
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Surg. , 01 February 2022
Sec. Surgical Oncology
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.812343
This article is part of the Research Topic Laparoscopic Surgery in Colorectal Cancer View all 10 articles
 Junwei Tang†
Junwei Tang† Yue Zhang†Dongsheng ZhangChuan ZhangKangpeng JinDongjian Ji
Yue Zhang†Dongsheng ZhangChuan ZhangKangpeng JinDongjian Ji Wen PengYifei Feng*
Wen PengYifei Feng* Yueming Sun*
Yueming Sun*Introduction: Transanal endoscopic microsurgery (TEM) is an organ-preserving treatment alternative for patients with early rectal cancer. However, TEM alone is associated with greater risk of local recurrence and inferior survival in comparison with total meso-rectal excision (TME). As an important adjuvant therapy, radiotherapy can effectively reduce the local recurrence rate of rectal cancer. This study aimed to investigate whether TEM followed by radiotherapy can be a valid alternative to TME in T2N0M0 distal rectal cancer treatment.
Methods: We plan to recruit 168 participants meeting established inclusion criteria. Following informed consent, participants will randomly receive treatment protocols of TEM followed by radiotherapy (a total dose of 45–50.4 Gy given in 25–28 factions) or TME. Depending on post-operative pathology, the participants will receive either long-term follow-up or further treatment. The primary endpoint of this trial is 3-year local recurrence rate. The secondary end points include 3-year disease-free survival rate, 3-year overall survival rate, 3-year mortality rate, post-operative quality of life, post-operative safety index, intraoperative evaluation index and post-operative short-term evaluation index.
Discussion: This trial is the first prospective randomized trial to investigate the rectum preserving treatment by using transanal local excision followed by radiotherapy.
Clinical trial registration: The trial was prospectively registered at ClinicalTrials.gov NCT04098471 on September 20, 2019.
Colorectal cancer (CRC) was the third most commonly diagnosed cancer and was the second leading cause of cancer-related death in the world (1). In China, CRC was also one of the most common malignant tumors, and the incidence continues to increase (2), which became a fatal health problem.
Rectal cancer accounts for more than 65% of CRC (3). In the early 1980s, Total meso-rectal excision (TME) was raised by Heald, which emphasized a sharp and meticulous dissection of the tumor and mesorectum with all associated lymph nodes through the avascular embryologic plane (4, 5). TME was considered to the most important progress in surgery for rectal cancer in the last two decades. With the application of TME, the local recurrence decreased to 6 to 12%, and 5-year survival rate improved by 53–87% (6–9). Hence, TME has gradually become a standard component of radical surgery in rectal cancer treatment (10). However, some complications, such as anastomotic leakage, anastomotic hemorrhage, anterior excision syndrome and sexual dysfunction, are common after TME, especially in distal rectal cancer treatment (11–13). Transanal local excision (TLE) is commonly used in benign neoplasms and low-risk superficial malignant rectal cancer. Transanal endoscopic microsurgery (TEM) created by Buess in 1980s, is a technique of TLE which enables the surgeon to perform a full thickness excision with great precision (14). Compared with TME, traditional TLE and TEM both have the significant advantages of preserving anorectal, sexual and urinary functions, reducing the mortality and improving the quality of life (15–17). However, lymph node dissection of rectal cancer was not involved in TLE, which leads to great concern about the increase of tumor recurrence rate and the decrease of survival rate. Although the risk of lymph node metastasis is closely related to the depth of invasion, lymph node metastasis has also been found in patients with early cancer. As reported in the literature, the incidence of lymph node metastasis could reach for 10.3% in T1 stage, 26.1% in T2 stage and 51.2% in T3 stage (18).
