
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 22 November 2021
Sec. Surgical Oncology
Volume 8 - 2021 | https://doi.org/10.3389/fsurg.2021.764887
This article is part of the Research Topic Novel Insights into the Treatment of HCC and Liver Tumors View all 41 articles
 Jiamin Zhou1,2†
Jiamin Zhou1,2† Xigan He1,2†Miao Wang1,2
Xigan He1,2†Miao Wang1,2 Yiming Zhao1,2Ning Zhang1,2Longrong Wang1,2Anrong Mao1,2*Lu Wang1,2*
Yiming Zhao1,2Ning Zhang1,2Longrong Wang1,2Anrong Mao1,2*Lu Wang1,2*Objective: To compare the effectiveness and safety of enhanced recovery after surgery (ERAS) in patients with hepatocellular carcinoma (HCC) undergoing laparoscopic hepatectomy.
Methods: From September 2016 to June 2019, 282 patients were enrolled, and ERAS was implemented since March 2018. All indicators related to surgery, liver function, and postoperative outcomes were included in the analysis. Propensity score matching (PSM) identified 174 patients for further comparison.
Results: After PSM, the clinicopathological baselines were well-matched. The group showed significantly less intraoperative blood loss (100.00 [100.00–200.00] vs. 200.00 [100.00–300.00] ml, P = 0.001), fewer days before abdominal drainage tube removal (4.00 [3.00–4.00] days vs. 4.00 [3.00–5.00] days, P = 0.023), shorter hospital stay after surgery (6.00 [5.00–6.00] days vs. 6.00 [6.00–7.00] days, P < 0.001), and reduced postoperative morbidity (18.39 vs. 34.48%, P = 0.026). The proportion of patients with a pain score ≥ 4 was significantly lower in the ERAS group within the first 2 days after surgery (1.15 vs. 13.79% and 8.05 vs. 26.44%, P = 0.002 and P = 0.001, respectively). Pringle maneuver was performed more frequently in the ERAS group (70.11 vs. 18.39%, P < 0.001), and a significantly higher postoperative alanine aminotransferase level was also observed (183.40 [122.85–253.70] vs. 136.20 [82.93–263.40] U/l, P = 0.026). The 2-year recurrence-free survival was similar between the two groups (72 vs. 71%, P = 0.946).
Conclusions: ERAS programs are feasible and safe and do not influence mid-term recurrence in HCC patients undergoing laparoscopic hepatectomy.
Since enhanced recovery after surgery (ERAS) programs were introduced by Kehlet in the 1990's, they have been widely applied in gastrointestinal, urologic, gynecological, orthopedic surgery, and many other surgical fields to minimize perioperative pain and stress, reduce morbidity, and accelerate postoperative recovery worldwide (1–11). Furthermore, the concept of ERAS is constantly being updated with continuous clinical practice (4).
Although the implementation of ERAS programs in hepatic surgery was slightly later than in other surgical fields (12), many randomized controlled trials (RCTs), meta-analyses, and guidelines and consensus have been performed or established specifically focusing on hepatectomy (13–20). However, most of the studies have only focused on the hepatectomy itself, while the type of liver tumors and the type of surgical approach used in these studies were always mixed.
Hepatocellular carcinoma (HCC) is still one of the leading causes of cancer-related mortality, especially in China. Most cases of hepatitis B virus (HBV)-related HCC occur in patients with cirrhosis (21, 22). In several previous studies, ERAS programs were considered to be beneficial to HCC patients, especially in patients with cirrhosis that may partly be attributed to the omission of overnight fasting and carbohydrate loading, which may lessen the nutritional stress (23, 24). However, only a few studies have focused on this field.
Since the second international consensus conference for laparoscopic liver resection in 2014, laparoscopic minor hepatectomy was the standard surgical practice (25). In addition, laparoscopic major hepatectomy was gradually accepted for its safety, feasibility, and good short- and long-term outcomes, including in HCC patients with cirrhosis in recent years (26, 27). Although many previous studies have explored the recovery of patients undergoing both ERAS programs and laparoscopic hepatectomy (LH), their results did not seem to be consistent (16, 23, 28, 29). The results might also be due to the mismatch of the type of liver tumors and the ratio of LH among these studies. Thus, it is meaningful to focus on the role of ERAS programs in patients with HCC undergoing LH.
Therefore, this study aimed to compare the effectiveness and safety of ERAS in patients with HCC undergoing LH.
The inclusion criteria were as follows: (1) patients were pathologically confirmed to have HCC after surgery; (2) all surgical procedures were successfully performed by laparoscopy; (3) radical resection was achieved; and (4) preoperative liver function was Child-Pugh A or B. The exclusion criteria were as follows: (1) patients underwent laparoscopic radiofrequency ablation alone, and (2) laparoscopic surgery was converted to open surgery for any reason. From September 2016 to June 2019, 282 eligible patients in the Department of Hepatic Surgery, Shanghai Cancer Center, Fudan University, were enrolled in the study retrospectively. ERAS programs were implemented in our center on March 1, 2018. All the patients who were suitable for undergoing LH routinely followed the ERAS protocol. Therefore, 108 patients from September 2016 to February 2018 were enrolled in the control group, and the subsequent 174 patients were enrolled in the ERAS group. All surgical operations were performed by the team of Prof. Lu Wang. This study was approved by the Research Ethics Committee of Shanghai Cancer Center, Fudan University.
