 Giacomo Calini
Giacomo Calini Pier Paolo Brollo1†
Pier Paolo Brollo1† Vittorio Bresadola
Vittorio Bresadola
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Surg. , 02 February 2022
Sec. Visceral Surgery
Volume 8 - 2021 | https://doi.org/10.3389/fsurg.2021.786158
Purpose: Currently, surgical drainage during a laparoscopic cholecystectomy (LC) is still placed in selected patients. Evidence of the non-beneficial effect of the surgical drain comes from studies with a heterogeneous population. This preliminary study aims to identify any clinical, demographic, or intraoperative predictive factors for a surgical drain placement during LC as the first step to identify population for a prospective randomized study.
Method: The study was conducted in a single referral center and academic hospital between 2014 and 2018. Patients who underwent unconverted LC were divided into two groups: Group A (drain) and Group B (no drain). We explored baseline, preoperative, intraoperative characteristics, and postoperative outcomes.
Results: Between 409 patients who underwent LC: 90 (22%) patients were in Group A (drain). Age >64 years, male sex, cholecystitis, Charlson comorbidity index (CCI) ≥ 1, experienced surgeon, intraoperative technical difficulties, need for an additional trocar, operative time >60 min, and estimated blood loss >10 ml were predictive factors at univariate analysis. While at multivariate analysis, cholecystitis (odds ratio [OR]: 2.8, 95% CI:1.5–5.1; p < 0.001), CCI ≥ 1 (OR:1.9, 95% CI:1.0–3.5; p = 0.05), intraoperative technical difficulties (OR: 3.6, 95% CI:1.8–6.2; p < 0.001), need of an additional trocar (OR: 2.5, 95% CI: 1.4–4.4; p < 0.005), and estimated blood loss >10 ml (OR: 3.0, 95% CI:1.7–5.3; p < 0.0001) were predictive factors for a surgical drain placement during LC.
Conclusions: This study identified predictive factors that currently drive the surgeons to a surgical drain placement after LC. Randomized prospective studies are needed to define the use of drain placement in these selected patients.
In the past decades, cholecystectomy has become one of the most frequently performed surgical procedures, both in the elective and in the urgency/emergency setting (1). The laparoscopic approach is now the first choice and in most cases, it allows to complete the surgical procedure with excellent patient outcomes, adding the laparoscopic advantages in terms of postoperative management (2–4). The usefulness of surgical drain placement after a cholecystectomy has long been debated. Although numerous randomized clinical trials and meta-analyses have already clearly shown that the use of surgical drain does not improve the postoperative outcomes of patients, surgical drains are still used in selected populations (5–7). Over the years, the evolution of surgical technique and the increasing life expectancy of the general population has led to an expansion of surgical indications to a wider and heterogeneous pool of patients (8–12). The progress of surgical technique, the increasing experience of operators, and the accumulation of scientific evidence greatly influenced a more restricted use of surgical drain at the end of a cholecystectomy (13). However, it still remains a device used in conditions that often raise serious concerns about its usefulness or even raise doubts about its potentially harmful effects. These considerations are particularly relevant for patients who are more fragile for clinical and age-related reasons, such as the elderly (4, 14). To date, the evidence of the non-beneficial effect of the surgical drain comes from studies with a heterogeneous population (5, 6, 15, 16). We hypothesize that the intraoperative drain placement might still have a role in selected populations. Hence, defining the predictive factors for surgical drain placement in the current practice is the first step to identify the population for a prospective randomized study. In light of the above, the aim of this preliminary study was to identify any predictive factors for the intraoperative drain placement in patients undergoing laparoscopic cholecystectomy (LC).
This study was conducted in an Italian Academic Hospital (AH) from March 2020 to September 2020. It was consisted of a retrospective analysis of hospital discharge data regarding all patients who underwent LC, identified by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code 51.23, as the primary procedure not associated with any other significant surgery during the 2014–2018 period. Data were collected, anonymously and in aggregate form, from the Regional Socio-Health Information System (SISSR) and analyzed by extracting information about the demographic characteristics of patients, urgency and diagnosis upon admission to the hospital, surgery procedure, perioperative course, comorbidities, and complications using ICD-9-CM codes. In the second step, two experienced surgeons reviewed all cases to exclude those with malignant biliary disease and with cholelithiasis complicated by acute pancreatitis or obstruction of the common bile duct. After local IRB approval of the study, hospital clinical computerized records were consulted to implement information not available in the regional database.
