 Dawei Wang
Dawei Wang Xue Chen
Xue Chen Pei Deng
Pei Deng- Department of Plastic and Cosmetic Surgery, Tongji Hospital of Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China
Background: Microtia is a congenital abnormality varying from slightly structural abnormalities to the complete absence of the external ear. However, there is no gold standard for assessing the severity of microtia.
Objectives: The purpose of this study was to develop and test models of artificial intelligence to assess the severity of microtia using clinical photographs.
Methods: A total of 800 ear images were included, and randomly divided into training, validation, and test set. Nine convolutional neural networks (CNNs) were trained for classifying the severity of microtia. The evaluation metrics, including accuracy, precision, recall, F1 score, receiver operating characteristic curve, and area under the curve (AUC) values, were used to evaluate the performance of the models.
Results: Eight CNNs were tested with accuracy greater than 0.8. Among them, Alexnet and Mobilenet achieved the highest accuracy of 0.9. Except for Mnasnet, all CNNs achieved high AUC values higher than 0.9 for each grade of microtia. In most CNNs, the grade I microtia had the lowest AUC values and the normal ear had the highest AUC values.
Conclusion: CNN can classify the severity of microtia with high accuracy. Artificial intelligence is expected to provide an objective, automated assessment of the severity of microtia.
Introduction
Microtia is a congenital abnormality with an estimated incidence of 0.83–17.4 per 10,000 births (1). Microtia generally presents as auricle malformation, varying from slight structural abnormalities to complete absence of the external ear (2). Moreover, congenital aural atresia or stenosis usually occurs together with microtia. Surgical auricular reconstruction using autologous costal cartilage has been widely performed since it was first reported by Tanzer (3). Then, the two-stage reconstruction procedure was developed by Brent (4) and Nagata (5). Nevertheless, auricular reconstruction remains one of the most complex and challenging procedures for plastic surgeons.
The severity of microtia can influence the surgical procedures and postoperative outcome of auricular reconstruction. To date, various classifications have been introduced for assessing the severity of microtia by Marx, Lapchenko, Gill, Rogers, Tanzer, Jahrsdoerfer, and Tasse et al. (6). However, these classification methods all rely on subjective assessment of auricular malformation, and no reliable objective method has been proposed to assess the severity of microtia. An objective diagnostic tool will provide a standardized, repeatable assessment of the severity of microtia, avoiding inconsistency between providers.
Artificial intelligence has been increasingly applied in various fields of medicine, particularly in the detection of skin diseases (7), breast cancer (8), oral cancer (9), and diabetic retinopathy (10). Convolutional neural networks (CNNs), as the most essential algorithms for deep learning, facilitate the development of artificial intelligence in image recognition, classification, and detection. In the field of plastic surgery, several studies have explored the effectiveness of CNN models in assessing the severity of unilateral cleft lip (11) and evaluating age reduction after face-lift (12). Due to the complex shape and composition of the ear, it is difficult to develop mathematical models to identify deformities in the ear. Previous studies have developed CNN models to identify ear abnormalities from two-dimensional photographs with satisfactory results (13–15). To our knowledge, no CNN model has been reported to evaluate the severity of microtia, for the reported models only distinguished between normal ears and malformed ears.
Thus, we hypothesized that CNN models have the potential to accurately classify the severity of microtia using two-dimensional photographs. In this study, we trained nine CNN models and evaluated their performance in assessing the severity of microtia using clinical photographs. The design of this study was illustrated in Figure 1. This study aimed to recommend better CNNs from the tested networks for clinical application, which would facilitate the objective classification of microtia.
