 Sayaka Horiuchi
Sayaka Horiuchi Kohei Kanaya
Kohei Kanaya Tetsuyoshi Horiuchi
Tetsuyoshi Horiuchi
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg., 19 April 2022
Sec. Neurosurgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.881874
This article is part of the Research TopicSeizures in Brain TumorsView all 5 articles
Objective: Postoperative seizures and epilepsy are common complications of craniotomy. In this study, we aimed to investigate the characteristics of seizures and epilepsy after craniotomy.
Methods: A total of 293 consecutive craniotomy surgeries were analyzed. Infratentorial surgeries, epilepsy surgeries, surgeries using the same approach conducted for the same patients, and the cases with incomplete clinical data were excluded. A total of 211 surgeries were included in this study. We evaluated the following clinical characteristics in all patients: sex, age, preoperative epilepsy, use of preoperative antiseizure medication (ASM), indication for operation, early postoperative seizure (EPS), delayed postoperative seizure (DPS), and postoperative de novo epilepsy. The day of onset of EPSs was defined as within 7 days post-surgery, and the day of onset of DPSs was defined as later than 7 days and less than 60 days post-surgery.
Results: Twenty-eight patients were previously diagnosed with epilepsy. Nine patients had EPSs (4.3%), and 10 patients had DPSs (4.7%). Seven cases of EPSs and six cases of DPSs were observed in 183 patients without previous epilepsy (3.8% and 3.3%, respectively). Three of the seven patients with EPSs (42.9%) and all six patients with DPSs (100%) developed de novo epilepsy. Postoperative de novo epilepsy was observed in 9 (4.9%) of the 183 patients without epilepsy. EPSs and DPSs were significant risk factors for epilepsy (p < 0.01). The odds ratios of EPSs and DPSs for the development of epilepsy were 12.71 (95% confidence interval [CI]: 3.94–112.80; p < 0.01) and 22.88 (95% CI: 5.38–55.72; p < 0.01), respectively. ASM was administered prophylactically to 51 patients. The prophylactic use of ASMs did not prevent EPSs or postoperative de novo epilepsy.
Conclusion: EPSs and DPSs occurred in 4.3% and 4.7% of the patients, respectively, after craniotomy. Postoperative de novo epilepsy occurred in 4.9% of patients. This study revealed that EPSs and DPSs were risk factors for de novo epilepsy. Previous epilepsy was not a significant risk factor for EPSs. The prophylactic use of ASMs did not prevent EPSs or de novo epilepsy.
Postoperative seizures and epilepsy are common complications of craniotomy surgery. Postoperative seizures were considered as early postoperative seizures (EPS) and delayed postoperative seizures (DPS). Previous reports showed that postcraniotomy seizures occurred in 11.9% of patients who underwent decompressive craniectomy (1). EPS was observed in 6.1% of patients undergoing supratentorial tumor surgery (2), and 17% of patients who underwent supratentorial surgery developed postoperative epilepsy (3). Another report showed that 43% of patients who underwent meningioma surgery experienced DPS (4).
Postoperative seizures and epilepsy can differ depending on the patient, disease, pathology, type of surgery, and previous history (5). Although some reports showed the risk of epilepsy following stroke (6, 7), meningioma surgery (8), and craniotomy (9), the relationship between EPS, DPS, and de novo epilepsy after craniotomy is not well known. The purpose of this study is to investigate the occurrence and relationship of EPS, DPS, and de novo epilepsy after various neurosurgical treatments. Furthermore, this study also aimed to evaluate the effectiveness of prophylactic use of antiseizure medication (ASM). Our research can provide unique contributions to how to treat postoperative seizures and when to diagnose de novo epilepsy after craniotomy surgeries.