Patients were allocated into two groups: Group A (patients with surgical drain placement during LC) and group B (patients without drain placement). Both groups of patients were investigated with respect to the following variables: (1) general characteristics: age, sex, body mass index (BMI) (underweight: <18.5; normal weight 18.5–24.9; overweight 25.0–29.9; and obese ≥30.0); (2) preoperative clinical conditions: severity of cholelithiasis, comorbidity (by using ICD-9-CM codes) and Charlson comorbidity index (CCI) with no age-adjustment (17); (3) surgical procedure: admission urgency (elective and non-elective), first surgeon (experienced surgeon with more than 10-year laparoscopic experience and resident), intraoperative technical difficulties described in the surgical report (defined as fibrotic adherence, intentional puncture to decompress the gallbladder, gallbladder rupture with bile contamination of the operating field, bleeding from the cystic artery, difficult individuation of the anatomical structures, liver steatosis/cirrhosis, and subtotal cholecystectomy), need for an additional trocar, operating time, and estimated blood loss. The ICD-9-CM diagnosis codes used to classify comorbidities related to cholecystectomy are reported in the Supplementary Material. CCI was grouped into 3 classes: 0, 1–2, and ≥3; we used the CCI without age to avoid the collinearity in multivariate analysis. The clinical severity of cholelithiasis was divided into two categories: (1) cholelithiasis only (ICD-9-CM codes: 574.20, 574.50, 574.90, 574.21, and 575.3) and (2) cholecystitis with or without cholelithiasis (ICD-9-CM codes: 574.10, 574.40, 574.70, 575.1, 574.00, 575.0, 575.11, and 575.12). The events considered as predictors of negative clinical outcome occurring in the two groups after LC were: (1) postoperative complications, as described in the postoperative notes, discharge summary, and post-discharge follow-up/imaging (bile leak, intra-abdominal fluid, wound complications, and incisional hernia), and their severity level expressed by the Clavien-Dindo classification (CDC) (18); (2) surgical re-intervention within 30 days; and (3) increase in the postoperative hospital stay.
In our center, LC has been performed according to a standardized technique (19). The patient is positioned in stirrups with the primary operator standing between the legs. A blunt umbilical trocar is positioned with an open technique. After exploration of the peritoneal cavity, other 2–3 trocars are inserted under vision. The dissection of the Calot's triangle is performed to reach the “critical view of safety” with the aim to identify and dissect the cystic duct and cystic artery. Clipping and division of the structures are then carried out. Intraoperative cholangiography and gallbladder needle decompression are not routinely performed. Retrograde dissection of liver bed is completed and the gallbladder removed by using an endobag. An abdominal surgical drain is not routinely placed; when it does, we place an 18 Fr tubular close drain (19).
All analyses were performed using the statistical software SPSS, V.20. The description of the data was done in the form of mean and SD for quantitative data and frequency and proportion for qualitative data. Age was described both as a continuous variable and as a qualitative variable. The population was divided into elderly (≥65 years) and non-elderly (<65 years). The first analysis of the data was done to test statistically significant differences between the two groups of patients, Group A (with surgical drain) and Group B (without drain placement), with regard to preoperative, intra-operative, and postoperative variables. An independent t-test for quantitative data and chi-square test for qualitative ones were used. The second endpoint was to explore the predictive factors that supported the decision of surgeon to insert a drain after LC. Univariate and multivariate analyses with odds ratios (ORs) and 95% CIs were used. The choice of potential predictive factors for the multivariate model was based on the results of univariate analysis, with p < 0.05 as the criterion for inclusion. The factors that did not maintain an association in the final model were considered not to be associated after correction by the confounding factors. Statistical significance was set at a p < 0.05.
In total, 409 patients underwent LC as the primary procedure during hospitalization in our AH between 2014 and 2018. An intraoperative surgical drain was placed in 90 patients (Group A) and was not placed in 319 patients (Group B). Preoperative and operative data in both groups are shown in Table 1. In regard to the preoperative data, group A was found to be statistically older (44.4 vs. 26.0%, p < 0.001), with a higher incidence of cholecystitis (52.2 vs. 21.3, p < 0.0001) and with a CCI (with no age) ≥1 (35.6 vs. 19.4, p < 0.01). There were statistically significant differences between the two groups in all operative data: group A presented a longer operative time (112.6' + 30.0' vs. 77.8' + 27.4', p < 0.0001), more intraoperative technical difficulties (77.8 vs. 42.3%, p < 0.0001), need of an additional trocar (50.0 vs. 21.9%, p < 0.0001), and estimated blood loss >10 ml in more patients (68.9 vs. 36.4%, p < 0.0001), as compared with group B. Among the postoperative outcomes of interest in Table 2, group A and group B had a statistically significant difference in the occurrence of postoperative surgical complications (18.9 vs. 8.8%, p < 0.01), overall postoperative complications (28.9 vs. 14.7%, p < 0.01) and mean postoperative hospital length of stay (2.3 + 2.1 vs. 1.2 + 0.7 days, p < 0.0001).
