 Cristina Batalla-Salgado1
Cristina Batalla-Salgado1 Javier Ferrer-Torregrosa2*
Javier Ferrer-Torregrosa2* Francisco Muñoz-Piqueras3
Francisco Muñoz-Piqueras3 Miguel Muñoz Bautista3
Miguel Muñoz Bautista3 Carlos Barrios4
Carlos Barrios4
- 1Doctorate School, Valencia Catholic University “San Vicente Mártir”, Valencia, Spain
- 2Podiatry Department, School of Medicine and Health Sciences, Valencia Catholic University “San Vicente Mártir”, Valencia, Spain
- 3Surgery Unit of Piqueras Clinic, Madrid, Spain
- 4Institute for Research on Musculoskeletal Disorders, School of Medicine and Health Sciences, Valencia Catholic University “San Vicente Mártir”, Valencia, Spain
Objective: To compare bone healing time in osteotomies performed in claw toes correction through minimal invasive surgery in diabetic vs. non-diabetic patients. The relation between the patient's ages and the American Orthopedic Foot and Ankle Surgery Society (AOFAS) functional scores before and after surgery was also analyze in the two types of patients.
Method: A series of 45 women, 23 of them suffering from Diabetes Mellitus, were operated to correct claw toes. The surgery was always performed through minimal invasive digital osteotomies. After the intervention, bone healing was controlled by a fluoroscopic weekly follow-up until a complete bone consolidation was reached. Bone healing time was compared in in two groups of patients, diabetic and non-diabetic. All patients were evaluated with AOFAS scale 48 h before and 90 days after the intervention.
Results: The time of bone healing ranged from 24 to 40 days after the surgery and took shorter time of consolidation in non-diabetic patients although the Mann Withney U test did not show statistically significant differences (p = 0,409, effect size (ES) = 0,14 [-0.20 to 0.45]) between both groups. A statistically significant association (r = 0.71, R2 = 50%, p < 0.001) was found between the healing days and the day of medical discharge, also between the ages of the patients and the medial discharge (r = 0.36, R2 = 13%, p < 0.001). However, no statistically significant associations were found between pre-intervention glycemia and days of bone consolidation, neither in medical discharge (r = 0.07, p = 0.646 y r = 0.07, p = 0.648, respectively). AOFAS test scores and the diabetes status showed statistically significant differences, both in the main effect of Diabetes (F[1,41] = 9.41, p = 0.004) as in the interaction between diabetes and age (F[1,41] = 9.17, p = 0.004).
Conclusions: The bone healing time in claw toes operated through minimal invasive osteotomy surgery is not influenced by the presence of diabetes. The consolidation speed and the improvement in AOFAS functional scale score post-surgery in diabetic and elder patients was related to duration of the medical discharge.
Introduction
The prevalence rate of diabetes mellitus (DM) is growing every day according to World Health Organization (WHO) reports (1) and the International Diabetes Federation (2). Since the end of the last century, the number of people with DM has doubled, reaching more than 463 million people last year, with type 2 diabetic patients representing 90% of those with the disease. This fact could reflect a significant lack of control of healthy lifestyle habits such as diet and/or smoking habits (3). On the other hand, epidemiological evidence has shown that the prevalence of this disease will increase up to 700 million people by 2045 (4), as a result, hospital burden resulting from DM treatments can rise steeply.
Particularly, the diabetic foot is one of the most serious DM conditions, with non-traumatic amputation of the limb being one of the major complications (5). A recent meta-analysis conducted by Sen et al. (6), with more than 1,800 patients, showed that male sex, smoking, history of amputation and history of osteomyelitis were the variables most associated with amputation in patients with diabetic foot infections. Therefore, it is important to analyze how to prevent severe complications with both resolutive and prophylactic treatments. In this sense, arthropathies linked to vasculopathy in the diabetic foot are triggers of potential amputations, so that the correction of the former benefits its preservation (7, 8). Among these arthropathies affecting the forefoot, digital deformities (i.e., claw, hammer, and mallet toe) and deformities of the first radius (i.e., hallux valgus) are the most common (9). An investigation leaded by Ababneh et al. (10) with 1,000 patients showed that foot deformities in patients showed that more than 17% had hallux valgus whilst 16% had claw or hammer toes.
Previous studies have shown that osteotomies can help as a treatment to relieve plantar pressures generated by anatomical deformities (11–14), flexor tenotomies for digital alterations (15), as well as gastrocnemius lengthening to unload excessive metatarsal and digital area load (16).
Other studies have described deleterious effects of diabetic hyperglycemia on bone tissue quality (17), for example fragility or energy absorption (18), changes in trabecular volume and thickness (19) as well as mechanical properties (20) in addition to variants in the properties of collagen, minerals, and AGEs (advanced glycation products) (20, 21). The accumulation of these diabetic exposure changes in bone cell activity could impair consolidation and long-term progenitor cell potential and may create vascular deficiencies at the fracture site (22). These effects could be comparable to those caused by aging on bone structural integrity (23). The sum of histological changes that the bone undergoes suggests standardized histomorphometry evaluations by means of radiographic images that allow the assessment of its evolution (24) and the relationship between different groups of patients.
