 Bjørn Hofmann1,2*
Bjørn Hofmann1,2*
- 1Centre of Medical Ethics, The University of Oslo, Oslo, Norway
- 2Institute of the Health Sciences, The Norwegian University of Science and Technology (NTNU), Gjøvik, Norway
Introduction
Surgery is impelled by triumphs and trailed by tragedies (1–5). While the triumphs are manifold, the tragedies have traditionally come in two kinds: harms and lack of benefits. Harms from surgery are well documented (6). So are treatments without benefit (7, 8). A recent review identified more than seventy general low-value surgical procedures where five high-volume, high-cost general surgical procedures alone could save the National Health Service more than €100 million yearly (9).
Lack of benefits and harms of surgery affect individuals, public health, and the standing of surgeons (10–12). However, a third type of challenge is pressing: surgery beyond bodily benefit, e.g., surgery with mental and social goals: cutting in bodies to improve self-esteem and social identity, i.e., “soul surgery” and “social surgery.”
Clearly, in surgery, as in medicine in general, there has been a move from targeting surrogate endpoints to hard endpoints, such as survival, morbidity, and functional status, and especially towards quality of life. Additionally, patient-reported outcome measures (PROMs) have received increased attention in surgery (13–17) as elsewhere. Hence surgery increasingly serves what matters to people.
The general move in the assessments of benefits of surgery from medical measures towards patient-centred measures calls for reflection, especially when the goals of surgery go beyond the body that is operated on. In particular, when the goals of surgery are mental (self-esteem) or social (recognition), it is crucial to reflect on the ethos of surgery. Moving the primary goals of surgery away from the site of incision may foster tragedies and hamper triumphs in the future. We therefore need to pay special attention to surgical goals that go beyond the body that is operated on, i.e., what can be called “soul surgery” and “social surgery.”
Soul surgery
Soul surgery can be defined as surgery of the body to obtain primarily mental outcomes. Historically, there has been a strong belief in brain surgery to treat mental illnesses (“psychosurgery”). However, even when one believed that there was a clear connection between the site of incision and the mental effect, the outcomes were often poor or even devastating (18–20). More recently, surgery is used indirectly to influence people's mental health (21). No parts of the body are untouched by the scalpel to improve people's appearance and self-esteem. Female genital cosmetic surgery is but one example (22, 23).
There are several problems with “soul surgery.” First, it can be difficult to provide high-quality evidence for the mental outcomes of surgery (24–27). Second, sculpting bodies according to the current aesthetical ideals supports and spreads the norms (the “new normal”) that may cause the mental problems in the first place. Third, while surgery for self-esteem and other mental states may be good for individuals and employment of cosmetic surgeons, it may not be good for public health and social norms in general. Fourth, soul surgery may only target the symptoms and not the causes, diverting attention and resources from more effective approaches. Fifth, many types of soul surgery may cross the line between therapy and enhancement (28), e.g., when moving from reconstruction to construction. Sixth, it can be difficult to set the limits to soul surgery, e.g., when autonomous persons request to remove well-functioning organs or limbs (29). Last but not least, soul surgery can imply substantial harms, including harms well beyond the body.
In other words, when the outcome measures of surgery are remote to the operating site, benefits and harms must be assessed in a different (mental) realm, which demands special attention, competence, and care.
In addition to the intended mental effects of surgery, surgery also can have social goals – as they are closely interconnected.
Social surgery
Corresponding to soul surgery, social surgery is defined as surgery of the body to obtain primarily social outcomes. Clearly surgery has implications beyond its biomedical outcomes. For example, a hip replacement or the reconstruction of a severely injured face influences the social life of the person. However, the challenges occur when incisions are made primarily to obtain social changes. Lobotomy was used to alter social behaviour and compulsory sterilization to prohibit reproduction. Genital modification (for religious, social, or cultural reasons) and surgery to confirm social constructs, such as gender identity, are other and more topical examples.
While this certainly illustrates the wide-reaching power of surgery and the intimate interconnection between the body, mind, and the social, it also challenges the traditional conception of surgery as a concrete physical biomedical discipline with traditional goals of curing, restoring biomedical function, and avoiding or reducing physical pain. Again, many of the same problems as with soul surgery emerge and demands competency and care – as well as delimiting definition of the discipline.
Beyond bodily benefit
Clearly, the power of surgery reaches well beyond the bodies that are operated on. Bodily health affects mental wellbeing and social functioning. Curing cancer gives psychological and existential relief and makes it possible to function socially. Surgery therefore has beneficial mental and social (side) effects that should be fully appreciated. However, problems occur when mental and social effects become the primary outcome of cutting in bodies – and when the effects are remotely connected to the corporal intervention.
Goals beyond the body
The trend of expanding the subject matter of surgery from the physical body to mental and social phenomena provides new opportunities to help people, but it also extends surgery's goals, outcome measures, and responsibility. This urges surgeons to familiarize with new phenomena, learn different aetiologies, acquire new competencies, decide on different endpoints, set new limits, and take on new duties and responsibilities. There is nothing wrong with changing or expanding ones goals, but it may warrant special care as it involves professional values, social norms, and alters the ethos of the profession (30).
