 Jun Yu1
Jun Yu1 Peng Zhu
Peng Zhu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 13 January 2023
Sec. Surgical Oncology
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.1027034
This article is part of the Research Topic 365 Days of Progress In Surgical Oncology View all 16 articles
Backgroud: The high or low inferior mesenteric artery (IMA) ligation in rectal cancer remains a great debate. This study retrospectively discussed the outcomes of the perioperative period, defecation and urinary function and long-term prognosis in rectal cancer patients with high or low IMA ligation.
Methods: This study enrolled 220 consecutive rectal cancer cases, including 134 with high IMA ligation and 86 with low ligation. A comparison between the two groups was made for anastomotic leakage, low anterior resection syndrome (LARS), international prostate symptom score (IPSS), 5-year disease-free survival (DFS) and 5-year overall survival (OS).
Results: Low-ligation group had a longer operative time, and larger intraoperative blood loss. No significant difference was noted in anastomotic leakage incidence. In multivariable analysis, the male gender and tumor located at the lower rectum were identified as risk factors for anastomotic leakage. No significant differences were observed between groups in their LARS and IPSS questionnaire responses. The high-ligation vs. the low-ligation 5-year OS and DFS were 78.3% vs. 82.4% and 72.4% vs. 76.6%, respectively, which were not statistically different.
Conclusion: The ligation level of the IMA had no significant effect on the anastomotic leakage incidence, defecation, urinary function, and long-term prognosis.
Currently, the incidence and mortality attributed to colorectal cancer both rank third, with patients becoming younger in average age (1). Surgical treatment is the mainstay for rectal cancer, amongst which low anterior resections are most valued. In domestic practice and overseas, there remains debate about the position of the inferior mesenteric artery (IMA) ligation during surgery (2–5). High ligation refers to a ligation located 1 to 2 cm away from the abdominal aorta origin, without the left colic artery preservation. In contrast, low ligation refers to a ligation at the left colic artery region, with dissection of the lymph nodes at IMA root and preservation of the left colic artery (6–9). Some scholars supported the use of high ligation mainly for two reasons: on the one hand, high ligation allows a sufficient length of the proximal free colon, which ensures a situation free of tension for colonic anastomosis; on the other hand, high ligation raises the lymph node yield, and improves the precision of disease staging, in the way of allowing lymph nodes dissection at IMA root to the maximum (10–13). However, according to some scholars, high ligation is at the cost of abandoning proximal colonic blood perfusion and declining anastomotic blood supply, which might increase the incidence of anastomotic leakage and lead to colon necrosis due to ischemia in severe cases (14–17). Researchers have not yet discovered if high ligation contributes to a higher lymph node yield in rectal resections, while it shows no superiority to low ligation regarding long-term oncologic prognosis (8, 18, 19).
In addition, high ligation with complete lymph node IMA root dissection may damage the inferior epigastric plexus, which governs defecation, urination, and sexual function. The results are conflicting on the effect of IMA ligation level on defecation and urinary function (20, 21).
This study retrospectively discussed the outcomes of the perioperative period, defecation, urinary function, and long-term prognosis in rectal cancer patients who had a laparoscopic lower rectal anterior resection with high or low IMA ligation.
This retrospective study involved 220 participants treated with radical laparoscopic for rectal cancer in the Second Affiliated Hospital of Chongqing Medical University between January 2014 and May 2016. Inclusion criteria were (1) Distance between tumor edge and the anal verge ≤15 cm; (2) Preoperative colonoscopy confirmed rectal tumor, and the pathological tissue biopsy revealed adenocarcinoma; (3) Preoperative chest and abdomen computer tomography (CT) and pelvic MRI confirmed locally progressive tumor; (4) Intraoperative sigmoid-rectal end-to-end anastomosis with a double stapling apparatus. Exclusion criteria were (1) Stage IV carcinoma with distant or peritoneal metastases before or during operation; (2) Emergency patients complicated with bleeding, perforation, and intestinal obstruction; (3) Patients with Hartmann's or abdominoperineal resections; (4) Multiple colorectal cancers. The patient whose preoperative MRI suggested T3–4 or N+ was treated with concurrent radiotherapy and chemotherapy. The long course of preoperative radiotherapy consisted of 50.4 Gray in 25 to 28 fractions, five times per week, over five weeks. Oral 5-fluorouracil (Capecitabin, Xeloda®, 825 mg/m2/day, twice a day, five times a week, for five weeks) was administered in conjunction with a long course of radiotherapy. After concurrent chemoradiotherapy, surgery was performed six weeks later. The hospital ethics committee approved this research.
