 J. Rosendorf
J. Rosendorf M. Klicova3
M. Klicova3 I. Herrmann
I. Herrmann V. Liska
V. Liska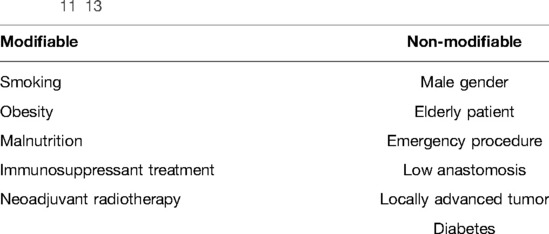

95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Surg. , 07 June 2022
Sec. Visceral Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.904810
This article is part of the Research Topic Anastomotic and Intestinal Wound Healing: Recent advances and future directions View all 11 articles
Colorectal surgery has developed rapidly in the recent decades. Nevertheless, colorectal anastomotic leakage continues to appear postoperatively in unpleasant rates and leads to life-threatening conditions. The development of valid complication-preventing methods is inefficient in many aspects as we are still lacking knowledge about the basics of the process of anastomotic wound healing in the gastrointestinal tract. Without the proper understanding of the crucial mechanisms, research for prevention of anastomotic leakage is predestined to be unsuccessful. This review article discusses known pathophysiological mechanisms together with the most lately found processes to be further studied. The aim of the article is to facilitate the orientation in the topic, support the better understanding of known mechanisms and suggest promising possibilities and directions for further research.
Colorectal surgery has developed rapidly in the recent decades. Many new techniques have been introduced lately and the perioperative care keeps changing quite agilely (1–3). Milestones have been taken towards better oncological outcomes, minimally invasive procedures, and improved postoperative quality of life (QoL). Individualized care and the role of the patient’s opinion on their treatment based on their good information and insight into the topic come to the fore. However, this article will discuss the unresolved issues in colorectal surgery, which raise questions not only in this specialization, but across gastrointestinal surgery in its full spectrum.
An essential part of gastrointestinal surgery is a construction of an anastomosis. The concept of resection and reconnection of the hollow parts of the tract is one of the cornerstones of visceral surgery and as such is not expected to be overcome or replaced by other treatment modalities in the foreseeable future.
Just as any other surgical procedure, this one has its specific complications as well. The dreaded anastomotic leak (AL), or dehiscence of the anastomosis, comes to mind first. It is a severe complication that requires a tailored approach depending on its severity. It poses a threat to the patient’s life in the early postoperative period, in many cases requires reoperation, and it is the cause of both longer hospitalizations and reduced postoperative QoL, altogether higher medical care expenses, and according to some studies even worse oncological results (4).
Anastomotic strictures or fistulae are other complications that can occur quite often (5). Strictures, in contrast to leaks, develop over a period of months, so patients are at risk of developing them after they have been placed in home care. In many cases, such stricture may be endoscopically affected, however, a large proportion of patients undergo eventually an additional surgery with resection of the stenotic section of the intestine and are thus again exposed to the risks of major surgical procedure (and risk of stoma for acute procedures) (5, 6). A relatively large number of experimental studies have been performed to find the optimal means to prevent these complications (7, 8). However, few will receive the transfer to clinical medicine.
This article aims to analyze current views on gastrointestinal anastomosis healing and its disorders, to develop the boundaries of these different approaches, the current state of knowledge and to outline areas for further research. The secondary intent of this work is also to draw attention to the fact that, however appealing it may appear to be, hopes for clinical success of current leak prevention research are modest.
The essence of the development of the complications mentioned above are disorders of the healing process. Because the healing process is very complex, the specific cause of the pathology can be located on a wide range of levels (9, 10).
Our current view on the prevention or eventual elimination of these complications relies on the identification of risk factors identified by the correlation of known information about patients with their postoperative course. Based on these data, patients are stratified according to the risk of these complications and appropriate precautions are performed on patients assessed as being at risk (11).
The problem is that we are only able to distinguish AL risk markers for standardly evaluated data. Very broad units such as the presence of immunosuppression, diabetes, old age or male sex thus become markers of high AL risk (Table 1) (11). Such large units in the planning of treatment modalities (Hartman’s resection, protective ileostomies, etc.) are difficult to grasp. Stratification is inaccurate and only some patients benefit from it. We assume AL occurs from a combination of healing abnormalities based on several factors that negatively affect the whole healing process.