Therefore, cutting in the bodies of mental and social beings certainly has mental and social effects – effects that we should be aware of and appreciate. However, mental norms and social values change over time. Their relationship with the bodies is indirect and contingent. What is considered to be a good mental or social effect today may not be so tomorrow. Self-esteem and social functioning depend on more than bodily appearance. Therefore, soul surgery and social surgery require skills of elusive norms and values. Table 1 provides an overview of some crucial issues, examples, and aspects to take into consideration when doing soul surgery and social surgery.
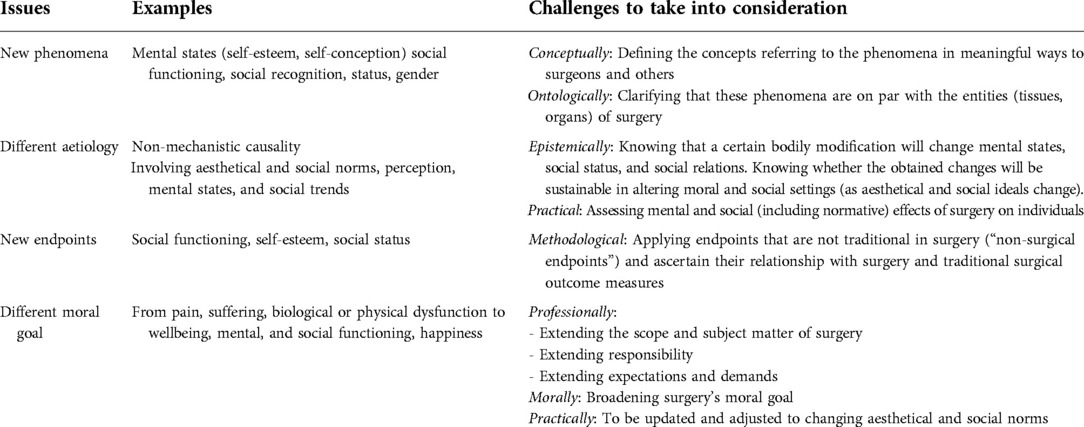
Table 1. Examples of issues and challenges to take into consideration when doing soul surgery and social surgery
Forming mental phenomena and social constructs by surgically shaping physical bodies disrupts traditional categories and transgresses basic boundaries. Moving the primary goals of surgery away from the site of incision, warrants critical reflection and is crucial to avoid tragedies and promote triumphs in the future of surgery.
Author contributions
Hofmann confirms that he is the only author of this manuscript and has written all parts of the article. He has also approved the submitted version.
Acknowledgments
I am most thankful to Kari Milch Agledahl for comments on an initial draft of the manuscript.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Clarke W. The triumphs of medicine and surgery. In: Whittemore WM, editor. Golden Hours: a Monthly Magazine for Family and General Reading. London: Passmore & Alabaster (1871). p. 127–33.
2. Lawrence C. Democratic, divine and heroic: The history and historiography of surgery. In: Lawrence C, editor. Medical theory, surgical practice. London, New York: Routledge (2018). p. 1–47.
3. Wootton D. Bad medicine: Doctors doing harm since hippocrates. Oxford: Oxford University Press (2007).
4. Porter R. The greatest benefit to mankind: a medical history of humanity (the norton history of science). New York: WW Norton & Company (1999).
5. Lawrence G. The ambiguous artifact: surgical instruments and the surgical past. In: Lawrence C, editor. Medical theory, surgical practice. London, New York: Routledge (2018). p. 295–314.
6. Anderson O, Davis R, Hanna GB, Vincent CA. Surgical adverse events: a systematic review. Am J Surg. (2013) 206(2):253–62. doi: 10.1016/j.amjsurg.2012.11.009
7. Dwyer-Hemmings L. ‘A wicked operation’? Tonsillectomy in twentieth-century britain. Med Hist. (2018) 62(2):217–41. doi: 10.1017/mdh.2018.5
8. Siemieniuk RA, Harris IA, Agoritsas T, Poolman RW, Brignardello-Petersen R, Van de Velde S, et al. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. BMJ. (2017) 357:357. doi: 10.1136/bmj.j1982
9. Malik H, Marti J, Darzi A, Mossialos E. Savings from reducing low-value general surgical interventions. J Br Surg. (2018) 105(1):13–25. doi: 10.1002/bjs.10719
10. Pearse RM, Moreno RP, Bauer P, Pelosi P, Metnitz P, Spies C, et al. Mortality after surgery in Europe: a 7 day cohort study. Lancet. (2012) 380(9847):1059–65. doi: 10.1016/S0140-6736(12)61148-9
11. Marsh KM, Fleming MA, Turrentine FE, Levin DE, Gander JW, Keim-Malpass J, et al. Pediatric surgical errors: a systematic scoping review. J Pediatr Surg. (2021) 57(4):616–621. doi: 10.1016/j.jpedsurg.2021.07.019.34366133
12. Donaldson MS, Corrigan JM, Kohn LT. To err is human: Building a safer health system. Washington, DC: National Academies Press (2000).
