 Yingnan Liu
Yingnan Liu Yongqing Zhuang1,2
Yongqing Zhuang1,2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 02 August 2022
Sec. Neurosurgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.961616
This article is part of the Research Topic Peripheral Nerve Surgery: Neurosurgery beyond technology View all 10 articles
Background: The aim of the study was to compare the clinical characteristics of diabetic carpal tunnel syndrome between patients with neuropathic pain (NeuP) and non-NeuP.
Methods: We enrolled 276 patients with diabetic carpal tunnel syndrome. Pain symptoms were evaluated using a visual analog scale. Douleur Neuropathique 4, the Neuropathic Pain Symptoms Inventory questionnaire, and the body map were used to assess neuropathic symptoms. Baseline information, clinical manifestations, electrophysiological test results, and psychological status were compared between the neuropathic pain (NeuP) and non-NeuP to identify the risk factor for NeuP occurrence.
Results: Results showed that the degree of pain was more severe in NeuP patients than in nociceptive pain patients (p = 0.025). The frequencies of light touch and pinprick were more pronounced in the NeuP group than in the non-NeuP group (light touch: p = 0.001; pinprick: p = 0.004). There were 48 and 27 NeuP patients with extramedian and proximal spread, respectively, whereas in the non-NeuP group, there were 11 and 9 patients, respectively (p = 0.03). Electrophysiological results showed that patients in the NeuP group exhibited greater sensory nerve conduction velocity impairment compared with the non-NeuP group (p = 0.033). Pain Catastrophizing Scale total scores of the NeuP group were significantly higher than those of the non-NeuP group (p = 0.006).
Conclusion: Of the 276 diabetic carpal tunnel syndrome patients studied, the majority had NeuP. Furthermore, light touch, electrophysiological test results, and psychological factors were found to be related to NeuP occurrence in patients with diabetic carpal tunnel syndrome.
Carpal tunnel syndrome is the most common peripheral nerve entrapment disease with an incidence as high as 10% in the general population (1). The primary symptoms of carpal tunnel syndrome include paresthesia and neuropathic pain (NeuP) in the median territory, weakness of hand grasp, and thenar wasting. NeuP, especially nocturnal pain, is the primary complaint of patients with carpal tunnel syndrome. Pain symptoms directly and negatively impact the sleep quality and hand function of patients, which results in psychological states of anxiety and depression (2).
The International Association for the Study of Pain (IASP) defines NeuP as “pain caused by a lesion or disease of the somatosensory nervous system.” The prevalence of NeuP in carpal tunnel syndrome patients varies from 31% to 80% across studies (3–5). Researchers have dedicated significant effort to determining the characteristics of NeuP in patients with carpal tunnel syndrome. Matesanz et al. reported that the severity of NeuP is associated with more pronounced deficits in emotional well-being and sleep quality (3). Oteo-Alvaro and Marin revealed that numbness/tingling, pain intensity, and neurologic affectation are risk factors for NeuP (4). Moreover, Sonohata et al. found that carpal tunnel release can alleviate NeuP (5).
Diabetes mellitus is a shared risk factor for NeuP and carpal tunnel syndrome (6), and NeuP is often the most pronounced manifestation of carpal tunnel syndrome. Carpal tunnel syndrome and diabetes mellitus have synergistic effects on median nerve injury (7–9). Thus, carpal tunnel syndrome, NeuP, and diabetes mellitus may interact to form a mutual response to the progress of the diseases. Therefore, patients with NeuP who have diabetic carpal tunnel syndrome are likely to present with characteristics that are distinct from those with nondiabetic carpal tunnel syndrome. Understanding the specific symptoms of this subgroup of carpal tunnel syndrome patients could enable more accurate diagnosis and the development of more focused therapies. However, analyses of the characteristics of NeuP in patients with diabetic carpal tunnel syndrome are scarce.
In our clinical practice, we have observed differences between NeuP patients and non-NeuP patients of carpal tunnel syndrome in terms of demographic information, clinical manifestation, and psychological state. Therefore, in the current study, we enrolled 276 diabetic carpal tunnel syndrome patients and divided them into two groups according to the pain symptoms .Then, we compared the clinical characteristics between these two groups to identify possible risk factors for the occurrence of NeuP in patients with diabetic carpal tunnel syndrome. The characteristics of NeuP in diabetic carpal tunnel syndrome patients would provide the hints for the hand surgeons to take some interventions earlier.
This study was approved by the Ethical Committee of Shenzhen People's Hospital.
