 Eleonora Maddalena Minerva
Eleonora Maddalena Minerva Adele Tessitore
Adele Tessitore Stefano Cafarotti
Stefano Cafarotti Miriam Patella
Miriam Patella
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 28 April 2022
Sec. Thoracic Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.884048
This article is part of the Research Topic Women in Thoracic Surgery View all 6 articles
Introduction: Rural populations in large countries often receive delayed or less effective diagnosis and treatment for lung cancer. Differences are related to population-based factors such as lower pro capita income or increased risk factors or to differences in access to facilities. Switzerland is a small, rich country with peculiar geographic and urban characteristics.
We explored the relationship between lung cancer diagnostic–surgical pathway and urban–rural residency in our region.
Methods: We retrospectively analyzed the medical records of 280 consecutive patients treated for primary non-small cell lung cancer at our institution (2017–2021). This is a regional tertiary center for diagnosis and treatment, and data were extracted from a prospectively collected clinical database. We included anatomical lung resection. Collected variables included patients and surgical characteristics, risk factors, comorbidities, histology and staging, symptoms (vs. incidental diagnosis), general practitioner (GP) involvement, health insurance, and suspected test-treatment interval. The exposure was rurality, defined by the 2009 rural–urban residency classification from the Department of Land.
Results: A total of 150 patients (54%) lived in rural areas. Rural patients had a higher rate of smoking history (93% vs. 82%; p = 0.007). Symptomatic vs. incidental diagnosis did not differ as well as previous cancer rate, insurance, and pathological staging. In rural patients, there was a greater burden of comorbidities (mean Charlson Comorbidity Index Age-Adjusted 5.3 in rural population vs. 4.8 in urban population, p = 0.05), and GP was more involved in the diagnostic pathway (51% vs. 39%, p = 0.04). The interval between the first suspected test and treatment was significantly shorter (56 vs. 66.5 days, p = 0.03). Multiple linear regression with backward elimination was run. These variables statistically predicted the time from the first suspected test and surgical treatment [F(3, 270), p < .05, R2 = 0.24]: rurality (p = 0.04), GP involvement (p = 0.04), and presence of lung cancer-related symptoms (p = 0.02).
Conclusions: In our territory with inhomogeneous population distribution and geographic barriers, residency has an impact on the lung cancer pathway. It seems paradoxical that rural patients had a shorter route. The more constant involvement of GP might explain this finding, having suggested more tests for high-risk patients in the absence of symptoms or follow-ups. This did not change the staging of surgical patients, but it might be essential for the organization of an effective lung cancer screening program.
In the recent past, there has been increasing interest in the literature in studying cancer outcome inequalities among population subgroups, such as urban vs. rural residents. Rurality is often presented as a risk factor for poor cancer outcomes in various types of malignancies (1–3).
The causes of these rural–urban disparities in lung cancer prognosis are yet poorly defined (4). It seems that people living in the countryside have more risk factors than urban residents. Several studies have recognized among rural residents higher rates of cancer-risk behaviors such as cigarette smoking, poorer diet, alcohol abuse, physical inactivity, and obesity (4–6). An additional explanatory factor in broad countries such as the United States and Australia is that a considerable percentage of uninsured or underinsured patients come from rural regions (1, 4, 6–8). Furthermore, rural inhabitants often present lower incomes and lower educational levels than their urban counterparts (1, 2, 6, 7). The result of these factors combined is a delay in healthcare referral. This delay causes in turn a later disease stage at presentation, meaning a reduced range of therapeutic choices and worse survival rates (1, 4).
However, the above-mentioned data are mostly extracted by studies performed in extremely wide and non-homogeneous countries, in terms of both population and socio-economical levels, such as the United States and Australia (1–3). Therefore, it seems to be interesting to study and verify this phenomenon at a local level in order not to generalize the results (8, 9), especially with a view to introducing a screening program (10). Switzerland is a tiny state with 8,670,000 inhabitants, with one of the highest per capita incomes worldwide. Its great environmental and administrative diversity may render the Helvetic Confederation a case study for the peculiar distribution of its healthcare system. Canton Ticino is not an exception, and the Department of Land provides a detailed chart of this variability, defining “functional regions” based on the local socio-economical development (11, 12).
