
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 02 August 2022
Sec. Otorhinolaryngology - Head and Neck Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.940391
 Jun Sung Lee1
Jun Sung Lee1 Hee Jun Kim2Jin Seok Lee1
Hee Jun Kim2Jin Seok Lee1 Hyeok Jun Yun1Suji Lee3Jae-Ho Cheong3Soo Young Kim4
Hyeok Jun Yun1Suji Lee3Jae-Ho Cheong3Soo Young Kim4 Seok-Mo Kim1*Hojin Chang1Yong Sang Lee1Cheong Soo Park2
Seok-Mo Kim1*Hojin Chang1Yong Sang Lee1Cheong Soo Park2 Hang-Seok Chang1
Hang-Seok Chang1
Background: With the recent advances in thyroid cancer surgery techniques and the increasing number of patients concerned about cosmetics, the use of transoral endoscopic thyroidectomy is increasing globally. The aim of this study was to determine whether transoral endoscopic thyroidectomy is truly a clean-contaminated surgery.
Methods: From September 2016 to April 2018, 20 patients with thyroid cancer underwent transoral endoscopic thyroidectomy performed by a single surgeon at Gangnam Severance Hospital. Before and after surgery, the oral cavity was swabbed to obtain culture samples, and antibiotics were administered before and after surgery each once.
Results: Of the total 20 patients, no bacteria were identified before or after surgery in eight (40%) patients. Bacteria were identified both before and after surgery in seven patients (35%). In four patients (20%), bacteria were not identified before surgery, but bacteria were identified after surgery. Bacteria were identified before surgery but not after surgery in one patient (5%). No surgical site infection was observed. All the bacteria identified were normal flora of the oral cavity and skin.
Conclusions: There was no difference between the preoperative culture and postoperative culture of the oral cavity in patients undergoing TOET, and there were no postoperative surgical site infection with prophylactic pre & post-operative antibiotics use. Considering the patient's position and surgical extent in TOET, it appears to be difficult for non-indigenous bacteria to invade the surgical site in oral cavity.
With the recent development in thyroid cancer surgery and the increasing number of patients concern about cosmetics, the use of transoral endoscopic thyroidectomy (TOET) is spreading globally (1, 2). After the first reports of TOET in 2008 (3), it has become one of the option of surgical treatment for papillary thyroid cancer (PTC).
The TOET approach is considered clean-contaminated surgery because the access through the oral cavity can transfer oral flora into the thyroid space and may increase the risk of surgical site infection (4). At the Gangnam Severance Hospital, we use one dose of flomoxef 1 g preoperatively and one dose of flomoxef 1 g postoperatively as a prophylactic antibiotic. The use of prophylactic antibiotics remains controversial and there are no standard guidelines for the use of antibiotics in TOET (5–8). The aim of this study was to determine whether or not antibiotics are required before and after surgery.
From October to December 2019, 20 patients who underwent TOET due to PTC were enrolled in this study. All surgeries were performed by a single surgeon at Gangnam Severance Hospital. Before and after surgery, the oral cavity was swabbed to for testing of bacteria culture, and flomoxef 1 g was administered once before surgery and once after surgery.
Figures 1, 2 show the swabbing procedure for obtaining the preoperative and postoperative culture at the incision site in the oral cavity. We irrigated oral cavity twice with 50 cc 1:1 saline with providone iodine after endotracheal induction. We used a culture tube including two cotton swabs for obtaining the specimens at the incision site. Swabbing was performed by the operator and first assistant once before surgery and once after surgery. The preoperative culture sample was obtained immediately before the incision was made, and the postoperative culture sample was obtained after the patient was delivered from the operating table and the bleeding was controlled.
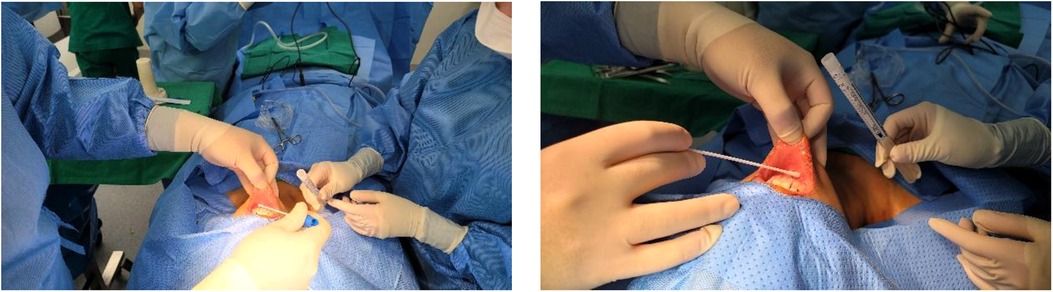
Figure 1. Preoperative culture.
