 Mingjie Zhang1
Mingjie Zhang1 Zixuan Song
Zixuan Song Yangzi Zhou
Yangzi Zhou Dandan Zhang
Dandan Zhang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 08 June 2022
Sec. Surgical Oncology
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.894083
This article is part of the Research Topic Challenges, Techniques and Pitfalls in Surgery: How Far Can We Push the Boundaries? View all 21 articles
Background: Enhanced recovery after surgery (ERAS), a new clinical surgical concept, has been applied in many surgical disciplines with good clinical results for the past 20 years. Bibliometric analysis is an effective method to quantitatively evaluate the academic productivity. This report aimed to perform a scientometric analysis of the ERAS research status and research hotspots.
Methods: Comprehensive scientific mapping analysis of a wide range of literature metadata using the scientometric tools, including the Bibliometrix R Package, Biblioshiny, and CiteSpace. Data were retrieved from the Web of Science Core Collection database of original articles from 2001 to 2020. Specific indicators and maps were analyzed to show the co-authorship, co-institute, co-country, co-citation, and international cooperation. Automatic literature screening, unsupervised cluster filtering, and topic cluster identification methods were used to display the conceptual framework and thematic evolution.
Results: A total of 1,403 research projects drafted by 6,966 authors and published in 413 sources were found. There was an exponential growth in the number of publications on ERAS. There were 709 collaborations between authors from different countries, and the US, China, and the UK had the greatest number of publications. The WORLD JOURNAL OF SURGERY, located in Bradford’s Law 1, had the highest number of published articles (n = 1,276; total citations = 3,193). CiteSpace network analysis revealed 15 highly correlated cluster ERAS studies, and the earliest study was on colonic surgery, and ERAS was recently applied in cardiac surgery. The etiology of ERAS is constantly evolving, with surgery and length of hospital as the main topics. Meta-analyses and perioperative care have tended to decline.
Conclusion: This is the first scientometric analysis of ERAS to provide descriptive quantitative indicators. This can provide a better understanding of how the field has evolved over the past 20 years, help identify research trends, and provide insights and research directions for academic researchers, policymakers, and medical practitioners who want to collaborate in these areas in the future.
Enhanced recovery after surgery (ERAS) was first proposed by Kehlet et al. at the University of Copenhagen in Denmark in the late 1990s and has been applied clinically (1, 2). ERAS was initially used primarily in Europe and North America to study the effects of surgical stress response on open colorectal surgery in terms of rapid recovery. ERAS represents the idea of synergy through a combination of effective measures, with the central aim of reducing trauma and stress. ERAS is the best result of multidisciplinary collaboration that perfectly blends the latest research findings from surgery, anesthesia, and nursing into an integrated innovative concept that represents an optimized clinical pathway. This optimized clinical pathway involves the whole process of patient diagnosis and treatment, emphasis on the patient-centered concept. The implementation of the ERAS pathway can improve perioperative safety and the satisfaction in surgical patients, shorten the postoperative hospital stay, and help reduce the incidence of postoperative complications (3). Using the ERAS, patients can be identified, compartmentalized, and accommodated at every step throughout the perioperative period to facilitate an effective and safe process from preoperative evaluation through discharge to recovery. The advantages of ERAS have been recognized by operators and specialists worldwide, and its application in the medical field has been actively promoted. The ERAS Society has developed numerous perioperative guidelines for ERAS for various specialties and disciplines since 2005 (4–11).
The postoperative rehabilitation of patients undergoing surgery is affected by various factors, such as stress response, pain, and postoperative intestinal paralysis (12). stress response after surgery is a physiological and pathological process in the body, including changes in the nerve, endocrine, metabolic, and immune functions. Similarly, pain can adversely affect patient recovery. Postoperative intestinal paralysis aggravates postoperative discomfort, especially in patients undergoing abdominal surgery, affecting oral feeding and delaying the recovery of patients. Therefore, the combination of new techniques in anesthesiology, pain control, and surgical methods with the improvement of the traditional postoperative nursing methods can reduce the postoperative stress reaction, incidence of postoperative complications and mortality, postoperative hospital stay, and hospitalization cost. This finding is consistent with the concept of minimally invasive surgery. ERAS generally includes the following: (1) Preoperative patient education. (2) better anesthesia, analgesia, and surgical techniques can reduce surgical stress, pain, and discomfort. (3) enhanced postoperative rehabilitation including early ambulation and enteral nutrition. Several surgical studies have shown that ERAS can significantly shorten the postoperative hospitalization time, reduce hospitalization costs, and maximize the use of limited hospital resources without increasing the incidence of complications and mortality, which will become the trend of surgery (13, 14).
ERAS has been applied and supplemented for 20 years since it was first proposed in 2001, and is now being developed in a more refined direction. Its research direction is not limited to the surgical field, and future research directions and current research hotspots need to be clarified. Bibliometric analysis is the application of statistical and mathematical tools to books and media communications (15). Bibliometric analysis is a transparent, systematic, and repeatable review process that significantly improves the quality of literature review. This provides a means of mapping research fields and influential work without subjective bias.
This study aimed to identify research flows and topics by analyzing the citation dynamics in ERAS studies from to 2001–2020 to measure their impact on the scientific community (qualitative indicators). These topics and streams of research can guide scholars to find directions for future research and to find answers to current questions.
This was a bibliometric network study using metadata from the Web of Science Core Collection on July 12, 2021. This is described in accordance with the STROBE guidelines (16). This was not a human-focused study and, as such, neither the institutional review board approval nor informed consent was required. This study was divided into five steps, known as the document metering workflow proposed by Zupic and Ater (17). Figure 1 represents the five steps used to complete the bibliometric analysis of ERAS.
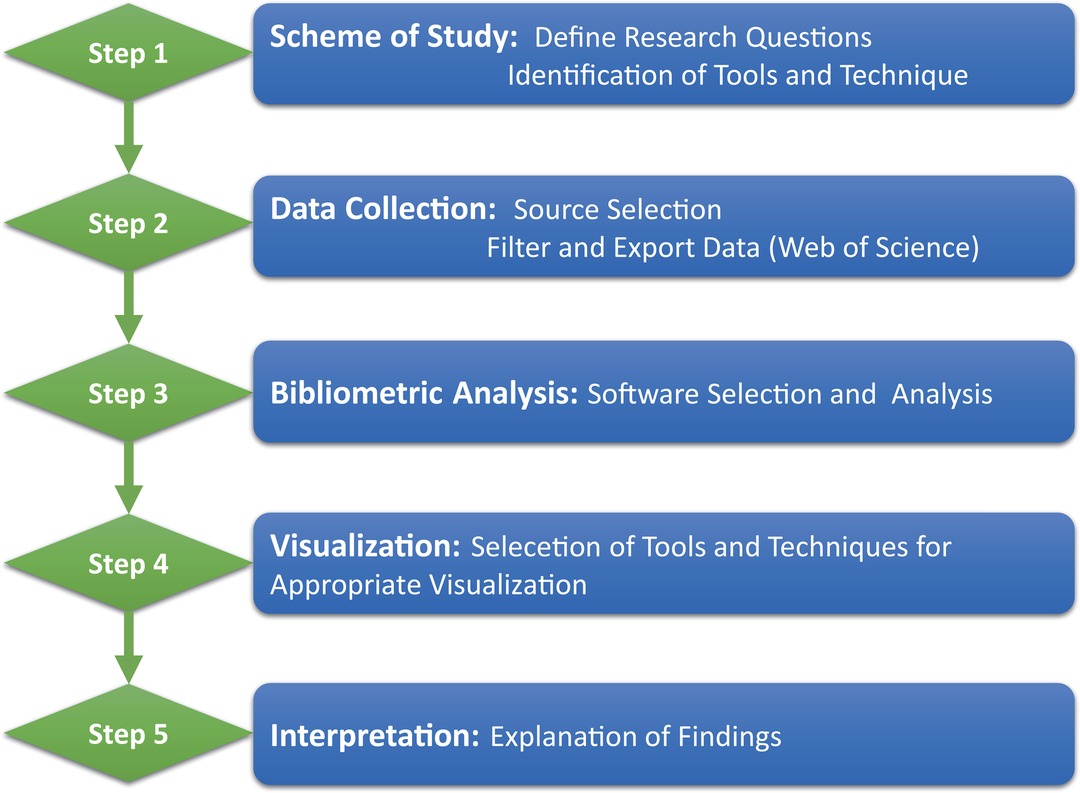
Figure 1. The Procedure of Bibliometric Analysis.