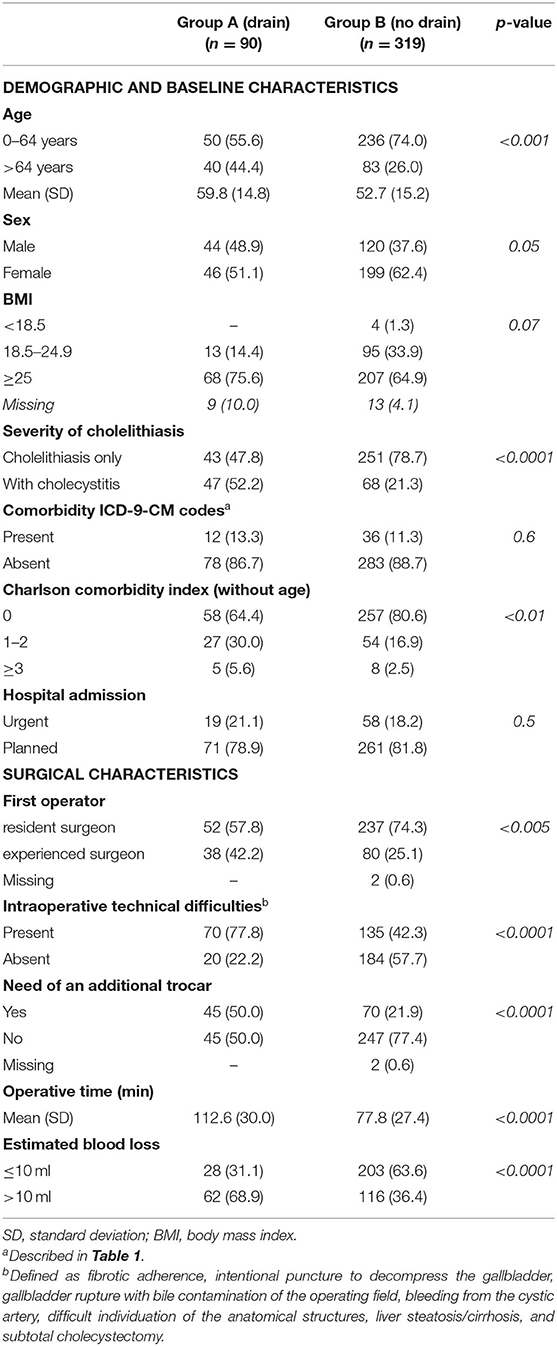
Table 1. Pre- and intra-operative data for patients undergoing laparoscopic cholecystectomy (LC).
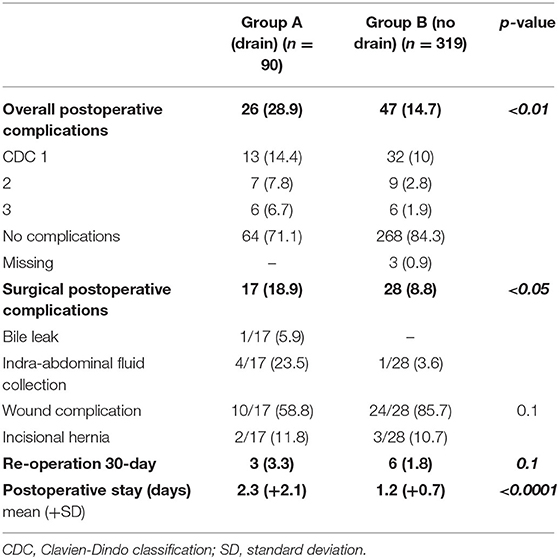
Table 2. Postoperative outcomes.
