 Ulrik Ørsø Andersen
Ulrik Ørsø Andersen Marie Røsland Rosenørn
Marie Røsland Rosenørn Preben Homøe
Preben Homøe- 1Department of Otorhinolaryngology and Maxillofacial Surgery, Zealand University Hospital, Køge, Denmark
- 2Department of Pathology, Zealand University Hospital, Roskilde, Denmark
Birt-Hogg-Dubé syndrome (BHD) is a rare inherited autosomal dominant condition caused by a mutation in the tumor suppressor gene FLCN. This mutation predisposes the carrier to multiple pulmonary cysts, recurrent pneumothorax, renal tumors and benign skin tumors. Since the first description of BHD, additional clinical signs have been added to the syndrome and a large variety of benign tumors, such as rhabdomyomas (RM), have been linked with the FLCN gene mutation. RMs are rare tumors derived from striated muscle. The adult extracardiac rhabdomyoma occurs mostly in elderly patients, with a male predominance. It is most often located in the head and neck area and it has a potential of recurrence. We report a case of recurrent multifocal ARM in the oral cavity, present in an elderly woman with BHD and treated surgically. This could add support to RMs being linked to BHD.
Introduction
Birt-Hogg-Dubé syndrome (BHD) is a rare inherited autosomal dominant condition caused by a mutation in the tumor suppressor gene FLCN. This condition predisposes to multiple pulmonary cysts, recurrent spontaneous pneumothorax, renal tumors and benign skin tumors. Since the first description of BHD, additional clinical signs have been added to the syndrome and a large variety of benign tumors, such as rhabdomyomas (RM), have been linked with the FLCN gene mutation (1). RMs are rare tumors derived from striated muscle and are topographically classified as cardiac or extracardiac. The adult extracardiac rhabdomyoma occurs mostly in elderly patients, with a male predominance. It is most often located in the head and neck area and it has a potential of recurrence (2). We report a case of recurrent multifocal ARM in the oral cavity, present in an elderly woman with BHD and treated surgically. This could add support to RMs being linked to BHD.
Case description and diagnostic assessment rhabdomyoma in BHD patient
An 87-year-old woman known with hypertension, wet macular degeneration, two episodes of pneumothorax (1978 and 1988) and previous excision of a rhabdomyoma in the sublingual region (2001, age 67 - the patient's medical record of this time is not available and further details or not available), had a femoral hernia surgery in 2015. During the intubation the anesthesiologist noticed an oropharyngeal tumor causing difficulties regarding the intubation. The patient was thereafter referred to the ENT department (See Figure 1 for timeline). She reported dysphagia but no other symptoms. At the examination a tumor of the basis of the left side of the tongue was seen covered with mucosa and without signs of malignancy. A magnetic resonance imaging (MRI) showed a homogenous tumor with contrast enhancement localized in the central tongue basis, with suspected growth into the surrounding tissue. The tumor was well-defined and was surgically removed in toto with free margins. Histologic examination showed a solid tumor composed of large tumor cells with eccentric located nuclei and cytoplasmic cross striations, consistent with RM.
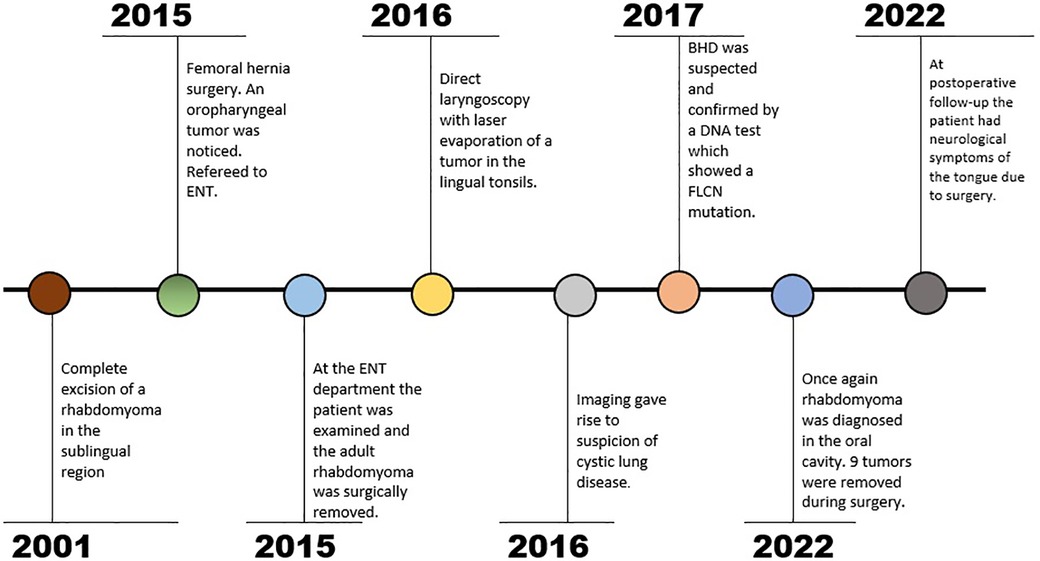
Figure 1. Text description: timeline.
