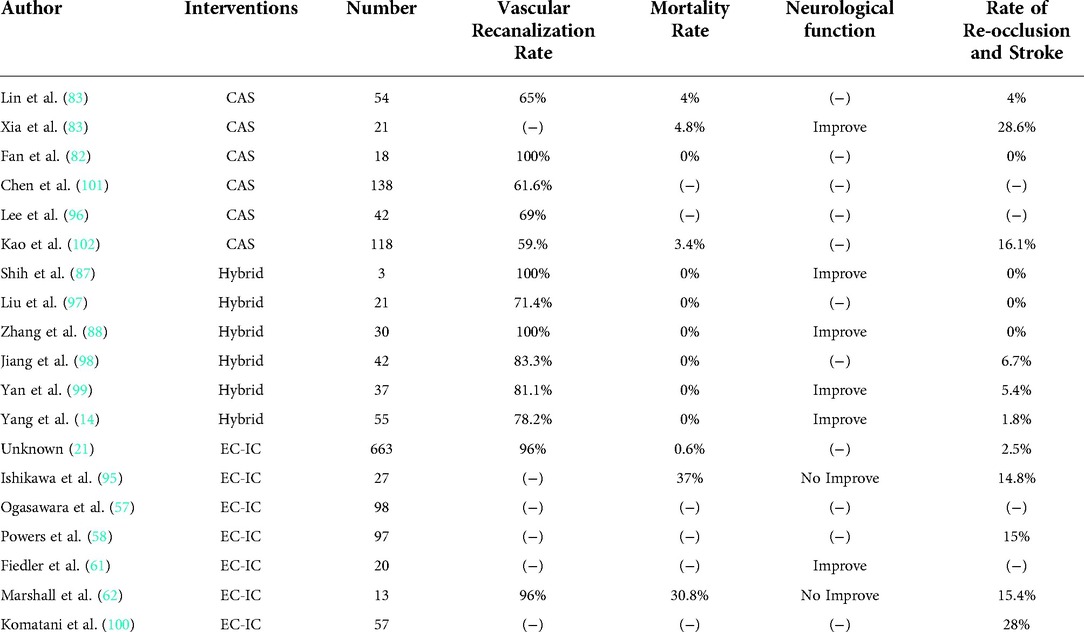
Table 2. Therapeutic effects and post-surgical complications of included studies.
In addition, Chen et al. analyzed the independent factors associated with surgical recanalization rates by reviewing 138 CICAO patients who underwent the endovascular recanalization technique. It was concluded that the absence of previous neurological events, unpunctured stump, reconstruction of the distal ICA by contralateral injection, and distal ICA reconstruction with communication or ophthalmic segments were identified as independent negative predictors of the success of the CAO endovascular recanalization technique (101).
Currently, the Modified Rankin Scale (mRS) and National Institute of Health Stroke Scale (NIHSS) are commonly used to assess neurological function. The mRS evaluates brain nerve function through the patient's clinical symptoms. It is divided into seven grades, ranging from asymptomatic to death (0–6 points) (103). The NIHSS evaluates neurological function in patients with stroke using fifteen items (104). Of the twelve included studies on endovascular treatment, a total of five studies mentioned neurological function after surgery. Xia et al. (83), Zhang et al. (88) and Yang et al. (14) evaluated the neurological function of patients by mRS, and the results showed improved function, and the effect was obvious when compared with that of the drug treatment group. ShiH et al. (87) and YAN et al. (99) reported that, according to NIHSS, endovascular therapy is helpful in the neurological recovery of CICAO patients. Only three studies on EC-IC bypass have reported neurological function. Ishikawa et al. designed a controlled trial comparing EC-IC bypass to medication (95). After two years of follow-up, there was no difference in neurological recovery between the two groups. Marshall et al. also shared the same point (62). Only the Fiedler et al. report showed a significant improvement in all areas of cognition twelve months after surgery (61) (See Table 2).
Only three studies have reported EC-IC bypass-related mortality rates of 0.6%, 37.0%, and 30.8%. Ten of the twelve studies on endovascular treatment reported mortality. The mortality rate of hybrid surgery is 0%, which is significantly better than that of other treatments. The reason may be the use of inconsistent methods to statistically measure mortality in the studies, some assessed perioperative mortality, or mortality at 2 or even 5 years after follow-up. However, overall, patients receiving endovascular treatment had significantly lower mortality (See Table 2).
