 Knut Jørgen Labori
Knut Jørgen Labori- 1Department of Hepato-Pancreato-Biliary Surgery, Oslo University Hospital, Rikshospitalet, Oslo, Norway
- 2Institute of Clinical Medicine, University of Oslo, Oslo, Norway
Neoadjuvant therapy improves overall survival compared with a surgery-first approach in patients with borderline resectable pancreatic cancer (BRPC). Evidence of higher quality is required to determine whether neoadjuvant therapy has potential benefits and improves survival for patients with resectable pancreatic cancer (RPC). Most randomized controlled trials (RCTs) have explored short-course neoadjuvant chemotherapy (SNT), but total neoadjuvant chemotherapy (TNT) is now the experimental arm of ongoing RCTs. This article reviews the current status of SNT and TNT in RPC and BRPC, and provides perspectives of future challenges and research directions in this field.
Introduction
Pancreatic ductal adenocarcinoma is a lethal malignancy, and surgical resection remains the only potential for cure. Data from population-based registries show resection rates of 13–21.7% (1). Resectable pancreatic cancer (RPC) is defined according to the National Comprehensive Cancer Network classification (NCCN) as the absence of distant organ or lymph node metastases; no tumor contact with the superior mesenteric/portal vein, or ≤ 180° contact with either vein without vein contour irregularity, and no tumor contact with the coeliac axis, common hepatic, and superior mesenteric artery (2). Borderline resectable pancreatic cancer (BRPC) is determined by limited involvement of the superior mesenteric/portal vein or arterial axis (2). Currently, a surgery-first approach is the universally accepted standard practice for RPC, followed by 6 months of adjuvant chemotherapy, preferably with mFOLFIRINOX (modified 5-fluorouracil with leucovorin, irinotecan, and oxaliplatin) in fit patients (3, 4). For BRPC contemporary approaches have focused on neoadjuvant chemotherapy with the goal of improving overall survival (2, 5).
Neoadjuvant chemotherapy is sometimes used for RPC, especially in patients with high-risk features, i.e., radiographic findings are suspicious but not diagnostic for metastatic disease, potentially reversible performance status or comorbidity profile that is not currently appropriate for major surgery, or a carbohydrate antigen 19-9 (CA19-9) level suggestive of metastatic disease (2). For patients with RPC, who are fit to undergo upfront surgery, neoadjuvant therapy is considered best to be managed within the boundaries of a clinical trial (2). A major criticism of published adjuvant RCTs in RPC is that these trials only included patients who recovered from a successful operation, and in some trials restaging with a CT and CA19-9 was performed to exclude patients with early recurrence (4, 6–11). Most retrospective studies on neoadjuvant therapy in RPC only include patients undergoing a successful operation and also suffer from selection bias (10). Currently, several RCTs are evaluating the effect of neoadjuvant chemotherapy in RPC and BRPC (Table 1). The data from these trials will expand the knowledge on treatment sequencing and survival in RPC and BRPC, and better delineate the completion rates of all parts of multimodal treatment.
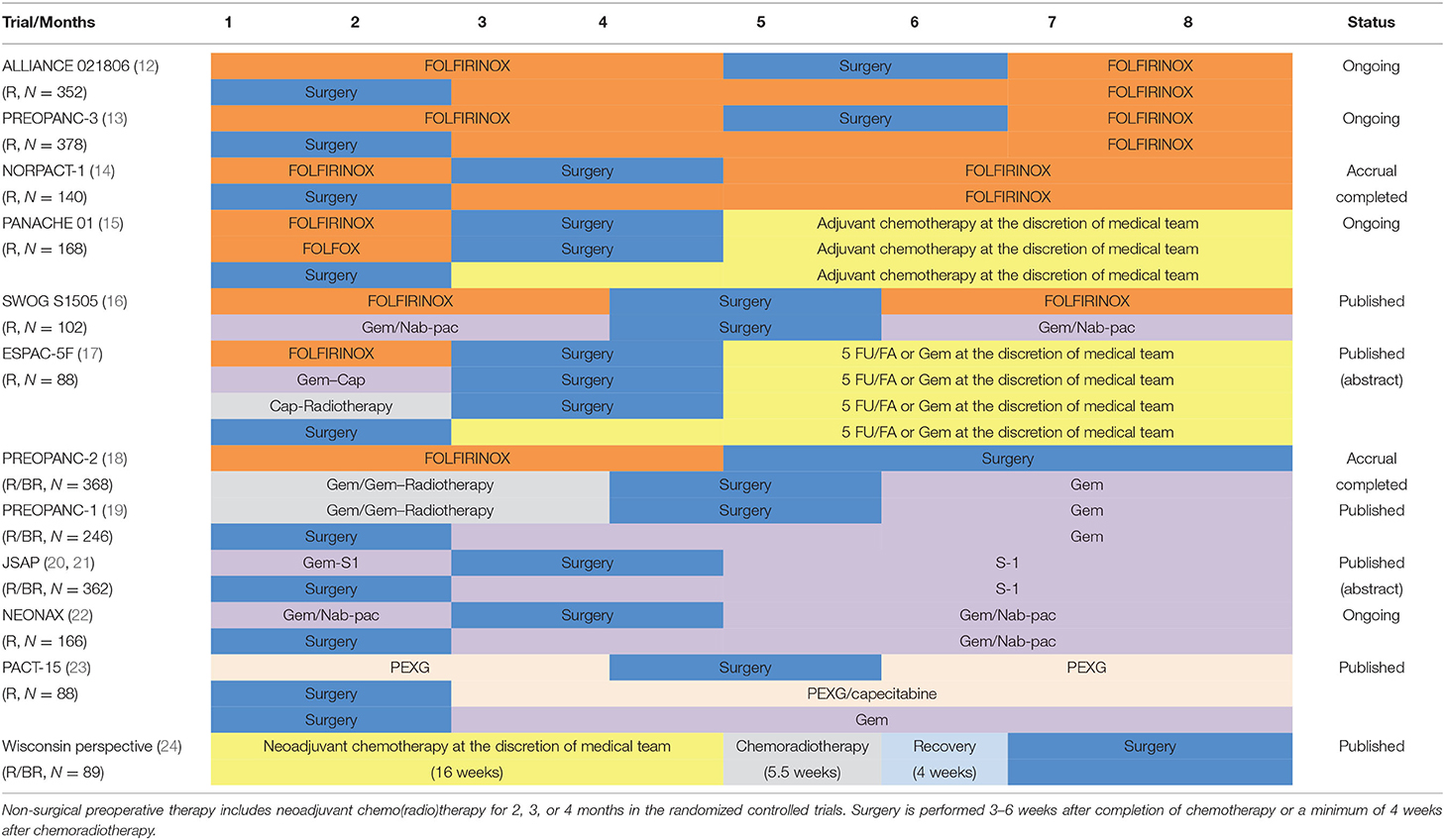
Table 1. Randomized controlled trials of neoadjuvant therapy in resectable and borderline resectable pancreatic cancer.