Adjuvant therapy for rectal cancer has made great process over the last 40 years, including the adjuvant radiotherapy (RT). Even after the development of the TME with its greatly improved local control rates, radiotherapy significantly decreased the risk of local recurrence (19). For example, the result of a randomized trial of 1,861 patients showed that the rate of local recurrence at 2 years was significantly higher in TME-only group (8.2%) than in TME+RT group (2.4%) (20). The presence of undiagnosed nodal disease, extramural vascular invasion and implantation of cancer cells are the common causes of high local recurrence rate in TLE, whereas radiotherapy can alleviate it by sterilizing the excision bed and adjacent meso-rectal lymph nodes (21). Recently, increasing evidence showed that the organ preservation strategies incorporated RT as an alternative to radical surgery for the early-stage rectal cancer (22, 23). Therefore, for better implementing the organ-preserving strategy, we hypothesized that TEM combined with radiotherapy could be safely and effectively used for the eligible T2N0M0 rectal cancer treatment. The primary objective of this study is to compare the local recurrence rate of TEM followed by radiotherapy and laparoscopic TME surgery in the treatment of T2N0M0 distal rectal cancer. Secondary objectives are long-term survival rate, intraoperative and post-operative situation, and quality of life.
The inclusion criteria were as followed: (1) Subjects were 18–75 years old; (2) Pre-operative pathological diagnosis was adenocarcinoma; (3) The location of tumor was within 4 cm of anal verge; (4) Tumor size ≤ 3 cm; (5) The mass is mobile and non-fixed; (6) Pre-operative MRI and rectal EUS suggest that the stage was T2 only; (7) Pre-operative high-resolution CT and MRI showed no evidence of lymphatic metastasis or distant metastasis; (8) The general condition of the subjects was fair and their ASA score ≤ 3; (9) Subjects signed an informed consent form.
The exclusion criteria were as followed: (1) Participants are Suffering from other malignant tumors within 5 years; (2) Pathological type were poorly differentiated adenocarcinoma, mucinous adenocarcinoma or signet-ring cell carcinoma; (3) Participants are diagnosed as multiple primary colorectal tumors; (4) Participants are pregnant or lactating women; (5) Participants are suffering from severe mental disorders; (6) Participants have Received radiotherapy or chemotherapy already; (7) Participants are suffering from other intestinal diseases (FAP, HNPCC, ulcerative colitis or Crohn's disease); (8) Participants can't suffer abdominal surgery for various reasons; (9) Participants are involved in other clinical trials.
The exit criteria were as followed: (1) Subjects fail for the implementation of the treatment plan for various reasons; (2) The study cannot be continued due to the poor compliance of subjects; (3) Subjects request to withdraw or terminate the treatment due to personal reasons.
The study is a prospective, randomized, open and parallel controlled study to determine whether TEM followed by radiotherapy can be considered as an effective therapeutic strategy in eligible T2N0M0 rectal cancer. Firstly, all the subjects who met the inclusion criteria were randomly divided into TME group and TEM followed by radiotherapy group, treated with TME and TEM surgery, respectively. Randomization was performed by an Electronic Data Capture System (EDC) called Clinflash EDC. After histological detection of the resected specimen, subjects undergoing TEM with a pT2N0M0 adenocarcinoma, clear margin and no neurovascular invasion, will receive the post-operative RT with a total dose of 45–50.4 Gy which is given in 25–28 factions. Whereas, subjects with undergoing TME surgery will not receive any other treatment in this situation. Finally, all patients will be followed up. The flow chart of the study is shown in Figure 1.