All surgeries were performed by five professors, each with 20 years of experience in gastrointestinal surgery, who decided on the ligation level of IMA according to the intraoperative situation and personal opinions. IMA was ligated 1 to 2 cm distant from the aorta origin, with clearance of lymph nodes at the root in the high-ligation cases. IMA was ligated in the lower part of the left colic artery following lymph node dissection at the root in the low-ligation cases. Following the sigmoid-rectal end-to-end anastomosis completion, one drainage tube was placed around the pelvic anastomosis and passed out through the abdominal wall. The surgeon decided the level of IMA ligation, whether to perform a preventive ileostomy, and whether to place an anal canal.
Training for bladder function was arranged by clamping the urinary catheter on day 2 after the operation, followed by removing the urinary catheter. The anal canal was removed on day 5. The abdominal drainage tube was removed on day 7 in case of the absence of anastomotic leakage. Ileostomy closure was arranged 1–3 months after the operation for patients with a preventive ileostomy.
The postoperative complications were categorized as per the Clavien-Dindo method. Mild and serious complications were determined if the Clavien-Dindo classification was ≤II or ≥III, respectively (22). Anastomotic leak was defined as fecal flow through the abdominal drainage tube or signs of peritonitis, and the presence of an anastomotic leak was confirmed by abdominal CT. The anastomotic leak was graded following the International Study Group of Rectal Cancer grading: grade A, no special treatment required; grade B, active treatment required without reoperation; grade C, operative treatment (23). Postoperative tumor TNM pathological staging followed the American Joint Committee on Cancer (AJCC) 8th edition. An involved circumferential resection margin (CRM) was defined as ≤1 mm between the margin of deepest tumor infiltration and the surgical resection margin.
Stage I patients were followed up regularly, stage II patients received adjuvant oral 5-FU-based chemotherapy (capecitabine), and stage III patients received Xelox (capecitabine plus oxaliplatin).
Low anterior resection syndrone (LARS) score was utilized to assess bowel function. LARS scoring questionnaire, consisting of five questions about liquid stool and flatus incontinence, stools clustering, bowel frequency, and fecal urgency, was scored from 0 to 42. The patients were classified as no LARS, minor LARS, and major LARS when the score was 0–20, 21–29, and 30–42 points, respectively (24). The international prostate symptom score (IPSS) for urinary function consisted of seven items: urgency, frequency, nocturia, weak stream, intermittency, incomplete emptying, and straining (25). IPSS was classified as mild, moderate, or severe when the score was 0–7, 8–19, or 20–35, respectively. Prior to and at 6 and 12 months after surgery, the patients were given a questionnaire. At 6 and 12 months after ileostomy closure, patients with ileostomies completed questionnaires to assess bowel function.
After surgery, all patients were followed up every six months for the first three years and then annually for three to five years. Follow-up visits, conducted in the clinic and by telephone, included a physical examination, carcinoembryonic antigen measurement, CT of the chest and abdomen, colonoscopy, and completion of a questionnaire. If patients were found to suffer recurrent metastasis for the follow-up period, the location and point in time of recurrent metastasis were recorded. Patients with recurrent metastasis were reexamined every three months, assessing serum carcinoembryonic antigen and CT of the chest and abdomen.
The study statistical analyses were done using macOS IBM SPSS Statistics 26.0. Comparing categorical variables and continuous data among different groups was done via Chi-square or Fisher's exact tests. Relying on the distribution, the continuous data were evaluated with an independent t-test or Mann–Whitney U test. Univariate and multivariate logistic regression assessed the risk factors for anastomotic leakage. p < 0.100 variables were included in the multivariable analysis. The 5-year OS and DFS were analyzed by Kaplan-Meier curves, and, to verify the groups' significant differences, a log-rank test was done. p < 0.05 was regarded as statistically significant.
Table 1 shows all patients' baseline and clinical characteristics. No statistically significant differences were found between patients who were treated with high ligation and those who underwent low ligation for gender, age, ASA stage, BMI, tumor location, neoadjuvant chemoradiotherapy, history of abdominal surgery, diabetes, coronary heart disease, and hypertension between the two groups (p > 0.05).

Table 1. Patients’ baseline and clinical characteristics.
Table 2 shows the surgical outcomes and complications. The high ligation group had a shorter operation time than the low ligation group (184.6 ± 14.4 min vs. 190.7 ± 16.4 min, p = 0.004). Intraoperative blood loss in the high ligation group was significantly higher than in the low ligation group (91.2 ± 21.8 ml vs. 84.3 ± 24.5 ml, p = 0.037). No statistical differences were shown in conversion to open surgery, splenic flexure mobilization, preventive ileostomy, indwelling anal canal, time to first flatus, and hospital stay (p > 0.05). The incidence of postoperative complications in the high and low ligation groups was 25.4% and 20.9%, respectively, and no significant difference was observed (p = 0.449). The anastomotic leakage in the high and low ligation groups was 10.4% (14 patients) and 8.1% (7 patients), respectively, with no significant difference (p = 0.570). Reoperation occurred in the high and low ligation groups at 3.7% and 3.5%, respectively (p = 0.534). The 30-day after surgery mortality in the high and low ligation groups were two and one case, respectively, which was not significantly different.