Outcomes of Neoadjuvant Treatment in Comparative Studies
A recent meta-analysis by van Dam et al., of randomized clinical trials (RCTs), found that neoadjuvant therapy improves survival compared with upfront surgery in patients with BRPC (10). However, more evidence is required on whether neoadjuvant therapy improves survival for patients with RPC (10). Long-term results of the PREOPANC-1 trial, the largest RCT to date comparing neoadjuvant chemoradiotherapy with upfront surgery in RPC and BRPC, found a difference in median survival of only 1.4 months (15.7 vs. 14.3 months, p = 0.025) (25). However, the 5-year overall survival rate was 20.5% with neoadjuvant chemoradiotherapy and 6.5% with upfront surgery. The survival benefit of neoadjuvant chemoradiotherapy was consistent across the pre-specified subgroups, including RPC and BRPC. Although only currently available as abstract, Unno et al. found a median overall survival of 36.7 months for neoadjuvant gemcitabine and S1, and 26.6 months for upfront surgery in 362 patients with RPC and BRPC (p = 0.015) (20). Both groups received adjuvant S1. All trials in the meta-analysis by van Dam et al. included a neoadjuvant gemcitabine-based chemotherapy arm, and none of these two trials used adjuvant FOLFIRINOX (10). Of note, most ongoing RCTs compare neoadjuvant FOLFIRINOX with upfront surgery and schedule patients in both arms to adjuvant FOLFIRINOX (Table 1).
Optimal Duration of Neoadjuvant Chemotherapy
Ongoing or completed RCTs in RPC and BRPC include different perioperative chemotherapy regimens, and the duration of neoadjuvant and adjuvant chemotherapy differs between studies (Table 1). Most trials perform surgical resection between short-course neoadjuvant therapy (SNT) and adjuvant therapy. The optimal duration of perioperative systemic chemotherapy is defined as 6 months based on the results from RCTs of adjuvant chemotherapy in patients undergoing upfront surgery (4, 6–9). Accordingly, 10 of 11 RCTs administer neoadjuvant chemotherapy for 2–4 months, followed by adjuvant chemotherapy for 2–4 months following a successful surgical resection. Only PREOPANC-2 does not include adjuvant chemotherapy as part of the treatment sequence in the experimental arm, but complete multimodal treatment after eight cycles (4 months) of FOLFIRINOX and surgical resection (18).
The added value of radiotherapy following neoadjuvant chemotherapy in patients with RPC and BRPC is unclear. Radiotherapy, in the treatment of RPC and BRPC, is more common in the United States (2). Only PREOPANC-1/2 and ESPAC-5F have included radiotherapy in the neoadjuvant arm (17–19). In recent meta-analysis, a radiotherapy following neoadjuvant FOLFIRINOX was associated with an improved R0 resection rate as compared with neoadjuvant FOLFIRINOX alone, but a difference in survival could not be demonstrated (26).
For BRPC, neoadjuvant therapy has been established as routine practice in many centers and countries (2, 27). In a recent systematic review and patient-level meta-analysis of 24 studies comprising 313 patients with BRPC treated with neoadjuvant FOLFIRINOX, the median number of neoadjuvant FOLFIRINOX cycles ranged from 4 to 9 (2–5 months) (28). In a large international, multicenter cohort study of 536 patients, including 243 (48.4%) with RPC and 208 (41.4%) with BRPC, underwent pancreatectomy after the neoadjuvant FOLFIRINOX. The median number of neoadjuvant FOLFIRINOX cycles was 6 (3 months) (29). To date, no data exist to define whether a higher number of neoadjuvant chemotherapy cycles is associated with improved survival.