It is important to keep in mind the functional assessment of patients after surgery. In this sense, the American Orthopedic Foot, and Ankle Surgery Society (AOFAS) questionnaire is usually the most used to measure the functional assessment of patients. The score ranges from 0 to 100 depending on the degree of limitation of the patient. A score close to 0 is evidence of poor function, while scores close to 100 show improved foot and ankle function (24, 25).
Given the importance of ulcer prevention in patients with DM and the high incidence of non-traumatic amputations of the foot (26), rapid action by means of an osteotomy to correct claw toes could help to avoid the outcome of amputation (27). However, scientific studies comparing variables such as consolidation time in DM patients are scarce. Therefore, this study aimed to compare the bone consolidation time of osteotomies performed for claw toe correction by minimally invasive surgery in diabetic patients compared to non-diabetic patients. On the other hand, the second objective of the present investigation was to analyze the relationship between patient age and functional scores (i.e., AOFAS) after surgery regarding the patient condition (i.e., diabetic vs. non-diabetic). We hypothesize that the time to consolidation in patients with diabetes (previous normal glucose levels) will be similar compared to patients without diabetes. On the other hand, older diabetic patients will have greater perceived improvement in functionality scores.
Material and methods
Participants
Consecutive subjects with a diagnosis of claw toes presenting to a Surgery Unit of Piqueras Clinic, Madrid, Spain. from January 2021 to January 2022 were screened for inclusion in this study. Finally, a total of 49 participants were recruited for this descriptive-correlational study. The mean and standard deviation (SD) of age was 70 ± 9.28 years. From the total sample size, 51.15% (n = 23) were diabetic (see Table 1). The eligibility criteria of the present study were, inclusion criteria: a) patient with central claw toes, b) > 50 years and c) women. On the other hand, the exclusion criteria were a) previous foot surgeries (i.e., hallux valgus surgery, hallux rigidus, metatarsal osteotomies, digital osteotomies, exostectomies, tenotomies, capsulotomies), and b) uncontrolled blood sugar levels (i.e., fasting plasma glucose <80 to 130 < mg/dl). All participants were informed about the risks and benefits of participating in the investigation. Subsequently, they signed an informed consent. The study was authorized by the Research Ethics Committee of the Universidad Católica de Valencia San Vicente Mártir (Ref. UCV/2029–2020/159).
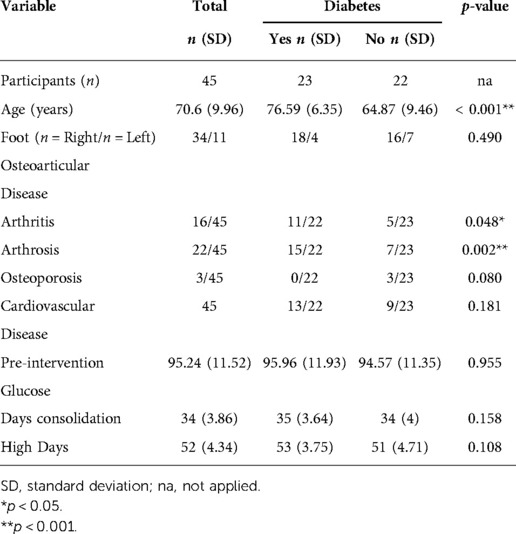
Table 1. Participants characteristics included in the present study.
Procedure
Prior to surgery, each patient underwent an initial anamnesis according to age, sex, smoker or non-smoker, pathologic status (i.e., diabetic and/or non-diabetic), glycemic value, osteoarticular diseases and cardiovascular alterations and peripheral vascular evaluation with Doppler and sphygmomanometer. Femoral, Popliteal, Posterior Tibial and Pedial pulses were measured, moreover to the Radial pulse for the calculation of the Ankle-Brachial Index (ABI). No alterations were observed in the pulses or ABI; all participants had normal values of 0.9 and 1, so the risk of peripheral vascular disease in the participants was minimal with perfect diabetic control in these patients.
In addition, an assessment of their metatarsophalangeal status by AOFAS scale (28, 29) and pain intensity with a visual analogue scale (VAS) was done (30). The AOFAS clinical scale system allows the assessment of 3 main dimensions: pain (i.e., mild, moderate, and severe), function (i.e., divided into six subscales) and foot alignment (i.e., good, fair, or poor). Previous research has shown the validity and adequate reliability of the AOFAS questionnaire (31, 32). The AOFAS clinical evaluation system was administered 48 h before surgery and 90 days after surgery.
Surgical procedure
All patients underwent plantar base osteotomy at the base of the proximal phalanx and dorsal base osteotomy at the middle phalanx, described by Dr. Isham, both by MIS (33–35) (Figure 1 and Figure 2). In some cases, soft tissue release through tenotomies was necessary according to accepted guidelines (35). All procedures were performed under regional anesthesia (Mepivacacia 2% and Bupivacaine 0.5%) of the operated limb by the same surgeon. Finally, a bandage was made to control the osteotomies and the correct alignment of the digits by means of Hypafix® (see Figure 3).
