 Zhongping Lang1†Yue Wu1†Minwei Bao2*
Zhongping Lang1†Yue Wu1†Minwei Bao2*- 1Department of Laboratory Medicine, Shanghai Pulmonary Hospital Affiliated to Tongji University, Shanghai, China
- 2Department of Thoracic Surgery, Shanghai Pulmonary Hospital Affiliated to Tongji University, Shanghai, China
Objective: Postoperative anemia is a common complication after a major surgery. Our study aims to identify factors that are associated with higher risk of developing postoperative anemia after thoracic surgery.
Methods: We conducted a retrospective study of 465 patients who underwent pulmonary surgery in 2017 in Shanghai Pulmonary Hospital, China. Of them, 191 patients underwent standard open thoracotomy (OT), and 274 patients underwent video-assisted thoracic surgery (VATS). A total of 350 patients were diagnosed with postoperative anemia, and 115 patients did not have anemia. Multiple logistic regression was used to compute odds ratios for predicting preoperative anemia.
Results: Postoperative anemia was associated with significantly lower weight (p < 0.001) and height (p = 0.022) of the patients, as well as higher prothrombin time (PT), and international normalized ratio (INR) (p = 0.012). Open thoracotomy resulted in a 1.2-fold increase in the incidence of postoperative anemia compared to VATS (p = 0.002). Multiple logistic regression analysis identified INR [OR (95% CI) 24.46 (2.05–292.27; p = 0.012] and surgical approach [OR (95% CI) 0.48 (0.31–0.74); p < 0.001] as predictors of postoperative anemia and postoperative drop in hemoglobin (Hb).
Conclusion: Postoperative coagulation status and surgical approach are statistically significant predictors of postoperative anemia in patients undergoing thoracic surgery. International normalized ratio and surgical approach are specifically associated with Hb drop immediately after the surgery.
Introduction
Postoperative anemia is a common complication after a major surgery, and can be present in as high as 80–90% of surgical patients (1, 2). It may have deleterious effects on patients' health, and is associated with prolonged hospitalization, an increased rate of postoperative complications (especially infections), and overall reduced survival (3).
Numerous studies show that preoperative anemia, perioperative blood loss, and postoperative blunted erythropoiesis are the main contributing factors to postoperative anemia and increased transfusion need after major surgery (4). Other risk factors include low preoperative hemoglobin (Hb), female sex, age, perioperative coagulopathy, lower body surface area (5–8). Type of surgery performed also shows correlation with the rates of postoperative anemia after major operation (4). As a minimal invasive operation, video-assisted thoracic surgery (VATS) has been more and more widely used for the diagnosis and management of pathologies in the thoracic cavity due to improved wound infection rates, decreased chance of wound dehiscence, and reduced recovery times compared with open thoracotomy (OT) (9). However, VATS may potentially results in significant perioperative blood loss due to the procedure's proximity to large vessels (10, 11), that may potentially lead to postoperative anemia. Nevertheless, there is still not enough data on the possible predictors of anemia in patients after major surgeries. Identifying these risk factors will allow clinicians to specifically target patients who may require specific attention postoperatively or after discharge. The goal of this study is to identify risk factors that may predict postoperative anemia in patients, undergoing VATS or OT surgeries.
Methods
The current retrospective study was conducted at Shanghai Pulmonary Hospital, China. Medical data of 465 patients that underwent pulmonary surgery in the year 2017 for benign or malignant conditions was analyzed. Pulmonary resection surgeries included 260 lobectomies, 45 pneumoectomies, 40 wedges, 110 segmentomies, and 10 lung transplants.
This study was approved by the ethics Tongji University Shanghai Pulmonary Hospital (No. K18-175). The data was routinely collected for all the patients, and included demographic, clinical and operational variables. Blood tests were done before and after surgery to measure Hb levels, prothrombin time (PT), international normalized ratio (INR), and activated partial thromboplastin time. Postoperative anemia was defined as a blood concentration of Hb <130g/L among men and <120g/L among women and was based on the WHO definition of anemia (12), and patients were stratified into two groups, patients with (n = 315) or without (n = 150) postoperative anemia. Postoperative Hb drop (g/L) was calculated based on the preoperative value.