Some centers suggest a role for total neoadjuvant therapy (TNT), also termed the surgery-last approach for RPC and BRPC (24, 30–32). Kim et al. recently published the Wisconsin experience with TNT in patients with operable pancreatic cancer and included all patients who initiated neoadjuvant therapy with surgical/curative intent (24). The study reviewed 541 patients including 226 (42%) with RPC and 315 (58%) with BRPC. The TNT was administered to 89 (16%) of the patients and 452 (84%) received SNT. Both groups underwent neoadjuvant chemotherapy for a minimum of 2 months in SNT and 4 months in TNT, followed by chemoradiotherapy for 5.5 weeks (Table 1). Patients who were treated with TNT received a median duration of 5.5 months of non-surgical therapy compared with 4 months for patients treated with SNT (p < 0.01). The study suggests that patients who can tolerate SNT would likely benefit from TNT. The rate of completion of all intended neoadjuvant therapy and surgery was not statistically different between the two groups (SNT: 71% and TNT: 72%, p = 0.90). Thus, TNT did not seem to risk the loss of a window of operability, which is an important finding when TNT is extended to patients with RPC. Thus, most RCTs in RPC administer SNT for 2–3 months; PREOPANC-2/3 and ALLIANCE-021806 have prolonged the duration of neoadjuvant therapy and administered neoadjuvant mFOLFIRINOX for 4 months in the experimental arm (12, 18, 19). In PREOPANC-3 and ALLIANCE-021806, additional adjuvant chemotherapy is administered for 2 months in the experimental arm. When giving TNT, restaging with CT is performed after the first 4 cycles (2 months) of mFOLFIRINOX, and patients with treatment response or stable disease according to Response Evaluation Criteria in Solid Tumors (RECIST) criteria are scheduled for an additional four cycles of neoadjuvant mFOLFIRINOX (18). According to the PREOPANC-2 protocol, discontinuation of neoadjuvant chemotherapy after 2 months was recommended if CT showed metastatic disease or local tumor progression determined by RECIST criteria (i.e., at least a 20% increase in the longest diameter of the tumor). Accordingly, patients with local tumor progression proceeded to surgical exploration after discontinuation of chemotherapy, unless a CT scan showed metastatic or locally advanced, unresectable disease (18). The risk of development of distant metastases during neoadjuvant therapy has been reported to be up to 15% (23, 33). This rate equals the occurrence of early disease recurrence in patients with RPC undergoing upfront surgery (34, 35). Patients with pancreatic cancer, who develop early distant metastases after upfront major pancreatectomy, has probably undergone the stress of pancreatectomy for no oncologic gain. However, the risk of local tumor progression during neoadjuvant chemotherapy is a major concern, especially if the patients are losing a curative surgical window. The PREOPANC-2/3 and ALLIANCE-021806 will give important information about the risk of local tumor progression during TNT. It is reasonable that patients with RPC experiencing local tumor progression after 2 months of neoadjuvant chemotherapy are offered discontinuation of chemotherapy and surgical resection in these trials. An alternative could be to switch chemotherapy regimens or give additional radiotherapy. In the TNT study by Kim et al., the chemotherapy regimen was changed if serum CA19-9 levels did not decrease or if the tumor appeared to increase on imaging after the first 2 months of neoadjuvant chemotherapy. However, details on the number of patients who had to change the chemotherapy regimen, or if any patients with local tumor progression discontinued chemotherapy and proceeded to surgical exploration, are not given in that paper (24).
Patients undergoing neoadjuvant chemotherapy may benefit from a chemotherapeutic switch before resection if the response evaluation shows tumor progression (32, 36). The TNT may allow for the switch of chemotherapy that is not possible to implement during SNT. Alva-Ruez et al. recently published the Mayo experience with a chemotherapeutic switch in 468 patients with BRPC and patients with locally advanced pancreatic cancer (LAPC), undergoing first-line chemotherapy without the development of metastatic disease on initial restaging examinations (36). After a median of six cycles of neoadjuvant chemotherapy, 70% (329/468) continued with the first-line chemotherapy regimen after restaging and subsequently underwent surgical resection. The remaining 30% (139/468) of patients underwent chemotherapy switch due to radiological or biochemical progression, no objective response, or toxicity/intolerance. Of patients who underwent chemotherapeutic switch, 72% were able to proceed to curative-intent surgical resection. Although these patients, probably, were highly selected and this was a non-randomized study, the strategy of the chemotherapeutic switch is interesting to implement in future RCTs on SNT vs. TNT in RPC and BRPC.
Kim et al. showed that patients undergoing TNT had improved histologic response [SNT vs. TNT; complete response 4 vs. 8%, near-complete response 15 vs. 16%, partial response 53 vs. 76%, no response 26 vs. 2%; (p < 0.01)] (24). A prognostic and reproducible system for histological tumor response that is scoring in pancreatic cancer may improve comparisons between different trials. More extensive tumor response in one treatment group could indicate a superior treatment effect, and histopathological tumor response scoring could function as a potential surrogate outcome in studies comparing the effectiveness of various durations of neoadjuvant chemotherapy (37).
Evaluation of Treatment Response
During neoadjuvant therapy, the patients are evaluated for treatment toxicities and objective clinical, radiologic, biochemical, or metabolic responses, typically every 2 months (24, 36). If TNT is given, a proper evaluation of treatment response is especially required. However, there is a lack of efficient biomarkers or imaging techniques to monitor treatment responses during neoadjuvant chemotherapy in pancreatic cancer (38, 39). Current assessments using CT or CA19-9 show only modest objective response rates during neoadjuvant chemotherapy (38). In resected patients, low post-treatment CA19-9 levels are independently associated with a histopathologic major response and normalization of CA19-9, rather than the magnitude of change, and has shown to be a strong prognostic marker for a long-term survival (40, 41). A recent systematic review of 17 eligible studies with complete information on CA19-9 response during neoadjuvant therapy found that post-neoadjuvant CA19-9 response >50% or CA19-9 normalization was related to a more promising overall survival, suggesting that optimal CA19-9 response may be a suitable prognostic index to guide treatment decisions (42).
Katz et al. have shown that radiographic downstaging is rare after neoadjuvant therapy, and RECIST response evaluated on CT was not considered as an effective treatment endpoint for patients with BRPC, since only 12% had partial radiographic response (43). Accordingly, patients with RPC and BRPC undergo pancreatectomy after neoadjuvant therapy in the absence of metastases or a locally advanced and unresectable disease. Perri et al. assessed radiographic and serologic measures of treatment responses associated with first-line chemotherapy with FOLFIRINOX or gemcitabine/nab-paclitaxel in 485 consecutive treatment-naive patients with localized pancreatic cancer (44). Among the 280 matched patients, RECIST partial response was more common among patients treated with FOLFIRINOX than with gemcitabine/nab-paclitaxel (19 vs. 6%; p = 0.001), whereas no differences were observed in the median change in tumor volume, the rate of local tumor downstaging, or the CA19-9 levels. In recent studies on TNT, a radiographic downstaging of 28% has been found, maybe due to the use of modern chemotherapy regimens (32, 38). Post-chemotherapy metabolic responses based on positron emission tomography (PET/CT or PET/MRI) metabolic imaging as surrogates of pathologic response is currently used in some centers to evaluate treatment response (32, 45, 46). Metabolic response by PET/CT or PET/MRI may be a more sensitive measure of tumor response than traditional CT or MRI and should be evaluated in future clinical trials (47). Criteria to be considered in the evaluation of treatment response during neoadjuvant therapy in pancreatic cancer are presented in Table 2.