Data were retrospectively collected from 293 consecutive craniotomy surgeries performed at the Neurosurgical Department of Shinshu University Hospital from January 2017 to May 2021. Infratentorial surgeries, epilepsy surgeries, surgeries using the same approach conducted for the same patients, and the cases with incomplete clinical data were excluded. A total of 211 surgeries were included in this study. The average observational period was 18.1 months. We evaluated the following clinical characteristics in all patients: sex, age, preoperative epilepsy, use of preoperative antiseizure medication (ASM), indication for operation, EPS, DPS, and de novo epilepsy. The day of onset of EPSs was defined as within 7 days post-surgery, and the day of onset of DPSs was defined as later than 7 days and less than 60 days post-surgery. Epilepsy was defined as the presence of any of the following conditions: (1) at least two unprovoked seizures occurring >24 h apart; (2) one unprovoked seizure and a probability of further seizures similar to the general recurrence risk after two unprovoked seizures, occurring over the next 10 years (10). De novo epilepsy was defined as postoperative newly diagnosed epilepsy in the observational period. This study was approved by the Ethics Committee of Shinshu University School of Medicine (IRB number 5391).
Data are presented as mean ± standard deviation. Fisher’s exact test was used to assess the relationship between EPS and DPS and epilepsy, and EPS and de novo epilepsy and ASM use. Univariate regression analysis was used to assess the strength of the association between EPSs and DPSs and postoperative de novo epilepsy. Statistical significance was set at p < 0.05. SPSS (version 27; SPSS, Inc., Chicago, IL, USA) was used for statistical analysis.
The patient characteristics are presented in Table 1. The study included 97 males and 114 females. The average age was 56.1 ± 18.4 (range 10–97) years. Twenty-eight patients were previously diagnosed with epilepsy. Nine patients had EPSs (4.3%), and ten patients had DPSs (4.7%). Among the 183 patients without epilepsy, seven patients had EPSs, and six patients had DPSs (3.8% and 3.3%, respectively). Among the 28 patients with epilepsy, two patients had EPSs, and four patients had DPSs (7.1% and 14.3%, respectively). Postoperative de novo epilepsy was observed in nine of the 183 patients without previous epilepsy (4.9%).
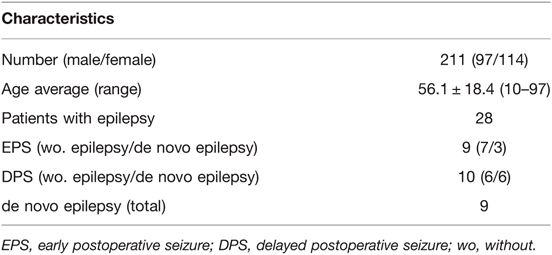
Table 1. Clinical characteristics.
The patient characteristics are presented in Table 2. Twelve patients of 41 gliomas (29.3%), five patients of 31 meningiomas (16.1%), two patients of 14 metastatic brain tumors (14.3%), one patient of 40 unruptured aneurysms (2.5%), and two patients of 12 moyamoya diseases (16.7%) had focal epilepsy preoperatively. Of the nine patients with EPSs, four cases of glioma, three cases of unruptured aneurysms, one case of moyamoya disease, and one case of intracranial hemorrhage (ICH) were observed. Among the patients with epilepsy, two had EPSs. Among the patients without epilepsy, seven had EPSs. EPSs only occurred in four cases, and three cases of EPSs developed into postoperative de novo epilepsy. Four cases of DPSs were observed in patients with epilepsy. Six cases had DPSs among the patients without epilepsy, and all six patients with DPSs with no history of epilepsy developed postoperative de novo epilepsy. The average diagnosis period from craniotomy to the onset of de novo epilepsy was 22.3 (range 9–52) postoperative days.
