 Bowen Zheng1,2
Bowen Zheng1,2 Xiaobin Wang
Xiaobin Wang Jing Li
Jing Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 23 June 2022
Sec. Orthopedic Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.852589
This article is part of the Research Topic Optimization of Spine Surgery Outcomes in the Pre-, Peri-, and Postoperative Settings View all 18 articles
Background: To investigate the efficacy and safety of preoperative intravenous tranexamic acid (TXA) combined with intraoperative immersion in reducing perioperative blood loss in one-stage posterior thoracolumbar tuberculosis.
Methods: All patients were divided into four groups: Group A received an intravenous drip of TXA before surgery, group B received multiple local immersions during the operation, group C received an intravenous drip combined with multiple local immersions, and the control group (group CG) were not treated with TXA during the same period. The total blood loss (TBL), intraoperative blood loss (IBL), hidden blood loss (HBL), postoperative drainage volume, maximum hemoglobin drop value (max Hb drop), liver and kidney function, coagulation indexes, blood transfusion rate, hospital stay and incidence of complications were compared among the four groups.
Results: TBL, IBL, HBL, max Hb drop, POD1 drainage, and POD2 drainage in group A, group B, and group C were significantly lower than those in group CG. TBL, IBL, HBL and max Hb drop were group C < group A < group B < group CG. The drainage volume of group C was significantly lower than that of the other groups. There was no significant difference in blood coagulation index (PT, D-D) or liver and kidney function (ALT, Cr) among the four groups. There was no difference in postoperative hospital stay between group A and group B, but it was significantly lower in group C than in the other three groups. All patients achieved satisfactory bone graft fusion at the last follow-up.
Conclusion: Preoperative intravenous drip of TXA combined with intraoperative multiple immersion can effectively reduce perioperative blood loss while not increasing the risk of thrombosis without affecting liver and kidney function, coagulation function or tuberculosis prognosis.
Typical thoracolumbar tuberculosis (T11-L2) is characterized by intervertebral disc involvement, destruction of adjacent vertebrae and formation of paraspinal abscesses, which usually require surgical treatment. Compared with other approaches, one-stage posterior focus debridement, bone grafting and pedicle screw internal fixation have the advantages of less trauma, faster recovery, stable internal fixation and better effect of deformity correction, which is accepted by the majority of spinal surgeons (1, 2). In spite of this, tuberculosis surgery itself still has the problems of long operation time and large blood loss, which brings great challenges to the safety of operation, and most tuberculosis patients are accompanied by anemia and hypoproteinemia due to long-term chronic nutritional consumption. For patients with poor physique, perioperative blood loss is not conducive to postoperative rehabilitation. Blood transfusion not only increases medical expenses but also may cause complications such as disease transmission, hemolysis, postoperative epidural hematoma, and allergic reaction (3, 4). Therefore, it is particularly important to control perioperative blood loss in patients with spinal tuberculosis.
In addition to improving surgical skills and shortening the time of operation to reduce bleeding, the rational use of hemostatic drugs is also a good choice. Tranexamic acid (TXA) is a synthetic lysine derivative. It binds to the lysine binding site of plasmin/plasminogen and then inhibits the fibrinolysis mediated by plasmin to achieve hemostasis (5). It was first used in clinical practice in the 1960s, and most studies have proven that it can effectively reduce perioperative blood loss and the blood transfusion rate in cardiology, obstetrics, urology, orthopedics and other specialties (6–9). The route of TXA is mainly divided into intravenous and topical routes. The effectiveness and safety of intravenous, intra-articular or combined medication for reducing perioperative blood loss in knee arthroplasty has been confirmed (10, 11). There are many studies about intravenous TXA in spinal surgery, and it is basically agreed that TXA can reduce blood loss and hospital stay (12). However, there are few reports of topical TXA, and its effect is still controversial (13, 14).
To the best of our knowledge, there are no reports about the application of TXA in one-stage posterior thoracolumbar tuberculosis surgery. We achieved a good hemostatic effect by using a preoperative intravenous drip combined with multiple immersions during the operation. The purpose of this study was to evaluate the efficacy and safety of intravenous, topical and combined TXA administration in reducing perioperative blood loss in thoracolumbar tuberculosis and to provide a reference for clinical treatment.
This study was approved by the Ethics Committee of The Second Xiangya Hospital of Central South University, and all the patients signed the informed consent form before the operation. Patients who underwent one-stage posterior focus debridement, interbody fusion and pedicle screw fixation for thoracolumbar tuberculosis from July 2014 to February 2019 were included in the study. The inclusion criteria were as follows: (1) patients with clinical manifestations, laboratory examination and postoperative pathology confirmed as tuberculosis; (2) single segmental thoracolumbar tuberculosis; (3) destruction of the anterior column with or without kyphosis and nerve injury; and (4) poor effect of conservative treatment. The exclusion criteria were as follows: (1) active pulmonary tuberculosis; (2) combined anterior and posterior surgery or conservative treatment; (3) coagulation dysfunction; (4) severe hepatic and renal dysfunction; (5) cardiovascular and cerebrovascular diseases such as myocardial infarction, cerebral infarction, atrial fibrillation, and angina pectoris; and (6) use of anticoagulants and antiplatelet drugs within 7 days before the operation.