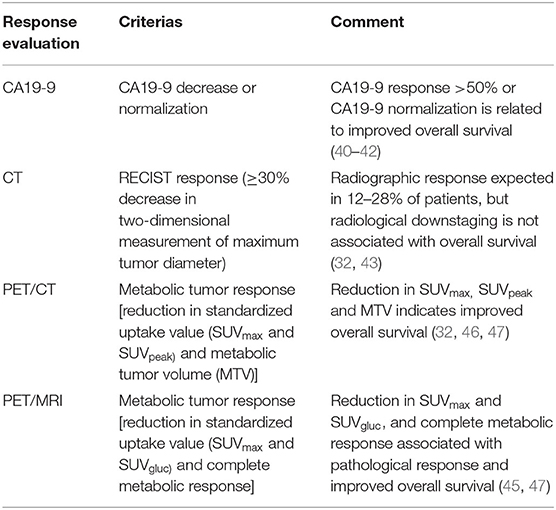
Table 2. Criteria to be considered in the evaluation of treatment response during neoadjuvant therapy in pancreatic cancer.
Impact of Adjuvant Chemotherapy After Neoadjuvant Chemotherapy
The potential benefits of adjuvant chemotherapy after neoadjuvant therapy are not well-defined (29). The choice of adjuvant regimen is often based on response seen to neoadjuvant therapy and other clinical considerations, such as performance status and patient tolerability (2). Whether continuation of the same regimen is worthwhile in case of poor histopathological response remains to be established. Based on data from the National Cancer Data Base, Kamarajah et al. showed that adjuvant chemotherapy, following neoadjuvant chemotherapy and resection, was associated with improved survival, even in R0 and N0 disease (48). However, van Rossel et al. showed that adjuvant chemotherapy after neoadjuvant FOLFIRINOX and resection was associated with improved survival only in patients with N1/N2 disease (29). This is by the treatment strategy given by Kim et al., where patients who received SNT, in general, were recommended to receive additional adjuvant therapy in the absence of a very favorable pathology report (e.g., a near-complete or complete response and N0) or inadequate recovery from surgery (24).
Refinement of Perioperative Chemotherapy in the Era of Precision Medicine
The personalized medicine approach in pancreatic cancer still needs to remove some barriers to be effective in clinical practice (11, 49). The patients with RPC and BRPC currently receive a one-size-fits-all treatment strategy based on results from RCTs on adjuvant and neoadjuvant therapy (4, 6–9, 16, 19). Ongoing RCTs also follow the principle of one-size-fits-all. However, a broad heterogeneity is observed in survival and response to neoadjuvant therapy with FOLFIRINOX and gemcitabine/nab-paclitaxel in patients with RPC and BRPC. The FOLFIRINOX has been associated with higher rates of RECIST partial response and subsequent pancreatectomy than gemcitabine/nab-paclitaxel, but the overall survival associated with these regimens are similar (16, 44). A neoadjuvant strategy should select and use the most effective and clinically tolerable chemotherapy regimen (36). Currently, a selection of combination regimen is based entirely on clinical criteria, and no biomarkers exist to guide the choice of chemotherapy in RPC and BRPC. A better patient stratification is needed to guide personalized treatment strategies and to prevent chemotherapy-related toxicity to improve outcomes. Interestingly, a pancreatic cancer patient-derived organoid library obtained gene expression signatures of chemosensitivity that predicted improved response to chemotherapy (50). Hopefully, this methodology may identify genomic, transcriptomic, and therapeutic profiling to guide the choice of chemotherapeutics and enable stratification of patients. By this approach, patients may rapidly achieve clinical benefits while more tailored treatments can be developed for each patient.
Liquid biopsies enable the collection of repeated samples during neoadjuvant therapy and can help to stratify patients to the most suitable treatment and to monitor treatment response. Several biomarkers, including circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), cell-free RNA (cfRNA), and exosomes are explored, with the potential to be applied to the clinical setting (51). Several ongoing clinical trials explore the use of liquid biopsies for early diagnosis or predictive and prognostic purposes in pancreatic cancer (51). Gemenetzis et al. showed that patients who had received neoadjuvant treatment had significantly lower numbers of CTCs across all phenotypes compared with a chemo-naive cohort undergoing upfront surgery (52). Moreover, Bernard et al. found that monitoring of exoDNA during neoadjuvant therapy provided predictive information on treatment response in patients with localized pancreatic cancer (53). In a recent multicenter study of 504 patients receiving neoadjuvant FOLFIRINOX or gemcitabine/nab-paclitaxel ± radiation, followed by pancreatectomy, 104 patients received TNT that was associated with an increased rate of major (complete/near-complete) pathologic response and overall survival (31). However, pathologic complete response (pCR) does not tell the whole story. Interestingly, Yin et al. found that somatic mutations, CTCs, and ctDNA existed even in patients with pancreatic cancer with pCR to neoadjuvant therapy, and proposed a new concept of regression assessment by combining genomic analysis of resected specimens and liquid biopsy data, namely, molecular complete response (mCR) (54). Efforts to develop predictive and therapy-response circulating biomarkers are underway, and will represent important tools for monitoring patients, supporting clinicians, and guiding treatment decisions in the future.