At present, the process of skin wound healing, including some pathological conditions, is relatively well described (14). However, a similar depth of knowledge is on the digestive tract our utopia. The process is not well documented even in its physiological nature, and certainly the basis of individual pathophysiological deviations is well not researched either (10). Several important points emerge from this statement:
1. Although we know some, we do not know all the risk factors
2. The stratification of patients according to risk is therefore far from being perfect
3. We do not have the opportunity to effectively intervene in the healing process based on its knowledge
4. Applied research in the field of means to prevent anastomotic leakage is in many cases untargeted and ineffective
The degree of unexploredness of such a basic process is an unusual vacuum in scientific knowledge, and the knowledge of the human body.
Before we make the leap into the unexplored, we will introduce the following text with a short discussion about some known pathophysiological mechanisms:
Blood supply is a key basis not only for the healing process but also for maintaining the vitality of any tissue. Depending on the subtlety of the surgical technique and the condition of the patient’s vascular anatomy and disease, the blood supply to the tissues may be compromised in the terrain of surgery. However, the presence of a sufficient blood supply is a generally valid condition not only to enable any healing process, but also to maintain tissue vitality in any other location. Lacking new information, the frequent research goal is to develop means both for perioperative evaluation of the quality of blood circulation and means to improve the regional blood supply to the anastomosed intestinal tissues. In the first of these, great progress has been made with the introduction of protocols involving the intravenous administration of indocyanine green (ICG) (15). Depending on the quality and speed of ICG distribution to the tissues of the anastomotic intestine, it is then possible to decide on a modification of the resection line. According to published works, individual protocols have the potential to reduce the incidence of anastomotic leakage by tens of percent (16). However, even such a refined technique has not contributed fully to elimination of this complication.
Another specific aspect comes to light especially in colorectal surgery. The results of both experimental and some clinical works show the association of the anastomotic leak with infection or colonization of the patient by typical bacterial strains (17). The anastomotic leak caused by the dehiscence of the intestinal anastomosis is certainly an infectious complication, however, the medical society has generally not accepted (at least until recently) the thought that the anastomotic leak is a complication caused by the infection. According to published works, this infection is either a direct cause of leakage development or at least a significant contributor if it develops over an existing healing disorder (17). Pseudomonas Aeruginosa or Streptococcus Faecalis belong among those risk associated pathogens (18, 19). The mechanism of the anastomotic dehiscence lays in the bacterial ability of production of special enzymes consuming newly formed connective tissue of the forming scar – bacterial collagenases (17). These were however identified also in other bacterial strains. If we keep in mind that the basis of collagenase production are bacterial plasmids, which bacteria can share across strains, it may be practically impossible to identify all risky bacterial strains. The second way of negative bacterial influence on the connective tissues of the intestinal anastomosis is mediated by human collagenases, where the bacteria do not produce collagenase itself, but a human collagenase activator, which acts locally by breaking down collagen fibers in a similar way as bacterial collagenases. Bacterial activator of matrix metalloproteinase 9 can play such role (20). During the process of formation the collagen-rich extracellular matrix is degraded by these enzymes. This can lead to mechanical weakness of the anastomosis or even dehiscence (20).
As stated before, today’s knowledge about intestinal anastomotic healing is limited (10). Wound healing is a process probably far more complex than we describe it by today’s view. Many works rely on similarities between the cutaneous wound healing and anastomotic wound healing. This is despite the fact these are completely different organs, located in a completely different environment of the human body. These organs differ in their morphology, representation of individual cell types, blood supply, type of function, etc. While monitoring skin healing is less technically demanding both in the clinical environment as well as in the experiment, direct monitoring of intestinal anastomosis healing inside the abdomen is at least for now, practically impossible. In addition, the intestinal wall consists of several completely different layers, where we can say with certainty that the contribution of each of them to a successful healing process is different, while the essence of the proper function of one of the layers is not to adhere to anything (the mucosa). Pathology in the process of peritoneal healing can form extensive peritoneal adhesions, at the level of the muscular layer, pseudodiverticula may form, and if the process of healing of the intestinal mucosa is altered, fistulas may develop (21). On the other hand, the large intestine is able to heal despite contamination by common feculent flora, while essentially any contamination of a similar type leads to a purulent complication in the skin wound.