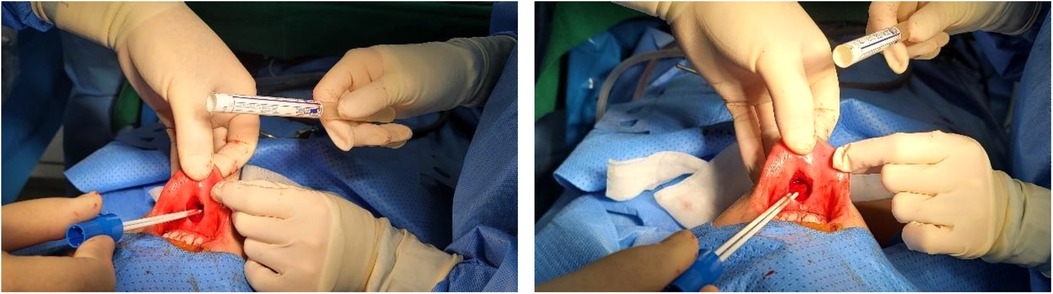
Figure 2. Postoperative culture.
The Institutional Review Board of Gangnam Severance Hospital, Yonsei University College of Medicine (Seoul, Korea) approved this study (approval number: 3-2017-0085).
From October 23, 2019 to December 17, 2019, 20 patients who underwent TOET surgery were enrolled. The patients' characteristics are summarized in Table 1. Nineteen patients were women, and the sex ratio was 19:1. The average BMI was 20.80 ± 3.558 kg/m2. Most patients had no medical history, except one patient who had hypertension, two patients who had hyperthyroidism, and one patient who had depression. Two patients underwent total bilateral thyroidectomy, and 18 patients underwent less than total bilateral thyroidectomy. Only one case involved multiplicity, and it was bilateral case. TOET is difficult to perform when there is severe invasion of cancer into adjacent tissue or a necessity for radical lymph node (LN) dissection, and it is impossible to perform modified radical neck dissection using a transoral incision. Given these reasons, the disease stage of all patients who participated in this study was Stage I. Central compartment LN dissection (CCND) was performed in all of cases, and the number of lymph node of CND was 3.8 ± 2.375. A BRAF mutation was identified in two patients.

Table 1. Patient characteristics.
The preoperative and postoperative bacteria culture results are presented in Table 2. Bacteria was detected in eight patients in the preoperative culture, and in 11 patients in the postoperative culture. In seven patients, bacteria were detected in both the preoperative and postoperative culture. In eight patients, there was no bacteria detected neither pre-operatively or postoperatively. Culture was positive in the postoperative culture but not in the preoperative culture in four patients, and there was only one patient with positive postoperative culture and negative preoperative culture. There were no postoperative surgical site infection observed in this study.
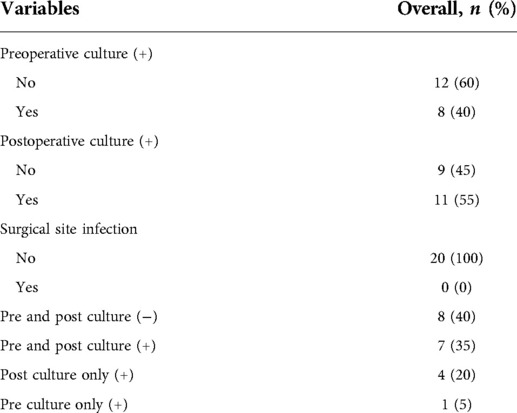
Table 2. Preoperative and postoperative culture results.
Table 3 shows the detail of preoperative and postoperative bacteria culture. In preoperative cultures, there were eight positive culture results in 20 patients. Most of the preoperative cultures detected were gram-positive cocci. α-streptococcus was detected in five cultures, and Streptococcus sanguinis and Staphylococcus epidermidis grew in one and two preoperative cultures, respectively. Gram-positive bacilli (diphtheroids) and anaerobic gram-positive bacilli (Propionibacterium acnes) were also detected in one patient each. Eleven postoperative cultures were positive. Similar to the preoperative cultures, the majority of positive results were gram-positive coccus. α-streptococcus, Staphylococcus epidermidis, and Streptococcus sanguinis were detected in four, three, and three cultures, respectively. Anaerobic gram-positive bacilli were also detected in three cultures. No gram-negative bacteria were detected in any cultures.
