
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Surg. , 31 May 2022
Sec. Visceral Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.916652
 Giovanni Fantola1*
Giovanni Fantola1* Enrico Moroni1Matteo Runfola2
Enrico Moroni1Matteo Runfola2 Emanuele Lai1Stefano Pintus1Pierpaolo Gallucci3
Emanuele Lai1Stefano Pintus1Pierpaolo Gallucci3 Francesco Pennestrì4
Francesco Pennestrì4 Marco Raffaelli4
Marco Raffaelli4
Laparoscopy is the surgical standard of care for bariatric procedures; however, during the last two decades, the robotic approach has gained increasing interest. It is currently considered a safe and effective alternative to laparoscopy. This literature review investigates the role of the robotic approach for primary and revisional bariatric procedures, with the particular aim of comparing this technique with the standard-of-care laparoscopic approach. The feasibility of robotic dissection and suturing could have potential advantages: robotics may prevent the risk of leak and bleeding and other surgical complications, determining potential benefits in terms of operative time, length of hospital stay, and learning curve. Considering primary procedures, the literature reveals no advantages in robotic versus the laparoscopic approach for adjustable gastric banding and sleeve gastrectomy. Robotic Roux-en-Y gastric bypass is associated with a longer operative time and a shorter hospital length of stay than laparoscopy. The robotic approach in revisional surgery has been proven to be safe and effective. Despite the longer operative time, the robotic platform could achieve a lower bleeding rate compared with laparoscopy. The surgeon’s selection criteria related to referrals to the robotic approach of difficult-perceived cases could represent a bias. In conclusion, robotic surgery can be considered a safe and effective approach in both primary and revisional bariatric surgery, despite the lack of evidence to support its routine use in primary bariatric surgery. However, in revisional bariatric surgery and in surgical complex procedures, the robotic approach could have potential benefits in terms of surgical complications and learning curves.
Bariatric surgery has emerged as a safe and effective treatment (1) for morbid obesity, defined as BMI ≥ 40 or BMI ≥ 35 associated with obesity-related diseases. In 2019, 256,000 bariatric surgery operations have been performed in the USA (2), and in 2021, 22,469 bariatric surgery operations have been performed in Italy (3).
Minimally invasive bariatric surgical procedures have been associated with improved early postoperative outcomes in comparison with open approaches, with very low mortality and low morbidity rates (4).
Laparoscopic surgery is currently considered the standard of care in the bariatric surgery approach, as open surgery remains only as a rescue operation or in case of contraindications to laparoscopy. However, advanced laparoscopic skills are required to achieve adequate surgical outcomes after laparoscopic bariatric procedures (5). In some conditions, such as patients with prior abdominal surgery or in complex bariatric procedures, like biliopancreatic diversion with duodenal switch (BPDDS), the laparoscopic approach can be challenging. With this background, the use of the robotic platform in bariatric surgery has been growing over the last two decades (6).
The aim of this review is to assess the current literature about the advantages and disadvantages of primary and revisional robot-assisted bariatric procedures in comparison with the standard-of-care laparoscopic approach.
A systematic literature search was performed on PubMed and Google Scholar. Searched terms included keywords [robotic] [bariatric] [surgery] [davinci] [rygb] [sleeve gastrectomy] [sadi-s] [revisional] [primary]. All titles and abstracts were assessed to select those focusing on robotic bariatric surgery. Subsequently, the full text of the selected trials was independently screened by the authors for eligibility. Inclusion criteria were comparative and non-comparative studies, including patients who underwent primary and revisional robotic bariatric surgery.
For two decades, the robotic platform has offered surgeons better instruments for performing minimally invasive procedures, allowing more difficult procedures to be performed, from esophageal to rectal resections, including bariatric surgery. Technical advantages include tridimensional viewing with a binocular camera, wristed graspers, dissectors, and staplers, providing both improved articulation and rotation, tremor filtering for more precise handling (7), allowing hand-sewn anastomosis (8), resulting in reduced fatigue (9), and improved surgical abilities (10) compared with laparoscopic surgery.
On the other hand, robotic surgery is still a subject of debate because of its longer learning curve, increased costs, and consequently reduced cost-effectiveness.