The small and the large intestines comprise many different cell types that are also specific for the location on the gastrointestinal tract. The current histological view recognizes in both the small and the large intestine four basic morphological layers: serosa, muscularis, submucosa and mucosa. However, these can be divided into even more units, and even these have their morphological variations depending on the level on the gastrointestinal tract. This situation is the reason why it is so complicated to describe the whole process, including its pathophysiological abnormalities, and why no one has yet been able to describe it in full scale (10).
It is practically impossible to create a comprehensive study monitoring all cell types and their metabolic changes in the healing process at once. Thus, although projects focusing on individual small aspects of the process, such as research into the effects of transient ischemia on peritoneal fibroblast metabolism, have received little attention and often little success in terms of financial support, they are the only means to push forward our current view on the issues of physiology and pathophysiology and the possibility of influencing the healing process in the digestive tract in a targeted matter.
Given the above lack of knowledge, we are not sure which cells, or which intestinal wall layers are the most important for the healing process, or if the interplay of individual layers in the whole process is essential.
The wound healing process is traditionally divided into several overlapping phases for the purpose of simplification: hemostasis, inflammation, proliferation, and remodeling phase (22) by the todays view. The initial three phases form together the acute period which is important for the possible development of anastomotic leakage. However, subtle disbalance can cause problems in the following period resulting in the healing pathologies as anastomotic strictures or fistulae formation.
We propose several issues appearing lately in the literature, that should be studied further for each intestinal layer to resolve some key questions about the healing process. These research topics are just the tip of the iceberg which is the yet to be discovered:
The peritoneum: The healing capacity of peritoneum is enormous (23). Most of the relevant known pathophysiological processes are described in studies focusing on the problematics of postoperative formation of extensive peritoneal adhesions, and not on the problematics of insufficient peritoneal healing. However, both processes start with peritoneal injury followed by inflammation.
A wide range of experimental models were created for the study of peritoneal adhesions, in which not only anti-adhesion agents were systematically verified, but also the very nature of their formation: patient related factors, perioperative factors, influence of surgical techniques on morphology, amount and properties of adhesions (24). The role of molecular factors, cytokines, in the cellular metabolism of peritoneal cells is also being discussed relatively deeply.
Because peritoneal adhesions have been studied extensively, also the peritoneal injury process that precedes the formation of adhesions is well described. The injured surface starts producing a thin fluid which is rich in many proteins and signal molecules as well as inflammatory and other cells (25). This fluid coagulates within 3 h and thus it ensures stable contact of the two peritoneal surfaces. A process of fibrinolysis takes place at the same time and inhibits the formation of adhesion in normal peritoneal healing within the first 72 h after the injury (25). A prolonged persistence (3–5 days) of this coagulated mass is needed for fibroblasts to migrate in it and start producing the extracellular matrix and other substances. This new scaffold is afterwards occupied by mesothelial cells (26, 27). Healthy peritoneum has fibrinolytic activity (prevents obliteration of abdominal cavity in normal circumstances), which can be however decreased in different situations (hypoxia, injury, infection, etc.) leading to adhesion formation (28).
In the formation of peritoneal adhesions, a permanent transformation of peritoneal fibroblasts into so called adhesion fibroblasts was described. It is a change causing increase in proliferation and deposition of collagenous fiber rich extracellular matrix. A variety of signal molecules play their role in regulation of this process but the pathways leading to adhesions formation seem to have common triggers, which are ischemia, hypoxia, and hypercapnia etc. (26, 27, 29). The changes are described as permanent on the cellular level.
The biological role of the peritoneum appears to be relatively clear in the injury: with the highest priority, it is necessary to prevent perforation of the gastrointestinal tract into the free space of the abdominal cavity. Factors such as localized incomplete tissue hypoxia, hypercapnia, or other local markers of cell damage are thus triggers for the proliferation of peritoneum cells and the production of connective tissue to an intense extent, which seems to hastily prevent an acute threat. A long-term disadvantage of the process is that it is a probable cause of over-deposition of collagen-rich connective tissue, for example in the construction of gastrointestinal anastomosis, and thus contributes to stricture formation.
Dysregulation of these molecular factors has been described in the literature to be triggered by local ischemia: Tissue plasminogen activator (tPA), Transforming growth factor-β1 (TGF-β1), Tumor necrosis factor α (TNF-α), Interleukin 6 (IL-6), Matrix metalloproteinases (MMPs), Cyclo-oxygenases (COX) (30–38). However, the aim of this article is not to describe individual events that are relatively complex, so we recommend the cited literature for a deeper study.