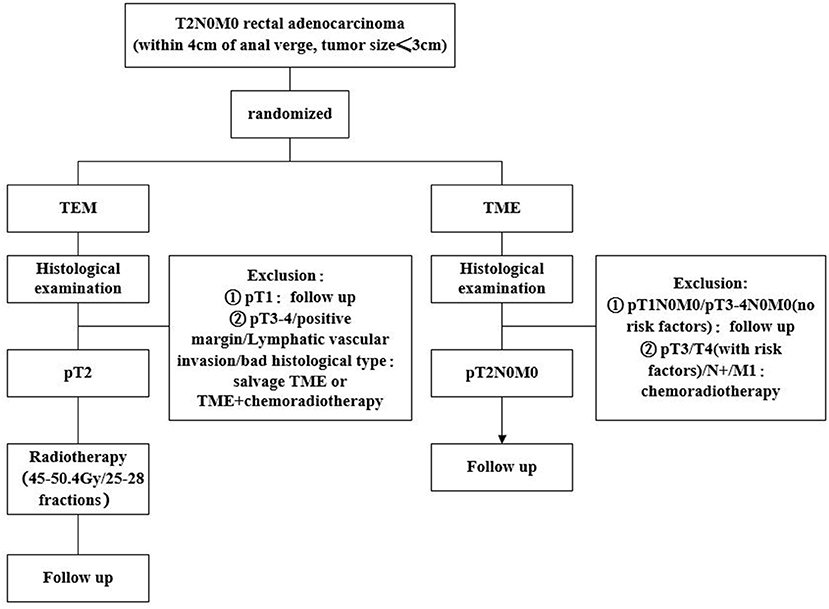
Figure 1. Flowchart of the study.
The primary end point is 3-year local recurrence rate. Secondary end points include 3-year disease-free survival rate, 3-year overall survival rate, 3-year mortality rate, post-operative quality of life, post-operative safety index, intraoperative evaluation index and post-operative short-term evaluation index. Specifically, post-operative safety index includes complication rate, perioperative mortality and R0 resection rate. Intraoperative evaluation index includes operative time, intraoperative blood loss, colostomy rate and intraoperative blood transfusion. Post-operative short-term evaluation index includes intestinal exhaust time, post-operative pain and hospital stay. All subjects will be followed up in the outpatient service every 3 months for 3 years. CT scan of abdomen and thorax and colonoscopy must be performed every 6 months. Moreover, ERUS should be performed in patients treated with TEM every 3 months. EORTC QLQ-C30 & LC13 will be measured the quality of life.
At least 5 Chinese hospitals will participate in the study, and all of which are experienced in laparoscopic TME and TEM surgery for rectal cancer treatment.
In a review of the laparoscopic TME surgery performed in our department, the 3-year recurrence free rate of T2N0M0 rectal cancer patients was nearly 95%. According to 10% of non-inferiority value, 1:1 of the sample size in two groups, 0.025 of the first type of error, 80% power and maximum 10% highest lost rate of follow-up, calculated by Pearson chi-square test, each group needs to include 84 cases, 168 cases in total.
Data collection and analysis will be performed by the SPSS 21.0, Graphpad prsim 5 and Excel software. The measurement data will be expressed as mean ± standard deviation. The statistical analyses will be performed using t-tests, Pearson's χ2 tests and ANOVA. Cumulative survival analysis will be performed by the Kaplan–Meier method. Differences are considered to be statistically significant at P ≤ 0.05.
A TME involves a complete excision of the mesorectum, including associated vascular, lymphatic structures and fatty tissue, is recommended in abdominal resections and significantly improved patients' prognosis (24). With the improvement of oncological outcome, the question has risen if new therapeutic schedule can be developed with safe efficacy and better organ preserving.
Transanal local excision, as a minimally invasive and rectum-preserving treatment, have its advantages of minimal morbidity and mortality, rapid post-operative recovery and a higher post-operative quality of life. Compared with traditional TLE, TEM may be technically feasible for more proximal lesions. A 2015 meta-analysis reported that TEM was oncologically superior to direct TLE for the excision of rectal neoplasms because of a higher rate of negative microscopic margins, a reduced rate of specimen fragmentation and lesion recurrence (25). However, due to the absence of pathologic staging of nodal involvement, the safety of TEM were still controversial for a long time (26–29). At present, TEM is only suggested to treat in selected T1N0M0 rectal cancer or patients physically unfit to undergo TME surgery based on the NCCN guidelines (30).