All participants diagnosed with both carpal tunnel syndrome and diabetes mellitus in the department of hand and microvascular surgery which focused on the peripheral nerve surgery in our hospital, between June 1, 2020 and June 2, 2021, who provided written informed consent and were willing to participate, were recruited into this cross-sectional study. We recruited 276 unilateral carpal tunnel syndrome patients (216 women and 60 men) who were screened according to the inclusion and exclusion criteria. Eligible participants included patients who were aged over 18 years, and who were diagnosed with both carpal tunnel syndrome and diabetes mellitus (Type 1 or Type 2) based on symptoms, physical examinations, and electrophysical tests. The exclusion criteria were as follows: bilateral carpal tunnel syndrome, acute complications of diabetes mellitus (e.g., renal failure, foot ulcers, and severe infection), other NeuP diseases (e.g., peripheral nerve lesions, brain and spinal cord lesions, thyroid dysfunction, and multiple sclerosis), and inability to read or write Chinese (illiterate or an ethnic minority). Patients diagnosed with bilateral carpal tunnel syndrome were excluded because they always presented with different clinical manifestations between the right and left hands, creating difficulties in the data analysis.
Firstly, the visual analog scale (VAS) was used to evaluate whether patients with diabetic carpal tunnel syndrome presented with pain symptoms. Patients after the VAS scale evaluation were diagnosed using the Douleur Neuropathique 4 (DN-4) scale, which is the common diagnosis standard for NeuP (10). The DN-4 scale was used for the definite diagnosis of NeuP in patients with diabetic carpal tunnel syndrome. The questionnaire consists of ten questions evaluating sensory descriptors, and a sensory examination assessing tactile sensation, pinprick, and allodynia. Patients with a DN-4 score of ≥4 were diagnosed with NeuP (11).
Diagnosis of carpal tunnel syndrome was based on clinical manifestations, physical examinations, and electrophysiological tests. The symptoms of carpal tunnel syndrome were numbness or tingling in the median nerve distribution for at least one month. The physical examination for carpal tunnel syndrome detected paresthesia with or without thenar atrophy. The electrophysiology test for carpal tunnel syndrome involved detection of delayed median nerve terminal latency (>3.6 ms). Patients with symptoms but the normal electrophysiology were also diagnosed with carpal tunnel syndrome (12). Patients with extramedian and proximal spread symptoms were also evaluated using spinal MRI or computed tomography to exclude cervical spine-related diseases.
We reviewed the medical records from the hospital database of all participants to collect basic information, including sex, age, height, weight, educational status, and living habits. We also reviewed the duration of clinical manifestations, including median symptom duration and diabetes symptom duration. Levels of glycosylated hemoglobin (HbA1c) were recorded to determine the severity of diabetes during the past 3 months.
To evaluate the clinical symptoms of diabetic carpal tunnel syndrome, we used the Boston Carpal Tunnel Syndrome Questionnaire (BCTQ). The BCTQ comprises a symptom severity score (BCTQ-S) and a functional status score (BCTQ-F), which represent symptom severity and functional deficit, respectively, after median nerve compression (13). The BCTQ-S consists of 11 questions related to symptom severity, whereas the BCTQ-F consists of eight questions on hand function during daily activities. Each question is rated on a five-point scale from 1 (none) to 5 (most severe), and the average score of each item is calculated. The validated translated Chinese version of the BCTQ was used for the current study (12).
In addition to the BCTQ, each participant underwent a physical examination of the sensory and motor function of the median nerve. Light touch and pinprick were evaluated using cotton wool and a neurotip on the palm side of the index finger. The sensation was recorded as normal or reduced compared with the same finger on the other hand. The Tinel sign test involves tapping over the median nerve at the entrance of the carpal tunnel, and is considered positive if the patient senses numbness, tingling, and shooting pains in the thumb, index finger, middle finger, the radial half of the ring finger, and the palm. The Phalen test involves flexion of the wrist to the unforced extreme angle for 60 s, and a positive test is recorded if numbness, tingling, and shooting pains are experienced or exaggerated at the distribution of the median nerve. We also evaluated the muscle strength of the abductor pollicis brevis muscle according to the Medical Research Council scale.
The electrophysiological test was performed using the KEY POINT (Alpine Biomed, Denmark) system. The hand temperature was maintained above 31°C. Median nerve motor function was evaluated by median nerve terminal latency and the compound muscle action potential (CMAP), which were recorded from the abductor pollicis brevis muscle while applying stimulation from the wrist to antecubital fossa. Median nerve sensory function was evaluated by sensory nerve conduction velocity (SNCV), which was recorded from the wrist while stimulating the index finger.
