 Salah Alghamdi1
Salah Alghamdi1 Hyder Mirghani2*Khalid Alhazmi3Amirah M. Alatawi4Haneen Brnawi1Tariq Alrasheed2Waleed Badoghaish2
Hyder Mirghani2*Khalid Alhazmi3Amirah M. Alatawi4Haneen Brnawi1Tariq Alrasheed2Waleed Badoghaish2
- 1Department of Surgery, Faculty of Medicine, University of Tabuk, Tabuk, Saudi Arabia
- 2Department of Internal Medicine, Faculty of Medicine, University of Tabuk, Tabuk, Saudi Arabia
- 3Department of Pathology, Faculty of Medicine, University of Tabuk, Tabuk, Saudi Arabia
- 4Department of Family and Community Medicine, Faculty of Medicine, University of Tabuk, Tabuk, Saudi Arabia
Roux-en-Y gastric bypass (LRYGB) and laparoscopic sleeve gastrectomy (LSG) are the most commonly used bariatric procedures. There is an increasing awareness about a comorbidity-based indication for bariatric surgery regardless of weight (metabolic surgery). The best operation to mitigate obesity-associated comorbidities is a matter of controversy. This review is aimed at comparing LRYGB and LSG for the treatment of diabetes, hypertension, dyslipidemias, obstructive sleep apnea (OSA), and gastroesophageal reflux (GERD). We searched PubMed, MEDLINE, SCOPUS, Web of Science, and Cochrane library for articles comparing these two commonly used bariatric approaches. We identified 2,457 studies, 1,468 of which stood after the removal of duplications; from them, 81 full texts were screened and only 16 studies were included in the final meta-analysis. LRYGB was equal weight to LSG for diabetes (P-value = 0.10, odd ratio, 1.24, 95% CI, 0.96–1.61, I2 for heterogeneity = 30%, P-value for heterogeneity, 0.14), and OSA (P-value = 0.38, odd ratio, 0.79, 95% CI, 0.47–1.33, I2 for heterogeneity = 0.0%, P-value for heterogeneity, 0.98). However, LRYGB was superior to LSG regarding hypertension (P-value = 0.009, odd ratio, 1.55, 95% CI, 1.20–2.0, I2 for heterogeneity = 0.0%, P-value for heterogeneity, 0.59), dyslipidemia (odd ratio, 2.18, 95% CI, 1.15–4.16, P-value for overall effect, 0.02), and GERD (P-value = 0.003, odd ratio, 3.16, 95% CI, 1.48–6.76). LRYGB was superior to LSG for gastroesophageal reflux, hypertension, and dyslipidemia remission. While the two procedures were equal regarding diabetes and obstructive sleep, further reviews comparing LSG, and one anastomosis gastric bypass are recommended.
Introduction
Obesity is one of the most challenging pandemics worldwide due to its various complications, which include diabetes mellitus, high blood pressure, respiratory disease, dyslipidemia, and cancer. The prevalence of obesity is rising worldwide (1). An intriguing study shows that despite attempting to lose weight in nearly 100% of participants, around two-thirds achieved a weight loss of ≥5%, but only 5% maintained the weight loss for 1 year (2). In addition, only half of the patients are motivated to lose weight (3). Diabetes mellitus is rapidly increasing, the prevalence worldwide is 9.2% and most patients are not reaching the recommended target for fasting plasma glucose, lipid profile, blood pressure, and lifestyles (4, 5). Furthermore, hypoglycemic medications are not without fatal complications including hypoglycemia and risk of falls, especially among the elderly and frail (6). Despite the emergence of novel antidiabetic medications with cardio-renal protection, their use is limited due to the cost and side effects such as toe amputation, osteoporosis, and infections. Furthermore, most patients with diabetes are not controlled (7, 8). There is a recent shift in the indication of bariatric surgery from a certain body mass index (BMI) to comorbidity-based approach where interdisciplinary care by surgeons, endocrinologists or internists, a psychologist, and a dietician is needed before surgery (9).
Although metabolic surgery is a rapidly growing effective measure for obesity treatment, the uptake is small due to the perceived invasive nature and fear of complications. A meta-analysis concluded the effectiveness of endoscopic sleeve gastroplasty (ESG) with a lower rate of side effects (10).
Roux-en-Y gastric bypass and sleeve gastrectomy are the two common bariatric procedures for obesity and comorbidities. Since its introduction by Mason in 1966, Roux-en-Y gastric bypass accounted for 60%–70% of bariatric surgeries in the US. It is both a restrictive and malabsorptive procedure. The procedure is associated with diabetes remission, lower use of antidiabetic medications, and lower body weight and triglyceride compared with the usual care for diabetes (11). Sleeve gastrectomy is a restrictive bariatric surgery, and due to its lower risk, it is increasingly used. Similar outcomes to bypass were observed. The laparoscopic approach through 1-day surgery is now the standard of care due to the lower morbidity and mortality (11).
The remission of obesity comorbidities such as hypertension, diabetes mellitus, dyslipidemias, obstructive sleep apnea (OSA), and gastroesophageal reflux were documented (12, 13). However, comparisons between various types of metabolic surgery on remission are lacking, therefore, this meta-analysis aimed to compare the effects of Roux-en-Y gastric bypass (LRYGB) and sleeve gastrectomy (LSG) on obesity comorbidities.
Methods
Eligibility criteria according to PICOS
Inclusion criteria
Studies were included if they were randomized controlled trials carried out among adults >18 years and with BMI >27.5 kg/m2 with a minimum of 12 months follow-up. The patients were those who underwent LSG or LRYGB without revision or conversion. The search engine was set to English.
Exclusion criteria
Retrospective and prospective cohorts, case-control studies, case reports, and case series were not included. Abstracts, opinions, letters, editorials, and expert opinions were also excluded. Studies with revisions or conversions were not included.
Outcome measures
The outcome measures were diabetes, hypertension, dyslipidemia, gastroesophageal reflux, and OSA remission. Diabetes remission was defined as HbA1c < 6 without diabetes medication for at least 1 year. Hypertension and dyslipidemia remission is normal blood pressure and lipids without drugs. GERD was defined in the presence of either reflux esophagitis (Los Angeles B, C, or D) or increased total acid exposure (>6%), as recommended by Lyon consensus regardless of typical GERD symptoms.
In the present study, we did not concentrate on specific body mass indexes. The BMI of the patients included in the analyzed studies varied widely. In addition, one study included LSG and Banded LRYGB and another one used LSG and OAGB.
The literature search
We searched PubMed, MEDLINE, Cochrane Library, SCOPUS, and Web of Science for articles published in English from the first inception up to January 2022. Two researchers (SA and HM) screened the titles, abstracts, and references of the included studies for relevant articles; any discrepancy was solved by a consensus. The search was performed using combinations of bariatric surgery, sleeve gastrectomy, Roux-en-Y gastric bypass, diabetes, hypertension, dyslipidemia, gastroesophageal reflux, OSA, 5 years, and comorbidity resolution. We identified 2,457 studies, 1,468 of which stood after the removal of duplications; from them, 81 full texts were screened and only 16 studies were included in the final meta-analysis. A datasheet was used to extract the author's name, year, and country of publication, as well as the study type, and comorbidities remission (Tables 1, 2 and Figure 1).