Although the long-term data on local resection in patients with T2N0M0 rectal cancer are limited, evidence showed that the oncological effect of TLE alone was not satisfactory for patients with T2N0M0 rectal cancer (23, 28, 31, 32). For example, a retrospective study of 1,030 patients showed the 5-year local recurrence rates of T2 tumors increased and the 5-year overall survival decreased after TLE compared to standard resection (31). Even though some reports supported the application of TEM in the treatment of T2 rectal cancer (26, 27), its safety is still worrying (33, 34). For better applying TEM to the treatment of T2N0M0 rectal cancer, TEM combined with adjuvant therapy have been carried out in recent years (35–37). For example, in a prospective multicenter trial named CARTS study (38, 39), patients with a clinical T1-3N0M0 rectal adenocarcinoma were treated with chemoradiation therapy (CRT) for reaching a near pCR, then TEM were performed in patients with good response. The result of 55 patients showed CRT enables organ preservation with additional TEM surgery in approximately two-thirds of patients with good long-term oncological outcome in cT1-3N0M0 rectal cancer. In another prospective multi-institutional trial (40), patients with T2N0M0 rectal cancer were treated with neoadjuvant chemoradiotherapy followed by local excision, the result of 79 patients showed that 3-year disease-free survival and overall survival were 88 and 95%, respectively, suggesting that CRT followed by TLE could be considered as an organ-preserving alternative in selected patients with T2N0M0 rectal cancer. All these findings allow the possibility of saving the rectum by the treatment modality of TEM after neoadjuvant chemoradiotherapy in patients with T2N0M0 rectal cancer. However, many patients cannot accept the strategy of TEM after neoadjuvant chemoradiotherapy and were dying to receive surgical treatment as soon as possible. Additionally, chemoradiotherapy followed by TEM possibly led to a high incidence of complications and gave rise to cumulative toxicities that detract from the benefits of organ preservation (39–42). The strategy of TEM combined with post-operative radiotherapy should be further considered.
Due to the function of adjuvant radiotherapy in sterilizing subclinical mesorectal lymph nodes and the excision bed, the treatment strategy with TLE followed by radiotherapy may be a valid alternative to TME in T2N0M0 rectal cancer (43). In a mutilative analyses of 3,786 patients base on the SEER database (23), survival rates were analyzed between local excision (LE) alone, LE followed by radiotherapy and major resection (MR). The results suggested that the 5-year cancer specific survival rate and 5-year overall survival rate were significantly higher in MR group than those in LE alone group, but similar with those in LE followed by radiotherapy group. However, data is limited and only a few small retrospective studies have reported in this field. To date, there is no prospective randomized study to prove the feasibility of LE followed by radiotherapy in patients with T2N0M0 rectal cancer, further studies are needed in this field.
The trial compared the long-term efficacy of TEM followed by radiotherapy and TME for patients with T2N0M0 rectal cancer, which is the first prospective randomized study in the area. This study will provide strong evidence whether this rectum saving strategy for the treatment of rectal cancer is feasible.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University. The patients/participants provided their written informed consent to participate in this study.
YS, YF, and JT conceived and designed the initial project. The protocol was drafted by YZ, which was modified by DZ, CZ, KJ, DJ, and WP. All authors have read and approved the final study protocol.