Our interest as oncological surgeons of the regional referral center is to analyze timing and possible variability of the diagnostic–therapeutic pathway of lung carcinoma within our region.
Tessin is a region defined as a canton in Switzerland, with a population of 351,000 residents. Its area extends 2,812.21 km2, with 80% of the land being constituted by mountains and 15% by hills. Approximately half of the inhabitants live in urban areas, while the rest of the population is distributed in rural territories (11). Based on population density, residency areas are divided into five categories according to the description provided by the Department of Land (12). High-density area (>80 inhabitants per hectare) is defined as primarily urban. This is followed by the communities of the suburban area (45–80 inhabitants per hectare), with decreasing density and specific urban characteristics. These two areas make up the agglomeration (urban), while the periurban, the hinterland, and the mountains constitute the suburban rural areas (<45 inhabitants per hectare).
The Swiss healthcare system is based on a federalist structure, which means that the federal government, cantons, and local municipalities assume different tasks in the healthcare system. In accordance with the Swiss Federal Health Insurance Act (KVG/HIA), basic insurance is compulsory for anyone and it can be public, semi-private, or private, depending on the level of coverage.
According to the Euro Health Consumer Index Report (13), which took into consideration patient rights, access to healthcare, preventive care, and a range of benefits, Switzerland ranked first in 2018.
Ente Ospedaliero Cantonale is the public regional tertiary center for the diagnosis and treatment of lung cancer with specific facilities and surgical expertise (14) and multidisciplinary team (MDT) discussion on a regular basis.
Patients with suspected/ascertained lung cancer are referred for MDT discussion and selected for surgery according to current functional (15) and oncological (16) guidelines. Referring physicians can include internal specialists as well as general practitioners (GPs) and other external physicians from either public or private settings.
The database containing the consecutive anatomical lung resections (segmentectomy, lobectomy, bilobectomy, and pneumonectomy) performed at our institution was screened. Being a clinical prospectively collected database, the completeness and the accuracy of the data were extremely high, with the maximum rate of missing data being 3% for a single variable. Between January 2017 and December 2021, the database included 350 procedures. Patients with a diagnosis of primary non-small cell lung cancer (NSCLC) were included in the study. Patients with a diagnosis of small cell lung cancer, typical carcinoid, benign disease, metastasis from other organs, and recurrence of lung cancer were excluded. For the purpose of the study, we also excluded patients who underwent neoadjuvant treatments. The study was approved by the local ethical committee (protocol number 2022-00184).
Collected variables included patients and surgical characteristics, together with risk factors (smoking exposure) and comorbidities [Charlson Comorbidity Index Age-Adjusted (CCI)], histology, symptoms (vs. incidental diagnosis), GP involvement, and type of health insurance. The outcome of interest was the suspected test-treatment interval (defined as the number of days between the first imaging leading to a suspicion of lung cancer and the surgical treatment). To verify the possible impact on cancer prognosis, we also analyzed the final pathological staging. The exposure variable was rurality.
Screened variables were considered based on their impact on the rapidity of the diagnostic–therapeutic pathway. As we can find in the literature, we identified possible confounders that could contribute to making a variation in the lung cancer diagnostic pathway: previous history of malignancy requiring follow-up, presence of lung cancer-related symptoms, and insurance status (5, 17, 18). Patients affected by previous cancer undergo radiological follow-ups, during which incidental findings of lung cancer can be observed with a higher probability compared to patients who do not undergo regular imaging (17). Moreover, the presence of typical symptoms usually leads to a timely diagnosis rather than their absence (18). Eventually, underinsured people are less likely to seek early medical attention in order not to face supplementary expenses (5).