EC-IC surgery is generally performed on the shallow temporal artery to supply cerebral blood flow, and its blood flow and perfusion are lower than those of the internal carotid artery, so the probability of stroke is relatively large. Five of these studies showed that the proportions of vascular reocclusion and stroke were 2.5%, 14.8%, 15%, 15.4%, and 28%, respectively (21, 58, 62, 95, 100). Although CAS can occlude open blood vessels, it does not remove endovascular plaque, and plaque inside or around the stent can easily cause thrombosis, so the proportion of vascular reocclusion and stroke will be relatively high. Four studies showed that the proportions of vascular reocclusion and stroke after CAS were 4%, 28.6%, and 0%, 16.1%, respectively (81–83, 100). Due to the removal of endovascular plaque in hybrid surgery, the proportions of vascular reocclusion and stroke are significantly reduced. Three (87, 88, 97) of six studies showed a proportion of 0%, while the proportions in the remaining three (14, 98, 99) were 6.7%, 5.4%, and 1.8% (See Table 2).
Other complications included cerebral hemorrhage, reperfusion injury, carotid artery cavernous sinus fistula, recurrent laryngeal nerve injury, pseudoaneurysm, etc. In a study on CAS, Lin et al. reported one carotid-cavernous sinus fistula (84), and Kao et al. reported four cases of cerebral hemorrhage (102). In a hybrid surgery study, Zhang et al. reported one cerebral hemorrhage and one recurrent laryngeal nerve injury (88); Yang et al. reported one reperfusion injury and one recurrent laryngeal nerve injury (14). In the study of EC-IC, Powers (58) reported 12 other complications: 4 TIAs, 2 intracranial hematomas, 2 seizures, 1 myocardial infarction, 1 case of respiratory disease, 1 case of hypotension and 1 wound infection. The occurrence of complications is closely related to the method of surgery. During endovascular treatment, the micro guidewire may cause vascular intimal injury, including a carotid cavernous sinus fistula, carotid-vascular perforation, and arterial dissection (6, 73). EC-IC bypass causes perfusion damage due to a mismatch in blood flow.
Overall, EC-IC bypass is characterized by high recanalization and fewer complications. However, the mortality rate was relatively high, and the incidence of stroke was not reduced when compared with that in the medication group. In addition, the neurological function of the patients did not improve significantly after surgical treatment, and the clinical treatment effect was not obvious. Compared with EI-IC bypass, CAS has a good effect on nerve function, but the vascular recanalization rate is not high. The main reason is that long vascular lesions or the vascular intima have calcification and organization, and the guidewire has difficulty crossing the occluded segment. Furthermore, nonresidual obstruction prevents the guidewire from entering the true lumen and increases the risk of vascular damage. For hybrid surgery, the vascular recanalization rate and neurological improvement were satisfactory. The combination of carotid stenting and endarterectomy in hybrid surgery removes plaque and the thrombus well. Moreover, placing the stent under direct vision reduces vascular damage to a greater extent. Another advantage is that distal embolization is also prevented in hybrid surgery because retrograde flow can flush out the debris at the arteriotomy site. Therefore, hybrid surgery is a relatively satisfactory treatment option for CICAO.
At present, in the study of CICAO treatment, there are several studies on the comparison between surgical treatment and drug treatment, but studies on the comparison between different surgical methods are still relatively few. The number of studies selected in this paper was limited, the purpose and method of each study were different, and there was heterogeneity. In addition, the collection of study data, surgical technique proficiency, and operator experience also have an impact on the consistency of the study results. Currently, there are no clear criteria for the selection of CICAO surgical procedures. This paper provides ideas and reference for the choice of treatment through the statistical, comparative and analysis of the results of several studies. EC-IC bypass seems to be a better option if the occlusion range is large and the accumulated vessels are long. If the occlusion site is located in the skull and the occlusion range is small, CAS is a good choice. Hybrid surgery provides better treatment if the occlusion is located at the beginning of the internal carotid artery. However, the number of studies selected in this paper is limited and not representative, and more studies are still needed to determine the utility of this surgical method. Therefore, we hope that more studies can compare the outcomes of different surgical methods in patients with CICAO to provide a better treatment reference for future clinical work.
JNW and CYF designed the review and wrote the manuscript. LYW, YBL, XYW and LY conceived the artwork and performed the bibliographical research. XYW, YZX and ANZ supervised the writing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2022.971066/full#supplementary-material.