The authors appreciate the help of all participants that are taking part in the study and the support by Jiangsu Provincial social development key project (BE2021742). Jiangsu Provincial Natural Science Foundation for Basic Research (Grant No. BK20201491), Jiangsu Key Medical Discipline (General Surgery, Grant No. ZDxKA2016005), and the National Key R&D Program of China (Grant No. 2017YFC0908200).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Erratum: global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2020) 70:313. doi: 10.3322/caac.21609
2. Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. (2016) 66:115–32. doi: 10.3322/caac.21338
3. Hamstra DA, Stenmark MH, Ritter T, Litzenberg D, Jackson W, Johnson S, et al. Age and comorbid illness are associated with late rectal toxicity following dose-escalated radiation therapy for prostate cancer. Int J Radiat Oncol Biol Phys. (2013) 85:1246–53. doi: 10.1016/j.ijrobp.2012.10.042
4. Heald RJ. The 'Holy Plane' of rectal surgery. J R Soc Med. (1988) 81:503–8. doi: 10.1177/014107688808100904
5. Knol J, Keller DS. Total mesorectal excision technique-past, present, and future. Clin Colon Rectal Surg. (2020) 33:134–43. doi: 10.1055/s-0039-3402776
6. Salomonsson M, Skott O, Persson AE. Lack of effect of intraluminal pressure on renin release from isolated afferent arterioles. Pflugers Arch. (1992) 421:466–8. doi: 10.1007/BF00370257
7. Ross A, Rusnak C, Weinerman B, Kuechler P, Hayashi A, MacLachlan G, et al. Recurrence and survival after surgical management of rectal cancer. Am J Surg. (1999) 177:392–5. doi: 10.1016/S0002-9610(99)00080-X
8. Hill GL, Rafique M. Extrafascial excision of the rectum for rectal cancer. Br J Surg. (1998) 85:809–12. doi: 10.1046/j.1365-2168.1998.00735.x
9. Bjerkeset T, Edna TH. Rectal cancer: the influence of type of operation on local recurrence and survival. Eur J Surg. (1996) 162:643–8.
10. Gopall J, Shen XF, Cheng Y. Current status of laparoscopic total mesorectal excision. Am J Surg. (2012) 203:230–41. doi: 10.1016/j.amjsurg.2011.03.011
11. Keating JP Sexual function after rectal excision. ANZ J Surg. (2004) 74:248–259. doi: 10.1111/j.1445-2197.2004.02954.x
12. Kim SH, Park IJ, Joh YG, Hahn KY. Laparoscopic resection for rectal cancer: a prospective analysis of thirty-month follow-up outcomes in 312 patients. Surg Endosc. (2006) 20:1197–202. doi: 10.1007/s00464-005-0599-2
13. Park JS, Choi GS, Kim SH, Kim HR, Kim NK, Lee KY, et al. Multicenter analysis of risk factors for anastomotic leakage after laparoscopic rectal cancer excision: the Korean laparoscopic colorectal surgery study group. Ann Surg. (2013) 257:665–71. doi: 10.1097/SLA.0b013e31827b8ed9
14. Buess G, Hutterer F, Theiss J, Bobel M, Isselhard W, Pichlmaier H. [A system for a transanal endoscopic rectum operation]. Chirurg. (1984) 55:677–80.
15. Lartigau C, Lebreton G, Alves A. Local resection for small rectal cancer. J Visc Surg. (2013) 150:325–31. doi: 10.1016/j.jviscsurg.2013.08.004
16. Althumairi AA, Gearhart SL. Local excision for early rectal cancer: transanal endoscopic microsurgery and beyond. J Gastrointest Oncol. (2015) 6:296–306. doi: 10.3978/j.issn.2078-6891.2015.022
17. Smart CJ, Cunningham C, Bach SP. Transanal endoscopic microsurgery. Best Pract Res Clin Gastroenterol. (2014) 28:143–57. doi: 10.1016/j.bpg.2013.11.005
18. Hashiguchi Y, Muro K, Saito Y, Ito Y, Ajioka Y, Hamaguchi T, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int J Clin Oncol. (2020) 25:1–42. doi: 10.1007/s10147-019-01485-z