Isolated defects of muscular layer can be seen in imperfectly healed anastomoses as fistulae or can form a pseudodiverticula when the peritoneal surface maintains integrity. However, fistulas are more suspicious of being a mucosal healing imperfection. The hypertrophy of the muscular layer is not usually recognized in intestinal anastomoses but often in patients with chronic inflammatory bowel disease, where it is responsible for intestinal wall thickening and formation of strictures. A state of chronic inflammation with constant production of inflammatory signal molecules and infiltration by inflammatory cells causes a change of metabolism of smooth muscle cells (SMCs). The SMCs gain proliferative ability and start producing extracellular matrix (ECM) (39, 40). The role of ischemia on the SMCs was not described though, and the effect of inflammatory cytokines on SMCs in the process of anastomotic healing is unknown as well. This is certainly material for further basic research.
The submucosa is the layer that is known to be the mechanically strongest. The fact that it contains a lot of collagen rich ECM makes most of clinicians suppose it is the most important layer for optimal anastomotic healing (41). Yet it is not known whether it really is activated in the process of anastomotic healing in sufficient amount to regain mechanical strength in time. And moreover, there is yet no proof suggesting that mechanical strength can be relied on in intestinal anastomosis and there is a probability that there is no link between anastomotic leakage risk and the mechanical strength. The metabolism of the submucosal tissue has not been studied thoroughly neither in normal circumstances nor after injury. Further basic research needs to be conducted urgently.
Intestinal epithelial cells belong among the most rapidly proliferating cells in human body. In normal situation thousands of cells are scrubbed from the mucosal surface by food passage every day. Mature enterocytes however do not have any proliferative capacity and so the mucosal renewal depends on proliferation and differentiation of stem cells located in intestinal crypts. They are responsible for re-epithelization when it comes to anastomotic healing as the mature enterocytes cannot regain this ability. Epithelial mesenchymal transition is a healing associated cellular transformation responsible for de-differentiation of mature epithelial cells and for their regain of the proliferative activity. Newly formed epithelial cells keep covering denuded luminal surface, but do not adhere to epithelized surfaces (One of the basic biological assumptions is that the mucosa must not grow another mucosa surface to surface in order to avoid loss of intestinal lumina). It has been described that the process of superficial proliferation is probably responsible for fistulae formation in patients with anorectal inflammatory bowel disease (42–44), whether the process is behind fistulae formation in case of intestinal and bowel anastomosis is not confirmed, but the mechanisms could be similar. The epithelium is not considered to participate in formation of anastomotic strictures, but not enough research has been conducted to rule out even this assumption.
An interesting view that has not been sufficiently explored is also the importance of barrier function of the mucosa and its loss from intestinal injury, the process of its regeneration, the factors that affect it, and last but not least, how this loss affects the metabolism of the remaining gastrointestinal wall. The basis for the loss of this function is, among other mechanisms, a disorder of tight junctions between enterocytes. It occurs, for example, in septic conditions, where it is another probable contributor to the healing disorder (45). The barrier function suffers also during diarrheic diseases and can be altered also by aggressive laxatives that are used for mechanical bowel preoperative preparation (46).
At present, we have the advantage of the existence of advanced laboratory methods that allow us to observe both metabolic and proliferative changes of individual cells of the gastrointestinal wall, as well as their dynamics and mutual interaction. It is necessary to maximize the use of these auxiliary methods in combination with a clinically relevant experimental model of gastrointestinal healing, both in physiological conditions and to compare these processes with processes taking place in the presence of pathological changes, factors negatively affecting the healing process.
There are many unanswered questions in the process of gastrointestinal healing. Only a thorough research of partial processes, changes at the level of cellular metabolism, at the level of individual layers of the gastrointestinal tract wall, the dynamics of these processes and their interactions under both physiological and pathophysiological conditions can contribute to advances in clinical visceral surgery and other targeted prevention of anastomotic complications including leaks and stenoses. Even though new methods and techniques are emerging in colorectal surgery, the anastomotic leakage continues to haunt us. New technologies allow us to create new kinds of materials for both local or systemic treatment, but not knowing the physiological process and its pathological changes means not knowing what we treat.
Conceptualization: J.R., V.L., V.T.; methodology: I.H., L.C., writing original draft: J.R., M.K., formal analysis: V.L., A.A., R.P., V.T. All authors contributed to the article and approved the submitted version.