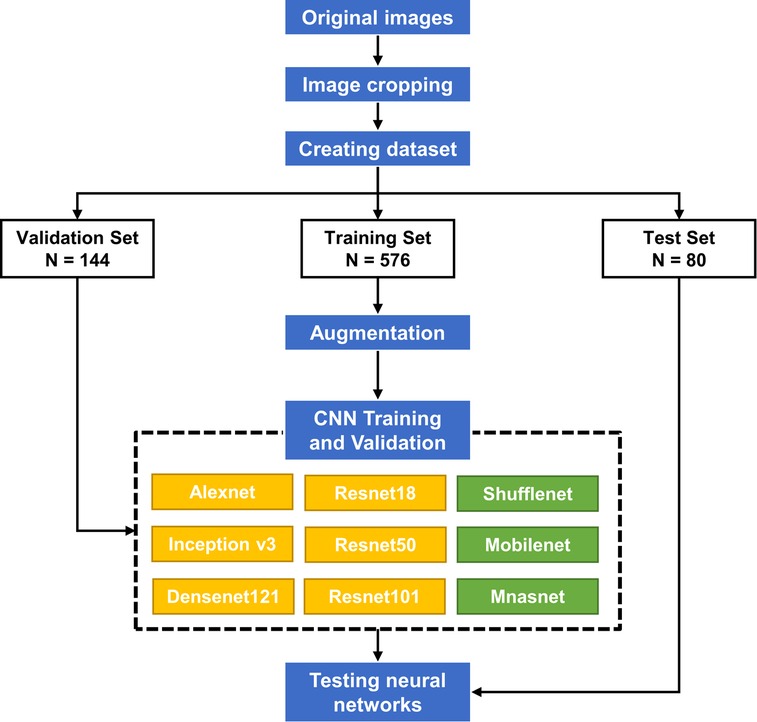
Figure 1. The schematic diagram of the whole process.
Methods
Image datasets
The image datasets were collected retrospectively from our hospital between January 2015 and June 2021 in this study. A total of 800 ear images (left or right side) were included, consisting of 360 images of normal ear and 440 images of microtia. Lateral view photographs of the ears were captured using a digital camera (Nikon D3100, Tokyo, Japan). The inclusion criteria were microtia or normal ears without previous ear surgery. The images that seem blurred or at undesired angulation were excluded. This study was approved by the local Ethical Committee (TJ-IRB20220112). The committee waived the need for individual informed consent as the study was retrospective and non-interventionist.
Severity assessment of microtia
The severity of microtia was classified according to the classification used by Mastroiacovo (16). Grade I microtia corresponded to concha-type microtia with a small auricle and some distinguishable anatomic structures (Figure 2). Grade II microtia as lobule-type microtia showed a residual vertical ridge of tissue shaped like a peanut. Grade III microtia was almost or complete absence of the pinna. The grades of 800 ear images were labeled by two experienced plastic surgeons.
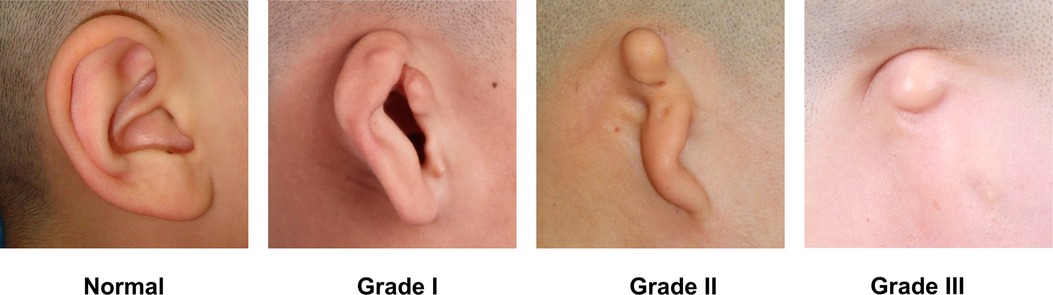
Figure 2. The severity assessment of microtia.
Pre-processing
The images were cropped to the ear boundary at a size of 1:1 and then used for deep learning. A total of 800 images were randomly divided into training, validation, and test sets with 640, 80, and 80 images, respectively (Figure 1). The training and validation sets were used to train CNN models, and the test set provided the final evaluation of the model's performance. To reduce overfitting due to the small dataset size, online data augmentation was applied to increase the data size. The training images were randomly flipped, rotated, and displaced to achieve data augmentation.
