 Rosa M. Egea-Gámez1
Rosa M. Egea-Gámez1 María Galán-Olleros
María Galán-Olleros- 1Spine Unit. Orthopaedic Surgery and Traumatology Department, Niño Jesús University Children's Hospital, Madrid, Spain
- 2Orthopaedic Surgery and Traumatology Department, Infanta Elena University Hospital, Valdemoro, Spain
Background: Although osteosarcoma is the most common primary malignant bone tumor in children, its location in the axial skeleton is rare, particularly at the cervical spine. Early diagnosis, together with multidisciplinary management, improves survival rates. Safe resection and stable reconstruction are complicated by the particular anatomy of the cervical spine, which raises the risks.
Case Presentation: A 12-year-old male patient presented with cervical pain for several months and a recent weight loss of 3 kg. The complementary workup revealed a large destructive bone lesion in C7 with vertebral body collapse, subluxation, partial involvement of C6 and T1, large associated anteroposterior soft tissue components, and spinal canal narrowing. A biopsy suggested giant cell-rich osteosarcoma (GCRO). After 10 cycles of neoadjuvant chemotherapy, surgical resection was performed through a double approach: anterior, for tumoral mass resection from C6-7 vertebral bodies and reconstruction placing a mesh cage filled with iliac crest allograft plus anterior plate fixation; and posterior, for C7 complete and C6 partial posterior arch resection, thus completing a total piecemeal spondylectomy preserving the dura intact, added to a C5-T3 posterior fusion with screws and transitional rods. Postoperative chemo and radiotherapy were administered. Clinical and radiological follow-up showed disease-free survival and no neurological involvement at 3 years.
Conclusion: An extensive review of the literature did not find any published cases of GCRO of the cervical spine in pediatric patients. This can be explained by the combination of three peculiar conditions: its location at the cervical spine region, the young age, and the GCRO variant.
Introduction
Primary tumors of the spine are rare, representing between 2% and 8% of skeletal tumors, but should always be considered in the differential diagnosis of back symptoms in children. Within this age group, benign bone lesions such as osteoid osteoma and osteoblastoma prevail (1). Osteosarcoma is the most common primary malignant bone tumor in young patients, frequently arising in the limbs but only rarely in the axial skeleton (3%–5%) (2, 3). In this location, it is more prevalent in the lumbar spine and sacrum and quite infrequent in the cervical spine.
It is common for osteosarcomas of the spine to be initially misinterpreted as benign osteoblastomas since their clinical, radiological, and histopathological characteristics are difficult to differentiate (3, 4), thus, biopsy is essential to conduct a proper approach. Giant cell-rich osteosarcoma (GCRO) is considered an uncommon variant of osteosarcoma (5), representing only about 3% of them (6). This atypical variant is characterized by an abundance of osteoclastic giant cells and a paucity of osteoid tumor (7), leading it to be confused with giant cell tumors (8, 9). Infiltration of adjacent bony trabeculae, focal osteoid deposits, and a Ki67 proliferative index of 20%–30% have been reported to be useful for differentiation from giant cell tumors (8).
This study aims to present a young patient diagnosed with this rare variant of osteosarcoma of the cervical spine, the diagnostic sequence, and multidisciplinary treatment, with a focus on the surgical strategy for oncologic resection and cervical spine reconstruction. In addition, the literature on cervical spine osteosarcoma is reviewed along with a summary workup of the published cases of GCRO.
Case presentation
A 12-year-old male patient presented with cervical pain with onset several months before and no reported history of trauma or overuse. After a detailed anamnesis, the pain appeared to be both mechanical and inflammatory in nature, causing the interruption of sleep and achieving only slight relief with basic analgesia. The patient also reported a recent weight loss of 3 kg. On examination, his neck appeared tilted to the left side and the pain was localized posteriorly on his lower cervical spine, irradiating to the left arm. Spurling test was negative, with limited motion of the neck and tenderness of the paravertebral muscles bilaterally. Strength and sensitivity were preserved in both upper and lower limbs.
Simple anteroposterior and lateral radiographs of the cervical spine were taken on the initial visit (Figure 1). Further examination by Computerized Tomography (CT) and Magnetic Resonance Imaging (MRI) revealed a significant destructive bone lesion in C7, with vertebral body collapse, subluxation, partial destruction of the left lamina and spinous process and large associated anterior and posterior soft tissue components. The spinal canal was markedly narrowed at C6–C7, partly due to altered alignment and partly due to invasion by the tumor, obliterating the left posterolateral subarachnoid space (Figure 2). There was also partial involvement of the left pedicle, lamina, and spinous process of C6 and, to a lesser extent, the T1 left pedicle. The left vertebral artery was not visible, suggesting tumoral invasion and blockage which was later confirmed by CT angiography.

Figure 1. Anteroposterior and lateral radiographs of the cervical spine: (A) Osteolytic expansive lesion on C7 vertebral body, with ill-defined borders, expansion and interruption of the upper and lower endplate of the left half of the vertebral body and absent spinous process and left pedicle; also, abnormal cervical alignment in the frontal plane with a slight left-sided tilt of the neck is noted. (B) Enlargement of the posterior elements and upper endplate of C7 vertebral body, thinning of the cortical bone, without apparent interruption, periosteal reaction, or soft tissue mass.