At a clinical control a couple of months later another tumor was found at the left side of the base of tongue, again without ulcerations or any other signs of malignancy. The tumor was removed by direct laryngoscopy with laser evaporation. ARM was suspected but histology surprisingly showed tonsillar tissue without remaining components of RM. She was seen a month later with no symptoms and was completed from the ENT department.
Prior to the direct laryngoscopy a computed tomography (CT) thorax was performed due to suspicion of pneumothorax. The scan showed several pulmonal bullae and a high-resolution computed tomography (HRCT) gave suspicion of cystic lung disease. At this point her family three revealed a history of several cases of pneumothorax (grandmother, three aunts and two cousins). BHD was suspected and confirmed with a DNA test showing a pathologic mutation in FLCN gene (c.1285dup, NM_144997).
In early 2022 she was referred to the ENT department because of dysphagia and she had problems with speech due to a feeling of fullness in the bottom of her mouth. A large tumor was seen in the floor of mouth and another in the left side of the oropharynx. A fine needle aspiration from one of the tumors showed large, atypical cells resembling RM (See Figure 2H). MRI of the head and neck showed several tumors at the right side of the base of tongue and anteriorly at the base of tongue at the transition to the floor of mouth (see Figures 2A,B). Subsequently the tumors of the oral floor were completely excised but the tumor in oropharynx was not excised due to the lack of symptoms from this area (see Figure 3). During the surgery additional small tumors was discovered in the floor of mouth and as many as possible was surgically removed. At macroscopic examination the surface of the three largest tumors was alternately smooth and irregular (see Figures 2C,D). On histological examination the tumors showed solid growth of large tumor cells with abundant granular, eosinophilic and vacuolated cytoplasm and occasional cross striations (see Figures 2E–G). The histopathological diagnosis was RM with no sign of malignancy.

Figure 2. Text description: (A) MRI, T1, sagittal view. ARM marked with red circle. (B) MRI, T2, Axial view. ARM marked with red circle. (C,D) The specimen consisted of nine separate parts which had a diameter of 7 to 38 mm. The surface was well delineated and uniformly brown. The cut surface was solid and light brown with a few, small, darker areas. The surface of the largest tumors was stained blue before sectioning. (E,F) The growth pattern is solid and the tumor cells are large and polygonal with eccentric nuclei and abundant eosinophilic, granular and often vacuolated cytoplasm. The nuclei are rounded and uniform with light staining chromatin and a single nucleolus. Occasionally characteristic striations can be seen in the cytoplasm of the tumor cells. Stained with HE (Hematoxylin-Eosin). The scale bar is set at 100 µm. (G) The tumor cells show a strong cytoplasmic expression of Desmin by immunohistochemical staining, confirming the myogenic origin of the tumor. The scale bar is set at 100 µm. (H) The overall number of tumor cells in the specimen is sparse. The tumor cells are large (compared with adjacent erythrocytes) and have peripherally located nuclei with a single nucleolus and abundant, finely granular cytoplasm. Stained with MGG (Mey-Grünwald-Giemsa). The scale bar is set at 100 µm.
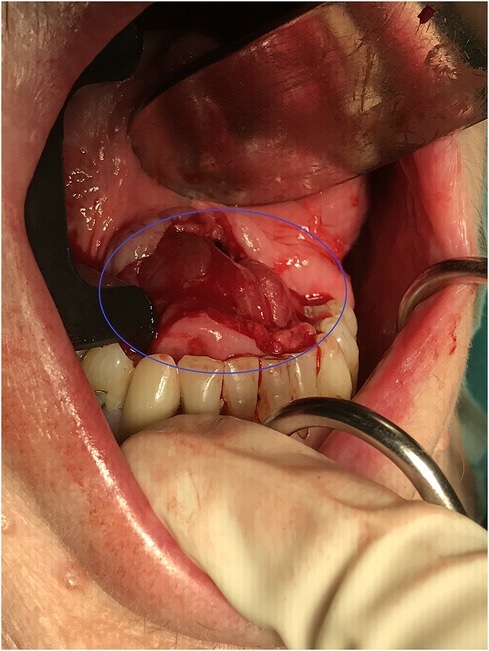
Figure 3. Text description: perioperative photos from the oral cavity showing an incision in the mucosa of the floor of mouth which gives direct contact with one of the RMs marked with a blue circle.