CNN models and training
Nine CNNs, including Alexnet, Inception v3, Densenet121, Resnet18, Resnet50, Resnet101, Shufflenet v2, Mobilenet v2, and Mnasnet were used for classifying the severity of microtia. The basic properties of the CNNs are listed in Table 1. Alexnet, Resnet101, Resnet50, Inception v3, Resnet18, and Densenet121 are relatively large networks, of which Alexnet is the largest with over sixty million parameters. Shufflenet, Mobilenet, and Mnasnet are relatively small networks with less than four million parameters. The training process consisted of forward propagation and backward propagation. With images input into the networks, forward propagation output the classification result, including the accuracy and loss between the predicted and true labels. Then, the model parameters were updated through backward propagation. The models were trained up to 100 epochs with 16 mini-batch sizes and established based on the maximum accuracy and minimum loss in the validation set.
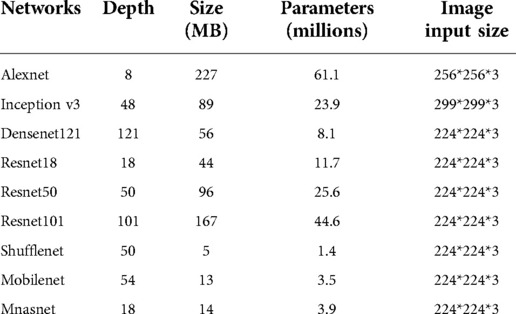
Table 1. The properties of the convolutional neural networks.
Performance evaluation
The evaluation metrics, including accuracy, precision, recall, F1 score were calculated with the confusion matrix of the test set. Additionally, the receiver operating characteristic (ROC) curve and area under the ROC curve (AUC) were used to assess the diagnostic performance of the CNN models. The calculation formulas for the evaluation metrics were as follows (TP: true positive, TN: true negative, FP: false positive, FN: false negative):
Results
Of the total 800 ear images, 360, 150, 240, and 50 images were classified as normal ears, grade I microtia, grade II microtia, and grade III microtia, respectively. The test set was composed of 30 images of normal ears, 20 images of grade I microtia, 20 images of grade II microtia, and 10 images of grade III microtia.
The training loss and validation accuracy of the nine CNNs were shown in Supplementary Figures S1, S2, respectively. The confusion matrices for each network between true and predicted labels of the test set were presented in Figure 3. The evaluation metrics of each network in the test set, including accuracy, precision, recall, and F1 score, were summarized in Table 2. Eight CNNs were tested with accuracy more than 0.8, while Mnasnet only reached 0.463. Among them, Alexnet achieved a relatively high accuracy of 0.900, a precision of 0.927, a recall of 0.875, and an F1 score of 0.897. As a small network, Mobilenet also achieved an accuracy of 0.900, a precision of 0.918, a recall of 0.879, and an F1 score of 0.898.