Surgery was done under general anesthesia (GA) followed by intubation using a double lumen endotracheal tube in order to support lung ventilation. Patients, undergoing VATS (n = 274), were placed in the full lateral decubitus position and a thoracoscope was introduced through the 6th or 7th intercostal space on the mid-axillary line using a trocar. A 3–4 cm long utility incision was made through the 4th or 5th intercostal space on the anterior axillary line.
In cases (n = 191) where lesions invaded important blood vessels and structures, and minimally invasive surgery could not guarantee the surgical schedule, the surgeon opted to perform OT. The procedure included posterolateral thoracotomy accompanied by division of the latissimus dorsi and serratus anterior muscles.
Postoperative fluid management for all patient was 500–800 ml per day.
Postoperative anticoagulation therapy included enoxaparin sodium and heparin sodium injections and aspirin administration based on the instructions of the treating physician.
Statistical Analysis
Categorical and binary variables were presented as counts and % of total and comparisons between cases with and cases without postoperative anemia were made using chi-square tests. Continuous variables were presented as mean and ± standard deviation (SD) and comparisons were made between cases with and cases without postoperative anemia using two-tailed independent samples t-tests. Demographic, clinical, and operative variables that were significant were included as independent variables in regression models for predicting postoperative. Independent variables were tested for multicollinearity using variance inflation factor. Multiple logistic regression was used to compute odds ratios for predicting preoperative anemia. Paired samples t-tests were performed within each independent variable to compare preoperative vs. postoperative concentrations of Hb. Relative change between preoperative and postoperative Hb was calculated as [(postoperative hemoglobin/preoperative hemoglobin – 1) × 100%]. For all tests, p-values < 0.05 were considered statistically significant.
Results
Demographic characteristics of 465 patients that underwent pulmonary surgery and were included in the study are summarized in Table 1. Of them, 315 patients were diagnosed with postoperative anemia, and 150 had no postoperative anemia. The average age of study participants, mean (SD), was 60.14 (11.6), with no statistically significant difference between two groups.
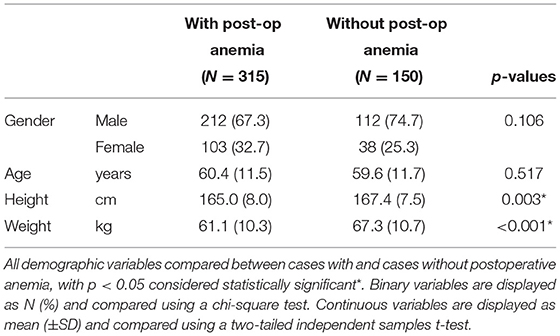
Table 1. Comparison of demographic variables between cases with and cases without postoperative anemia.
The average height and weight were significantly lower in patients who were diagnosed with postoperative anemia. The average weight of patients with anemia was 61.7 (10.3) vs. 67.3 (10.7) kg in the non-anemic group (p < 0.001), and the average height of postoperative and normal groups was 165.1 (8.0) and 166.8 (7.6) cm, respectively (p = 0.022).
Clinical variables of the study cohort are summarized in Table 2. Preoperative Hb was markedly lower in the postoperative anemia group [124.4 (17.1) vs. 142.9 (13.0), p < 0.001], which correlated with lower postoperative Hb [107.8 (14.9) vs. 136.5 (9.6) in the group of patients without anemia, p < 0.001]. Higher PT, and INR were slightly but statistically significantly associated with postoperative anemia (p = 0.012) (Table 2).