The original data for this article were obtained from the Web of Science core collection database, including SCI-EXPAND and SSCI. This following titles were used for the selection: “enhanced recovery after surgery” or “enhanced postsurgical recovery” or “enhanced recovery program” or “enhanced recovery pathways” or “accelerated rehabilitation” or “fast track surgery.” The publication date was restricted from January 1, 2001 to December 31, 2020. The manuscript type was “article” and the target results were filtered. The file format recorded content was set to “plain text” and was exported as “full record”.
Bibliometrix is an R language based bibliometric software with multiple toolkits for full-process bibliometrics and visual presentation of scientific documents, which was developed by Aria (18). Based on the data exported from the WOS database and then completed by the team researchers (XX Wang and ZX Song), the bibliometric analysis was conducted using the R software version 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org) through the Bibliometrix R package.
CiteSpace is a visual tool for bibliometric analysis developed by Chaomei Chen, based on the Java platform (19). As an interactive analysis tool, it combines bibliometrics and data-mining algorithms to complete scientific mapping through the visualization of results. CiteSpace can be used to analyze cooperative networks and co-citations (20). Version 5.8.3 was used in this study for the analysis of the co-authorship, co-institute, co-country, and document co-citation of the articles published from 2001 to 2020. The time slice was two years, and the selection criterion was the first 50% of each time period. In collaborative networks, the size of the circles represents the number of studies published; the shorter the distance between the circles, the greater the collaboration between the two authors/institutions/countries. The blue-purple nodes represented earlier studies, whereas the yellow-red nodes represented more recent studies. In the co-citation analysis, the size of the nodes represented the frequency of citations, nodes with different colors represented different years, the line between the nodes represented the relationship between the co-citations, and the thickness of the line represented the strength of the relationship. The color corresponds to the time of the node’s first co-citation, and the color from cold to warm represented early to recent co-citation. The thickness of the tree-ring was proportional to the number of citations in a given time zone. Modularity (Q) and weighted mean silhouette (S) were the two indicators used to evaluate clustering in the co-citation analysis. A Q value >0.3 meant very important network and an S value >0.5 meant reasonable clustering results.
Descriptive analysis was used to explain the core sources, authors, countries, publications, and affiliations of publications. Price’s law was used to assess whether the growing trend in the ERAS was scientific. Simultaneously, we identified the core sources using the Bradford’s law (21). According to the Bradford’s law, the data was divided into three regions. Zone 1 was highly productive and was considered a nuclear zone.
The author/publication-level metrics, such as the h-, m-, and g indices were determined (22, 23). In addition, we used keyword plus for the analysis, which was provided by the database to describe the knowledge structure of the study more concisely and standardized. The core research areas and key themes were essential for determining the direction of future research, therefore, thematic maps and thematic evolution were used.
In the thematic maps, each quadrant could be separated by centrality and density to form a two-dimensional graph. Centrality was the importance of a topic in the research field, and the density was used to measure the development of the topic. Quadrant I, located in the upper-right quadrant, named motor themes, suggested that the themes of the region have developed and formed important pillars that shape the field of research. Quadrant II, located in the upper left quadrant, named niche themes, reflected highly developed but isolated themes. Quadrant III, located in the lower-left quadrant and named emerging or declining themes, suggested weak development and marginalization of the research field. Quadrant IV, located in the lower-right quadrant, was named as basic themes. Although these topics are less developed, they are important to the field of study.
Table 1 presents the descriptive features of the ERAS literature. A total of 1,403 studies were selected according to the search strategy. We identified 1,320 articles and 81 articles and proceedings papers. A total of 2,098 keywords plus 1,991 author keywords were used. Furthermore, 6,966 authors wrote the documents; among them, only 26 articles were written by one author. The collaboration index was 5.07, which showed the highly collaborative nature of ERAS publications. The document-per-author ratio was 0.201, implying that, on average, approximately five authors wrote a document.
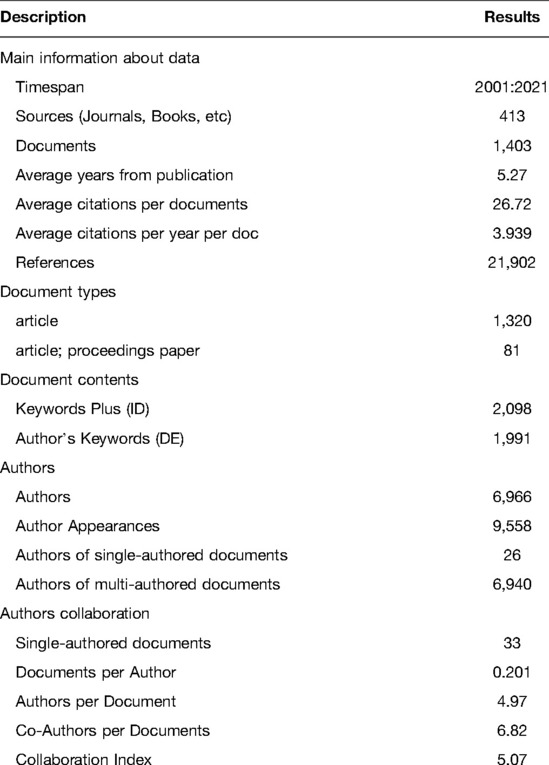
Table 1. Descriptive characteristics of ERAS literature.
By summarizing the number of papers published over the years, Figure 2A shows the overall trend of ERAS studies published worldwide from 2001 to 2020. ERAS research has an overall upward trend, and according to the curves analyzed from the data, it was found to be more suitable for exponential adjustment than linear adjustment, thus satisfying the Price’s law. The correlation coefficient (r) after mathematical adjustment of the exponential curve was 0.9804, while the linear adjustment of the measured values, R, was 0.8051. Therefore, the percentage of unexplained variation was 19.49%.
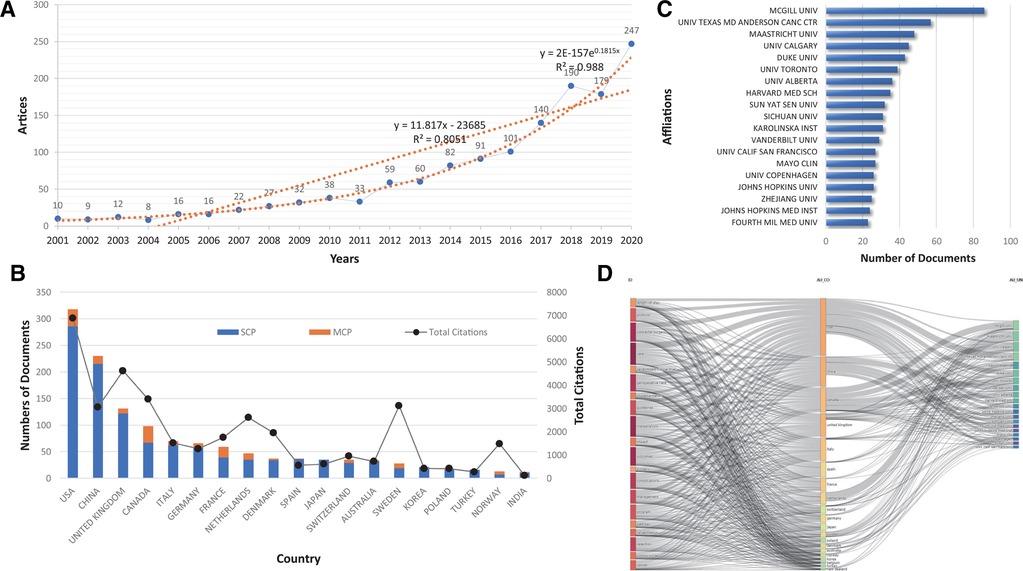
Figure 2. (A) Growth of scientific production on ERAS from 2001 to 2020. A linear adjustment of the data and an adjustment to the exponential curve were made, in order to assess whether the production fulfilled the Price’s Law. Linear adjustment: y = 11.8176x – 23685, R2 = 0.8051; Exponential adjustment: y = 2E-157e0.1815x, R2 = 0.9804. (B) The countries of the top 20 most relevant corresponding authors of the articles on ERAS. MCP, Multi-country publications; SCP, simple-country publications. (C) Top 20 of the Most Relevant Affiliations. (D) R Studio - Three-fields plot: left – keywords plus from the data records, middle – countries, right – authors affiliations.