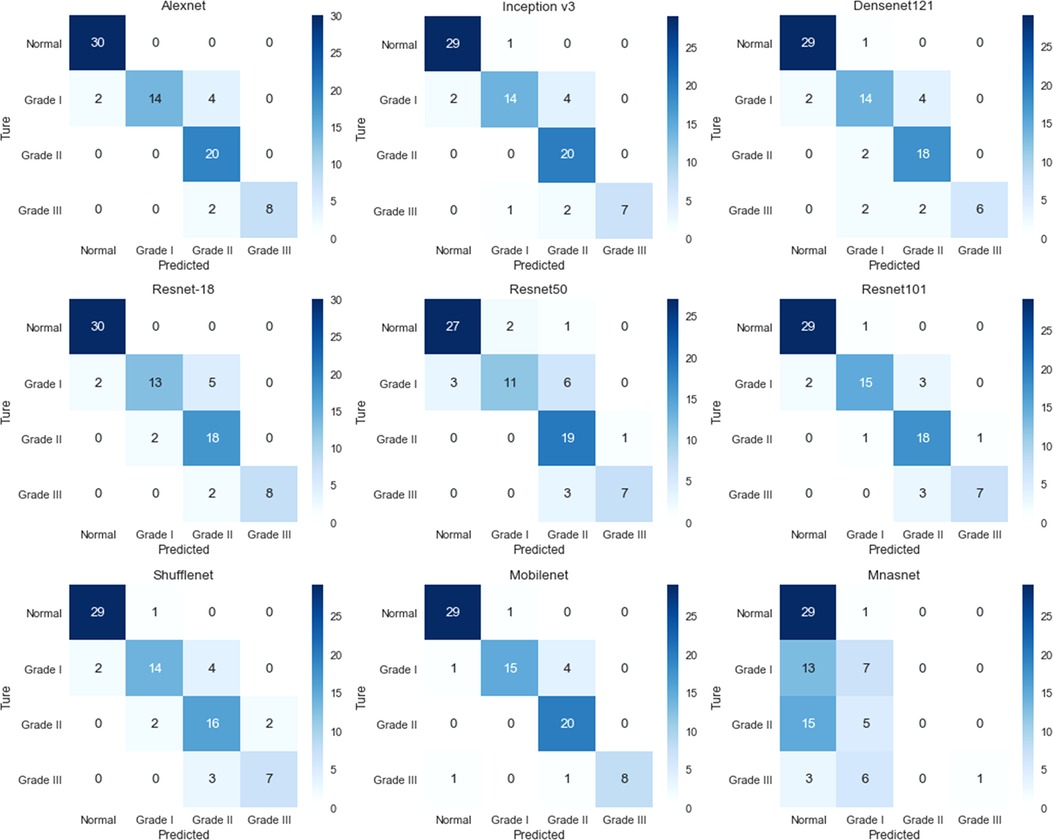
Figure 3. The confusion matrix of the convolutional neural networks for assessing the severity of microtia.
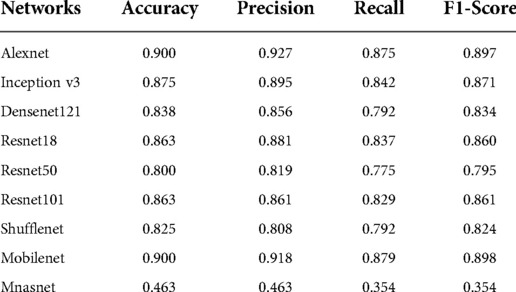
Table 2. The performance of convolutional neural networks for assessing the severity of microtia.
ROC curves and AUC values were obtained for each grade of microtia corresponding to each CNN (Figure 4). All CNNs except Mnasnet achieved high AUC values more than 0.9 for each grade of microtia. Particularly in the Alexnet, Resnet50, Resnet101, and Mobilenet, the AUC values for each grade of microtia were greater than 0.95. In most CNNs, such as Alexnet, Inception v3, Densenet121, Resnet18, Resnet101, and Shufflenet, the grade I microtia had the lowest AUC values and the normal ear had the highest AUC values.