The VAS was used to evaluate the degree of general pain of participants. Patients selected a number that corresponded to their recently experienced pain, on a scale from 0 (no pain) to 10 (the worst pain). We then applied the Neuropathic Pain Symptom Inventory (NPSI), which is a widely used tool for characterizing NeuP symptoms (14, 15). NPSI is a self-reported questionnaire that is specifically designed to evaluate NeuP symptoms and has been validated in more than 50 different languages, including Chinese. This questionnaire comprises five subgroups that represent four aspects of NeuP: burning spontaneous pain, pressing spontaneous pain, paroxysmal pain, evoked pain, and paresthesia/dysesthesia. We also used a combination of the VAS and the body map to indicate pain distributions involved in diabetic carpal tunnel syndrome. We determined and analyzed the involved nerve distribution areas, which included fingers, palm, extramedian distributions, and proximal areas. After comparing the pain distributions between the NeuP group and the non-NeuP group, we investigated the characterstics of neuropathic pain distribution.
The pain catastrophizing scale (PCS) consists of 13 self-reported items that measure pain-related catastrophizing phenomena in the context of actual or anticipated pain (16). The PCS questionnaire was used to evaluate patients' psychological status. The PCS measures catastrophizing phenomena along three dimensions: rumination, magnification, and helplessness (17). It has been widely applied to evaluate various pain conditions, such as low back pain, diabetic pain, NeuP, and stroke pain, and has been shown to be related to pain outcomes. We compared PCS scores between NeuP and non-NeuP groups to determine the pain catastrophizing effect of NeuP in patients with diabetic carpal tunnel syndrome.
Student's t-tests were used to compare the continuous variables between groups, chi-square tests were used to analyze the rate and constituent ratio index, the Shapiro-Wilk test was used to test data normality, and non-normal data were analyzed using the Wilcoxon test. We calculated means and standard deviations for continuous data and frequencies for categorical data. The SPSS software (version 23.0, IBM, New York) was used for all data analyses. We used a p < 0.05 to signify significance.
The demographic information is listed in Tables 1. A total of 198 (71.7%) participants with a DN-4 score of ≥4 were classified into the NeuP group, and the remaining 78 (28.3%) participants with a DN-4 score of <4 were classified into the non-NeuP group. Among the non-NeuP group, half (n = 39) of the patients were classified as having no pain, and the other half were classified as having nociceptive pain. We also tested the VAS scores of the NeuP and non-NeuP groups. The VAS score of the NeuP group was 5.5 ± 3.2, which was significantly higher than that of the non-NeuP group (p = 0.021). We also compared VAS scores between the NeuP and nociceptive pain patients, and found that the degree of pain of NeuP patients was greater than that of nociceptive pain patients (p = 0.025). Notably, we also found that the median symptom duration of the NeuP group was 4.12 ± 2.11 months, whereas the median symptom duration of the non- NeuP group was 8.4 ± 3.22 months (p = 0.014). This indicated that diabetic carpal tunnel syndrome patients with NeuP experienced pain symptoms over a shorter period. Finally, we compared the neuropathic pain proportion between the Type 1 or Type 2 diabetic mellitus and the results showed no significant difference (p = 0.423).
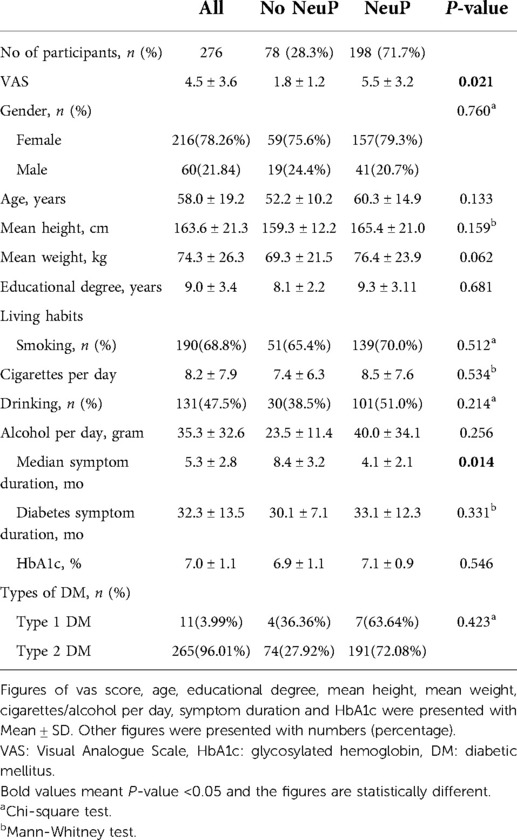
Table 1. Demographic information of the two groups.
Comparisons of clinical manifestations between the two groups are shown in Table 2. We used the BCTQ to assess symptom severity and limb function. Results showed that there was no significant difference between the two groups in terms of functional status (p = 0.391). However, symptom severity was greater in the NeuP group than in the non-NeuP group (p = 0.037).