Univariate analysis for the predictive factors that drove the decision of surgeon to place the drain after a cholecystectomy is reported in Table 3. Predictive variables were age > 64 years (OR = 2.3; 95% CI: 1.4–3.7; p < 0.0001), male sex (OR = 1.6; 95% CI: 1.0–2.5; p < 0.05), cholecystitis with or without cholelithiasis (OR = 4.0; 95% CI: 2.5–6.6; p < 0.0001), CCI (with no age) value ≥1 (OR = 2.3; 95% CI: 1.4–3.8; p < 0.01), experienced surgeon as first operator (OR = 2.2; 95% CI: 1.3–3.5; p < 0.005), the presence of an intraoperative technical difficulty (OR = 4.8; 95% CI: 2.7–8.2; p < 0.0001), the need of an additional trocar (OR: 3.5, 95% CI: 2.1–5.8; p < 0.0001), operative time >60 min (13.6, 95% CI: 4.2–44.1; p < 0.0001) and estimated blood loss >10 ml (OR: 3.9, 95% CI: 2.3–6.4; p < 0.0001).
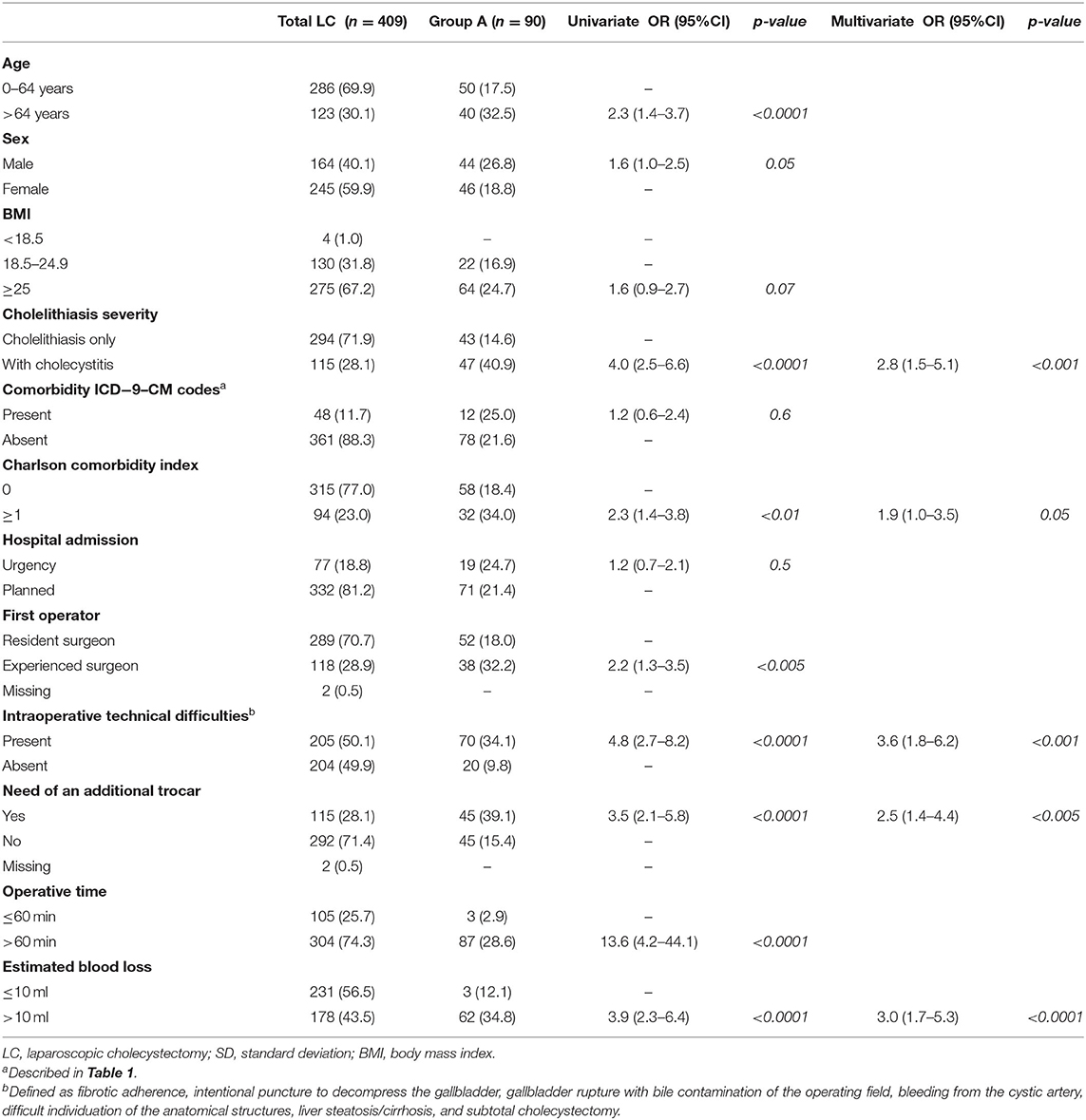
Table 3. Univariate and multivariate analysis for drain placement after LC.