More patients with pancreatic cancer might benefit to undergo tumor molecular profiling or receive targeted therapies (55). Some novel attempts to incorporate tumor profiling into the treatment of pancreatic cancer have been published. A retrospective analysis of the Know Your Tumor registry trial showed that patients who had actionable molecular alterations had benefited from receiving a matched therapy (56). However, only a small percentage of all pancreatic cancer patients have mutations that can be targeted. Best-in-class examples of potentially targetable genetic alterations were found in about 8% of the patients; Poly (ADP-ribose) polymerase (PARP) inhibitors targeting germline Breast cancer gene (BRCA)1/2 mutations, Tropomyosin receptor kinase (TRK) inhibitors for Neurotrophic tyrosine receptor kinase (NTRK)1/2/3 fusions, and immune checkpoint inhibitors for Mismatch repair (MMR)-deficient or Microsatellite instability high (MSI-H) tumors (56). Although most treatment recommendations are largely based on data from treatment of metastatic and locally advanced pancreatic cancer, some of these findings could be explored in RPC and BPRC in future clinical trials. The European Society of Medical Oncology (ESMO) recommends clinical research centers propose multi-gene sequencing to patients with advanced pancreatic cancer in the context of molecular screening programs, for patients to get access to innovative drugs (57). If multigene sequencing is not carried out, the ESMO currently recommends that detection of MSI-H and NTRK fusions should be done using cheaper standard methods. In BRPC, the NCCN currently recommends core tumor biopsy to be performed at the time of diagnosis to obtain adequate tissue for possible ancillary studies (2). However, at present, there is limited evidence to recommend specific neoadjuvant regimens other than FOLFIRINOX and gemcitabine/nab-paclitaxel off-study. The NCCN suggests that testing for actionable somatic findings with fusions [Anaplastic lymphoma kinase (ALK), Neuregulin-1 gene (NRG1), NTRK, ROS proto-oncogene 1 (ROS1)], mutations [Proto-oncogene B-Raf (BRAF), BRCA1/2, Human epidermal growth factor receptor 2 (HER2), Kirsten rat sarcoma viral oncogene homologue (KRAS), Partner and Localizer of BRCA2 (PALB2)], and MMR deficiency must be considered in metastatic or locally advanced, unresectable disease (2). For known BRCA1/2 or PALB2 mutations, NCCN recommends gemcitabine/cisplatin or (m)FOLFIRINOX. For MSI or MMR tumors, pembrolizumab is considered as an option, whereas for NTRK gene fusion-positive disease, larotrectinib or entrectinib may be considered (2). At present, targeted therapy is probably most important to explore in patients with LAPC to achieve downstaging and surgical resection or in metastatic disease. However, given the risk of progression during neoadjuvant therapy and high risk of recurrence after surgical resection in patients with RPC and BRPC, tumor/somatic gene profiling to identify uncommon mutations should also be considered in these patients at the time of diagnosis, so that tailored treatments can be considered early in patients with progressive disease.
Conclusion
Most RCTs in RPC and BRPC have explored SNT, but TNT is now evaluated in several ongoing trials. The chemotherapeutic switch could be incorporated into neoadjuvant treatment sequencing in future trials. Components of an objective response include clinical, biochemical (CA19-9 decrease), radiologic (decreased tumor size/less vascular involvement), or metabolic responses (decreased tumoral PET avidity/viability). In the future, biomarker hypothesis-driven clinical trials and better-circulating biomarkers (CTCs, ctDNA, cfRNA, and exosomes) and imaging techniques (PET/CT, PET/MRI) to evaluate treatment responses are needed to guide personalized therapy and improve outcomes for patients with pancreatic cancer.
Author Contributions
KJL contributed to conception and design of the review, wrote the first draft of the manuscript and revised, read, and approved the submitted version.
Funding
This work was supported by the South-Eastern Norway Regional Health Authority (grant number 2019029).
Conflict of Interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Huang L, Jansen L, Balavarca Y, Molina-Montes E, Babaei M, van der Geest L, et al. Resection of pancreatic cancer in Europe and USA: an international large-scale study highlighting large variations. Gut. (2019) 68:130–9. doi: 10.1136/gutjnl-2017-314828
2. Pancreatic Adenocarcinoma Version 2. 2021, NCCN Practice Guidelines in Oncology. Available online at: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1455 (accessed December 1, 2021).
3. Mavros MN, Moris D, Karanicolas PJ, Katz MHG, O'Reilly EM, Pawlik TM. Clinical trials of systemic chemotherapy for resectable pancreatic cancer: a review. JAMA Surg. (2021) 156:663–72. doi: 10.1001/jamasurg.2021.0149
4. Conroy T, Hammel P, Hebbar M, Ben Abdelghani M, Wei AC, Raoul JL, et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med. (2018) 379:2395–406. doi: 10.1056/NEJMoa1809775
5. Bockhorn M, Uzunoglu FG, Adham M, Imrie C, Milicevic M, Sandberg AA, et al. Borderline resectable pancreatic cancer: a consensus statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery. (2014) 155:977–88. doi: 10.1016/j.surg.2014.02.001
6. Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. (2004) 350:1200–10. doi: 10.1056/NEJMoa032295
7. Neoptolemos JP, Stocken DD, Bassi C, Ghaneh P, Cunningham D, Goldstein D, et al. Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: a randomized controlled trial. JAMA. (2010) 304:1073–81. doi: 10.1001/jama.2010.1275
8. Oettle H, Neuhaus P, Hochhaus A, Hartmann JT, Gellert K, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: the CONKO-001 randomized trial. JAMA. (2013) 310:1473–81. doi: 10.1001/jama.2013.279201
9. Neoptolemos JP, Palmer DH, Ghaneh P, Psarelli EE, Valle JW, Halloran CM, et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet. (2017) 389:1011–24. doi: 10.1016/S0140-6736(16)32409-6
10. van Dam JL, Janssen QP, Besselink MG, Homs MYV, van Santvoort HC, van Tienhoven G, et al. Neoadjuvant therapy or upfront surgery for resectable and borderline resectable pancreatic cancer: a meta-analysis of randomised controlled trials. Eur J Cancer. (2022) 160:140–9. doi: 10.1016/j.ejca.2021.10.023
11. Lambert A, Schwarz L, Borbath I, Henry A, Van Laethem JL, Malka D, et al. An update on treatment options for pancreatic adenocarcinoma. Ther Adv Med Oncol. (2019) 11:1758835919875568. doi: 10.1177/1758835919875568
12. Testing the Use of the Usual Chemotherapy Before and After Surgery for Removable Pancreatic Cancer. ClinicalTrials.gov identifier. Available online at: https://clinicaltrials.gov/ct2/show/NCT04340141 (accessed December 1, 2021).