Eligible patients were divided into four groups: group A (n = 32) received 20 mg/kg TXA intravenously 15 min before the operation; group B (n = 30) was treated with 300 mL of 3 g TXA saline solution to soak the wound during the operation; group C (n = 34) received a preoperative intravenous drip combined with intraoperative multiple immersion; and the control group (group CG, n = 32) were not treated with TXA during the same period (Figure 1).
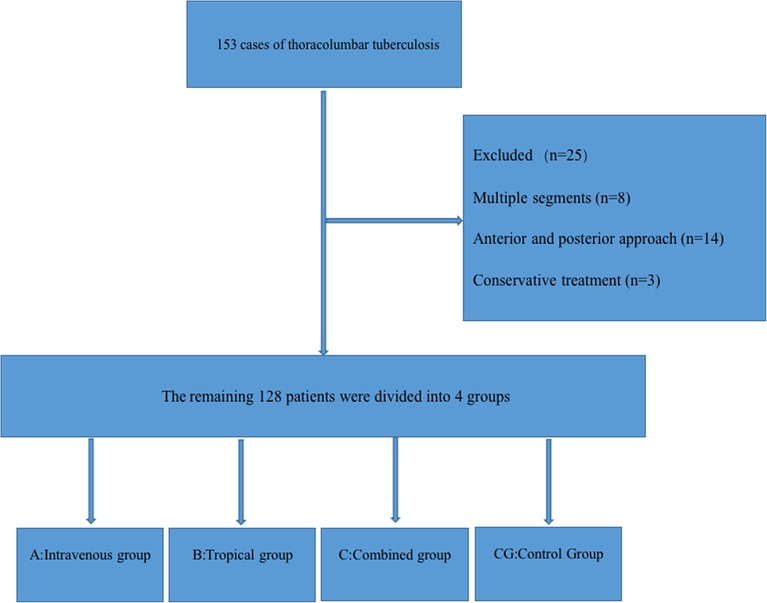
Figure 1. Experimental flow chart.
Ninety-six patients using TXA were followed up for more than 18 months, including 55 males and 41 females (mean age 45.43 years, range 27–67 years). There were 22 cases with T10-T11, 24 cases with T11-T12, 21 cases with T12-L1 and 29 cases with L1-L2. The control group included 18 males and 14 females (mean age 47.69 years, range 29–66 years). Of these, 7 were T10-T11, 8 were T11-T12, 7 were T12-L1, and 10 were L1-L2, Similarly, 32 patients in the control group were also followed up for more than 18 months.
All patients were treated with four regular antituberculosis drugs (isoniazid 5 mg/kg, rifampicin 10 mg/kg, ethambutol 15 mg/kg, pyrazinamide 25 mg/kg) for 2 to 4 weeks. Surgical treatment was performed after the erythrocyte sedimentation rate, C-reactive protein, body temperature returned to normal or significantly decreased, anemia and hypoproteinemia were corrected, and the general condition improved.
The operation was performed by the same group of doctors. A posterior midline incision was made, and the paravertebral muscles were dissected under the periosteum to expose the lamina, articular process, transverse process, costal transverse process and medial rib. Pedicle screws were inserted into the two vertebral bodies above and below the affected vertebra, and short screws were placed in the affected vertebra as appropriate. To avoid spinal cord injury caused by spinal instability during the operation, temporary rod fixation was used on the side with mild lesions. A small piece of rib (approximately 2 cm) and part of the facet joint were removed on the severe side, and then the pleura was carefully pushed outward. The intercostal nerves on one side could be sacrificed as needed to fully expose the lesions. The dead bone, tuberculous granulation tissue and pus were removed under direct vision. Then, a prebending rod was used to correct kyphosis, and the trimmed ribs or ilium was implanted into the intervertebral body. After proper compression, the screw tail cap was locked, and a posterolateral bone graft was performed. The gelatin sponge containing 0.4 g isoniazid and 0.8 g amikacin was placed into the focus. The drainage tube was placed, and the incision was sutured layer by layer.
Patients in group A were given 100 mL of 20 mg/kg TXA saline solution intravenously before the operation, and 100 mL saline was used for local irrigation after paravertebral muscle dissection, after lesion exposure and before incision closure. In group B, 100 mL saline was intravenously dripped 15 min before the operation. Meanwhile, 300 mL of 3 g TXA saline solution was divided into three equal parts, local immersion was performed after paravertebral muscle dissection, after lesion exposure and before incision closure for 2 min, 2 min, 5 min, and then sucked away; group C received intravenous drip of 100 mL of 20 mg/kg TXA saline 15 min before operation, and 100 mL of 1 g TXA saline solution was used to soak the wound after paravertebral muscle dissection, after lesion exposure and before incision closure, respectively.