Figure 2B shows three sets of data: simple-country authors, multicountry authors, and the citation rate of each country. The USA was at the top with several publications, China was ranked second, and the UK was ranked third, but concerning citations, China’s total citations were worse than those of the UK. In contrast, although Sweden has a relatively small number of publications, it was at the top four the most cited countries, after the USA, the UK, and Canada. The country with the highest international cooperation was the USA, followed by Canada and the France. The most relevant affiliations are reported in Figure 2C. The McGill University was the first, and provided a strong basis for ERAS. The University of Texas MD Anderson Cancer Center and Maastricht University were the second and third affiliations of most publications, respectively.
In addition to the annual production, major topics, locations, and affiliations of ERAS-related publications were viewed. Figure 2D shows a threefold analysis of the ERAS publications, with keywords plus on the left, affiliations on the right, and relevant countries in the middle. The chart shows that the USA was working with most of the top agencies to focus on ERAS-related topics. In addition, China, Canada, and the UK have made significant contributions to ERAS science topics. Issues related to outcomes and care are the most widely studied in most countries.
We used source impact and Bradford’s Law to find publications on ERAS in the core journals in the scientific literature. Table 2 ranks the articles by h, M, G-index, total citations (TC), net output (NP), and pub year of publication (PYstart), and represents the Bradford’s Law (Figure 3A), which divides journals into three regions. We found that 24 of the 413 journals were in core zone 1, and the top 24 journals were the core publishing sources for corona literature in the social sciences.
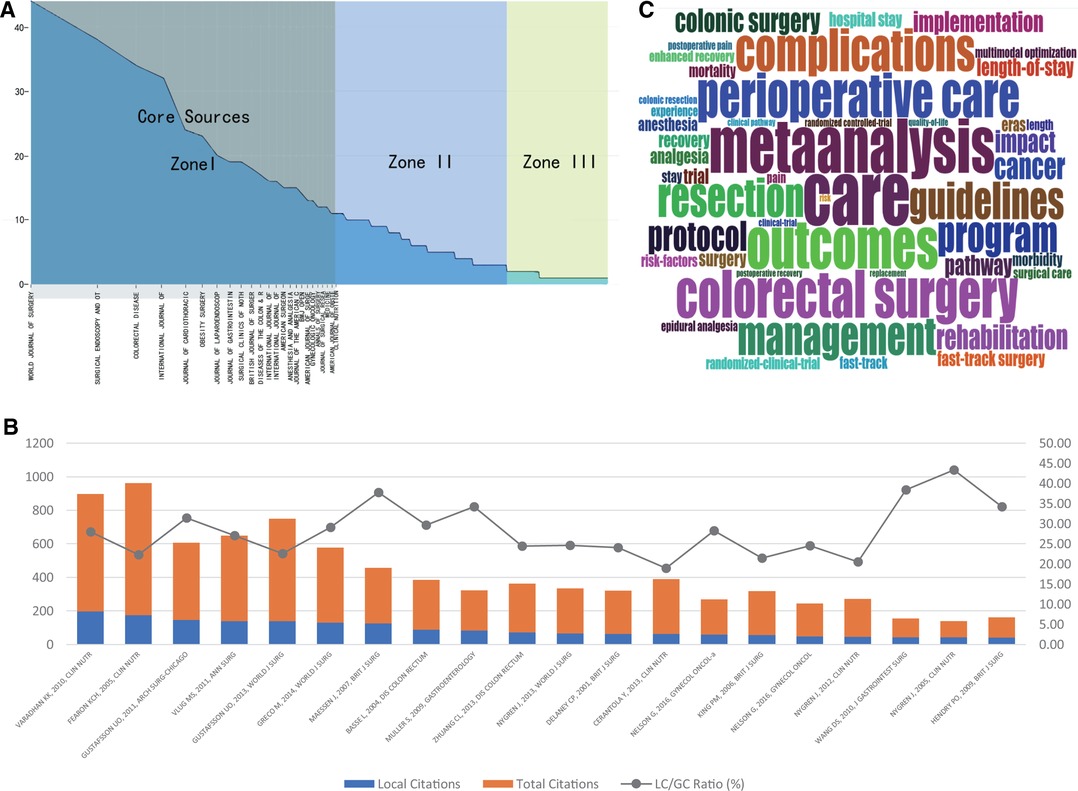
Figure 3. (A) Journal Rankings According to the Bradford Law. (B) Top 20 of the Most Globally Cited Article and their located cited. (C) Word cloud based on the most frequent words (Keywords Plus) used in the articles on ERAS.
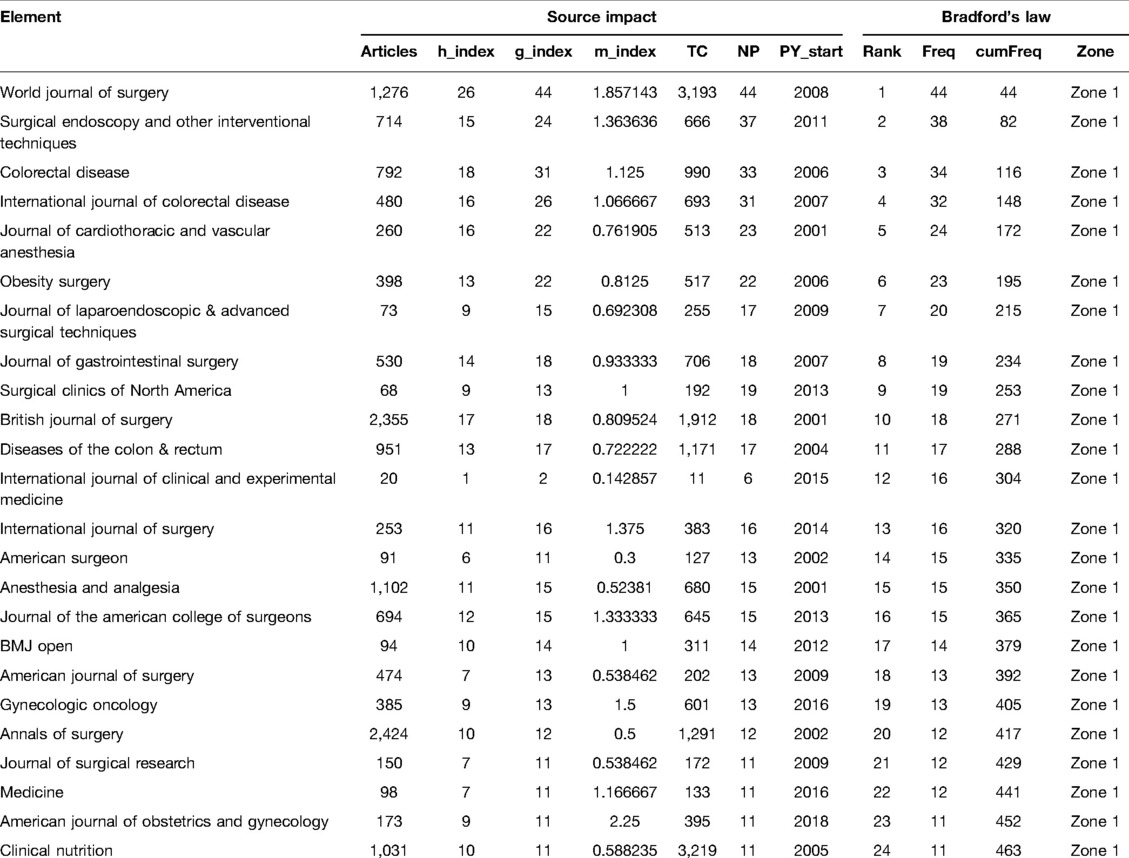
Table 2. Zone 1 journals according Bradford’s law and the source impact.
Table 3 lists the top 20 most-cited articles in the database along with their global citations. Figure 3B shows the local and global citations for highly cited papers. Table 4 provides the most frequent words used in the ERAS literature, which is divided into four parts: keywords plus, authors’ keywords, abstracts, and titles. Figure 3C shows the word cloud created using keyword plus. Words with a high frequency in the literature were larger in size.