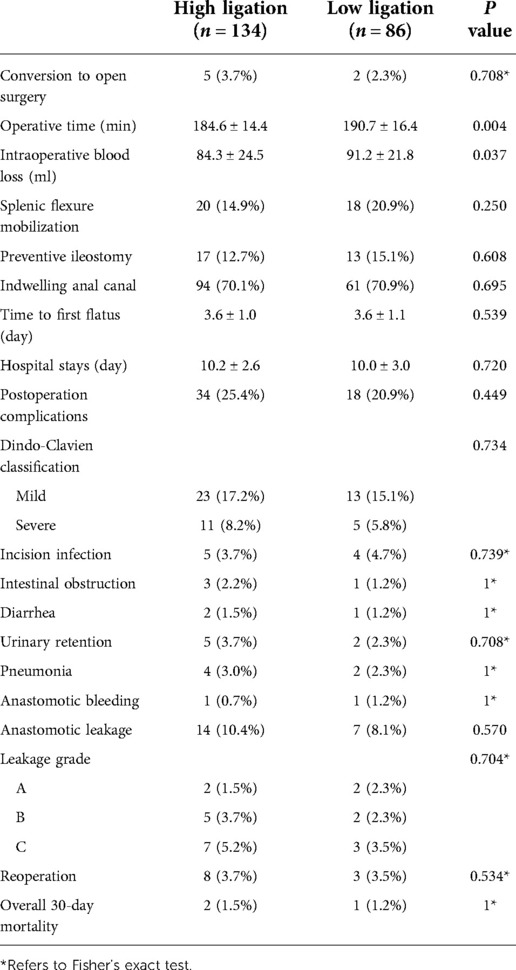
Table 2. Surgical data and postoperative complications.
The male gender, neoadjuvant therapy, and the lower rectum tumors were considerably related to anastomotic leakage incidence, as revealed by univariable analysis. The male gender and the lower rectum tumors were considered anastomotic leakage risk factors, as the multivariable analysis revealed (Table 3).
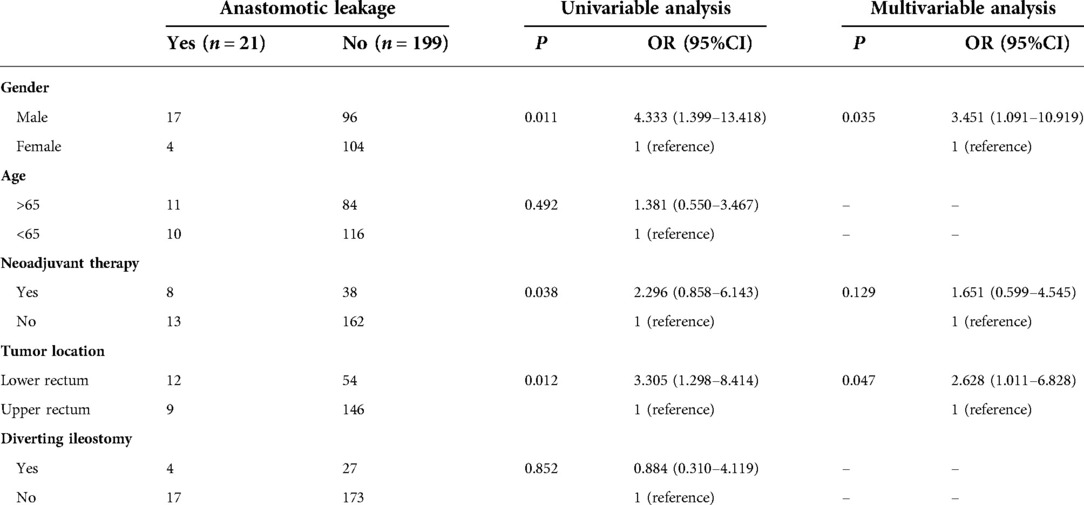
Table 3. Risk factors for anastomotic leakage.
Table 4 lists the pathological results summary. The tumor size, proximal margin, and distal margin were measured without differences between the two groups (p > 0.05). The number of lymph nodes harvested in the high and low ligation groups was 16.3 ± 2.8 and 15.5 ± 2.4, respectively (p = 0.053). No significant difference was observed between the two groups in the number of positive lymph nodes (p = 0.493). No statistical differences were identified between the two groups in CRM, neural invasion, vascular invasion, degree of differentiation, pN stage, pT stage, and pTNM stage (p > 0.05; Table 4).