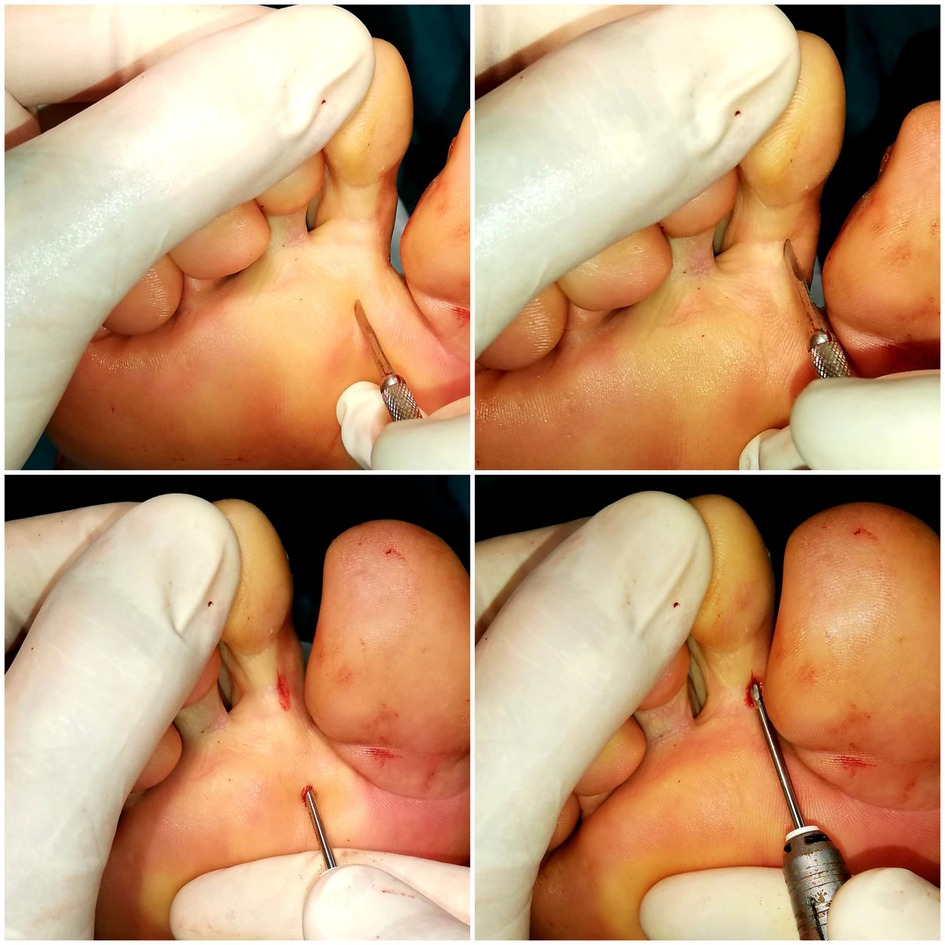
Figure 1. Surgical procedure for the correction of claw toe with osteotomy at the base of the phalanx and claw toe.
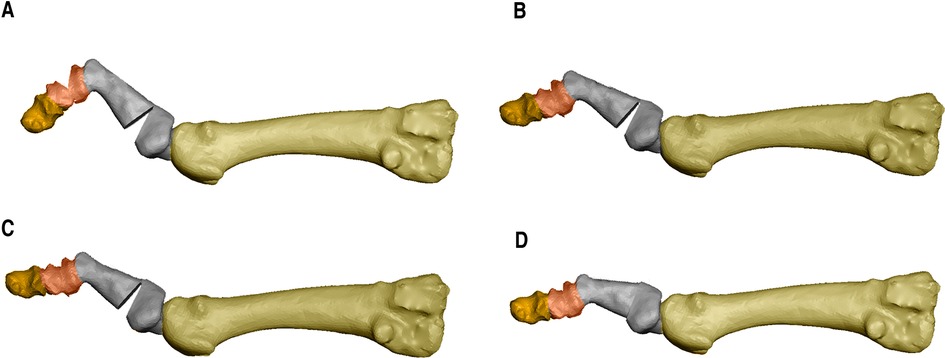
Figure 2. (A) design of a double osteotomy of the proximal phalanx at proximal and distal level and an osteotomy of the middle phalanx in case of claw toe; (B) closing of the middle phalanx osteotomy; (C) closing of the distal osteotomy of the proximal phalanx; (D) closing of the proximal osteotomy of the first phalanx with complete reduction of the deformity.

Figure 3. Post-surgical dressing, weekly change.