After the operation, patients were given air pressure pump treatment of both lower extremities, and patients were encouraged to perform isometric contractile exercise of lower limb muscles to prevent deep venous thrombosis (DVT)). The drainage tube was removed when the drainage volume was less than 30 mL/d. Antibiotics were used for 5–7 days, and the treatment of four antituberculosis drugs was continued. Pyrazinamide was stopped after 3 months, and the other three antituberculosis drugs lasted for 12–18 months. The patient can wear a brace and leave the bed for appropriate activities after 2 weeks, but bed rest should still be the mainstay before bone graft fusion. All patients were followed up at 1, 3, 6, 12, and 18 months after surgery and then reviewed once a year.
The operation time, postoperative hospital stay, hemoglobin (Hb), hematocrit (HCT), D-dimer (D-D), prothrombin time (PT), glutamic pyruvic transaminase (ALT) and creatinine (Cr) were recorded before and after the operation.
The total blood loss (TBL) was calculated according to the estimated blood volume (EBV) formula of Nadler et al. (15). TBL = 2*EBV (Hctpre-Hctpost)/(Hctpre + Hctpost), Hctpre was Hct on the day before the operation, and Hctpost was Hct on the third day after the operation. Visible blood loss (VBL) = intraoperative blood loss (IBL) + postoperative drainage, hidden blood loss (HBL) = TBL-VBL. If the patient received a blood transfusion during the period, HBL = TBL+ transfusion volume-VBL. The maximum hemoglobin drop value (Max Hb drop) = Hbpre-Hblowest (Hbpre is the level of Hb one day before operation; Hblowest is the lowest value within 3 days after operation).
Routine ultrasound examination of the lower extremities was performed before discharge or at any time when the patient had lower limb pain and swelling to determine whether there was deep venous thrombosis (DVT). Perioperative complications, such as incision infection, epidural hematoma, epilepsy, DVT, pulmonary embolism, visual impairment, myocardial ischemia and ischemic encephalopathy and final bone graft fusion, were recorded.
Spss23.0 was used to analyze the data. Continuous variables were expressed as the mean ± SD. The data of four groups were compared by one-way ANOVA. When there was a significant difference among the four groups, the Bonferroni test was used for pairwise comparisons. The chi-square test was used to compare categorical variables. When P < 0.05, the difference was considered statistically significant.
All patients were followed up for at least 18 months, and satisfactory implant fusion was achieved at the last follow-up. There were no significant differences between the four groups in terms of age, sex, BMI, lesion segment, time to surgery, or other baseline data (Table 1).
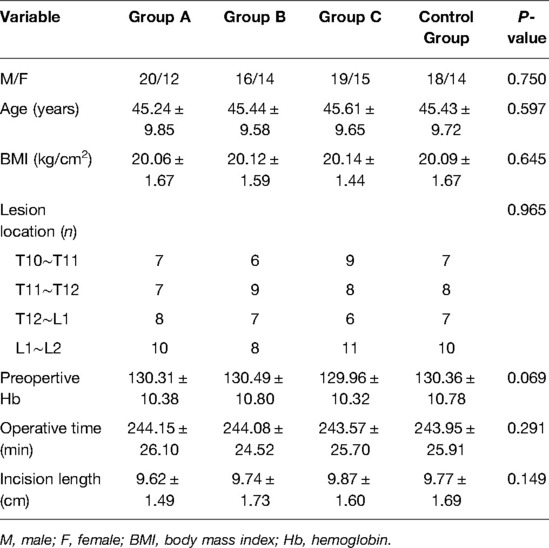
Table 1. Baseline parameters of patients in the 4 groups.
TBL, IBL, HBL, max Hb drop, POD1 drainage, and POD2 drainage in group A, group B, and group C were significantly lower than those in group CG. TBL, IBL and HBL in group C were significantly lower than those in groups A and B, while group A was significantly lower than group B. There was no significant difference in preoperative Hb between the four groups, and the max Hb drop after surgery was (group C < group A < group B < group CG). On the first postoperative day, the drainage in group C was significantly lower than that in group A, group B and group CG, while group A was lower than group B and group CG, and group CG had the most drainage; on the second day, there was no significant difference between group A and group B, while group C was still lower than the other three groups. On the third day, there was no significant difference between the four groups. The transfusion rates of the four groups were 18.75%, 16.67%, 5.88% and 15.63%, respectively, but were not statistically significant. There was no difference in the postoperative hospitalization time between groups A and B, but the hospitalization time in group CG was significantly higher than that in the other groups, and the hospitalization time in group C was the shortest (Table 2).