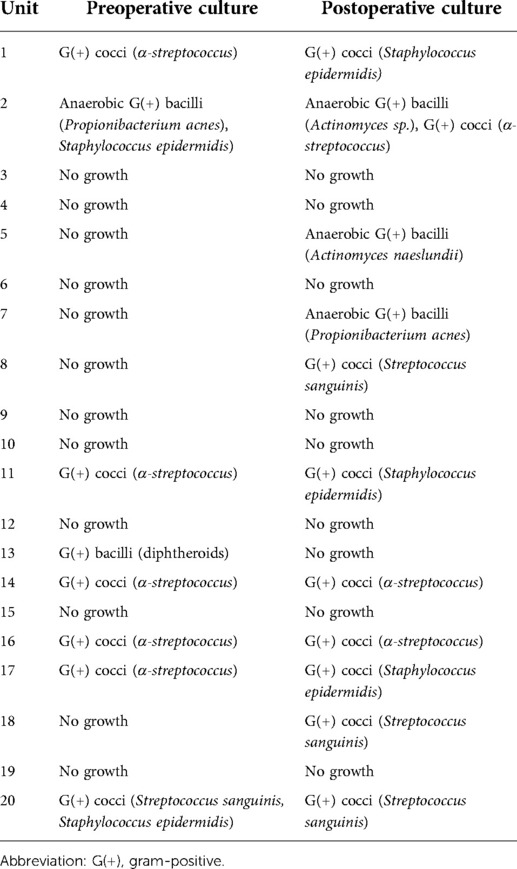
Table 3. Details of preoperative and postoperative bacteria culture.
TOET surgery was first reported in 2008 and first performed on cadavers and pigs (3). Since then, it has become a significant choice for patients who regard cosmetic appearance to be important. It results in no skin scarring and requires only a relatively small skin flap in the gingival mucosa. In conventional open thyroidectomy, there is no need for prophylactic antibiotics usage to prevent surgical site infection because the thyroidectomy wound that occurs as a result of the use of an anterior neck approach is a clean wound (9). However, in TOET surgery, the oral cavity is the incision site and this is considered part of the alimentary tract, so the TOET wound is not considered a clean wound, but a clean-contaminated wound (4, 10). Currently, prophylactic antibiotics in TOET are controversial and the prophylactic antibiotics usage for TOET is different depending on medical centers. Usually antibiotics used for 7 days routinely (6, 8), but there have been several literature to have a trial about reducing the amounts of prophylactic antibiotics or not using antibiotics before and after surgery (5, 7). At the Gangnam Severance Hospital, we use flomoxef, a type of third generation cephalosporin, as a prophylactic antibiotic.
In this study, we planned to check preoperative and postoperative surgical site bacteria culture and postoperative surgical site infection. Through analysis of the collected cultures, we aimed to determine if prophylactic antibiotics usage is essential in TOET, and what was the main infection source if surgical site infection occurred. Specimens for bacteria culture were collected twice, once before the incision was made at the gingival mucosa, and once before the incision site was closed. After the surgery, no drain was inserted at the surgical site. Flomoxef 1 g was used preoperatively and postoperatively each once as a prophylactic antibiotic.
The results showed that there was no difference between the preoperative and postoperative culture. In addition, all bacteria detected were normal flora of the oral cavity, and no non-indigenous flora were detected in the oral cavity of any of the patients. There were no postoperative complications, so it was impossible to determine the infection source of any surgical site infections.
These results may indicate that the normal flora function as a barrier (11). The normal bacterial flora of the oral cavity clearly benefit from their host who provides nutrients and habitat. There may also be benefits to the host. The normal flora occupy available colonization sites and this makes it more difficult for non-indigenous species to live in the oral cavity. Moreover, the oral cavity flora also create microbial antagonism against non-indigenous species by production of inhibitory substances such as fatty acids, peroxides, and bacteriocins (12).
The study results show that it is difficult for potential pathogens, such as non-resident bacterial flora, to invade the surgical site of TOET. In this regard, the TOET would have a possibility as a surgery that don't need prophylactic antibiotics because there was no invasion of non-resident bacterial flora but just a normal flora of oral cavity. If further studies are conducted on transoral surgery that is performed without about prophylactic antibiotics, this may lead to less demand for antibiotics for TOET.
There were some limitations in this study. First, the number of patients enrolled in this study was relatively small, thereby reducing the statistical strength of the results. This study can be a preliminary data for the possibility of non-antibiotics need in TOET, but can't play a role as solid evidence because of limitation of the study. Second, the study was retrospective in design which may indicate the presence of selection bias. In addition, antibiotics were used in every patient in this study, so we did not investigate of the rates of surgical site infection when prophylactic antibiotics were not used.