Follow up
After the first surgery in 2015 the patient had oral pain which disappeared after the direct laryngoscopy in 2016. In 2022, the patient had a postoperative infection of the floor of mouth treated with intravenous and per oral antibiotics. At a later clinical control, the patient had a lack of sensation of the right side of the tongue, altered sense of taste and the food tended to accumulate anteriorly in the mouth. She was later diagnosed with fibrofolliculomas at a dermatologist and due to BHD. The patient is currently being monitored with scans of the kidneys at a medical department, where no signs of tumors have been found so far.
Discussion
BHD is a very rare syndrome which is caused by an autosomal dominant mutation in the tumor suppressor gene FLCN. Patients with BHD are characterized by a wide phenotypic heterogeneity but most commonly presents with pulmonary cysts, recurrent pneumothorax, renal tumors and cutaneous tumors of the type fibrofolliculomas. Other clinical manifestations have been seen, such as different benign and malignant tumors, for example RM. It is still debated if they are a part of the syndrome (1). RMs are rare benign tumors which originate from striated muscle. They are classified as cardiac and extracardiac. The cardiac RM which mostly occurs in the heart of infants is usually linked to the tuberous sclerosis complex disease and has only once been reported one case of BHD (3). The extracardiac RM is subdivided into three types; adult, fetal and genital, of which the adult is the most frequent. ARM has a male predominance with and the median age is 65 years (2). They are mainly present in the head and neck region where the majority are located in the parapharyngeal space, larynx and the submandibular region. All of this fits with our case except from the gender (2). The most common clinical symptoms of ARM are globus sensation, hoarseness, a soft painless slow growing mass or dysphagia (2).
To determine the spatial localization of the tumor(s) CT and MRI are commonly used for imaging modalities. On MRI RM appears as isointense or hyperintense nodules with discrete enhancement upon gadolinium injection. On CT RM appears as an isodense tumor with discrete iodine contrast inhancement (2). The findings on MRI and CT are not specific for ARM and cannot be used in the diagnostics of RM but mostly to illuminate the anatomical relations. RM has a high uptake on F-FDG PET CT which could be used for anatomically localization of the RMs and to ensure complete removal of the multifocal RMs, but again the imaging modality is not specific for ARM (2). In our case the F-FDG PET CT could have predicted the large number of tumors and thereby potentially affected the planning of the surgery. For correct diagnosis a histologic examination is needed.
The standard treatment for ARM is surgical removal but with asymptomatic patients a watchfull waiting strategy is preferable when one has in mind that no previous malignant transformation of RM has been seen (2).
We conducted a Pubmed search on “rhabdomyoma and BHD syndrome (MESH terms)” and five cases occurred – see Table 1 (4–8). The localization of RMs in these case reports were the larynx, the paratracheal and paralaryngeal region, the heart, the sublingual and submandibular region – with a maximum of 3 tumors. Khalaf et al. illustrates that the localization varies a lot but is mainly within the head and neck area. In our search the mean age at presentation was 52 years – noted that one of the cases was a 5 years old child with a cardiac RM. The mean age of the cases with ARM was 61 years. The male to female ratio has been reported to be 13.5:1 but in our search the ratio was a 1:1 (2). This difference may be due to the small sample sizes.

Table 1. Table description: overview of the literature search.
Our BHD case is the first with a recurrent history of RMs and the first with such a high number of tumors. A reason for the recurrent incidence could be that RMs are multilobulated and is overlooked perioperatively as seen in this case where several additional tumors were found during surgery. Khalaf et al. report recurrence of RM up to 10 years after the primary surgery in three out of fifteen cases.
The causal association between RMs and BHD in humans has yet to be established. Studies conducted on mice with inactive BHD genes suggest that the FLCN mutation causes an altered activity of the mTOR cellular pathway which regulates cell proliferation, autophagy and apoptosis. The mice phenotypically developed cysts and renal tumors similar to those found in BHD patients (9–11). In the BHD case of Bajwa et al. D.NA analysis were performed on the RM and they found loss of heterozygosity (LOH) at the site of the patients FLCNs pathogenic variant. Studies have shown the occurrence of LOH at the BHD locus in sporadic kidney tumors and tumors from patients with germline FLCN mutations (12, 13). All together this indicates that the FLCN mutation in the BHD could play a role in the tumorgenesis of RMs.
