
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg., 08 November 2021
Sec. Genitourinary Surgery and Interventions
Volume 8 - 2021 | https://doi.org/10.3389/fsurg.2021.759487
This article is part of the Research TopicRecent Advances in Bladder Cancer Diagnosis and TreatmentView all 10 articles
 Zheng Liu1,2†
Zheng Liu1,2† Gongwei Long1,2†
Gongwei Long1,2† Yucong Zhang1,2,3
Yucong Zhang1,2,3 Guoliang Sun1,2Wei Ouyang1,2Shen Wang1,2Hao Xu1,2Zhihua Wang1,2Wei Guan1,2Xiao Yu1,2
Guoliang Sun1,2Wei Ouyang1,2Shen Wang1,2Hao Xu1,2Zhihua Wang1,2Wei Guan1,2Xiao Yu1,2 Zhiquan Hu1,2Zhong Chen1,2
Zhiquan Hu1,2Zhong Chen1,2 Shaogang Wang1,2*
Shaogang Wang1,2* Heng Li1,2*
Heng Li1,2*Background: Thulium laser resection of bladder tumors (TmLRBT) is recently considered as a common treatment option for non-muscle-invasive bladder cancers (NMIBC), but whether it is superior to Transurethral resection of bladder tumors (TURBT) are still undetermined.
Materials and Methods: We retrospectively screened our institution database to identify patients who were treated by conventional TURBT or TmLRBT for NMIBC and followed by intravesical bacillus Calmette-Guérin (BCG) immunotherapy. The preoperative characteristics, perioperative outcomes, and recurrence-free survival were compared to assess the safety and efficacy of the two procedures.
Results: Eventually, 90 patients who underwent TmLRBT (n = 37) or TURBT (n = 53) followed by intravesical BCG immunotherapy were included. Two groups were similar in baseline characteristics except for the smaller tumor size of the TmLRBT group(1.7 cm vs. 2.2 cm; P = 0.036). Obturator nerve reflex occurred in eight patients in the TURBT group and 3 of them suffered from bladder perforation while none happened in the TmLRBT group. The TmLRBT also had a shorter irrigation duration. In the multivariate Cox regression, the TmLRBT was related to less recurrence risk (HR: 0.268; 95% CI, 0.095–0.759; P = 0.013).
Conclusion: Our results suggested that TmLRBT is safer than conventional TURBT with fewer perioperative complications, and it offers better cancer control, therefore might be a superior option for NMIBC patients with intermediate and high recurrence risk.
Bladder cancer ranks second common urological malignancy worldwide (1). It represents a spectrum of diseases, from non-muscle-invasive bladder cancer (NMIBC), which is defined as the tumor confined to the bladder mucosa or submucosa, to invasiveand advanced diseases that demand aggressive treatment. Approximately 75% of newly diagnosed bladder cancer is NMIBC (2).
The conventional transurethral resection of bladder tumor (TURBT) is the most common strategy for NMIBC and it is recommended by the guidelines (3, 4). However, the TURBT has a complication rate of ~4–6%, of which urinary tract infections and significant haematuria are most common (5). In some cases, major complications including obturator nerve reflex (ONR) and bladder perforation could occur. To overcome these drawbacks, lasers including holmium YAG and thulium YAG were introduced. Several studies have suggested the superior safety of Thulium laser resection of bladder tumors (TmLRBT) compared with conventional TURBT (6, 7).
The TmLRBT is increasingly used in the treatment of NMIBC recently, but whether it can provide better cancer control than TURBT is still unclear. Previous studies have compared the recurrence rates of these two therapies but no significant difference was detected (7). However, in all these studies, intravesical therapies were conducted using epirubicin or mitomycin C, instead of bacillus Calmette-Guérin (BCG), which is superior for preventing the recurrence of NMIBC (8–10). Here we retrospectively collected the data of patients who underwent TmLRBT or TURBT followed by BCG therapy to assess the safety and efficacy of these two therapies.
The study and all its protocols were approved by the institutional review board of the Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (Grant number: TJ-IRB20210106). The informed consent was exempted for this retrospective and observational study. All data has been de-identified.