19. Ramsey S, Tepper JE. Rectal cancer radiotherapy. Cancer J. (2007) 13:204–9. doi: 10.1097/PPO.0b013e318074def2
20. Tiefenbacher U, Wenz F. [Pre-operative radiotherapy combined with total mesorectal excision for resectable rectal cancer]. Strahlenther Onkol. (2001) 177:682–4. doi: 10.1056/NEJMoa010580
21. Jones HJS, Goodbrand S, Hompes R, Mortensen N, Cunningham C. Radiotherapy after local excision of rectal cancer may offer reduced local recurrence rates. Colorectal Dis. (2019) 21:451–9. doi: 10.1111/codi.14546
22. Sasaki T, Ito Y, Ohue M, Kanemitsu Y, Kobatake T, Ito M, et al. Post-operative chemoradiotherapy after local resection for high-risk T1 to T2 low rectal cancer: results of a single-arm, multi-institutional, phase II clinical trial. Dis Colon Rectum. (2017) 60:914–21. doi: 10.1097/DCR.0000000000000870
23. Wang XJ, Chi P, Zhang YY, Lin HM, Lu XR, Huang Y, et al. Survival outcome of adjuvant radiotherapy after local excision for T2 early rectal cancer: an analysis based on the surveillance, epidemiology, and end result registry database. Eur J Surg Oncol. (2018) 44:1865–72. doi: 10.1016/j.ejso.2018.08.024
24. Delibegovic S. Introduction to total mesorectal excision. Med Arch. (2017) 71:434–8. doi: 10.5455/medarh.2017.71.434-438
25. Clancy C, Burke JP, Albert MR, O'Connell PR, Winter DC. Transanal endoscopic microsurgery versus standard transanal excision for the removal of rectal neoplasms: a systematic review and meta-analysis. Dis Colon Rectum. (2015) 58:254–61. doi: 10.1097/DCR.0000000000000309
26. Lezoche G, Guerrieri M, Baldarelli M, Paganini AM, D'Ambrosio G, Campagnacci R, et al. Transanal endoscopic microsurgery for 135 patients with small nonadvanced low rectal cancer (iT1-iT2, iN0): short- and long-term results. Surg Endosc. (2011) 25:1222–9. doi: 10.1007/s00464-010-1347-9
27. Lezoche E, Baldarelli M, De Sanctis A, Lezoche G, Guerrieri M. Early rectal cancer: definition and management. Dig Dis. (2007) 25:76–9. doi: 10.1159/000099173
28. Elmessiry MM, Van Koughnett JA, Maya A, DaSilva G, Wexner SD, Bejarano P, et al. Local excision of T1 and T2 rectal cancer: proceed with caution. Colorectal Dis. (2014) 16:703–9. doi: 10.1111/codi.12657
29. De Graaf EJ, Doornebosch PG, Tollenaar RA, Meershoek-Klein Kranenbarg E, de Boer AC, Bekkering FC, et al. Transanal endoscopic microsurgery versus total mesorectal excision of T1 rectal adenocarcinomas with curative intention. Eur J Surg Oncol. (2009) 35:1280–5. doi: 10.1016/j.ejso.2009.05.001
30. Willett CG, Compton CC, Shellito PC, Efird JT. Selection factors for local excision or abdominoperineal resection of early stage rectal cancer. Cancer. (1994) 73:2716–20.
31. You YN, Baxter NN, Stewart A, Nelson H. Is the increasing rate of local excision for stage I rectal cancer in the United States justified?: a nationwide cohort study from the National Cancer Database. Ann Surg. (2007) 245:726–33. doi: 10.1097/01.sla.0000252590.95116.4f
32. Veereman G, Vlayen J, Robays J, Fairon N, Stordeur S, Rolfo C, et al. Systematic review and meta-analysis of local resection or transanal endoscopic microsurgery versus radical resection in stage i rectal cancer: a real standard? Crit Rev Oncol Hematol. (2017) 114:43–52. doi: 10.1016/j.critrevonc.2017.03.008
33. Chiniah M, Ganganah O, Cheng Y, Sah SK. Transanal endoscopic microsurgery is an oncologically safe alternative to total mesorectal excision for stage I rectal cancer: results of a meta-analysis of randomized controlled trials. Int J Colorectal Dis. (2016) 31:1501–4. doi: 10.1007/s00384-016-2530-9