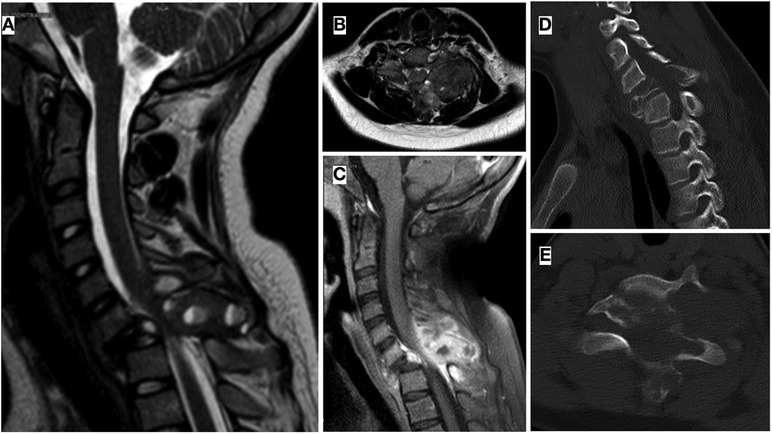
Figure 2. (A–C) Sagittal and axial MRI cuts of the cervical spine showing a multiloculated bone lesion in C7 that conditioned vertebral body collapse and subluxation, associated large soft tissue component, with intradural and paravertebral extension, without myelopathy signs. Partial destruction of left posterior elements of C6 and T1 is also visible. (D,E) Cervical spine CT revealing a destructive collapsing lesion in C7 vertebra, affecting the posterior part of the vertebral body and the posterior elements, and causing subluxation and angular kyphosis of the cervical spine. There was also partial involvement of the left pedicle, lamina, and spinous process of C6 and, to a lesser extent, the T1 left pedicle.
A CT-guided percutaneous core needle biopsy was suggestive of GCRO. Extension studies ruled out distant disease, being staged as: stage IIB of the Enneking (10) and American Joint Committee on Cancer (AJCC) systems (11); Tomita type 6, this being an extra-compartmental tumor with adjacent vertebral extension (12) and 1–10/A–D of the Weinstein-Boriani-Biagini (WBB) tumor classification system (13). The Spinal Instability Neoplastic Score (SINS) was 16 points indicating instability.
According to the national protocol for localized osteosarcoma in children (SEHOP-SO-2010) (14), the patient underwent ten cycles of neoadjuvant chemotherapy, two of them being omitted due to nephrotoxicity and hepatotoxicity. He remained immobilized during this time with a plain cervical collar. Once neoadjuvant ChT was over, new imaging examinations were done, showing minimal bone tumor size reduction, but delimitation and a slight decrease of the soft tissue component. Also, spinal canal compromise (Figure 3) was evidenced on MR myelography that manifested clinically with increased left radiculopathy.
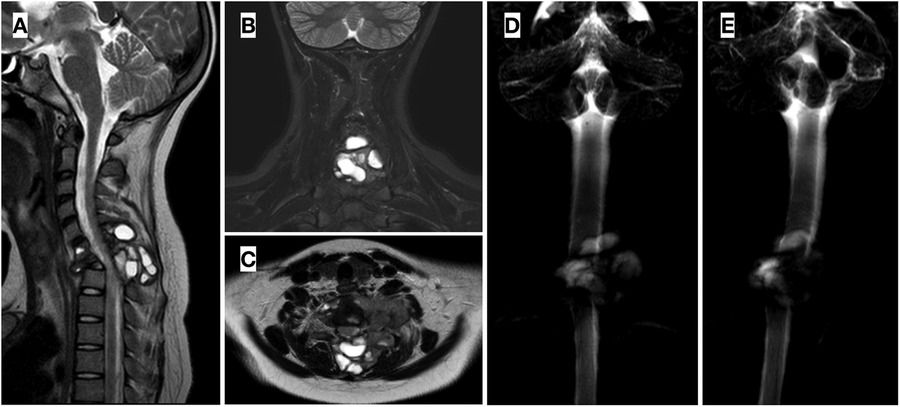
Figure 3. (A,B,C) post neoadjuvant chemotherapy MRI showing delimitation and minor shrink of the soft tumor mass. (D,E). MR myelography demonstrating significant compromise of the spinal canal, especially at C7 level.