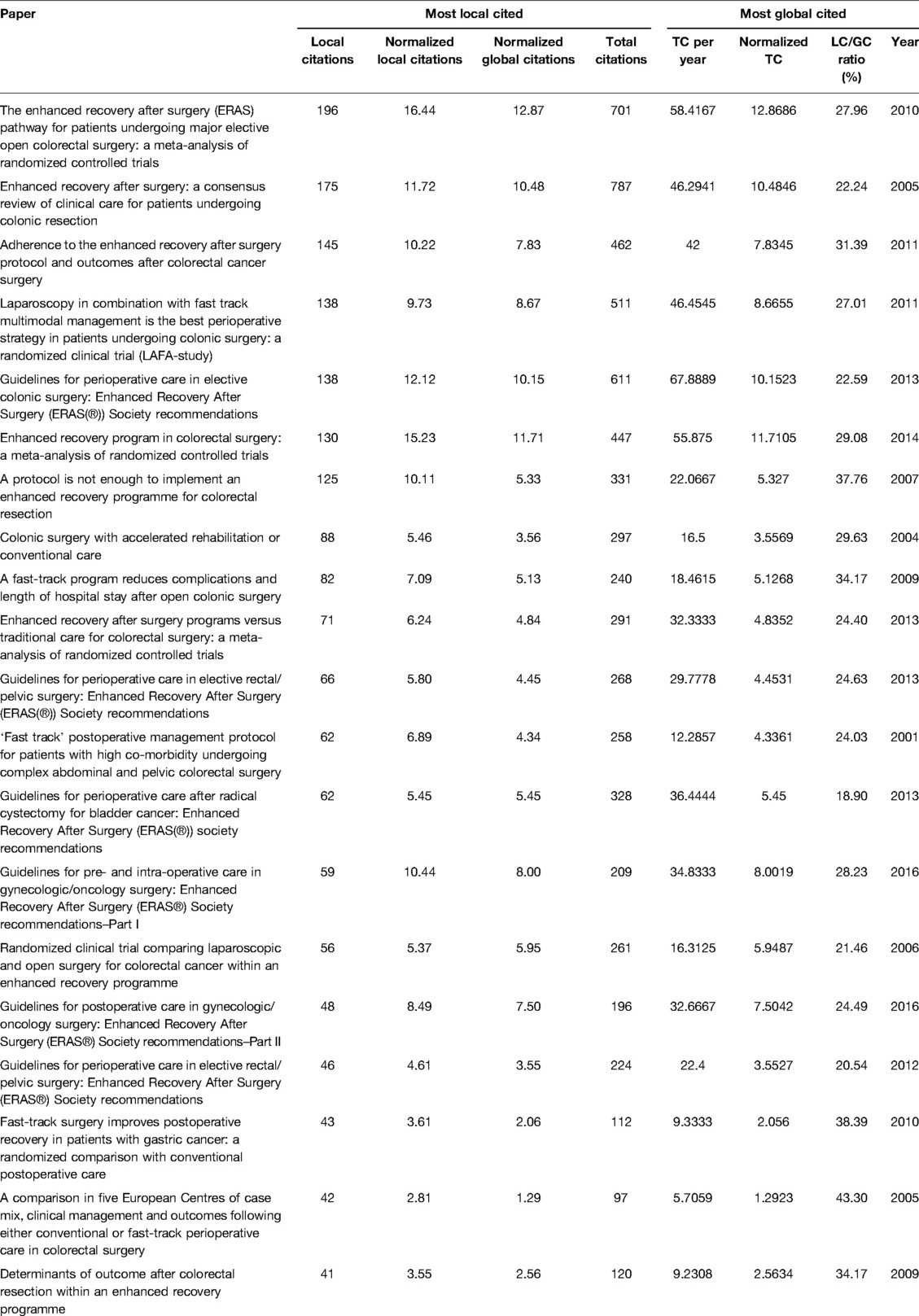
Table 3. Top 20 most cited articles.
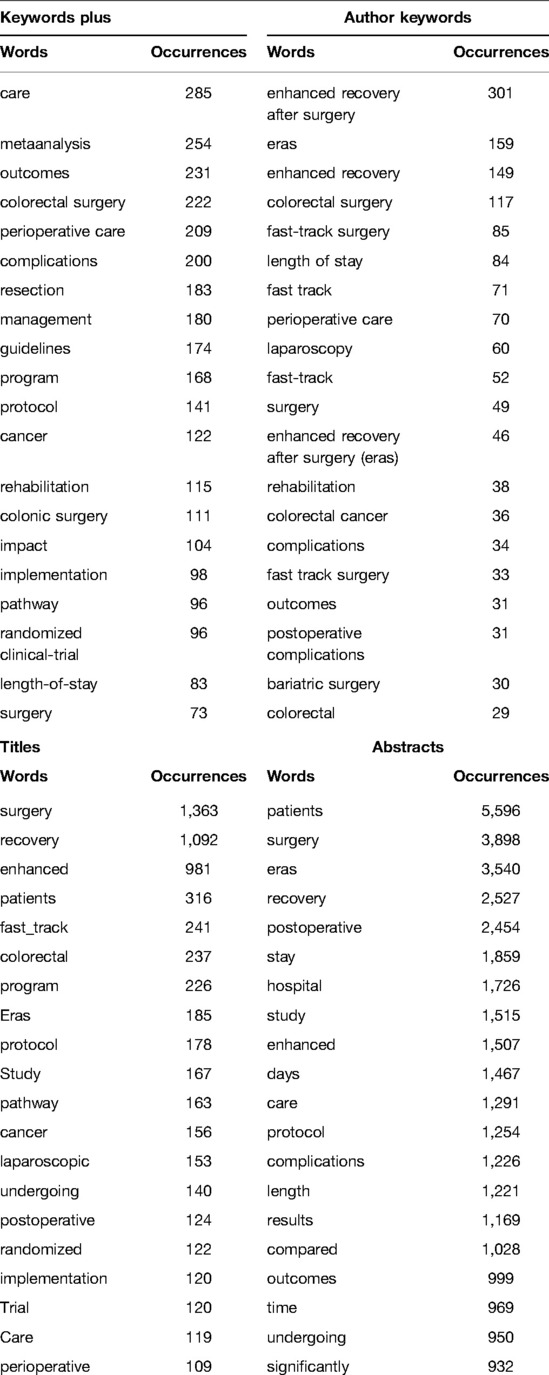
Table 4. Most frequent words.
The results of the generating collaborator mappings using CiteSpace were 676 nodes and 1,440 links (Figure 4A), which means that 1,401 articles were published by 676 authors. As shown in Figure 4A, many authors preferred to combine with relatively stable collaborators, resulting in a relatively large cluster of authors. In earlier studies, only a few core authors cooperated less with the central clusters. The most representative author was LJUNGQVIST O, who published 33 studies, followed by DEMARTINES N and KEHLET H. The top-ranked item by centrality was O LJUNGQVIST (2005) with a centrality of 30, and the second one was OLLE LJUNGQVIST (2010) with a centrality of 28. The third was H KEHLET (2002) and GREGG NELSON (2016), with centralities of 25.