Collected variables and outcomes were analyzed and compared in the two groups of exposure. Continuous variables were tested for normality with the Shapiro–Wilk W test. Normally distributed variables were analyzed using the Student t-test; skewed distributed ones were analyzed with the Mann–Whitney U test. Categorical variables were tested by means of Fisher’s exact test (in case the number of observations was less than 10 in at least one cell) or the chi-squared test. Variables with statistical significance difference at univariable analysis and, regardless of their statistical significance, variables considered as potential confounders were included in a multiple regression analysis with backward elimination to verify the impact on the outcome. The level of significance was set at 0.05; all statistical analyses were performed using STATA software (StataCorp LLC, College Station, TX, USA).
A total of 280 patients were eligible for the analysis. A total of 150 patients (54%) lived in rural areas. We performed 248 lobectomies/bilobectomies, 28 segmentectomies, and 4 pneumonectomies (Table 1). Lymphadenectomy was performed in all cases. Demographic characteristics did not differ significantly across residencies. Rural patients had a higher rate of smoking history (93% vs. 82%; p = 0.007) and a slightly significant trend to have a greater burden of comorbidities (mean CCI 4.8 vs. 5.3, p = 0.05). The number of patients who had positron emission tomography scan, preoperative mediastinal staging by means of endoscopic ultrasound or mediastinoscopy, and the number of cancer diagnoses obtained before the curative resection did not differ between groups. For rural patients, GPs were significantly more involved in the diagnostic pathway (51% vs. 39%, p = 0.04) and the interval between the first suspected test and treatment was significantly shorter (56 vs. 66.5 days, p = 0.03). The cumulative median interval time between the first suspected test and surgery was 61 days (IQR: 46–90) with a difference of 10.5 days. Figure 1 shows the difference in days between the median interval between the first suspected test and treatment for the two groups. The final pathological staging did not differ in the two groups. Adenocarcinoma histology was more frequent in urban patients (78% vs. 67%, p = 0.04).
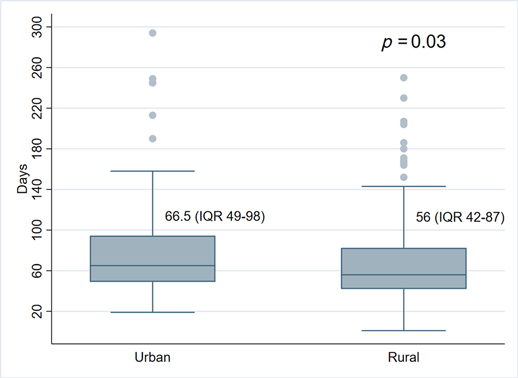
Figure 1. Median first suspected test-operation interval in urban–rural patients.
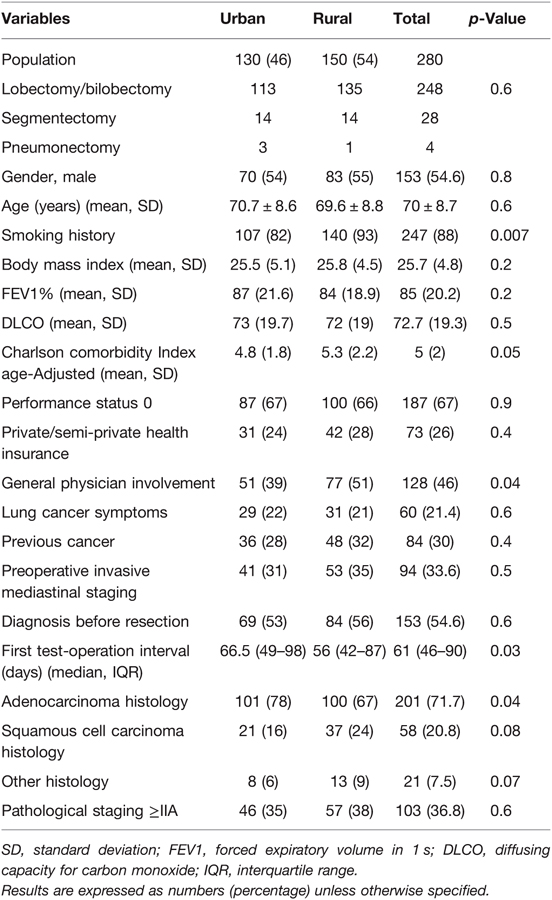
Table 1. Patients’ characteristics and differences based on the results of univariable analysis.