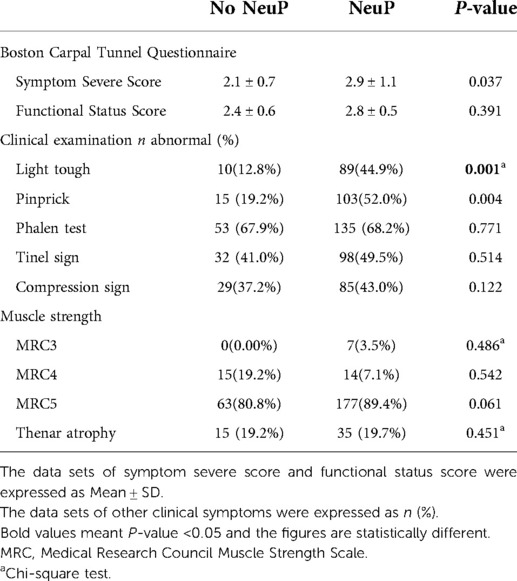
Table 2. Clinical presentations of the two groups.
Furthermore, the frequencies of light touch and pinprick were more pronounced in the NeuP group than in the non-NeuP group (light touch: p = 0.001; pinprick: p = 0.004). There were no significant differences in Phalen and Tinel signs, which are considered two important physical examination components in the diagnosis of carpal tunnel syndrome, between the two groups.
Electrophysiological results showed that patients in the NeuP group exhibited more SNCV impairment than the non-NeuP group (p = 0.033), which provides evidence that nerve injury is related to the occurrence of NeuP (Table 3). Although the CMAP did not significantly differ between the two groups, the median nerve terminal latency of the NeuP group was more prolonged than that of the non-NeuP group (CMAP: p = 0.341; median nerve terminal latency: p = 0.043; Table 3).
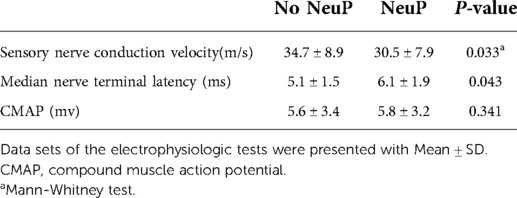
Table 3. Electrophysiologic tests of the two groups.
After determining the possible risk factors for NeuP in diabetic carpal tunnel syndrome patients, we analyzed the symptom characteristics of NeuP in both groups (Tables 4, 5).
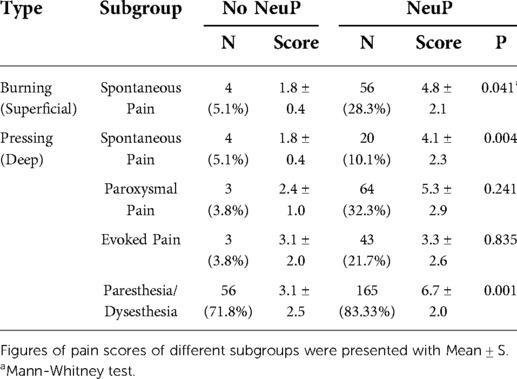
Table 4. Symptomatic comparison of neuropathic pain symptoms between two groups.
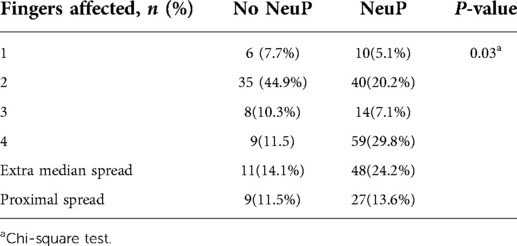
Table 5. Comparison of symptoms distributions between different groups.
Firstly, we found that the symptom distribution of both groups differed significantly. There were 48 and 27 patients in the NeuP group who had extramedian and proximal spread, respectively, whereas 11 and 9 patients in the non-NeuP group had extramedian and proximal spread, respectively (p = 0.03). This suggests that NeuP was not strictly confined to the median nerve distribution. In the non-NeuP group, the majority of patients (44.9%) had symptoms involving two fingers. However, in the NeuP group, most patients (37.8%) had symptoms around the area outside of the median nerve. The analysis of the pain symptoms of diabetic carpal tunnel syndrome patients using the NPSI showed that the most predominant symptoms were paresthesia/dysesthesia, which was observed in 83.33% of patients in the NeuP group and 71.80% of patients in the non-NeuP group. However, we also found that the severity of paresthesia/dysesthesia in the NeuP group was higher than in the non-NeuP group (p = 0.001). In addition, the NeuP group had more deep and superficial spontaneous pain than the non-NeuP group (deep spontaneous pain: p = 0.004; superficial spontaneous pain: p = 0.041).