Consecutively, surgical resection of the tumoral mass and reconstruction (Figure 4) was performed at week 15. Firstly, with the patient in a supine position, a standard left sternocleidomastoid anterior cervical approach was used to expose the anterior longitudinal ligament and C6–C7 vertebral bodies. With a gentle and thorough dissection, laterally to the vertebral bodies, the tumor was found to have invaded the left pedicle and the posterior part of the C7 vertebral body and the inferior part of C6, as seen in the preoperative images. Resection of the tumoral mass in C6 and C7 vertebral bodies was performed followed by an anterior reconstruction, placing a titanium mesh (DePuy Synthes®) filled with iliac crest allograft and completing the first stage fixation with an anterior plate and screws secured to C5 and T1 vertebral bodies (SkylineTM Anterior Cervical Plate, DePuy Synthes®). Subsequently, with the patient in a prone position and through a longitudinal posterior approach, ligaments and muscles were dissected to expose the tumoral mass and C7 posterior elements. A solid cystic tumoral mass was identified in the left paravertebral region, and infiltration of the left posterior arch was also perceived. Wide resection of the posterior arch of C7 and left part of C6 was completed, performing a total spondylectomy of C7 and partial of C6, thereby releasing the spinal cord, preserving the dura intact and verifying bilateral decompression of C6-T1 roots. T1 left pedicle was also resected due to apparent tumoral invasion. To provide spinal stability, adequate alignment, and balance, a C5-T3 fusion was performed, with bilateral screws to the lateral masses of C5 and right C6, as well as pedicle screws to T1 right and bilaterally to T2 and T3 pedicles plus transitional rods (Synapse System, DePuy Synthes®). Drainage was applied and the wound was closed in layers. Neurophysiological monitoring showed no alterations during the procedure, and fluoroscopic control was satisfactory.
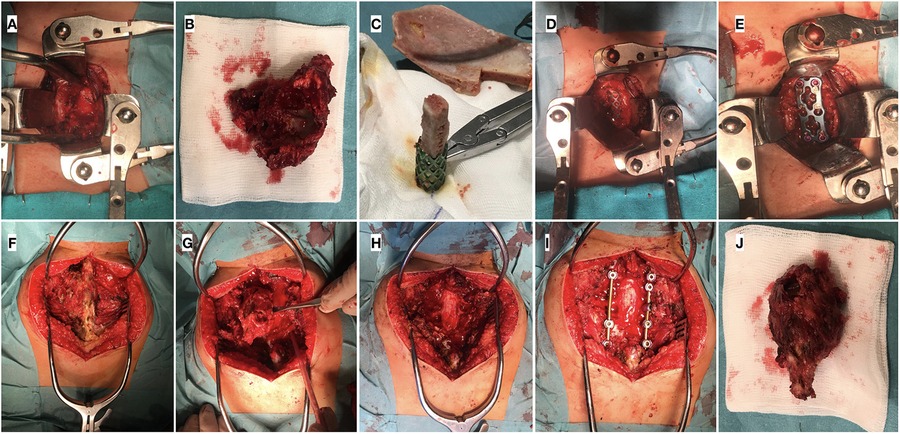
Figure 4. Intraoperative images: (A–E). Anterior approach: (A) Exposure of anterior part of C6-C7 vertebral bodies; (B) Tumoral mass within vertebral bodies; (C) Preparation of Moss mesh with iliac crest allograft; (D) Placement of mesh with allograft in the cervical spine defect; (E) Anterior plate fixation. (F–J). Posterior approach: (F) Exposure of posterior vertebral elements; (G) Posterior vertebral arch resection for total piecemeal spondylectomy; (H) Spinal cord and roots decompressed; (I) Posterior instrumentation fusion C5-T3 with bilateral screws and rods; (J) Posterior part of the tumoral piece.
The histopathological results mentioned that the surgical resection piece consisted of a bony tissue measuring 7 × 3.5 × 2.5 cm covered by muscular tissue (Figure 5). Osteoforming neoplastic proliferations infiltrating into adjacent reticular bone trabeculae were identified. They were arranged in a fibrovascular stroma in which numerous osteoclastic multinucleated giant cells could be observed. Ki-67 proliferative index was 26%. A larger piece showed various cystic areas, accompanied by areas of postchemotherapy necrosis that accounted for 30% of the total area of the neoplasm.
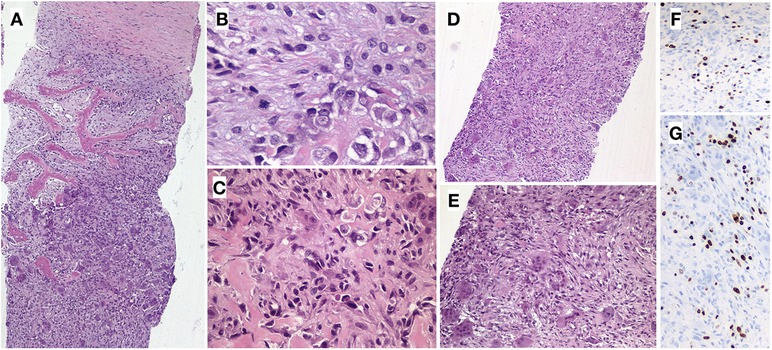
Figure 5. Resected tumor histology of the patient. (A) Plexiform and fibrous bone tissue infiltrated by solid neoplastic proliferation (HE, 40x). (B) Tumor cells with fusiform and epithelioid morphology with marked cellular atypia and numerous mitotic figures (HE, 400x). (B,C) Malignant cells are surrounded by fibrovascular stroma and subtle osteoid deposits (HE, 400x, 200x). (D,E) Numerous osteoclastic multinucleated giant cells are identified (HE, 100x, 200x). (F,G). Expression of the Ki-67 proliferation marker.