Enhanced recovery after surgery (ERAS) management measures at our center were introduced in our previous study (30) and are briefly described in Table 1. The underlying diseases of the patients were defined as cardiovascular disease, cerebrovascular disease, hypertension, diabetes, and other chronic diseases, namely, chronic bronchitis, chronic kidney disease, and rheumatoid arthritis. HBV infection referred to patients with HBsAg positivity, regardless of whether the HBV DNA was replicating or not. The tumor stage was defined according to the Barcelona Clinic Liver Cancer (BCLC) staging. Postoperative complications were defined and classified according to the Clavien–Dindo classification criteria. The pain score was classified according to the visual analog scale, and a score ≥ 4 was defined as severe pain requiring analgesic treatment. Four liver function-related indicators, namely, alanine aminotransferase (ALT), total bilirubin (TB), prothrombin time (PT), and prealbumin (PAB), were used to express the postoperative recovery of liver function, all of which were recorded before the surgery and on the 3rd day after surgery. Abdominal contrast-enhanced computed tomography scanning or magnetic resonance imaging, serum alpha-fetoprotein levels, and chest radiographs were monitored at an interval of 3 months after liver resection within the first 2 years. Recurrence-free survival (RFS) was defined as the interval between surgery and recurrence. If recurrence was not diagnosed, patients were censored on the date of death or the last follow-up. Two years was generally set as the cutoff value to define early recurrence (31).
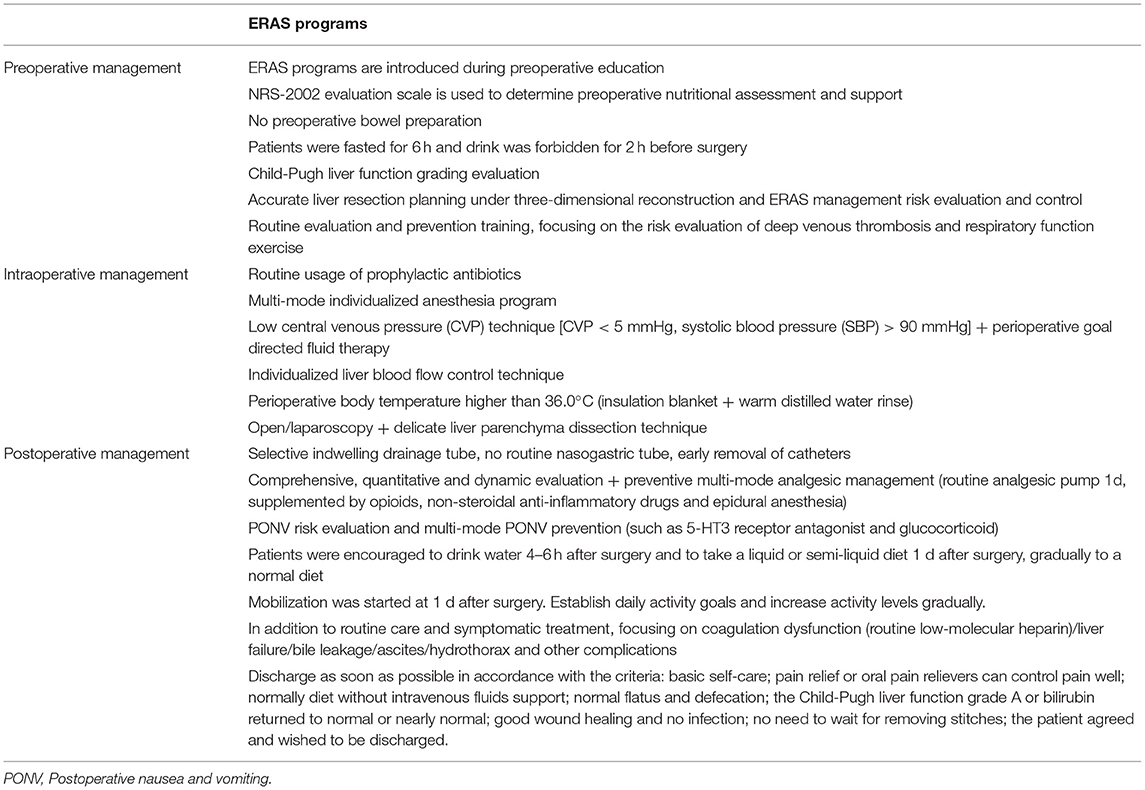
Table 1. Enhanced recovery after surgery (ERAS) programs in our center.
Propensity score matching (PSM) analysis was performed in this study to reduce bias in patient selection using SPSS 22.0 for Windows (SPSS Inc., Chicago, IL, USA). The variables in the clinicopathological baseline that were not balanced and might affect the results, namely, age, sex, underlying diseases, HBV infection, American Society of Anesthesiologists (ASA) score, body mass index (BMI), preoperative level of ALT, TB, PT, PAB, and type of hepatectomy were included in the calculation. The propensity score was generated using logistic regression with these variables, and the caliper value was set to 0.02. The patients were selected using nearest-neighbor matching without replacement at a ratio of 1:1. A two-sample Student's t-test or Mann–Whitney U-test was performed to compare quantitative variables. For data analyzed with a two-sample Student's t-test, the data were presented as mean ± standard error, and for data analyzed with Mann–Whitney U test, the data were presented as median (interquartile range). Pearson's χ2 test or Fisher's exact test was used to comparing qualitative variables. Statistical analyses were performed using the SPSS 22.0. Plot analysis was performed using GraphPad Prism 5 for Windows (GraphPad Software, Inc. San Diego, CA, USA). Statistical significance was set at P < 0.05.