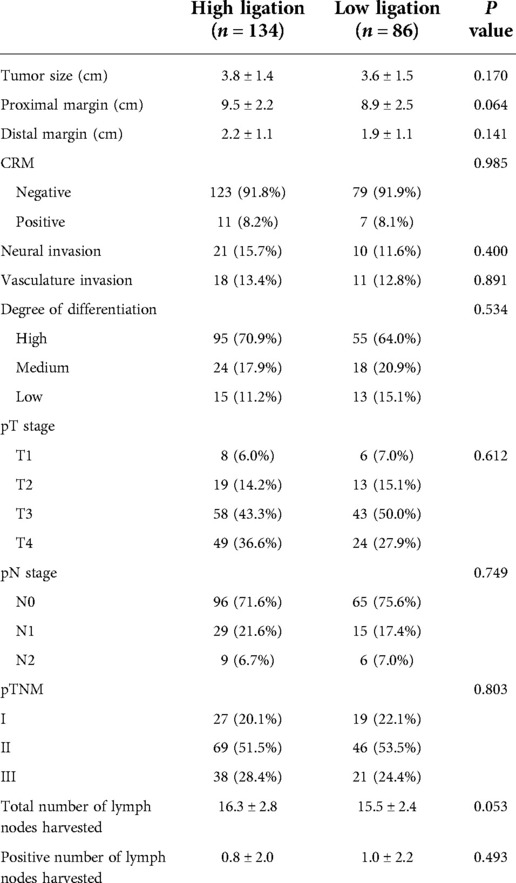
Table 4. Pathological data.
The functional outcomes of LARS and IPSS questionnaires are shown in Table 5. No significant differences were observed before surgery, or 6 and 12 months following surgery, in both LARS and IPSS questionnaire responses between groups.
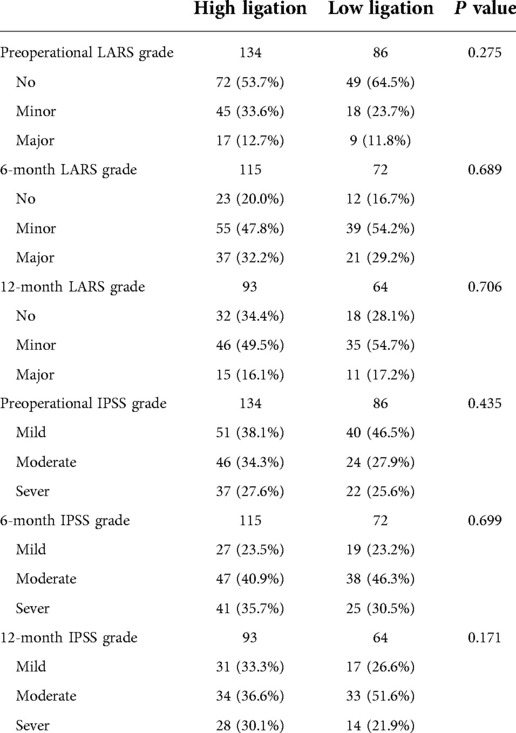
Table 5. Function outcomes of LARS and IPSS.
The follow-up rate at five-years was 90.5%, with 12 patients in the high ligation group and nine patients in the low ligation lost to follow-up. The occurrence of recurrent metastases in the high and low ligation groups was 26.5% vs. 22.4%, respectively, which was not statistically different (Table 6). The 5-year OS and DFS for the high and low ligation groups were 78.3% vs. 82.4% (p = 0.463), and 72.4% vs. 76.6% (p = 0.485), respectively, showing no statistical differences (Figures 1 and 2).
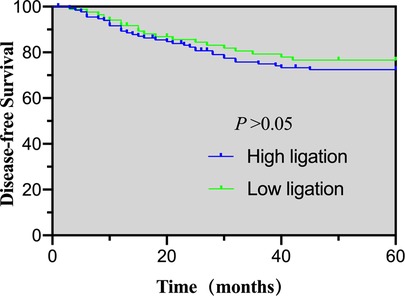
Figure 1. 5-year disease-free survival of the high- and low-ligation groups.
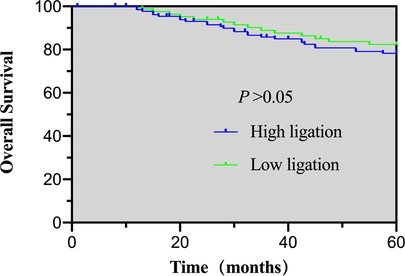
Figure 2. 5-year overall survival of the high- and low-ligation groups.