The number of symptomatic vs. incidental diagnoses did not differ between groups (Table 2). Among symptomatic patients, there was no difference in the interval between the first suspected test and treatment [median 57 days (IQR: 46–91) vs. 56 days (IQR: 40–73); p = 0.2]. Neither was there a statistical difference in the interval between symptoms onset and the first suspected test for the same patients [median 33.5 days (IQR: 12.5–73.5) vs. 29.5 days (IQR: 10–61); p = 0.8]. On the other hand, regarding patients with no cancer-related symptoms, we found a statistically significant difference in the interval between the first suspected test and treatment across urban/rural residency [median 69.5 days (IQR: 53–105) vs. 60.5 days (IQR: 42–92); p = 0.04]. The number of patients under regular follow-ups for previous malignancies was similar in the two groups, as well as the insurance status.
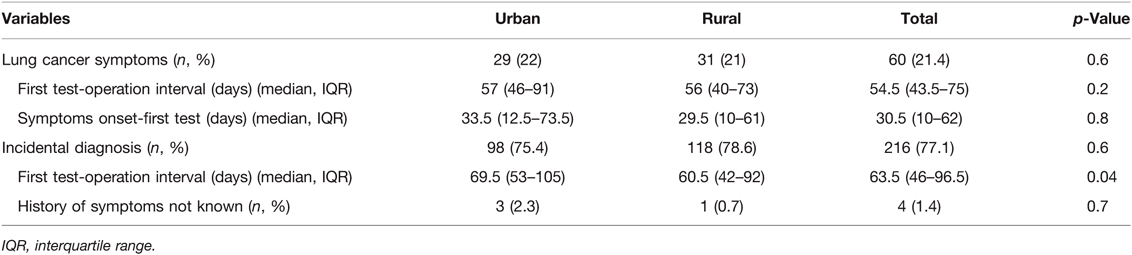
Table 2. Details of analysis according to the presence/absence of cancer-related symptoms.
Results of the univariable analysis are summarized in Table 1.
Statistical significantly different variables and confounders were included in a multivariable analysis. Multiple linear regression with backward elimination was run. These variables statistically predicted the time from the first suspected test and surgical treatment [F(3, 270), p < 0.05, R2 = 0.24]: rurality (p = 0.04), GP involvement (p = 0.04), and presence of lung cancer-related symptoms (p = 0.02) (Table 3).

Table 3. Results of multiple linear regression analysis after backward elimination.
Our analysis showed that patients residing in rural areas in Tessin had a shorter lung cancer diagnostic and surgical treatment pathway compared with the ones who lived in urban areas, with a difference of 10.5 days between groups. These results are in contrast with most published literature on this topic. As demonstrated by the large number of papers published in the last few years, the interest in the disparities in cancers incidence, timing of diagnosis, appropriateness of treatment, and survival, related to patients’ residency, is constantly increasing (1–6). Most studies showed that all indicators have a steady inverse relationship with residency as they progressively worsened with increasing remoteness from the urban area (2). The reason leading to these disparities could be found in population-based factors or in provider issues. Increased rural lung cancer mortality might be explained by increased smoking prevalence in rural populations with subsequent greater cancer incidence (2). In general, the major behavioral determinants of cancer, such as smoking, diet, alcohol use, and occupational and environmental exposures, are influenced by the individual- and area-socio-economic factors (19).
In our population, we identified higher smoking exposure prevalence in rural populations even though this did not strictly correspond with socio-economic differences, as indirectly demonstrated by the lack of association with the insurance level. Indeed, we should consider that talking about economic deprivation might not be appropriate, as Switzerland is one of the richest European Countries. In 2018, the GDP (gross domestic product) percapita in Tessin stood at 94,700 US dollars, which is well above the average of the Western European Countries and the United States (34,000 and 63,600 US dollars, respectively) (19–21).