A total of 282 patients were recruited for this study. Among these, 108 patients (38.30%) received traditional perioperative care in the control group, and 174 patients (61.70%) received ERAS programs in the ERAS group. The clinicopathological characteristics of these cohorts are summarized in Table 2. The sex, HBV infection, BMI, preoperative TB, PT, PAB, type of hepatectomy, and BCLC stage of patients in these two groups were balanced. However, a significantly higher proportion of elderly patients (P = 0.025), patients with underlying diseases (P = 0.010), higher ASA scores (P = 0.017), and lower preoperative ALT levels (P = 0.032) were observed in the ERAS group.
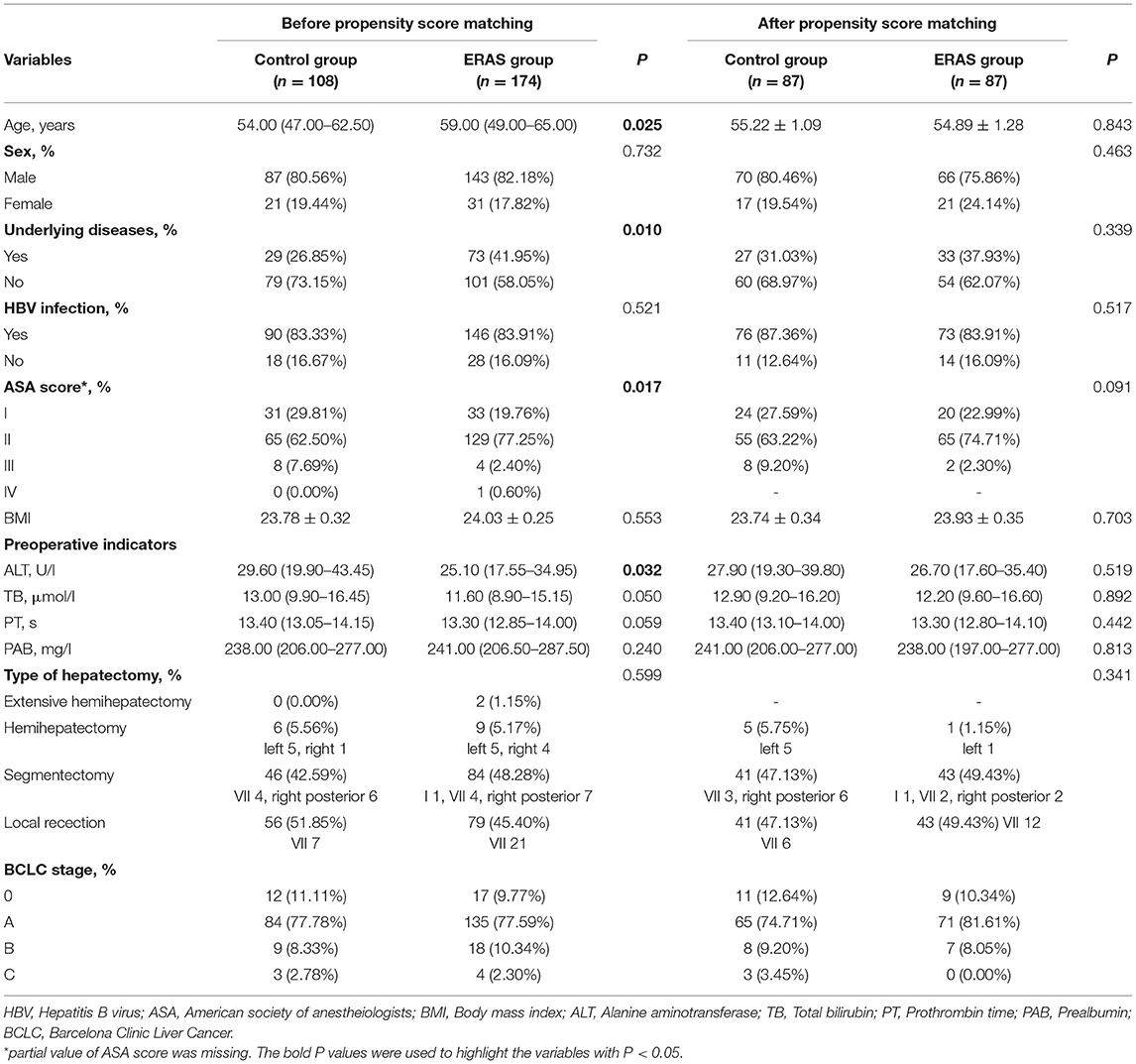
Table 2. The clinicopathological characteristics of patients.