We accessed our institutional database to retrospectively screened all the patients who were treated by conventional TURBT or TmLRBT from August 2018 to December 2019. The inclusion criteria were as follows. (1) Pathologically confirmed as NMIBC. (2) Underwent conventional TURBT or TmLRBT. (3) Intermediate or high risk according to EAU risk stratification (11). (4) Received standard BCG intravesical therapy. (5) With complete clinical and follow-up data. The exclusion criteria were as follows. (1) Locally advanced (T2 or higher), or metastatic bladder cancers. (2) Loss of contact or inadequate clinical information for further analysis. (3) Unable to finish BCG intravesical therapy due to intolerance or other reasons. (4) Comorbidity of other neoplastic diseases.
The medical records of all patients were retrieved and the baseline characteristics were collected. Ultrasonography, intravenous urography, computerized tomography of urinary system (CTU), and cystoscopy were routinely performed before resection to assess the clinical characteristics of the tumors. All the patients chose TmLRBT or TURBT after being informed of the advantages and drawbacks of the two surgical procedures and signed the informed consent. All the surgeries were performed according to standard protocols which have been described in our previous study (12).
If postoperative gross hematuria occurred after surgery, continuous bladder irrigation would be maintained until no sign of postoperative bleeding for 4 h. 30 mg gemcitabine was used for intravesical instillation therapy within 24 h after surgery for the first time.
For patients with intermediate or high risk (11), intravesical BCG therapy would be recommended. Two weeks after that, according to the drug instructions, 2 g BCG in 50 ml of saline was given weekly for 6 weeks, then biweekly for 6 weeks, and then once a month for 10 months. For high-risk patients, monthly intravesical instillations were added for 1–2 years. The ultrasonography and cystoscopy were performed every 3 months for the first 2 years after surgery for recurrence surveillance. An additional telephone follow-up was conducted for patients who performed examinations in local medical institutions.
The statistical analysis was conducted using the SPSS 20.0 software. Continuous data were presented as mean ± standard deviation and compared using Student's t-test. Categorical data were presented as number (percentage) and compared with the Chi-square or Fisher exact test. Univariate Cox regressions were used to evaluate the predictive role of covariates, including surgery type, age, gender, previous bladder tumor, second resection, tumor number, tumor size, tumor location, pathologic stage, and pathologic grade for recurrence-free survival (RFS). Variables with a P-value <0.1 were furtherly included in multivariate Cox regression. The Kaplan-Meier(K-M) curve of RFS was plotted and the log-rank test was conducted with the Graphpad Prism 8.0.1 software.
Eventually, 37 patients who underwent TmLRBT and 57 patients who conducted TURBT group were enrolled in the analysis. As listed in Table 1, the baseline characteristics such as age, gender, tumor number, tumor stage, and pathological grade were similar between two groups. The tumor size of the TmLRBT is smaller than that of the TURBT group (1.7 cm vs. 2.2 cm; P = 0.036). Nine patients in the TmLRBT group and 6 patients in the TURBT group have a history of bladder tumor and the proportion was comparable in these two groups.
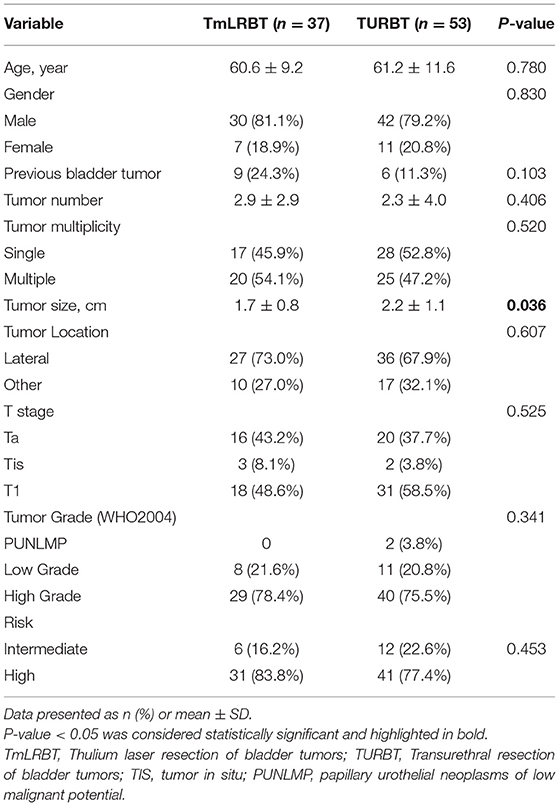
Table 1. Characteristics of included patients and tumors.
