
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 28 June 2022
Sec. Surgical Oncology
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.918348
This article is part of the Research Topic Surgery and COVID-19: Which strategies to apply in oncologic patients, Volume II View all 7 articles
 Francesca Carissimi1,2
Francesca Carissimi1,2 Mauro Alessandro Scotti1Cristina Ciulli1,2Alessandro Fogliati1,2
Mauro Alessandro Scotti1Cristina Ciulli1,2Alessandro Fogliati1,2 Fabio Uggeri1,2
Fabio Uggeri1,2 Marco Chiarelli3Marco Braga1,2
Marco Chiarelli3Marco Braga1,2 Fabrizio Romano1,2Mattia Garancini1
Fabrizio Romano1,2Mattia Garancini1
Introduction: While the COVID-19 pandemic is still ongoing, it is even more evident that victims of the pandemic are not only those who contract the virus, but also the countless patients suffering from other serious diseases (i.e., tumor) who have undergone delayed potentially life-saving surgery due to a lack of beds. Like many hospitals, ours also initially blocked all elective oncologic surgery, but these operations were “recovered” and reintegrated in a relatively short time, thanks to the establishment of COVID-free wards and operating rooms with staff dedicated to oncological surgery. In tis context, our aim is to assess whether and how the severe acute respiratory syndrome Coronavirus-2 (SARS-CoV-2) pandemic has impacted our hepatobiliary surgery unit.
Methods: From our prospective database, we retrospectively took data from patients undergoing liver surgery in 2018–2019 (pre-COVID) and 2020–2021 (COVID period). Patients admitted to COVID-free wards must necessarily have a negative nasal swab from the previous 24 h.
Results: Between January 1, 2018, and December 31, 2019 (Group 1), 101 patients were treated; during the pandemic [January 1, 2020, and December 31, 2021 (Group 2)], 126 patients were treated. There was no statistical difference between the groups. The median postoperative hospital stay was 7 days for both groups; 7 patients had major complications (Clavien-Dindo > 3) in Group 1 and 11 in Group 2 (p = 0.795). A total of 4 patients died in Group 1 and 6 during the pandemic (p = 0.754). Tumor burden was significantly greater in Group 2 where nodule size, lymphadenectomy, and extrahepatic disease were significantly greater (p = 0.011, p = 0.004, and p = 0.026, respectively).
Conclusion: During the COVID pandemic, our HPB unit managed to offer a volume of tertiary-center hepatobiliary surgery without a significant impact in terms of length of stay, morbidity, or mortality despite the increase in tumor burden during the pandemic years.
The severe acute respiratory syndrome Coronavirus-2 (SARS-CoV-2) has spread globally since the end of December 2019, exponentially increasing the need for intensive care of the affected population; this growth has focused health forces on new interstitial pneumonia (1, 2). Italy, in particular the Northern region, was the European nation to suffer the most from the devastating effects of COVID-19, with mortality peaks much higher than the European median (over 15 daily deaths per million inhabitants) (3, 4). To ensure access to care for all patients with SARS-CoV-2 pneumonia, profound changes were made in hospital activities to redistribute resources with a consequent radical decrease in outpatient visits and surgical interventions (5). Follow-up and non-urgent visits were suspended, as were all routine diagnostic tests. Surgery was reorganized guaranteeing only elective cancer surgery and emergency surgery (6–8). Neoplastic liver diseases were also affected by the pandemic; in fact, outpatient visits were drastically reduced due to the lack of human resources and the reluctance and fear of patients to go to hospital, causing a delay in the diagnosis of primary cancers or relapses.