During the immediate postoperative period, the patient evolved positively, and the surgical wound showed no signs of infection. The patient initiated sitting and ambulation with a rigid cervical collar for two weeks and no neurological symptoms or other complications appeared. Two weeks after surgery, adjuvant chemotherapy was started and subsequently radiotherapy was added as indicated in the proposed protocol. The cervical and upper dorsal spine C4-D1 was irradiated with Volumetric Intensity Modulated Arcotherapy technique with daily Cone Beam CT, 6 MV photons, using isocentric technique, planned with CT at a dose of 50.4 Gy with fractions of 1.8 Gy/fraction. Periodical clinical and radiological visits were set for 1, 3, 6, 12, 24, and 36 months after surgery at the spine clinic, as well as closer visits by the oncologists, with the patient being disease-free to date. In the last evaluation, he was healthy, did not require technical aids for walking or cervical immobilization, and had neither pain nor neurological symptoms. The last radiological examination can be seen in Figure 6.
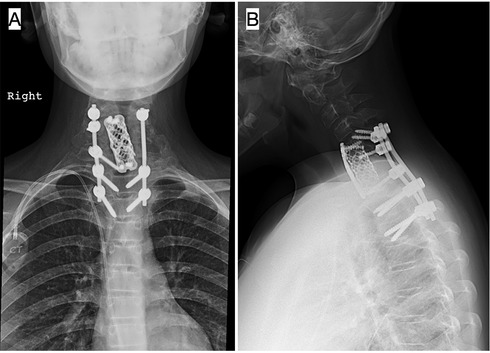
Figure 6. Anteroposterior (A) and lateral (B) x-rays of the cervical spine at 3 years postoperatively: interbody moss mesh, anterior plate fixation, and bilateral posterior instrumentation fusion with screws and rods from C5 to T3. Adequate alignment and balance, without signs of implant loosening or lack of consolidation.
Discussion
The case of a rare variant of osteosarcoma located in the cervical spine of a pediatric patient is presented here. A complete initial investigation revealed an aggressive bone lytic lesion located at C7 with soft tissue involvement and compromised spine stability. Distant disease was discarded, and a biopsy confirmed the GCRO diagnosis. Treatment followed the national protocol that combined neoadjuvant ChT, surgical resection and reconstruction, adjuvant ChT, and RT.
After a thorough review of the literature, we were only able to find 42 published cases of GCRO (Table 1), none of which located in the spine, aside from ours. In the current case, infiltration of bone tissue by a solid neoplastic proliferation, subtle osteoid deposits, and a Ki67 proliferative index of 26% help to differentiate it from a giant cell tumor. GCRO is found mostly in children, adolescents, and young adults, with half of the cases analyzed occurring in patients under 20 years old. However, there are reported cases in patients up to 67 years old (23). Most of the reported GRCO occurred in the knee region, 13/42 in the proximal tibia, and 10/42 in the distal femur. Regarding the treatment strategy, 12 out of 42 patients received neoadjuvant chemotherapy, whereas 21 patients were treated with postoperative chemotherapy and only 5 patients received postoperative radiotherapy. Regarding the first surgical treatment, the resection performed was radical in 11 cases, wide in 14 cases, and intralesional in 13 cases. On follow-up, local recurrence was reported in 12 cases and metastasis in 13, with a median follow-up of 36 months.