The perioperative results of the two groups are illustrated in Table 2. The operation duration of the two groups was similar. During the TURBT, 8 (15.1%) patients encountered ONR, and 3 (5.7%) patients had bladder perforation. Meanwhile, no ONR or bladder perforation occurred during the TmLRBT surgery. After surgery, only one patient in the TURBT group experienced TUR syndrome, and no second surgery for hemostasis was conducted. Postoperative gross hematuria happened in 51 (96.2%) patients in the TURBT group and 16 (43.2%) patients in the TmLRBT group. 50 patients in the TURBT group and 12 patients in the TmLRBT group received postoperative irrigation. Among these patients who underwent postoperative irrigation, the TmLRBT group also has a shorter irrigation duration (6.5 h vs. 24.3 h; P < 0.001) than conventional TURBT. Besides, the TmLRBT could shorten the catheterization time (2.2 d vs. 3.1 d; P = 0.002).
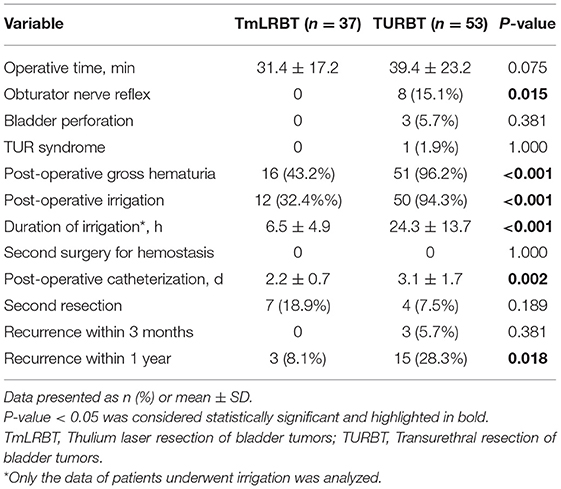
Table 2. Intraoperative, postoperative and oncological outcomes.
The RFS graph was illustrated in Figure 1 and the K-M curve of RFS showed that the TmLRBT group has a longer RFS than the TURBT group (HR: 0.376; 95% CI, 0.162–0.873; Log-rank P = 0.043). Univariate and multivariate Cox regressions were conducted to evaluate the predictive value of variates and the results were shown in Table 3. As the multivariate Cox analysis suggested, the surgery type (HR: 0.268; 95% CI, 0.095–0.759; P = 0.013), history of bladder tumor (HR: 4.319; 95% CI, 1.733–10.769; P = 0.002), and pathologic stage (HR: 3.033; 95% CI, 1.023–8.997; P = 0.045) are independent predictive factors of RFS. Notably, 3 patients who underwent TURBT experienced recurrence within 3 months after the surgery.
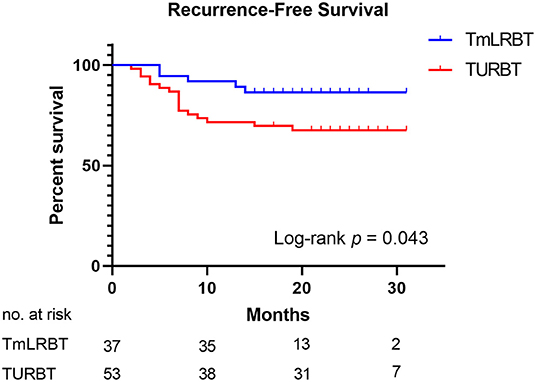
Figure 1. The K-M curve of recurrence-free survival of the patients who underwent TmLRBT or TURBT.