1. Malhotra K, Goyal N, Tsivgoulis G. Internal carotid artery occlusion: pathophysiology, diagnosis, and management. Curr Atheroscler Rep. (2017) 19(10):41. doi: 10.1007/s11883-017-0677-7
2. Saini H, Cerejo R, Williamson R, Malhotra K. Internal carotid artery occlusion: management. Curr Neurol Neurosci Rep. (2022) (7):383–8. doi: 10.1007/s11910-022-01201-x
3. Liu S, Han S, Dai Q, Li S, Li J. BICAO-induced ischaemia caused depressive-like behaviours and caspase-8/-9-dependent brain regional neural cell apoptosis in mice. Stroke Vasc Neurol. (2018) 3(1):1–8. doi: 10.1136/svn-2017-000109
4. Mo D, Luo G, Wang B, Ma N, Gao F, Sun X, et al. Staged carotid artery angioplasty and stenting for patients with high-grade carotid stenosis with high risk of developing hyperperfusion injury: a retrospective analysis of 44 cases. Stroke Vasc Neurol. (2016) 1(4):147–53. doi: 10.1136/svn-2016-000024
5. Iwata T, Mori T, Tajiri H, Miyazaki Y, Nakazaki M. Long-term angiographic and clinical outcome following stenting by flow reversal technique for chronic occlusions older than 3 months of the cervical carotid or vertebral artery. Neurosurgery. (2012) 70(1):82–90; discussion 90. doi: 10.1227/NEU.0b013e31822e074c
6. Xu B, Li C, Guo Y, Xu K, Yang Y, Yu J. Current understanding of chronic total occlusion of the internal carotid artery. Biomed Rep. (2018) 8(2):117–25. doi: 10.3892/br.2017.1033
7. Paciaroni M, Caso V, Venti M, Milia P, Kappelle LJ, Silvestrelli G, et al. Outcome in patients with stroke associated with internal carotid artery occlusion. Cerebrovasc Dis. (2005) 20(2):108–13. doi: 10.1159/000086800
8. Harrison MJ, Marshall J. The finding of thrombus at carotid endarterectomy and its relationship to the timing of surgery. Br J Surg. (1977) 64(7):511–2. doi: 10.1002/bjs.1800640717
9. Chen YH, Kao HL. Concern on article “predicting procedure successful rate and 1-year patency after endovascular recanalization for chronic carotid artery occlusion by CT angiography”. Int J Cardiol. (2017) 229:59. doi: 10.1016/j.ijcard.2016.11.274
10. Nico L, Cester G, Viaro F, Baracchini C, Causin F. Endovascular recanalization of the common carotid artery in a patient with radio induced chronic occlusion. J Neurointerv Surg. (2017) 9(6):e23. doi: 10.1136/neurintsurg-2016-012722.rep
11. Lee JI, Jander S, Oberhuber A, Schelzig H, Hänggi D, Turowski B, et al. Stroke in patients with occlusion of the internal carotid artery: options for treatment. Expert Rev Neurother. (2014) 14(10):1153–67. doi: 10.1586/14737175.2014.955477
12. Virmani R, Ladich ER, Burke AP, Kolodgie FD. Histopathology of carotid atherosclerotic disease. Neurosurgery. (2006) 59(5 Suppl 3):S219–27; discussion S3–S13. doi: 10.1227/01
13. Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. Br Med J. (2002) 324(7329):71–86. doi: 10.1136/bmj.324.7329.71
14. Yang Y, Liu X, Wang R, Zhang Y, Zhang D, Zhao J. A treatment option for symptomatic chronic complete internal carotid artery occlusion: hybrid surgery. Front Neurosci. (2020) 14:392. doi: 10.3389/fnins.2020.00392
15. Rudolf J, Neveling M, Grond M, Schmulling S, Stenzel C, Heiss WD. Stroke following internal carotid artery occlusion—a contra-indication for intravenous thrombolysis? Eur J Neurol. (1999) 6(1):51–5. doi: 10.1046/j.1468-1331.1999.610051.x
16. Grubb RL Jr, Powers WJ, Clarke WR, Videen TO, Adams HP Jr. Surgical results of the carotid occlusion surgery study. J Neurosurg. (2013) 118(1):25–33. doi: 10.3171/2012.9.JNS12551
17. Flaherty ML, Flemming KD, McClelland R, Jorgensen NW, Brown RD Jr. Population-based study of symptomatic internal carotid artery occlusion: incidence and long-term follow-up. Stroke. (2004) 35(8):e349–52. doi: 10.1161/01.STR.0000135024.54608.3f
18. He Y, Wang B. Hybrid surgery for symptomatic chronic complete occlusion of the internal carotid artery: a case report. J Interv Med. (2019) 2(4):171–7. doi: 10.1016/j.jimed.2019.10.007
19. Low SW, Teo K, Lwin S, Yeo LL, Paliwal PR, Ahmad A, et al. Improvement in cerebral hemodynamic parameters and outcomes after superficial temporal artery-middle cerebral artery bypass in patients with severe stenoocclusive disease of the intracranial internal carotid or middle cerebral arteries. J Neurosurg. (2015) 123(3):662–9. doi: 10.3171/2014.11.JNS141553
20. Yogendrakumar V, Shamy M, Dewar B, Fergusson DA, Dowlatshahi D, Hamel C, et al. Identifying sex-specific differences in the carotid revascularisation literature: findings from a scoping review. Stroke Vasc Neurol. (2021) 6(3):496–9. doi: 10.1136/svn-2020-000744