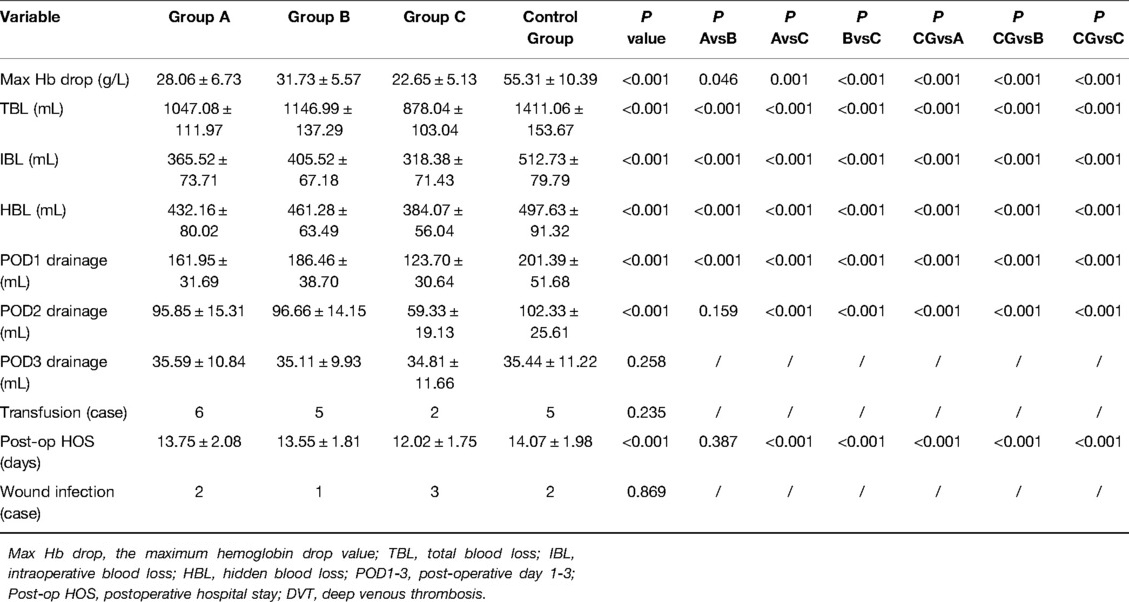
Table 2. Postoperative outcome among the 4 groups.
There was no significant difference in the coagulation indexes (PT, D-D) before and 3 days after surgery, and there was no significant difference in the liver and kidney function indexes (ALT, Cr) before and 3 days after surgery among the four groups (Table 3).
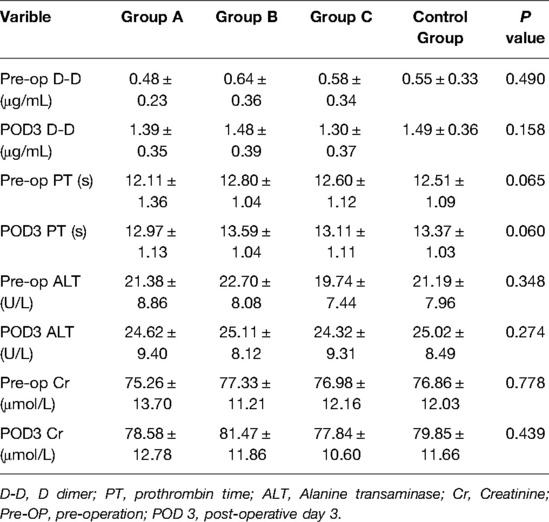
Table 3. Preoperative and postoperative blood biochemical indexes among the 4 groups.
No serious adverse events, such as pulmonary embolism, epidural hematoma, epilepsy, myocardial ischemia, visual impairment or ischemic encephalopathy, occurred in any patient. Only one patient in each of the B and CG groups developed slight swelling of the lower extremities at 5 and 7 days postoperatively. B-ultrasound showed intermuscular venous thrombosis, and the symptoms improved with active treatment. One patient in group A had sinus tract formation, which was cured with local debridement and intensive dressing changes. In addition, two case in group A, one case in group B, three cases in group C, and two cases in group CG had superficial infection of the incision, which was cured after anti-infection, drug change and other symptomatic treatment.
The local blood supply of the spine is abundant, and exposure of the operative area and osteotomy will lead to hyperfibrinolysis and increased blood loss (16). Compared with combined anterior and posterior surgery, one-stage posterior tuberculosis focus debridement and bone graft internal fixation shorten the operation time and reduce the amount of trauma and blood loss to a certain extent, but its exposure range and visual field are limited, which is not conducive to hemostasis during the operation. The exposed bone surface is not suitable for standard hemostasis in soft tissue surgery, and the deeper wound cannot be effectively oppressed, resulting in large postoperative drainage (17). Tuberculosis patients are prone to malnutrition, anemia and hypoproteinemia due to long-term poor appetite and lack of sleep, so ensuring a good systemic condition is an important part of anti-tuberculosis treatment (18). Perioperative blood loss will lead to worse immunity in tuberculosis patients and prolong the time of hospitalization and rehabilitation. The successful application of TXA in other orthopedic surgeries provides us with a good reference. We used different methods of TXA for perioperative hemostasis of spinal tuberculosis and achieved satisfactory results in long-term follow-up.