13. Sharma K, Steele K, Birks M, Jones G, Miller G. Patient-reported outcome measures in plastic surgery: an introduction and review of clinical applications. Ann Plast Surg. (2019) 83(3):247–52. doi: 10.1097/SAP.0000000000001894
14. Ramkumar P, Harris JD, Noble P. Patient-reported outcome measures after total knee arthroplasty: a systematic review. Bone Joint Res. (2015) 4(7):120–7. doi: 10.1302/2046-3758.47.2000380
15. Shamsunder MG, Chu JJ, Polanco TO, Yin S, Muniz RC, James MC, et al. The impact of psychiatric diagnoses on patient-reported satisfaction and quality of life in post-mastectomy breast reconstruction. Ann Surg. (2022). doi: 10.1097/SLA.0000000000005478. Epub ahead of print.35793069
16. Ottenhof MJ, Veldhuizen IJ, Hensbergen LJV, Blankensteijn LL, Bramer W, Hoogbergen MM, et al. The use of the FACE-Q aesthetic: a narrative review. Aesthetic Plast Surg. (2022):1–12. doi: 10.1007/s00266-022-02974-9. Epub ahead of print.
17. Black N, Varaganum M, Hutchings A. Relationship between patient reported experience (PREMs) and patient reported outcomes (PROMs) in elective surgery. BMJ Qual Saf. (2014) 23(7):534–42. doi: 10.1136/bmjqs-2013-002707
18. Sachdev P, Sachdev J. Sixty years of psychosurgery: its present status and its future. Aust N Z J Psychiatry. (1997) 31(4):457–64. doi: 10.3109/00048679709065065
19. Valenstein ES. Great and desperate cures: The rise and decline of psychosurgery and other radical treatments for mental illness. New York: Basic Books (1986).
21. Chappell AG, Kane RL, Wood SM, Wescott AB, Chung KC. Representation of ethics in the plastic surgery literature: a systematic review. Plast Reconstr Surg. (2021) 148(2):289e–98e. doi: 10.1097/PRS.0000000000008232
22. Gaffney-Rhys R. Female genital cosmetic surgery: legitimate refinement or illegal mutilation? Eur J Health Law. (2021) 28(3):244–62. doi: 10.1163/15718093-BJA10046
23. Kelly B, Foster C. Should female genital cosmetic surgery and genital piercing be regarded ethically and legally as female genital mutilation? BJOG BJOG-Int J Obstet Gy. (2012) 119(4):389–92. doi: 10.1111/j.1471-0528.2011.03260.x
24. Cook SA, Rosser R, Salmon P. Is cosmetic surgery an effective psychotherapeutic intervention? A systematic review of the evidence. J Plast Reconstr Aesthet Surg. (2006) 59(11):1133–51. doi: 10.1016/j.bjps.2006.03.047
25. Dreher R, Blaya C, Tenório JLC, Saltz R, Ely PB, Ferrão YA. Quality of life and aesthetic plastic surgery: a systematic review and meta-analysis. Plast Reconstr Surg Glob Open. (2016) 4(9):e862. doi: 10.1097/GOX.0000000000000833
26. Imadojemu S, Sarwer DB, Percec I, Sonnad SS, Goldsack JE, Berman M, et al. Influence of surgical and minimally invasive facial cosmetic procedures on psychosocial outcomes: a systematic review. JAMA Dermatol. (2013) 149(11):1325–33. doi: 10.1001/jamadermatol.2013.6812
27. Margraf J, Meyer AH, Lavallee KL. Well-being from the knife? Psychological effects of aesthetic surgery. Clin Psychol Sci. (2013) 1(3):239–52. doi: 10.1177/2167702612471660
28. Parens E. Enhancing human traits: Ethical and social implications. Washington, DC: Georgetown University Press (2000).
Keywords: outcomes, mental, social, ethics, goal, aesthetics, gender
Citation: Hofmann B (2022) Surgery beyond bodies: Soul surgery and social surgery. Front. Surg. 9:950172. doi: 10.3389/fsurg.2022.950172
Received: 22 May 2022; Accepted: 16 August 2022;
Published: 7 September 2022.
Edited by:
Ilyas Khan, Swansea University Medical School, United KingdomReviewed by:
Bassey Enodien, GZO Spital Wetzikon, Switzerland© 2022 Hofmann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bjørn Hofmann YmpvZXJuLmhvZm1hbm5AbnRudS5ubw==; Yi5tLmhvZm1hbm5AbWVkaXNpbi51aW8ubm8=
Specialty Section: This article was submitted to Reconstructive and Plastic Surgery, a section of the journal Frontiers in Surgery