Indeed, cost is an important drawback in robotic surgery. Costs include robotic platform purchase, instruments with a limited life span, and annual service maintenance (20% of total cost/year). Overall, the DaVinci Robotic Surgical System with dual console and fourth arm costs about 4.5 million Euros on a 7-year pay-off period. Consequently, direct procedural costs are generally higher for robotic bariatric procedures in comparison with conventional laparoscopy. This overcost is on average about 2.3 times more expensive per patient (11). There are several factors that could reduce the cost per patient and improve cost-effectiveness. The number of robotic procedures per year using a specific robotic system may reduce the costs of initial purchase and annual maintenance. It is generally estimated that less than 250 procedures/year is not sufficient for a medical center to rationalize robotic overcosts. Decreasing the length of hospital and ICU stay could also be used to balance the overcosts in comparison with laparoscopic procedures. However, this remains to be proven using clear comparative data, because Bertoni et al. recently demonstrated that robotic surgery is only non-inferior to laparoscopic surgery (12).
In 2000, Sudan et al. described the first case of robotic Sleeve Gastrectomy (SG) as the first part of robotic BPDDS (13). Current data have shown no clear postoperative improvements in comparison with the conventional laparoscopic approach. In this review, we only selected studies including more than 50 patients (Table 1). Romero et al. compared 134 patients who underwent a robotic SG with a systematic review of 3,148 patients after conventional laparoscopic sleeve (14). Sixty-three cases of anastomotic leaks (1.97%), 12 gastric strictures (0.43%), and 34 bleedings (1.21%) in the laparoscopic group were observed. No leak, no stricture, and only one bleeding (0.7%) were observed in the robotic group. The mean surgical time was longer in the robotic group (106 versus 94.5 min). However, the mean hospital stay was significantly shorter in the robotic group (2.2 versus 3.3 days). This study concluded that similar perioperative outcomes were observed in both approaches, although the robotic platform could provide a more comfortable environment for the operating surgeon.
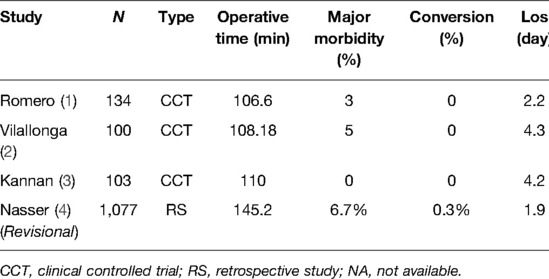
Table 1. Literature review of robotic Sleeve Gastrectomy.
Another comparative study analyzed 100 robotic versus 100 laparoscopic SG (15). It reported three leaks in the robotic group (3%) and four in the laparoscopic group (4%). The mean hospital stay was similar in both groups ranging from 3 to 4 days. This study concluded that the robotic approach was feasible, but cost issues and mean operative times may need to be improved. Kannan et al. (16) reported 108 patients (62 laparoscopic versus 46 robotic SG). This study showed no difference in terms of postoperative complication rates and mean operating time.
In this literature review, we selected six clinical controlled trials, three case series, one systematic review, and one meta-analysis (Table 2). Only published series including more than 50 patients were considered. Ayloo et al. (17) reported a total of 135 RYGB (Roux-en-Y gastric bypass). Among them, 45 RYGB were performed laparoscopically and 90 were robot-assisted. This study showed no difference in terms of postoperative morbidity rates. Intraoperative data also showed a shorter operative time in robotic group patients (207 versus 227 min). Hagen et al. (18) reported 990 patients who underwent a gastric bypass from June 1997 to July 2010. There were 524 open, 323 laparoscopic, and 143 robotic cases. This study concluded that significantly fewer anastomotic complications were observed after open and robotic RYGB (0%) in comparison with laparoscopic RYGB (4.1%). However, this study is associated with potential bias due to its long inclusion period spanning over 13 years.
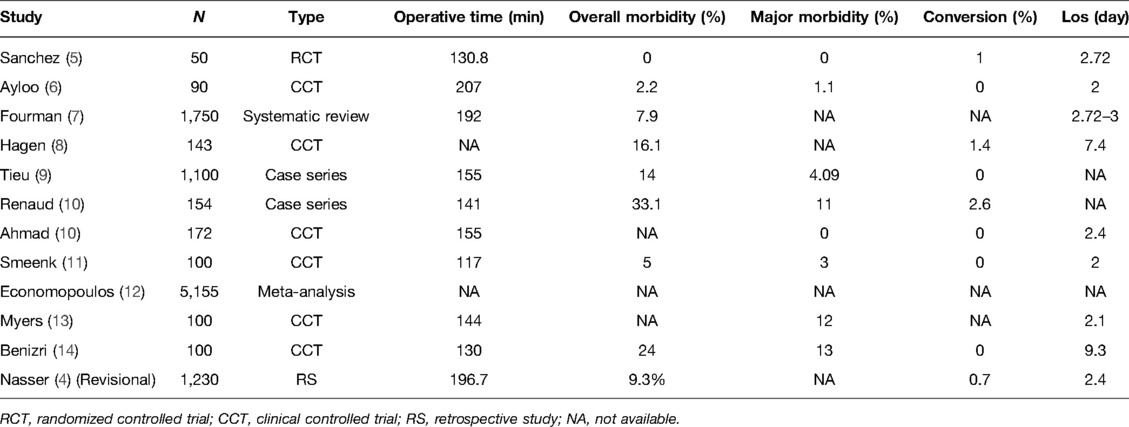
Table 2. Literature review of robotic Roux-en-Y Gastric Bypass.