Cancer patients have, therefore, become a category affected by COVID-19 without being infected due to the delay in diagnosis and the consequent progression of the disease, worsening the long-term outcome of these patients. Furthermore, when the operating rooms were reactivated for cancer patients, the infection (even asymptomatic or paucisymptomatic) represented a contraindication to the planned intervention due to the possible liver damage related to the COVID infection (9) which would complicate the already delicate post-operative course. COVID-19 infection could be responsible for the development of post-hepatectomy liver failure (PHLF), and SARS-CoV-2-related pneumonia after liver surgery could be an independent risk factor for morbidity and mortality (10). PHLF is the most life-threatening complication after liver surgery (11, 12). Only a very few papers have focused on the effect of COVID-19 on liver surgery practice. We report here the experience of our medium-volume Liver Surgery Center (13). The aim of the study is to evaluate the effects of the COVID-19 pandemic on liver surgery in a middle-volume Italian Center.
We retrospectively analyzed the data collected from a prospectively maintained database of all patients undergoing liver surgery at the HPB Unit of the San Gerardo Hospital, Monza, University of Milano Bicocca from January 1, 2018, to December 31, 2021.
According to Torzilli et al. (13), we are considered a middle-volume center for liver surgery. Patients were divided into two groups: Group 1 (January 1, 2018, to December 31, 2019) before the pandemic and Group 2 (January 1, 2020, to December 31, 2021) during the pandemic.
Every patient who underwent elective surgery in 2020–2021 was screened for COVID-19; if any patient was affected by SARS-CoV-2, surgery was always delayed until the resolution of COVID-19. During hospitalization, patients underwent control nasal swabs on days 3–5–10 and every week until discharge. If a patient became positive at control swabs, he was immediately transferred to the COVID ward and his roommates placed in isolation.
A comparative analysis of the two periods was conducted to evaluate the effects of the COVID-19 pandemic on liver surgery; preoperative data and surgical and postoperative outcomes were analyzed and compared between study periods.
Clavien–Dindo classification (14) and the Comprehensive Complication Index (CCI) (15) were used to assess the complication rate in our population. Statistical significance was accepted at p < 0.05. The study was conducted in accordance with the regulations for retrospective studies of our hospital.
Data analysis was performed using IBM SPSS Statistics. Statistical analysis was obtained for the main descriptive indexes. Quantitative data were expressed as mean ± standard deviation (SD) or median and interquartile range (IQR) depending on the statistical appropriateness. The qualitative data were elaborated as absolute frequencies, relative frequencies, cumulative frequencies, and percentages.
From January 2018 to December 2019 (Group 1), a total of 101 patients were treated in our HPB unit, and from January 2020 to December 2021 (Group 2), the total number was 126; Table 1 shows that there was no alteration in the patient baseline, decision making, and quality of care as there was no statistical difference in patient demographics, indications for surgery, and complexity of procedures.
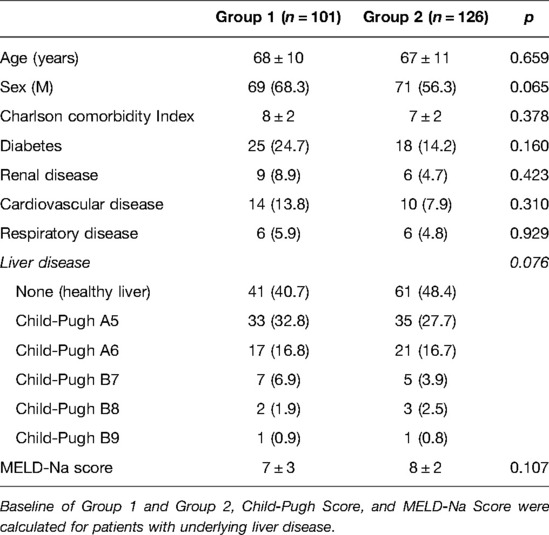
Table 1. Baseline of Group 1 and Group 2.
Mainly liver resection in the two groups was done for HCC and liver metastases; Table 2 shows in detail the pathologies treated. Most of the interventions were segmentectomies and atypical liver resections with similar rates in the two groups; in Group 1, 4% of patients underwent major resection [3 or more contiguous liver segments (16)], whereas in Group 2, this percentage rose to 7% without reaching statistical significance with a p of 0.476 (Table 3).