21. EC/IC Bypass Study Group. Failure of extracranial-intracranial arterial bypass to reduce the risk of ischemic stroke. Results of an international randomized trial. N Engl J Med. (1985) 313(19):1191–200. doi: 10.1056/NEJM198511073131904
22. Esposito G, Amin-Hanjani S, Regli L. Role of and indications for bypass surgery after carotid occlusion surgery study (COSS)? Stroke. (2016) 47(1):282–90. doi: 10.1161/STROKEAHA.115.008220
23. Thanvi B, Robinson T. Complete occlusion of extracranial internal carotid artery: clinical features, pathophysiology, diagnosis and management. Postgrad Med J. (2007) 83(976):95–9. doi: 10.1136/pgmj.2006.048041
24. Lichtman JH, Jones MR, Leifheit EC, Sheffet AJ, Howard G, Lal BK, et al. Carotid endarterectomy and carotid artery stenting in the US medicare population, 1999–2014. JAMA. (2017) 318(11):1035–46. doi: 10.1001/jama.2017.12882
25. Otite FO, Khandelwal P, Malik AM, Chaturvedi S. National patterns of carotid revascularization before and after the carotid revascularization endarterectomy vs stenting trial (CREST). JAMA Neurol. (2018) 75(1):51–7. doi: 10.1001/jamaneurol.2017.3496
26. Lall A, Yavagal DR, Bornak A. Chronic total occlusion and spontaneous recanalization of the internal carotid artery: natural history and management strategy. Vascular. (2021) 29(5):733–41. doi: 10.1177/1708538120978043
27. Hennerici M, Hülsbömer HB, Rautenberg W, Hefter H. Spontaneous history of asymptomatic internal carotid occlusion. Stroke. (1986) 17(4):718–22. doi: 10.1161/01.STR.17.4.718
28. Paty PS, Adeniyi JA, Mehta M, Darling RC 3rd, Chang BB, Kreienberg PB, et al. Surgical treatment of internal carotid artery occlusion. J Vasc Surg. (2003) 37(4):785–8. doi: 10.1067/mva.2003.203
29. Grubb RL Jr, Powers WJ. Risks of stroke and current indications for cerebral revascularization in patients with carotid occlusion. Neurosurg Clin N Am. (2001) 12(3):473–87, vii. doi: 10.1016/S1042-3680(18)30037-8
30. Giddens DP, Zarins CK, Glagov S. The role of fluid mechanics in the localization and detection of atherosclerosis. J Biomech Eng. (1993) 115(4b):588–94. doi: 10.1115/1.2895545
31. Xu H, Li S, Liu YS. Roles and mechanisms of DNA methylation in vascular aging and related diseases. Front Cell Dev Biol. (2021) 9:699374. doi: 10.3389/fcell.2021.699374
32. Vane JR, Anggård EE, Botting RM. Regulatory functions of the vascular endothelium. N Engl J Med. (1990) 323(1):27–36. doi: 10.1056/NEJM199007053230106
33. Gimbrone MA Jr, García-Cardeña G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ Res. (2016) 118(4):620–36. doi: 10.1161/CIRCRESAHA.115.306301
34. Sorensen KE, Celermajer DS, Georgakopoulos D, Hatcher G, Betteridge DJ, Deanfield JE. Impairment of endothelium-dependent dilation is an early event in children with familial hypercholesterolemia and is related to the lipoprotein(a) level. J Clin Invest. (1994) 93(1):50–5. doi: 10.1172/JCI116983
35. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation. (2002) 105(9):1135–43. doi: 10.1161/hc0902.104353
36. Faggiotto A, Ross R, Harker L. Studies of hypercholesterolemia in the nonhuman primate. I. Changes that lead to fatty streak formation. Arteriosclerosis. (1984) 4(4):323–40. doi: 10.1161/01.ATV.4.4.323
37. Gerrity RG, Naito HK, Richardson M, Schwartz CJ. Dietary induced atherogenesis in swine. Morphology of the intima in prelesion stages. Am J Pathol. (1979) 95(3):775–92.453335
38. Ross R. Atherosclerosis is an inflammatory disease. Am Heart J. (1999) 138(5 Pt 2):S419–20. doi: 10.1016/S0002-8703(99)70266-8
39. Kim D, Bresette C, Liu Z, Ku DN. Occlusive thrombosis in arteries. APL Bioeng. (2019) 3(4):041502. doi: 10.1063/1.5115554
40. Cohen A, Ederhy S, Di Angelantonio E. Mechanisms of thrombogenesis in atrial fibrillation. Lancet. (2009) 373(9668):1005–6; author reply 1006–7. doi: 10.1016/S0140-6736(09)60603-6
41. Fisher CM. Facial pulses in internal carotid artery occlusion. Neurology. (1970) 20(5):476–8. doi: 10.1212/WNL.20.5.476
42. Klijn CJ, Kappelle LJ, van Schooneveld MJ, Hoppenreijs VP, Algra A, Tulleken CA, et al. Venous stasis retinopathy in symptomatic carotid artery occlusion: prevalence, cause, and outcome. Stroke. (2002) 33(3):695–701. doi: 10.1161/hs0302.104619
43. Kashiwazaki D, Kuroda S, Terasaka S, Ishikawa T, Shichinohe H, Aoyama T, et al. [Carotid occlusive disease presenting with loss of consciousness]. No Shinkei Geka. (2005) 33(1):29–34.