Post-surgical control
All the surgeries were successfully performed. Each patient who underwent surgery was able to walk immediately after the surgery with the post-surgical shoe (Herbitas ® surgical shoe model, valid for right/left foot) with a flat non-slip sole and Velcro fastening. The first revision by the surgeon took place 48 h after each operation. Each revision had a thorough fluoroscopic control. The patients were supervised on a weekly basis. Bone consolidation was assessed based on the Montoya Scale for post diaphyseal fracture bone callus formation (36, 37), whilst the fluoroscope was used to monitor the evolution of the osteotomies until complete consolidation and recovery of the finger was obtained. The degree of consolidation was classified as grade I mild consolidation, grade II and III moderate consolidation and grade IV total consolidation.
Statistical analysis
All variables were expressed as a mean and SD. The normality assumption (i.e., Kormogorov-Smirnov test) and homogeneity of variances (i.e., Levene's test) were analyzed. Generally, whenever both assumptions were met, an independent samples t-test was performed. If either assumption was not met, the nonparametric version (i.e., Mann-Withney U) was performed. The effect size (ES) was calculated using Cohen's formulas, considering an ES < 0.19 trivial, 0.20–0.49 small, 0.50–0.79 moderate and > 0.80 large (18). The relationships between variables were performed using Pearson's or Spearman's correlation coefficient, in case of non-normality, The level of statistical significance was set at p < 0.05. All analyses were performed using the statistical analysis software JASP (The Netherlands).
Results
Of the forty-nine (n = 49) participants with potential to be evaluated in this study, finally forty-five (n = 45) patients were recruited. Four participants were excluding due to no meet the inclusion criteria “c”. Therefore, a total of twenty-three participants (n = 23, 51%) were categorized as a diabetic condition, being twenty-two participants (n = 22, 49%) non-diabetics (see Figure 4).
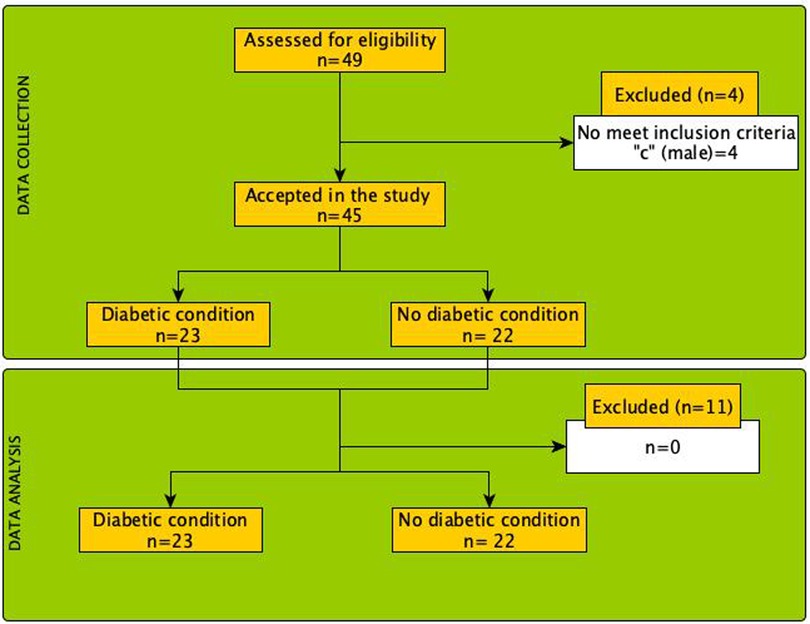
Figure 4. Flow diagram of the process of selection and analysis of the patients included in the present study.
Although non-diabetic patients took less time to complete bone consolidation (range between 24 and 40 days) after the intervention, the Mann-Withney U did not reveal statistically significant differences (p = 0.409, ES = 0.14 [-0.20 to 0.45]) in the comparison of consolidation time between patients with diabetes vs. non-diabetic patients. The mean and SD of consolidation time are summarized in Table 1.
On the other hand, a statistically significant relationship was found (r = 0.71, R2 = 50%, p < 0.001) between the period of bone consolidation and days of discharge, as well as age and days of discharge (r = 0.36, R2 = 13%, p < 0.001). However, no statistically significant relationships were found between pre-intervention glycemia scores and days to consolidation, nor discharge (r = 0.07, p = 0.646 and r = 0.07, p = 0.648, respectively).
Finally, ANCOVA of the percentage improvement in AOFAS test scores and diabetes status (i.e., diabetic vs. non-diabetic) showed statistically significant differences, both in the main effect of diabetes (F[1,41] = 9.41, p = 0.004) and in the diabetes × age interaction (F[1,41] = 9.17, p = 0.004). Figure 5 details the relationship between the percentage change in AOFAS scores and age.