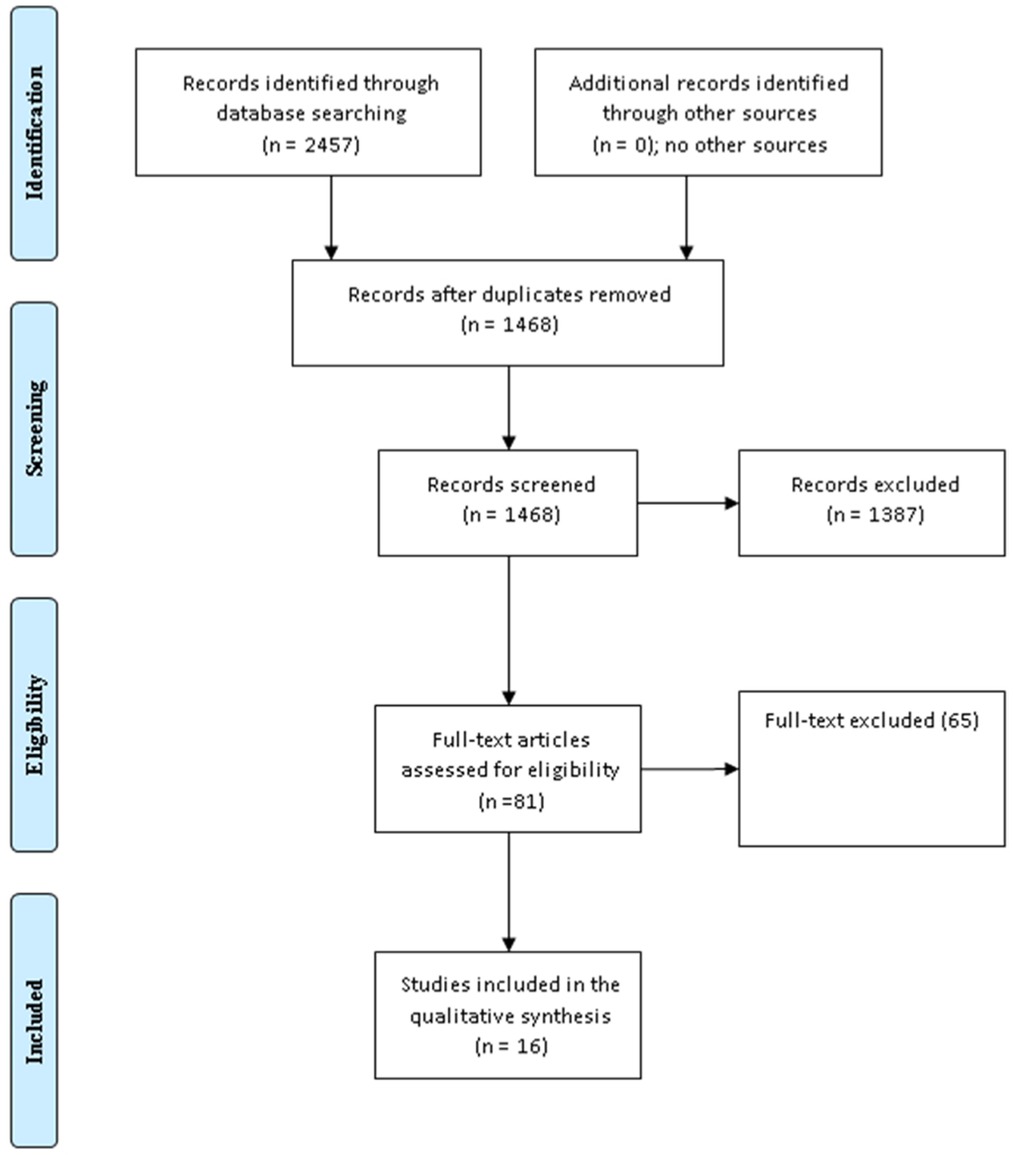
Figure 1. The PRISMA chart (30) for studies comparing Roux-en-Y gastric bypass (LRYGB) and sleeve gastrectomy (LSG).
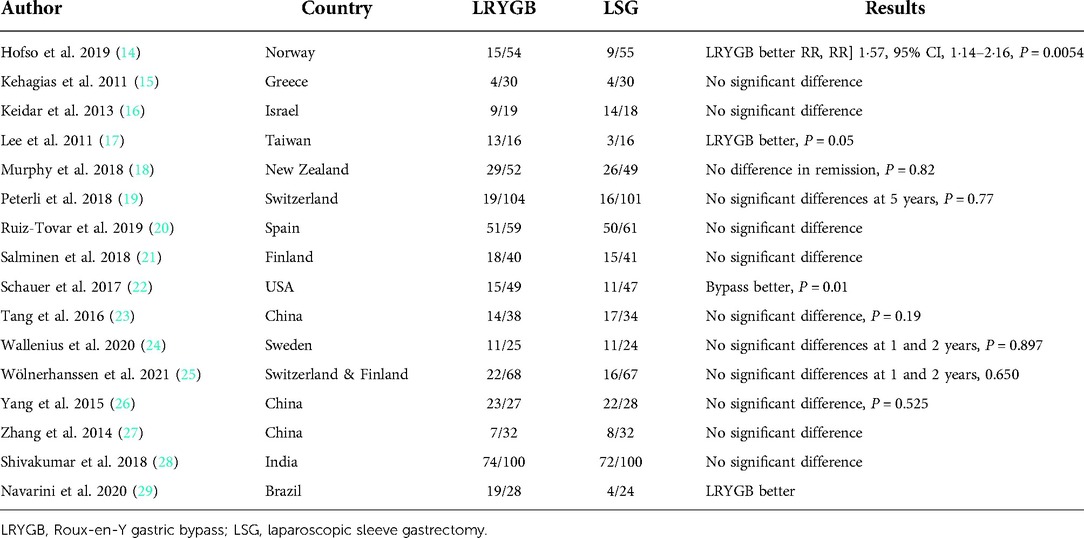
Table 1. Randomized controlled trials comparing LRYGB and LSG regarding diabetes remission.