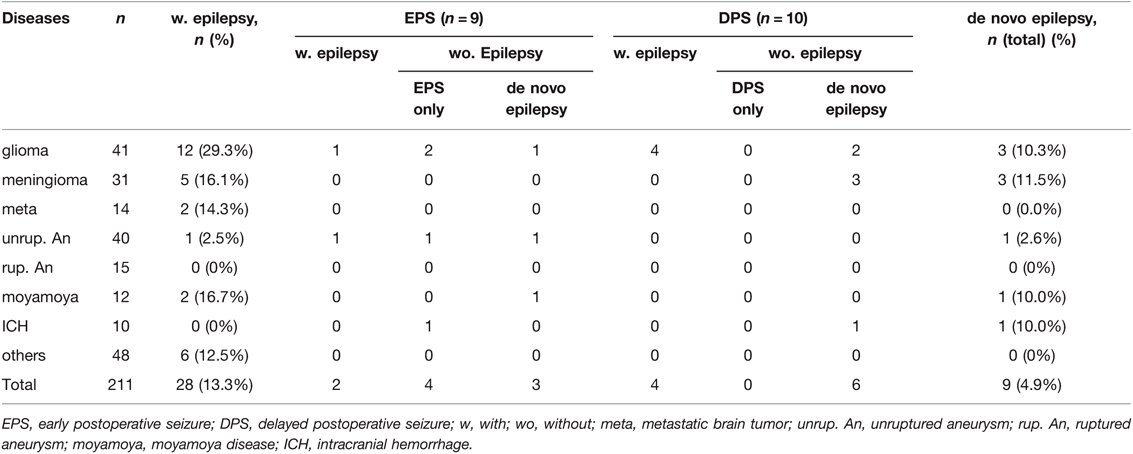
Table 2. Clinical characteristics of epilepsy, EPS, DPS and de novo epilepsy.
Three of the 29 gliomas (10.3%), three of the 26 meningiomas (11.5%), one of the 39 unruptured aneurysms (2.6%), one of the cases of 10 moyamoya diseases (10.0%), and one of the 10 ICHs (10.0%) developed into postoperative de novo epilepsy. In total, nine of the 183 patients who underwent craniotomy surgeries (4.9%) developed postoperative de novo epilepsy.
There was no significant difference between EPSs and the presence of preoperative epilepsy (p = 0.34); however, there was a significant difference between DPSs and the presence of preoperative epilepsy (p = 0.029) (Table 3). No significant relationship was observed between EPSs and the presence of preoperative epilepsy.

Table 3. The relationship of EPS, DPS and previously diagnosed epilepsy.
Of the 183 patients without epilepsy, three of the seven patients with EPS (42.9%) and all six patients with DPS (100%) developed postoperative de novo epilepsy. EPSs and DPSs were significant risk factors for epilepsy (p < 0.01). The odds ratios of EPSs and DPSs for the development of epilepsy were 12.71 (95% confidence interval [CI]: 3.94–112.80; p < 0.01) and 22.88 (95% CI: 5.38–55.72; p < 0.01), respectively (Table 4).
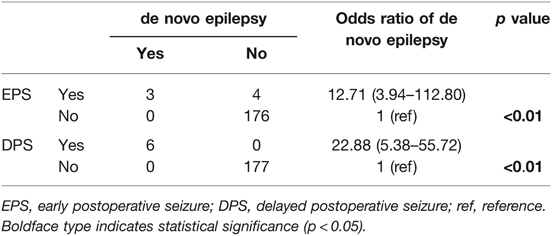
Table 4. The relationship and univariate regression analysis of EPS, DPS and de novo epilepsy.
ASM was administered prophylactically to 51 patients. Interestingly, the prophylactic use of ASMs did not prevent EPS; however, ASM use was also a risk factor for EPSs (p = 0.039). Furthermore, the prophylactic use of ASMs did not prevent postoperative de novo epilepsy (p = 0.71) (Table 5).
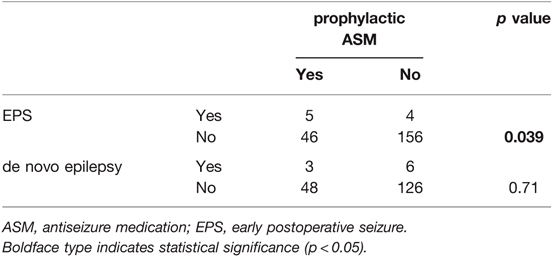
Table 5. The relationship of EPS, de novo epilepsy and prophylactic ASM.