A review including a total of 18 studies was published by Fourman et al. (19). A total of 1,750 patients was included with a mean operative time of 192 min in robotic versus 173 min in laparoscopic group patients. The postoperative complication rate was similar in both groups (7.9% versus 8.6%). This review concluded that robotic group patients had fewer anastomotic leaks (4 versus 21 patients) and fewer anastomotic strictures (17 versus 40 patients).
In 2013, Benizri et al. (20) reported 200 RYGB performed by two experienced bariatric surgeons (100 robotic versus 100 conventional laparoscopic RYGB). This study showed a significantly higher postoperative morbidity rate in robotic group patients regarding surgical complications (13% versus 1%; p = 0.001). Consequently, more patients had a reoperation (9% versus 1%). However, intraoperative data showed a shorter mean operative time in the robotic group (130 versus 147 min). Overall, the mean hospital stay was longer in the robotic group (9.3 versus 6.7 days, p = 0.001). Later, Ahmad et al. (21) reported 173 laparoscopic versus 172 robotic RYGB procedures. No difference was observed in terms of intraoperative events, conversions to open procedures, leaks, strictures, returns to the operating room within 30 days, and mortality. Smeenk et al. (22) reported 100 laparoscopic versus 100 robotic RYGB procedures. The morbidity rate was 5% in both groups and major morbidity rates (Clavien-Dindo class 3–4) were similar (3% versus 1%; p = 0.62), and there was no mortality. The mean operative room time was 117 min in robotic versus 66 min in laparoscopic group patients (p < 0.05).
Non-comparative series was also used to evaluate robotic RYGB. Tieu et al. (23) included 1,100 patients with robotic RYGB from two high-volume medical centers. The ninety-day major complication rate was 4.09% (45 patients). Fantola et al. analyzed 302 consecutive robotic RYGB. In this study, the 60-day major complication rate (Clavien-Dindo score 3 or 4) and reoperation rate were 12.2% and 10.2%, respectively. Fourteen patients (4.6%) had a postoperative anastomotic leak requiring specific surgical management (24).
Single Anastomosis Duodenal-ileostomy with Sleeve gastrectomy (SADI-S) is a novel surgical technique, emerging from the BDPDDS legacy, aiming to reduce BPDDS risks, while maintaining its efficacy as one of the most effective interventions. It is considered a valid alternative to BPDDS, associated with a lower complication rate (25). It has also usually been considered an alternative to one-anastomosis gastric bypass (OAGB), more challenging from a technical point of view, but associated with a lower risk of complications.
Very few studies reported data from robotic SADI-S procedures. Nelson et al. reported a case series of robotic procedures (also including 10 laparoscopic procedures) and demonstrated that the robotic approach is safe and effective with an acceptable risk–benefit ratio but does not offer a comparison with the laparoscopic or open approach.
In the last few years, the number of reoperative procedures is rapidly increasing, as every year, more and more primary bariatric procedures are performed.
Reoperative bariatric surgery has been classified by Brethauer et al. (26) into the following:
• Conversion: procedures that change from an index procedure to a different type of procedure.
• Corrective: procedures addressing complications or incomplete treatment effect of a previous bariatric operation.
• Reversal: procedures that restore original anatomy.
Insufficient weight loss or weight regain, initial defect or late-surgical complication (e.g., GERD (27)), excessive weight loss, and malnutrition are an indication for revisional bariatric surgery (28) that must be taken into account in a multidisciplinary setting that includes surgical, nutritional, and psychological risks and benefits (29).
Revisional surgery has been associated with poorer outcomes in both RYGB (30), with increased intraoperative blood loss, longer operative time, longer adhesiolysis, longer hospital length of stay, higher rate of splenic injury, anastomotic leakage, and surgical site infections in comparison with primary RYGB, and in revisional SG compared with primary SG (31), with longer operative time, higher complication rate, and anastomotic leakage rate.
Due to increased operative difficulty, because revisional surgery is more challenging and requires a higher level of technical skills, the robotic platform may be considered for better visualization, dissection, and a wider range of movement provided by robotic instruments that could provide a better outcome to bariatric revisional procedures (32).