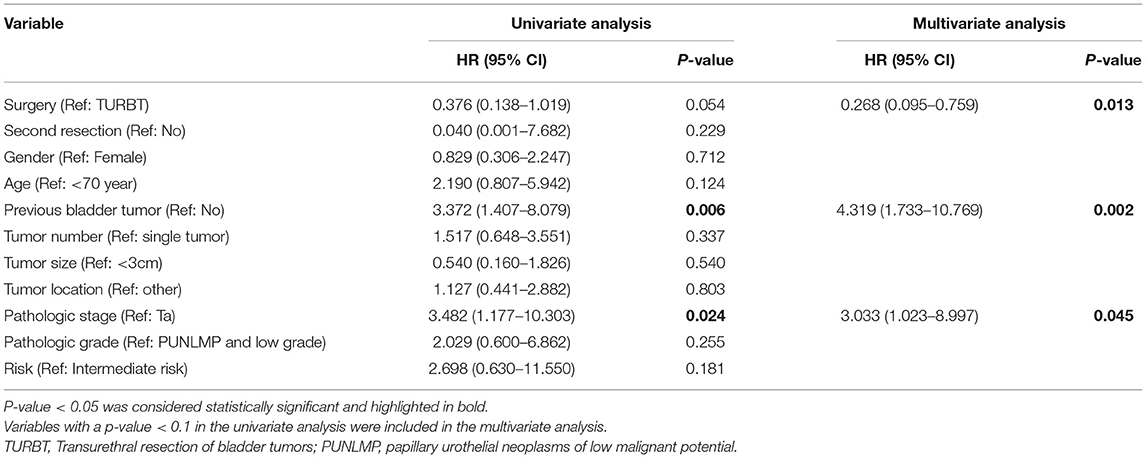
Table 3. Univariate and multivariate Cox analyses of recurrence-free survival.
Currently, TURBT combined with intravesical therapy is still the “gold standard” for intermediate and high risk NMIBC, and BCG immunotherapy is the recommended adjuvant therapy by guidelines (3, 4). Compared with intravesical chemotherapy including epirubicin and mitomycin C, BCG immunotherapy showed better efficacy in recurrence prevention (9, 10). However, in the previous studies comparing the prognosis of TmLRBT and TURBT, BCG immunotherapy was not applied to these patients (13–18). To the best of our knowledge, the present study is the first research to compare the efficacy of TmLRBT and TURBT under BCG intravesical therapy. In this study, over 90% (89 of 90) patients completed intravesical BCG therapy for 1 year. The completion of each groups was summarized in Table 4.
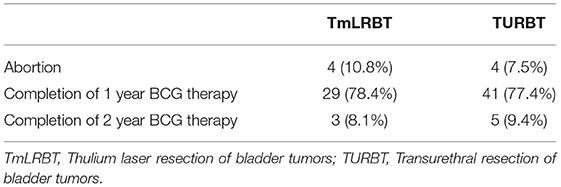
Table 4. Summary of the BCG therapy completion.
Cancer control is the most critical purpose in the treatment of malignancies. The spreading of tumor cells caused by TURBT could be a potential reason for recurrence and progression (19–22). During the TmLRBT procedures, the en bloc technique allows a complete enucleation of lesions and avoid tumor fragmentation. Therefore it can potentially minimize the amount of floating tumor cells and diminish the risk of dissemination (23). However, the previous studies did not suggest a significant advantage of TmLRBT in cancer control. In our analysis, after a standard BCG immunotherapy, the TmLRBT showed superior efficacy in the prevention of recurrence than TURBT, which is quite different from the results of most previous studies, in which postoperative intravesical chemotherapy was applied. On the one hand, compared with previous researches, our research included more patients with pathologic high grades (76.7% vs. 10.0% to 30.0%), T1 or Tis stages(60.0% vs. 26.4% to 48.6%), and most patients were high risk (80%) (14–16, 18). The benefit of TmLRBT might be more significant in these tumors with higher risk. On the other hand, the use of BCG immunotherapy might reinforce cancer control of TmLRBT and both treatments synergically suppressed the recurrence. For these tumors with signs of aggressive properties in the preoperative assessments, TmLRBT might be a preferred option.
The complications of TURBT are an essential concern in the treatment of NMIBC. During the TURBT procedure, especially for tumors locating at the lateral bladder wall, the current flow may stimulate the obturator nerve and lead to muscle contraction. In some cases, it could even bring bladder perforation. Several techniques were developed to prevent ONR during the TURBT, including the use of bipolar electrodes and the obturator nerve block. However, the efficacy of bipolar electrodes in the prevention of ONR is still controversial (24–26). As for the obturator nerve block, to achieve a higher success rate, the assistance of ultrasound or nerve stimulator might be needed and the procedure could be time-consuming and complicated. While in the TmLRBT, no current flow was produced and the ONR and bladder perforation could be perfectly avoided.