Our study revealed that EPS and DPS occurred in 4.3% and 4.7% after craniotomy surgery, respectively. Three of the seven patients with EPS (42.9%) and all six patients with DPS (100%) developed de novo epilepsy. Postoperative de novo epilepsy occurred in 4.9% of patients after craniotomies in our study. Furthermore, the prophylactic use of ASMs did not prevent EPSs or de novo epilepsy.
Although the incidence of de novo epilepsy after craniotomies can be influenced by the observational period, a recent report showed that the overall 6-month, 1-year, and 5-year postoperative cumulative risks of de novo epilepsy after craniotomy were 9.7% (95% CI: 9.1–10.3), 13.9% (95% CI: 13.2–14.6), and 20.4% (95% CI: 19.5–21.3), respectively (9).
Our study revealed that DPSs and EPSs could be risk factors for de novo epilepsy. On the other hand, Beghi reported that early seizures alone are not sufficient to diagnose epilepsy, as they are deemed to be provoked (11). Seizures are considered acute symptomatic if they occur within the first 7 days of cerebrovascular disease (12, 13). Our data showed that all DPSs cases developed de novo epilepsy; on the other hand, about half of EPSs cases developed de novo epilepsy. We speculated that although EPSs can be similar to provoked seizures, DPSs can be related to unprovoked seizures, which is necessary for defining epilepsy. Therefore, DPSs seem to be a prominent factor for postoperative de novo epilepsy. Several studies have reported that seizure recurrence is more common in patients with late seizures than in those with early seizures (14, 15). Furthermore, Doria reported that late seizure following stroke had a high risk (55%–93%) for the development of epilepsy, although early seizure had a low risk (29%–35%) (16), which is concordant to our data although the patient cohorts were different. Early seizure after stroke may be related to acute neuronal injury and subsequent glutamate-mediated excitotoxicity, ion channel dysfunction, and blood barrier disruption (17–20). Late seizures after stroke may be related to secondary gliotic scarring with associated changes in membrane properties, chronic inflammation, neurodegeneration, and altered synaptic plasticity, eventually leading to hyperexcitability and increased synchronization of neuronal activities (21, 22).
In general, the prediction of postoperative seizures and de novo epilepsy may be challenging, Galovic proposed the SeLECT score to predict the risk of late seizures after stroke. The model incorporated five items: severity of stroke, large-artery atherosclerotic aetiology, early seizures, cortical involvement, and territory of middle cerebral artery involvement (7). Wirsching also reported that the predictors of poor postoperative seizure control after meningioma resection included preoperative epilepsy, epileptiform potentials on postoperative EEG recordings, severe surgical complications including CNS infections, hydrocephalus, recraniotomy, and symptomatic intracranial hemorrhage, younger age, and tumor progression (8).
Our study showed that previous epilepsy was a risk factor for DPSs but not EPSs. Furthermore, the prophylactic use of ASMs did not prevent EPSs and de novo epilepsy. Controversially, the prophylactic usage of ASMs was a risk factor for EPSs. This result suggests that the use of ASMs was not effective in preventing EPSs, although the possible risk factors of EPS such as the location of the lesion, indication for operation, and preoperative epilepsy were concerned. Previous studies have found no significant difference in the development of late seizures between patients receiving and not receiving prophylactic ASMs, suggesting that ASMs do not prevent epileptogenesis (23–25). Prophylactic ASM in patients with newly diagnosed brain tumors is not recommended because it is not effective in preventing seizures (26), and prophylactic ASM is not recommended routinely because of drug-related side effects (27). Postoperative seizures occur most often in the first week to the first month after surgery for patients with and without tumors (28, 29). If patients are treated perioperatively, tapering and discontinuing ASMs after the first postoperative week are recommended (26). The prophylactic use of ASMs was not effective in preventing postoperative seizures and epilepsy in our study. Therefore, ASM should be used based on the diagnosis of epilepsy. If ASMs are used prophylactically, they should not be used inappropriately for a longer time and should be discontinued in the early postoperative period.