The research was funded by the project Czech health research council project AZV NU20J-08-00009 Prevention of intestinal anastomotic leakage and postoperative adhesions by using nanofibrous biodegradable materials, and by European Regional Development Fund-Project AMTMI No. CZ.02.1.01/0.0/0.0/17_048/0007280, grant UNCE/MED006 Center of Excellence (Charles University “Center of Clinical and Experimental Liver Surgery”).
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rentsch M, Schiergens T, Khandoga A, Werner J. Surgery for colorectal cancer - trends, developments, and future perspectives. Visc Med. (2016) 32(3):184–91. doi: 10.1159/000446490
2. Daher R, Chouillard E, Panis Y. New trends in colorectal surgery: single port and natural orifice techniques. World J Gastroenterol. (2014) 20(48):18104–20. doi: 10.3748/wjg.v20.i48.18104.25561780
3. Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for perioperative care in elective colorectal surgery: enhanced recovery after surgery (ERAS®) society recommendations: 2018. World J Surg. (2019) 43(3):659–95. doi: 10.1007/s00268-018-4844-y.30426190
4. Lee SW, Gregory D, Cool CL. Clinical and economic burden of colorectal and bariatric anastomotic leaks. Surg Endosc. (2019). doi: 10.1007/s00464-019-07210-1.
5. Clifford RE, Fowler H, Manu N, Vimalachandran D. Management of benign anastomotic strictures following rectal resection: a systematic review. Colorectal Dis. (2021) 23(12):3090–100. doi: 10.1111/codi.15865
6. Acar T, Aslan F, Acar N, Kamer E, Ünsal B, Hacıyanlı M. Role of endoscopic interventions and electroincision in benign anastomotic strictures following colorectal surgery. Turk J Gastroenterol. (2019) 30(8):673–9. doi: 10.5152/tjg.2019.18673
7. Rosendorf J, Klicova M, Cervenkova L, Horakova J, Klapstova A, Hosek P, et al. Reinforcement of colonic anastomosis with improved ultrafine nanofibrous patch: experiment on pig. Biomedicines. (2021) 9(2):102. doi: 10.3390/biomedicines9020102
8. Yauw ST, Wever KE, Hoesseini A, Ritskes-Hoitinga M, van Goor H. Systematic review of experimental studies on intestinal anastomosis. Br J Surg. (2015) 102(7):726–34. doi: 10.1002/bjs.9776
9. Thornton FJ, Barbul A. Healing in the gastrointestinal tract. Surg Clin North Am. (1997) 77(3):549–73. doi: 10.1016/s0039-6109(05)70568-5
10. Bosmans JW, Jongen AC, Bouvy ND, Derikx JP. Colorectal anastomotic healing: why the biological processes that lead to anastomotic leakage should be revealed prior to conducting intervention studies. BMC Gastroenterol. (2015) 15:180. doi: 10.1186/s12876-015-0410-3
11. McDermott FD, Heeney A, Kelly ME, Steele RJ, Carlson GL, Winter DC. Systematic review of preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks. Br J Surg. (2015) 102(5):462–79. doi: 10.1002/bjs.9697
12. Vasiliu EC, Zarnescu NO, Costea R, Neagu S. Review of risk factors for anastomotic leakage in colorectal surgery. Chirurgia (Bucur). (2015) 110(4):319–2626305194
13. Zarnescu EC, Zarnescu NO, Costea R. Updates of risk factors for anastomotic leakage after colorectal surgery. Diagnostics (Basel). (2021) 11(12):2382. doi: 10.3390/diagnostics1112238
14. Rodrigues M, Kosaric N, Bonham CA, Gurtner GC. Wound healing: a cellular perspective. Physiol Rev. (2019) 99(1):665–706. doi: 10.1152/physrev.00067.2017
15. Safiejko K, Tarkowski R, Kozlowski TP, Koselak M, Jachimiuk M, Tarasik A, et al. Safety and efficacy of indocyanine green in colorectal cancer surgery: a systematic review and meta-analysis of 11,047 patients. Cancers (Basel). (2022) 14(4):1036. doi: 10.3390/cancers14041036