Another advantage of TmLRBT is the excellent performance in hemostasis. Under the thulium laser, the exposed tissue could be vaporized after being heated to a temperature of 90–100°C. As for the tissue adjacent to the vaporized part, it could be coagulated under 60–80°C (27). The instantly coagulated tissue layer made the hemostasis more efficient. Several studies suggested that TmLRBT was related to a lower postoperative irrigation rate (14) and a shorter irrigation length (15, 16). In our study, fewer postoperative gross hematuria and a lower postoperative irrigation rate in the TmLRBT group were also observed. Even for these patients who need irrigation, the TmLRBT had a shorter irrigation time. Compared with conventional TURBT, the TmLRBT is more feasible for NMIBC.
Notably, thulium laser is not the only laser used in the resection of bladder cancers. Studies had suggested the safety and efficacy of different lasers to treat NMIBC including holmium laser (6), green-light lithium triborate laser (28), and potassium-titanyl-phosphate laser (29). Thulum laser has a wavelength of 2 um, which is nearing the absorption peak of water, therefore it has the most efficient vaporization (30). Another advantage of thulium laser is its shallowest penetration depth compared to holmium and green-light laser (31), which allows more accurate resection and might reduce the risk of bladder perforation.
This present study has several limitations. The limited sample size is the main drawback of this study. As BCG immunotherapy was not widely used in China until recent years, most patients received maintain chemotherapy such as gemcitabine and epirubicin instead of BCG therapy in the past. Also, the retrospective nature of this study might bring potential bias. For example, in our study, we included these patients who received BCG therapy after surgery, which resulted in a significantly higher proportion of patients with pathologic high grades. The significant oncological outcomes alert us to conduct subgroup analysis in future prospective research to assess the efficacy of TmLRBT. The selection bias during the therapy determination should also be noted. The tumor characteristics could affect the therapy choosing. For example, the TURBT could be often used when handling large size tumors, which could be reflected in the imbalanced tumor size in Table 1. Also, the surgeon's preference could also affect the final resection strategy. Besides, as a retrospective study, all cases were collected from the clinical practice. The clinicians managing post-operative care were aware of the surgical methods of each patient. The postoperative parameters such as catheterization and irrigation duration could be biased.
In summary, our results suggested that TmLRBT is safer than conventional TURBT with fewer perioperative complications. Besides, TmLRBT could offer better cancer control, therefore might be a superior option for NMIBC patients with intermediate and high recurrence risk. The findings of our study should be ascertained in a further prospective study with larger sample size and longer follow-up.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by Institutional Review Board of the Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (Grant Number: TJ-IRB20210106). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
ZL and GL wrote this manuscript. YZ, GS, WO, SheW, and HX collected the data. GL analyzed the data. ZW, WG, XY, ZH, and ZC read and edited the manuscript. ShaW and HL designed the study. All authors approved the submitted version.
This work is supported by the Natural Science Fund of Hubei Province (Grant Number: 2018CFB459, Recipient: HL). The funding sources had no role in the design and conduct of the study, collection, management, analysis, and interpretation of the data, and preparation, review, or approval of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2021.759487/full#supplementary-material
Figure S1. Diagram for the BCG intravesical therapy schedule.
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2018) 68:394–424 doi: 10.3322/caac.21492
2. Cumberbatch MGK, Jubber I, Black PC, Esperto F, Figueroa JD, Kamat AM, et al. Epidemiology of bladder cancer: a systematic review and contemporary update of risk factors in 2018. Eur Urol. (2018) 74:784–95. doi: 10.1016/j.eururo.2018.09.001
3. Babjuk M, Burger M, Compérat EM, Gontero P, Mostafid AH, Palou J, et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and carcinoma in situ)-2019 Update. Eur Urol. (2019) 76:639–57. doi: 10.1016/j.eururo.2019.08.016