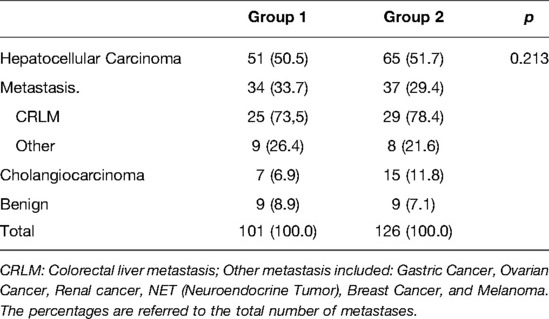
Table 2. Liver pathologies treated pre-COVID (Group 1) and during pandemic (Group 2).
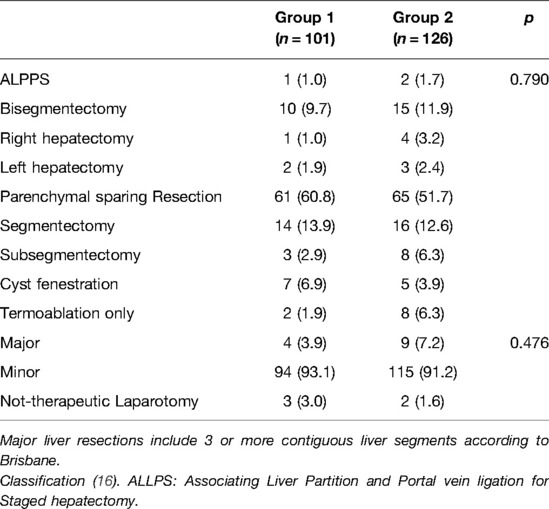
Table 3. Type of surgery and extension of liver resection.
The tumor burden in the group of patients treated before the pandemic was 2 ± 2 nodules, but during the pandemic, the mean increased to 2 ± 2 nodules. The size of the major nodule increased from a median of 21 (IQR 15–30) in Group 1 to 25 (IQR 11–28) in Group 2 with a statistically significant difference (p = 0.011). We also noticed in patients affected by cholangiocarcinoma and metastases an increase in lymphadenopathy and extrahepatic disease from 6 to 16 and from 9 to 21 in the two groups, respectively, with a p of 0.004 and 0.026, respectively. During cholangiocarcinoma surgery, we performed lymphadenectomy, and the number of lymph nodes collected in Group 1 was 3 (IQR 0–5), and in Group 2, it was 4 (IQR 2–6) with p = 0.361; of these, the number of metastatic lymph nodes increased from 1 (0–1) to 3 (1–5) between two study periods (p = 0.015). The length of surgery was 277 ± 129 min in Group 1 and 360 ± 162 min in Group 2 with no difference; during the pandemic, the number of intraoperative RF treatments increased from 2 (Group 1) to 14 (Group 2) with a p of 0.008. The laparoscopic approach was employed in 44.6% of patients in Group 1 and in 59.5% in Group 2, with a significant increase (p = 0.049); the conversion rate was 31.1% and 22.6%, respectively, in Group 1 and Group 2 (p = 0.127). The laparotomy approach did not change significantly (p = 0.09) in the two groups: 55.4% in Group 1 and 40.5% in Group 2 (Table 4).
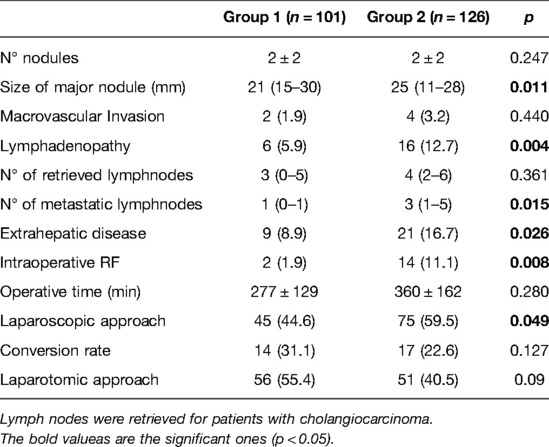
Table 4. Comparison of tumor burden between Group 1 and Group 2.