At multivariate analysis in Table 3, cholecystitis (OR: 2.8, 95% CI: 1.5–5.1; p < 0.001), CCI (with no age) value ≥1 (OR:1.9, 95% CI: 1.0–3.5; p = 0.05), intraoperative technical difficulties (OR: 3.6, 95% CI: 1.8–6.2; p < 0.001), need of an additional trocar (OR: 2.5, 95% CI: 1.4–4.4; p < 0.005), and estimated blood loss >10 ml (OR: 3.0, 95% CI: 1.7–5.3; p < 0.0001), were the predictive factors that drove the surgeons to surgical drain placement after LC.
This study highlights how the surgical drain is used in a small number of patients undergoing unconverted LC from a purely descriptive point of view. In fact, in the patients under consideration, a surgical drain was placed in only 22% of the cases. This reflects the careful selection of the patient to use this device, according to what is widely reported in the current literature (5, 6, 8, 13). In their study, Park et al. (5) underline how the placement of intraoperative surgical drain has proved useful only in cases of difficult ligation of the cystic duct or hemostasis of the operative field and in the case of a suspected biliary leak. Conversely, they did not show a statistically significant difference in the onset of infected intra-abdominal collections between the group of patients with and without surgical drain after LC for acute cholecystitis. They conclude that the surgical drain should not be used prophylactically during LC because it does not reduce the morbidity and does not prevent local complications (such as, surgical site infection); rather it could be a risk factor for their onset (5). Qiu and Li (20) and Picchio et al. in their meta-analysis (6), have reported an increased number of complications, such as fever, wound infections, hemorrhage, wound herniations, increased postoperative pain, and hospital stay in patients with surgical drain placement. In our study, intraoperative drain placement was more frequent in older male subjects with BMI ≥ 25. This is particularly interesting considering that older age, male sex, and obesity are associated with a more severe acute cholecystitis clinical presentation (7, 21–25). Among the clinical conditions, the choice to place surgical drain correlates with the greater severity of the disease, particularly with the diagnosis of cholecystitis. This evidence is in agreement with what has been reported in the meta-analysis by Picchio et al. (6). Besides, these patients are clinically more complex, as expressed by their CCI (with no age). Both conditions put this group of subjects at a higher risk of perioperative complications, often the reason for the decision to use the drain at the end of surgery (26, 27). The emergency admission to the hospital has not shown to be significant in the decision to place surgical drain. Probably, the correct selection of the patient undergoing surgery, in accordance with the 2018 Tokyo Guidelines (28, 29), plays a key role. For example, in the case of fragile patients with emergency admission, it is preferable to adopt a conservative treatment with percutaneous drainage and antimicrobial therapy scheduling elective surgery subsequently, reducing the risk to place a drain (30–34). However, the results of the study by Ferrarese et al. (31), while confirming the safety and feasibility of LC in elderly patients both in the elective and emergency regimes, showed a statistically significant increase in the placement of surgical drain in patients operated in the emergency regime.