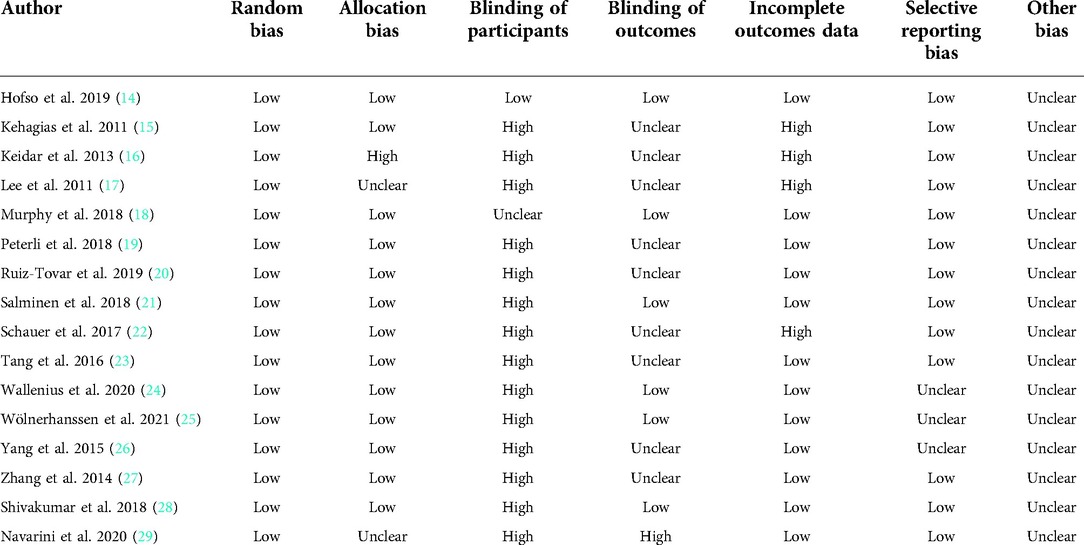
Table 2. The quality of the included trials.
Statistical analysis
The most recent version of the RevMan system (version 5, 4.) was used to compare LSG and LRYGB. The dichotomous data of 33 cohorts from 16 randomized controlled trials (14 studies comparing sleeve gastrectomy and Roux-en-Y gastric bypass on diabetes remission, 8 on hypertension, 5 on dyslipidemia, 4 on OSA, and 2 on gastroesophageal reflux) were entered manually. The odd ratio, 95% CI, and standard mean difference were measured. The Chi-square and I2 were used to quantify the heterogeneity, where the random effect was used if significant (dyslipidemia arm). Otherwise, the fixed effect was applied. A P-value of <0.05 was considered significant. A modified Cochrane risk of bias assessed the quality of the included studies (14). We strictly followed the standards of the Preferred Reporting Items for Meta-analysis (PRISMA) (15).
Results
Characteristics of the included trials
The author's name, country, year of publication, age, sex, BMI, duration of diabetes, waist circumference, HbA1c, and period of follow-up at baseline are depicted in Table 3. Diabetes remission only was reported in references (14, 16–18, 23, 24), diabetes and hypertension in (15, 19–22, 25–27), diabetes, hypertension, and dyslipidemia in (19–21, 25, 27). In addition, reference (19) reported all the ends and reference number (15) reported all ends except dyslipidemia. The current meta-analysis assessed the short (seven studies) and medium outcomes (nine studies). Regarding the diagnoses of diabetes mellitus, some of the studies followed the American guidelines (19, 21), while others were not (14, 17, 18, 20).
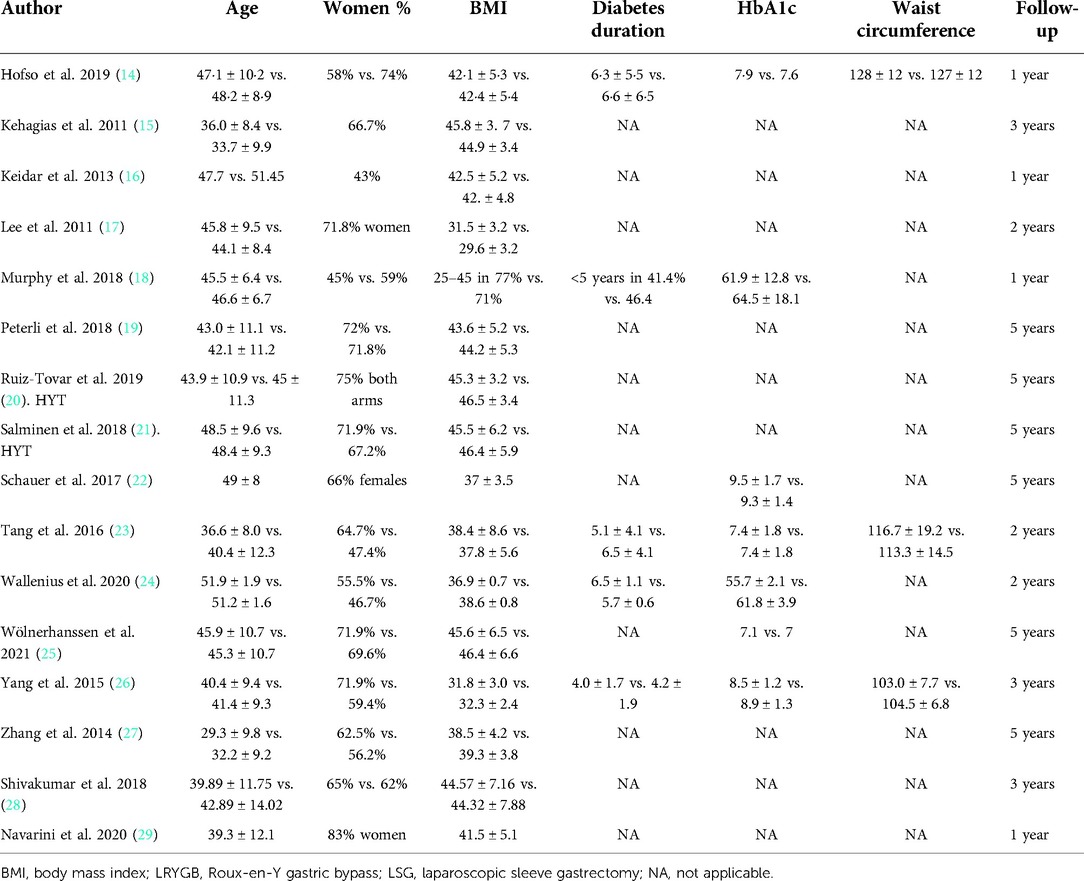
Table 3. Basic characters of the randomized controlled trials comparing LSG and LRYGB (LSG vs. LRYGB).
Diabetes remission
In the present meta-analysis, 14 randomized controlled trials assessed diabetes remission following Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy (14–27). No significant statistical difference was found between LRYGB and LSG regarding diabetes remission, P-value = 0.10, odd ratio, 1.24, 95% CI, 0.96–1.61, I2 for heterogeneity = 30%, P-value for heterogeneity, 0.14 (Figure 2).