TXA can effectively reduce bleeding by inhibiting fibrinolysis and stabilizing blood clots. A number of studies have shown that intravenous administration of the antifibrinolytic drug TXA during spinal surgery can significantly reduce blood loss, blood transfusion volume and blood transfusion rate; however, there is no consensus on the optimal timing and dosage of intravenous administration (19, 20). In view of the fact that the half-life of single-dose intravenous administration is 120 min, it is generally reported that dual-dose or preoperative load dose supplemented by maintenance dose. Raksakietisak et al. (21) used 15 mg/kg TXA intravenously at the beginning of 39 cases of complex spinal surgery and 3 h later, which resulted in lower blood loss and transfusion rates than the placebo group. Elwatidy et al. (22) used 2 g TXA intravenously before spinal surgery in 64 cases, and supplemented with a 100 mg/h maintenance dose within 5 h after the operation, the blood loss was 49% less than that of the placebo group. Raman et al. (16) considered that the hemostatic effect of a high dose (load 30 mg/kg, maintenance dose 1–10 mg/kg/h) was better than that of a low dose (load dose 10 mg/kg, maintenance dose 1–2 mg/kg/h) in adult spinal deformities. However, the incidence of postoperative atrial fibrillation and myocardial infarction was higher in the high-dose group.
A high load dose, additional maintenance dose or repeated use of TXA can significantly inhibit fibrinolytic activity, and the imbalance of the fibrinolytic system is closely related to thrombosis (23). Systemic administration of TXA can penetrate the blood–brain barrier and then spread throughout the central nervous system (5). Although complications of intravenous TXA are rare, they do exist, especially in patients with hypercoagulability, severe renal failure and ischemic heart disease (24). High-dose intravenous administration of TXA in patients undergoing cardiac surgery has been reported to lead to nonischemic seizures (25). On the other hand, single-dose application also achieved good results. Sun et al. (26) intravenously dripped 15 mg/kg TXA 30 min before lumbar fusion surgery, and IBL and drainage volume 24 h after surgery were significantly reduced compared with the placebo group. Wang (27) et al. used 15 mg/kg TXA intravenously 15 min before lumbar degeneration surgery, and the postoperative blood loss was 13% less than that of the control group. To reduce the potential complications caused by systemic medication and considering the time-consuming operation of tuberculosis and the ceiling effect of drugs, we chose to intravenously drip 20 mg/kg TXA 15 min before surgery, combined with multiple immersions during the operation, in an attempt to enhance its hemostatic effect. The results are satisfactory.
The application of topical TXA in joint surgery is relatively mature. A multicenter randomized controlled study showed that topical 1–3 g TXA was effective in knee arthroplasty (28). A meta-analysis of topical application of TXA in spine surgery showed that methods such as local soaking or indwelling gelatin sponge with TXA before incision closure can also reduce blood loss and drainage while not increasing the risk of complications (29). Xu et al. (30) found that local immersion with 1 g TXA before closing the incision in spinal fusion surgery significantly reduced postoperative drainage compared with gelatin sponge and collagen hemostatic sponge. Ren et al. (17) used 100 mL of 1 g TXA saline to soak the wound for 5 min before incision closure in 50 patients undergoing lumbar fusion, and the postoperative blood loss was 44.29% of the control group, while shortening the hospital stay. Compared with intravenous medication, this method is convenient to manage and can provide a higher concentration in the bleeding area, inhibiting the fibrinolytic activity of the local tissue and preventing the fibrin clot from dissolving, increasing the volume and strength on the wound surface, thereby enhancing microvascular coagulation while reducing system exposure (31, 32). In theory, it may be better to prolong the soaking time and increase the absorption of drugs by local tissues, but that will prolong the time of operation and anesthesia, and spine surgery cannot prolong drug absorption time by clamping the drainage tube as it does after joint replacement. Therefore, unlike the previously reported single-dose local administration before incision closure, we used TXA solution to soak wounds after paravertebral muscle dissection, after lesion exposure and before incision closure. The results showed that although the hemostatic effect was slightly worse than that of intravenous administration alone, the combination was better than that of single administration.
In this study, the combined group was superior to the single-medication group in reducing TBL, IBL, and HBL, which indicated that intravenous drip before the operation, soaking and flushing during the operation simultaneously not only reduced the total blood loss but also made the surgical field cleaner and increased the safety of the operation. A single intravenous administration could maintain the effective plasma concentration for approximately 16 h (33), and resoaking the wound at the end of the operation further prolonged the action time of the drug, so the postoperative drainage was significantly less than that of the other groups. The blood transfusion rate in the combined group (5.88%) was lower than that in the other two groups (16.67%, 18.75%), but there was no statistical significance in the blood transfusion rate among the three groups. The result may be due to the small sample size on the one hand and the strict grasp of the indication for blood transfusion on the other hand. Less blood loss in the combined group means that the general condition recovers quickly, and early functional exercise makes the length of hospital stay significantly lower than that in the other two groups. TXA has a low price, which is much lower than the cost of blood transfusion and prolonged hospitalization. Therefore, preoperative intravenous drip combined with intraoperative multiple local immersion for hemostasis not only contributes to the recovery of spinal tuberculosis but also reduces their economic pressure.