Given that NeuP affects the psychological status of carpal tunnel syndrome patients, we also evaluated PCS scores between the two groups (Table 6). The PCS total score of the NeuP group was significantly higher than that of the non-NeuP group (p = 0.006). The rumination score of the NeuP group was 4.7 ± 3.4, whereas that of the non-NeuP group was 2.6 ± 1.2 (p = 0.03). The magnification score of the NeuP group was also significantly higher than that of the non-NeuP group (p = 0.04). The helplessness score of the NeuP group was markedly higher than the non-NeuP group, although the difference was not significant (p = 0.062).
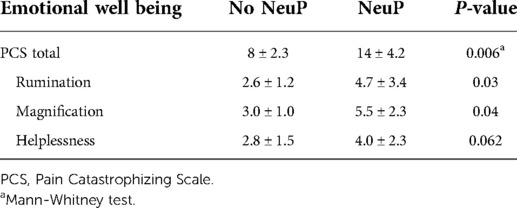
Table 6. Comparison of psychologic factors in two groups in diabetic CTS patients.
Diabetes mellitus is considered a putative risk factor for carpal tunnel syndrome and is also a shared risk factor for NeuP (18, 19). There has been extensive research investigating the characteristics of NeuP in patients with carpal tunnel syndrome and diabetic carpal tunnel syndrome (3, 4, 20). However, few studies have elucidated the risk factors, symptom characteristics, and related psychological factors of patients with both diabetic carpal tunnel syndrome and NeuP. Therefore, we studied 276 diabetic carpal tunnel syndrome patients and divided them into a NeuP and non-NeuP groups according to DN-4 scale scores. We compared clinical data between the two groups to obtain a better understanding of this subgroup of patients with carpal tunnel syndrome.
The prevalence of NeuP in this cohort of patients was 71.7%, which indicated that the majority of the diabetic carpal tunnel syndrome patients experienced NeuP. Previous studies have also reported similar results. Oteo-Alvaro and Marin reported that 76.7% of patients with carpal tunnel syndrome have NeuP (4). Matesanz et al. also reported a prevalence as high as 80% (3). Moreover, Esma reported that 72.7% of carpal tunnel syndrome patients develop NeuP symptoms. Taken together, we found that the occurrence rate of NeuP in diabetic carpal tunnel syndrome patients is comparable to that in all carpal tunnel syndrome patients.
We then compared demographic data between the two groups, which included sex, age, height, weight, educational status, living habits, symptom duration, and HbA1c level. Of these risk factors, median symptom duration showed a significant difference between the non-NeuP and NeuP groups. The median symptom duration of the NeuP group was shorter than that of the non-NeuP group, which indicated that the NeuP patients developed NeuP at an earlier period. This contradicts the common notion that severity of pain symptoms is correlated with disease duration. A possible explanation is that the median nerve injury of the NeuP group was more severe than that of the non-NeuP group; therefore, patients in the NeuP group developed pain symptoms earlier (21). Although differences in alcohol use and the amount of alcohol consumed did not reach significance, the difference between the NeuP and non-NeuP groups is nevertheless notable because alcoholic neuropathy may contribute to NeuP.
Light touch is a prominent symptom of diabetic carpal tunnel syndrome (1). We found that the incidence of abnormal light touch in the NeuP group was significantly higher than that in the non-NeuP group. Previous studies have shown that sensory function is related to the pain phenomenon (22, 23). Different sensory functional deficits may have different underlying mechanisms. In addition, we found that the SNCV of the NeuP group was significantly slower than that of the non-NeuP group. However, the CMAP did not differ significantly between the two groups. The electrophysiological results showed that the sensory nerve is predisposed to be affected in the NeuP group, whereas motor nerve function does not play a central role in the occurrence of NeuP. The electrophysiological results also suggested that the slower SNCV of the NeuP group accounts for the prolonged median nerve terminal latency.
Comparison of the degree of pain showed that spontaneous pain, both superficial and deep, was more severe in the NeuP group compared with the non-NeuP group. Paresthesia and dysesthesia were also significantly different between the two groups. These results were consistent with the clinical manifestations and electrophysiological results.
In addition to pain symptoms, we investigated pain distributions in the two groups. Results showed that the NeuP group had more extramedian and proximal distributions than the non-NeuP group. It has been reported that central mechanisms are also involved in NeuP in patients with carpal tunnel syndrome (24–26). Our results confirmed that central mechanisms play a vital role in diabetic NeuP. The central mechanisms of carpal tunnel syndrome include sensitization and descending facilitation. Previous studies have reported that hyperalgesia, allodynia, and wind-up in extramedian territories are the main sensitization presentations (27–29). In our study, we found that sensitization also correlated with the occurrence of NeuP in diabetic carpal tunnel syndrome patients.