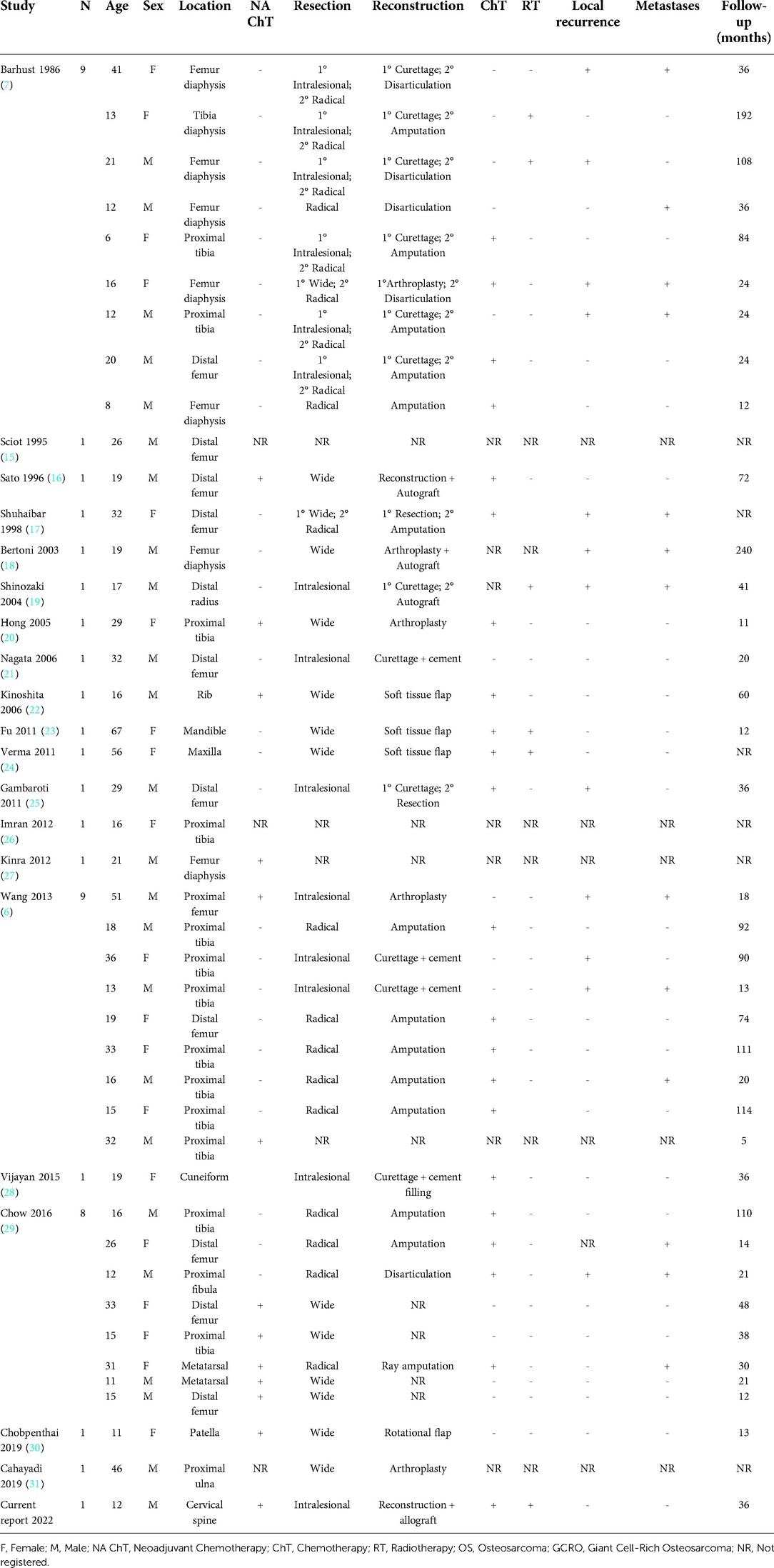
Table 1. Outline of the cases of giant cell-rich osteosarcoma published in the literature.
The appearance of osteosarcomas in the cervical region has rarely been reported in the literature. There are only 5 published cases of cervical spine osteosarcoma in pediatric patients and the number would increase by 8 more if our research were to include adult patients (Table 2), for a total of 13 cases. Regarding the treatment strategy, 8 cases received neoadjuvant chemotherapy, while 12 patients were treated with postoperative chemotherapy and 10 patients received postoperative radiotherapy. Even though radiotherapy has not proven remarkably effective at influencing the long-term prognosis of osteosarcomas, the difficulty of achieving free tumoral resection margins at this anatomical location justifies the necessity of adding radiotherapy as a supplemental therapeutic tool. The histological type of osteosarcoma was telangiectasic in 3 cases, osteoblastic in 2 cases, and chondroblastic, giant cell osteosarcoma, and osteoblastoma type in one case each, with 6 other cases in which the type of osteosarcoma was not registered. As previously mentioned, to date there have been no published cases of GCRO located at the cervical spine. At a median follow-up of 44 months in the published cases, there were 4 local recurrences and 4 metastases.