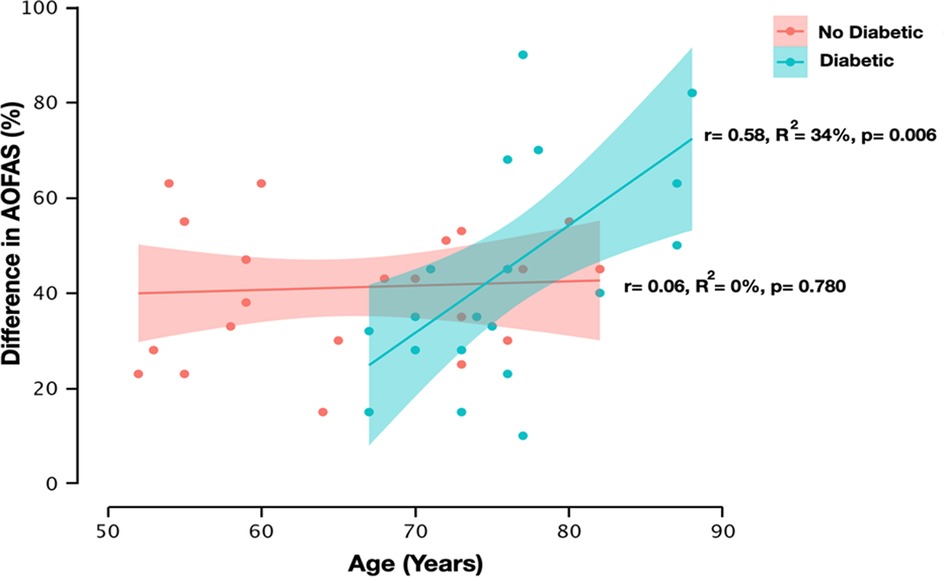
Figure 5. Relationship between American Orthopedic Foot and Ankle Surgery Society (AOFAS) test difference scores and age as a function of patients’ condition (i.e., diabetic vs. non-diabetic). The red dots reflect the AOFAS test difference scores in the non-diabetic condition, while the green dots reflect the AOFAS test difference scores in the diabetic condition. The shaded portion around the regression line reflects the 95% confidential interval. r = Pearson's correlation coefficient, R2 = coefficient of determination, p = p-value.
Discussion
The main objective of the present study was to describe and compare the bone consolidation time after osteotomy in diabetic vs. non-diabetic patients. The main finding of this study was that, regardless of the diabetic condition, the consolidation time was similar between both groups, showing no statistically significant differences and trivial effect size. The glycemia of the two groups was similar, being the group with diabetes a low-risk group, and for this reason we cannot determine the delay in consolidation as other studies have done (22).
On the other hand, a small but statistically significant relationship between patient age and discharge time was observed. Similarly, a statistically significant relationship was found between consolidation time and discharge days. Finally, it could be observed that as a function of diabetes status, the degree of functionality and age correlated in a statistically significant way in diabetic patients. The findings of this study provide evidence in favor of deformity correction the younger the patient and the better the metabolic control.
Nowadays, there are no specific classifications on the consolidation of osteotomies in intervened claw toes, what is described is the process of consolidation of bone fractures in general, based on scales already described for the formation of bone callus (36). In the absence of these classifications, Gerstenfeld et al. (24) carried out a review of histomorphometry methods in osteogenic processes in which they emphasized the need to study the bone repair process in detail to establish standardized criteria for evaluations that would serve to create a universal classification that would also detail observational tools for precise radiographic measurements (24).
Previous studies have shown that the evolution of fractures describes the existence of complications in the consolidation period related to smoking or age (37) although, loss of bone minerals or diabetes highly influence the process. The most recent evidence (18, 20, 22, 38) have pointed out that the bone tissue of diabetic patients presents loss of collagen (21), a high percentage of AGE advanced glycation products and a worse quality of trabecular bone which could compromise, in addition, its mechanical properties (20, 39). Our results showed that bone consolidation time was similar between diabetic and non-diabetic patients (see Table 1), achieving a solid and effective consolidation in both groups. Interestingly, these findings could suggest that correct glycemic control as well as good choice of surgical technique could favor the results of interventions in all types of patients, including those with type 2 DM.
Recently, foot minimally invasive surgery has gained popularity in DM patients (40, 41). The scarcity of scarring or tissue damage, the low number of complications (33, 42) as well as the absence of osteosynthesis reduce the number of infections while could favor the recovery time (13, 43). Several studies have pointed out that, given the existence of these techniques (i.e., minimally invasive), surgical interventions in diabetic patients should not be extended to the threat of loss of parts or tissues, since they could be used preventively (13, 44). Postponing interventions, especially in patients who have presented ulcers or suffer from reulcerations, could increase the risk of non-union of osteotomies. For example, a study leaded by Tamir et al. (43) showed that 6 months after surgery some patients failed to unite, although this lack of bone callus formation was asymptomatic. In 2003, Armstrong and Frykberg (45), published a study mainly aimed to classify diabetic foot surgery performed in the absence of critical limb ischemia considering three variables: the presence or absence of neuropathy, ulceration, and/or acute infection with risk of limb loss. The objective was to classify surgery based on the increasing order of amputation from I to IV. Our proposal in this study is related to class I or elective surgery, which includes those procedures performed to treat a painful deformity without loss of protective sensibility and class II, prophylactic surgery, formed by procedures performed to reduce the risk of ulceration (45).