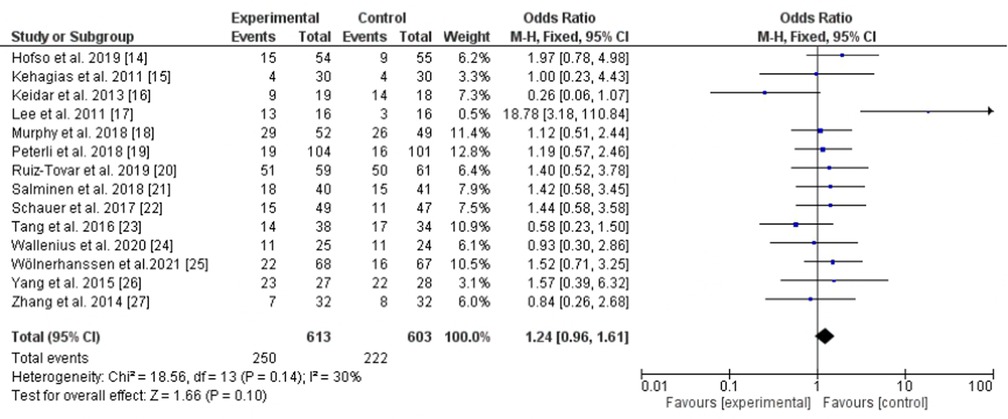
Figure 2. Diabetes remission following Roux-en-Y gastric bypass and sleeve gastrectomy.
Hypertension and dyslipidemia remission
LRYGB was superior to LSG regarding hypertension remission (eight cohorts) (15, 19–21, 25–28) with significant statistical difference, P-value = 0.009, odd ratio, 1.55, 95% CI, 1.20–2.0, I2 for heterogeneity = 0.0%, P-value for heterogeneity, 0.59 (Figure 3). LRYGB was also superior for dyslipidemia remission (five cohorts) (19–21, 25, 27). However, substantial heterogeneity was observed, I2 = 65%, P-value for heterogeneity, 0.02, odd ratio, 2.18, 95% CI, 1.15–4.16, P-value for overall effect, 0.02 (Figure 4).
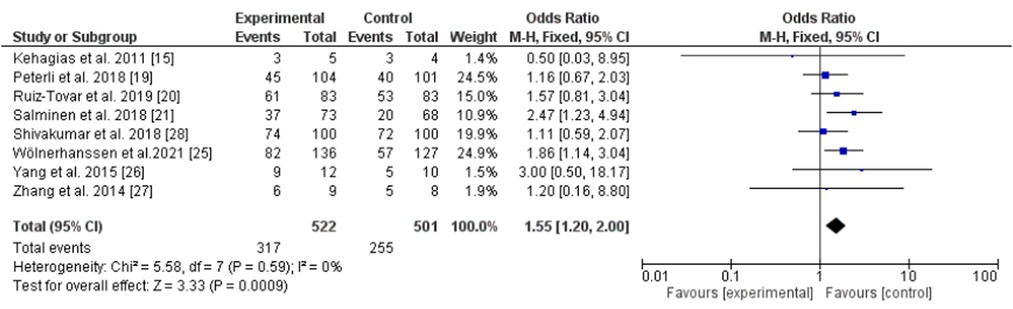
Figure 3. Hypertension remission following Roux-en-Y gastric bypass and sleeve gastrectomy.
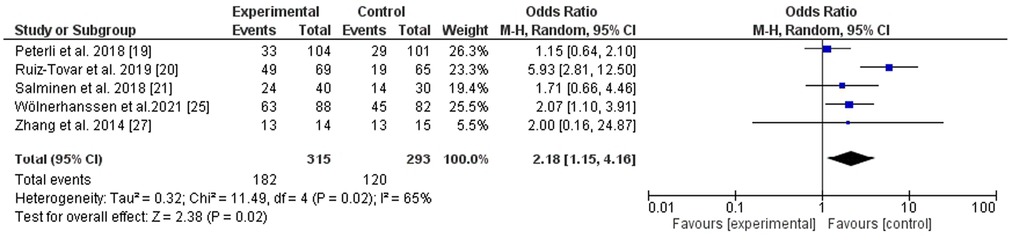
Figure 4. Dyslipidemia remission following Roux-en-Y gastric bypass and sleeve gastrectomy.
Obstructive sleep apnea remission
Obstructive sleep apnea was assessed by four trials (15, 19, 25, 32), LSG was equal weight to LRYGB, P-value = 0.38, odd ratio, 0.79, 95% CI, 0.47–1.33, I2 for heterogeneity = 0.0%, P-value for heterogeneity, 0.98 (Figure 5).
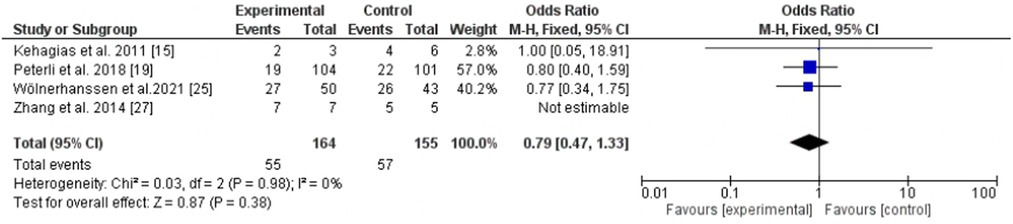
Figure 5. Obstructive sleep apnea remission following Roux-en-Y gastric bypass and sleeve gastrectomy.
Gastroesophageal reflux remission and new-onset reflux following surgery
LRYGB was better for GERD remission (two trials) (15, 19), P-value = 0.003, odd ratio, 3.16, 95% CI, 1.48–6.76, heterogeneity not applicable. However, no significant statistical difference between LRYGB and LSG regarding the new-onset of GERD (four trials) (21, 22, 25, 28), P-value = 0.55, odd ratio, 0.42, 95% CI, 0.02–7.24, with substantial heterogeneity, I2 = 089%, P-value for heterogeneity, 0.0001 (Figures 6, 7).

Figure 6. Gastroesophageal reflux remission following Roux-en-Y gastric bypass and sleeve gastrectomy.
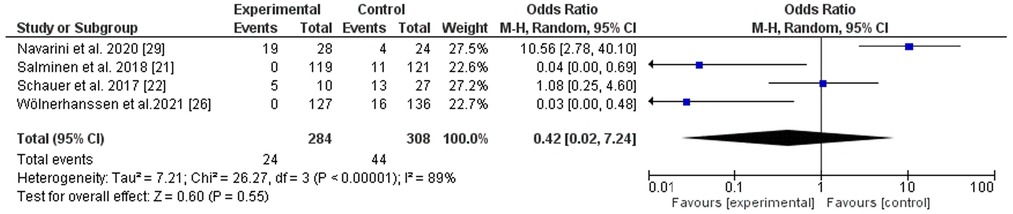
Figure 7. New-onset gastroesophageal reflux following Roux-en-Y gastric bypass and sleeve gastrectomy.
Discussion
Diabetes remission after Roux-en-Y gastric bypass and sleeve gastrectomy
There is a recent shift in an indication of bariatric surgery from a certain BMI to a comorbidity-based approach where interdisciplinary care by surgeons, endocrinologists or internists, a psychologist, and a dietician is needed before surgery.