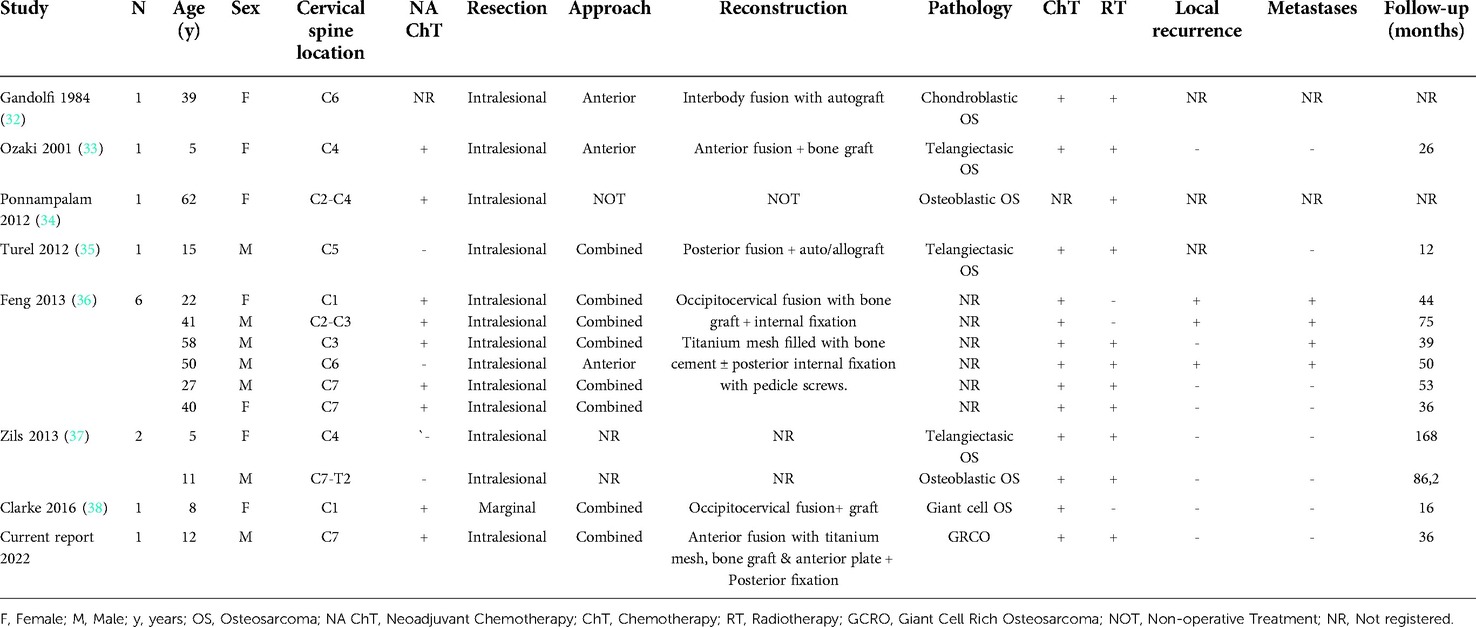
Table 2. Summary of the cases of cervical spine osteosarcoma reported in the literature.
Concerning local tumor management, the definitive treatment for any malignant tumor should be a wide en-bloc resection including surrounding intact tissue, without violating the tumor capsule to avoid the risk of satellite tumor cells being left behind and thus limiting the possibility of recurrence. Total en-bloc resections of tumors at the cervical spine with vertebral artery control or sacrifice of one of them have been described previously (39, 40). However, in some cases, the proximity of the spinal cord and roots and vascular structures can prevent a wide resection, which forces the surgeon to obtain limited margins. Hence, this being a rare location for osteosarcoma, management poses a special challenge. Total en-bloc spondylectomy refers to a resection where the tumor mass together with the vertebral body and posterior elements are removed as a single unit. Although, it is not a synonym for a wide resection since it is usually a marginal type of resection alongside the tumor capsule. On the other hand, a total piecemeal spondylectomy is an intralesional resection where most of the tumor is excised, but some macroscopic tumor cells might be left, usually due to their proximity to noble structures or, as in the case of our patient, due to the need to remove the tumor from two different approaches and in two separate pieces. In all the cervical spine osteosarcoma cases reviewed, an intralesional resection was performed, except for one en-bloc marginal resection (38). Three of them were done by an anterior approach, and seven with a combined anteroposterior approach as in our case.
Following tumor resection, the challenge is to restore the stability, biomechanics, and global alignment of the cervical spine. Most of the cases evaluated were reconstructed with a circumferential fusion. The cases involving the upper cervical spine were handled with an occipitocervical fusion. A special concern in our case was that the tumor was located in the cervicothoracic area, which is a high-stress junctional zone that is exposed to high mobility and does not tolerate bone loss easily. Hence, a stable reconstruction was performed using a combination of anterior and posterior spinal fusion with the addition of a tricortical iliac crest allograft, a titanium Moss mesh, and an anterior plate. Transitional rods and screws were applied in the transition from the cervical to the thoracic spine, and the screw diameter employed was different for the cervical vertebrae (4.5 mm) than the thoracic ones (5.5 mm).