The operative results and postoperative outcomes in the entire patient population are shown in Table 3. As for the operation-related indicators, significantly less intraoperative blood loss was observed in the ERAS group (200.00 [100.00–400.00] vs. 175.00 [100.00–275.00] ml, P = 0.009). Although the proportion of intraoperative blood transfusion was similar (5.56 vs. 3.45%, P = 0.545) in the two groups, the type of hepatectomy was different (control group: segmentectomy 3 and local resection 3 vs. ERAS group: extensive hemihepatectomy 1, segmentectomy 4, and local resection 1). The use of the Pringle maneuver was also significantly more frequent in the ERAS group (66.10 vs. 17.59%, P < 0.001). As an indicator of postoperative liver function recovery, the TB level was significantly lower in the ERAS group (24.00 [18.00–35.00] vs. 27.25 [22.68–41.63] μmol/l, P = 0.002), while the ALT, PT, and PAB levels showed no significant difference between these two groups. The postoperative outcomes, namely, the days that semiliquid diet was allowed after surgery and hospital stay after surgery, were significantly less in the ERAS group (2.00 [2.00–2.00] days vs. 3.00 [3.00–4.00] days and 6.00 [5.00–6.00] days vs. 6.00 [6.00–7.00] days, both P < 0.001). In terms of pain score, the proportion of patients with a score ≥ 4 was significantly lower in the ERAS group within the first 2 days after surgery (2.87 vs. 12.96% and 9.77 vs. 24.07%, both P < 0.001). There was no significant difference in the abdominal drainage tube indwelling duration and the hospital costs between these two groups were also similar (47,069.39 [40,980.86–54,488.74] CNY vs. 49,498.55 [42,812.30–57,936.92] CNY, P = 0.158). The incidence of complications was not significantly different between the two groups (25.29 vs. 36.11%, P = 0.182). Furthermore, the 2-year RFS was similar between the two groups (71 vs. 72%, P = 0.887).
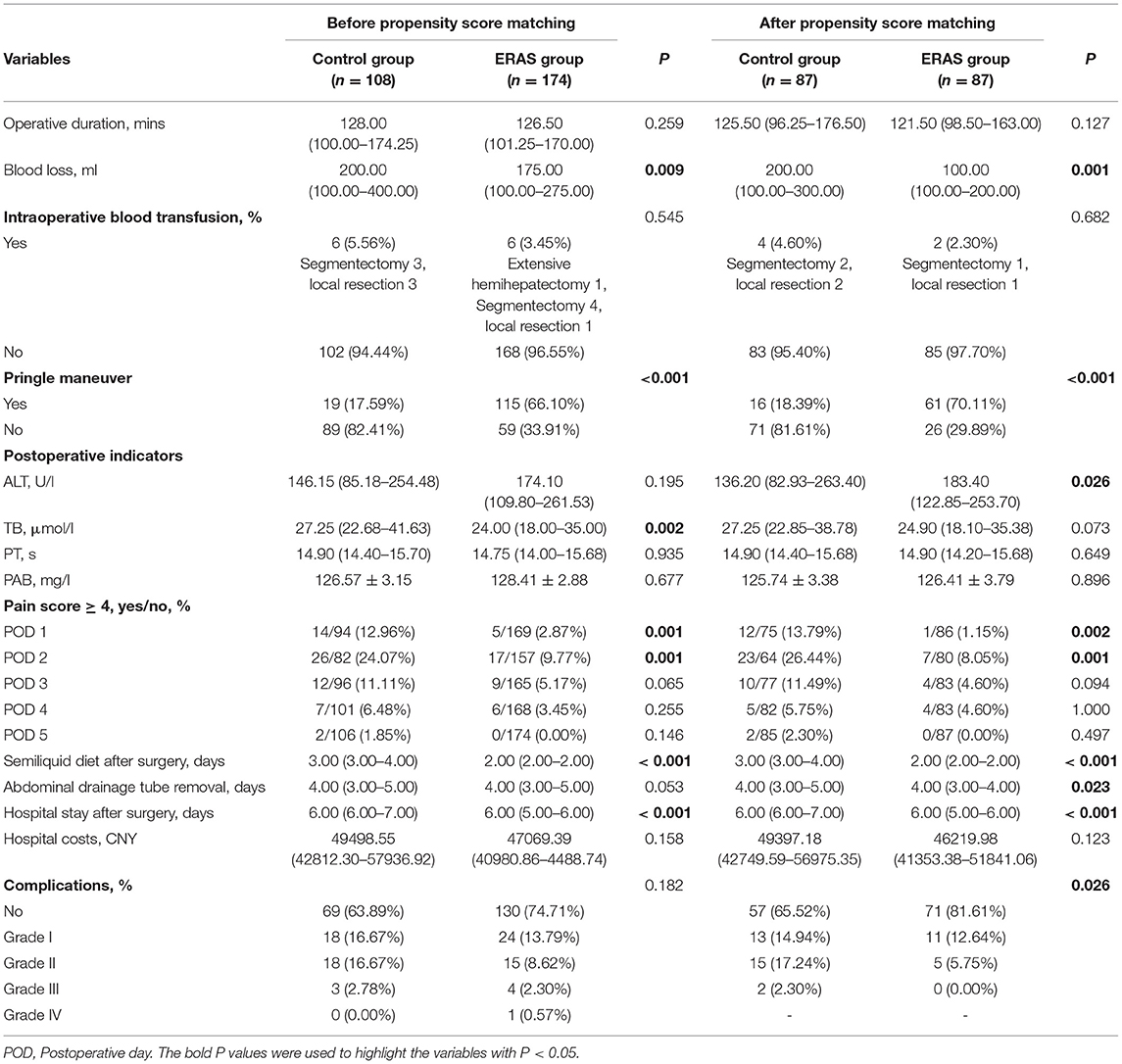
Table 3. The operative results and postoperative outcomes.