4. Chang SS, Boorjian SA, Chou R, Clark PE, Daneshmand S, Konety BR, et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO Guideline. J Urol. (2016) 196:1021–9. doi: 10.1016/j.juro.2016.06.049
5. Kim LHC, Patel MI. Transurethral resection of bladder tumour (TURBT). Transl Androl Urol. (2020) 9:3056–72. doi: 10.21037/tau.2019.09.38
6. Li C, Gao L, Zhang J, Yang X, Liu C. The effect of holmium laser resection versus standard transurethral resection on non-muscle-invasive bladder cancer: a systematic review and meta-analysis. Lasers Med Sci. (2020) 35:1025–34. doi: 10.1007/s10103-020-02972-w
7. Long G, Zhang Y, Sun G, Ouyang W, Liu Z, Li H. Safety and efficacy of thulium laser resection of bladder tumors versus transurethral resection of bladder tumors: a systematic review and meta-analysis. Lasers Med Sci. (2021) 18:1–0. doi: 10.1007/s10103-021-03272-7
8. Sylvester RJ, van der Meijden AP, Witjes JA, Kurth K. Bacillus calmette-guerin versus chemotherapy for the intravesical treatment of patients with carcinoma in situ of the bladder: a meta-analysis of the published results of randomized clinical trials. J Urol. (2005) 174:86–91; discussion 91–2 doi: 10.1097/01.ju.0000162059.64886.1c
9. Sylvester RJ, Brausi MA, Kirkels WJ, Hoeltl W, Calais Da Silva F, Powell PH, et al. Long-term efficacy results of EORTC genito-urinary group randomized phase 3 study 30911 comparing intravesical instillations of epirubicin, bacillus Calmette-Guérin, and bacillus Calmette-Guérin plus isoniazid in patients with intermediate- and high-risk stage Ta T1 urothelial carcinoma of the bladder. Eur Urol. (2010) 57:766–73. doi: 10.1016/j.eururo.2009.12.024
10. Malmström PU, Sylvester RJ, Crawford DE, Friedrich M, Krege S, Rintala E, et al. An individual patient data meta-analysis of the long-term outcome of randomised studies comparing intravesical mitomycin C versus bacillus Calmette-Guérin for non-muscle-invasive bladder cancer. Eur Urol. (2009) 56:247–56. doi: 10.1016/j.eururo.2009.04.038
11. Babjuk M, Böhle A, Burger M, Capoun O, Cohen D, Compérat EM, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2016. Eur Urol. (2017) 71:447–61. doi: 10.1016/j.eururo.2016.05.041
12. Liu Z, Zhang Y, Sun G, Ouyang W, Wang S, Xu H, et al. Comparison of thulium laser resection of bladder tumors and conventional transurethral resection of bladder tumors for non-muscle-invasive bladder cancer. Urol Int. (2021) 30:1–6 doi: 10.1159/000514042
13. Chen X, Liao J, Chen L, Qiu S, Mo C, Mao X, et al. En bloc transurethral resection with 2-micron continuous-wave laser for primary non-muscle-invasive bladder cancer: a randomized controlled trial. World J Urol. (2015) 33:989–95. doi: 10.1007/s00345-014-1342-1
14. Huang JH, Hu YY, Liu M, Wang GC, Peng B, Yao XD. Comparative study of 2 um laser versus holmium laser for the resection of non-muscle invasive bladder cancer. Int J Clin Exp Med. (2016) 9:23618–23.
15. Liu H, Wu J, Xue S, Zhang Q, Ruan Y, Sun X, et al. Comparison of the safety and efficacy of conventional monopolar and 2-micron laser transurethral resection in the management of multiple nonmuscle-invasive bladder cancer. J Int Med Res. (2013) 41:984–92. doi: 10.1177/0300060513477001
16. Xu H, Ma J, Chen Z, Yang J, Yuan H, Wang T, et al. Safety and efficacy of en bloc transurethral resection with 19 microm vela laser for treatment of non-muscle-invasive bladder. Cancer Urol. (2018) 113:246–50. doi: 10.1016/j.urology.2017.11.030
17. Zhang XR, Feng C, Zhu JM, Gu BJ, Guo H, et al. Two micrometer continuous-wave thulium laser treating primary non-muscle-invasive bladder cancer: is it feasible? A randomized prospective study. Photomed Laser Surg. (2015) 33:517–23. doi: 10.1089/pho.2015.3913
18. Zhong C, Guo S, Tang Y, Xia S. Clinical observation on 2 micron laser for non-muscle-invasive bladder tumor treatment: single-center experience. World J Urol. (2010) 28:157–61. doi: 10.1007/s00345-010-0532-8
19. Hafner C, Knuechel R, Zanardo L, Dietmaier W, Blaszyk H, Cheville J, et al. Evidence for oligoclonality and tumor spread by intraluminal seeding in multifocal urothelial carcinomas of the upper and lower urinary tract. Oncogene. (2001) 20:4910–5. doi: 10.1038/sj.onc.1204671
20. Pode D, Alon Y, Horowitz AT, Vlodavsky I, Biran S. The mechanism of human bladder tumor implantation in an in vitro model. J Urol. (1986) 136:482–6. doi: 10.1016/S0022-5347(17)44926-3
21. Soloway MS, Masters S. Urothelial susceptibility to tumor cell implantation: influence of cauterization. Cancer. (1980) 46:1158–63. doi: 10.1002/1097-0142(19800901)46:5<1158::aid-cncr2820460514>3.0.co;2-e.