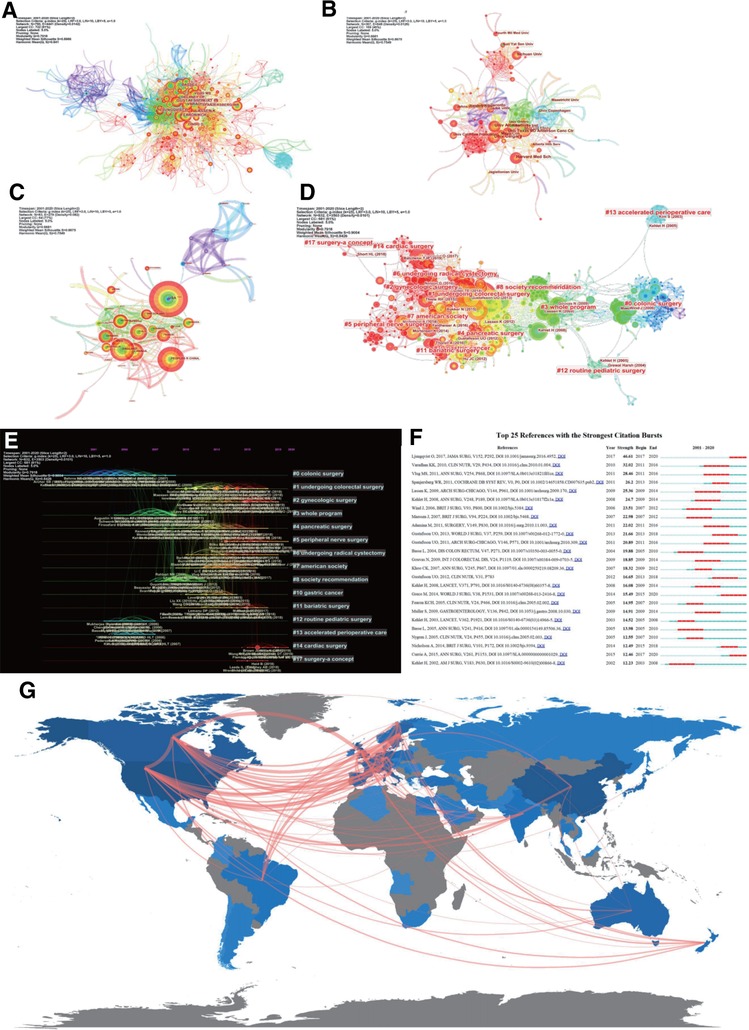
Figure 4. (A) An author cooperation map related to ERAS research from 2001 to 2020. (B) An institution cooperation map related to ERAS research from 2001 to 2020. (C) A country cooperation map related to ERAS research from 2001 to 2020. (D) Reference co-citation map related to ERAS research from 2001 to 2020. (E) The timeline view of cited reference related to ERAS. (F) Top 25 references with the strongest citation bursts. (G) The country collaboration map of the global authors of the ERAS research.
The institute of the two authors appeared in the same article as a cooperative organization, namely, the co-institute. The Citesapce software was used to calculate the co-occurrence frequency matrix to determine the degree of cooperation. Figure 4B shows the collaborative institutes in the era domain, with an institution map of 367 nodes and 848 links. Generally, the institutions were concentrated in universities and a few in hospitals.
Authors from two different countries appear in the same article; that is, a co-country. Figure 4C shows the results for co-countries in the era domain. As shown in Figure 4C, although the United States was ranks first worldwide in terms of publication volume, European countries had a relatively close cooperative relationship.
After analysis using CiteSpace, Figure 4D shows a document co-citation network diagram containing 832 nodes, 3,503 links, and 15 main clusters. The modularity Q value was 0.7918, and the weighted mean silhouette S was 0.9004.
A literature co-citation analysis of ERAS studies yielded 15 co-citation categories, marked by their citation index terms. To obtain the key cluster of the cited references, log-likelihood tests (LLR) were used to select the noun phrase from the title of the article in Citespace. The contour value of each cluster was >0.9, indicating reliable and meaningful results. Figure 4E summarizes the details of the 15 clusters using a timeline view to reflect the research patterns and emerging trends in the network map. Articles with the strongest citation bursts showed a significant increase in interest in ERAS. Figure 4F shows the 25 strongest references from 2008 to 2020.
Collaborative World Map as a Measure of the Social Structure: There were 709 collaborations between authors from different countries. The world map (Figure 4G and Supplementary material) shows that the most frequent cooperation was between the United States and Canada (24), followed by the United Kingdom and Canada (25), Canada and Sweden, and the United Kingdom and Sweden (23).
Based on the relationship between the keywords plus, the research content was roughly divided into several topics. The identified topics were categorized into a strategic map to analyze the importance and development of the research topic. The strategy map was based on the full-time span from 2001 to 2020. We used the first 400 keywords, but the items displayed in the cluster were set to a minimum frequency of 40. The number of representative labels in each theme was set to three so that the thematic map based on density (Y-axis) and centrality (X-axis) could be obtained, as shown in Figure 5. The centrality measured the importance of a topic, and density measured the development of the topic. The topics appearing in the lower left were the emerging or declining topics, which are new topics that can emerge better or decline from the research field. The upper right panel represented high density and high centrality. The developed theme of this section was the motor theme, and was necessary.
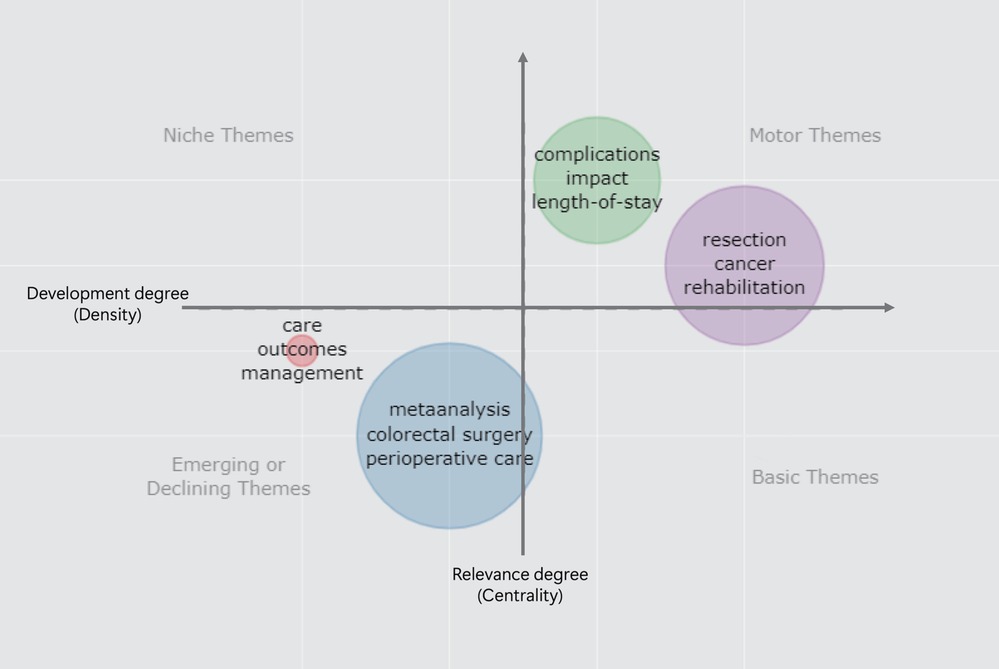
Figure 5. The strategy map of identified topics clustered by keywords plus.
Thematic evolution showed the historical development of the ERAS literature. The use of keywords and topic evolution described the history and evolution of the topics. This time division was based on the author’s subjective judgment while allowing for a better representation of the evolution of the subject. The first part was from 2001 to 2006, the second from 2007 to 2011, the third from 2012 to 2016, and the last from 2017 to 2021. Figure 6 shows the topic evolution of the keyword plus (Supplementary material).
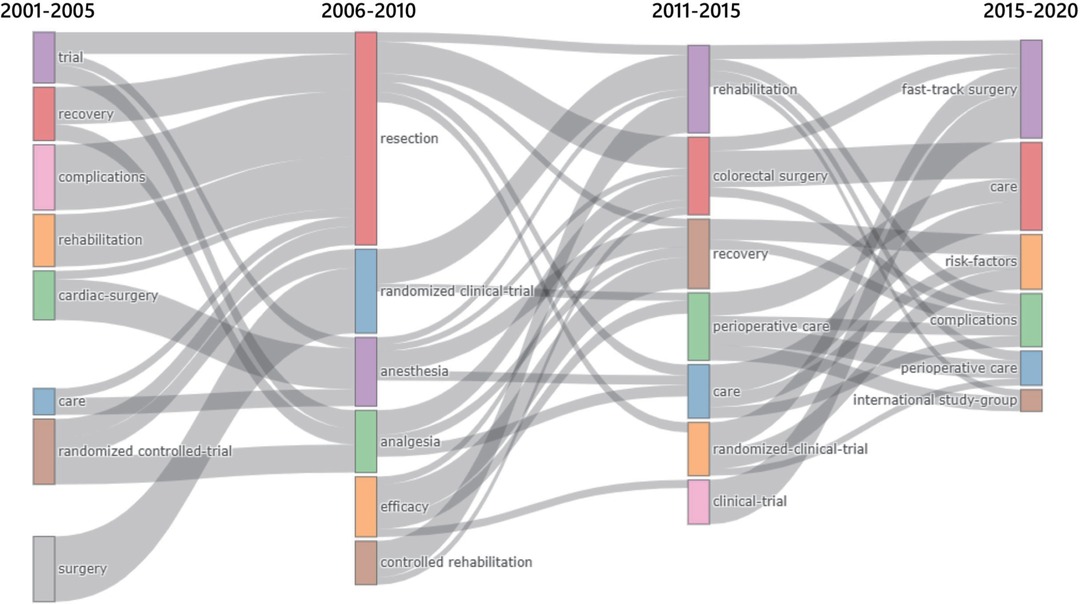
Figure 6. Thematic Evolution of ERAS research from 2001 to 2020.