Previous studies have reported that carpal tunnel syndrome patients' mindset and pain catastrophization are related to outcomes (2). We revealed that the NeuP symptoms of diabetic carpal tunnel syndrome patients involved pain catastrophization (30). The underlying mechanism may be that nocturnal pain exerts a negative effect on sleep quality. Moreover, declining grip strength may hinder the work and daily life abilities of patients (31). Insomnia and other life disturbances may also predispose patients to catastrophize, which subsequently creates a vicious cycle (32). Furthermore, pain catastrophization is considered to be related to central mechanisms. The pain catastrophization process is involved in mediating the association between central sensitization and pain expectancy (33). Pain catastrophization also exerts harmful and maladaptive effects on the social environment, and amplifies the central processing of pain (34). Therefore, sociopsychological interventions should be developed to disrupt the pain catastrophization process.
Several limitations of the current research warrant discussion. This was a croos-sectional study; thus,we could only provide potentially related factors for the occurrence of NeuP in diabetic carpal tunnel syndrome patients. Determining the exact cause-effect relationship requires further case-control and cohort studies. In addition, we excluded bilateral carpal tunnel syndrome patients because bilateral clinical manifestations present difficulties in making comparisons. However, bilateral symptoms may also be a factor relevant to NeuP. Therefore, in future research, we encourage case-control and cohort studies that include bilateral carpal tunnel syndrome patients.
Our cross-sectional study of 276 diabetic carpal tunnel syndrome patients revealed that NeuP accounted for the majority of those patients. A total of 198 (71.7%) participants were diagnosed as NeuP. Light touch and electrophysiological test results were related to the occurrence of NeuP. Patients in the NeuP group tended to experience more extramedian and proximal symptoms. Moreover, pain catastrophization was associated with the occurrence of NeuP in patients with diabetic carpal tunnel syndrome.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethical Committee of Shenzhen First People's Hospital. The patients/participants provided their written informed consent to participate in this study.
YL was the primary contributor to the study designation and implementation. YZ supervised all study procedures and revised the manuscript. RHW completed part of the manuscript writing. ZT performed all statistical analyses and checked the data. CC participated in the design of the pain scale. DY supervised and developed the clinical follow-up process. All authors contributed to the article and approved the submitted version.
This study was supported by the Sanming Project of Medicine in Shenzhen (No. SZSM202111025), Shenzhen Key Medical Discipline Construction Fund (No. SZXK024), and Shenzhen Key Laboratory of Musculoskeletal Tissue Reconstruction and Function Restoration (No. ZDSYS20200811143752005).
This study was supported by the Sanming Project of Medicine in Shenzhen (No. SZSM202111025), Shenzhen Key Medical Discipline Construction Fund (No. SZXK024), and Shenzhen Key Laboratory of Musculoskeletal Tissue Reconstruction and Function Restoration (No. ZDSYS20200811143752005).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Padua L, Coraci D, Erra C, Pazzaglia C, Paolasso I, Loreti C, et al. Carpal tunnel syndrome: clinical features, diagnosis, and management. Lancet Neurol. (2016) 15(12):1273–84. doi: 10.1016/S1474-4422(16)30231-9
2. Sun PO, Walbeehm ET, Selles RW, Slijper HP, Ulrich DJO, Porsius JT, et al. Patient mindset and the success of carpal tunnel release. Plast Reconstr Surg. (2021) 147(1):66e–75e. doi: 10.1097/PRS.0000000000007441
3. Matesanz L, Hausheer AC, Baskozos G, Bennett DLH, Schmid AB. Somatosensory and psychological phenotypes associated with neuropathic pain in entrapment neuropathy. Pain. (2021) 162(4):1211–20. doi: 10.1097/j.pain.0000000000002102