The postoperative hospital length of stay was 7 (IQR 5–11) days before the pandemic and 7 (IQR 5–17) during the pandemic (p = 0.183). The complication rate was comparable in the two groups, as shown in Table 5; the major complications (CD >3) were 7.9% and 8.7% in Groups 1 and 2, respectively (p = 0.795), four patients died during the prepandemic period and six died during the pandemic (p = 0.754). The CCI demonstrated no significant differences between the two groups, 0.0 (IQR 0–20.9) in Group 1 vs. 8.7 (IQR 0.0–24.2) in Group 2 (p = 0.559). No patient developed COVID-related pneumonia or became positive when the control nasal swab was applied during hospitalization.
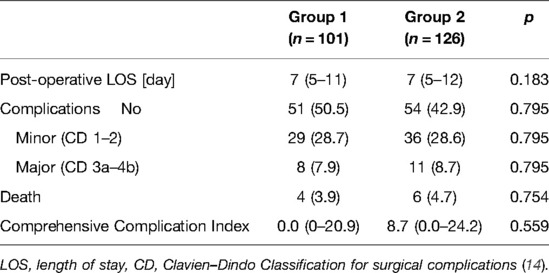
Table 5. Post-operative course and complication.
The COVID pandemic put a strain on the Italian health system, which suddenly found itself facing several critically ill patients for whom there were insufficient resources (17). A shortage of healthcare professionals and limited bed capacity were major hurdles in the care of patients with oncological disease during the pandemic. To tackle this problem, HUB hospitals were identified to refer patients affected by COVID-19, including our center. A large part of medical staff was recruited into COVID departments due to this reorganization; this choice caused problems in the management of all other wards and activities. The unusual, altered allocation of healthcare resources might be responsible for collateral damage to oncological patients: screening interruption, treatments deleted or downgraded, and follow-up delay (18). Moreover, cancer patients are at major risk to contract COVID-19 infection both from nosocomial exposure and from their immunocompromised states (19). In our Liver Surgery Unit, all cases are discussed in multidisciplinary meetings and are managed following European Association for the Study of the Liver (EASL) guidelines and the Barcelona Clinic Liver Cancer (BCLC) staging system (20, 21). From our experience, we noted a reduction in hepatic procedures during the first and second pandemic wave (Group 1), with an increasing rebound in Group 2, during which hospital resources were organized to deal with COVID but to maintain activity for oncologic patients. The multidisciplinary group, during the first period of the pandemic, had suspended the meetings to avoid contagion of the involved specialists; moreover, the possibility of treating the patients already discussed was almost impossible due to the suspension of the elective activity—albeit short—of the first wave. Furthermore, the absence of outpatient clinics and follow-ups did not allow the enrollment of new patients. Obviously, specialists have always had the opportunity to communicate with one another telematically if necessary, and as soon as it was possible, multidisciplinary discussion was reintroduced. Overlooking our data, we could see how the number of patients treated during the COVID pandemic (Group 2) did not decrease, but rather increased even if in a not statistically significant way (p 0.213); this demonstrated how the impressive rearrangement of the health system permitted to maintain a high level of assistance for patients undergoing liver surgery (4).
With the gradual resumption of normal activities since January 2020, we have had a rebound in the number of patients and outpatient visits due to the waiting lists caused by the blockade during the pandemic.
The resumption of visits led to the diagnosis of new tumors in patients who were not followed up. Our data, in agreement with those of the existing literature (22, 23), did not show statistically significant differences in the number and type of liver disease treated (p = 0.213).