34. Stornes T, Wibe A, Nesbakken A, Myklebust TA, Endreseth BH. National early rectal cancer treatment revisited. Dis Colon Rectum. (2016) 59:623–9. doi: 10.1097/DCR.0000000000000591
35. Perez RO, Habr-Gama A, Lynn PB, Sao Juliao GP, Bianchi R, Proscurshim I, et al. Transanal endoscopic microsurgery for residual rectal cancer (ypT0-2) following neoadjuvant chemoradiation therapy: another word of caution. Dis Colon Rectum. (2013) 56:6–13. doi: 10.1097/DCR.0b013e318273f56f
36. Allaix ME, Arezzo A, Giraudo G, Morino M. Transanal endoscopic microsurgery vs. laparoscopic total mesorectal excision for T2N0 rectal cancer. J Gastrointest Surg. (2012) 16:2280–7. doi: 10.1007/s11605-012-2046-8
37. Lezoche E, Baldarelli M, Lezoche G, Paganini AM, Gesuita R, Guerrieri M. Randomized clinical trial of endoluminal locoregional resection versus laparoscopic total mesorectal excision for T2 rectal cancer after neoadjuvant therapy. Br J Surg. (2012) 99:1211–8. doi: 10.1002/bjs.8821
38. Bokkerink GM, de Graaf EJ, Punt CJ, Nagtegaal ID, Rutten H, Nuyttens JJ, et al. The CARTS study: chemoradiation therapy for rectal cancer in the distal rectum followed by organ-sparing transanal endoscopic microsurgery. BMC Surg. (2011) 11:34. doi: 10.1186/1471-2482-11-34
39. Stijns RCH, de Graaf EJR, Punt CJA, Nagtegaal ID, Nuyttens J, van Meerten E, et al. Long-term oncological and functional outcomes of chemoradiotherapy followed by organ-sparing transanal endoscopic microsurgery for distal rectal cancer: the CARTS study. JAMA Surg. (2019) 154:47–54. doi: 10.1001/jamasurg.2018.3752
40. Garcia-Aguilar J, Renfro LA, Chow OS, Shi Q, Carrero XW, Lynn PB, et al. Organ preservation for clinical T2N0 distal rectal cancer using neoadjuvant chemoradiotherapy and local excision (ACOSOG Z6041): results of an open-label, single-arm, multi-institutional, phase 2 trial. Lancet Oncol. (2015) 16:1537–46. doi: 10.1016/S1470-2045(15)00215-6
41. Arezzo A, Arolfo S, Allaix ME, Munoz F, Cassoni P, Monagheddu C, et al. Results of neoadjuvant short-course radiation therapy followed by transanal endoscopic microsurgery for t1-t2 n0 extraperitoneal rectal cancer. Int J Radiat Oncol Biol Phys. (2015) 92:299–306. doi: 10.1016/j.ijrobp.2015.01.024
42. Rullier E, Vendrely V, Asselineau J, Rouanet P, Tuech JJ, Valverde A, et al. Organ preservation with chemoradiotherapy plus local excision for rectal cancer: 5-year results of the GRECCAR 2 randomised trial. Lancet Gastroenterol Hepatol. (2020) 5:465–74. doi: 10.1016/S2468-1253(19)30410-8
Keywords: radiotherapy, total meso-rectal excision, T2N0M0, rectal cancer, transanal endoscopic microsurgery
Citation: Tang J, Zhang Y, Zhang D, Zhang C, Jin K, Ji D, Peng W, Feng Y and Sun Y (2022) Total Mesorectal Excision vs. Transanal Endoscopic Microsurgery Followed by Radiotherapy for T2N0M0 Distal Rectal Cancer: A Multicenter Randomized Trial. Front. Surg. 9:812343. doi: 10.3389/fsurg.2022.812343
Received: 10 November 2021; Accepted: 10 January 2022;
Published: 01 February 2022.
Edited by:
Ren Zhao, Shanghai Jiao Tong University, ChinaReviewed by:
Dario D'Antonio, ASL Napoli 2 Nord, ItalyCopyright © 2022 Tang, Zhang, Zhang, Zhang, Jin, Ji, Peng, Feng and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yueming Sun, c3VueXVlbWluZ0Buam11LmVkdS5jbg==; Yifei Feng, ZmVuZ3lpZmVpMTk4MkAxNjMuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.