The osteotomies performed for the correction of claw toes in patients operated in this study required weekly monitoring, not only for fluoroscopic assessment of the bony evolution, but also for the change of the post-surgical dressing. In this regard, percutaneous techniques require delicate management of the dressing. Previous studies have shown that the meticulousness of the dressing benefits the correct alignment of the fingers in the absence of osteosynthesis (33, 42). The compression of these bandages and their traction favor the formation of bone and fibrous tissue based on Roux's Law, which relates bone remodeling to the adaptive process of cells influenced by local stresses in the area. This application, which avoids osteosynthesis, also avoids infections that are sometimes triggered by metal fixations (13) and the final consolidation time does not vary between their use or not; while in the present case no infections have developed and total consolidation without osteosynthesis has been 4 to 6 weeks, other findings point to the removal of kirschner wires at 4 to 5 weeks (46).
There are several limitations to this study that should be keep in mind when interpret the findings. First, although no differences were found regarding bone consolidation time between diabetics and non-diabetic patients, we only included a sample of females' patients. Further studies including both sexes are necessary. In addition, the sample was carefully biased so that all patients in the study had tightly controlled glucose levels, including those of diabetic patients, so that the conditions between the two groups were as similar as possible for assessing the influence of balanced pathology.
Conclusions
The bone healing time of claw toes operated by osteotomies using the minimal incision technique is almost similar between diabetic (controlled) and non-diabetic patients. In both type of patients, the length of discharge was statistically related to the days of consolidation: the faster the consolidation, the shorter the days of medical discharge. Finally, the degree of functionality after the operation correlated statistically significantly with age, only for DM patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by UCV Ethics Committee (Ref.UCV/2029-2020/159. The patients/participants provided their written informed consent to participate in this study.
Author contributions
CBS, FMP, and MMB performed the surgeries JFT, and CB analyzed and interpreted the data. JFT and CB contributed to the study concept and design and participated in the figure designs. CBS collected and analyzed the data. CBS and JFT and CB contributed to the study concept, design, and interpretation of data. CBS, JFT, FMP, MMB and CB participated in the study design and statistical analysis and were major contributors in writing the manuscript. All authors read, discussed, and approved the final manuscript. The authors declare that this article represents an honest work. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. GLOBAL REPORT ON DIABETES WHO Library Cataloguing-in-Publication Data Global report on diabetes. (2016) http://www.who.int/about/licensing/copyright_form/index.html (Accessed May 17, 2022).
2. IDF Diabetes Atlas 10th edition. www.diabetesatlas.org (Accessed May 17, 2022).
3. Sarwar N, Gao P, Kondapally Seshasai SR, Gobin R, Kaptoge S, di Angelantonio E, et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. (2010) 375:2215–22. doi: 10.1016/S0140-6736(10)60484-9
4. Standl E, Khunti K, Hansen TB, Schnell O. The global epidemics of diabetes in the 21st century: current situation and perspectives. Eur J Prev Cardiol. (2019) 26:7–14. doi: 10.1177/2047487319881021
5. Uysal S, Arda B, Taşbakan MI, Çetinkalp Ş, Şimşir IY, Öztürk AM, et al. Risk factors for amputation in patients with diabetic foot infection: a prospective study. Int Wound J. (2017) 14:1219–24. doi: 10.1111/iwj.12788
6. Sen P, Demirdal T, Emir B. Meta-analysis of risk factors for amputation in diabetic foot infections. Diabetes Metab Res Rev. (2019) 35. doi: 10.1002/DMRR.3165
7. Khan N, Sapsed S. Diabetes foot complication: assessing primary and secondary outcomes of multidisciplinary team versus standard care (a systematic review). Int J Diabetes Dev Ctries. (2017) 37:129–36. doi: 10.1007/s13410-015-0422-0
8. Dewi F, Hinchliffe RJ. Foot complications in patients with diabetes. Surg (United Kingdom). (2020) 38:108–13. doi: 10.1016/j.mpsur.2019.12.002
9. Shirzad K, Kiesau CD, DeOrio JK, Parekh SG. Lesser toe deformities. J Am Acad Orthop Surg. (2011) 19:505–14. doi: 10.5435/00124635-201108000-00006
10. Ababneh A, Bakri FG, Khader Y, Lazzarini P, Ajlouni K. Prevalence and associates of foot feformities among patients with diabetes in Jordan. Curr Diabetes Rev. (2019) 16:471–82. doi: 10.2174/1573399815666191001101910
11. Chiu WK, Yang TF, Wang HJ, Chen C. Assessment of outcomes of a metatarsal bone ostectomy for chronic plantar ulcers: a preliminary study. Ann Plast Surg. (2020) 84:S112–5. doi: 10.1097/SAP.0000000000002174
12. Tamir E, Tamar M, Ayalon M, Koren S, Shohat N, Finestone AS. Effect of Mini-invasive floating metatarsal osteotomy on plantar pressure in patients with diabetic plantar metatarsal head ulcers. Foot Ankle Int. (2021) 42:536–43. doi: 10.1177/1071100720976099