44. Tatemichi TK, Desmond DW, Prohovnik I, Eidelberg D. Dementia associated with bilateral carotid occlusions: neuropsychological and haemodynamic course after extracranial to intracranial bypass surgery. J Neurol Neurosurg Psychiatry. (1995) 58(5):633–6. doi: 10.1136/jnnp.58.5.633
45. Macchi C, Molino Lova R, Miniati B, Zito A, Catini C, Gulisano M, et al. Collateral circulation in internal carotid artery occlusion. A study by duplex scan and magnetic resonance angiography. Minerva Cardioangiol. (2002) 50(6):695–700.12473991
46. Lin MS, Chiu MJ, Wu YW, Huang CC, Chao CC, Chen YH, et al. Neurocognitive improvement after carotid artery stenting in patients with chronic internal carotid artery occlusion and cerebral ischemia. Stroke. (2011) 42(10):2850–4. doi: 10.1161/STROKEAHA.111.613133
47. Hafner CD, Tew JM. Surgical management of the totally occluded internal carotid artery: a ten-year study. Surgery. (1981) 89(6):710–7.7245033
48. Kuroda S, Kawabori M, Hirata K, Shiga T, Kashiwazaki D, Houkin K, et al. Clinical significance of STA-MCA double anastomosis for hemodynamic compromise in post-JET/COSS era. Acta Neurochir (Wien). (2014) 156(1):77–83. doi: 10.1007/s00701-013-1961-0
49. Yasargil MG, Yonekawa Y. Results of microsurgical extra-intracranial arterial bypass in the treatment of cerebral ischemia. Neurosurgery. (1977) 1(1):22–4. doi: 10.1227/00006123-197707000-00005
50. Mendelowitsch A, Taussky P, Rem JA, Gratzl O. Clinical outcome of standard extracranial-intracranial bypass surgery in patients with symptomatic atherosclerotic occlusion of the internal carotid artery. Acta Neurochir (Wien). (2004) 146(2):95–101. doi: 10.1007/s00701-003-0154-7
51. Belykh E, Lei T, Safavi-Abbasi S, Yagmurlu K, Almefty RO, Sun H, et al. Low-flow and high-flow neurosurgical bypass and anastomosis training models using human and bovine placental vessels: a histological analysis and validation study. J Neurosurg. (2016) 125(4):915–28. doi: 10.3171/2015.8.JNS151346
52. Sekhar LN, Bucur SD, Bank WO, Wright DC. Venous and arterial bypass grafts for difficult tumors, aneurysms, and occlusive vascular lesions: evolution of surgical treatment and improved graft results. Neurosurgery. (1999) 44(6):1207–23; discussion 1223–4. doi: 10.1097/00006123-199906000-00028
53. Iwama T, Hashimoto N, Hayashida K. Cerebral hemodynamic parameters for patients with neurological improvements after extracranial-intracranial arterial bypass surgery: evaluation using positron emission tomography. Neurosurgery. (2001) 48(3):504–10; discussion 510–2. doi: 10.1097/00006123-200103000-00008
54. Orbay T, Seçkin Z, Ergün R, Alp H. Double-donor, single-lumen, end-to-side anastomosis. Surg Neurol. (1990) 33(4):253–5. doi: 10.1016/0090-3019(90)90044-P
55. Guthikonda M, Guyot LL, Diaz FG. Future of extracranial-intracranial bypass. Neurol Res. (2002) 24(Suppl 1):S80–3. doi: 10.1179/016164102101199954
56. Caplan LR, Piepgras DG, Quest DO, Toole JF, Samson D, Futrell N, et al. EC-IC bypass 10 years later: is it valuable? Surg Neurol. (1996) 46(5):416–23. doi: 10.1016/S0090-3019(96)90802-2
57. Ogasawara K, Ogawa A. [JET study (Japanese EC-IC bypass trial)]. Nihon Rinsho. (2006) 64(Suppl 7):524–7.17461199
58. Powers WJ, Clarke WR, Grubb RL Jr, Videen TO, Adams HP Jr, Derdeyn CP. Extracranial-intracranial bypass surgery for stroke prevention in hemodynamic cerebral ischemia: the Carotid Occlusion Surgery Study randomized trial. JAMA. (2011) 306(18):1983–92. doi: 10.1001/jama.2011.1610
59. Amin-Hanjani S, Barker FG 2nd, Charbel FT, Connolly ES Jr, Morcos JJ, Thompson BG. Extracranial-intracranial bypass for stroke-is this the end of the line or a bump in the road? Neurosurgery. (2012) 71(3):557–61. doi: 10.1227/NEU.0b013e3182621488