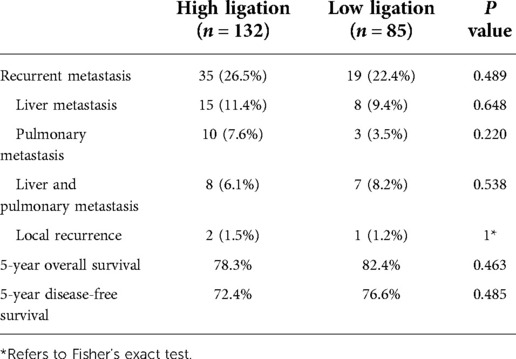
Table 6. Recurrent metastasis and long-time outcome.
This study discloses that low ligation increases operation time and intraoperative blood loss compared to high ligation. Furthermore, no significant difference was observed between the high and low ligation groups in anastomotic leakage. The male gender and lower rectum tumors are anastomotic leakage risk factors. No significant differences were observed between the groups in oncologic outcomes, such as 5-year OS and 5-year DFS, as well as functional outcomes, such as bowel and urine functions.
The study revealed that the low ligation group had a longer operative time (184.56 ± 14.4 vs. 190.7 ± 16.4, p = 0.004) and more intraoperative blood loss (84.3 ± 24.5 vs. 91.2 ± 21.8, p = 0.037). Given that low-ligation works by lymph node clearance at IMA root to expose the left colic artery, on the premise of IMA safety, it is harder to run and requires more experienced surgeons. A recent study found that whether the left colic artery is preserved or not was independent of the operative time and intra-operative blood loss (5). Similarly, some meta-analyses showed that the left colic artery preservation would not increase the operative time and intra-operative blood loss (26, 27). However, Park et al. (8) reported that the low-ligation strategy contributed to a shorter operative time but was not superior in decreasing intraoperative blood loss. The discrepancy might be associated with the operative experience of the surgeons.
Anastomotic leakage is a high-risk complication during low anterior rectal resections, leading to a longer hospital stay and higher medical costs, as well as increasing the ileostomy rate and mortality. In the current research, the anastomotic leakage incidence in the high and low ligation groups were 10.4% and 8.1%, respectively, which was not statistically significant, and the male gender and the lower rectum tumor were considered risk factors. Several studies showed that the anastomotic leakage incidence during low anterior rectal resections would not be increased when high-ligation was applied, and gender and the distance from the tumor to the anus were major factors causing anastomotic leakage after operation (28, 29). The level of IMA ligation does not correlate with anastomotic leakage and must be selected according to factors, including the presence or absence of tension anastomosis (30). Additionally, it has been suggested that anatomical variants of the left colic artery should be of concern, as insufficient vascularization of the proximal colonic conduit in the absence of the left colic artery is also an important factor in the occurrence of anastomotic leakage (31). However, anastomotic blood perfusion remains one of the important factors affecting anastomotic healing. Intraoperative colonic perfusion was measured using laser Doppler flowmetry and was found to be slightly decreased in the high ligation group and slightly increased in the low ligation group, independent of blood pressure (16). Seike et al. (15) reported that, after clamping the IMA, the anastomotic blood flow of the proximal colon was significantly reduced, which was more evident in elderly men, along with a higher risk of anastomotic leakage. Other studies also demonstrated that low ligation could decrease the anastomotic leakage risk (32–34). Therefore, larger samples are required to further explore the relationship between anastomotic leakage and IMA ligation level in the future.
Bowel and urinary function were poor after rectal cancer surgery. A Japanese randomized controlled trial reported no significant differences between patients with high and low ligation, assessed at three months and one year postoperatively, on defecatory function, fecal incontinence quality of life scale defaecation self-assessment, or continence score (9). Defecation function, related to levels of IMA ligation resulting in different blood supply to the anastomosis, is also related to other factors, such as the denervated neorectum motility, rectal compliance, anal sphincter, and anastomosis level. Although neither group returned to preoperative IPSS levels, there was an improvement in IPSS at nine months after low ligation compared to high ligation (20). Park (8) reported no difference in bowel and urinary function between the two groups before surgery, three months after surgery, and 12 months after surgery. Similarly, this research revealed no significant statistical difference in LARS and IPSS between high and low ligation in preoperative, six months postoperative, and 12 months postoperative. The difference may be related to autonomic nerve injury during IMA peripheral lymph node dissection in our surgery.
The number of lymph nodes dissected during operation is vital for operation assessment, guiding postoperative adjuvant chemoradiotherapy and prognosis. Patients with lymph node metastasis are more likely to have tumor recurrence and experience a shorter survival time compared to those without metastasis (35). Research revealed no evidence showing the benefits of high-ligation in long-term prognosis, although it could get more lymph nodes dissected (36). Many current studies have suggested that there were no more lymph nodes dissected by high-ligation, and still, no superiority was demonstrated in long-term prognosis compared to low-ligation (37–41). There were no statistical differences between the total number of lymph nodes dissected and the number of positive ones. Moreover, the 5-year OS and 5-year DFS showed no evident differences between the two groups.