In the present meta-analysis, diabetes remission was similar between LRYGB and LSG in contradiction to Gu et al. (32). However, Gu and colleagues’ study was limited by pooling different methodologies and including only four trials. A recent meta-analysis (33) included 10 RCTs, which showed the superiority of LRYGB over LSG over the short term only. Another meta-analysis published by Sharples et al. (34) showed that LRYGB and LSG were similar regarding glycemic control at 5 years, in line with our findings. In addition, more reduction of serum cholesterol and lower gastrointestinal reflux were observed among patients following LRYGB in similarity to the present findings, however, the study included only four trials.
Higher levels of bile acids were observed in LRYGB patients with a similar rate of diabetes remission in LRYGB and LSG, indicating a role of BA in glycemic control (35).
Sha et al. (36) Lee et al. (37), Huang et al. (38), and Zhao et al. (39) meta-analyses concluded the similarity of LRYGB and LSG regarding diabetes remission. The previous studies were limited by pooling studies with different methodologies, a small number of the included studies, and a short period of follow-up.
The effects on hypertension and dyslipidemias
The effects of LRYGB and LSG on hypertension and dyslipidemia were discussed controversially. In addition, all the meta-analyses were limited by pooling different methodologies and a small sample of well-randomized studies. A meta-analysis of 14 studies showed no difference regarding the resolution of hypertension and improvement of cholesterol and triglycerides (40); further meta-analysis supported these findings (41, 42) in contradiction to Gu et al. (32) Li et al. (43) and Zhao et al., who showed the superiority of LRYGB. In the present study, LRYGB was superior regarding hypertension and dyslipidemia remission. The current findings were consistent with Climent et al. who showed a more sustained effect of LRYGB on blood pressure (44). A meta-analysis of randomized controlled trials (45) showed a higher resolution of dyslipidemia with a high certainty at 1 year and moderate evidence at 3 years with no differences regarding hypertension.
Gastroesophageal reflux
The evidence regarding gastroesophageal reflux is largely based on observational studies and systematic reviews. A retrospective analysis with a large sample size showed that LSG is associated with more gastroesophageal reflux; indeed 16% need conversion to LRYGB at 10 years (46). More retrospective studies showed similar observations (47). Recent systematic reviews showed a higher rate of GERD among patients with LSG (48, 49). A retrospective analysis showed that conversion to LRYGB is an effective approach for those with significant GERD (48). A randomized controlled trial concluded the superiority of LRYGB for the treatment of GERD (50). Thus, LRYGB is better for those with GERD.
Obstructive sleep apnea
Bariatric surgery poses beneficial effects on pulmonary function; a previous study showed that 48% and 80% of patients with bronchial asthma and OSA were symptom-free at 5 years, and another study showed remission/improvement in 90% and 90.74% (51, 52). Regarding OSA, no differences in remission were noted regarding the type of operation (53–55) in line with the present study in which LRG and LRYGB were similar.
Surgical complications
In LRYGB, a gastric pouch was performed by dividing the stomach with a linear stapler and then gastrojejunal anastomosis was created. LSG was conducted by dividing the stomach with the linear stapler through the large gastric curvature; resection was completed and running imbricated absorbable suture (29).
Sleeve gastrectomy is associated with fewer early and late postoperative complications and reoperation when compared to LRYGB, Sha et al. (36) reported a higher dumping syndrome among patients after LRYGB. The operation time is an advantage for LSG (27–29, 32–41, 56). Furthermore, LSG showed lower rates of iron and vitamin D deficiency, and fewer calcium and phosphorus abnormalities (57, 58). Postoperative bleeding was lower in LSG (59). On the other hand, LRYGB was associated with lower rates of gastroesophageal reflux (60).
Effects on gut hormones
The effects of LSG and LRYGB on gut hormones are complex and inconsistent. Some studies showed no difference in body weight between LSG and LRYGB (61, 62). Although the great effects of LRYGB on body weight compared to LSG might be mediated in part through gut hormones (32, 45, 63).
LSG showed lower Ghrelin and higher resistin than LRYGB, with no differences regarding glucagon-like peptide-1, gastric inhibitory peptide, and leptin (17). Gu et al. (64) found a significant reduction in fasting peptide YY among patients following LRYGB, while ghrelin was reduced after LSG. A great area under the curve of fasting peptide YY and increased glucagon-like peptide-1 was observed among patients with LRYGB (65). Other studies found no differences between the two procedures regarding glucagon-like peptide-1, gastric inhibitory peptide (66).
This manuscript gave insight into patients' categorization before bariatric surgery and choosing the suitable type of surgery according to comorbidities. However, the small number of studies included, the heterogeneity observed in the dyslipidemia arm, and the discrepancy in the diagnosis of ends and remission are limitations.
Nonalcoholic fatty liver disease (NAFLD)
Bariatric surgery is beneficial for nonalcoholic fatty liver disease (NAFLD), recently renamed metabolic-related fatty liver disease. The mechanism involves bile acid pathways, gut hormones, and intestinal microbiota. The data on the effects of LRYGB and LSG on liver enzymes are scarce; however, LSG seems better at normalizing liver enzymes in 1 year (67, 68).