However, upon analyzing our data, what emerged was an increase in tumor burden, with an increase in the size of nodules (p = 0.011), lymphadenopathy (p = 0.004), and extrahepatic disease (p = 0.026) in patients treated after the pandemic (Group 2); in a recent study from six academic referral centers in France, the authors reported a delay longer than one month in the diagnosis and treatment of HCC in the pre-COVID era, and the COVID period was found to be a strong independent predictor of treatment delay or cancellation (24). This could justify the presence of an increased tumor burden at diagnosis compared with the pre-COVID era (Group 1). As demonstrated by our experience, tumor progression occurred in patients with more aggressive tumor biology during the pandemic due to delayed or discontinued follow-up and treatment, and the consequence was a shift toward a higher tumor burden at diagnosis (25). Furthermore, cirrhotic patients may be more prone to hepatic decompensation during the period of social lockdown due to the lack of controls, and the worsening of liver function in these cases has made the HCC management plan more complex in case of cirrhosis (26).
Tellez et al. (27) show how the COVID-19 pandemic had a huge impact on the routine care of liver cancer patients; what can be seen from our data is the increase in patients who underwent intraoperative radiofrequency (as a single treatment strategy or associated with liver resections) during the pandemic (p = 0.008) due to a greater tumor burden, which made the technically more complex or impossible surgical resection possible (i.e. vascular invasion at the IOUS). Balakrishnan et al. (28), in their survey, show how this change in therapeutic strategy has occurred worldwide. Internationally, HPB centers have reported a reduction in the number of surgical resections and the adoption of a non-surgical management of pathologies that were traditionally treated surgically, although the Society of Surgical Oncology (29) asserts that the surgical approach is recommended for aggressive hepatobiliary malignancies, also stating that neoadjuvant chemotherapy, ablation therapies, or stereotactic radiotherapy could be considered for resectable liver metastases or HCC. The Italian Association for the Study of the Liver conducted a survey to evaluate the impact of COVID-19 on the activity of some hepatology units, reporting that the surgical treatment of HCC had been significantly reduced or even stopped (30, 31).
The shift of liver cancer therapy toward nonsurgical treatment is justified by a lower complication rate associated with a good outcome in oncological terms for the patient (32). The use of intraoperative radiofrequency impacts less on the post-operative course by requiring a stay in intensive care in a very limited number of cases. This is a key issue in the COVID era due to the limited number of beds in ICU; and radiofrequency also reduces the post-operative hospital stay by reducing the patient’s risk of contracting the virus (33).
Liver resection during a pandemic should be limited to: (i) patients with a low risk of liver decompensation; and (ii) those without comorbidities that increase the risk of severe COVID-19 (34). Since January 2020, the COVID-19 pandemic has led to several debates regarding different aspects of the management of the surgical patient, especially related to the possible risk for healthcare professionals during surgery (35). The use of minimally invasive surgery when an indication for hepatic resection has been established is to be preferred due to its advantages such as a decreased length of stay, reduced postoperative complications, and, in general, less need for treatment (36).
The possible aerosolization of viral pathogens during laparoscopy is still controversial (37, 38). It is essential that all staff in the operating room wear personal protective equipment and use the AIRSEAL® system as suggested by the SAGES-EAES Guidelines (39) for gas recirculation.
Following these pieces of advice, we do not reduce laparoscopic approach to liver surgery in the pandemic period; instead, we increase significantly (p = 0.049) the number of laparoscopic procedures to be performed.
Postoperative complications did not show differences between our two groups in terms of LOS, major complications, and death (p > 0.05). Our results differ from the survey, and based on the IHPBA-COVID Registry, reported that COVID-19 was associated with a high mortality rate after hepato-pancreato-biliary (HPB) surgery (29% for pancreaticoduodenectomy, 15% major hepatectomy, and 3% cholecystectomy); moreover, cancer patients are at major risk to contract COVID-19 infection both from nosocomial exposure and from their immunocompromised states (19). Fortunately, none of our patients developed SARS-CoV-2 infection, thanks to our prevention measures aforementioned: dedicated COVID-19-free areas of the hospital (ward and operating room); (ii) healthcare personnel dedicated only to COVID-19-free areas, using protective equipment; and (iii) periodic nasal swab to all patients to confirm negativity or identify early positivity in order to protect frail patients.