4. Oteo-Alvaro A, Marin MT. Predictive factors of the neuropathic pain in patients with carpal tunnel syndrome and its impact on patient activity. Pain Manag. (2018) 8(6):455–63. doi: 10.2217/pmt-2018-0045
5. Sonohata M, Tsuruta T, Mine H, Asami A, Ishii H, Tsunoda K, et al. The effect of carpal tunnel release on neuropathic pain in carpal tunnel syndrome. Pain Res Manag. (2017) 2017:8098473. doi: 10.1155/2017/8098473
6. Zhang Y, Liu X, Jia J, Zhang Q, Lin Y, Zhang L, et al. Diabetic polyneuropathy and carpal tunnel syndrome together affect hand strength, tactile sensation and dexterity in diabetes patients. J Diabetes Investig. (2021) 12(11):2010–18. doi: 10.1111/jdi.13580
7. Thomsen N, Dahlin LB. Vibrotactile sense 5 years after carpal tunnel release in people with diabetes: a prospective study with matched controls. Diabet Med. (2021) 38(7):e14453. doi: 10.1111/dme.14453
8. Thomsen NO, Cederlund RI, Andersson GS, Rosen I, Bjork J, Dahlin LB. Carpal tunnel release in patients with diabetes: a 5-year follow-up with matched controls. J Hand Surg Am. (2014) 39(4):713–20. doi: 10.1016/j.jhsa.2014.01.012
9. Kamel SR, Sadek HA, Hamed A, Sayed OA, Mahmud MH, Mohamed FA, et al. Ultrasound-guided insulin injection for carpal tunnel syndrome in type 2 diabetes mellitus patients. Clin Rheumatol. (2019) 38(10):2933–40. doi: 10.1007/s10067-019-04638-7
10. Sadatsune EJ, Leal Pda C, Cossetti RJ, Sakata RK. Effect of preoperative gabapentin on pain intensity and development of chronic pain after carpal tunnel syndrome surgical treatment in women: randomized, double-blind, placebo-controlled study. Sao Paulo Med J. (2016) 134(4):285–91. doi: 10.1590/1516-3180.2015.00980710
11. Bouhassira D, Attal N, Alchaar H, Boureau F, Brochet B, Bruxelle J, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. (2005) 114(1-2):29–36. doi: 10.1016/j.pain.2004.12.010
12. Lee JK, Yoon BN, Cho JW, Ryu HS, Han SH. Carpal tunnel release despite normal nerve conduction studies in carpal tunnel syndrome patients. Ann Plast Surg. (2021) 86(1):52–7. doi: 10.1097/SAP.0000000000002570
13. Fok M, Leung HB, Lee WM. Evaluation of a Hong Kong Chinese version of a self-administered questionnaire for assessing symptom severity and functional status of carpal tunnel syndrome: cross-cultural adaptation and reliability. Hong Kong Med J. (2007) 13(5):342–7. PMID: 1791413817914138
14. Bouhassira D, Attal N, Fermanian J, Alchaar H, Gautron M, Masquelier E, et al. Development and validation of the neuropathic pain symptom inventory. Pain. (2004) 108(3):248–57. doi: 10.1016/j.pain.2003.12.024
15. Lu LC, Chang SY, Liu CY, Tsay SL. Reliability and validity of the Chinese version neuropathic pain symptom inventory in patients with colorectal cancer. J Formos Med Assoc. (2018) 117(11):1019–26. doi: 10.1016/j.jfma.2017.11.010
16. Darnall BD, Sturgeon JA, Cook KF, Taub CJ, Roy A, Burns JW, et al. Development and validation of a daily pain catastrophizing scale. J Pain. (2017) 18(9):1139–49. doi: 10.1016/j.jpain.2017.05.003
17. Cheng ST, Chen PP, Chow YF, Chung JWY, Law ACB, Lee JSW, et al. The pain catastrophizing scale-short form: psychometric properties and threshold for identifying high-risk individuals. Int Psychogeriatr. (2019) 31(11):1665–74. doi: 10.1017/S1041610219000024
18. Abuzinadah AR, Alzabidi ZH, Abuzaid AE, Kattan KW, Alsubaie BS, Altunisi AM, et al. Carpal tunnel decompression surgery outcome and effect of diabetes. Eur Neurol. (2020) 83(2):189–94. doi: 10.1159/000507957
19. Urits I, Gress K, Charipova K, Orhurhu V, Kaye AD, Viswanath O. Recent advances in the understanding and management of carpal tunnel syndrome: a comprehensive review. Curr Pain Headache Rep. (2019) 23(10):70. doi: 10.1007/s11916-019-0811-z
20. Sonohata M, Tsuruta T, Mine H, Asami A, Ishii H, Tsunoda K, et al. Clinical characteristics of neuropathic pain in patients with carpal tunnel syndrome. Hand Surg. (2014) 19(1):43–8. doi: 10.1142/S0218810414500087
21. Gursoy AE, Kolukisa M, Yildiz GB, Kocaman G, Celebi A, Kocer A. Relationship between electrodiagnostic severity and neuropathic pain assessed by the LANSS pain scale in carpal tunnel syndrome. Neuropsychiatr Dis Treat. (2013) 9:65–71. doi: 10.2147/NDT.S38513