Clapp et al. (33) systematically analyzed revisional weight loss robotic surgery from the MBSAQIP database spanning from 2015 to 2016 and compared them with laparoscopic revisional procedures. One thousand nine hundred twenty-nine robotic procedures and 35,998 laparoscopic revisional procedures were found. Statistical analysis showed a longer operative time, prolonged hospital length of stay, and higher ICU admission rate in the robotic group than in the laparoscopic group. Other parameters taken into account showed no differences, which led the authors to state that no difference exists in postoperative complications. As a higher number of anastomosis revisions were done in the robotic group, the authors hypothesized that a selection bias could exist, with surgeons preferring robotic surgery in high-difficulty-perceived procedures.
A comparative analysis from Nasser et al. (34) (Tables 1, 2) taking into account procedures from the MBSAQIP database performed between 2015 and 2017 analyzed a series of revisional procedures, comparing the laparoscopic and robotic approaches.
As for revisional SG, 15,935 procedures were laparoscopic and 1,077 were robotic. Demographic characteristics were homogeneous in the two groups, and the authors found differences in terms of longer operative time in the robotic group, higher incidence of intraoperative adhesiolysis in the robotic group, higher incidence of overall morbidity in the robotic group, and higher incidence of ICU admission, sepsis, and organ-space SSI in the robotic group. No differences were found in terms of other parameters.
As for revisional RYGB, 11,212 procedures were laparoscopic and 1,230 were robotic. Demographic characteristics were homogeneous, a higher rate of drainage placement was found in the laparoscopic group, the operative time was longer in the robotic group, respiratory complications, postoperative pneumonia, and superficial SSI were higher in the laparoscopic group, and the incidence of bleeding requiring transfusion was higher in the laparoscopic group. No differences were found in terms of other parameters. Study limitation embraced a possible surgeon’s selection bias, as challenging cases might have been purposely selected for the robotic or laparoscopic group, and the MBSAQIP database provides postoperative data only up to 30 days, from a variety of heterogeneous centers.
Vilallonga et al. (35) presented a 3-case report of robotic revisional SADI-S (36) secondary to SG. In this study (35), the authors conclude the feasibility of robotic revisional SADI-S and its advantages over RYGB, as the Billroth-2 style duodenal-ileal-anastomosis might reduce operative time and postoperative complications.
A single-center study from King et al. (37) including 167 revisional procedures (115 laparoscopic, 52 robotic) demonstrated a reduced major complication rate in the robotic group than in the laparoscopic group (1 [1.9%] versus 6 [5.2%], p > 0.05) and a shorter hospital length of stay in the robotic group than in the other group (40.2 versus 62.6 h, respectively, p < 0.05), with no differences in minor complications, blood loss, and readmission rates.
Rebecchi et al. (38), reporting their results from a single-center study, performed a cost-related analysis of revisional robotic RYGB performed with the DaVinci Robotic Surgical System. The mean cost was found to be 14,334.70€ ± 2,920.40€, but they demonstrated that specific-robot expenses decreased in the last 10 cases of the study (9,708.50€ ± 515.70€) compared with the first 30 cases (12,168.70€ ± 1,438.40€), as the total cost for a laparoscopy procedure was 3,176.50€ ± 850.50€.
The increased costs of the robotic procedure have to be addressed in specific semidisposable instruments and robotic maintenance fees, even though the clinical benefits could overcome increased costs.
Between the period January 2013 and March 2022, over 3,659 bariatric procedures (403—11.6% revisional ones) were performed at the Division of Endocrine and Metabolic Surgery (Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, Italy). Sixty-seven (1.8%) patients were scheduled for a robotic approach. Specifically, 37 RYGB, 23 SADI-S, 6 OAGB, and one BPD were performed.
The first robotic procedure, an RYGB, was performed in January 2013, while the first robotic SADI-S was performed in July 2016. However, the robotic approach was implemented starting from 2019, with a relative reduction in the number of performed procedures during the first phases of the COVID-19 pandemic (2020–2021).
As previously reported, 37 robotic-assisted RYGBs were performed. The median operative time was 201 min. We experienced only one postoperative surgical complication, a gastroenteric anastomotic leak, in a super-super-obese patient (BMI ≥ 60 kg/m2), which required surgical exploration (Clavien-Dindo IIIb). The subsequent postoperative course was uneventful, and the patient was discharged after 14 days.