After PSM, the clinicopathological baselines of the two groups were well-matched (Table 2). In the operation-related indicators, the ERAS group showed significantly less intraoperative blood loss than the control group (100.00 [100.00–200.00] vs. 200.00 [100.00–300.00] ml, P = 0.001). The proportion of patients with intraoperative blood transfusion was slightly more in the control group (4.60 vs. 2.30%, P = 0.682) and the type of hepatectomy between the two groups was similar (control group: segmentectomy 2 and local resection 2 vs. ERAS group: segmentectomy 1 and local resection 1). The operative duration and intraoperative blood transfusion did not demonstrate any obvious differences. The Pringle maneuver was performed more frequently in the ERAS group (70.11 vs. 18.39%, P < 0.001). Impressively, in the liver function recovery indicators, the ALT level in the ERAS group was significantly higher than that in the control group (183.40 [122.85–253.70] vs. 136.20 [82.93–263.40] U/l, P = 0.026), which was completely consistent with the results of our previous study (30). On the contrary, the TB level in the ERAS group was lower than that in the control group, although the difference was not significant (24.90 [18.10–35.38] vs. 27.25 [22.85–38.78] U/l, P = 0.073). PT and PAB levels were also similar between the two groups.
In the postoperative outcomes, the ERAS group showed significantly fewer days that a semiliquid diet was allowed (2.00 [2.00–2.00] days vs. 3.00 [3.00–4.00] days, P < 0.001), abdominal drainage tube removal (4.00 [3.00–4.00] days vs. 4.00 [3.00–5.00] days, P = 0.023), and hospital stay after surgery (6.00 [5.00–6.00] days vs. 6.00 [6.00–7.00] days, P < 0.001) than in the control group. Similar to that before PSM, the proportion of patients with a pain score ≥ 4 was significantly lower in the ERAS group within the first 2 days after surgery (1.15 vs. 13.79% and 8.05 vs. 26.44%, P = 0.002 and P = 0.001, respectively). In the patient population after PSM, there was also no significant difference in the hospital costs between these two groups (46,219.98 [41,353.38–51,841.06] CNY vs. 49,397.18 [42,749.59–56,975.35] CNY, P = 0.123). Interestingly, the ERAS group demonstrated significantly less postoperative morbidity (18.39 vs. 34.48%, P = 0.026) after PSM. Furthermore, after PSM, 2-year RFS was similar in these two groups (72 vs. 71%, P = 0.946).
Laparoscopic hepatectomy (LH) has been considered as a landmark development in the progression of a surgical treatment since it was gradually introduced to cure liver lesions in the 1990s (32, 33). LH was first applied to a patient with HCC in 1998 (34). The majority of HCC patients were infected with HBV (appropriate 85% of patients in this study), which caused cirrhosis or at least an inflammatory background in the liver. Thus, the surgical risk of LH correspondingly increased. Compared with open hepatectomy, LH showed better surgical safety, faster postoperative recovery, and comparable long-term survival (35). LH itself could be regarded as an ERAS approach to reduce the impact of surgery on HCC patients (20, 36, 37). The combination of LH and ERAS programs seemed to demonstrate lower postoperative morbidity and more satisfactory functional recovery than open surgery in both minor and major liver resections (37, 38), although several meta-analyses have yielded inconsistent conclusions (15, 16, 28, 29, 39).
In this study, PSM was performed to minimize the confounding bias of the baselines due to the retrospective design. Early abdominal drainage tube removal, better pain control, shorter hospital stay, and lower postoperative morbidity after ERAS were confirmed. These results proved the effectiveness of ERAS programs in patients with HCC who had undergone LH. Furthermore, alterations in postoperative liver function and mid-term recurrence were also investigated in these patients. Several representative indicators, namely, ALT, TB, and PT were selected, and these indicators generally peaked on the 3rd day after surgery. The postoperative ALT level was significantly higher in the ERAS group. Conversely, the TB level was lower in the ERAS group, although the difference was not statistically significant. The PT levels were also not affected. Similar results were also observed in LH, but not open surgery, in our previous study (30). These indicators reflected that liver function was stable and trended to recover faster. The increasing level of ALT revealed that laparoscopic surgery combined with controlled low central venous pressure (CVP) according to the ERAS programs might enhance the ischemia-reperfusion injury (IRI) of the liver. Laparoscopic pneumoperitoneum can also cause hepatic IRI as a result of the temporary decrease in blood inflow into the portal vein (40, 41). Above all, the Pringle maneuver was performed more frequently in the ERAS group. Laparoscopic Pringle maneuver combined with low CVP obviously decreased intraoperative blood loss and tended to reduce the proportion of blood transfusion, which made LH safer. Meanwhile, low inflow and easy outflow reduce the amount of residual blood in the liver, which inevitably increases the severity of IRI (42, 43). The enrollment design of this study had a chronological sequence and the appropriate laparoscopic Pringle maneuver was gradually determined and more frequently used in the development of LH in our center, which made the Pringle maneuver used more in the ERAS group. Regardless of enhanced IRI, the laparoscopic Pringle maneuver might be considered as a step in ERAS programs.