In the present study, the first operator is associated with the surgical drain placement after LC. In particular, residents place fewer drains than experienced surgeons. However, we believe that this association is more than a difference in management itself due to the patient selection. Indeed, the experienced surgeon attends during the surgery of residents, partake in the decision-making process, and takes the lead in the most complex intraoperative scenario. Therefore, experienced surgeons are the first surgeon for surgeries with a greater risk of intra- and postoperative complications, as demonstrated in the literature (19, 35, 36). Indeed, a greater complexity of the procedure, identified with the need to place an additional trocar, the finding of estimated blood losses >10 ml or a longer operating time, correlates with the choice to place the surgical drain after laparoscopic cholecystectomy in our study. At the univariate analysis, the potential preoperative predictors for a possible drain placement were found to be as follows: age over 64, male sex, diagnosis of cholecystitis, and a CCI (with no age) score ≥1. In their study, Bawahab et al. (15) show how the clinical condition, the preoperative complications, and the diagnosis of cholecystitis have a statistically significant correlation with the abdominal drain placement at the end of a LC. On the other hand, no study found an association between the CCI and abdominal drain placement during an LC. Among the intraoperative variables, as we have already mentioned, the need to insert an additional trocar, the presence of estimated blood loss >10 ml, and the operative time exceeding 60 min have been confirmed as predictors for the surgical drain placement. According to our bibliographic research, while increased operative time has already been correlated with the increased frequency of surgical drain use (15), no studies have reported the same evidence regarding the use of the additional trocar and intraoperative estimated blood loss. In particular, the diagnosis of cholecystitis, presence of intraoperative technical difficulties, need of an additional trocar, and an estimated blood loss >10 ml are found to be independent predictive factors for surgical drain placement in the multivariate analysis. The overall postoperative complications and those specifically related to surgery (wound infections, abdominal collections, biliary leaks, and incisional hernias) have shown a statistically significant correlation with the intraoperative placement of surgical drain. This correlation is confirmed by several sources in the literature (6, 13). For example, Tzovaras et al. (16) report how drain placement is associated with an increased frequency of postoperative pain and biliary leakage; therefore, its routine use in all elective cholecystectomies is not indicated. This aspect finds confirmation in Lewis et al. (37), who showed that no patient without surgical drain required reoperation or subsequent drainage procedure for subhepatic collections formation, as well as no difference in the frequency of wound infections. However, in other studies, such correlations are not confirmed with the statistical consistency (5, 20). As a result of our study, patients undergoing LC with surgical drain placement have a longer length of hospital stay than those without the placement of this device, as confirmed in previous studies (5, 6). In addition, if our study did not compare costs, a longer length of hospital stay associated with the use of surgical drain raise an economic issue as both hospitalization and materials drive cost.
The main limitation of this study is to be non-randomized, unbalanced, and retrospective. In addition, number of patients and multi-surgeon decisions on drain placement could limit results of this study. However, this preliminary study aimed to describe predictive factors for surgical drain placement during an LC into the current practice. Defining the predictive factors is the first step in identifying the target population for a future prospective study to evaluate the drain placement. The results of this study need to be carefully interpreted, according to the limitations and the aim of the study.