Osteosarcoma of the cervical spine is exceptional (5 cases in children and 8 in adults), as is the GCRO variant in any location (42 cases). To the best of our knowledge, this is the first published case of GCRO in the cervical spine in a pediatric patient, which can be explained by the combination of three peculiar conditions: its location in the cervical spine region, the young age of the patient, and the GCRO variant. Henceforward, despite its unlikeness, this diagnosis should be considered when dealing with a tumor in the spine. In the cervical spine in particular, oncological resection is almost always intralesional due to the proximity of the neuraxis, which is why radiotherapy is often administered. Following oncological resection, the reconstruction phase pursues local stability, regional alignment, and global spine balance, bearing in mind the growing condition of pediatric patients.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
RME-G, MG-O, AG-M and RG-D contributed to the conception and acquisition of data, drafting the manuscript and revising the manuscript critically for important intellectual content, provided final approval of the version of the manuscript to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
Acknowledgments
This study was presented at the GEER meeting 2020.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Dormans JP, Conway SC. Pediatric neoplasms of the spine. In: Errico TJ, Lonner BS, Moulton AW, editors. Surgical management of spinal deformities. Philadelphia, PA: W.B. Saunders (2009). p. 195–209. https://doi.org/10.1016/B978-141603372-1.50017-2
2. Kim HJ, McLawhorn AS, Goldstein MJ, Boland PJ. Malignant osseous tumors of the pediatric spine. J Am Acad Orthop Surg. (2012) 20(10):646–56. doi: 10.5435/JAAOS-20-10-646
3. Ilaslan H, Sundaram M, Unni KK, Shives TC. Primary vertebral osteosarcoma: imaging findings. Radiology. (2004) 230:697–702. doi: 10.1148/radiol.2303030226
4. Egea-Gámez RM, Ponz-Lueza V, Cendrero-Torrado A, Martínez-González C, Certucha-Barragán JA, González-Díaz R. Spinal osteosarcoma in the paediatric age group: case series and literature review. Osteosarcoma lumbar en edad pediátrica: reporte de casos y revisión de la literatura. Rev Esp Cir Ortop Traumatol. (2019) 63(2):122–31. doi: 10.1016/j.recot.2018.09.001
5. Klein MJ, Siegal GP. Osteosarcoma: anatomic and histologic variants. Am J Clin Pathol. (2006) 125:555–81. doi: 10.1309/UC6KQHLD9LV2KENN
6. Wang CS, Yin QH, Liao JS, Lou JH, Ding XY, Zhu YB. Giant cell-rich osteosarcoma in long bones: clinical, radiological and pathological features. Radiol Med. (2013) 118(8):1324–34. doi: 10.1007/s11547-013-0936-9
7. Bathurst N, Sanerkin N, Watt I. Osteoclast-rich osteosarcoma. Br J Radiol. (1986) 59(703):667–73. doi: 10.1259/0007-1285-59-703-667
8. Chow LT. Fibular giant cell-rich osteosarcoma virtually indistinguishable radiographically and histopathologically from giant cell tumor-analysis of subtle differentiating features. APMIS. (2015) 123(6):530–9. doi: 10.1111/apm.12382
9. Fletcher CDM, Bridge JA, Hogendoorn P, Mertens F. WHO Classification of tumours of soft tissue and bone. 4 edn Lyon: IARC Press (2013);5: 282–8.
10. Enneking WF. A system of staging musculoskeletal neoplasms. Clin Orthop Relat Res. (1986) 204:9–24.
11. Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. (2017) 67(2):93–9. doi: 10.3322/caac.21388
12. Tomita K, Kawahara N, Baba H, Tsuchiya H, Nagata S, Toribatake Y. Total en bloc spondylectomy for solitary spinal metastases. Int Orthop. (1994) 18:291–8. doi: 10.1007/BF00180229
13. Boriani S, Weinstein JN, Biagini R. Primary bone tumors of the spine: terminology and surgical staging. Spine. (1997) 22(9):1036–44. doi: 10.1097/00007632-199705010-00020
14. Sociedad Española de Hematología y Oncología Pediátricas (SEHOP). Protocolo de tratamiento del sarcoma osteogénico con enfermedad localizada en niños SEHOPO-SO-2010. Edition: May 2010.
15. Sciot R, Samson I, Dal Cin P, Lateur L, van Damme B, van den Berghe H, et al. Giant cell rich parosteal osteosarcoma. Histopathology. (1995) 27(1):51–5. doi: 10.1111/j.1365-2559.1995.tb00290.x
16. Sato K, Yamamura S, Iwata H, Sugiura H, Nakashima N, Nagasaka T. Giant cell-rich osteosarcoma: a case report. Nagoya J Med Sci. (1996) 59(3-4):151–7.
17. Shuhaibar H, Friedman L. Dedifferentiated parosteal osteosarcoma with high-grade osteoclast-rich osteogenic sarcoma at presentation. Skeletal Radiol. (1998) 27(10):574–7. doi: 10.1007/s002560050440
18. Bertoni F, Bacchini P, Staals EL. Malignancy in giant cell tumor of bone. Cancer. (2003) 97(10):2520–9. doi: 10.1002/cncr.11359
19. Shinozaki T, Fukuda T, Watanabe H, Takagishi K. Giant cell-rich osteosarcoma simulating giant cell tumor of bone. Kitakanto Med J. (2004) 54:147–51. doi: 10.2974/kmj.54.147
20. Hong SJ, Kim KA, Yong HS, Choi JW, Suh SI, Lee JH, et al. Giant cell-rich osteosarcoma of bone. Eur J Radiol Extr. (2005) 53(2):87–90. doi: 10.1016/j.ejrex.2004.12.001
21. Nagata S, Nishimura H, Uchida M, Hayabuchi N, Zenmyou M, Harada H. Giant cell-rich osteosarcoma of the distal femur: radiographic and magnetic resonance imaging findings. Radiat Med. (2006) 24(3):228–32. doi: 10.1007/s11604-005-1546-9
22. Kinoshita G, Yasoshima H. Giant cell-rich tumor of the rib. J Orthop Sci. (2006) 11(3):312–7. doi: 10.1007/s00776-006-1018-9
23. Fu HH, Zhuang QW, He J, Wang LZ, He Y. Giant cell-rich osteosarcoma or giant cell reparative granuloma of the mandible? J Craniofac Surg. (2011) 22(3):1136–9. doi: 10.1097/SCS.0b013e3182108fbf
24. Verma RK, Gupta G, Bal A, Yadav J. Primary giant cell rich osteosarcoma of maxilla: an unusual case report. J Maxillofac Oral Surg. (2011) 10(2):159–62. doi: 10.1007/s12663-010-0066-z
25. Gambarotti M, Donato M, Alberghini M, Vanel D. A strange giant cell tumor. Eur J Radiol. (2011) 77(1):3–5. doi: 10.1016/j.ejrad.2010.06.050
26. Imran AA, Khaleel ME, Salaria SM, Hasan M. Giant cell- rich osteosarcoma: unravelling an elusive, enigmatic entity. Int J Pathol. (2012) 10(1):36–8.