16. Blanco-Colino R, Espin-Basany E. Intraoperative use of ICG fluorescence imaging to reduce the risk of anastomotic leakage in colorectal surgery: a systematic review and meta-analysis. Tech Coloproctol. (2018) 22(1):15–23. doi: 10.1007/s10151-017-1731-8
17. Sparreboom CL, Wu ZQ, Ji JF, Lange JF. Integrated approach to colorectal anastomotic leakage: communication, infection and healing disturbances. World J Gastroenterol. (2016) 22(32):7226–35. doi: 10.3748/wjg.v22.i32.7226
18. Christley S, Shogan B, Levine Z, Koo H, Guyton K, Owens S, et al. Comparative genetics of Enterococcus faecalis intestinal tissue isolates before and after surgery in a rat model of colon anastomosis. PLoS One. (2020) 15(4):e0232165. doi: 10.1371/journal.pone.0232165
19. Shogan BD, Belogortseva N, Luong PM, Zaborin A, Lax S, Bethel C, et al. Collagen degradation and MMP9 activation by Enterococcus faecalis contribute to intestinal anastomotic leak. Sci Transl Med. (2015) 7(286):286ra68. doi: 10.1126/scitranslmed.3010658
20. Edomskis P, Goudberg MR, Sparreboom CL, Menon AG, Wolthuis AM, D’Hoore A, et al. Matrix metalloproteinase-9 in relation to patients with complications after colorectal surgery: a systematic review. Int J Colorectal Dis. (2021) 36(1):1–10. doi: 10.1007/s00384-020-03724-6
21. Lam A, Fleischer B, Alverdy J. The biology of anastomotic healing-the unknown overwhelms the known. J Gastrointest Surg. (2020) 24(9):2160–6. doi: 10.1007/s11605-020-04680-w
22. Wang PH, Huang BS, Hornr HC, Yeh CC, Chen YJ. Wound healing. J Chin Med Assoc. (2018) 81(2):94–101. doi: 10.1016/j.jcma.2017.11.002.29169897
23. Cheong YC, Laird SM, Li TC, Shelton JB, Ledger WL, Cooke ID. Peritoneal healing and adhesion formation/reformation. Hum Reprod Update. (2001) 7(6):556–66. doi: 10.1093/humupd/7.6.556
24. Tang J, Xiang Z, Bernards MT, Chen S. Peritoneal adhesions: occurrence, prevention and experimental models. Acta Biomater. (2020) 116:84–104. doi: 10.1016/j.actbio.2020.08.036
25. Arung W, Meurisse M, Detry O. Pathophysiology and prevention of postoperative peritoneal adhesions. World Journal of Gastroenterology. (2011) 17(41):4545–53. doi: 10.3748/wjg.v17.i41.4545
26. Saed GM, Diamond MP. Molecular characterization of postoperative adhesions: the adhesion phenotype. J Am Assoc Gynecol Laparosc. (2004) 11(3):307–14. doi: 10.1016/S1074-3804(05)60041-2
27. Alpay Z, Saed GM, Diamond MP. Postoperative adhesions: from formation to prevention. Semin Reprod Med. (2008) 26(4):313–21. doi: 10.1055/s-0028-1082389
28. Braun KM, Diamond MP. The biology of adhesion formation in the peritoneal cavity. Semin Pediatr Surg. (2014) 23(6):336–43. doi: 10.1053/j.sempedsurg.2014.06.004
29. Fletcher NM, Jiang ZL, Diamond MP, Abu-Soud HM, Saed GM. Hypoxia-generated superoxide induces the development of the adhesion phenotype. Free Radic Biol Med. (2008) 45(4):530–6. doi: 10.1016/j.freeradbiomed.2008.05.002
30. Brokelman WJA, Lensvelt M, Rinkes IHMB, Klinkenbijl JHG, Reijnen MMPJ. Peritoneal changes due to laparoscopic surgery. Surg Endosc. (2011) 25(1):1–9. doi: 10.1007/s00464-010-1139-2
31. Saed GM, Diamond MP. Modulation of the expression of tissue plasminogen activator and its inhibitor by hypoxia in human peritoneal and adhesion fibroblasts. Fertil Steril. (2003) 79(1):164–8. doi: 10.1016/S0015-0282(02)04557-0
32. Ivarsson ML, Diamond MP, Falk P, Holmdahl L. Plasminogen activator/plasminogen activator inhibitor-1 and cytokine modulation by the PROACTTM System. Fertil Steril. (2003) 79(4):987–92. doi: 10.1016/S0015-0282(02)04851-3