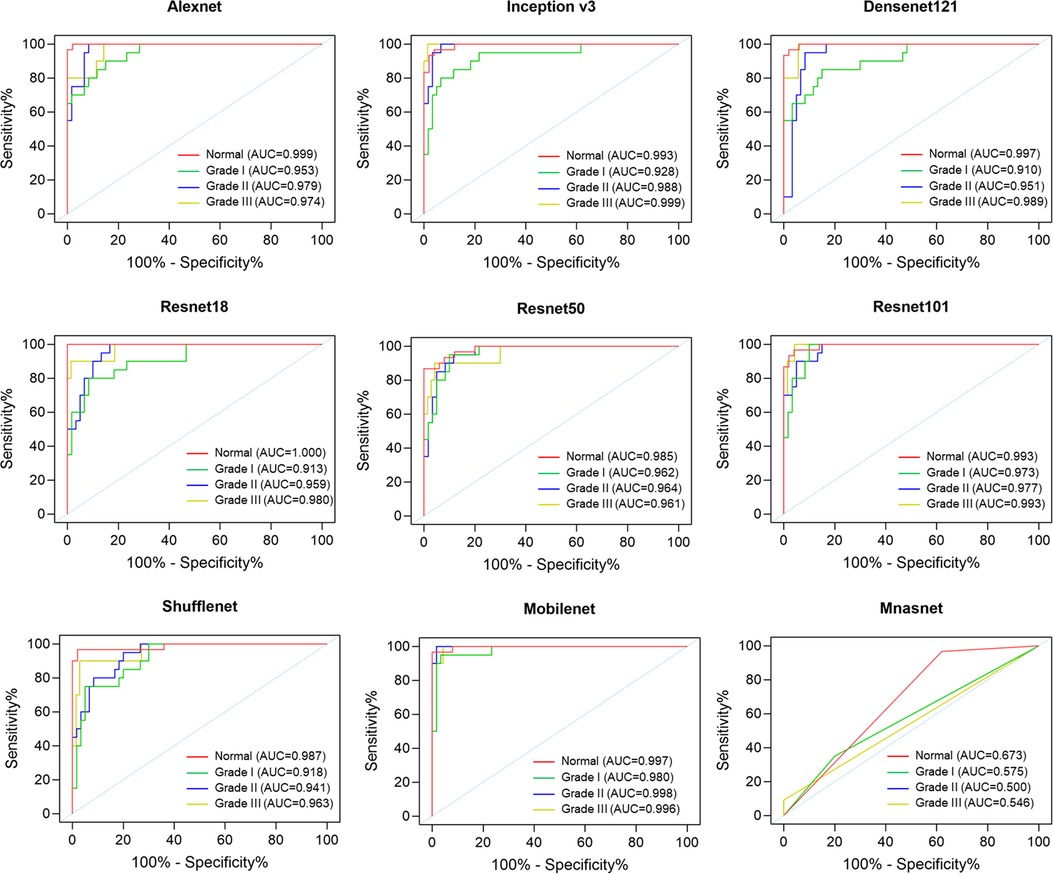
Figure 4. The ROC curves of the convolutional neural networks for assessing the severity of microtia.
Discussion
In recent years, artificial intelligence has attracted increasing attention in healthcare. As an important technique of artificial intelligence, machine learning is used for data analysis that enables computers to learn from data, extract meaningful patterns and make reliable decisions (17). Deep learning, a subset of machine learning, can extract higher-level features from data using neural networks. Among deep learning methods, convolutional neural networks (CNNs) have made considerable progress in image analysis, such as image recognition, classification, and detection, attributed to their deep layer structure (18).
The appearance of the outer ear is characterized by morphological features, including tragus, lobule, antitragus, concha, helix, antihelix, scapha, navicular fossa, and other structures. Besides face, iris and fingerprints, ear allows for personal identification due to a large number of unique features. Recently, several studies have demonstrated the effectiveness of CNNs in ear recognition with high recognition rates (19–22). Additionally, studies have reported that CNNs can identify normal ear and congenital ear abnormalities from two-dimensional photographs (13–15). Hallac et al. found that the CNN GoogLeNet could serve as an ear deformity detection model with a test accuracy of about 94.1% (13). Besides, CNN was demonstrated to be a robust tool for assessing outcomes of ear molding therapy by removing the subjectivity of human evaluation (14). Similarly, Ye et al. revealed that the CNN ResNet can evaluate reconstructed auricles in a manner resembling that of a medical student, indicating the potential of CNN for assessing the outcomes of auricular reconstruction (15). Overall, CNN has the ability to identify the morphological structure of the ear.