Due to the antifibrinolytic effect of TXA, most users are concerned about whether it increases the risk of thrombosis, leading to DVT, ischemic cerebral infarction, myocardial infarction and pulmonary embolism. In this study, there was no significant difference in the indexes of coagulation function among the four groups, and there were no serious complications of thrombosis in the perioperative period, which again proved that TXA could inhibit fibrinolysis within the effective drug action window but had no significant effect on coagulation function and did not increase the incidence of thrombosis (34, 35). The reason may be attributed to the fact that the inhibitory effect of TXA on fibrinolysis is mainly located in the surgical wound rather than in the circulatory system, and it has no effect on the vein wall (36). Among them, 1 case of postoperative intermuscular venous thrombosis was considered to be related to his refusal to use a lower limb air pressure pump after the operation. Therefore, for the sake of safety, we believe that postoperative intervention measures such as active use of a lower limb air pressure pump and encouraging patients to carry out isometric contraction of lower limb muscles are of great benefit to the prevention of thrombosis. In addition, the number of incision infections in the four groups was similar, and satisfactory bone graft fusion was achieved in the four groups after long-term follow-up, indicating that the drug would not affect the short-term and long-term prognosis of patients with spinal tuberculosis.
There are some limitations in this study. First, this is a single-center retrospective cohort study. Due to the low incidence of perioperative complications, the small sample size may not be able to identify all complications, e.g. the conclusion that “while not increasing the risk of thrombosis without affecting liver and kidney function, coagulation function or tuberculosis prognosis” may be inaccurate Secondly, the medication method of this study is empirical medication, and the optimal dosage and administration time need to be further explored. In the future, further large-scale prospective experiments are needed to further explore and verify this conclusion.
Preoperative intravenous drip of TXA combined with intraoperative multiple immersion can effectively reduce perioperative blood loss and shorten hospital stay while not increasing the risk of thrombosis without affecting liver and kidney function, coagulation function or tuberculosis prognosis.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by The Second Xiangya Hospital of Central South University, Hunan, P.R. China. The patients/participants provided their written informed consent to participate in this study.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
All authors participated in data acquisition. BWZ, JL, BYZ and JYW contributed to the conception and design of the study. BWZ, GHL and XBW did the data analysis and interpretation. HQN, XBW, BYZ, JL and JYW contributed to drafting and revision of the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the National Natural Science Foundation of China (81871821 to JL) and China Scholarship Council (202106370071 to BWZ).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Tang Y, Wu WJ, Yang S, Wang DG, Zhang Q, Liu X, et al. Surgical treatment of thoracolumbar spinal tuberculosis-a multicentre, retrospective, case-control study. J Orthop Surg Res. (2019) 14(1):233. doi: 10.1186/s13018-019-1252-4
2. Zeng Y, Cheng P, Tan J, Li Z, Chen Y, Li LT, et al. Comparison of three surgical approaches for thoracolumbar junction (T12-L1) tuberculosis: a multicentre, retrospective study. BMC Musculoskelet Disord. (2019) 20(1):524. doi: 10.1186/s12891-019-2891-7
3. Vamvakas EC, Blajchman MA. Transfusion-related mortality: the ongoing risks of allogeneic blood transfusion and the available strategies for their prevention. Blood. (2009) 113(15):3406–17. doi: 10.1182/blood-2008-10-167643
4. Yerneni K, Burke JF, Tuchman A, Li XJ, Metz LN, Lehman RA Jr, et al. Topical tranexamic acid in spinal surgery: a systematic review and meta-analysis. J Clin Neurosci. (2019) 61:114–9. doi: 10.1016/j.jocn.2018.10.121
5. McCormack PL. Tranexamic acid: a review of its use in the treatment of hyperfibrinolysis. Drugs. (2012) 72(5):585–617. doi: 10.2165/11209070-000000000-00000
6. Myles PS, Smith JA, Painter T. Tranexamic acid in patients undergoing coronary-artery surgery. N Engl J Med. (2017) 376(19):1893. doi: 10.1056/NEJMc1703374