27. Kinra P, Valdamani S, Singh V, Dutta V. Diaphyseal giant cell-rich osteosarcoma: unusual histological variant in an unusual site. Indian J Pathol Microbiol. (2012) 55(4):600–2. doi: 10.4103/0377-4929.107848
28. Vijayan S, Naik MA, Hameed SA, Rao SK. Giant cell rich osteosarcoma of the cuneiforms. J Cancer Res Ther. (2015) 11(4):989–92. doi: 10.4103/0973-1482.157318
29. Chow LT. Giant cell rich osteosarcoma revisited-diagnostic criteria and histopathologic patterns, Ki67, CDK4, and MDM2 expression, changes in response to bisphosphonate and denosumab treatment. Virchows Arch. (2016) 468(6):741–55. doi: 10.1007/s00428-016-1926-9
30. Chobpenthai T, Thanindratarn P. Giant cell-rich variant of extraskeletal osteosarcoma above the Patella – A rare case study and review of the literature. Biomed J Sci Tech Res. (2019) 19(5):14633–8. doi: 10.26717/BJSTR.2019.19.003369
31. Cahayadi SD, Antoro A, Swandika B. A giant cell rich osteosarcoma of the proximal ulnar bone treated by elbow arthroplasty: a case report. Int J Surg Case Rep. (2019) 58:157–61. doi: 10.1016/j.ijscr.2019.04.017
32. Gandolfi A, Bordi C. Primary osteosarcoma of the cervical spine causing neurological symptoms. Surg Neurol. (1984) 21(5):441–4. doi: 10.1016/0090-3019(84)90448-8
33. Ozaki T, Flege S, Liljenqvist U, Hillmann A, Delling G, Salzer-Kuntschik M, et al. Osteosarcoma of the spine: experience of the cooperative osteosarcoma study group. Cancer. (2002) 94(4):1069–77. doi: 10.1002/cncr.10258
34. Ponnampalam SN, Tan WY, Wazir NN, George J. Unusual cause of neuropathy: extensive dural spread of primary cervical osteosarcoma. Acta Radiol Short Rep. (2012) 1(1):arsr.2012.110028. Published 2012 Feb 10. doi: 10.1258/arsr.2012.110028
35. Turel MK, Joseph V, Singh V, Moses V, Rajshekhar V. Primary telangiectatic osteosarcoma of the cervical spine. J Neurosurg Spine. (2012) 16(4):373–8. doi: 10.3171/2011.12.SPINE111037
36. Feng D, Yang X, Liu T, Xiao J, Wu Z, Huang Q, et al. Osteosarcoma of the spine: surgical treatment and outcomes. World J Surg Oncol. (2013) 11(1):89. Published 2013 Apr 18. doi: 10.1186/1477-7819-11-89
37. Zils K, Bielack S, Wilhelm M, Werner M, Schwarz R, Windhager R, et al. Osteosarcoma of the mobile spine. Ann Oncol. (2013) 24(8):2190–5. doi: 10.1093/annonc/mdt154
38. Clarke MJ, Price DL, Cloft HJ, Segura LG, Hill CA, Browning MB, et al. En bloc resection of a C-1 lateral mass osteosarcoma: technical note. J Neurosurg Pediatr. (2016) 18(1):46–52. doi: 10.3171/2015.12.PEDS15496
Keywords: osteosarcoma - pathology, spine, cervical cancer, surgical oncology, reconstructive surgical procedure
Citation: Egea-Gámez RM, Galán-Olleros M, González-Menocal A and González-Díaz R (2022) Case Report: Giant cell-rich osteosarcoma of the cervical spine in the pediatric age. A rare entity to consider. Front. Surg. 9:1001149. doi: 10.3389/fsurg.2022.1001149
Received: 22 July 2022; Accepted: 26 September 2022;
Published: 14 October 2022.
Edited by:
Gianluca Testa, Università degli Studi di Catania, ItalyReviewed by:
Antonio Martín-Benlloch, Chief of Spine Unit. Doctor Peset Hospital, SpainInmaculada Vilalta Vidal, Spine Unit. Sant Joan de Deu Hospital, Spain
© 2022 Egea-Gámez, Galán-Olleros, González-Menocal and González-Díaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Galán-Olleros bWdhbGFub2xsZXJvc0BnbWFpbC5jb20=