Conclusion
LRYGB was superior to LSG for gastroesophageal reflux, hypertension, and dyslipidemia remission. While the two procedures were equal regarding diabetes and obstructive sleep, LSG may be better for metabolic-related fatty liver disease and is associated with fewer surgical complications. Further reviews comparing LSG and one anastomosis gastric bypass are recommended.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
HM and SA contributed to the conceptualization, design, drafting of the introduction, and methodology. TA and HB searched the literature and drafted part of the discussion. WB drafted part of the discussion. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. (2019) 15(5):288–98. doi: 10.1038/s41574-019-0176-8
2. Alfadda AA, Al Qarni A, Alamri K, Ahamed SS, Abo’ouf SM, Shams M, et al. Perceptions, attitudes, and barriers toward obesity management in Saudi Arabia: data from the ACTION-IO study. Saudi J Gastroenterol. (2021) 27:166–72. doi: 10.4103/sjg.sjg_500_20
3. Hedjoudje A, Abu Dayyeh BK, Cheskin LJ, Adam A, Neto MG, Badurdeen D, et al. Efficacy and safety of endoscopic sleeve gastroplasty: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. (2020) 18(5):1043–53.e4. doi: 10.1016/j.cgh.2019.08.022
4. Saeedi P, Petersohn I, Salpea P, Malanda B, Karuranga S, Unwin N, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. (2019) 157:107843. doi: 10.1016/j.diabres.2019.107843
5. Lovic D, Piperidou A, Zografou I, Grassos H, Pittaras A, Manolis A. The growing epidemic of diabetes mellitus. Curr Vasc Pharmacol. (2020) 18(2):104–9. doi: 10.2174/1570161117666190405165911
6. Sesti G, Antonelli Incalzi R, Bonora E, Consoli A, Giaccari A, Maggi S, et al. Management of diabetes in older adults. Nutr Metab Cardiovasc Dis. (2018) 28(3):206–18. doi: 10.1016/j.numecd.2017.11.007
7. Le Pen C, Bauduceau B, Ansolabehere X, Troubat A, Bineau S, Ripert M, et al. Penetration rates of new pharmaceutical products in Europe: a comparative study of several classes recently launched in type-2 diabetes. Ann Endocrinol. (2021) 82(2):99–106. doi: 10.1016/j.ando.2020.12.009
8. Yimam Ahmed M, Hambisa Ejigu S, Zewudie Zeleke A, Yimam Hassen M. Glycemic control, diabetes complications and their determinants among ambulatory diabetes mellitus patients in Southwest Ethiopia: a prospective cross-sectional study. Diabetes Metab Syndr Obes. (2020) 13:1089–95. doi: 10.2147/DMSO.S227664
9. Billeter AT, Schwarz AC, Rühle A, Boskovic A, Nickel F, Zech U, et al. Indikationsqualität in der Adipositaschirurgie [Quality of indications in bariatric surgery]. Chirurg. (2020) 91(9):727–35. doi: 10.1007/s00104-020-01183-x
10. Altaf A, Abbas MM. Public perception of bariatric surgery. Saudi Med J. (2019) 40(4):379–84. doi: 10.15537/smj.2019.4.24050
11. Mitchell BG, Gupta N. Roux-en-Y Gastric Bypass. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing (2022). p. 1-3. Available at: https://www.ncbi.nlm.nih.gov/books/NBK553157/
12. Guillaud A, Moszkowicz D, Nedelcu M, Caballero-Caballero A, Rebibo L, Reche F, et al. Gastrobronchial fistula: a serious complication of sleeve gastrectomy. Results of a French Multicentric Study. Obes Surg. (2015) 25(12):2352–9. doi: 10.1007/s11695-015-1702-y
13. Nudotor RD, Canner JK, Haut ER, Prokopowicz GP, Steele KE. Comparing remission and recurrence of hypertension after bariatric surgery: vertical sleeve gastrectomy versus Roux-en-Y gastric bypass. Surg Obes Relat Dis. (2021) 17(2):308–18. doi: 10.1016/j.soard.2020.09.035
14. Hofsø D, Fatima F, Borgeraas H, Birkeland KI, Gulseth HL, Hertel JK, et al. Gastric bypass versus sleeve gastrectomy in patients with type 2 diabetes (Oseberg): a single-centre, triple-blind, randomised controlled trial. Lancet Diabetes Endocrinol. (2019) 7(12):912–24. doi: 10.1016/S2213-8587(19)30344-4
15. Kehagias I, Karamanakos SN, Argentou M, Kalfarentzos F. Randomized clinical trial of laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy for the management of patients with BMI < 50 kg/m2. Obes Surg. (2011) 21(11):1650–6. doi: 10.1007/s11695-011-0479-x
16. Keidar A, Hershkop KJ, Marko L, Schweiger C, Hecht L, Bartov N, et al. Roux-en-Y gastric bypass vs sleeve gastrectomy for obese patients with type 2 diabetes: a randomised trial. Diabetologia. (2013) 56(9):1914–18. doi: 10.1007/s00125-013-2965-2
17. Lee WJ, Chen CY, Chong K, Lee YC, Chen SC, Lee SD. Changes in postprandial gut hormones after metabolic surgery: a comparison of gastric bypass and sleeve gastrectomy. Surg Obes Relat Dis. (2011) 7(6):683–90. doi: 10.1016/j.soard.2011.07.009
18. Murphy R, Clarke MG, Evennett NJ, John Robinson S, Lee Humphreys M, Hammodat H, et al. Laparoscopic sleeve gastrectomy versus banded Roux-en-Y gastric bypass for diabetes and obesity: a prospective randomised double-blind trial. Obes Surg. (2018) 28(2):293–302. doi: 10.1007/s11695-017-2872-6
19. Peterli R, Wölnerhanssen BK, Peters T, Vetter D, Kröll D, Borbély Y, et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic Roux-en-Y gastric bypass on weight loss in patients with morbid obesity: the SM-BOSS randomized clinical trial. JAMA. (2018) 319(3):255–65. doi: 10.1001/jama.2017.20897
20. Ruiz-Tovar J, Carbajo MA, Jimenez JM, Castro MJ, Gonzalez G, Ortiz-de-Solorzano J, et al. Long-term follow-up after sleeve gastrectomy versus Roux-en-Y gastric bypass versus one-anastomosis gastric bypass: a prospective randomized comparative study of weight loss and remission of comorbidities. Surg Endosc. (2019) 33(2):401–10. doi: 10.1007/s00464-018-6307-9
21. Salminen P, Helmiö M, Ovaska J, Juuti A, Leivonen M, Peromaa-Haavisto P, et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic Roux-en-Y gastric bypass on weight loss at 5 years among patients with morbid obesity: the SLEEVEPASS randomized clinical trial. JAMA. (2018) 319(3):241–54. doi: 10.1001/jama.2017.20313
22. Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Aminian A, Brethauer SA, et al. Bariatric surgery versus intensive medical therapy for diabetes—5-year outcomes. N Engl J Med. (2017) 376(7):641–51. doi: 10.1056/NEJMoa1600869
23. Tang Q, Sun Z, Zhang N, Xu G, Song P, Xu L, et al. Cost-effectiveness of bariatric surgery for type 2 diabetes mellitus: a randomized controlled trial in China. Medicine. (2016) 95(20):e3522. doi: 10.1097/MD.0000000000003522
24. Wallenius V, Alaraj A, Björnfot N, Orrenius B, Kylebäck A, Björklund P, et al. Sleeve gastrectomy and Roux-en-Y gastric bypass in the treatment of type 2 diabetes. Two-year results from a Swedish multicenter randomized controlled trial. Surg Obes Relat Dis. (2020) 16(8):1035–44. doi: 10.1016/j.soard.2020.04.033
25. Wölnerhanssen BK, Peterli R, Hurme S, Bueter M, Helmiö M, Juuti A, et al. Laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy: 5-year outcomes of merged data from two randomized clinical trials (SLEEVEPASS and SM-BOSS). Br J Surg. (2021) 108(1):49–57. doi: 10.1093/bjs/znaa011
26. Yang J, Wang C, Cao G, Yang W, Yu S, Zhai H, et al. Long-term effects of laparoscopic sleeve gastrectomy versus Roux-en-Y gastric bypass for the treatment of Chinese type 2 diabetes mellitus patients with body mass index 28-35 kg/m (2). BMC Surg. (2015) 15:88. doi: 10.1186/s12893-015-0074-5
27. Zhang Y, Zhao H, Cao Z, Sun X, Zhang C, Cai W, et al. A randomized clinical trial of laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy for the treatment of morbid obesity in China: a 5-year outcome. Obes Surg. (2014) 24(10):1617–24. doi: 10.1007/s11695-014-1258-2
28. Shivakumar S, Tantia O, Goyal G, Chaudhuri T, Khanna S, Ahuja A, et al. LSG vs MGB-OAGB-3 year follow-up data: a randomised control trial. Obes Surg. (2018) 28(9):2820–8. doi: 10.1007/s11695-018-3255-3
29. Navarini D, Madalosso CAS, Tognon AP, Fornari F, Barão FR, Gurski RR. Predictive factors of gastroesophageal reflux disease in bariatric surgery: a controlled trial comparing sleeve gastrectomy with gastric bypass. Obes Surg. (2020) 30(4):1360–7. doi: 10.1007/s11695-019-04286-5
30. Higgins JP, Savovic J, Page MJ, Strene JA. The development group for RoB 2.0. Revised Cochrane risk of bias tool for randomized trials (RoB2.0) (2016). Available from: https://sites.google.com/site/riskofbiastool/wel-come/rob-2-0-tool (Accessed December 18, 2022).
31. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. (2010) 8(5):336–41. doi: 10.1016/j.ijsu.2010.02.007
32. Gu L, Huang X, Li S, Mao D, Shen Z, Khadaroo PA, et al. A meta-analysis of the medium- and long-term effects of laparoscopic sleeve gastrectomy and laparoscopic Roux-en-Y gastric bypass. BMC Surg. (2020) 20(1):30. doi: 10.1186/s12893-020-00695-x
33. Castellana M, Procino F, Biacchi E, Zupo R, Lampignano L, Castellana F, et al. Roux-en-Y gastric bypass vs sleeve gastrectomy for remission of type 2 diabetes. J Clin Endocrinol Metab. (2021) 106(3):922–33. doi: 10.1210/clinem/dgaa737
34. Sharples AJ, Mahawar K. Systematic review and meta-analysis of randomised controlled trials comparing long-term outcomes of Roux-en-Y gastric bypass and sleeve gastrectomy. Obes Surg. (2020) 30(2):664–72. doi: 10.1007/s11695-019-04235-2
35. Nemati R, Lu J, Dokpuang D, Booth M, Plank LD, Murphy R. Increased bile acids and FGF19 after sleeve gastrectomy and Roux-en-Y gastric bypass correlate with improvement in type 2 diabetes in a randomized trial. Obes Surg. (2018) 28(9):2672–86. doi: 10.1007/s11695-018-3216-x
36. Sha Y, Huang X, Ke P, Wang B, Yuan H, Yuan W, et al. Laparoscopic Roux-en-Y gastric bypass versus sleeve gastrectomy for type 2 diabetes mellitus in nonseverely obese patients: a systematic review and meta-analysis of randomized controlled trials. Obes Surg. (2020) 30(5):1660–70. doi: 10.1007/s11695-019-04378-2
37. Lee Y, Doumouras AG, Yu J, Aditya I, Gmora S, Anvari M, et al. Laparoscopic sleeve gastrectomy versus laparoscopic Roux-en-Y gastric bypass: a systematic review and meta-analysis of weight loss, comorbidities, and biochemical outcomes from randomized controlled trials. Ann Surg. (2021) 273(1):66–74. doi: 10.1097/SLA.0000000000003671
38. Huang X, Liu T, Zhong M, Cheng Y, Hu S, Liu S. Predictors of glycemic control after sleeve gastrectomy versus Roux-en-Y gastric bypass: a meta-analysis, meta-regression, and systematic review. Surg Obes Relat Dis. (2018) 14(12):1822–31. doi: 10.1016/j.soard.2018.08.027
39. Zhao H, Jiao L. Comparative analysis for the effect of Roux-en-Y gastric bypass vs sleeve gastrectomy in patients with morbid obesity: evidence from 11 randomized clinical trials (meta-analysis). Int J Surg. (2019) 72:216–23. doi: 10.1016/j.ijsu.2019.11.013
40. Shoar S, Saber AA. Long-term and midterm outcomes of laparoscopic sleeve gastrectomy versus Roux-en-Y gastric bypass: a systematic review and meta-analysis of comparative studies. Surg Obes Relat Dis. (2017) 13(2):170–80. doi: 10.1016/j.soard.2016.08.011
41. Han Y, Jia Y, Wang H, Cao L, Zhao Y. Comparative analysis of weight loss and resolution of comorbidities between laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass: a systematic review and meta-analysis based on 18 studies. Int J Surg. (2020) 76:101–10. doi: 10.1016/j.ijsu.2020.02.035
42. Yang P, Chen B, Xiang S, Lin XF, Luo F, Li W. Long-term outcomes of laparoscopic sleeve gastrectomy versus Roux-en-Y gastric bypass for morbid obesity: results from a meta-analysis of randomized controlled trials. Surg Obes Relat Dis. (2019) 15(4):546–55. doi: 10.1016/j.soard.2019.02.001
43. Li JF, Lai DD, Lin ZH, Jiang TY, Zhang AM, Dai JF. Comparison of the long-term results of Roux-en-Y gastric bypass and sleeve gastrectomy for morbid obesity: a systematic review and meta-analysis of randomized and nonrandomized trials. Surg Laparosc Endosc Percutan Tech. (2014) 24(1):1–11. doi: 10.1097/SLE.0000000000000041
44. Climent E, Goday A, Pedro-Botet J, Solà I, Oliveras A, Ramón JM, et al. Laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy for 5-year hypertension remission in obese patients: a systematic review and meta-analysis. J Hypertens. (2020) 38(2):185–95. doi: 10.1097/HJH.0000000000002255
45. Lee Y, Doumouras AG, Yu J, Aditya I, Gmora S, Anvari M, et al. Laparoscopic sleeve gastrectomy versus laparoscopic Roux-en-Y gastric bypass: a systematic review and meta-analysis of weight loss, comorbidities, and biochemical outcomes from randomized controlled trials. Ann Surg. (2021) 273(1):66–74. doi: 10.1097/SLA.0000000000003671
46. Abu Sneineh M, Abu Sneineh M, Abu Sneineh M, Abu Sneineh M, Abu Sneineh M, Abu Sneineh M. Sleeve gastrectomy is the most common cause of gastroesophageal reflux disease in comparison with other bariatric operations. Dig Dis. (2021) 39(5):462–6. doi: 10.1159/000514377
47. Itani MI, Farha J, Marrache MK, Fayad L, Badurdeen D, Kumbhari V. The effects of bariatric surgery and endoscopic bariatric therapies on GERD: an update. Curr Treat Options Gastroenterol. (2020) 18:97–108. doi: 10.1007/s11938-020-00278-y
48. Nedelcu M, Noel P, Loureiro M, Palermo M, Nedelcu A, Nocca D. Bariatric surgery and the mechanisms of gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A. (2020) 30(8):907–11. doi: 10.1089/lap.2020.0323
49. Langer FB, Bohdjalian A, Shakeri-Leidenmühler S, Schoppmann SF, Zacherl J, Prager G. Conversion from sleeve gastrectomy to Roux-en-Y gastric bypass – indications and outcome. Obes Surg. (2010) 20(7):835–40. doi: 10.1007/s11695-010-0125-z
50. Johnsen EM, Sidhu G, Chen J, Moore R, Le Jemtel T, Samson R. Roux-en-Y gastric bypass and sleeve gastrectomy for obesity-associated hypertension. J Investig Med. (2021) 69(3):730–5. doi: 10.1136/jim-2020-001586
51. Hewitt S, Humerfelt S, Søvik TT, Aasheim ET, Risstad H, Kristinsson J, et al. Long-term improvements in pulmonary function 5 years after bariatric surgery. Obes Surg. (2014) 24(5):705–11. doi: 10.1007/s11695-013-1159-9