60. Hänggi D, Steiger HJ, Vajkoczy P. The role of MCA-STA bypass surgery after COSS and JET: the European point of view. Acta Neurochir Suppl. (2014) 119:77–8. doi: 10.1007/978-3-319-02411-0_13
61. Fiedler J, Přibáň V, Skoda O, Schenk I, Schenková V, Poláková S. Cognitive outcome after EC-IC bypass surgery in hemodynamic cerebral ischemia. Acta Neurochir (Wien. (2011) 153(6):1303–11; discussion 1311–2. doi: 10.1007/s00701-011-0949-x
62. Marshall RS, Festa JR, Cheung YK, Pavol MA, Derdeyn CP, Clarke WR, et al. Randomized evaluation of carotid occlusion and neurocognition (RECON) trial: main results. Neurology. (2014) 82(9):744–51. doi: 10.1212/WNL.0000000000000167
63. Eller JL, Snyder KV, Siddiqui AH, Levy EI, Hopkins LN. Endovascular treatment of carotid stenosis. Neurosurg Clin N Am. (2014) 25(3):565–82. doi: 10.1016/j.nec.2014.04.012
64. Gensicke H, Engelter S, Bonati L. [Endovascular treatment for carotid artery stenosis]. Ther Umsch. (2012) 69(9):523–35. doi: 10.1024/0040-5930/a000325
65. Naylor AR. Endarterectomy versus stenting for stroke prevention. Stroke Vasc Neurol. (2018) 3(2):101–6. doi: 10.1136/svn-2018-000146
66. Yu W, Jiang WJ. Stenting for intracranial stenosis: potential future for the prevention of disabling or fatal stroke. Stroke Vasc Neurol. (2018) 3(3):140–6. doi: 10.1136/svn-2018-000158
67. Zhu XJ, Wang W, Liu ZJ. High-resolution magnetic resonance vessel wall imaging for intracranial arterial stenosis. Chin Med J (Engl). (2016) 129(11):1363–70. doi: 10.4103/0366-6999.182826
68. Hou Z, Yan L, Zhang Z, Jing J, Lyu J, Hui FK, et al. High-resolution magnetic resonance vessel wall imaging-guided endovascular recanalization for nonacute intracranial artery occlusion. J Neurosurg. (2021):1–7. doi: 10.3171/2021.9.JNS211770
69. Zanaty M, Roa JA, Jabbour PM, Samaniego EA, Hasan DM. Recanalization of the chronically occluded internal carotid artery: review of the literature. World Neurosurg X. (2020) 5:100067. doi: 10.1016/j.wnsx.2019.100067
70. Müller MD, Lyrer P, Brown MM, Bonati LH. Carotid artery stenting versus endarterectomy for treatment of carotid artery stenosis. Cochrane Database Syst Rev. (2020) 2(2):Cd000515. doi: 10.1002/14651858.CD000515.pub5
71. Dalyai RT, Chalouhi N, Singhal S, Jabbour P, Gonzalez LF, Dumont AS, et al. Stent-assisted endovascular recanalization of extracranial internal carotid artery occlusion in acute ischemic stroke. World Neurosurg. (2013) 79(1):143–8. doi: 10.1016/j.wneu.2012.08.017
72. Burke JF, Morgenstern LB, Osborne NH, Hayward RA. Combined risk modelling approach to identify the optimal carotid revascularisation approach. Stroke Vasc Neurol. (2021) 6(3):476–82. doi: 10.1136/svn-2020-000558
73. Terada T, Yamaga H, Tsumoto T, Masuo O, Itakura T. Use of an embolic protection system during endovascular recanalization of a totally occluded cervical internal carotid artery at the chronic stage. Case report. J Neurosurg. (2005) 102(3):558–64. doi: 10.3171/jns.2005.102.3.0558
74. Shojima M, Nemoto S, Morita A, Miyata T, Namba K, Tanaka Y, et al. Protected endovascular revascularization of subacute and chronic total occlusion of the internal carotid artery. AJNR Am J Neuroradiol. (2010) 31(3):481–6. doi: 10.3174/ajnr.A1843
75. Terada T, Okada H, Nanto M, Shintani A, Yoshimura R, Kakishita K, et al. Endovascular recanalization of the completely occluded internal carotid artery using a flow reversal system at the subacute to chronic stage. J Neurosurg. (2010) 112(3):563–71. doi: 10.3171/2009.6.JNS09125
76. Ishihara H, Sakai N, Kuroiwa T, Sakaguchi M, Morizane A, Sakai C, et al. Percutaneous transluminal angioplasty and stenting for chronic total occlusion of intracranial carotid artery: a case report. Interv Neuroradiol. (2006) 12(3):263–8. doi: 10.1177/159101990601200310