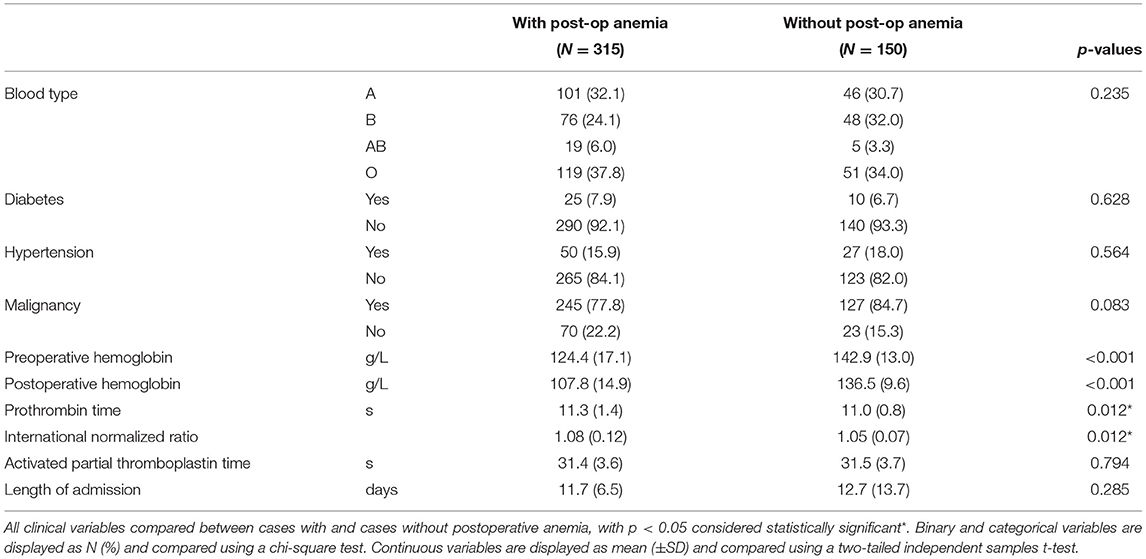
Table 2. Comparison of clinical variables between cases with and cases without postoperative anemia.
Operative variables of the patients are summarized in Table 3. Surgical approach was significantly associated with postoperative anemia. Open thoracotomy was associated with a 1.2-fold increase in the incidence of postoperative anemia compared to VATS (p = 0.002), and with 1.45-fold increase in the units of transfused blood required (p < 0.001). Postoperative anticoagulant use was strongly associated with lower incidence of postoperative anemia. Sixty-eight percent of patients without anemia received postoperative anticoagulants, as compared to only 57.1% in the postoperative anemia group (p = 0.025).
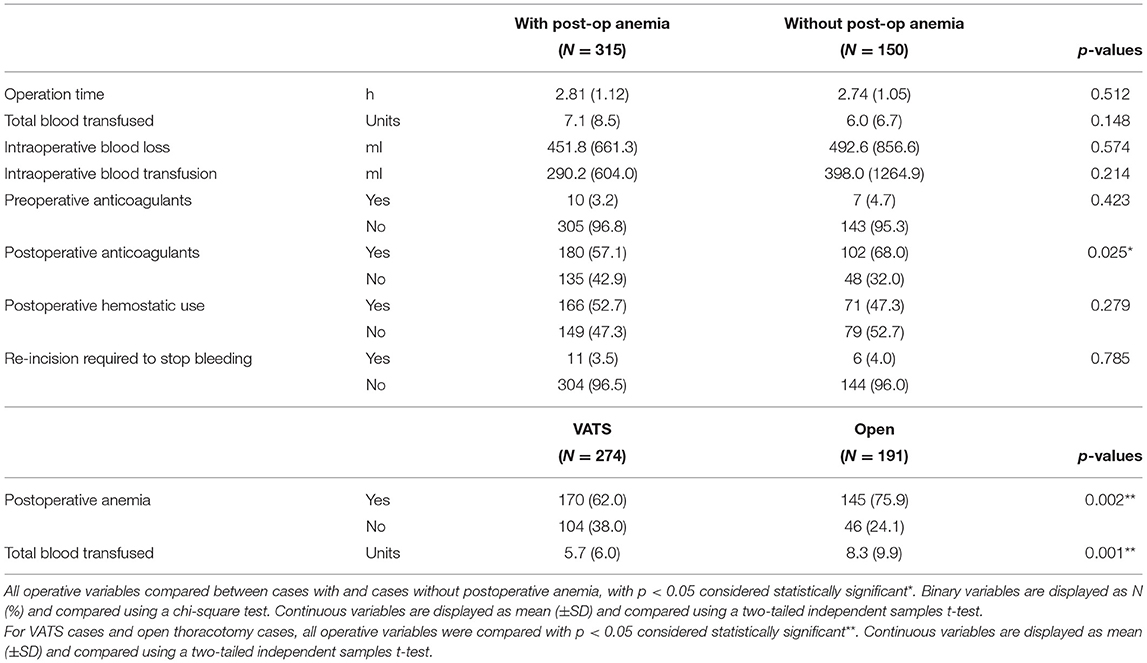
Table 3. Comparison of operative variables between cases with and cases without postoperative anemia.