13. Perioperative or Adjuvant mFOLFIRINOX for Resectable Pancreatic Cancer. ClinicalTrials.gov identifier. Available online at: https://clinicaltrials.gov/ct2/show/NCT04927780 (accessed December 1, 2021).
14. Labori KJ, Lassen K, Hoem D, Gronbech JE, Soreide JA, Mortensen K, et al. Neoadjuvant chemotherapy versus surgery first for resectable pancreatic cancer (Norwegian Pancreatic Cancer Trial - 1 (NorPACT-1)) - study protocol for a national multicentre randomized controlled trial. BMC Surg. (2017) 17:94. doi: 10.1186/s12893-017-0291-1
15. Schwarz L, Vernerey D, Bachet JB, Tuech JJ, Portales F, Michel P, et al. Resectable pancreatic adenocarcinoma neo-adjuvant FOLF(IRIN)OX-based chemotherapy - a multicenter, non-comparative, randomized, phase II trial (PANACHE01-PRODIGE48 study). BMC Cancer. (2018) 18:762. doi: 10.1186/s12885-018-4663-4
16. Sohal DPS, Duong M, Ahmad SA, Gandhi NS, Beg MS, Wang-Gillam A, et al. Efficacy of perioperative chemotherapy for resectable pancreatic adenocarcinoma: a phase 2 randomized clinical trial. JAMA Oncol. (2021) 7:421–7. doi: 10.1001/jamaoncol.2020.7328
17. Ghaneh P, Palmer DH, Cicconi S, Halloran C, Psarelli EE, Rawcliffe CL, et al. ESPAC-5F: Four-arm, prospective, multicenter, international randomized phase II trial of immediate surgery compared with neoadjuvant gemcitabine plus capecitabine (GEMCAP) or FOLFIRINOX or chemoradiotherapy (CRT) in patients with borderline resectable pancreatic cancer. J Clin Oncol. (2020) 38(15_suppl):4505. doi: 10.1200/JCO.2020.38.15_suppl.4505
18. Janssen QP, van Dam JL, Bonsing BA, Bos H, Bosscha KP, Coene P, et al. Total neoadjuvant FOLFIRINOX vs. neoadjuvant gemcitabine-based chemoradiotherapy and adjuvant gemcitabine for resectable and borderline resectable pancreatic cancer (PREOPANC-2 trial): study protocol for a nationwide multicenter randomized controlled trial. BMC Cancer. (2021) 21:300. doi: 10.1186/s12885-021-08031-z
19. Versteijne E, Suker M, Groothuis K, Akkermans-Vogelaar JM, Besselink MG, Bonsing BA, et al. Preoperative chemoradiotherapy versus immediate surgery for resectable and borderline resectable pancreatic cancer: results of the dutch randomized phase III PREOPANC trial. J Clin Oncol. (2020) 38:1763–73. doi: 10.1200/JCO.19.02274
20. Unno M, Motoi F, Matsuyama Y, Satoi S, Matsumoto I, Aosasa S, et al. Randomized phase II/III trial of neoadjuvant chemotherapy with gemcitabine and S-1 vs. upfront surgery for resectable pancreatic cancer (Prep-02/JSAP-05). J Clin Oncol. (2019) 37(4_Suppl.):189. doi: 10.1200/JCO.2019.37.4_suppl.189
21. Motoi F, Kosuge T, Ueno H, Yamaue H, Satoi S, Sho M, et al. Randomized phase II/III trial of neoadjuvant chemotherapy with gemcitabine and S-1 versus upfront surgery for resectable pancreatic cancer (Prep-02/JSAP05). Jpn J Clin Oncol. (2019) 49:190–4. doi: 10.1093/jjco/hyy190
22. Ettrich TJ, Berger AW, Perkhofer L, Daum S, Konig A, Dickhut A, et al. Neoadjuvant plus adjuvant or only adjuvant nab-paclitaxel plus gemcitabine for resectable pancreatic cancer - the NEONAX trial (AIO-PAK-0313), a prospective, randomized, controlled, phase II study of the AIO pancreatic cancer group. BMC Cancer. (2018) 18:1298. doi: 10.1186/s12885-018-5183-y
23. Reni M, Balzano G, Zanon S, Zerbi A, Rimassa L, Castoldi R, et al. Safety and efficacy of preoperative or postoperative chemotherapy for resectable pancreatic adenocarcinoma (PACT-15): a randomised, open-label, phase 2-3 trial. Lancet Gastroenterol Hepatol. (2018) 3:413–23. doi: 10.1016/S2468-1253(18)30081-5
24. Kim RY, Christians KK, Aldakkak M, Clarke CN, George B, Kamgar M, et al. Total neoadjuvant therapy for operable pancreatic cancer. Ann Surg Oncol. (2021) 28:2246–56. doi: 10.1245/s10434-020-09149-3
25. Versteijne E, van Dam JL, Suker M, Janssen QP, Groothuis K, Akkermans-Vogelaar JM, et al. Neoadjuvant chemoradiotherapy versus upfront surgery for resectable and borderline resectable pancreatic cancer: long-term results of the dutch randomized PREOPANC trial. J Clin Oncol. (2022). doi: 10.1200/JCO.21.02233. [Epub ahead of print].