Several limitations remain in this study. First, this is a retrospective study involving a small sample size from a single institute, requiring larger-scale, multi-center, and randomized controlled trials for further validation. Second, selection bias might not be ignored. Finally, sexual functions, such as the international index of erectile function (IIEF-5), and the female sexual function index (FSFI), were not assessed in this study.
The ligation level of IMA has no significant effect on the incidence of anastomotic leakage, defecation, urinary function, or long-term prognosis. However, larger randomized controlled trials are still required to further validate this result.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by YC and PZ. The first draft of the manuscript was written by JY. LT, CL and BS prepared Tables 1–6. ZZ and QY prepared Figures 1–2. JZ commented on previous versions of the manuscript. All authors contributed to the article and approved the submitted version.
The authors would like to thank all the gastroenterologists and patients who participated in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. (2021) 71:7–33. doi: 10.3322/caac.21654
2. Cirocchi R, Trastulli S, Farinella E, Desiderio J, Vettoretto N, Parisi A, et al. High tie versus low tie of the inferior mesenteric artery in colorectal cancer: a RCT is needed. Surg Oncol. (2012) 21:e111–123. doi: 10.1016/j.suronc.2012.04.004
3. Dimitriou N, Felekouras E, Karavokyros I, Pikoulis E, Vergadis C, Nonni A, et al. High versus low ligation of inferior mesenteric vessels in rectal cancer surgery: a retrospective cohort study. J Buon. (2018) 23:1350–61. PMID: 30570858
4. Fujii S, Ishibe A, Ota M, Suwa H, Watanabe J, Kunisaki C, et al. Short-term and long-term results of a randomized study comparing high tie and low tie inferior mesenteric artery ligation in laparoscopic rectal anterior resection: subanalysis of the HTLT (high tie vs. Low tie) study. Surg Endosc. (2019) 33:1100–10. doi: 10.1007/s00464-018-6363-1
5. Chen JN, Liu Z, Wang ZJ, Zhao FQ, Wei FZ, Mei SW, et al. Low ligation has a lower anastomotic leakage rate after rectal cancer surgery. World J Gastrointest Oncol. (2020) 12:632–41. doi: 10.4251/wjgo.v12.i6.632
6. Hajibandeh S, Hajibandeh S, Maw A. Meta-analysis and trial sequential analysis of randomized controlled trials comparing high and low ligation of the Inferior mesenteric artery in rectal cancer surgery. Dis Colon Rectum. (2020) 63:988–99. doi: 10.1097/dcr.0000000000001693
7. Guo Y, Wang D, He L, Zhang Y, Zhao S, Zhang L, et al. Marginal artery stump pressure in left colic artery-preserving rectal cancer surgery: a clinical trial. ANZ J Surg. (2017) 87:576–81. doi: 10.1111/ans.13032
8. Park SS, Park B, Park EY, Park SC, Kim MJ, Sohn DK, et al. Outcomes of high versus low ligation of the inferior mesenteric artery with lymph node dissection for distal sigmoid colon or rectal cancer. Surg Today. (2020) 50:560–8. doi: 10.1007/s00595-019-01942-2
9. Matsuda K, Hotta T, Takifuji K, Yokoyama S, Oku Y, Watanabe T, et al. Randomized clinical trial of defaecatory function after anterior resection for rectal cancer with high versus low ligation of the inferior mesenteric artery. Br J Surg. (2015) 102:501–8. doi: 10.1002/bjs.9739
10. Girard E, Trilling B, Rabattu PY, Sage PY, Taton N, Robert Y, et al. Level of inferior mesenteric artery ligation in low rectal cancer surgery: high tie preferred over low tie. Tech Coloproctol. (2019) 23:267–71. doi: 10.1007/s10151-019-01931-0
11. Bonnet S, Berger A, Hentati N, Abid B, Chevallier JM, Wind P, et al. High tie versus low tie vascular ligation of the inferior mesenteric artery in colorectal cancer surgery: impact on the gain in colon length and implications on the feasibility of anastomoses. Dis Colon Rectum. (2012) 55:515–21. doi: 10.1097/DCR.0b013e318246f1a2
12. Thum-umnuaysuk S, Boonyapibal A, Geng YY, Pattana-Arun J. Lengthening of the colon for low rectal anastomosis in a cadaveric study: how much can we gain? Tech Coloproctol. (2013) 17:377–81. doi: 10.1007/s10151-012-0930-6