Microtia is a common congenital disease in plastic surgery, however, no reliable objective method exists to assess its severity. There is no gold standard for the severity of microtia, although multiple classifications have been introduced relying on subjective assessment. The complexity of the ear makes it difficult to establish mathematical models to assess microtia. To our knowledge, there is no previous study to assess the severity of microtia using CNN.
In this study, we tested nine CNNs that have been applied and performed well in medical image classification (23–28). The Alexnet architecture won the 2012 ImageNet Large Scale Visual Recognition Challenge, and since then CNNs have been flourishing. The innovations of the Inception-v3 architecture were factorized convolutions and aggressive regularization to improve classification accuracy. Then, the Resnet architecture was proposed to learn residual functions with reference to the layer inputs instead of learning unreferenced functions. Subsequently, Densenet extended the network connectivity on the basis of Resnet by connecting each layer to other layers in a feed-forward fashion. Additionally, Shufflenet, Mobilenet, and Mnasnet were lightweight neural networks and specialized toward use in mobile devices.
The dataset in this study was relatively small, which could lead to the overfitting of the CNN model. Therefore, the technique of data augmentation was performed to increase the performance of the CNN models. We found that most CNN models achieved high accuracy over 0.8 in assessing the severity of microtia, particularly Alexnet and Mobilenet even achieved a high accuracy of 0.9. In general, the deeper the CNN, the higher the accuracy. However, this trend was not obvious in this study, where the depth of network was not proportional to the classification accuracy. The results showed that Resnet50 and Resnet101 were no more accurate than Resnet18, indicating adequate learning could still be achieved despite the small number of layers. Similarly, this study did not reveal a positive correlation between the number of parameters in CNN and classification accuracy. Although Shufflenet and Mobilenet were lightweight networks with less than 4 million parameters, the accuracy remained high in this study. Regarding the accuracy of each grade of microtia in the CNNs, the AUC values for grade I microtia were relatively low compared to the other grades. It is presumed that grade I microtia varies widely from near normal to near peanut-shaped auricles, resulting in lower classification accuracy.
An ideal diagnostic tool for microtia needs to be objective, reproducible, low-cost, simple to implement, and allow for real-time feedback. The findings in the present study demonstrate the high accuracy of CNNs in classifying microtia, even with a lightweight CNN. Therefore, to make the use convenient and practical in clinical situations, the CNN models are available for mobile platforms, such as smartphones, with relatively small memory size and computing power. In clinical use, a doctor or non-professional can take a photo of the ear using mobile devices, and the machine will automatically provide real-time feedback on the severity of the microtia. Importantly, the performance of the CNN model can continue to improve, with the development of algorithms and the expansion of training data.
Some limitations exist in this study. Firstly, a relatively small data set of 800 clinical images was included, and a large number and high-quality images from multicenter are required for better-performing CNN models. Secondly, due to the absence of a gold standard for assessing the severity of microtia, we have adopted a popular classification as ground truth based on subjective observation of the auricular shape. Although this classification method may not be accepted by all surgeons, our results indicate deep learning can be a feasible and automated method for microtia severity. Thirdly, current classification methods mostly rely on subjective assessment by surgeons, and no reliable objective method to evaluate the severity of microtia has been reported before. The lack of comparison with state of art methods is another limitation of our study. Finally, images were cropped manually in the pre-processing, which required automation of image acquisition and pre-processing when developing diagnostic tools for clinical use.
Conclusion
Artificial intelligence is a potentially practical method to objectively assess the severity of microtia. This study tested the performance of nine CNNs for classifying microtia, and most CNN models possessed high accuracy, even with lightweight networks and insufficient training images. The CNN models applied to mobile platforms could be a more available and standardized tool in future clinical practice.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by Tongji Hospital, Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author contributions
DW and XC performed the experiment. YW, HT, and PD conceived the project and revised the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This section acknowledges contributions from the China GuangHua Science and Technology Foundation (No. 2019JZXM001) and Wuhan Science and Technology Bureau (No. 2020020601012241).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2022.929110/full#supplementary-material.