In addition, 23 SADI-S were performed, in 22 cases as a primary procedure and in 1 case as a revisional operation. Recently, we reported our personal experience (currently under peer review) comparing the robotic and laparoscopic approaches in SADI-S, using propensity score matching analysis to avoid potential bias selection. The median operative time for robotic SADI-S was 191.5 min with the docking step requiring approximately 10 min. Using the CUSUM method to analyze the learning curves of the different approaches (laparoscopic versus robotic) for SADI-S, we observed a significant reduction in operating time after the first seven cases for the robotic SADI-S and after the first 47 cases for the laparoscopic approach. Thus, the use of the robotic platform reduces the time required to complete the learning curve for these challenging procedures. In addition, our analysis highlights that the laparoscopic and robotic approaches for SADI-S are comparable in terms of safety for reoperative and postoperative complications.
Furthermore, we performed six OAGBs (five primary procedures and one revisional) with a median operative time of 191 min. We chose this procedure at the beginning of our experience with the robotic platform in obese patients before the introduction of SADI-S in our clinical practice. For the same reason, we also performed a DPD with an operative time of 240 min.
From July 2021, the Obesity Surgery Unit (ARNAS G. Brotzu, Cagliari, Italy) started a robotic bariatric program. Eight robotic-assisted RYGB were performed. The median operative time was 240 min, with an improvement after the first five cases. One patient was reoperated because of alimentary limb occlusion due to jejuno-jejunal kinking.
Overall, after combining both series, no intraoperative deaths occurred in our robotic experience. No conversion was necessary, either to open or laparoscopic surgery. No 30-day mortality was recorded.
In our experience, the main indications for the robotic approach are challenging for bariatric patients. “Challenging cases” are a clinical characteristic that cannot be assessed by a single parameter but is determined by the presence of one or more of these conditions: patients with a BMI ≥ 50 kg/m2, especially if they are male and/or with a previous major abdominal surgery. Furthermore, according to other authors, we trust that the robotic platform can add value to these patients by reducing the number of two-stage procedures.
Laparoscopy has been the standard of care in choosing a surgical approach in bariatric surgery since the last two decades and has contributed to the large diffusion of bariatric procedures worldwide. In this context, robotic surgery remains controversial.
In our review, we analyzed some of the most performed procedures, considering both primary and revisional procedures, and we observed that in primary surgery, robotic surgery is safe and effective but offers no advantages in perioperative care compared with laparoscopic surgery. However, in revisional surgery, which has a higher rate of postoperative complications due to adhesions and altered anatomy and, therefore, requiring higher laparoscopic skills, the robotic approach could have a primary role. This was proved by Nasser et al. (34), who demonstrated a reduced complication rate in revisional robotic RYGB compared with the laparoscopic approach.
It must also be considered that in most studies taken into account, there was no patient randomization, and patients who were perceived more challenging by the surgeon were assigned to robotic surgery, with a clear selection bias. These obviously included superobese patients (BMI > 50 kg/m2) in whom fine dissection and, especially, suturing could be particularly challenging without the robotic platform. Further studies comparing a similar group of patients, eventually by randomization, are, thus, necessary in order to draw a definitive conclusion in this regard.
On the other hand, as most of the bariatric procedures are performed on a single abdominal quadrant, robotic platform benefits could be less emphasized compared with other surgical fields and have a longer learning curve and longer operative time than laparoscopy (39). However, the authors’ personal experience has demonstrated that the robotic platform is able to reduce the learning curve for a single, complex procedure, as SADI-S does.
Cost-effectiveness has been, since its adoption, one of the main drawbacks in robotic surgery, as DRG reimburses might be insufficient to cover robotic extra costs (40). A cost analysis by Khorgami et al. (41) demonstrated that robotic surgery is the factor associated with the highest impact on extra costs in bariatric surgery.
However, as Hagen et al. (42) demonstrated that laparoscopic staplers might reduce robotic costs compared with robotic staplers, robotic costs can be further mitigated with avoidance of staplers with handsewn anastomosis, which showed a reduced complication rate compared with laparoscopic-stapled anastomosis (18) and, therefore, a further cost mitigation. Moreover, as a robotic platform enhances the surgeon’s ability in sewing compared with laparoscopy, further studies are needed to compare handsewn anastomosis and stapled mechanical anastomosis, considering that handsewn anastomosis is tailored, is opposed to standardized staplers, and the anastomotic stricture rate tends to be lower with a handsewn technique (43), and that could be most useful in complex procedures (i.e., SADI-S).
Most studies found in the current literature were based on the DaVinci Robotic Surgical System, while no data were found in regard to other robotic platforms.
More studies are, however, necessary to address the efficacy and sustainability of the robotic approach, as most studies to date have lacked randomization and, therefore, have a selection bias that has prevented a proper data evaluation. It should also be noted that a fully trained surgeon in robotic bariatric surgery, and, therefore, able to deal with challenging cases intended for robotic surgery, has to complete a learning curve that, especially in the initial stages, cannot be based on challenging cases and, therefore, includes primary bariatric procedures that currently, due to increased costs, are not routinely performed with the robotic platform but with laparoscopy instead.