7. Topsoee MF, Settnes A, Ottesen B, Bergholt T. A systematic review and meta-analysis of the effect of prophylactic tranexamic acid treatment in major benign uterine surgery. Int J Gynaecol Obstet. (2017) 136(2):120–7. doi: 10.1002/ijgo.12047
8. Zaid HB, Yang DY, Tollefson MK, Frank I, Winters JL, Thapa P, et al. Efficacy and safety of intraoperative tranexamic acid infusion for reducing blood transfusion during open radical cystectomy. Urology. (2016) 92:57–62. doi: 10.1016/j.urology.2016.02.044
9. Franchini M, Mengoli C, Marietta M, Marano G, Vaglio S, Pupella S, et al. Safety of intravenous tranexamic acid in patients undergoing majororthopaedic surgery: a meta-analysis of randomised controlled trials. Blood Transfus. (2018) 16(1):36–43. doi: 10.2450//2017.0219-17
10. Sun Q, Li J, Chen J, Zheng C, Liu C, Jia Y. Comparison of intravenous, topical or combined routes of tranexamic acid administration in patients undergoing total knee and hip arthroplasty: a meta-analysis of randomised controlled trials. BMJ Open. (2019) 9(1):e024350. doi: 10.1136/bmjopen-2018-024350
11. Abdel MP, Chalmers BP, Taunton MJ, Pagnano MW, Trousdale RT, Sierra RJ, et al. Intravenous versus topical tranexamic acid in total knee arthroplasty: both effective in a randomized clinical trial of 640 patients. J Bone Joint Surg Am. (2018) 100(12):1023–9. doi: 10.2106/JBJS.17.00908
12. Cheriyan T, 2nd Maier SP, Bianco K, Slobodyanyuk K, Rattenni RN, Lafage V, et al. Efficacy of tranexamic acid on surgical bleeding in spine surgery: a meta-analysis. Spine J. (2015) 15(4):752–61. doi: 10.1016/j.spinee.2015.01.013
13. Wang X, Yang R, Sun H, Zhang Y. Different effects of intravenous, topical, and combined application of tranexamic acid on patients with thoracolumbar fracture. World Neurosurg. (2019) 127:e1185–9. doi: 10.1016/j.wneu.2019.04.095
14. Xiong Z, Liu J, Yi P, Wang H, Tan M. Comparison of intravenous versus topical tranexamic acid in nondeformity spine surgery: a meta-analysis. Biomed Res Int. (2020) 2020:7403034. doi: 10.1155/2020/7403034
15. Nadler SB, Hidalgo JH, Bloch T. Prediction of blood volume in normal human adults. Surgery. (1962) 51(2):224–32. PMID: 21936146
16. Raman T, Varlotta C, Vasquez-Montes D, Buckland AJ, Errico TJ. The use of tranexamic acid in adult spinal deformity: is there an optimal dosing strategy? Spine J. (2019) 19(10):1690–7. doi: 10.1016/j.spinee.2019.06.012
17. Ren Z, Li S, Sheng L, Zhuang Q, Li Z, Xu D, et al. Efficacy and safety of topical use of tranexamic acid in reducing blood loss during primary lumbar spinal surgery: a retrospective case control study. Spine (Phila Pa 1976). (2017) 42(23):1779–84. doi: 10.1097/BRS.0000000000002231
18. Yin XH, Liu SH, Li JS, Chen Y, Hu XK, Zeng KF, et al. The role of costotransverse radical debridement, fusion and postural drainage in the surgical treatment of multisegmental thoracic spinal tuberculosis: a minimum 5-year follow-up. Eur Spine J. (2016) 25(4):1047–55. doi: 10.1007/s00586-015-4283-5
19. Bai J, Zhang P, Liang Y, Wang J, Wang Y. Efficacy and safety of tranexamic acid usage in patients undergoing posterior lumbar fusion: a meta-analysis. BMC Musculoskelet Disord. (2019) 20(1):390. doi: 10.1186/s12891-019-2762-2
20. Hui S, Xu D, Ren Z, Chen X, Sheng L, Zhuang Q, et al. Can tranexamic acid conserve blood and save operative time in spinal surgeries? A meta-analysis. Spine J. (2018) 18(8):1325–37. doi: 10.1016/j.spinee.2017.11.017
21. Raksakietisak M, Sathitkarnmanee B, Srisaen P, Duangrat T, Chinachoti T, Rushatamukayanunt P, et al. Two doses of tranexamic acid reduce blood transfusion in complex spine surgery: a prospective randomized study. Spine (Phila Pa 1976). (2015) 40(24):E1257–63. doi: 10.1097/BRS.0000000000001063
22. Elwatidy S, Jamjoom Z, Elgamal E, Zakaria A, Turkistani A, El-Dawlatly A. Efficacy and safety of prophylactic large dose of tranexamic acid in spine surgery: a prospective, randomized, double-blind, placebo-controlled study. Spine (Phila Pa 1976). (2008) 33(24):2577–80. doi: 10.1097/BRS.0b013e318188b9c5
23. Bagoly Z, Ariëns RAS, Rijken DC, Pieters M, Wolberg AS. Clot structure and fibrinolysis in thrombosis and hemostasis. Biomed Res Int. (2017) 2017:4645137. doi: 10.1155/2017/4645137
24. Wang S, Gao X, An Y. Topical versus intravenous tranexamic acid in total knee arthroplasty: a meta-analysis of randomized controlled trials. Int Orthop. (2017) 41(4):739–48. doi: 10.1007/s00264-016-3296-y