We next performed regression analysis to identify factors that have a significant association with postoperative anemia (summarized in Table 4).
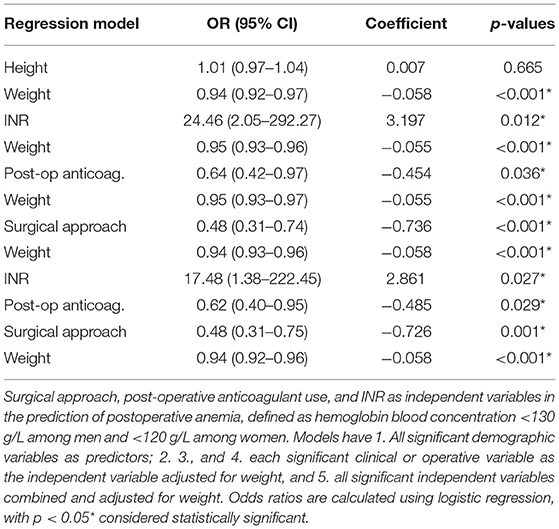
Table 4. Prediction of postoperative anemia from clinical and operative variables.
When combined in a model, out of two demographic variables that were significantly associated with postoperative anemia, only weight remained significant and was used as an independent factor. Our analysis shows that INR [OR (95% CI) 24.46 (2.05–292.27; p = 0.012], and surgical approach [OR (95% CI) 0.48 (0.31–0.74); p < 0.001] remain statistically significant as predictors of postoperative anemia even when adjusted for weight (Table 4).
We next looked at the influence of the factors, significantly associated with postoperative anemia, on the postoperative changes in Hb levels (rather than just risk of low Hb, i.e., anemia). As summarized in Table 5, INR and surgical strategy were significantly associated with the observed drop in Hb (p < 0.001).
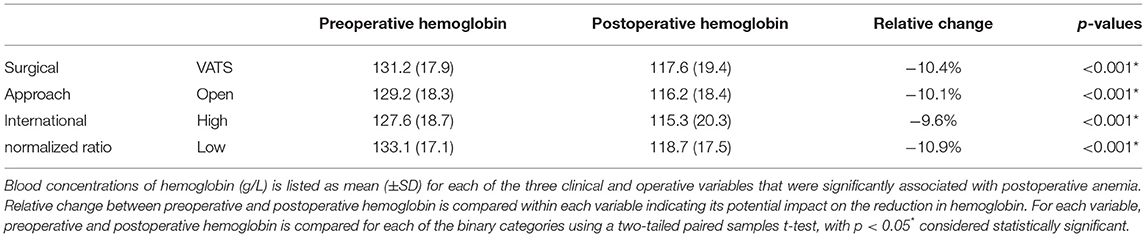
Table 5. Comparison of relative change in preoperative and postoperative hemoglobin among clinical and operative variables.
Discussion
The data on the possible adverse effects of postoperative anemia on the recovery of surgical patients is limited. Generally, it is associated with worse morbidity- and mortality-related outcomes, and increased risks of readmission (4). Although multifactorial in origin, preoperative anemia, perioperative blood loss (surgical bleeding, coagulopathy, phlebotomies, etc.), and postoperative blunted erythropoiesis are the main contributing factors to postoperative anemia after major surgery.
The current study shows that postoperative coagulation profile and surgical approach are statistically significant as predictors of postoperative anemia in patients that underwent pulmonary surgery.
We found that lower weight and height correlated with higher incidence of postoperative anemia, with an average difference of 6.2 kg and 1.6 cm difference between patients, diagnosed with postoperative anemia, and a normal cohort. These results are in agreement with the previous studies that showed a significant association between anemia and BMI, and that smaller body surface area is a risk factor for the development of postoperative anemia and increased transfusion needs (13). When combined in a model where height and weight adjust for each other, only weight remained a significant risk factor for postoperative anemia.