Robotic surgery remains a valid surgical approach in treating morbid obesity, but, because of its inflated costs, it cannot be a first-choice option as its advantages over laparoscopy are restricted to surgeon ergonomics and not to patient perioperative care and, therefore, it is not financially sustainable. However, in selected cases, including revisional cases and superobese patients, robotic surgery could have a potential role in reducing postoperative complications and improving perioperative care, and, therefore, it also could be economically sustainable.
GF contributed to primary procedures, EL, MR, SP, EM, FP, and PG contributed to introduction, revisional procedures, and discussion, and MR reviewed the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Arterburn DE, Telem DA, Kushner RF, Courcoulas AP. Benefits and risks of bariatric surgery in adults: a review. JAMA. (2020) 324:879–87. doi: 10.1001/jama.2020.12567
2. Estimate of Bariatric Surgery Numbers, 2011–2019. American Society for Metabolic and Bariatric Surgery (2021). Available from: https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers (Accessed December 29, 2021).
3. SICOB. Indagine conoscitiva anno 2021. Soc Ital Chir Dell Obesità (2022). Available from: https://www.sicob.org/00_allegati_news/indagine_2021.pdf (Accessed February 16, 2022).
4. DeMaria EJ, Pate V, Warthen M, Winegar DA. Baseline data from American society for metabolic and bariatric surgery-designated bariatric surgery centers of excellence using the bariatric outcomes longitudinal database. Surg Obes Relat Dis Off J Am Soc Bariatr Surg. (2010) 6:347–55. doi: 10.1016/j.soard.2009.11.015
5. Wilson EB, Sudan R. The evolution of robotic bariatric surgery. World J Surg. (2013) 37:2756–60. doi: 10.1007/s00268-013-2125-3
6. Antanavicius G, Mohammed R, Van Houtte O. Total robotic biliopancreatic diversion with duodenal switch technique. Obes Surg. (2017) 27:1104–8. doi: 10.1007/s11695-016-2513-5
7. Vining CC, Skowron KB, Hogg ME. Robotic gastrointestinal surgery: learning curve, educational programs and outcomes. Updat Surg. (2021) 73:799–814. doi: 10.1007/s13304-021-00973-0
8. Jiang H-P, Lin L-L, Jiang X, Qiao H-Q. Meta-analysis of hand-sewn versus mechanical gastrojejunal anastomosis during laparoscopic Roux-en-Y gastric bypass for morbid obesity. Int J Surg. (2016) 32:150–7. doi: 10.1016/j.ijsu.2016.04.024
9. Aitchison LP, Cui CK, Arnold A, Abbott J. The ergonomics of laparoscopic surgery in live surgical environments. J Minim Invasive Gynecol. (2015) 22:S105. doi: 10.1016/j.jmig.2015.08.283
10. Moorthy K, Munz Y, Dosis A, Hernandez J, Martin S, Bello F, et al. Dexterity enhancement with robotic surgery. Surg Endosc Interv Tech. (2004) 18:790–5. doi: 10.1007/s00464-003-8922-2
11. Myers SR, McGuirl J, Wang J. Robot-assisted versus laparoscopic gastric bypass: comparison of short-term outcomes. Obes Surg. (2013) 23:467–73. doi: 10.1007/s11695-012-0848-0
12. Bertoni MV, Marengo M, Garofalo F, Volontè F, La Regina D, Gass M, et al. Robotic-assisted versus laparoscopic revisional bariatric surgery: a systematic review and meta-analysis on perioperative outcomes. Obes Surg. (2021) 31:5022–33. doi: 10.1007/s11695-021-05668-4
13. Sudan R, Puri V, Sudan D. Robotically assisted biliary pancreatic diversion with a duodenal switch: a new technique. Surg Endosc. (2007) 21:729–33. doi: 10.1007/s00464-006-9171-y
14. Romero RJ, Kosanovic R, Rabaza JR, Seetharamaiah R, Donkor C, Gallas M, et al. Robotic sleeve gastrectomy: experience of 134 cases and comparison with a systematic review of the laparoscopic approach. Obes Surg. (2013) 23:1743–52. doi: 10.1007/s11695-013-1004-1
15. Vilallonga R, Fort JM, Caubet E, Gonzalez O, Armengol M. Robotic sleeve gastrectomy versus laparoscopic sleeve gastrectomy: a comparative study with 200 patients. Obes Surg. (2013) 23:1501–7. doi: 10.1007/s11695-013-1039-3