To make a constructive comparison with the published literature, we should also underline that most studies have been conducted in large countries as the United States and Australia (1–6), in which the population density and the extent of the geographic area are extremely different compared to a Swiss region. However, Tessin has its peculiar territorial organization and geographic characteristics. From the administrative point of view, residential areas are fragmented in more than 100 municipalities, and the territory is 80% mountainous. Moreover, if we consider historical and cultural aspects, Tessin is characterized by strong and ingrained parochial behaviors toward foreign countries but also internally within the canton (22). Along with the multicenter organization of the public hospital (EOC) divided into four structures located in the four major cities, it certainly contributes to patients’ reluctance to move between different hospital facilities for specialist visits. It is therefore important to study the association between cancer pathways disparities and rurality at the local level. As demonstrated by other authors, rurality can increase or decrease cancer-related risks and outcomes, suggesting a complex pattern (8).
After multivariable analysis, and controlling for confounders, we confirmed that the elements influencing the time between the first suspected test and surgical treatment were rurality, GP involvement, and the presence of lung cancer-related symptoms. This refers to the early stages of NSCLC for which upfront surgery is indicated.
These results are particularly interesting in the light of a future lung cancer screening program. The main difference in the timing from the first suspected test and surgery between urban–rural residents has been found in the group of non-symptomatic patients. Awareness of lung cancer symptoms seems equal across urban–rural residency, which is not a given assumption, as demonstrated by studies on other types of cancer (1). While there was no difference in the rate of patients under follow-up for previous malignancies, we found a statistical difference in comorbidities burden between the urban–rural groups. This might mean that rural residents presented more risk factors for lung cancer and underwent more prompt screening examinations in the absence of lung cancer symptoms. Moreover, the GP involvement during the diagnostic process, which was greater in the rural group, might have played a role. GPs represent the frontline healthcare professional with a comprehensive knowledge of patients’ general status, behavior, and clinical history, and the relationship of trust should not be underestimated. Whereas rurality has been pointed out as a limit in lung cancer screening programs in other studies because of the lack of access to facilities (10) or inadequacy of referral (23), our results indirectly suggest that people living in rural areas in Tessin have an adequate healthcare support. Enhancing symptoms awareness is important in detecting lung cancer diagnosis, but it seems to be not sufficient to change prognosis and survival and to increase GP attendance (24). In line with our results, efficient GP to specialist referral is a key point to minimizing delays in lung cancer diagnostic and treatment pathways (25).
Our study has some limitations. We analyzed only the lung cancer diagnosis that underwent surgical treatment. This means that we focused only on a specific population with early stages, sufficient reserves to support lung resection, and on the treatment with curative intent. We did not analyze advanced stages, which represent most lung cancer diagnoses. Indeed, we can extrapolate some data from a report from the Ticino Cancer Registry: in 2015–2016, out of 367 diagnoses of NSCLC, 50% were already in stage IV and 18% in stage III (24). In the same way, we did not have sufficient data to describe the diagnostic/treatment pathway for early stages that underwent nonsurgical treatment. However, according to the available reports, only 1.8% of stages I and II NSCLC at diagnosis did not receive radical surgery as treatment in Tessin (26). Therefore, a definitive conclusion on the effectiveness of diagnostic and treatment pathways across urban–rural residences cannot be made. In the same way, we did not know if and how many patients were excluded from the surgical treatment because of delay. Further studies should be pursued in this sense.
We did not have a personal patients’ income; we used the insurance status as a surrogate. We did not consider other factors, such as the educational level, which might have influenced the outcome.
We retrospectively analyzed a prospectively collected database. The retrospective analysis carries an inherent bias, but it is necessary to critically evaluate the quality of the care. Furthermore, the study considered a limited number of patients compared to the published literature, but the use of a clinical database increased enormously the quality of data. Compared to epidemiological databases used for the vast majority of studies on this topic, there was no indirect extrapolation of data about patients’ characteristics or diagnostic steps.