77. Mo D, Jia B, Shi H, Sun Y, Liu Q, Fan C, et al. Staged angioplasty versus regular carotid artery stenting in patients with carotid artery stenosis at high risk of hyperperfusion: a randomised clinical trial. Stroke Vasc Neurol. (2021) 6(1):95–102. doi: 10.1136/svn-2020-000391
78. Bhatt A, Majid A, Kassab M, Gupta R. Chronic total symptomatic carotid artery occlusion treated successfully with stenting and angioplasty. J Neuroimaging. (2009) 19(1):68–71. doi: 10.1111/j.1552-6569.2008.00212.x
79. Kao HL, Lin MS, Wang CS, Lin YH, Lin LC, Chao CL, et al. Feasibility of endovascular recanalization for symptomatic cervical internal carotid artery occlusion. J Am Coll Cardiol. (2007) 49(7):765–71. doi: 10.1016/j.jacc.2006.11.029
80. Myrcha P, Gloviczki P. A systematic review of endovascular treatment for chronic total occlusion of the internal carotid artery. Ann Transl Med. (2021) 9(14):1203. doi: 10.21037/atm-20-6980
81. Chen K, Hou X, Zhou Z, Li G, Liu Q, Gui L, et al. The efficacy and safety of endovascular recanalization of occluded large cerebral arteries during the subacute phase of cerebral infarction: a case series report. Stroke Vasc Neurol. (2017) 2(3):124–31. doi: 10.1136/svn-2017-000086
82. Fan YL, Wan JQ, Zhou ZW, Chen L, Wang Y, Yao Q, et al. Neurocognitive improvement after carotid artery stenting in patients with chronic internal carotid artery occlusion: a prospective, controlled, single-center study. Vasc Endovascular Surg. (2014) 48(4):305–10. doi: 10.1177/1538574414525863
83. Xia ZY, Yang H, Xu JX, Zhang M, Qu HQ, Xu GL, et al. Effect of stenting on patients with chronic internal carotid artery occlusion. Int Angiol. (2012) 31(4):356–60.22801401
84. Lin MS, Lin LC, Li HY, Lin CH, Chao CC, Hsu CN, et al. Procedural safety and potential vascular complication of endovascular recanalization for chronic cervical internal carotid artery occlusion. Circ Cardiovasc Interv. (2008) 1(2):119–25. doi: 10.1161/CIRCINTERVENTIONS.108.772350
85. Zanaty M, Samaniego EA, Teferi N, Kung DK, Nakagawa D, Hudson J, et al. Hybrid surgery for internal carotid artery revascularization. World Neurosurg. (2019) 121:137–44. doi: 10.1016/j.wneu.2018.09.230
86. Yu LB, Yan W, Zhang Q, Zhao JZ, Zhang Y, Wang R, et al. Carotid endarterectomy for treatment of carotid in-stent restenosis: long-term follow-up results and surgery experiences from one single centre. Stroke Vasc Neurol. (2017) 2(3):140–6. doi: 10.1136/svn-2017-000089
87. Shih YT, Chen WH, Lee WL, Lee HT, Shen CC, Tsuei YS. Hybrid surgery for symptomatic chronic total occlusion of carotid artery: a technical note. Neurosurgery. (2013) 73(1 Suppl Operative):onsE117–23; discussion onsE123. doi: 10.1227/NEU.0b013e31827fca6c
88. Zhang K, Gao BL, Zhao TY, Li TX, Xue JY, He YK, et al. Hybrid operation to revascularize long-segment occluded internal carotid artery prevent further ischemic events. Neuroradiology. (2019) 61(2):217–24. doi: 10.1007/s00234-018-2145-7
89. Lovett JK, Dennis MS, Sandercock PA, Bamford J, Warlow CP, Rothwell PM. Very early risk of stroke after a first transient ischemic attack. Stroke. (2003) 34(8):e138–40. doi: 10.1161/01.STR.0000080935.01264.91
90. Huo X, Raynald R, Jing J, Wang A, Mo D, Gao F, et al. Safety and efficacy of oral antiplatelet for patients who had acute ischaemic stroke undergoing endovascular therapy. Stroke Vasc Neurol. (2020) 6(2):230–7. doi: 10.1136/svn-2020-000466
91. Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D, et al. 2021 Guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American heart association/American stroke association. Stroke. (2021) 52(7):e364–e467. doi: 10.1161/STR.0000000000000375
92. Shah J, Liu S, Yu W. Contemporary antiplatelet therapy for secondary stroke prevention: a narrative review of current literature and guidelines. Stroke Vasc Neurol. (2022) 5:406–414. doi: 10.1136/svn-2021-001166