22. Soloway MS, Nissenkorn I, McCallum L. Urothelial susceptibility to tumor cell implantation: comparison of cauterization with N-methyl-N-nitrosourea. Urology. (1983) 21:159–61. doi: 10.1016/0090-4295(83)90013-4
23. Teoh JY, MacLennan S, Chan VW, Miki J, Lee HY, Chiong E, et al. An international collaborative consensus statement on en bloc resection of bladder tumour incorporating two systematic reviews, a two-round delphi survey, and a consensus meeting. Eur Urol. (2020) 78:546–69. doi: 10.1016/j.eururo.2020.04.059
24. Zhao C, Tang K, Yang H, Xia D, Chen Z. Bipolar versus monopolar transurethral resection of nonmuscle-invasive bladder cancer: a meta-analysis. J Endourol. (2016) 30:5–12. doi: 10.1089/end.2015.0410
25. Cui Y, Chen H, Liu L, Chen J, Qi L, Zu X. Comparing the efficiency and safety of bipolar and monopolar transurethral resection for non-muscle invasive bladder tumors: a systematic review and meta-analysis. J Laparoendosc Adv Surg Tech A. (2016) 26:196–202. doi: 10.1089/lap.2015.0507
26. Tzelves L, Mourmouris P, Skolarikos A. Does bipolar energy provide any advantage over monopolar surgery in transurethral resection of non-muscle invasive bladder tumors? A systematic review and meta-analysis. World J Urol. (2020) 39:1093–105. doi: 10.1007/s00345-020-03396-5
27. Liang JH, Pan YL, Kang J, Qi J. Influence of irrigation on incision and coagulation of 20-μm continuous-wave laser: an ex vivo study. Surg Laparosc Endosc Percutan Tech. (2012) 22:e122–5. doi: 10.1097/SLE.0b013e318248b69e
28. Chen J, Zhao Y, Wang S, Jin X, Sun P, Zhang L, et al. Green-light laser en bloc resection for primary non-muscle-invasive bladder tumor vs. transurethral electroresection: a prospective, nonrandomized two-center trial with 36-month follow-up. Lasers Surg Med. (2016) 48:859–65. doi: 10.1002/lsm.22565
29. Xu Y, Guan W, Chen W, Xie C, Ouyang Y, Wu Y, et al. Comparing the treatment outcomes of potassium-titanyl-phosphate laser vaporization and transurethral electroresection for primary nonmuscle-invasive bladder cancer: a prospective, randomized study. Lasers Surg Med. (2015) 47:306–11. doi: 10.1002/lsm.22342
30. Jansen ED, van Leeuwen TG, Motamedi M, Borst C, Welch AJ. Temperature dependence of the absorption coefficient of water for midinfrared laser radiation. Lasers Surg Med. (1994) 14:258–68. doi: 10.1002/lsm.1900140308
Keywords: thulium laser, en bloc resection of bladder tumor, non-muscle-invasive bladder cancer, bacillus Calmette-Guérin vaccine, transurethral resection of bladder tumors
Citation: Liu Z, Long G, Zhang Y, Sun G, Ouyang W, Wang S, Xu H, Wang Z, Guan W, Yu X, Hu Z, Chen Z, Wang S and Li H (2021) Thulium Laser Resection of Bladder Tumors vs. Conventional Transurethral Resection of Bladder Tumors for Intermediate and High Risk Non-Muscle-Invasive Bladder Cancer Followed by Intravesical BCG Immunotherapy. Front. Surg. 8:759487. doi: 10.3389/fsurg.2021.759487
Received: 16 August 2021; Accepted: 18 October 2021;
Published: 08 November 2021.
Edited by:
Jeremy Teoh, The Chinese University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Bryan Kwun-Chung Cheng, United Christian Hospital, Hong Kong SAR, ChinaCopyright © 2021 Liu, Long, Zhang, Sun, Ouyang, Wang, Xu, Wang, Guan, Yu, Hu, Chen, Wang and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shaogang Wang, c2d3YW5ndGptQDE2My5jb20=; Heng Li, bGloZW5ndGptdUAxNjMuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.