References
1. Luquetti DV, Leoncini E, Mastroiacovo P. Microtia-anotia: a global review of prevalence rates. Birth Defects Res A Clin Mol Teratol. (2011) 91(9):813–22. doi: 10.1002/bdra.20836
2. Zhang Y, Jiang H, Yang Q, Zhang Y, Jiang H, Yang Q, He L, Yu X, Huang X, et al. Microtia in a Chinese specialty clinic population: clinical heterogeneity and associated congenital anomalies. Plast Reconstr Surg. (2018) 142(6):892e–903e. doi: 10.1097/PRS.0000000000005066
3. Tanzer RC. Total reconstruction of the external ear. Plast Reconstr Surg Transplant Bull. (1959) 23(1):1–15. doi: 10.1097/00006534-195901000-00001
4. Brent B. Auricular repair with autogenous rib cartilage grafts: two decades of experience with 600 cases. Plast Reconstr Surg. (1992) 90(3):355–74. doi: 10.1097/00006534-199209000-00001
5. Nagata S. A new method of total reconstruction of the auricle for microtia. Plast Reconstr Surg. (1993) 92(2):187–201. doi: 10.1097/00006534-199308000-00001
6. Kelley PE, Scholes MA. Microtia and congenital aural atresia. Otolaryngol Clin North Am. (2007) 40(1):61–80. doi: 10.1016/j.otc.2006.10.003
7. Arshad M, Khan MA, Tariq U, Armghan A, Alenezi F, Younus Javed M, et al. A computer-aided diagnosis system using deep learning for multiclass skin lesion classification. Comput Intell Neurosci. (2021) 2021:9619079. doi: 10.1155/2021/9619079
8. Yala A, Mikhael PG, Strand F, Lin G, Satuluru S, Kim T, et al. Multi-institutional validation of a mammography-based breast cancer risk model. J Clin Oncol. (2021) 40(16):1732–40. doi: 10.1200/JCO.21.01337
9. Warin K, Limprasert W, Suebnukarn S, Jinaporntham S, Jantana P. Performance of deep convolutional neural network for classification and detection of oral potentially malignant disorders in photographic images. Int J Oral Maxillofac Surg. (2021) 51(5):699–704. doi: 10.1016/j.ijom.2021.09.001
10. Chen P-N, Lee C-C, Liang C-M, Pao S-I, Huang K-H, Lin K-F. General deep learning model for detecting diabetic retinopathy. BMC Bioinform. (2021) 22(Suppl 5):84. doi: 10.1186/s12859-021-04005-x
11. McCullough M, Ly S, Auslander A, Yao C, Campbell A, Scherer S, et al. Convolutional neural network models for automatic preoperative severity assessment in unilateral cleft lip. Plast Reconstr Surg. (2021) 148(1):162–9. doi: 10.1097/PRS.0000000000008063
12. Zhang BH, Chen K, Lu SM, Nakfoor B, Cheng R, Gibstein A, et al. Turning back the clock: artificial intelligence recognition of age reduction after face-lift surgery correlates with patient satisfaction. Plast Reconstr Surg. (2021) 148(1):45–54. doi: 10.1097/PRS.0000000000008020
13. Hallac RR, Lee J, Pressler M, Seaward JR, Kane AA. Identifying ear abnormality from 2D photographs using convolutional neural networks. Sci Rep. (2019) 9(1):18198. doi: 10.1038/s41598-019-54779-7
14. Hallac RR, Jackson SA, Grant J, Fisher K, Scheiwe S, Wetz E, et al. Assessing outcomes of ear molding therapy by health care providers and convolutional neural network. Sci Rep. (2021) 11(1):17875. doi: 10.1038/s41598-021-97310-7
15. Ye J, Lei C, Wei Z, Wang Y, Zheng H, Wang M, et al. Evaluation of reconstructed auricles by convolutional neural networks. J Plast Reconstr Aesthetic Surg. (2022) 75:2293–301. doi: 10.1016/j.bjps.2022.01.037