Few studies have explored the role of ERAS programs in long-term or mid-term survival. Recently, stage III gastric cancer patients undergoing laparoscopic radical gastrectomy were verified to have a survival benefit from ERAS implementation (44). In colon cancer, laparoscopic surgery combined with ERAS has a longer overall survival than open surgery combined with ERAS (45). The potential explanations are as follows: (1) reducing stress might improve antitumor immunity and (2) quick recovery reduces delayed adjuvant therapy. Two years after surgery is a significant recurrence timing of HCC, and 2-year recurrence has an obvious influence on long-term prognosis (31). Our results showed no difference in 2-year RFS between the two groups. The potential explanation is that there is no standard adjuvant therapy for HCC, and thus, the implementation of adjuvant therapy would not be affected by ERAS. At the same time, both groups in this study were laparoscopic surgery groups, in which the role of the ERAS program alone on prognosis might be limited. In fact, ERAS implementation did not improve patient survival in all tumors (46).
Generally, in HCC patients undergoing LH, ERAS programs were verified to improve postoperative recovery significantly but did not show their role in 2-year recurrence. Although hepatic IRI might be enhanced, laparoscopic Pringle maneuver combined with low CVP might make LH safer by improving intraoperative blood loss, which should be considered as a step of ERAS programs. Although PSM was used to reduce confounding bias and make the conclusion more convincing, a following prospective RCT is still necessary to further confirm the conclusion.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Shanghai Cancer Center, Fudan University. The patients/participants provided their written informed consent to participate in this study.
Study concept: AM and LW. Data collection: JZ and XH. First draft: JZ. Data analysis and review and editing: All authors.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. (1997) 78:606–17. doi: 10.1093/bja/78.5.606
2. Kehlet H, Dahl JB. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet. (2003) 362:1921–8. doi: 10.1016/S0140-6736(03)14966-5
3. Kehlet H, Wilmore DW. Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg. (2008) 248:189–98. doi: 10.1097/SLA.0b013e31817f2c1a
4. Schultz NA, Larsen PN, Klarskov B, Plum LM, Frederiksen HJ, Kehlet H, et al. Second generation of a fast-track liver resection programme. World J Surg. (2018) 42:1860–6. doi: 10.1007/s00268-017-4399-3
5. Muehling B, Schelzig H, Steffen P, Meierhenrich R, Sunder-Plassmann L, Orend KH. A prospective randomized trial comparing traditional and fast-track patient care in elective open infrarenal aneurysm repair. World J Surg. (2009) 33:577–85. doi: 10.1007/s00268-008-9892-2
6. Kim JW, Kim WS, Cheong JH, Hyung WJ, Choi SH, Noh SH. Safety and efficacy of fast-track surgery in laparoscopic distal gastrectomy for gastric cancer: a randomized clinical trial. World J Surg. (2012) 36:2879–87. doi: 10.1007/s00268-012-1741-7
7. Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for perioperative care in elective colorectal surgery: enhanced recovery after surgery (ERAS((R))) society recommendations: 2018. World J Surg. (2019) 43:659–95. doi: 10.1007/s00268-018-4844-y
8. Hu ZC, He LJ, Chen D, Li XB, Feng ZH, Fu CW, et al. An enhanced recovery after surgery program in orthopedic surgery: a systematic review and meta-analysis. J Orthop Surg Res. (2019) 14:77. doi: 10.1186/s13018-019-1116-y
9. Macones GA, Caughey AB, Wood SL, Wrench IJ, Huang J, Norman M, et al. Guidelines for postoperative care in cesarean delivery: Enhanced Recovery After Surgery (ERAS) Society recommendations (part 3). Am J Obstet Gynecol. (2019) 221:247.e1–247.e9. doi: 10.1016/j.ajog.2019.04.012
10. Moschini M, Stabile A, Mattei A, Montorsi F, Cathelineau X, Sanchez-Salas R. Enhanced recovery after surgery (ERAS) in radical cystectomy patients: from consensus to evidences. Int Braz J Urol. (2019) 45:655–7. doi: 10.1590/s1677-5538.ibju.2019.04.02
11. Pache B, Joliat GR, Hubner M, Grass F, Demartines N, Mathevet P, et al. Cost-analysis of enhanced recovery after surgery (ERAS) program in gynecologic surgery. Gynecol Oncol. (2019) 154:388–93. doi: 10.1016/j.ygyno.2019.06.004