In conclusion, we pictured the real-world lung cancer surgical pathway at a local level. We identified significant differences in the timing of diagnosis and treatment between urban and rural populations, with the latter having a shorter route. Possible greater GP involvement might have contributed to this result, specifically in asymptomatic patients. Even though the results cannot be, and must not be, universally applied, our study gives some insights into a critical development of more equal and effective lung cancer pathways and suggests the need for a local tailored approach to lung cancer screening programs.
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
The studies involving human participants were reviewed and approved by Comitato Etico Cantonale Ticino. The patients/participants provided their written informed consent to participate in this study.
MP, EMM, SC, and AT contributed to the conception and design of the study. E-MM organized the database. MP performed the statistical analysis. E-MM and MP wrote the first draft of the manuscript. E-MM, MP, and AT wrote sections of the manuscript. All authors contributed to manuscript revision and read and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bergin RJ, Emery J, Bollar RC. Rural–urban disparities in time to diagnosis and treatment for colorectal and breast cancer. Cancer Epidemiol Biomarkers Prev. (2018) 27(9):1036–46. doi: 10.1158/1055-9965.EPI-18-0210
2. Atkins GT, Kim T, Munson J. Residence in rural areas of the United States and lung cancer mortality. Disease incidence, treatment disparities, and stage-specific survival. Ann Am Thorac Soc. (2017) 14(3):403–11. doi: 10.1513/AnnalsATS.201606-469OC
3. Ray MA, Faris NR, Rurality DA. Stage-stratified use of treatment modalities, and survival of non-small cell lung cancer. Chest. (2020) 158(2):787–96. doi: 10.1016/j.chest.2020.04.042
4. Fairfield KM, Black AW, Ziller EC. Area deprivation index and rurality in relation to lung cancer prevalence and mortality in a rural state. JNCI Cancer Spectr. (2020) 4(4): pkaa011. doi: 10.1093/jncics/pkaa011
5. Zahnd WE, James AS, Jenkins WD. Rural–urban differences in cancer incidence and trends in the United States. Cancer Epidemiol Biomarkers Prev. (2018) 27(11):1265–74. doi: 10.1158/1055-9965.EPI-17-0430
6. Fairfield KM, Black AW, Lucas FL. Association between rurality and lung cancer treatment characteristics and timeliness. J Rural Health. (2019) 35(4):560–5. doi: 10.1111/jrh.12355
7. Odahowski CL, Zahnd WE, Eberth JM. Challenges and opportunities for lung cancer screening in rural America. J Am Coll Radiol. (2019) 16(4 Pt B):590–5. doi: 10.1016/j.jacr.2019.01.001
8. Thompson JA, Chollet-Hinton L. The need to study rural cancer outcome disparities at the local level: a retrospective cohort study in Kansas and Missouri. BMC Public Health. (2021) 21(1):2154. doi: 10.1186/s12889-021-12190-w
9. Nelson D, McGonagle I, Jackson C. What is known about the role of rural-urban residency in relation to self-management in people affected by cancer who have completed primary treatment? A scoping review. Support Care Cancer. (2021) 29(1):67–78. doi: 10.1007/s00520-020-05645-0
10. Hasson RM, Fay KA, Phillips JD. Rural barriers to early lung cancer detection: exploring access to lung cancer screening programs in New Hampshire and Vermont. Am J Surg. (2021) 221(4):725–30. doi: 10.1016/j.amjsurg.2020.06.030
11. Structure of resident population. Ufficio federale di Statistica. Available from: https://www.bfs.admin.ch/bfs/it/home/statistiche/popolazione.assetdetail.18344219.html (Accessed February 13, 2022).
12. Revisione del Piano Direttore, Regioni e spazi funzionali (2009) del PD. Available from: https://www4.ti.ch/fileadmin/DT/temi/piano_direttore/pubblicazioni/Regioni_spazi_funzionali_2009_PD.pdf (Accessed February 13, 2022).
13. Euro Health Consumer Index (2018) Report. Issued by Health Consumer Powerhouse Ltd. Available from: https://healthpowerhouse.com/media/EHCI-2018/EHCI-2018-report.pdf (Accessed February 13, 2022).