In conclusion, the placement of intraoperative drain after LC is done in selected patients as per the decision of the leading surgeon, with the theoretical purpose of early detection and minimizing complications. At the multivariate analysis, cholecystitis, CCI (with no age) ≥1, intraoperative technical difficulties, the need for an additional trocar, and estimated blood loss >10 ml were the predictive factors for surgical drain placement during LC. Otherwise, surgical drain placement is often associated with increased complications, length of stay, and re-intervention. Since studies showing high-quality evidence in patients with these characteristics are lacking, randomized prospective studies are needed to define the use of surgical drain during an LC in these specific populations.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
GC and PB contributed to the study conception, study design, data acquisition, data interpretation, and manuscript drafting. RQ contributed to the study design, data acquisition, data analysis, and manuscript drafting. VB contributed to the study conception, study design, data interpretation, and manuscript drafting. All authors contributed to the article and approved the submitted version.
Open access funding was provided by University of Udine.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2021.786158/full#supplementary-material
1. Tsui C, Klein R, Garabrant M. Minimally invasive surgery: national trends in adoption and future directions for hospital strategy. Surg Endosc. (2013) 27:2253–7. doi: 10.1007/s00464-013-2973-9
2. Okamoto K, Suzuki K, Takada T, Strasberg SM, Asbun HJ, Endo I, et al. Tokyo Guidelines 2018: flowchart for the management of acute cholecystitis. J Hepatobiliary Pancreat Sci. (2018) 25:55–72. doi: 10.1002/jhbp.516
3. Keus F, de Jong JA, Gooszen HG, van Laarhoven CJ. Laparoscopic versus open cholecystectomy for patients with symptomatic cholecystolithiasis. Cochrane Database Syst Rev. (2006) CD006231. doi: 10.1002/14651858.CD006231
4. Lord AC, Hicks G, Pearce B, Tanno L, Pucher PH. Safety and outcomes of laparoscopic cholecystectomy in the extremely elderly: a systematic review and meta-analysis. Acta Chir Belgica. (2019) 119:349–56. doi: 10.1080/00015458.2019.1658356
5. Park JS, Kim JH, Kim JK, Yoon DS. The role of abdominal drainage to prevent of intra-abdominal complications after laparoscopic cholecystectomy for acute cholecystitis: prospective randomized trial. Surg Endosc. (2015) 29:453–7. doi: 10.1007/s00464-014-3685-5
6. Picchio M, De Cesare A, Di Filippo A, Spaziani M, Spaziani E. Prophylactic drainage after laparoscopic cholecystectomy for acute cholecystitis: a systematic review and meta-analysis. Updates Surg. (2019) 71:247–54. doi: 10.1007/s13304-019-00648-x
7. Yong L, Guang B. Abdominal drainage versus no abdominal drainage for laparoscopic cholecystectomy: a systematic review with meta-analysis and trial sequential analysis. Int J Surg. (2016) 36(Pt. A):358–68. doi: 10.1016/j.ijsu.2016.11.083
8. Coccolini F, Catena F, Pisano M, Gheza F, Fagiuoli S, Di Saverio S, et al. Open versus laparoscopic cholecystectomy in acute cholecystitis. Systematic review and meta-analysis. Int J Surg. (2015) 18:196–204. doi: 10.1016/j.ijsu.2015.04.083
9. Kuwabara K, Matsuda S, Fushimi K, Ishikawa KB, Horiguchi H, Fujimori K. Relationships of age, cholecystectomy approach and timing with the surgical and functional outcomes of elderly patients with cholecystitis. Int J Surg. (2011) 9:392–9. doi: 10.1016/j.ijsu.2011.03.026
10. Lyu Y, Cheng Y, Wang B, Zhao S, Chen L. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis: an up-to-date meta-analysis of randomized controlled trials. Surg Endosc. (2018) 32:4728–41. doi: 10.1007/s00464-018-6400-0
11. Wakabayashi G, Iwashita Y, Hibi T, Takada T, Strasberg SM, Asbun HJ, et al. Tokyo Guidelines 2018: surgical management of acute cholecystitis: safe steps in laparoscopic cholecystectomy for acute cholecystitis (with videos). J Hepato-Biliary-Pancreat Sci. (2018) 25:73–86. doi: 10.1002/jhbp.517
12. Yokoe M, Hata J, Takada T, Strasberg SM, Asbun HJ, Wakabayashi G, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepato Biliary Pancreat Sci. (2018) 25:41–54. doi: 10.1002/jhbp.515
13. Gurusamy KS, Samraj K, Mullerat P, Davidson BR. Routine abdominal drainage for uncomplicated laparoscopic cholecystectomy. Cochrane Database Syst Rev. (2007) CD006004. doi: 10.1002/14651858.CD006004.pub2
14. Mayol J, Martinez-Sarmiento J, Tamayo FJ, Alvarez Fernández-Represa J. Complications of laparoscopic cholecystectomy in the ageing patient. Age Ageing. (1997) 26:77–81. doi: 10.1093/ageing/26.2.77
15. Bawahab MA, Abd El Maksoud WM, Alsareii SA, Al Amri FS, Ali HF, Nimeri AR, et al. Drainage vs. non-drainage after cholecystectomy for acute cholecystitis: a retrospective study. J Biomed Res. (2014) 28:240–5. doi: 10.7555/JBR.28.20130095
16. Tzovaras G, Liakou P, Fafoulakis F, Baloyiannis I, Zacharoulis D, Hatzitheofilou C. Is there a role for drain use in elective laparoscopic cholecystectomy? A controlled randomized trial. Am J Surg. (2009) 197:759–63. doi: 10.1016/j.amjsurg.2008.05.011
17. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. (1987) 40:373–83. doi: 10.1016/0021-9681(87)90171-8
18. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. (2009) 250:187–96. doi: 10.1097/SLA.0b013e3181b13ca2
19. Bresadola V, Pravisani R, Pighin M, Seriau L, Cherchi V, Giuseppe S, et al. Clinical strategies to aim an adequate safety profile for patients and effective training for surgical residents: the laparoscopic cholecystectomy model. Ann Med Surg. (2016) 11:58–61. doi: 10.1016/j.amsu.2016.09.006
20. Qiu J, Li M. Nondrainage after laparoscopic cholecystectomy for acute calculous cholecystitis does not increase the postoperative morbidity. Biomed Res Int. (2018) 2018:8436749. doi: 10.1155/2018/8436749
21. European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol. (2016) 65:146–81. doi: 10.1016/j.jhep.2016.03.005
22. Agarwal N, Sharma BC, Sarin SK. Endoscopic management of acute cholangitis in elderly patients. World J Gastroenterol. (2006) 12:6551–5. doi: 10.3748/wjg.v12.i40.6551
23. Ambe PC, Papadakis M, Zirngibl H. A proposal for a preoperative clinical scoring system for acute cholecystitis. J Surg Res. (2016) 200:473–9. doi: 10.1016/j.jss.2015.09.010
24. Ansaloni L, Pisano M, Coccolini F, Peitzmann AB, Fingerhut A, Catena F, et al. 2016 WSES guidelines on acute calculous cholecystitis. World J Emerg Surg. (2016) 11:25. doi: 10.1186/s13017-016-0082-5
25. Lee HK, Han HS, Min SK. The association between body mass index and the severity of cholecystitis. Am J Surg. (2009) 197:455–8. doi: 10.1016/j.amjsurg.2008.01.029
26. Lu P, Yang N-P, Chang N-T, Lai KR, Lin K-B, Chan C-L. Effect of socioeconomic inequalities on cholecystectomy outcomes: a 10-year population-based analysis. Int J Equity Health. (2018) 17:22. doi: 10.1186/s12939-018-0739-7
27. Sandblom G, Videhult P, Crona Guterstam Y, Svenner A, Sadr-Azodi O. Mortality after a cholecystectomy: a population-based study. HPB. (2015) 17:239–43. doi: 10.1111/hpb.12356
28. Buckman SA, Mazuski JE. Review of the Tokyo guidelines 2018: antimicrobial therapy for acute cholangitis and cholecystitis. JAMA Surg. (2019) 154:873–4. doi: 10.1001/jamasurg.2019.2169
29. Mori Y, Itoi T, Baron TH, Takada T, Strasberg SM, Pitt HA, et al. Tokyo Guidelines 2018: management strategies for gallbladder drainage in patients with acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. (2018) 25:87–95. doi: 10.1002/jhbp.504
30. Endo I, Takada T, Hwang T-L, Akazawa K, Mori R, Miura F, et al. Optimal treatment strategy for acute cholecystitis based on predictive factors: Japan-Taiwan multicenter cohort study. J Hepato Biliary Pancreat Sci. (2017) 24:346–61. doi: 10.1002/jhbp.456
31. Ferrarese AG, Solej M, Enrico S, Falcone A, Catalano S, Pozzi G, et al. Elective and emergency laparoscopic cholecystectomy in the elderly: our experience. BMC Surg. (2013) 13(Suppl. 2):S21. doi: 10.1186/1471-2482-13-S2-S21
32. Lau H, Lo CY, Patil NG, Yuen WK. Early versus delayed-interval laparoscopic cholecystectomy for acute cholecystitis: a metaanalysis. Surg Endosc. (2006) 20:82–7. doi: 10.1007/s00464-005-0100-2
33. Lo CM, Liu CL, Fan ST, Lai EC, Wong J. Prospective randomized study of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Ann Surg. (1998) 227:461–7. doi: 10.1097/00000658-199804000-00001
34. Solej M, Martino V, Mao P, Enrico S, Rosa R, Fornari M, et al. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Minerva Chir. (2012) 67:381–7.
35. Bresadola V, Intini S, Terrosu G, Baccarani U, Marcellino MG, Sistu M, et al. Intraoperative cholangiography in laparoscopic cholecystectomy during residency in general surgery. Surg Endosc. (2001) 15:812–5. doi: 10.1007/s004640090006
36. Lee VS, Chari RS, Cucchiaro G, Meyers WC. Complications of laparoscopic cholecystectomy. Am J Surg. (1993) 165:527–32. doi: 10.1016/S0002-9610(05)80955-9
Keywords: preliminary study, predictive factor, laparoscopic cholecystectomy, drain placement, retrospective study
Citation: Calini G, Brollo PP, Quattrin R and Bresadola V (2022) Predictive Factors for Drain Placement After Laparoscopic Cholecystectomy. Front. Surg. 8:786158. doi: 10.3389/fsurg.2021.786158
Received: 29 September 2021; Accepted: 29 December 2021;
Published: 02 February 2022.
Edited by:
Sanoop Koshy Zachariah, Kerala Institute of Medical Sciences (KIMS), IndiaCopyright © 2022 Calini, Brollo, Quattrin and Bresadola. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vittorio Bresadola, dml0dG9yaW8uYnJlc2Fkb2xhQHVuaXVkLml0; orcid.org/0000-0002-0098-3540
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.