The postoperative seizures were classified as either EPSs or DPSs. EPSs can be related to acute symptomatic seizures associated with craniotomy; however, DPSs can be comparable to unprovoked seizures, which may indicate seizures associated with epilepsy. Of seven DPS cases without previous epilepsy, four cases with focal motor seizure (FMS), one case with focal impaired awareness seizure (FIAS), and one case with focal to bilateral tonic-clonic seizure (FBTCS) were observed as DPSs based on the basic ILAE 2017 operational classification of seizure types (30).
The day of seizure onset after craniotomy is an important factor in diagnosing epilepsy. It can be hard to diagnose epilepsy if only one seizure occurs, especially during the early postoperative period. We consider these cases are preferred to be followed conservatively and carefully without administering ASMs. It is estimated that 20%–30% of cases are indeed misdiagnosed as epileptic seizures (31, 32). Perrig emphasized that patients should not be treated if there is uncertainty about the diagnosis of epilepsy, and “wait and see” for the next event can prevent the misdiagnosis of epilepsy (33).
This study has several limitations. First, this was a retrospective analysis of patients treated at a single institution with a relatively small sample size. Second, the follow-up duration varied among the patients. The incidence of delayed postoperative seizures and postoperative epilepsy could be influenced by follow-up duration. Third, electroencephalography (EEG) is an important test for diagnosing epilepsy; however, EEG was not performed on all patients, and its data was not included in the analysis. Despite these limitations, this study highlights the occurrence and characteristics of EPSs, DPSs, and de novo epilepsy, and the appropriate usage of ASMs after craniotomy. This study can contribute to help how to treat EPSs and DPSs. Furthermore, this study revealed that postoperative de novo epilepsy was developed about one month after craniotomy, which can be valuable information for surgeons and patients.
The mechanism of de novo epilepsy after craniotomy surgery can be multifactorial, Giraldi suggested that cortical trauma, gliosis, and changes in microcirculation following a craniotomy can be a risk of de novo epilepsy (9). The activation of neuroinflammatory pathways was also reported as a contribution to epilepsy (34). Further basic and clinical studies are necessary to elucidate the mechanism of de novo epilepsy after craniotomy surgery.
Herein, we reported the clinical characteristics and occurrence of EPSs, DPSs, and de novo epilepsy after craniotomy. Our study revealed that EPSs and DPSs occurred in 4.3% and 4.7% of the patients, respectively. De novo epilepsy occurred in 4.9% of the patients. EPSs and DPSs are risk factors for de novo epilepsy. Previous epilepsy was not a significant risk factor for EPSs. The prophylactic use of ASMs did not prevent EPSs or de novo epilepsy.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by The Ethics Committee of Shinshu University School of Medicine (IRB number 5391). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
All authors contributed to the conception and design of the study. Data collection and analysis were performed by SH and KK. The first draft of the manuscript was written by SH and KK. TH critically revised the final manuscript draft. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wang H, Zhang K, Cao H, Zhang X, Li Y, Wei Q, et al. Seizure after cranioplasty: incidence and risk factors. J Craniofac Surg. (2017) 28:e560–4. doi: 10.1097/SCS.0000000000003863
2. Ersoy TF, Ridwan S, Grote A, Coras R, Simon M. Early postoperative seizures (EPS) in patients undergoing brain tumour surgery. Sci Rep. (2020) 10(1): 13674. doi: 10.1038/s41598-020-70754-z
3. Shaw MD, Foy PM. Epilepsy after craniotomy and the place of prophylactic anticonvulsant drugs: discussion paper. J R Soc Med. (1991) 84:221–3. doi: 10.1177/014107689108400412
4. Baumgarten P, Sarlak M, Monden D, Spyrantis A, Bernatz S, Gessler F, et al. Early and late postoperative seizures in meningioma patients and prediction by a recent scoring system. Cancers (Basel). (2021) 13(3):450. doi: 10.3390/cancers13030450
5. Manaka S, Ishijima B, Mayanagi Y. Postoperative seizures: epidemiology, pathology, and prophylaxis. Neurol Med Chir (Tokyo). (2003) 43:589–600. doi: 10.2176/nmc.43.589
6. Doria JW, Forgacs PB. Incidence, implications, and management of seizures following ischemic and hemorrhagic stroke. Curr Neurol Neurosci Rep. (2019) 19(7):37. doi: 10.1007/s11910-019-0957-4
7. Galovic M, Döhler N, Erdélyi-Canavese B, Felbecker A, Siebel P, Conrad J, et al. Prediction of late seizures after ischaemic stroke with a novel prognostic model (the SeLECT score): a multivariable prediction model development and validation study. Lancet Neurol. (2018) 17(2):143–52. doi: 10.1016/S1474-4422(17)30404-0.