16. Kannan U, Ecker BL, Choudhury R, Dempsey DT, Williams NN, Dumon KR. Laparoscopic hand-assisted versus robotic-assisted laparoscopic sleeve gastrectomy: experience of 103 consecutive cases. Surg Obes Relat Dis Off J Am Soc Bariatr Surg. (2016) 12:94–9. doi: 10.1016/j.soard.2015.07.011
17. Ayloo SM, Addeo P, Buchs NC, Shah G, Giulianotti PC. Robot-assisted versus laparoscopic Roux-en-Y gastric bypass: is there a difference in outcomes? World J Surg. (2011) 35:637–42. doi: 10.1007/s00268-010-0938-x
18. Hagen ME, Pugin F, Chassot G, Huber O, Buchs N, Iranmanesh P, et al. Reducing cost of surgery by avoiding complications: the model of robotic roux-en-Y gastric bypass. Obes Surg. (2012) 22:52–61. doi: 10.1007/s11695-011-0422-1
19. Fourman MM, Saber AA. Robotic bariatric surgery: a systematic review. Surg Obes Relat Dis Off J Am Soc Bariatr Surg. (2012) 8:483–8. doi: 10.1016/j.soard.2012.02.012
20. Benizri EI, Renaud M, Reibel N, Germain A, Ziegler O, Zarnegar R, et al. Perioperative outcomes after totally robotic gastric bypass: a prospective nonrandomized controlled study. Am J Surg. (2013) 206:145–51. doi: 10.1016/j.amjsurg.2012.07.049
21. Ahmad A, Carleton JD, Ahmad ZF, Agarwala A. Laparoscopic versus robotic-assisted Roux-en-Y gastric bypass: a retrospective, single-center study of early perioperative outcomes at a community hospital. Surg Endosc. (2016) 30:3792–6. doi: 10.1007/s00464-015-4675-y
22. Smeenk RM, van 't Hof G, Elsten E, Feskens PGBM. The results of 100 robotic versus 100 laparoscopic gastric bypass procedures: a single high volume centre experience. Obes Surg. (2016) 26:1266–73. doi: 10.1007/s11695-015-1933-y
23. Tieu K, Allison N, Snyder B, Wilson T, Toder M, Wilson E. Robotic-assisted Roux-en-Y gastric bypass: update from 2 high-volume centers. Surg Obes Relat Dis Off J Am Soc Bariatr Surg. (2013) 9:284–8. doi: 10.1016/j.soard.2011.11.022
24. Fantola G, Nguyen-Thi PL, Reibel N, Sirveaux MA, Germain A, Ayav A, et al. Risk factors for postoperative morbidity after totally robotic gastric bypass in 302 consecutive patients. Obes Surg. (2015) 25:1229–38. doi: 10.1007/s11695-014-1530-5
25. Pennestrì F, Sessa L, Prioli F, Salvi G, Gallucci P, Ciccoritti L, et al. Single anastomosis duodenal-ileal bypass with sleeve gastrectomy (SADI-S): experience from a high-bariatric volume center. Langenbecks Arch Surg. (2022). doi: 10.1007/s00423-022-02501-z
26. Brethauer SA, Kothari S, Sudan R, Williams B, English WJ, Brengman M, et al. Systematic review on reoperative bariatric surgery: American society for metabolic and bariatric surgery revision task force. Surg Obes Relat Dis. (2014) 10:952–72. doi: 10.1016/j.soard.2014.02.014
27. Clapp B, Wynn M, Martyn C, Foster C, O’Dell M, Tyroch A. Long term (7 or more years) outcomes of the sleeve gastrectomy: a meta-analysis. Surg Obes Relat Dis. (2018) 14:741–7. doi: 10.1016/j.soard.2018.02.027
28. Bion AL, Le Roux Y, Alves A, Menahem B. Bariatric revisional surgery: what are the challenges for the patient and the practitioner? J Visc Surg. (2021) 158:38–50. doi: 10.1016/j.jviscsurg.2020.08.014
29. Vilallonga R, Fort JM, Rodríguez Luna MR, García Ruiz de Gordejuela A, Gonzalez O, Caubet E, et al. The panoramic view of revisional bariatric surgery. J Laparoendosc Adv Surg Tech. (2022) 32:6–11. doi: 10.1089/lap.2021.0506
30. Zhang L, Tan WH, Chang R, Eagon JC. Perioperative risk and complications of revisional bariatric surgery compared to primary Roux-en-Y gastric bypass. Surg Endosc. (2015) 29:1316–20. doi: 10.1007/s00464-014-3848-4
31. Mahawar KK, Graham Y, Carr WRJ, Jennings N, Schroeder N, Balupuri S, et al. Revisional roux-en-Y gastric bypass and sleeve gastrectomy: a systematic review of comparative outcomes with respective primary procedures. Obes Surg. (2015) 25:1271–80. doi: 10.1007/s11695-015-1670-2