13. Biz C, Ruggieri P. Minimally invasive surgery: osteotomies for diabetic foot disease. Foot Ankle Clin. (2020) 25:441–60. doi: 10.1016/j.fcl.2020.05.006
14. Yammine K, Nahed M, Assi C. Metatarsal osteotomies for treating neuropathic diabetic foot ulcers: a meta-analysis. Foot Ankle Spec. (2019) 12:555–62. doi: 10.1177/1938640018819784
15. Tamir E, Vigler M, Avisar E, Finestone AS. Percutaneous tenotomy for the treatment of diabetic toe ulcers. Foot Ankle Int. (2014) 35:38–43. doi: 10.1177/1071100713509604
16. Lazzarini PA, Jarl G, Gooday C, Viswanathan V, Caravaggi CF, Armstrong DG, et al. Effectiveness of offloading interventions to heal foot ulcers in persons with diabetes: a systematic review. Diabetes Metab Res Rev. (2020) 36. doi: 10.1002/dmrr.3275
17. Cunha JS, Ferreira VM, Maquigussa E, Naves MA, Boim MA. Effects of high glucose and high insulin concentrations on osteoblast function in vitro. Cell Tissue Res. (2014) 358:249–56. doi: 10.1007/S00441-014-1913-X
18. Sihota P, Yadav RN, Dhaliwal R, Bose JC, Dhiman V, Neradi D, et al. Investigation of mechanical, material, and compositional determinants of human trabecular bone quality in type 2 diabetes. J Clin Endocrinol Metab. (2021) 106:e2271–e2289. doi: 10.1210/clinem/dgab027
19. Ho-Pham LT, Nguyen Tv. Association between trabecular bone score and type 2 diabetes: a quantitative update of evidence. Osteoporos Int. (2019) 30:2079–85. doi: 10.1007/S00198-019-05053-Z
20. Giner M, Miranda C, Vázquez-Gámez MA, Altea-Manzano P, Miranda MJ, Casado-Díaz A, et al. Microstructural and strength changes in trabecular bone in elderly patients with type 2 diabetes Mellitus. Diagnostic. (2021) 11:577. doi: 10.3390/DIAGNOSTICS11030577
21. Schwartz Av. Impact of diabetes and its treatment on bone. Clin Rev Bone Miner Metab. (2009) 7:249–60. doi: 10.1007/s12018-009-9049-3
22. Murray CE, Coleman CM. Impact of diabetes Mellitus on bone health. Int J Mol Sci. (2019) 20:4873. doi: 10.3390/IJMS20194873
23. Fleischli JG, Laughlin TJ, Lavery LA, Shah B, Lanctot D, Agrawal CM, et al. The effects of diabetes mellitus on the material properties of human metatarsal bones. J Foot and Ankle Surg. (1998) 37:195–8. doi: 10.1016/S1067-2516(98)80110-5
24. Gerstenfeld LC, Wronski TJ, Hollinger JO, Einhorn TA. Application of histomorphometric methods to the study of bone repair. J Bone Miner Res. (2005) 20:1715–22. doi: 10.1359/JBMR.050702
25. Jansen H, Jordan M, Frey S, Hölscher-Doht S, Meffert R, Heintel T. Active controlled motion in early rehabilitation improves outcome after ankle fractures: a randomized controlled trial. Clin Rehabil. (2018) 32:312–8. doi: 10.1177/0269215517724192
26. Rodrigues BT, Vangaveti VN, Urkude R, Biros E, Malabu UH. Prevalence and risk factors of lower limb amputations in patients with diabetic foot ulcers: a systematic review and meta-analysis. Diabetes & Metab Syndr: Clin Res & Rev. (2022) 16:102397. doi: 10.1016/J.DSX.2022.102397
27. Yammine K, Assi C. Surgical offloading techniques should be used more often and earlier in treating forefoot diabetic ulcers: an evidence-based review. Int J Low Extrem Wounds. (2020) 19:112–9. doi: 10.1177/1534734619888361
28. Ibrahim T, Beiri A, Azzabi M, Best AJ, Taylor GJ, Menon DK. Reliability and validity of the subjective component of the American orthopaedic foot and ankle society clinical rating scales. J Foot and Ankle Surg. (2007) 46:65–74. doi: 10.1053/j.jfas.2006.12.002
29. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. (1994) 15:349–53. doi: 10.1177/107110079401500701
30. Carlsson AM. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain. (1983) 16:87–101. doi: 10.1016/0304-3959(83)90088-X
31. Piat C, Raboudi T, Cazeau C, Stiglitz Y. Postoperative hallux Varus treatment by reverse scarf osteotomy. Foot Ankle Int. (2021) 42. doi: 10.1177/10711007211001027
32. Goh GS, Tay AYW, Rikhraj IS, Koo K. Defining the patient acceptable symptom state for the American orthopaedic foot & ankle society score following hallux valgus surgery. Foot Ankle Surg. (2021) 27. doi: 10.1016/j.fas.2020.06.013
33. Nieto-García E, Ferrer-Torregrosa J, Ramírez-Andrés L, Nieto-González E, Martinez-Nova A, Barrios C. The impact of associated tenotomies on the outcome of incomplete phalangeal osteotomies for lesser toe deformities. J Orthop Surg Res. (2019) 14. doi: 10.1186/s13018-019-1353-0
34. Frey S, Hélix-Giordanino M, Piclet-Legré B. Percutaneous correction of second toe proximal deformity: proximal interphalangeal release, flexor digitorum brevis tenotomy and proximal phalanx osteotomy. Orthop and Traumatol: Surg and Res. (2015) 101:753–8. doi: 10.1016/j.otsr.2015.06.009
35. Cordier G, Nunes GA. Minimally invasive advances: lesser toes deformities. Foot Ankle Clin. (2020) 25:461–78. doi: 10.1016/j.fcl.2020.05.008
36. Calderón Garcidueñas J, Castillo Carranza MJ, Pavón Salas D, Mireles Díaz JA, González Gutiérrez R. Fracturas con retardo en la consolidación ósea o pseudoartrosis: tratamiento no invasivo con electroestimulación galvánica transcutánea. Acta Ortop Mex. (2001) 15:262–5.