Fast-track surgery (FTS) or ERAS is the inevitable result of the development of medical theory and technology, “Pain and Risk “Free” was the goal of surgery (26). The connotation of ERAS was to reduce the body’s stress response to trauma, promote rapid functional recovery, reduce the incidence of clinical complications, and shorten the length of hospital stay. A large number of clinical studies have proven that perioperative process optimization and multidisciplinary collaboration of minimally invasive techniques can improve the treatment effects, reduce medical interventions (over-treatment), and promote patient recovery (27). For ERAS to be practiced clinically, its philosophy and associated pathways must be based on evidence-based medicine and multidisciplinary collaboration. It should not only reflect the core concept of accelerating recovery, but should consider the patient’s underlying diseases, types of surgery, perioperative complications, and other specific conditions. Moreover, in-depth clinical studies are required to demonstrate the safety, feasibility, and necessity of ERAS-related pathways.
According to a bibliometric analysis, the United States has the largest number of ERAS-related articles published followed by China. Despite the large number of published reports in China, there were fewer citations. Most of the top 20 most-cited articles were published in the early period of ERAS in Europe and the United States because ERAS originated in Europe and the United States, and were the first to carry out relevant research on ERAS (28, 29). In contrast, as a North American country, Canada was ranks fourth in the total number of articles published; however, the proportion of multi-country publications was high, and most of the articles were from the McGill University, which reflects the high concentration of research. The university with the second highest research focus was the MD Anderson Cancer Center in the United States, which may be due to the fact that the previous studies on ERAS were on radical surgery for patients with tumor.
Earlier researches on ERAS were mainly related to surgery, therefore, the most cited journals in zone 1 of the Bradford’s Law were journals of the surgery discipline, such as the WORLD JOURNAL OF SURGERY, SURGICAL ENDOSCOPY AND OTHER INTERVENTIONAL TECHNIQUES, and COLORECTAL DISEASE. According to the Word Cloud, “colorectal surgery” and “resection” played important roles in surgery and colorectal surgery was the most mature surgical method that used ERAS. With ERAS, the hospital stay and complications in patients who underwent colorectal surgery effectively reduced without an increase in the readmission rates (30).
The ERAS Society was founded in 2001, and in 2005, the first worldwide expert consensus on accelerated recovery for colon resection was developed (29). In addition, relevant studies on ERAS mainly focused on research directions, such as meta-analysis and perioperative care. Randomized controlled trials and meta-analyses have been used in ERAS studies, and a large number of high-quality clinical studies are important for further evidence-based practice and guidelines development. Meta-analysis and clinical research have mainly focused on perioperative nursing, postoperative complications, length of hospital stay, final results, and process management (25, 31). In addition to the ERAS, perioperative care was very important in the implementation to surgical management. Currently, the relevant care specifications are clearly specified in the guidelines for various specialties (7–9). Clinical evidence has shown that perioperative FTS care can promote postoperative rehabilitation and shorten the hospitalization time of patients with gynecological diseases (32). Magheli provided FTS care to 50 patients undergoing laparoscopic radical prostatectomy, which significantly improved the recovery time of the bowel function and defecation time, shortened the postoperative hospital stay, and improved the overall satisfaction rate of patients (33).
Among the 15 clusters obtained through CiteSpace cluster analysis, most studies on ERAS were still related to surgery, but were developed from colorectal surgery in the early stages of cardiac surgery, neurosurgery, and other surgical disciplines. Guidelines are emerging for other general surgery procedures (pancreaticoduodenectomy, elective colon surgery, and elective rectal and pelvic surgery) (10, 11, 24). ERAS has gained acceptance worldwide over time and is widely used in a range of surgical specialties, such as urology, orthopaedics, and obstetrics and gynecology. Although a study on FTS was published in cardiac surgery as early as 1994 (34), it was not until 2015 that Zaouter from France first reported the systematic application of ERAS in cardiac surgery (35). In 2018, Noss systematically reviewed the relevant issues of ERAS in cardiac surgery and provided an in-depth consideration of the existing problems (36). Many urological studies have reported the use of ERAS in the perioperative period of laparoscopic nephrectomy (37), open partial nephrectomy (38), laparoscopic radical prostatectomy (39), and TVT or TVT-O (40). Compared to the control group, the duration of hospital-stay in the patients who underwent ERAS was significantly shorter, with better pain control and patient satisfaction. Similarly, to promote and regulate the use of ERAS in gynecology, the International ERAS Society in 2016 proposed guidelines for the use of ERAS in gynecology/gynecological oncology (41, 42).
After more than 20 years of research, evidence-based medicine demonstrated the effectiveness of ERAS in a rational manner, and ERAS models have demonstrated unprecedented advantages in the recovery of patients undergoing surgery (28). From the thematic maps, studies on complications, impact, length of hospital stay, resection, and cancer were mature, and several of the research directions were supported by evidence-based evidence in the guide. However, research topics such as meta-analyses, colorectal surgery, and perioperative care are declining despite the current large number of studies. Similarly, the thematic evolution of ERAS research in the past 20 years showed that ERAS application and anesthesiology research in tumor surgery were prominent in 2006–2010, while in the next five years, more attention will be paid to the comprehensive management of the perioperative period and the emergence of large randomized controlled clinical trials. Simultaneously, ERAS-related meta-analyses began to appear (43). After 2015, patient-reported outcomes were the purpose of ERAS. More attention has been paid to the comfort and safety of patients in hospitals, as well as the reduction of surgical complications, rather than the reduction of hospital days and cost alone (44–47).
ERAS is not a new technology but an integrated and innovative management mode. Its theoretical system has been relatively well-developed after more than 20 years of development. ERAS concepts and models in different disciplines need to consider the characteristics of their respective disciplines; therefore, there are some differences. Despite the success of the ERAS concept, it still has several challenges. The implementation of the ERAS protocol requires good patient and doctor compliance. A multicenter study found that a reduction in the complications was positively correlated with ERAS compliance (OR = 0.69, P < 0.001) (48, 49). At the same time, team cooperation and continuous quality improvement plans are required. The team will formulate the ERAS plan and target management, such as the length of stay, and continue to adhere to and learn the summarized strategies (50). For example, many hospitals in Canada have continuously improved and perfected the clinical practice guideline (CPG) with the application of the “Knowledge-to-Action Cycle” (51), thus slimming the ERAS protocol and increasing the clinical application compliance. Preoperative assessment, preparation, and treatment of patients with high-risk factors and reduction in the failure rate of the ERAS protocols are the major measures to increase patient compliance (52–54). Based on multimodal or multidisciplinary collaboration, the preoperative emphasis on patient education, communication, and collaboration underpins the success of ERAS (55, 56).
Although ERAS has many advantages and is accepted by doctors, there may be limitations to its future use. ① Firstly, the doctors and patients rely on “traditional practices” and “safety considerations.” ② Secondly, from the different systemic conditions, diseases, surgical procedures and hospitals, it was concluded that the ERAS protocols must be “diversified and individualized,” which makes them less evidence-based. ③ Thirdly, the combination of different disciplines may make ERAS processes too convoluted, impeding accelerated recovery. The payment system of medical insurance and cultural background influence the promotion of ERAS programs.
The literature included in this study is from the core collection database of WOS, which has high quality studies, but selection bias cannot be avoided. It is well known that various databases have their advantages and disadvantages, but we chose the WoS over PubMed because PubMed does not store reference metadata, and references were an important part of the research output indicators. In addition, according to the bibliometric research principles, there is a potential length time-lapse bias that puts newer articles at a disadvantage in receiving citations. Of course, bibliometric analyses of the same topic will be used by other authors, and our results may be compared with those of others in the future.