93. Wang P, Zhou M, Pan Y, Meng X, Zhao X, Liu L, et al. Comparison of outcome of patients with acute minor ischaemic stroke treated with intravenous t-PA, DAPT or aspirin. Stroke Vasc Neurol. (2021) 6(2):187–93. doi: 10.1136/svn-2019-000319
94. Batchelder A, Hunter J, Cairns V, Sandford R, Munshi A, Naylor AR. Dual antiplatelet therapy prior to expedited carotid surgery reduces recurrent events prior to surgery without significantly increasing peri-operative bleeding complications. Eur J Vasc Endovasc Surg. (2015) 50(4):412–9. doi: 10.1016/j.ejvs.2015.07.019
95. Ishikawa T, Houkin K, Abe H, Isobe M, Kamiyama H. Cerebral haemodynamics and long-term prognosis after extracranial-intracranial bypass surgery. J Neurol Neurosurg Psychiatry. (1995) 59(6):625–8. doi: 10.1136/jnnp.59.6.625
96. Lee CW, Lin YH, Liu HM, Wang YF, Chen YF, Wang JL. Predicting procedure successful rate and 1-year patency after endovascular recanalization for chronic carotid artery occlusion by CT angiography. Int J Cardiol. (2016) 221:772–6. doi: 10.1016/j.ijcard.2016.07.127
97. Liu B, Wei W, Wang Y, Yang X, Yue S, Zhang J. Estimation and recanalization of chronic occluded internal carotid artery: hybrid operation by carotid endarterectomy and endovascular angioplasty. World Neurosurg. (2018) 120:e457–65. doi: 10.1016/j.wneu.2018.08.104
98. Jiang WJ, Liu AF, Yu W, Qiu HC, Zhang YQ, Liu F, et al. Outcomes of Multimodality In situ Recanalization in Hybrid Operating Room (MIRHOR) for symptomatic chronic internal carotid artery occlusions. J Neurointerv Surg. (2019) 11(8):825–32. doi: 10.1136/neurintsurg-2018-014384
99. Yan L, Wang Z, Liu Z, Yin H, Chen X. Combined endovascular and surgical treatment of chronic carotid artery occlusion: hybrid operation. Biomed Res Int. (2020) 2020:6622502. doi: 10.1155/2020/6622502
100. Komatani H, Okamoto Y, Aoki T, Noguchi K, Morioka M. Long-term prognosis after extracranial-intracranial bypass surgery for symptomatic cerebrovascular occlusive disease. Kurume Med J. (2018) 64(1.2):1–4. doi: 10.2739/kurumemedj.MS6400016
101. Chen YH, Leong WS, Lin MS, Huang CC, Hung CS, Li HY, et al. Predictors for successful endovascular intervention in chronic carotid artery total occlusion. JACC Cardiovasc Interv. (2016) 9(17):1825–32. doi: 10.1016/j.jcin.2016.06.015
102. Kao HL, Hung CS, Li HY, Yeh CF, Huang CC, Chen YH, et al. Long-term outcomes after endovascular recanalization in patients with chronic carotid artery occlusion. Am J Cardiol. (2018) 122(10):1779–83. doi: 10.1016/j.amjcard.2018.07.049
103. Broderick JP, Adeoye O, Elm J. Evolution of the modified rankin scale and its use in future stroke trials. Stroke. (2017) 48(7):2007–12. doi: 10.1161/STROKEAHA.117.017866
Keywords: chronic internal carotid artery occlusion, endovascular interventional therapy, external carotid-internal carotid bypass, review, comparison
Citation: Wu J, Fang C, Wei L, Liu Y, Xu H, Wang X, Yuan L, Wu X, Xu Y and Zhang A (2022) Spotlight on clinical strategies of Chronic Internal Carotid Artery Occlusion: Endovascular interventions and external-intracarotid bypasses compared to conservative treatment. Front. Surg. 9:971066. doi: 10.3389/fsurg.2022.971066
Received: 16 June 2022; Accepted: 18 October 2022;
Published: 8 November 2022.
Edited by:
Ying Jiang, Shanghai Changzheng Hospital, ChinaReviewed by:
Daniel Raper, University of California San Francisco, United States© 2022 Wu, Fang, Wei, Liu, Xu, Wang, Yuan, Wu, Xu and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoya Wu d3V4aWFveWExOTg2MDkxM0AxNjMuY29t Yuanzhi Xu ZHIueXVhbnpoaS54dUBnbWFpbC5jb20= Anke Zhang dGhlYW5rZUAxNjMuY29t
†These authors have contributed equally to this work
Specialty Section: This article was submitted to Neurosurgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.