22. Zhou Y, Liu P, Rui J, Zhao X, Lao J. The associated factors and clinical features of neuropathic pain after brachial plexus injuries: a cross-sectional study. Clin J Pain. (2017) 33(11):1030–6. doi: 10.1097/AJP.0000000000000493
23. Guo J, Gao K, Zhou Y, Zhao X, Lao J. Comparison of neuropathic pain characteristics associated with total brachial plexus injury before and after surgical repair: a retrospective study. Clin Neurol Neurosurg. (2020) 191:105692. doi: 10.1016/j.clineuro.2020.105692
24. Maeda Y, Kim H, Kettner N, Kim J, Cina S, Malatesta C, et al. Rewiring the primary somatosensory cortex in carpal tunnel syndrome with acupuncture. Brain. (2017) 140(4):914–27. doi: 10.1093/brain/awx015
25. Fernandez-de-Las-Penas C, Fernandez-Munoz JJ, Navarro-Pardo E, da-Silva-Pocinho RF, Ambite-Quesada S, Pareja JA. Identification of subgroups of women with carpal tunnel syndrome with central sensitization. Pain Med. (2016) 17(9):1749–56. doi: 10.1093/pm/pnw054
26. Fernandez-de-las-Penas C, de la Llave-Rincon AI, Fernandez-Carnero J, Cuadrado ML, Arendt-Nielsen L, Pareja JA. Bilateral widespread mechanical pain sensitivity in carpal tunnel syndrome: evidence of central processing in unilateral neuropathy. Brain. (2009) 132(Pt 6):1472–9. doi: 10.1093/brain/awp050
27. Dhond RP, Ruzich E, Witzel T, Maeda Y, Malatesta C, Morse LR, et al. Spatio-temporal mapping cortical neuroplasticity in carpal tunnel syndrome. Brain. (2012) 135(Pt 10):3062–73. doi: 10.1093/brain/aws233
28. Zanette G, Cacciatori C, Tamburin S. Central sensitization in carpal tunnel syndrome with extraterritorial spread of sensory symptoms. Pain. (2010) 148(2):227–36. doi: 10.1016/j.pain.2009.10.025
29. Soon B, Vicenzino B, Schmid AB, Coppieters MW. Facilitatory and inhibitory pain mechanisms are altered in patients with carpal tunnel syndrome. PLoS One. (2017) 12(8):e0183252. doi: 10.1371/journal.pone.0183252
30. Sun PO, Walbeehm ET, Selles RW, Jansen MC, Slijper HP, Ulrich DJO, et al. Influence of illness perceptions, psychological distress and pain catastrophizing on self-reported symptom severity and functional status in patients with carpal tunnel syndrome. J Psychosom Res. (2019) 126:109820. doi: 10.1016/j.jpsychores.2019.109820
31. Nunez-Cortes R, Cruz-Montecinos C, Antunez-Riveros MA, Perez-Alenda S. Does the educational level of women influence hand grip and pinch strength in carpal tunnel syndrome? Med Hypotheses. (2020) 135:109474. doi: 10.1016/j.mehy.2019.109474
32. Lozano Calderon SA, Paiva A, Ring D. Patient satisfaction after open carpal tunnel release correlates with depression. J Hand Surg Am. (2008) 33(3):303–7. doi: 10.1016/j.jhsa.2007.11.025
33. Carriere JS, Martel MO, Meints SM, Cornelius MC, Edwards RR. What do you expect? Catastrophizing mediates associations between expectancies and pain-facilitatory processes. Eur J Pain. (2019) 23(4):800–11. doi: 10.1002/ejp.1348
34. Malfliet A, Kregel J, Meeus M, Danneels L, Cagnie B, Roussel N, et al. Patients with chronic spinal pain benefit from pain neuroscience education regardless the self-reported signs of central sensitization: secondary analysis of a randomized controlled multicenter trial. PM R. (2018) 10(12):1330–43.e1. doi: 10.1016/j.pmrj.2018.04.010
Keywords: carpal tunnel syndrome, neuropathic pain, diabetic mellitus, cross-sectional study, psychologcal assessment
Citation: Liu Y, Zhuang Y, Wei R, Tan Z, Chen C and Yang D (2022) Comparison of characteristics between neuropathic pain and non-neuropathic pain in patients with diabetic carpal tunnel syndrome: A cross-sectional study. Front. Surg. 9:961616. doi: 10.3389/fsurg.2022.961616
Received: 5 June 2022; Accepted: 18 July 2022;
Published: 2 August 2022.
Edited by:
Lukas Rasulić, University of Belgrade, SerbiaReviewed by:
Sanja Lepić, Military Medical Academy, Serbia© 2022 Liu, Zhuang, Wei, Tan, Chen and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dazhi Yang eWFuZ2R6c3pAMTYzLmNvbQ==
Specialty Section: This article was submitted to Neurosurgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.