12. van Dam Hendry PO, Coolsen MME, Bemelmans MHA, Lassen K, Revhaug A, Fearon KCH, et al. Initial experience with a multimodal enhanced recovery programme in patients undergoing liver resection. Brit J Surg. (2008) 95:969–75. doi: 10.1002/bjs.6227
13. Qi S, Chen G, Cao P, Hu J, He G, Luo J, et al. Safety and efficacy of enhanced recovery after surgery (ERAS) programs in patients undergoing hepatectomy: A prospective randomized controlled trial. J Clin Lab Anal. (2018) 32:e22434. doi: 10.1002/jcla.22434
14. Ni CY, Wang ZH, Huang ZP, Zhou H, Fu LJ, Cai H, et al. Early enforced mobilization after liver resection: A prospective randomized controlled trial. Int J Surg. (2018) 54:254–8. doi: 10.1016/j.ijsu.2018.04.060
15. Liang X, Ying H, Wang H, Xu H, Liu M, Zhou H, et al. Enhanced recovery care versus traditional care after laparoscopic liver resections: a randomized controlled trial. Surg Endosc. (2018) 32:2746–57. doi: 10.1007/s00464-017-5973-3
16. Rouxel P, Beloeil H. Enhanced recovery after hepatectomy: A systematic review. Anaesth Crit Care Pain Med. (2019) 38:29–34. doi: 10.1016/j.accpm.2018.05.003
17. Damania R, Cocieru A. Impact of enhanced recovery after surgery protocols on postoperative morbidity and mortality in patients undergoing routine hepatectomy: review of the current evidence. Ann Transl Med. (2017) 5:341. doi: 10.21037/atm.2017.07.04
18. Wang C, Zheng G, Zhang W, Zhang F, Lv S, Wang A, et al. Enhanced recovery after surgery programs for liver resection: a meta-analysis. J Gastrointest Surg. (2017) 21:472–86. doi: 10.1007/s11605-017-3360-y
19. Melloul E, Hubner M, Scott M, Snowden C, Prentis J, Dejong CH, et al. Guidelines for perioperative care for liver surgery: enhanced recovery after surgery (ERAS) society recommendations. World J Surg. (2016) 40:2425–40. doi: 10.1007/s00268-016-3700-1
20. Jia W, Liu W, Qiao X. Chinese expert consensus on enhanced recovery after hepatectomy (Version 2017). Asian J Surg. (2019) 42:11–8. doi: 10.1016/j.asjsur.2018.01.007
21. Kulik L, El-Serag HB. Epidemiology and management of hepatocellular carcinoma. Gastroenterology. (2019) 156:477–91.e1. doi: 10.1053/j.gastro.2018.08.065
22. Sayiner M, Golabi P, Younossi ZM. Disease burden of hepatocellular carcinoma: a global perspective. Dig Dis Sci. (2019) 64:910–7. doi: 10.1007/s10620-019-05537-2
23. Chong CCN, Chung WY, Cheung YS, Fung AKY, Fong AKW, Lok HT, et al. Enhanced recovery after surgery for liver resection. Hong Kong Med J. (2019) 25:94–101. doi: 10.12809/hkmj187656
24. Kaibori M, Matsui K, Ishizaki M, Iida H, Yoshii K, Asano H, et al. Effects of implementing an “enhanced recovery after surgery” program on patients undergoing resection of hepatocellular carcinoma. Surg Today. (2017) 47:42–51. doi: 10.1007/s00595-016-1344-2
25. Wakabayashi G, Cherqui D, Geller DA, Buell JF, Kaneko H, Han HS, et al. Recommendations for laparoscopic liver resection: a report from the second international consensus conference held in Morioka. Ann Surg. (2015) 261:619–29. doi: 10.1097/SLA.0000000000001184
26. Xu HW, Liu F, Li HY, Wei YG, Li B. Outcomes following laparoscopic versus open major hepatectomy for hepatocellular carcinoma in patients with cirrhosis: a propensity score-matched analysis. Surg Endosc. (2018) 32:712–9. doi: 10.1007/s00464-017-5727-2
27. Shehta A, Han HS, Yoon YS, Cho JY, Choi Y. Laparoscopic liver resection for hepatocellular carcinoma in cirrhotic patients: 10-year single-center experience. Surg Endosc. (2016) 30:638–48. doi: 10.1007/s00464-015-4253-3
28. Liang X, Ying H, Wang H, Xu H, Yu H, Cai L, et al. Enhanced recovery program versus traditional care in laparoscopic hepatectomy. Medicine (Baltimore). (2016) 95:e2835. doi: 10.1097/MD.0000000000002835
29. Li L, Chen J, Liu Z, Li Q, Shi Y. Enhanced recovery program versus traditional care after hepatectomy: A meta-analysis. Medicine (Baltimore). (2017) 96:e8052. doi: 10.1097/MD.0000000000008052
30. Zhou JM, He XG, Wang M, Zhao YM, Shu L, Wang LR, et al. Enhanced recovery after surgery program in the patients undergoing hepatectomy for benign liver lesions. Hepatobiliary Pancreat Dis Int. (2020) 19:122–8. doi: 10.1016/j.hbpd.2019.12.012
31. Wang MD, Li C, Liang L, Xing H, Sun LY, Quan B, et al. Early and late recurrence of Hepatitis B virus-associated hepatocellular carcinoma. Oncologist. (2020) 25:e1541–51. doi: 10.1634/theoncologist.2019-0944
32. Klotz HP, Schlumpf R, Weder W, Largiader F. Minimal invasive surgery for treatment of enlarged symptomatic liver cysts. Surg Laparosc Endosc. (1993) 3:351–3.