In this study, Bibliometrix and Citespace were used to analyze ERAS literature over the past 20 years. Despite the rapid development of ERAS in various disciplines, the effective coordination of multidisciplinary physicians and the change in patients’ deeply rooted traditional views were the major obstacles to its further development. The bibliometric analysis conducted in this study is expected to provide a reference for the development of ERAS.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The data are available from the authors upon request. Because of the policies of Clarivate, data cannot be shared openly.
MZ and DZ designed the study and drafted the manuscript. XW, XC, YW and YZ designed the statistical analysis plan. ZS and DZ reviewed the manuscript. All authors take responsibility for the appropriateness of the content. All authors contributed to the article and approved the submitted version.
This research was supported by internal funding from the Shengjing Hospital, China Medical University (SJ-M0133) and 345 Talent Project of Shengjing Hospital of China Medical University (No. M0946).
The authors would like to express their appreciation to Massimo Aria and CM Chen, who invented the bibliometrix and CiteSpace, which are free to use. We would like to express our gratitude to all those who helped us in the writing of this manuscript. We thank all peer reviewers for their opinions and suggestions.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2022.894083/full#supplementary-material.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wilmore DW, Kehlet H. Management of patients in fast track surgery. BMJ (Clin Res Ed). (2001) 322(7284):473–6. doi: 10.1136/bmj.322.7284.473
2. Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg. (2002) 183(6):630–41. doi: 10.1016/s0002-9610(02)00866-8
3. Sun YM, Wang Y, Mao YX, Wang W. The safety and feasibility of enhanced recovery after surgery in patients undergoing pancreaticoduodenectomy: an updated meta-analysis. BioMed Res Int. (2020) 2020:7401276. doi: 10.1155/2020/7401276
4. Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, Brunelli A, Cerfolio RJ, Gonzalez M, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. (2019) 55(1):91–115. doi: 10.1093/ejcts/ezy301
5. Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential elements of multimodal analgesia in enhanced recovery after surgery (ERAS) guidelines. Anesthesiology Clin. (2017) 35(2):e115–43. doi: 10.1016/j.anclin.2017.01.018
6. Brindle M, Nelson G, Lobo DN, Ljungqvist O, Gustafsson UO. Recommendations from the ERAS® Society for standards for the development of enhanced recovery after surgery guidelines. BJS Open. (2020) 4(1):157–63. doi: 10.1002/bjs5.50238
7. Brindle ME, McDiarmid C, Short K, Miller K, MacRobie A, Lam JYK, et al. Consensus guidelines for perioperative care in neonatal intestinal surgery: enhanced recovery after surgery (ERAS(®)) society recommendations. World J Surg. (2020) 44(8):2482–92. doi: 10.1007/s00268-020-05530-1
8. Brustia R, Monsel A, Skurzak S, Schiffer E, Carrier FM, Patrono D, et al. Guidelines for perioperative care for liver transplantation: enhanced recovery after surgery (ERAS) recommendations. Transplantation. (2022) 106(3):552–61. doi: 10.1097/tp.0000000000003808
9. Cerantola Y, Valerio M, Persson B, Jichlinski P, Ljungqvist O, Hubner M, et al. Guidelines for perioperative care after radical cystectomy for bladder cancer: enhanced recovery after surgery (ERAS(®)) society recommendations. Clin Nutr. (2013) 32(6):879–87. doi: 10.1016/j.clnu.2013.09.014
10. Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for perioperative care in elective colorectal surgery: enhanced recovery after surgery (ERAS(®)) society recommendations: 2018. World J Surg. (2019) 43(3):659–95. doi: 10.1007/s00268-018-4844-y
11. Melloul E, Lassen K, Roulin D, Grass F, Perinel J, Adham M, et al. Guidelines for perioperative care for pancreatoduodenectomy: enhanced recovery after surgery (ERAS) recommendations 2019. World J Surg. (2020) 44(7):2056–84. doi: 10.1007/s00268-020-05462-w
12. Basse L, Raskov HH, Hjort Jakobsen D, Sonne E, Billesbølle P, Hendel HW, et al. Accelerated postoperative recovery programme after colonic resection improves physical performance, pulmonary function and body composition. Br J Surg. (2002) 89(4):446–53. doi: 10.1046/j.0007-1323.2001.02044.x
13. de Groot JJ, van Es LE, Maessen JM, Dejong CH, Kruitwagen RF, Slangen BF. Diffusion of enhanced recovery principles in gynecologic oncology surgery: is active implementation still necessary? Gynecol Oncol. (2014) 134(3):570–5. doi: 10.1016/j.ygyno.2014.06.019
14. Pędziwiatr M, Kisialeuski M, Wierdak M, Stanek M, Natkaniec M, Matłok M, et al. Early implementation of enhanced recovery after surgery (ERAS®) protocol - compliance improves outcomes: a prospective cohort study. Int J Surg. (2015) 21:75–81. doi: 10.1016/j.ijsu.2015.06.087
15. Andrés A. Measuring academic research: How to undertake a bibliometric study. Witney: Oxford: Chandos Publishing (2009). ISBN: 978 1 84334-528-2.
16. Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. Int J Surg. (2014) 12(12):1500–24. doi: 10.1016/j.ijsu.2014.07.014
17. Zupic I, Čater T. Bibliometric methods in management and organization. Organ Res Methods. (2015) 18(3):429–72. doi: 10.1177/1094428114562629
18. Aria M, Cuccurullo C. Bibliometrix: an R-tool for comprehensive science mapping analysis. J Informetrics. (2017) 11(4):959–75. doi: 10.1016/j.joi.2017.08.007
19. Chen C. Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci U S A. (2004) 101(Suppl 1):5303–10. doi: 10.1073/pnas.0307513100
20. Chen C. Science mapping: a systematic review of the literature. J Data Inf Sci. (2017) 02/20(2):1–40. doi: 10.1515/jdis-2017-0006
21. Joshi SB, Mamdapur G, Rajgoli IU. Application of bradford’s law of sattering to the literature of stellar. Physics. Pearl: A Journal of Library and Information Science (2015) p. 133–40. doi: 10.5958/0975-6922.2015.00018.2
22. Koo M. Systemic lupus erythematosus research: a bibliometric analysis over a 50-year period. Int J Environ Res Public Health. (2021) 18(13). doi: 10.3390/ijerph18137095
23. Martynov I, Klima-Frysch J, Schoenberger J. A scientometric analysis of neuroblastoma research. BMC Cancer. (2020) 20(1):486. doi: 10.1186/s12885-020-06974-3
24. Nygren J, Thacker J, Carli F, Fearon KC, Norderval S, Lobo DN, et al. Guidelines for perioperative care in elective rectal/pelvic surgery: enhanced recovery after surgery (ERAS(®)) society recommendations. World J Surg. (2013) 37(2):285–305. doi: 10.1007/s00268-012-1787-6
25. Hajibandeh S, Hajibandeh S, Bill V, Satyadas T. Meta-analysis of enhanced recovery after surgery (ERAS) protocols in emergency abdominal surgery. World J Surg. (2020) 44(5):1336–48. doi: 10.1007/s00268-019-05357-5
26. Steenhagen E. Enhanced recovery after surgery: it’s time to change practice!. Nutr Clin Pract. (2016) 31(1):18–29. doi: 10.1177/0884533615622640
27. Hoffmann H, Kettelhack C. Fast-track surgery–conditions and challenges in postsurgical treatment: a review of elements of translational research in enhanced recovery after surgery. European Surg Res. (2012) 49(1):24–34. doi: 10.1159/000339859
28. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. (2017) 152(3):292–8. doi: 10.1001/jamasurg.2016.4952