26. Janssen QP, van Dam JL, Kivits IG, Besselink MG, van Eijck CHJ, Homs MYV, et al. Added value of radiotherapy following neoadjuvant FOLFIRINOX for resectable and borderline resectable pancreatic cancer: a systematic review and meta-analysis. Ann Surg Oncol. (2021) 28:8297–308. doi: 10.1245/s10434-021-10276-8
27. Helsedirektoratet. Nasjonalt handlingsprogram med retningslinjer for diagnostikk, behandling og oppfølging av pancreaskreft. Available online at: https://www.helsedirektoratet.no/retningslinjer/pancreaskreft-bukspyttkjertelkreft-handlingsprogram. IS-2624 (accessed December 1, 2021).
28. Janssen QP, Buettner S, Suker M, Beumer BR, Addeo P, Bachellier P, et al. Neoadjuvant FOLFIRINOX in patients with borderline resectable pancreatic cancer: a systematic review and patient-level meta-analysis. J Natl Cancer Inst. (2019) 111:782–94. doi: 10.1093/jnci/djz073
29. van Roessel S, van Veldhuisen E, Klompmaker S, Janssen QP, Abu Hilal M, Alseidi A, et al. Evaluation of adjuvant chemotherapy in patients with resected pancreatic cancer after neoadjuvant FOLFIRINOX treatment. JAMA Oncol. (2020) 6:1733–40. doi: 10.1001/jamaoncol.2020.3537
30. Murphy JE, Wo JY, Ryan DP, Jiang W, Yeap BY, Drapek LC, et al. Total neoadjuvant therapy with FOLFIRINOX followed by individualized chemoradiotherapy for borderline resectable pancreatic adenocarcinoma: a phase 2 clinical trial. JAMA Oncol. (2018) 4:963–9. doi: 10.1001/jamaoncol.2018.0329
31. Datta J, Collier A, Kronenfeld J, Wilson G, Maduekwe U, Snyder RA, et al. Association of total neoadjuvant therapy with major pathologic response and survival in localized pancreatic cancer: a multi-institutional analysis of 504 patients. J Clin Oncol. (2021) 39(15_suppl):4145. doi: 10.1200/JCO.2021.39.15_suppl.4145
32. Truty MJ, Kendrick ML, Nagorney DM, Smoot RL, Cleary SP, Graham RP, et al. Factors predicting response, perioperative outcomes, and survival following total neoadjuvant therapy for borderline/locally advanced pancreatic cancer. Ann Surg. (2021) 273:341–9. doi: 10.1097/SLA.0000000000003284
33. Tzeng CW, Fleming JB, Lee JE, Xiao L, Pisters PW, Vauthey JN, et al. Defined clinical classifications are associated with outcome of patients with anatomically resectable pancreatic adenocarcinoma treated with neoadjuvant therapy. Ann Surg Oncol. (2012) 19:2045–53. doi: 10.1245/s10434-011-2211-4
34. Labori KJ, Katz MH, Tzeng CW, Bjornbeth BA, Cvancarova M, Edwin B, et al. Impact of early disease progression and surgical complications on adjuvant chemotherapy completion rates and survival in patients undergoing the surgery first approach for resectable pancreatic ductal adenocarcinoma - A population-based cohort study. Acta Oncol. (2016) 55:265–77. doi: 10.3109/0284186X.2015.1068445
35. Groot VP, Rezaee N, Wu W, Cameron JL, Fishman EK, Hruban RH, et al. Patterns, timing, and predictors of recurrence following pancreatectomy for pancreatic ductal adenocarcinoma. Ann Surg. (2018) 267:936–45. doi: 10.1097/SLA.0000000000002234
36. Alva-Ruiz R, Yohanathan L, Yonkus JA, Abdelrahman AM, Gregory LA, Halfdanarson TR, et al. Neoadjuvant chemotherapy switch in borderline resectable/locally advanced pancreatic cancer. Ann Surg Oncol. (2022) 29:1579–91. doi: 10.1245/s10434-021-10991-2
37. van Roessel S, Janssen BV, Soer EC, Farina Sarasqueta A, Verbeke CS, Luchini C, et al. Scoring of tumour response after neoadjuvant therapy in resected pancreatic cancer: systematic review. Br J Surg. (2021) 108:119–27. doi: 10.1093/bjs/znaa031
38. Perri G, Prakash LR, Katz MHG. Response to preoperative therapy in localized pancreatic cancer. Front Oncol. (2020) 10:516. doi: 10.3389/fonc.2020.00516
39. Evans DB, George B, Tsai S. Non-metastatic pancreatic cancer: resectable, borderline resectable, and locally advanced-definitions of increasing importance for the optimal delivery of multimodality therapy. Ann Surg Oncol. (2015) 22:3409–13. doi: 10.1245/s10434-015-4649-2
40. Perri G, Prakash L, Wang H, Bhosale P, Varadhachary GR, Wolff R, et al. Radiographic and serologic predictors of pathologic major response to preoperative therapy for pancreatic cancer. Ann Surg. (2021) 273:806–13. doi: 10.1097/SLA.0000000000003442
41. Tsai S, George B, Wittmann D, Ritch PS, Krepline AN, Aldakkak M, et al. Importance of normalization of CA19-9 levels following neoadjuvant therapy in patients with localized pancreatic cancer. Ann Surg. (2020) 271:740–7. doi: 10.1097/SLA.0000000000003049
42. Ye C, Sadula A, Ren S, Guo X, Yuan M, Yuan C, et al. The prognostic value of CA19-9 response after neoadjuvant therapy in patients with pancreatic cancer: a systematic review and pooled analysis. Cancer Chemother Pharmacol. (2020) 86:731–40. doi: 10.1007/s00280-020-04165-2