33. Ambler DR, Fletcher NM, Diamond MP, Saed GM. Effects of hypoxia on the expression of inflammatory markers IL-6 and TNF-a in human normal peritoneal and adhesion fibroblasts. Syst Biol Reprod Med. (2012) 58(6):324–9. doi: 10.3109/19396368.2012.713439
34. Chegini N, Zhao Y, Kotseos K, Ma C, Bennett B, Diamond MP, et al. Differential expression of matrix metalloproteinase and tissue inhibitor of MMP in serosal tissue of intraperitoneal organs and adhesions. BJOG An Int J Obstet Gynaecol. (2002) 109(9):1041–9. doi: 10.1111/j.1471-0528.2002.01334.x
35. Visse R, Nagase H. Matrix metalloproteinases and tissue inhibitors of metalloproteinases: structure, function, and biochemistry. Circ Res. (2003) 92(8):827–39. doi: 10.1161/01.RES.0000070112.80711.3D
36. Rout UK, Oommen K, Diamond MP. Altered expressions of VEGF mRNA splice variants during progression of uterine-peritoneal adhesions in the rat. Am J Reprod Immunol. (2000) 43(5):299–304. doi: 10.1111/j.8755-8920.2000.430509.x
37. Diamond MP, El-Hammady E, Munkarah A, Bieber EJ, Saed G. Modulation of the expression of vascular endothelial growth factor in human fibroblasts. Fertil Steril. (2005) 83(2):405–9. doi: 10.1016/j.fertnstert.2004.06.073
38. Saed GM, Munkarah AR, Abu-Soud HM, Diamond MP. Hypoxia upregulates cyclooxygenase-2 and prostaglandin E2 levels in human peritoneal fibroblasts. Fertil Steril. (2005) 83(Suppl 1):1216–9. doi: 10.1016/j.fertnstert.2004.11.037
39. Stanzel RD, Lourenssen S, Nair DG, Blennerhassett MG. Mitogenic factors promoting intestinal smooth muscle cell proliferation. Am J Physiol Cell Physiol. (2010) 299(4):C805–17. doi: 10.1152/ajpcell.00086.2010
41. Yu J, Zeng Y, Zhao J, Liao D, Gregersen H. Quantitative analysis of collagen fiber angle in the submucosa of small intestine. Comput Biol Med. (2004) 34(6):539–50. doi: 10.1016/j.compbiomed.2003.06.001
42. Lovisa S, Genovese G, Danese S. Role of epithelial-to-mesenchymal transition in inflammatory bowel disease. J Crohns Colitis. (2019) 13(5):659–68. doi: 10.1093/ecco-jcc/jjy201.30520951
43. Lamouille S, Xu J, Derynck R. Molecular mechanisms of epithelial-mesenchymal transition. Nat Rev Mol Cell Biol. (2014) 15(3):178–96. doi: 10.1038/nrm3758.24556840
44. Jiang H, Shen J, Ran Z. Epithelial-mesenchymal transition in Crohn’s disease. Mucosal Immunol. (2018) 11(2):294–303. doi: 10.1038/mi.2017.107
45. Obermüller B, Frisina N, Meischel M, Singer G, Stanzl-Tschegg S, Lichtenegger H, et al. Examination of intestinal ultrastructure, bowel wall apoptosis and tight junctions in the early phase of sepsis. Sci Rep. (2020) 10(1):11507. doi: 10.1038/s41598-020-68109-9
Keywords: colorectal anastomosis, anastomotic healing, intestinal healing, anastomotic leakage, wound healing
Citation: Rosendorf J, Klicova M, Herrmann I, Anthis A, Cervenkova L, Palek R, Treska V and Liska V (2022) Intestinal Anastomotic Healing: What do We Know About Processes Behind Anastomotic Complications. Front. Surg. 9:904810. doi: 10.3389/fsurg.2022.904810
Received: 25 March 2022; Accepted: 11 May 2022;
Published: 7 June 2022.
Edited by:
Hans Martin Schardey, Agatharied Hospital GmbH, GermanyReviewed by:
Narimantas Samalavicius, Vilnius University, LithuaniaCopyright © 2022 Rosendorf, Klicova, Herrmann, Anthis, Cervenkova, Palek, Treska and Liska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jachym Rosendorf amFjaHltcm9zZW5kb3JmQGdtYWlsLmNvbQ==
Specialty section: This article was submitted to Visceral Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.