29. Fearon KC, Ljungqvist O, Von Meyenfeldt M, Revhaug A, Dejong CH, Lassen K, et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr. (2005) 24(3):466–77. doi: 10.1016/j.clnu.2005.02.002
30. Ban KA, Berian JR, Ko CY. Does implementation of enhanced recovery after surgery (ERAS) protocols in colorectal surgery improve patient outcomes? Clin Colon Rectal Surg. (2019) 32(2):109–13. doi: 10.1055/s-0038-1676475
31. Noba L, Rodgers S, Chandler C, Balfour A, Hariharan D, Yip VS. Enhanced recovery after surgery (ERAS) reduces hospital costs and improve clinical outcomes in liver surgery: a systematic review and meta-analysis. J Gastrointestinal Surg. (2020) 24(4):918–32. doi: 10.1007/s11605-019-04499-0
32. Ottesen M, Sørensen M, Rasmussen Y, Smidt-Jensen S, Kehlet H, Ottesen B. Fast track vaginal surgery. Acta Obstet Gynecol Scand. (2002) 81(2):138–46. doi: 10.1034/j.1600-0412.2002.810209.x
33. Magheli A, Knoll N, Lein M, Hinz S, Kempkensteffen C, Gralla O. Impact of fast-track postoperative care on intestinal function, pain, and length of hospital stay after laparoscopic radical prostatectomy. J Endourol. (2011) 25(7):1143–7. doi: 10.1089/end.2011.0020
34. Engelman RM, Rousou JA, Flack JE 3rd, Deaton DW, Humphrey CB, Ellison LH, et al. Fast-track recovery of the coronary bypass patient. Ann Thorac Surg. (1994) 58(6):1742–6. doi: 10.1016/0003-4975(94)91674-8
35. Zaouter C, Imbault J, Labrousse L, Abdelmoumen Y, Coiffic A, Colonna G, et al. Association of robotic totally endoscopic coronary artery bypass graft surgery associated with a preliminary cardiac enhanced recovery after surgery program: a retrospective analysis. J Cardiothorac Vasc Anesth. (2015) 29(6):1489–97. doi: 10.1053/j.jvca.2015.03.003
36. Noss C, Prusinkiewicz C, Nelson G, Patel PA, Augoustides JG, Gregory AJ. Enhanced recovery for cardiac surgery. J Cardiothorac Vasc Anesth. (2018) 32(6):2760–70. doi: 10.1053/j.jvca.2018.01.045
37. Recart A, Duchene D, White PF, Thomas T, Johnson DB, Cadeddu JA. Efficacy and safety of fast-track recovery strategy for patients undergoing laparoscopic nephrectomy. J Endourol. (2005) 19(10):1165–9. doi: 10.1089/end.2005.19.1165
38. Chughtai B, Abraham C, Finn D, Rosenberg S, Yarlagadda B, Perrotti M. Fast track open partial nephrectomy: reduced postoperative length of stay with a goal-directed pathway does not compromise outcome. Adv Urol. (2008) 2008:507543. doi: 10.1155/2008/507543
39. Gralla O, Haas F, Knoll N, Hadzidiakos D, Tullmann M, Romer A, et al. Fast-track surgery in laparoscopic radical prostatectomy: basic principles. World J Urol. (2007) 25(2):185–91. doi: 10.1007/s00345-006-0139-2
40. McAchran SE, Goldman HB. Contemporary length of stay and resource utilization when using a fast-track regimen for mid-urethral sling surgery. Urology. (2009) 74(3):531–4. doi: 10.1016/j.urology.2009.04.039
41. Nelson G, Altman AD, Nick A, Meyer LA, Ramirez PT, Achtari C, et al. Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: enhanced recovery after surgery (ERAS®) society recommendations–Part I. Gynecol Oncol. (2016) 140(2):313–22. doi: 10.1016/j.ygyno.2015.11.015
42. Bisch SP, Jago CA, Kalogera E, Ganshorn H, Meyer LA, Ramirez PT, et al. Outcomes of enhanced recovery after surgery (ERAS) in gynecologic oncology - a systematic review and meta-analysis. Gynecol Oncol. (2021) 161(1):46–55. doi: 10.1016/j.ygyno.2020.12.035
43. Varadhan KK, Neal KR, Dejong CH, Fearon KC, Ljungqvist O, Lobo DN. The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr. (2010) 29(4):434–40. doi: 10.1016/j.clnu.2010.01.004
44. Taniguchi H, Sasaki T, Fujita H, Kobayashi H, Kawasaki R, Goloubev M, et al. Modified ERAS protocol using preoperative oral rehydration therapy: outcomes and issues. J Anesth. (2014) 28(1):143–7. doi: 10.1007/s00540-013-1769-3
45. Zhou B, Ji H, Liu Y, Chen Z, Zhang N, Cao X, et al. ERAS reduces postoperative hospital stay and complications after bariatric surgery: a retrospective cohort study. Medicine. (2021) 100(47):e27831. doi: 10.1097/md.0000000000027831
46. Tweed TTT, Woortman C, Tummers S, Bakens M, van Bastelaar J, Stoot J. Reducing hospital stay for colorectal surgery in ERAS setting by means of perioperative patient education of expected day of discharge. Int J Colorectal Dis. (2021) 36(7):1535–42. doi: 10.1007/s00384-021-03948-0
47. Tamang T, Wangchuk T, Zangmo C, Wangmo T, Tshomo K. The successful implementation of the Enhanced Recovery After Surgery (ERAS) program among caesarean deliveries in Bhutan to reduce the postoperative length of hospital stay. BMC Pregnancy Childbirth. (2021) 21(1):637. doi: 10.1186/s12884-021-04105-9
48. Currie A, Burch J, Jennie JT, Faiz O, Kennedy RH, Ljungqvist O, et al. The impact of enhanced recovery protocol compliance on elective colorectal cancer resection: results from an international registry. Ann Surg. (2015) 261(6):1153–9. doi: 10.1097/sla.0000000000001029
49. Geltzeiler CB, Rotramel A, Wilson C, Deng L, Whiteford MH, Frankhouse J. Prospective study of colorectal enhanced recovery after surgery in a community hospital. JAMA Surg. (2014) 149(9):955–61. doi: 10.1001/jamasurg.2014.675
50. Ament SM, Gillissen F, Moser A, Maessen JM, Dirksen CD, von Meyenfeldt MF, et al. Identification of promising strategies to sustain improvements in hospital practice: a qualitative case study. BMC Health Serv Res. (2014) 14:641. doi: 10.1186/s12913-014-0641-y
51. McLeod RS, Aarts MA, Chung F, Eskicioglu C, Forbes SS, Conn LG, et al. Development of an enhanced recovery after surgery guideline and implementation strategy based on the knowledge-to-action cycle. Ann Surg. (2015) 262(6):1016–25. doi: 10.1097/sla.0000000000001067
52. Renz BW, Kasparek MS, Seeliger H, Worthley DL, Jauch KW, Kreis ME, et al. The CR-POSSUM risk calculator predicts failure of enhanced recovery after colorectal surgery. Acta Chir Belg. (2015) 115(1):20–6. doi: 10.1080/00015458.2015.11681062
53. Chaudhary A, Barreto SG, Talole SD, Singh A, Perwaiz A, Singh T. Early discharge after pancreatoduodenectomy: what helps and what prevents? Pancreas. (2015) 44(2):273–8. doi: 10.1097/mpa.0000000000000254
54. Carli F, Scheede-Bergdahl C. Prehabilitation to enhance perioperative care. Anesthesiol Clin. (2015) 33(1):17–33. doi: 10.1016/j.anclin.2014.11.002
55. Lyon A, Solomon MJ, Harrison JD. A qualitative study assessing the barriers to implementation of enhanced recovery after surgery. World J Surg. (2014) 38(6):1374–80. doi: 10.1007/s00268-013-2441-7
Keywords: enhanced recovery after surgery, fast-track surgery, bibliometrics, bibliometrix, citespace
Citation: Zhang M, Wang X, Chen X, Song Z, Wang Y, Zhou Y and Zhang D (2022) A Scientometric Analysis and Visualization Discovery of Enhanced Recovery After Surgery. Front. Surg. 9:894083. doi: 10.3389/fsurg.2022.894083
Received: 11 March 2022; Accepted: 19 May 2022;
Published: 8 June 2022.
Edited by:
Francesco Giovinazzo, Agostino Gemelli University Polyclinic (IRCCS), ItalyReviewed by:
Vincenzo Lizzi, Azienda Ospedaliero-Universitaria Ospedali Riuniti di Foggia, ItalyCopyright © 2022 Zhang, Wang, Chen, Song, Wang, Zhou and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dandan Zhang emhhbmdkZEBzai1ob3NwaXRhbC5vcmc=
Specialty section: This article was submitted to Surgical Oncology, a section of the journal Frontiers in Surgery
Abbreviations: ERAS, Enhanced recovery after surgery; TC, total citations; NP, Net output; FTS, Fast-track surgery.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.