33. Kaneko H, Takagi S, Shiba T. Laparoscopic partial hepatectomy and left lateral segmentectomy: technique and results of a clinical series. Surgery. (1996) 120:468–75. doi: 10.1016/S0039-6060(96)80065-1
34. Mizoe A, Tomioka T, Inoue K, Azuma T, Fujioka H, Furui J, et al. Systematic laparoscopic left lateral segmentectomy of the liver for hepatocellular carcinoma. J Hepatobiliary Pancreat Surg. (1998) 5:173–8. doi: 10.1007/s005340050029
35. Chen K, Pan Y, Zhang B, Liu XL, Maher H, Zheng XY. Laparoscopic versus open surgery for hepatocellular carcinoma: a meta-analysis of high-quality case-matched studies. Can J Gastroenterol Hepatol. (2018) 2018:1746895. doi: 10.1155/2018/1746895
36. Ratti F, Cipriani F, Reineke R, Catena M, Comotti L, Beretta L, et al. Impact of ERAS approach and minimally-invasive techniques on outcome of patients undergoing liver surgery for hepatocellular carcinoma. Dig Liver Dis. (2016) 48:1243–8. doi: 10.1016/j.dld.2016.06.032
37. Pagano D, Ricotta C, Barbàra M, Cintorino D, di Francesco F, Tropea A, et al. ERAS protocol for perioperative care of patients treated with laparoscopic nonanatomic liver resection for hepatocellular carcinoma: the ISMETT experience. J Laparoendosc Adv Surg Tech A. (2020) 30:1066–71. doi: 10.1089/lap.2020.0445
38. Ratti F, Cipriani F, Reineke R, Comotti L, Paganelli M, Catena M, et al. The clinical and biological impacts of the implementation of fast-track perioperative programs in complex liver resections: A propensity score-based analysis between the open and laparoscopic approaches. Surgery. (2018) 164:395–403. doi: 10.1016/j.surg.2018.04.020
39. He F, Lin X, Xie F, Huang Y, Yuan R. The effect of enhanced recovery program for patients undergoing partial laparoscopic hepatectomy of liver cancer. Clin Transl Oncol. (2015) 17:694–701. doi: 10.1007/s12094-015-1296-9
40. Hasegawa Y, Nitta H, Takahara T, Katagiri H, Kanno S, Umemura A, et al. Glucocorticoid use and ischemia-reperfusion injury in laparoscopic liver resection: Randomized controlled trial. Ann Gastroenterol Surg. (2020) 4:76–83. doi: 10.1002/ags3.12298
41. Lai H, Mo X, Yang Y, Xiao J, He K, Chen J, et al. Association between duration of carbon dioxide pneumoperitoneum during laparoscopic abdominal surgery and hepatic injury: a meta-analysis. PLoS ONE. (2014) 9:e104067. doi: 10.1371/journal.pone.0104067
42. Xia F, Wang S, Chen M, Wang X, Feng X, Dong J. Protective effect of Verapamil on hepatic ischemia-reperfusion injury during hepatectomy in the cirrhotic patients with hepatocellular carcinoma. Langenbecks Arch Surg. (2009) 394:1041–6. doi: 10.1007/s00423-009-0491-y
43. Hughes MJ, Ventham NT, Harrison EM, Wigmore SJ. Central venous pressure and liver resection: a systematic review and meta-analysis. HPB. (2015) 17:863–71. doi: 10.1111/hpb.12462
44. Tian YL, Cao SG, Liu XD, Li ZQ, Liu G, Zhang XQ, et al. Short- and long-term outcomes associated with enhanced recovery after surgery protocol vs conventional management in patients undergoing laparoscopic gastrectomy. World J Gastroenterol. (2020) 26:5646–60. doi: 10.3748/wjg.v26.i37.5646
45. Curtis NJ, Taylor M, Fraser L, Salib E, Noble E, Hipkiss R, et al. Can the combination of laparoscopy and enhanced recovery improve long-term survival after elective colorectal cancer surgery? Int J Colorectal Dis. (2018) 33:231–4. doi: 10.1007/s00384-017-2935-0
46. Ziegelmueller BK, Jokisch JF, Buchner A, Grimm T, Kretschmer A, Schulz GB, et al. Long-term follow-up and oncological outcome of patients undergoing radical cystectomy for bladder cancer following an enhanced recovery after surgery (ERAS) protocol: results of a large randomized, prospective, single-center study. Urol Int. (2020) 104:55–61. doi: 10.1159/000504236
Keywords: enhanced recovery after surgery, hepatocellular carcinoma, hepatectomy, laparoscopy, liver function
Citation: Zhou J, He X, Wang M, Zhao Y, Zhang N, Wang L, Mao A and Wang L (2021) Enhanced Recovery After Surgery in Patients With Hepatocellular Carcinoma Undergoing Laparoscopic Hepatectomy. Front. Surg. 8:764887. doi: 10.3389/fsurg.2021.764887
Received: 26 August 2021; Accepted: 21 October 2021;
Published: 22 November 2021.
Edited by:
Alessandro Vitale, University Hospital of Padua, ItalyReviewed by:
Duilio Pagano, Mediterranean Institute for Transplantation and Highly Specialized Therapies (ISMETT), ItalyCopyright © 2021 Zhou, He, Wang, Zhao, Zhang, Wang, Mao and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anrong Mao, MTMwMjAxNDMwNjBAMTYzLmNvbQ==; Lu Wang, d2FuZy5sdTk5QGhvdG1haWwuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.