13. Charan I, Kapoor A, Singhal MK, Jagawat N, Bhavsar D, Jain V, et al. High ligation of Inferior mesenteric artery in left colonic and rectal cancers: lymph node yield and survival benefit. Indian J Surg. (2015) 77:1103–8. doi: 10.1007/s12262-014-1179-2
14. Park MG, Hur H, Min BS, Lee KY, Kim NK. Colonic ischemia following surgery for sigmoid colon and rectal cancer: a study of 10 cases and a review of the literature. Int J Colorectal Dis. (2012) 27:671–5. doi: 10.1007/s00384-011-1372-8
15. Seike K, Koda K, Saito N, Oda K, Kosugi C, Shimizu K, et al. Laser Doppler assessment of the influence of division at the root of the inferior mesenteric artery on anastomotic blood flow in rectosigmoid cancer surgery. Int J Colorectal Dis. (2007) 22:689–97. doi: 10.1007/s00384-006-0221-7
16. Komen N, Slieker J, de Kort P, de Wilt JH, van der Harst E, Coene PP, et al. High tie versus low tie in rectal surgery: comparison of anastomotic perfusion. Int J Colorectal Dis. (2011) 26:1075–8. doi: 10.1007/s00384-011-1188-6
17. Sörelius K, Svensson J, Matthiessen P, Rutegård J, Rutegård M. A nationwide study on the incidence of mesenteric ischaemia after surgery for rectal cancer demonstrates an association with high arterial ligation. Colorectal Dis. (2019) 21:925–31. doi: 10.1111/codi.14674
18. Fiori E, Crocetti D, Lamazza A, Felice FD, Sterpetti AV, Irace L, et al. Is low Inferior mesenteric artery ligation worthwhile to prevent urinary and sexual dysfunction after total mesorectal excision for rectal cancer? Anticancer Res. (2020) 40:4223–8. doi: 10.21873/anticanres.14423
19. You X, Liu Q, Wu J, Wang Y, Huang C, Cao G, et al. High versus low ligation of inferior mesenteric artery during laparoscopic radical resection of rectal cancer: a retrospective cohort study. Medicine. (2020)) 99:e19437. doi: 10.1097/md.0000000000019437
20. Mari GM, Crippa J, Cocozza E, Berselli M, Livraghi L, Carzaniga P, et al. Low ligation of inferior mesenteric artery in laparoscopic anterior resection for rectal cancer reduces genitourinary dysfunction: results from a randomized controlled trial (HIGHLOW trial). Ann Surg. (2019) 269:1018–24. doi: 10.1097/sla.0000000000002947
21. Kverneng Hultberg D, Afshar AA, Rutegård J, Lange M, Haapamäki MM, Matthiessen P, et al. Level of vascular tie and its effect on functional outcome 2 years after anterior resection for rectal cancer. Colorectal Dis. (2017) 19:987–95. doi: 10.1111/codi.13745
22. Clavien P, Barkun J, de Oliveira M, Vauthey J, Dindo D, Schulick R, et al. The clavien-dindo classification of surgical complications: five-year experience. Ann Surg. (2009) 250:187–96. doi: 10.1097/SLA.0b013e3181b13ca2
23. Rahbari N, Weitz J, Hohenberger W, Heald R, Moran B, Ulrich A, et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: a proposal by the international study group of rectal cancer. Surgery. (2010) 147:339–51. doi: 10.1016/j.surg.2009.10.012
24. Emmertsen KJ, Laurberg S. Low anterior resection syndrome score: development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Ann Surg. (2012) 255:922–8. doi: 10.1097/SLA.0b013e31824f1c21
25. Barry MJ, Fowler FJ Jr., O’Leary M P, Bruskewitz RC, Holtgrewe HL, Mebust WK, et al. The American urological association symptom index for benign prostatic hyperplasia. J Urol. (2017) 197:S189–97. doi: 10.1016/j.juro.2016.10.071
26. Liu J, Gong Y, He M, Zeng X, Liu Y. Clinical effect of preservation or nonpreservation of left colic artery in total mesorectal excision under laparoscopy: a meta-analysis. Gastroenterol Res Pract. (2020) 2020:1958573. doi: 10.1155/2020/1958573
27. Fan YC, Ning FL, Zhang CD, Dai DQ. Preservation versus non-preservation of left colic artery in sigmoid and rectal cancer surgery: a meta-analysis. Int J Surg. (2018) 52:269–77. doi: 10.1016/j.ijsu.2018.02.054
28. Kong M, Chen H, Xin Y, Jiang Y, Han Y, Sheng H. High ligation of the inferior mesenteric artery and anastomotic leakage in anterior resection for rectal cancer: a systematic review and meta-analysis of randomized controlled trial studies. Colorectal Dis. (2021) 23:614–24. doi: 10.1111/codi.15419