COVID has had a great impact on patient care activities due to the profound readjustment of the health system to address the new needs dictated by the pandemic. Liver cancer patients have seen their follow-up postponed or even deleted with later diagnosis, which has led to a greater tumor burden, with a consequently different curative approach to the pathology (an increase in thermoablative treatments). Besides, what we have learned from the pandemic is that a rapid and prompt reorganization of activities, focused on cancer patients, does not affect the type of surgical approach or the patient’s outcome; in fact, despite all changes, the complication rate remains stable in our HBP unit.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
FR, MG, and FC developed the study, AF, CC, and FU analyzed data, and MB and MC revised the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Arshad Ali S, Baloch M, Ahmed N, Arshad Ali A, Iqbal A. The outbreak of coronavirus disease 2019 (COVID-19)—An emerging global health threat. J Infect Public Health. (2020) 13:644–6. doi: 10.1016/j.jiph.2020.02.033
2. Kannan S, Shaik Syed Ali P, Sheeza A, Hemalatha K. COVID-19 (novel coronavirus 2019)—Recent trends. Eur Rev Med Pharmacol Sci. (2020) 24:2006–11. doi: 10.26355/eurrev_202002_20378
3. Rovetta A, Bhagavathula AS. The effects of COVID-19 first waves in italy: an answer through a retrospective analysis of mortality. JMIR Public Health Surveill. (2022). doi: 10.2196/36022
4. Bontempi E. First data analysis about possible COVID-19 virus airborne diffusion due to air particulate matter (PM): the case of Lombardy (Italy). Environ Res. (2020) 186:109639. doi: 10.1016/j.envres.2020.109639
5. Santacroce L, Bottalico L, Charitos IA. The impact of COVID-19 on Italy: a lesson for the future. Int J Occup Environ Med. (2020) 11:151–2. doi: 10.34172/ijoem.2020.1984
6. Vigneswaran Y, Prachand VN, Posner MC, Matthews JB, Hussain M. What is the appropriate use of laparoscopy over open procedures in the current COVID-19 climate? J Gastrointest Surg. (2020) 24:1686–91. doi: 10.1007/s11605-020-04592-9
7. De Simone B, Chouillard E, Di Saverio S, Pagani L, Sartelli M, Biffl WL, et al. Emergency surgery during the COVID-19 pandemic: what you need to know for practice. Ann R Coll Surg Engl. (2020) 102:323–32. doi: 10.1308/rcsann.2020.0097
8. Patriti A, Baiocchi GL, Catena F, Marini P, Catarci M. FACS on behalf of the Associazione Chirurghi Ospedalieri Italiani (ACOI). Emergency general surgery in Italy during the COVID-19 outbreak: first survey from the real life. World J Emerg Surg. (2020) 15:36. doi: 10.1186/s13017-020-00314-3
9. Zhang C, Shi L, Wang F-S. Liver injury in COVID-19: management and challenges. Lancet Gastroenterol Hepatol. (2020) 5:428–30. doi: 10.1016/s2468-1253(20)30057-1
10. Tzeng C-WD, Cooper AB, Vauthey J-N, Curley SA, Aloia TA. Predictors of morbidity and mortality after hepatectomy in elderly patients: analysis of 7621 NSQIP patients. HPB. (2014) 16:459–68. doi: 10.1111/hpb.12155
11. Pulitano C, Crawford M, Joseph D, Aldrighetti L, Sandroussi C. Preoperative assessment of postoperative liver function: the importance of residual liver volume. J Surg Oncol. (2014) 110:445–50. doi: 10.1002/jso.23671
12. van den Broek MAJ, Olde Damink SWM, Dejong CHC, Lang H, Malagó M, Jalan R, et al. Liver failure after partial hepatic resection: definition, pathophysiology, risk factors and treatment. Liver Int. (2008) 28:767–80. doi: 10.1111/j.1478-3231.2008.01777.x