52. Chopra A, Chao E, Etkin Y, Merklinger L, Lieb J, Delany H. Laparoscopic sleeve gastrectomy for obesity: can it be considered a definitive procedure? Surg Endosc. (2012) 26(3):831–7. doi: 10.1007/s00464-011-1960-2
53. Hariri K, Kini SU, Herron DM, Fernandez-Ranvier G. Resolution of symptomatic obstructive sleep apnea not impacted by preoperative body mass Index, choice of operation between sleeve gastrectomy and Roux-en-Y gastric bypass surgery, or severity. Obes Surg. (2018) 28(5):1402–7. doi: 10.1007/s11695-017-3042-6
54. Celio AC, Wu Q, Kasten KR, Manwaring ML, Pories WJ, Spaniolas K. Comparative effectiveness of Roux-en-Y gastric bypass and sleeve gastrectomy in super obese patients. Surg Endosc. (2017) 31(1):317–23. doi: 10.1007/s00464-016-4974-y
55. Xu C, Yan T, Liu H, Mao R, Peng Y, Liu Y. Comparative safety and effectiveness of Roux-en-Y gastric bypass and sleeve gastrectomy in obese elder patients: a systematic review and meta-analysis. Obes Surg. (2020) 30(9):3408–16. doi: 10.1007/s11695-020-04577-2
56. Hu Z, Sun J, Li R, Wang Z, Ding H, Zhu T, et al. A comprehensive comparison of LRYGB and LSG in obese patients including the effects on QoL, comorbidities, weight loss, and complications: a systematic review and meta-analysis. Obes Surg. (2020) 30(3):819–27. doi: 10.1007/s11695-019-04306-4
57. Zhao K, Liu J, Wang M, Yang H, Wu A. Safety and efficacy of laparoscopic sleeve gastrectomy versus laparoscopic Roux-en-Y gastric bypass: a systematic review and meta-analysis. J Eval Clin Pract. (2020) 26(1):290–8. doi: 10.1111/jep.13170
58. Gu L, Fu R, Chen P, Du N, Chen S, Mao D, et al. In terms of nutrition, the most suitable method for bariatric surgery: laparoscopic sleeve gastrectomy or Roux-en-Y gastric bypass? A systematic review and meta-analysis. Obes Surg. (2020) 30(5):2003–14. doi: 10.1007/s11695-020-04488-2
59. Gu L, Zafar SN, Shockcor N, Prasad N, Wise ES, Jackson HT, et al. Laparoscopic sleeve gastrectomy has a lower risk of postoperative bleeding than laparoscopic Roux-en-Y gastric bypass. Surg Laparosc Endosc Percutan Tech. (2019) 29(1):53–7. doi: 10.1097/SLE.0000000000000598
60. Chen B, Du N, Fu R, Huang X, Mao F, Khadaroo PA, et al. Relationship between bariatric surgery and gastroesophageal reflux disease: a systematic review and meta-analysis. Obes Surg. (2019) 29(12):4105–13. doi: 10.1007/s11695-019-04218-3
61. Shenoy SS, Gilliam A, Mehanna A, Kanakala V, Bussa G, Gill T, et al. Laparoscopic sleeve gastrectomy versus laparoscopic Roux-en-Y gastric bypass in elderly bariatric patients: safety and efficacy – a systematic review and meta-analysis. Obes Surg. (2020) 30(11):4467–73. doi: 10.1007/s11695-020-04819-3
62. Han Y, Jia Y, Wang H, Cao L, Zhao Y. Comparative analysis of weight loss and resolution of comorbidities between laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass: a systematic review and meta-analysis based on 18 studies. Int J Surg. (2020) 76:101–10. doi: 10.1016/j.ijsu.2020.02.035
63. Guraya SY, Strate T. Effectiveness of laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy for morbid obesity in achieving weight loss outcomes. Int J Surg. (2019) 70:35–43. doi: 10.1016/j.ijsu.2019.08.010
64. Gu L, Lin K, Du N, Ng DM, Lou D, Chen P. Differences in the effects of laparoscopic sleeve gastrectomy and laparoscopic Roux-en-Y gastric bypass on gut hormones: systematic and meta-analysis. Surg Obes Relat Dis. (2021) 17(2):444–55. doi: 10.1016/j.soard.2020.10.018
65. Arakawa R, Febres G, Cheng B, Krikhely A, Bessler M, Korner J. Prospective study of gut hormone and metabolic changes after laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass. PLoS ONE. (2020) 15(7):e0236133. doi: 10.1371/journal.pone.0236133
66. Ramón JM, Salvans S, Crous X, Puig S, Goday A, Benaiges D, et al. Effect of Roux-en-Y gastric bypass vs sleeve gastrectomy on glucose and gut hormones: a prospective randomised trial. J Gastrointest Surg. (2012) 16(6):1116–22. doi: 10.1007/s11605-012-1855-0
67. Xu G, Song M. Recent advances in the mechanisms underlying the beneficial effects of bariatric and metabolic surgery. Surg Obes Relat Dis. (2021) 17(1):231–8. doi: 10.1016/j.soard.2020.08.028
Keywords: Roux-en Y gastric bypass, laparoscopic sleeve gastrectomy, obesity-related comorbidities, obesity, comorbidities
Citation: Alghamdi S, Mirghani H, Alhazmi K, Alatawi AM, Brnawi H, Alrasheed T and Badoghaish W (2022) Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy effects on obesity comorbidities: A systematic review and meta-analysis. Front. Surg. 9:953804. doi: 10.3389/fsurg.2022.953804
Received: 26 May 2022; Accepted: 17 October 2022;
Published: 2 December 2022.
Edited by:
Pradeep Chowbey, Max Healthcare, IndiaReviewed by:
Salman Yousuf Guraya, College of Medicine University of Sharjah, United Arab EmiratesMahdieh Golzarand, Shahid Beheshti University of Medical Sciences, Iran
© 2022 Alghamdi, Mirghani, Alhazmi, Alatawi, Brnawi, Alrasheed and Badoghaish. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hyder Mirghani cy5oeWRlcjYzQGhvdG1haWwuY29t
Specialty Section: This article was submitted to Visceral Surgery, a section of the journal Frontiers in Surgery
Abbreviations GERD, gastroesophageal reflux disease; LRYGB, Roux-en-Y gastric bypass; LSG, laparoscopic sleeve gastrectomy; OSA, obstructive sleep apnea.