29. Fujii S, Ishibe A, Ota M, Watanabe K, Watanabe J, Kunisaki C, et al. Randomized clinical trial of high versus low inferior mesenteric artery ligation during anterior resection for rectal cancer. BJS Open. (2018) 2:195–202. doi: 10.1002/bjs5.71
30. Draginov A, Chesney TR, Quereshy HA, Chadi SA, Quereshy FA. Association of high ligation versus low ligation of the inferior mesenteric artery on anastomotic leak, postoperative complications, and mortality after minimally invasive surgery for distal sigmoid and rectal cancer. Surg Endosc. (2020) 34:4593–600. doi: 10.1007/s00464-019-07203-0
31. Cirocchi R, Randolph J, Cheruiyot I, Davies JR, Wheeler J, Lancia M, et al. Systematic review and meta-analysis of the anatomical variants of the left colic artery. Colorectal Dis. (2020) 22:768–78. doi: 10.1111/codi.14891
32. Si MB, Yan PJ, Du ZY, Li LY, Tian HW, Jiang WJ, et al. Lymph node yield, survival benefit, and safety of high and low ligation of the inferior mesenteric artery in colorectal cancer surgery: a systematic review and meta-analysis. Int J Colorectal Dis. (2019) 34:947–62. doi: 10.1007/s00384-019-03291-5
33. Zeng J, Su G. High ligation of the inferior mesenteric artery during sigmoid colon and rectal cancer surgery increases the risk of anastomotic leakage: a meta-analysis. World J Surg Oncol. (2018) 16:157. doi: 10.1186/s12957-018-1458-7
34. Luo Y, Yu MH, Huang YZ, Jing R, Qin J, Qin SL, et al. Lymphadenectomy around inferior mesenteric artery in low-tie vs high-tie laparoscopic anterior resection: short- and long-term outcome of a cohort of 614 rectal cancers. Cancer Manag Res. (2021) 13:3963–71. doi: 10.2147/cmar.S282986
35. Zhao X, Ma J, Fu Z, Hong H, Zhang L, Xue P, et al. Prognostic value of apical lymph node metastasis at the inferior mesenteric artery in sigmoid and rectal cancer patients who undergo laparoscopic surgery. J Surg Oncol. (2021) 123(Suppl 1):S88–s94. doi: 10.1002/jso.26346
36. Titu LV, Tweedle E, Rooney PS. High tie of the inferior mesenteric artery in curative surgery for left colonic and rectal cancers: a systematic review. Dig Surg. (2008) 25:148–57. doi: 10.1159/000128172
37. Matsuda K, Yokoyama S, Hotta T, Takifuji K, Watanabe T, Tamura K, et al. Oncological outcomes following rectal cancer surgery with high or low ligation of the inferior mesenteric artery. Gastrointest Tumors. (2017) 4:45–52. doi: 10.1159/000477805
38. Nayeri M, Iskander O, Tabchouri N, Artus A, Michot N, Muller O, et al. Low tie compared to high tie vascular ligation of the inferior mesenteric artery in rectal cancer surgery decreases postoperative complications without affecting overall survival. Anticancer Res. (2019) 39:4363–70. doi: 10.21873/anticanres.13605
39. Yasuda K, Kawai K, Ishihara S, Murono K, Otani K, Nishikawa T, et al. Level of arterial ligation in sigmoid colon and rectal cancer surgery. World J Surg Oncol. (2016) 14:99. doi: 10.1186/s12957-016-0819-3
40. Zhang C, Chen L, Cui M, Xing J, Yang H, Yao Z, et al. Short- and long-term outcomes of rectal cancer patients with high or improved low ligation of the inferior mesenteric artery. Sci Rep. (2020) 10:15339. doi: 10.1038/s41598-020-72303-0
Keywords: rectal cancer, high ligation, low ligation, inferior mesenteric artery (IMA), anastomotic leakage (AL)
Citation: Yu J, Chen Y, Li T, Sheng B, Zhen Z, Liu C, Zhang J, Yan Q and Zhu P (2023) High and low inferior mesenteric artery ligation in laparoscopic low anterior rectal resections: A retrospective study. Front. Surg. 9:1027034. doi: 10.3389/fsurg.2022.1027034
Received: 24 August 2022; Accepted: 18 October 2022;
Published: 13 January 2023.
Edited by:
Francesco Giovinazzo, Agostino Gemelli University Polyclinic (IRCCS), ItalyReviewed by:
Cihangir Akyol, Ankara University School of Medicine, Turkey© 2023 Yu, Chen, Li, Sheng, Zhen, Liu, Zhang, Yan and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yi Chen Y2hlbnlpQGhvc3BpdGFsLmNxbXUuZWR1LmNu Peng Zhu enVwZW5nQGNxbXUuZWR1LmNu
Specialty Section: This article was submitted to Surgical Oncology, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.