Our case and several other cases have diagnosed ARM in patients with BHD, indicating a potential link of the two. Our case is, to our knowledge, the first published case of multifocal and recurrent ARM in a patient with BHD and this should be a differential diagnosis when finding several RM tumors in the head and neck region.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
Author contributions
UØA: General script, literature search, gathering information and making of the timeline and productions of figures. MRR: Provider of images of pathology, text description, specialist consulting, revisions. PH: Specialist consulting, rewriting and revisions, consent from the patient. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Daccord C, Good JM, Morren MA, Bonny O, Hohl D, Lazor R. Birt–Hogg–Dubé syndrome. Eur Respir Rev. (2020) 29:20042. doi: 10.1183/16000617.0042-2020
2. Khalaf MG, Haddad R, Akiki M, Khazen J, Melkane AE. Multifocal adult rhabdomyoma of the head and neck: case report and systematic review of the literature. Int J Oral Maxillofac Surg. (2021) 50:327–34. doi: 10.1016/j.ijom.2020.07.018
3. de Trey LA, Schmid S, Huber GF. Multifocal adult rhabdomyoma of the head and neck manifestation in 7 locations and review of the literature. Case Rep Otolaryngol. (2013) 2013:1–5. doi: 10.1155/2013/758416
4. Bajwa DS, Cook S, Winn R, Winship IM, McQueen A, Husain A, et al. Multifocal extracardiac rhabdomyomas: extending the phenotype of Birt–Hogg–Dubé syndrome. Brit J Dermatol. (2021) 185:861–3. doi: 10.1111/bjd.20521
5. Black M, Wei X, Sun W, Simms A, Negron R, Hagiwara M, et al. Adult rhabdomyoma presenting as thyroid nodule on fine-needle aspiration in patient with Birt-Hogg-Dubé syndrome: case report and literature review. Diagn Cytopathol. (2020) 48:576–80. doi: 10.1002/dc.24413
6. Balakumar R, Farr MRB, Fernando M, Jebreel A, Ray J, Sionis S. Adult-Type rhabdomyoma of the larynx in Birt–Hogg–Dubé syndrome: evidence for a real association. Head Neck Pathol. (2019) 13:507–11. doi: 10.1007/s12105-018-0922-6
7. Bondavalli D, White SM, Steer A, Pflaumer A, Winship I. Is cardiac rhabdomyoma a feature of Birt Hogg Dubé syndrome? Am J Med Genet A. (2015) 167:802–4. doi: 10.1002/ajmg.a.36917
8. Mikesell Kv, Kulaylat AN, Donaldson KJ, Saunders BD, Crist HS. A rare soft tissue tumor masquerading as a parathyroid adenoma in a patient with Birt-Hogg-Dubé syndrome and multiple cervical endocrinopathies. Case Rep Pathol. (2014) 2014:1–5. doi: 10.1155/2014/753694
9. Hartman TR, Nicolas E, Klein-Szanto A, Al-Saleem T, Cash TP, Simon MC, et al. The role of the Birt–Hogg–Dubé protein in mTOR activation and renal tumorigenesis. Oncogene. (2009) 28:1594–604. doi: 10.1038/onc.2009.14
10. Baba M, Furihata M, Hong SB, Tessarollo L, Haines DC, Southon E, et al. Kidney-targeted birt-hogg-dube gene inactivation in a mouse model: erk1/2 and akt-mTOR activation, cell hyperproliferation, and polycystic kidneys. J Natl Cancer Inst. (2008) 100:140–54. doi: 10.1093/jnci/djm288
11. Hudon V, Sabourin S, Dydensborg AB, Kottis V, Ghazi A, Paquet M, et al. Renal tumour suppressor function of the Birt-Hogg-Dube syndrome gene product folliculin. J Med Genet. (2010) 47:182–9. doi: 10.1136/jmg.2009.072009
12. Khoo SK, Kahnoski K, Sugimura J, Petillo D, Chen J, Shockley K, et al. Inactivation of BHD in sporadic renal tumors. Cancer Res. (2003) 63(15):4583–7. PMID: 12907635
Keywords: multifocal, recurrent, rhabdomyoma (MeSH), Birt-Hogg-Dubé (BHD), oral cavity
Citation: Andersen UØ, Rosenørn MR and Homøe P (2022) Recurrent multifocal adult rhabdomyoma in an elderly woman diagnosed with Birt-Hogg-Dubé syndrome: A case report. Front. Surg. 9:1017725. doi: 10.3389/fsurg.2022.1017725
Received: 12 August 2022; Accepted: 16 September 2022;
Published: 30 September 2022.
Edited by:
Jose Angelito Ugalde Hardillo, Erasmus Medical Center, NetherlandsReviewed by:
Laura Schmidt, National Cancer Institute at Frederick (NIH), United StatesJean Kanitakis, Hospices Civils de Lyon, France
© 2022 Andersen, Rosenørn and Homøe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ulrik Ørsø Andersen dWFuQHJlZ2lvbnNqYWVsbGFuZC5kaw==
†ORCID Preben Homøe orcid.org/0000-0003-2877-3518
Specialty Section: This article was submitted to Otorhinolaryngology - Head and Neck Surgery, a section of the journal Frontiers in Surgery