13. Torzilli G, Viganò L, Giuliante F, Pinna AD. Liver surgery in Italy. Criteria to identify the hospital units and the tertiary referral centers entitled to perform it. Updat Surg. (2016) 68:135–42. doi: 10.1007/s13304-016-0373-0
14. Dindo D, Demartines N, Clavien P-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. (2004) 240:205–13. doi: 10.1097/01.sla.0000133083.54934.ae
15. Slankamenac K, Graf R, Barkun J, Puhan MA, Clavien P-A. The comprehensive complication index: a novel continuous scale to measure surgical morbidity. Ann Surg. (2013) 258:1–7. doi: 10.1097/SLA.0b013e318296c732
16. Strasberg SM, Phillips C. Use and dissemination of the Brisbane 2000 nomenclature of liver anatomy and resections. Ann Surg. (2013) 257:377–82. doi: 10.1097/SLA.0b013e31825a01f6
17. Carenzo L, Costantini E, Greco M, Barra FL, Rendiniello V, Mainetti M, et al. Hospital surge capacity in a tertiary emergency referral centre during the COVID-19 outbreak in Italy. Anaesthesia. (2020) 75:928–34. doi: 10.1111/anae.15072
18. Yang X, Yu Y, Xu J, Shu H, Xia J‘, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. (2020) 8:475–81. doi: 10.1016/s2213-2600(20)30079-5
19. Yu J, Ouyang W, Chua MLK, Xie C. SARS-CoV-2 transmission in patients with cancer at a tertiary care hospital in Wuhan, China. JAMA Oncol. (2020) 6:1108. doi: 10.1001/jamaoncol.2020.0980
20. European Association for the Study of the Liver. Electronic address:ZWFzbG9mZmljZUBlYXNsb2ZmaWNlLmV1LA== European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. (2018) 69:182–236. doi: 10.1016/j.jhep.2018.03.019
21. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. (2018) 391:1301–14. doi: 10.1016/S0140-6736(18)30010-2
22. Ribaldone DG, Caviglia GP, Gaia S, Rolle E, Risso A, Campion D, et al. Effect of COVID-19 pandemic on hepatocellular carcinoma diagnosis: results from a tertiary care center in North-West Italy. Curr Oncol. (2022) 29:1422–9. doi: 10.3390/curroncol29030119
23. Pomej K, Scheiner B, Hartl L, Balcar L, Meischl T, Mandorfer M, et al. COVID-19 pandemic: impact on the management of patients with hepatocellular carcinoma at a tertiary care hospital. PLoS One. (2021) 16:e0256544. doi: 10.1371/journal.pone.0256544
24. Amaddeo G, Brustia R, Allaire M, Lequoy M, Hollande C, Regnault H, et al. Impact of COVID-19 on the management of hepatocellular carcinoma in a high-prevalence area. JHEP Rep. (2021) 3:100199. doi: 10.1016/j.jhepr.2020.100199
25. Rao A, Rich NE, Marrero JA, Yopp AC, Singal AG. Diagnostic and therapeutic delays in patients with hepatocellular carcinoma. J Natl Compr Canc Netw. (2021) 19:1063–71. doi: 10.6004/jnccn.2020.7689
26. Téllez L, Martín Mateos RM. COVID-19 and liver disease: an update. Gastroenterol Hepatol. (2020) 43:472–80. doi: 10.1016/j.gastrohep.2020.06.006
27. Muñoz-Martínez S, Sapena V, Forner A, Nault J-C, Sapisochin G, Rimassa L, et al. Assessing the impact of COVID-19 on liver cancer management (CERO-19). JHEP Rep. (2021) 3:100260. doi: 10.1016/j.jhepr.2021.100260
28. Balakrishnan A, Lesurtel M, Siriwardena AK, Heinrich S, Serrablo A, Besselink MGH, et al. Delivery of hepato-pancreato-biliary surgery during the COVID-19 pandemic: an European-African Hepato-Pancreato-Biliary Association (E-AHPBA) cross-sectional survey. HPB. (2020) 22:1128–34. doi: 10.1016/j.hpb.2020.05.012