43. Katz MH, Fleming JB, Bhosale P, Varadhachary G, Lee JE, Wolff R, et al. Response of borderline resectable pancreatic cancer to neoadjuvant therapy is not reflected by radiographic indicators. Cancer. (2012) 118:5749–56. doi: 10.1002/cncr.27636
44. Perri G, Prakash L, Qiao W, Varadhachary GR, Wolff R, Fogelman D, et al. Response and survival associated with first-line FOLFIRINOX vs gemcitabine and nab-paclitaxel chemotherapy for localized pancreatic ductal adenocarcinoma. JAMA Surg. (2020) 155:832–9. doi: 10.1001/jamasurg.2020.2286
45. Panda A, Garg I, Truty MJ, Kline TL, Johnson MP, Ehman EC, et al. Borderline resectable and locally advanced pancreatic cancer: FDG PET/MRI and CT tumor metrics for assessment of pathologic response to neoadjuvant therapy and prediction of survival. Am J Roentgenol. (2021) 217:730–40. doi: 10.2214/AJR.20.24567
46. Lee W, Oh M, Kim JS, Park Y, Kwon JW, Jun E, et al. Metabolic activity by FDG-PET/CT after neoadjuvant chemotherapy in borderline resectable and locally advanced pancreatic cancer and association with survival. Br J Surg. (2021) 109:61–70. doi: 10.1093/bjs/znab229
47. Evangelista L, Zucchetta P, Moletta L, Serafini S, Cassarino G, Pegoraro N, et al. The role of FDG PET/CT or PET/MRI in assessing response to neoadjuvant therapy for patients with borderline or resectable pancreatic cancer: a systematic literature review. Ann Nucl Med. (2021) 35:767–76. doi: 10.1007/s12149-021-01629-0
48. Kamarajah SK, White SA, Naffouje SA, Salti GI, Dahdaleh F. Adjuvant chemotherapy associated with survival benefit following neoadjuvant chemotherapy and pancreatectomy for pancreatic ductal adenocarcinoma: a population-based cohort study. Ann Surg Oncol. (2021) 28:6790–802. doi: 10.1245/s10434-021-09823-0
49. Chantrill LA, Nagrial AM, Watson C, Johns AL, Martyn-Smith M, Simpson S, et al. Precision medicine for advanced pancreas cancer: the individualized molecular pancreatic cancer therapy (IMPaCT) trial. Clin Cancer Res. (2015) 21:2029–37. doi: 10.1158/1078-0432.CCR-15-0426
50. Tiriac H, Belleau P, Engle DD, Plenker D, Deschenes A, Somerville TDD, et al. Organoid profiling identifies common responders to chemotherapy in pancreatic cancer. Cancer Discov. (2018) 8:1112–29. doi: 10.1158/2159-8290.CD-18-0349
51. Heredia-Soto V, Rodriguez-Salas N, Feliu J. Liquid biopsy in pancreatic cancer: are we ready to apply it in the clinical practice? Cancers. (2021) 13:1986. doi: 10.3390/cancers13081986
52. Gemenetzis G, Groot VP, Yu J, Ding D, Teinor JA, Javed AA, et al. Circulating tumor cells dynamics in pancreatic adenocarcinoma correlate with disease status: results of the prospective CLUSTER study. Ann Surg. (2018) 268:408–20. doi: 10.1097/SLA.0000000000002925
53. Bernard V, Kim DU, San Lucas FA, Castillo J, Allenson K, Mulu FC, et al. Circulating nucleic acids are associated with outcomes of patients with pancreatic cancer. Gastroenterology. (2019) 156:108–18 e4. doi: 10.1053/j.gastro.2018.09.022
54. Yin L, Pu N, Thompson E, Miao Y, Wolfgang C, Yu J. Improved assessment of response status in patients with pancreatic cancer treated with neoadjuvant therapy using somatic mutations and liquid biopsy analysis. Clin Cancer Res. (2021) 27:740–8. doi: 10.1158/1078-0432.CCR-20-1746
55. Miyabayashi K, Nakagawa H, Koike K. Molecular and phenotypic profiling for precision medicine in pancreatic cancer: current advances and future perspectives. Front Oncol. (2021) 11:682872. doi: 10.3389/fonc.2021.682872
56. Pishvaian MJ, Blais EM, Brody JR, Lyons E, DeArbeloa P, Hendifar A, et al. Overall survival in patients with pancreatic cancer receiving matched therapies following molecular profiling: a retrospective analysis of the Know Your Tumor registry trial. Lancet Oncol. (2020) 21:508–18. doi: 10.1016/S1470-2045(20)30074-7
57. Mosele F, Remon J, Mateo J, Westphalen CB, Barlesi F, Lolkema MP, et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO Precision Medicine Working Group. Ann Oncol. (2020) 31:1491–505. doi: 10.1016/j.annonc.2020.07.014
Keywords: pancreatic cancer, neoadjuvant chemotherapy, precision medicine, surgery, Response Evaluation Criteria
Citation: Labori KJ (2022) Short-Course or Total Neoadjuvant Chemotherapy in Resectable and Borderline Resectable Pancreatic Cancer - Current Status and Future Perspectives. Front. Surg. 9:839339. doi: 10.3389/fsurg.2022.839339
Received: 19 December 2021; Accepted: 28 February 2022;
Published: 25 April 2022.
Edited by:
Casper Van Eijck, Erasmus University Rotterdam, NetherlandsReviewed by:
Wooil Kwon, Seoul National University Hospital, South KoreaJose M. Pimiento, Moffitt Cancer Center, United States
Copyright © 2022 Labori. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Knut Jørgen Labori, dXhrbmFiQG91cy1oZi5ubw==