25. Murkin JM, Falter F, Granton J, Young B, Burt C, Chu M. High-dose tranexamic Acid is associated with nonischemic clinical seizures in cardiac surgical patients. Anesth Analg. (2010) 110(2):350–3. doi: 10.1213/ANE.0b013e3181c92b23
26. Sun H, Deng L, Deng J, Wang J, Zhang H, Chen K, et al. The efficacy and safety of prophylactic intravenous tranexamic acid on perioperative blood loss in patients treated with posterior lumbar interbody fusion. World Neurosurg. (2019) 125:e198–204. doi: 10.1016/j.wneu.2019.01.040
27. Wang Q, Liu J, Fan R, Chen Y, Yu H, Bi Y, et al. Tranexamic acid reduces postoperative blood loss of degenerative lumbar instability with stenosis in posterior approach lumbar surgery: a randomized controlled trial. Eur Spine J. (2013) 22(9):2035–8. doi: 10.1007/s00586-013-2836-z
28. Aguilera X, Martínez-Zapata MJ, Hinarejos P, Jordán M, Leal J, González JC, et al. Topical and intravenous tranexamic acid reduce blood loss compared to routine hemostasis in total knee arthroplasty: a multicenter, randomized, controlled trial. Arch Orthop Trauma Surg. (2015) 135(7):1017–25. doi: 10.1007/s00402-015-2232-8
29. Luo W, Sun RX, Jiang H, Ma XL. The efficacy and safety of topical administration of tranexamic acid in spine surgery: a meta-analysis. J Orthop Surg Res. (2018) 13(1):96. doi: 10.1186/s13018-018-0815-0
30. Xu D, Zhuang Q, Li Z, Ren Z, Chen X, Li S. A randomized controlled trial on the effects of collagen sponge and topical tranexamic acid in posterior spinal fusion surgeries. J Orthop Surg Res. (2017) 12(1):166. doi: 10.1186/s13018-017-0672-2
31. Katsumata S, Nagashima M, Kato K, Tachihara A, Wauke K, Saito S, et al. Changes in coagulation-fibrinolysis marker and neutrophil elastase following the use of tourniquet during total knee arthroplasty and the influence of neutrophil elastase on thromboembolism. Acta Anaesthesiol Scand. (2005) 49(4):510–6. doi: 10.1111/j.1399-6576.2005.00621.x
32. Damji KF, Noël LP, Peterson RG, Ma PE, Clarke WN, Gilberg S, et al. Topical versus intravenous administration of tranexamic acid: a comparison of intraocular and serum concentrations in the rabbit. Can J Ophthalmol. (1998) 33(6):308–13. PMID: 9818127
33. Tsutsumimoto T, Shimogata M, Ohta H, Yui M, Yoda I, Misawa H. Tranexamic acid reduces perioperative blood loss in cervical laminoplasty: a prospective randomized study. Spine (Phila Pa 1976). (2011) 36(23):1913–8. doi: 10.1097/BRS.0b013e3181fb3a42
34. Wang W, Duan K, Ma M, Jiang Y, Liu T, Liu J, et al. Tranexamic acid decreases visible and hidden blood loss without affecting prethrombotic state molecular markers in transforaminal thoracic interbody fusion for treatment of thoracolumbar fracture-dislocation. Spine (Phila Pa 1976). (2018) 43(13):E734–9. doi: 10.1097/BRS.0000000000002491
35. Ou Y, Wei J, Li R, Liang B, Qiu D, Wei M, et al. Clinical research of combined intravenous administration and topical application of tranexamic acid to a surgical wound during posterior lumbar fusion. Surg Innov. (2018) 25(2):128–35. doi: 10.1177/1553350617751449
36. Mu X, Wei J, Wang C, Ou Y, Yin D, Liang B, et al. Intravenous administration of tranexamic acid significantly reduces visible and hidden blood loss compared with its topical administration for double-segment posterior lumbar interbody fusion: a single-center, placebo-controlled, randomized trial. World Neurosurg. (2019) 122:e821–7. doi: 10.1016/j.wneu.2018.10.154
Keywords: thoracolumbar tuberculosis, tranexamic acid, blood loss, local immersion, drainage
Citation: Zheng B, Zheng B, Niu H, Wang X, Lv G, Li J and Wang J (2022) Effect Analysis of Preoperative Intravenous Tranexamic Acid Combined With Intraoperative Immersion in Reducing Perioperative Blood Loss of One Stage Posterior Thoracolumbar Tuberculosis. Front. Surg. 9:852589. doi: 10.3389/fsurg.2022.852589
Received: 11 January 2022; Accepted: 6 June 2022;
Published: 23 June 2022.
Edited by:
Jeremy Steinberger, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Junlin Zhou, Beijing Chaoyang Hospital, Capital Medical University, ChinaCopyright © 2022 Zheng, Zheng, Niu, Wang, Lv, Li and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jing Li amluZ2xpMTk2OUBjc3UuZWR1LmNu Jingyu Wang d2FuZ2p5c3BpbmVAY3N1LmVkdS5jbg==
†These authors have contributed equally to this work
Specialty section: This article was submitted to Orthopedic Surgery, a section of the journal Frontiers in Surgery
Abbreviations: TBL, Total blood loss; HBL, Hidden blood loss; VBL, Visible blood loss; IBL, Intraoperative blood loss; TXA, Tranexamic acid; Hct, Hematocrit; Hb, Hemoglobin.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.