8. Wirsching HG, Morel C, Gmür C, Neidert MC, Baumann CR, Valavanis A, et al. Predicting outcome of epilepsy after meningioma resection. Neuro Oncol. (2016) 18(7):1002–10. doi: 10.1093/neuonc/nov303
9. Giraldi L, Vinsløv Hansen J, Wohlfahrt J, Fugleholm K, Melbye M, Munch TN. Postoperative de novo epilepsy after craniotomy: a nationwide register-based cohort study. J Neurol Neurosurg Psychiatry. (2021) 29:jnnp-2021-326968. doi: 10.1136/jnnp-2021-326968
10. Fisher RS, Acevedo C, Arzimanoglou A, Bogacz A, Cross JH, Elger CE, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. (2014) 55:475–82. doi: 10.1111/epi.12550
11. Beghi E, Carpio A, Forsgren L, Hesdorffer DC, Malmgren K, Sander JW, et al. Recommendation for a definition of acute symptomatic seizure. Epilepsia. (2010) 51:671–5. doi: 10.1111/j.1528-1167.2009.02285.x
12. Jennett B, Teather D, Bennie S. Epilepsy after head injury. Residual risk after varying fit-free intervals since injury. Lancet. (1973) 2:652–3. doi: 10.1016/s0140-6736(73)92488-4
13. Camilo O, Goldstein LB. Seizures and epilepsy after ischemic stroke. Stroke. (2004) 35:1769–75. doi: 10.1161/01.STR.0000130989.17100.96
14. Shinton RA, Gill JS, Melnick SC, Gupta AK, Beevers DG. The frequency, characteristics and prognosis of epileptic seizures at the onset of stroke. J Neurol Neurosurg Psychiatry. (1988) 51:273–6. doi: 10.1136/jnnp.51.2.273
15. Lesser RP, Lüders H, Dinner DS, Morris HH. Epileptic seizures due to thrombotic and embolic cerebrovascular disease in older patients. Epilepsia. (1985) 26:622–30. doi: 10.1111/j.1528-1157.1985.tb05702.x
16. Doria JW, Forgacs PB. Incidence, implications, and management of seizures following ischemic and hemorrhagic stroke. Curr Neurol Neurosci Rep. (2019) 19(7):37. doi: 10.1007/s11910-019-0957-4
17. Tanaka T, Ihara M. Post-stroke epilepsy. Neurochem Int. (2017) 107:219–28. doi: 10.1016/j.neuint.2017.02.002
18. Reddy DS, Bhimani A, Kuruba R, Park MJ, Sohrabji F. Prospects of modeling poststroke epileptogenesis. J Neurosci Res. (2017) 95:1000–16. doi: 10.1002/jnr.23836
19. Myint PK, Staufenberg EF, Sabanathan K. Post-stroke seizure and post-stroke epilepsy. Postgrad Med J. (2006) 82:568–72. doi: 10.1136/pgmj.2005.041426
20. Lynch MW, Rutecki PA, Sutula TP. The effects of seizures on the brain. Curr Opin Neurol. (1996) 9:97–102. doi: 10.1097/00019052-199604000-00007
21. Camilo O, Goldstein LB. Seizures and epilepsy after ischemic stroke. Stroke. (2004) 35:1769–75. doi: 10.1161/01.STR.0000130989.17100.96
22. Ferlazzo E, Gasparini S, Beghi E, Sueri C, Russo E, Leo A, et al. Epilepsy in cerebrovascular diseases: review of experimental and clinical data with meta-analysis of risk factors. Epilepsia. (2016) 57:1205–14. doi: 10.1111/epi.13448
23. Boarini DJ, Beck DW, VanGilder JC. Postoperative prophylactic anticonvulsant therapy in cerebral gliomas. Neurosurgery. (1985) 16:290–2. doi: 10.1227/00006123-198503000-00002