In conclusion, there was no difference between the preoperative culture and postoperative culture of the oral cavity in patients undergoing TOET, and there were no postoperative surgical site infection with prophylactic pre & post-operative antibiotics use. Considering the patient's position and surgical extent in TOET, it appears to be difficult for non-indigenous bacteria to invade the surgical site in oral cavity.
The original contributions presented in the study are included in the article/Suplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by The Institutional Review Board of Gangnam Severance Hospital, Yonsei University College of Medicine (Seoul, Korea). The patients/participants provided their written informed consent to participate in this study.
Study concept and design: S-MK. Acquisition, analysis, or interpretation of data: JSL, HJK. Drafting of the manuscript: JSL, HJK, HJY, S-MK. Statistical analysis: JSL, HJK. All authors contributed to the article and approved the submitted version.
We thank the team of the Gangnam Severance Thyroid Cancer Center for their contribution to writing and preparing this manuscript for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Yap RV, Villamor M Jr. Scarless total thyroidectomy via transoral endoscopic vestibular approach: initial case series in a developing Asian country. J Surg Case Rep. (2022) 2022(1):rjab623. doi: 10.1093/jscr/rjab623
2. Yi JW, Yoon SG, Kim HS, Yu HW, Kim SJ, Chai YJ, et al. Transoral endoscopic surgery for papillary thyroid carcinoma: initial experiences of a single surgeon in South Korea. Ann Surg Treat Res. (2018) 95(2):73–9. doi: 10.4174/astr.2018.95.2.73
3. Witzel K, von Rahden BH, Kaminski C, Stein HJ. Transoral access for endoscopic thyroid resection. Surg Endosc. (2008) 22(8):1871–5. doi: 10.1007/s00464-007-9734-6
4. Leaper DJ, Edmiston CE. World Health Organization: global guidelines for the prevention of surgical site infection. J Hosp Infect. (2017) 95(2):135–6. doi: 10.1016/j.jhin.2016.12.016
5. Yi JW, Kim SJ, Lee KE. Evaluation of the efficacy of postoperative antibiotic treatment in transoral endoscopic thyroidectomy: a prospective randomised controlled trial. Br J Oral Maxillofac Surg. (2020) 58(3):334–40. doi: 10.1016/j.bjoms.2020.01.004
6. Zhang D, Park D, Sun H, Anuwong A, Tufano R, Kim HY, et al. Indications, benefits and risks of transoral thyroidectomy. Best Pract Res Clin Endocrinol Metab. (2019) 33(4):101280. doi: 10.1016/j.beem.2019.05.004
7. Karakas E, Klein G, Michlmayr L, Schardey M, Schopf S, Endoscopic T, et al. Transoral thyroid surgery vestibular approach: is there an increased risk of surgical site infections? Updates Surg. (2022) 74(1):303–8. doi: 10.1007/s13304-021-01191-4
8. Anuwong A. Transoral endoscopic thyroidectomy vestibular approach: a series of the first 60 human cases. World J Surg. (2016) 40(3):491–7. doi: 10.1007/s00268-015-3320-1
9. Polistena A, Prete FP, Avenia S, Cavallaro G, Di Meo G, Pasculli A, et al. Effect of antibiotic prophylaxis on surgical site infection in thyroid and parathyroid surgery: a systematic review and meta-analysis. Antibiotics (Basel). (2022) 11(3):290. doi: 10.3390/antibiotics11030290
10. Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. CDC Definitions of nosocomial surgical site infections, 1992: a modification of CDC definitions of surgical wound infections. Infect Control Hosp Epidemiol. (1992) 13(10):606–8. doi: 10.2307/30148464
Keywords: thyroid cancer, transoral thyroidectomy, culture, antibiotics, surgical site infection
Citation: Lee JS, Kim HJ, Lee JS, Yun HJ, Lee S, Cheong J, Kim SY, Kim S, Chang H, Lee YS, Park CS and Chang H (2022) Prophylactic antibiotics may not be necessary for transoral endoscopic thyroidectomy. Front. Surg. 9:940391. doi: 10.3389/fsurg.2022.940391
Received: 10 May 2022; Accepted: 8 July 2022;
Published: 2 August 2022.
Edited by:
Mahesh C. Misra, All India Institute of Medical Sciences, IndiaReviewed by:
Anurag Srivastava, National Institute of Cancer Prevention and Research (ICMR), India© 2022 Lee, Kim, Lee, Yun, Lee, Cheong, Kim, Kim, Chang, Lee, Park and Chang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Seok-mo Kim c2Vva21va2ltQHl1aHMuYWM=
Specialty Section: This article was submitted to Otorhinolaryngology—Head and Neck Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.