29. Bartlett DL, Howe JR, Chang G, Crago A, Hogg M, Karakousis G, et al. Management of cancer surgery cases during the COVID-19 pandemic: considerations. Ann Surg Oncol. (2020) 27:1717–20. doi: 10.1245/s10434-020-08461-2
30. Quero G, Pecorelli N, Paiella S, Fiorillo C, Petrone MC, Rosa F, et al. Quantitative assessment of the impact of COVID-19 pandemic on pancreatic surgery: an Italian multicenter analysis of 1423 cases from 10 tertiary referral centers. Updates Surg. (2022) 74:255–66. doi: 10.1007/s13304-021-01171-8
31. Aghemo A, Masarone M, Montagnese S, Petta S, Ponziani FR, Russo FP. Assessing the impact of COVID-19 on the management of patients with liver diseases: a national survey by the Italian association for the study of the liver. Dig Liver Dis. (2020) 52:937–41. doi: 10.1016/j.dld.2020.07.008
32. Swan RZ, Sindram D, Martinie JB, Iannitti DA. Operative microwave ablation for hepatocellular carcinoma: complications, recurrence, and long-term outcomes. J Gastrointest Surg. (2013) 17:719–29. doi: 10.1007/s11605-013-2164-y
33. Iavarone M, Sangiovanni A, Carrafiello G, Rossi G, Lampertico P. Management of hepatocellular carcinoma in the time of COVID-19. Ann Oncol. (2020) 31:1084–5. doi: 10.1016/j.annonc.2020.04.007
34. Shiina S, Gani RA, Yokosuka O, Maruyama H, Nagamatsu H, Payawal DA, et al. APASL practical recommendations for the management of hepatocellular carcinoma in the era of COVID-19. Hepatol Int. (2020) 14:920–9. doi: 10.1007/s12072-020-10103-4
35. Bracale U, Silvestri V, Pontecorvi E, Russo I, Triassi M, Cassinotti E, et al. Smoke evacuation during laparoscopic surgery: a problem beyond the COVID-19 period. A quantitative analysis of CO environmental dispersion using different devices. Surg Innov. (2022) 29(2):154–9. doi: 10.1177/15533506211014857
36. Fancellu A, Rosman AS, Sanna V, Nigri GR, Zorcolo L, Pisano M, et al. Meta-analysis of trials comparing minimally-invasive and open liver resections for hepatocellular carcinoma. J Surg Res. (2011) 171:e33–45. doi: 10.1016/j.jss.2011.07.008
37. Choi SH, Kwon TG, Chung SK, Kim T-H. Surgical smoke may be a biohazard to surgeons performing laparoscopic surgery. Surg Endosc. (2014) 28:2374–80. doi: 10.1007/s00464-014-3472-3
38. Serban D, Smarandache CG, Tudor C, Duta LN, Dascalu AM, Aliuș C. Laparoscopic surgery in COVID-19 era-safety and ethical issues. Diagnostics (Basel). (2020) 10:673–88. doi: 10.3390/diagnostics10090673
Keywords: COVID-19, liver surgery, liver disease, pandemic, laparoscopy
Citation: Carissimi F, Scotti MA, Ciulli C, Fogliati A, Uggeri F, Chiarelli M, Braga M, Romano F and Garancini M (2022) COVID-19 and Liver Surgery: How the Pandemic Affected an Italian Medium-Volume HBP Center. Front. Surg. 9:918348. doi: 10.3389/fsurg.2022.918348
Received: 12 April 2022; Accepted: 2 June 2022;
Published: 28 June 2022.
Edited by:
Andrea Laurenzi, IRCCS Azienda Ospedaliero-Universitaria di Bologna, ItalyReviewed by:
Raffaele de Luca, National Cancer Institute (IRCCS), ItalyCopyright © 2022 Carissimi, Scotti, Ciulli, Fogliati, Uggeri, Chiarelli, Braga, Romano and Garancini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabrizio Romano ZmFicml6aW8ucm9tYW5vQHVuaW1pYi5pdA==
Specialty section: This article was submitted to Surgical Oncology, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.