24. Cohen N, Strauss G, Lew R, Silver D, Recht L. Should prophylactic anticonvulsants be administered to patients with newly-diagnosed cerebral metastases? A retrospective analysis. J Clin Oncol. (1988) 6:1621–4. doi: 10.1200/JCO.1988.6.10.1621
25. Mahaley MS Jr, Dudka L. The role of anticonvulsant medications in the management of patients with anaplastic gliomas. Surg Neurol. (1981) 16:399–401. doi: 10.1016/0090-3019(81)90227-5
26. Glantz MJ, Cole BF, Forsyth PA, Recht LD, Wen PY, Chamberlain MC, et al. Practice parameter: anticonvulsant prophylaxis in patients with newly diagnosed brain tumors. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. (2000) 54:1886–93. doi: 10.1212/wnl.54.10.1886
27. Foy PM, Chadwick DW, Rajgopalan N, Johnson AL, Shaw MD. Do prophylactic anticonvulsant drugs alter the pattern of seizures after craniotomy? J Neurol Neurosurg Psychiatry. (1992) 55:753–7. doi: 10.1136/jnnp.55.9.753
28. North JB. Anticonvulsant prophylaxis in neurosurgery. Br J Neurosurg. (1989) 3:425–7. doi: 10.3109/02688698909002827
29. North JB, Penhall RK, Hanieh A, Hann CS, Challen RG, Frewin DB. Postoperative epilepsy: a double-blind trial of phenytoin after craniotomy. Lancet. (1980) 1:384–6. doi: 10.1016/s0140-6736(80)90941-1
30. Fisher RS, Cross JH, French JA, Higurashi N, Hirsch E, Jansen FE, et al. Operational classification of seizure types by the International League Against Epilepsy: position Paper of the ILAE Commission for Classification and Terminology. Epilepsia. (2017) 58(4):522–30. doi: 10.1111/epi.13670
31. Scheepers B, Clough P, Pickles C. The misdiagnosis of epilepsy: findings of a population study. Seizure. (1998) 7(5):403–6. doi: 10.1016/s1059-1311(05)80010-x
32. Chadwick D, Smith D. The misdiagnosis of epilepsy. BMJ. (2002) 324(7336):495–6. doi: 10.1136/bmj.324.7336.495
33. Perrig S, Jallon P. Is the first seizure truly epileptic? Epilepsia. (2008) 49(Suppl 1): 2–7. doi: 10.1111/j.1528-1167.2008.01442.x
Keywords: seizure, epilepsy, postoperative, craniotomy, neurosurgery, antiseizure medication (ASM)
Citation: Horiuchi S, Kanaya K and Horiuchi T (2022) The Occurrence and Relationship of Postoperative Seizure and de novo Epilepsy after Craniotomy Surgery: A Retrospective Single-Center Cohort Study. Front. Surg. 9:881874. doi: 10.3389/fsurg.2022.881874
Received: 23 February 2022; Accepted: 6 April 2022;
Published: 19 April 2022.
Edited by:
Erez Nossek, NYU Grossman School of Medicine, United StatesReviwed by:
Meng-Han Tsai, Kaohsiung Chang Gung Memorial Hospital, Taiwan*Correspondence: Kohei Kanaya kanaya@shinshu-u.ac.jp
Speciality section: This article was submitted to Neurosurgery, a section of the journal Frontiers in Surgery
Copyright Copyright © 2022 Horiuchi, Kanaya and Horiuchi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.