37. Zak L, Arnhold R, Tiefenboeck TM, Wozasek GE. The influence of advanced age in bone healing after intramedullary limb lengthening. Orthop and Traumatol: Surg and Res. (2021) 107. doi: 10.1016/j.otsr.2021.103055
38. Lekkala S, Taylor EA, Hunt HB, Donnelly E. Effects of diabetes on bone material properties. Curr Osteoporos Rep. (2019) 17:455–64. doi: 10.1007/S11914-019-00538-6
39. Samelson EJ, Demissie S, Cupples LA, Zhang X, Xu H, Liu CT, et al. Diabetes and deficits in cortical bone density, microarchitecture, and bone size: framingham HR-pQCT study. J Bone Miner Res. (2018) 33:54–62. doi: 10.1002/jbmr.3240
40. Biz C, Gastaldo S, Dalmau-Pastor M, Corradin M, Volpin A, Ruggieri P. Minimally invasive distal metatarsal diaphyseal osteotomy (DMDO) for chronic plantar diabetic foot ulcers. Foot Ankle Int. (2018) 39:83–92. doi: 10.1177/1071100717735640
41. Mehlhorn AT, Harrasser N, Walther M. Treatment of plantar, neuropathic and metatarsal ulcers by minimally invasive metatarsal osteotomy. Orthopade. (2020) 49:625–31. doi: 10.1007/s00132-019-03848-w
42. Naranjo-Ruiz C, Martínez-Nova A, Canel-Pérez M de los Á, López-Vigil M, Ferrer-Torregrosa J, Barrios C. Influence of foot type on the clinical outcome of minimally invasive surgery for metatarsalgia. A prospective pilot study. Front Surg. (2021) 8:1–9. doi: 10.3389/fsurg.2021.748330
43. Tamir E, Finestone AS, Avisar E, Agar G. Mini-Invasive floating metatarsal osteotomy for resistant or recurrent neuropathic plantar metatarsal head ulcers. J Orthop Surg Res. (2016) 11. doi: 10.1186/s13018-016-0414-x
44. Ahluwalia R, Maffulli N, Lázaro-Martínez JL, Kirketerp-Møller K, Reichert I. Diabetic foot off loading and ulcer remission: exploring surgical off-loading. Surgeon. (2021) 19(6):526–35. doi: 10.1016/j.surge.2021.01.005
45. Armstrong DG, Frykberg RG. Classifying diabetic foot surgery: toward a rational definition. Diabetic Med. (2003) 20:329–31. doi: 10.1046/j.1464-5491.2003.00933.x
Keywords: claw toe, minimally invasive surgery, diabetic patients, bone consolidation, AOFAS scale
Citation: Batalla-Salgado C, Ferrer-Torregrosa J, Muñoz-Piqueras F, Muñoz Bautista M and Barrios C (2022) Comparative analysis of bone consolidation chronology in claw toes operated through minimal invasive osteotomies in diabetic vs. non-diabetic patients. Front. Surg. 9:1027094. doi: 10.3389/fsurg.2022.1027094
Received: 24 August 2022; Accepted: 24 November 2022;
Published: 12 December 2022.
Edited by:
Jaimo Ahn, University of Michigan, United StatesReviewed by:
A Federico Palomar Llatas, Hospital General Universitario De Valencia, SpainAlmudena Cecilia Matilla, Ramón y Cajal University Hospital, Spain
Raquel Sánchez-Rodríguez, University of Extremadura, Spain
© 2022 Batalla-Salgado, Ferrer-Torregrosa, Muñoz-Piqueras, Muñoz Bautista and Barrios. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Javier Ferrer Torregrosa amF2aWVyLmZlcnJlckB1Y3YuZXM=
Specialty section: This article was submitted to Orthopedic Surgery, a section of the journal Frontiers in Surgery