16. Mastroiacovo P, Corchia C, Botto LD, Lanni R, Zampino G, Fusco D. Epidemiology and genetics of microtia-anotia: a registry based study on over one million births. J Med Genet. (1995) 32(6):453–7. doi: 10.1136/jmg.32.6.453
17. Deo RC. Machine learning in medicine. Circulation. (2015) 132(20):1920–30. doi: 10.1161/CIRCULATIONAHA.115.001593
18. Anwar SM, Majid M, Qayyum A, Awais M, Alnowami M, Khan MK. Medical image analysis using convolutional neural networks: a review. J Med Syst. (2018) 42(11):226. doi: 10.1007/s10916-018-1088-1
19. Aiadi O, Khaldi B, Saadeddine C. MDFNet: an unsupervised lightweight network for ear print recognition. J Ambient Intell Humaniz Comput. (2022) 2022:1–14. Epub ahead of print.. doi: 10.1007/s12652-022-04028-z
20. Lei Y, Qian J, Pan D, Xu T. Research on small sample dynamic human ear recognition based on deep learning. Sensors (Basel). (2022) 22(5):1718. doi: 10.3390/s22051718
21. Ahila Priyadharshini R, Arivazhagan S, Arun M. A deep learning approach for person identification using ear biometrics. Appl Intell (Dordrecht, Netherlands). (2021) 51(4):2161–72. doi: 10.1007/s10489-020-01995-8
22. Alshazly H, Linse C, Barth E, Martinetz T. Ensembles of deep learning models and transfer learning for ear recognition. Sensors (Basel). (2019) 19(19):4139. doi: 10.3390/s19194139
23. Hosny KM, Kassem MA, Fouad MM. Classification of skin lesions into seven classes using transfer learning with AlexNet. J Digit Imaging. (2020) 33(5):1325–34. doi: 10.1007/s10278-020-00371-9
24. Al Husaini MAS, Habaebi MH, Gunawan TS, Islam MR, Elsheikh EAA, Suliman FM. Thermal-based early breast cancer detection using inception V3, inception V4 and modified inception MV4. Neural Comput Appl. (2021) 34(1):333–48. doi: 10.1007/s00521-021-06372-1
25. Fulton L V, Dolezel D, Harrop J, Yan Y, Fulton CP. Classification of Alzheimer’s disease with and without imagery using gradient boosted machines and ResNet-50. Brain Sci. (2019) 9(9):212. doi: 10.3390/brainsci9090212
26. Li X, Shen X, Zhou Y, Wang X, Li T-Q. Classification of breast cancer histopathological images using interleaved DenseNet with SENet (IDSNet). PLoS ONE. (2020) 15(5):e0232127. doi: 10.1371/journal.pone.0232127
27. He Z, Wang Y, Qin X, Yin R, Qiu Y, He K, et al. Classification of neurofibromatosis-related dystrophic or nondystrophic scoliosis based on image features using bilateral CNN. Med Phys. (2021) 48(4):1571–83. doi: 10.1002/mp.14719
Keywords: artificial intelligence, microtia, severity, convolutional neural networks, objective
Citation: Wang D, Chen X, Wu Y, Tang H and Deng P (2022) Artificial intelligence for assessing the severity of microtia via deep convolutional neural networks. Front. Surg. 9:929110. doi: 10.3389/fsurg.2022.929110
Received: 26 April 2022; Accepted: 23 August 2022;
Published: 8 September 2022.
Edited by:
Rocco Furferi, University of Florence, ItalyReviewed by:
Pedro Martins, Instituto Politecnico de Viseu, PortugalJay Kant Pratap Singh Yadav, Ajay Kumar Garg Engineering College, India
© 2022 Wang, Chen, Wu, Tang and Deng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pei Deng ZGVuZ3BlaXRqQDE2My5jb20= Hongbo Tang MTY5NTIyNDNAcXEuY29t
Specialty Section: This article was submitted to Reconstructive and Plastic Surgery, a section of the journal Frontiers in Surgery