32. Vilallonga R, Cirera de Tudela A, Möller EG, Piñeiro LV, Segura MB, Ferreruela MP, et al. Robotic revisional experience. single centre prospective cohort study and review of the literature. Chir Buchar Rom 1990. (2021) 116:7–15. doi: 10.21614/chirurgia.116.1.7
33. Clapp B, Liggett E, Jones R, Lodeiro C, Dodoo C, Tyroch A. Comparison of robotic revisional weight loss surgery and laparoscopic revisional weight loss surgery using the MBSAQIP database. Surg Obes Relat Dis. (2019) 15:909–19. doi: 10.1016/j.soard.2019.03.022
34. Nasser H, Munie S, Kindel TL, Gould JC, Higgins RM. Comparative analysis of robotic versus laparoscopic revisional bariatric surgery: perioperative outcomes from the MBSAQIP database. Surg Obes Relat Dis. (2020) 16:397–405. doi: 10.1016/j.soard.2019.11.018
35. Vilallonga R, Fort JM, Caubet E, Gonzalez O, Balibrea JM, Ciudin A, et al. Robotically assisted single anastomosis duodenoileal bypass after previous sleeve gastrectomy implementing high valuable technology for complex procedures. J Obes. (2015) 2015:1–6. doi: 10.1155/2015/586419
36. Sánchez-Pernaute A, Rubio Herrera MA, Pérez-Aguirre E, García Pérez JC, Cabrerizo L, Díez Valladares L, et al. Proximal duodenal–ileal end-to-side bypass with sleeve gastrectomy: proposed technique. Obes Surg. (2007) 17:1614–8. doi: 10.1007/s11695-007-9287-8
37. King K, Galvez A, Stoltzfus J, Claros L, El Chaar M. Robotic-assisted surgery results in a shorter hospital stay following revisional bariatric surgery. Obes Surg. (2021) 31:634–9. doi: 10.1007/s11695-020-05022-0
38. Rebecchi F, Ugliono E, Allaix ME, Toppino M, Borello A, Morino M. Robotic roux-en-Y gastric bypass as a revisional bariatric procedure: a single-center prospective cohort study. Obes Surg. (2020) 30:11–7. doi: 10.1007/s11695-019-04117-7
39. Addison P, Yoo A, Duarte-Ramos J, Addy J, Dechario S, Husk G, et al. Correlation between operative time and crowd-sourced skills assessment for robotic bariatric surgery. Surg Endosc. (2021) 35:5303–9. doi: 10.1007/s00464-020-08019-z
40. Mühlmann G, Klaus A, Kirchmayr W, Wykypiel H, Unger A, Höller E, et al. DaVinci robotic-assisted laparoscopic bariatric surgery: is it justified in a routine setting? Obes Surg. (2003) 13:848–54. doi: 10.1381/096089203322618632
41. Khorgami Z, Aminian A, Shoar S, Andalib A, Saber AA, Schauer PR, et al. Cost of bariatric surgery and factors associated with increased cost: an analysis of national inpatient sample. Surg Obes Relat Dis. (2017) 13:1284–9. doi: 10.1016/j.soard.2017.04.010
42. Hagen ME, Jung MK, Fakhro J, Buchs NC, Buehler L, Mendoza JM, et al. Robotic versus laparoscopic stapling during robotic Roux-en-Y gastric bypass surgery: a case-matched analysis of costs and clinical outcomes. Surg Endosc. (2018) 32:472–7. doi: 10.1007/s00464-017-5707-6
Keywords: robotic surgery, daVinci, revisional surgery, gastric bypass, SADIS
Citation: Fantola G, Moroni E, Runfola M, Lai E, Pintus S, Gallucci P, Pennestrì F and Raffaelli M (2022) Controversial Role of Robot in Primary and Revisional Bariatric Surgery Procedures: Review of the Literature and Personal Experience. Front. Surg. 9:916652. doi: 10.3389/fsurg.2022.916652
Received: 9 April 2022; Accepted: 2 May 2022;
Published: 31 May 2022.
Edited by:
Francesco Frattini, ASST Sette Laghi, ItalyReviewed by:
Ramon Vilallonga, Vall d’Hebron University Hospital, SpainCopyright © 2022 Fantola, Moroni, Runfola, Lai, Pintus, Gallucci, Pennestrì and Raffaelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giovanni Fantola Z2lvdmFubmlmYW50b2xhQGFvYi5pdA==
Specialty section: This article was submitted to Visceral Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.