14. Brunelli A, Falcoz PE, D’Amico T. European guidelines on structure and qualification of general thoracic surgery. Eur J Cardiothorac Surg. (2014) 45(5):779–86. doi: 10.1093/ejcts/ezu016
15. Brunelli A, Kim AW, Berger KI. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. (2013) 143(5 Suppl):e166S–90S. doi: 10.1378/chest.12-2395
16. National Comprehensive Cancer Network. Non-small cell lung cancer guideline. Version 1.2022. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1450 (Accessed February 20, 2022).
17. Cegla P, Scibisz-Dziedzic K, Witkowska K, Kubiak A, Wierzchoslawska E, Kycler W, et al. Detection of a second primary cancer in a 18F-fluorocholine PET/CT—multicentre retrospective analysis on a group of 1345 prostate cancer patients. Nucl Med Rev Cent East Eur. (2022) 25(1):25–30. doi: 10.5603/NMR.a2022.0006
18. Olsson JK, Schultz EM, Gould MK. Timeliness of care in patients with lung cancer: a systematic review. Thorax. (2009) 64(9):749–56. doi: 10.1136/thx.2008.109330
19. Singh GK, Williams SD, Siahpush M. Socioeconomic, rural–urban, and racial inequalities in US cancer mortality: Part I—all cancers and lung cancer and part II—colorectal, prostate, breast, and cervical cancers. J Cancer Epidemiol. (2011) 2011:107497. doi: 10.1155/2011/107497
20. Federal Statistical Office. Regional Portraits and Key Figures. Available from: https://www.bfs.admin.ch/bfs/en/home/statistics/regional-statistics/regional-portraits-key-figures/cantons/ticino.html (Accessed February 15, 2022).
21. GDP Per Capita – Current US $ European Union, 1970–2020. Available from: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=EU (Accessed March 23rd, 2022).
22. Keel S, Mondada L. The micro-politics of sequential organization contributions from conversation analysis and ethnomethodology. J Lang Polit. (2017) 16(1):1–19. doi: 10.1075/jlp.16.1.01kee
23. Le T, Miller S, Berry E. Implementation and uptake of rural lung cancer screening. J Am Coll Radiol. (2022) 19: 480–7. doi: 10.1016/j.jacr.2021.12.003
24. Ball S, Hyde C, Hamilton W. An evaluation of a national mass media campaign to raise public awareness of possible lung cancer symptoms in England in 2016 and 2017. Br J Cancer. (2022) 126(2):187–95. doi: 10.1038/s41416-021-01573-w
25. Malalasekera A, Dhillon HM, Shunmugasundaram C. Why do delays to diagnosis and treatment of lung cancer occur? A mixed methods study of insights from Australian clinicians. Asia Pac J Clin Oncol. (2021) 17(2):e77–e86. doi: 10.1111/ajco.13335
26. Quality Indicators for Lung Cancer Care in Canton Ticino (Southern Switzerland), 2015–2016. Available from: https://m4.ti.ch/fileadmin/DSS/DSP/RCT/pdf/Relazioni_poster/2019/Ortelli_Giornata_Ricerca.pdf (Accessed April 3, 2022).
Keywords: lung cancer, treatment disparities, surgical treatment, rurality, screening
Citation: Minerva EM, Tessitore A, Cafarotti S and Patella M (2022) Urban–Rural Disparities in the Lung Cancer Surgical Treatment Pathway: The Paradox of a Rich, Small Region. Front. Surg. 9:884048. doi: 10.3389/fsurg.2022.884048
Received: 25 February 2022; Accepted: 7 April 2022;
Published: 28 April 2022.
Edited by:
Monica Casiraghi, European Institute of Oncology (IEO), ItalyReviewed by:
Lucia Mangone, IRCCS Local Health Authority of Reggio Emilia, ItalyCopyright © 2022 Minerva, Tessitore, Cafarotti and Patella. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miriam Patella bWlyaWFtLnBhdGVsbGFAZW9jLmNo
†These authors have contributed equally to this work and share the first authorship
Specialty section: This article was submitted to Thoracic Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.