Prior studies have reported that higher levels of anticoagulation may be considered as an independent risk factor of increased incidence of bleeding (14–17) in patients, treated with anticoagulants. Although INR of patients in both groups of our study was within a normal range, postoperative anemia was associated with slightly but significantly increased INR. Interestingly, we showed that postoperative anemia was more prevalent in the group that did not receive anticoagulant treatment after surgery. A possible explanation for these results may be that anticoagulants are less frequently prescribed for patients diagnosed with anemia to lower the risk of further bleeding.
Our study showed that OT is associated with a significantly higher risk of postoperative anemia than VATS. The current evidence in support of VATS over conventional OT is mainly based on observational non-randomized studies, national database analyses and institutional reports (18, 19). Studies in lung carcinoma patients showed that VATS was associated with a shorter duration of chest intubation, shorter hospitalization times, and overall improved survival (20). However, data is lacking on the correlation between surgery type and postoperative complications, such as bleeding and subsequent need for blood transfusion following bleeding. In our study, surgical approach had the most significant association with postoperative anemia and remained the strongest factor when combined in a regression model with INR and anticoagulant use [OR (95% CI) 0.48 (0.31–0.75); p = 0.001]. Open thoracotomy was also associated with 1.45-fold increase in the required units of transfused blood in surgical patients. Studies show that blood transfusion independently increases the risk of acute kidney injury in patients after cardiopulmonary surgery (21, 22). The increased requirement for blood transfusion in the OT cohort in our study may, therefore, suggest potentially increased postoperative morbidity.
Another variable, assessed in our study, was postoperative Hb drop immediately after surgery. Previous studies reported that the magnitude of postoperative downward Hb drift depends on the type of surgical procedure, as well as coagulation status of surgical patients (23, 24). Surgeries associated with greater intraoperative blood loss and postoperative bleeding are associated with a greater drop in Hb. In our study, coagulation status of patients (higher INR) had the greatest influence on reducing the postoperative drop in Hb (−9.6 vs. −10.9%). There was also a small, but still statistically significant association of VATS as a surgery method with a bigger postoperative Hb drop. Previous studies showed that the risk of injury to the pulmonary vessels leading to greater blood loss is higher in VATS compared to the standard OT, and is highly dependent on the skills of the operating surgeon (10, 25). We may speculate that this factor may contribute to the discrepancy between the overall lower incidence of postoperative anemia in VATS patients and larger initial postoperative Hb drop.
This study has some limitations. Since the study is retrospective, causality may be difficult to establish. Therefore, there is a risk that variables that were not assessed in the study may have affected the outcome of the analysis. Lung cancer staging for both groups was unavailable for analysis, and therefore, its potential impact on the type of surgery and postoperative anemia was not evaluated. There was no information on the type of chemotherapy, received by the patients prior to surgery, which may potentially affect the rates of preoperative and postoperative anemia. Additionally, OT in our study was performed on more difficult and complexed cases than VATS, which may introduce additional risk of biased outcome analysis. Randomized controlled studies are needed to further evaluate the effect of surgery type and coagulation status of patients on the risk of postoperative anemia.
Conclusion
The current study shows that postoperative coagulation status of the patients and surgical approach are statistically significant predictors of postoperative anemia in patients undergoing pulmonary surgery. International normalized ratio and surgical approach correlate with Hb drop immediately after the surgery. These findings may help to develop more effective guidelines for efficient patient blood management that will reduce the need for blood transfusion, healthcare costs and morbidity and mortality.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
ZL and YW conceived and designed the study. YW and MB were involved in literature search and data collection. ZL and YW analyzed the data. ZL and MB wrote the paper. YW reviewed and edited the manuscript. All authors read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Shander A, Knight K, Thurer R, Adamson J, Spence R. Prevalence and outcomes of anemia in surgery: a systematic review of the literature. Am J Med. (2004) 116(Suppl. 7A):58S–69S. doi: 10.1016/j.amjmed.2003.12.013
2. Spahn DR. Anemia and patient blood management in hip and knee surgery: a systematic review of the literature. Anesthesiology. (2010) 113:482–95. doi: 10.1097/ALN.0b013e3181e08e97
3. Franchini M, Muñoz M. Towards the implementation of patient blood management across Europe. Blood Transfus Trasfus Sangue. (2017) 15:292–3. doi: 10.2450/2017.0078-17
4. Muñoz M, Acheson AG, Bisbe E, Butcher A, Gómez-Ramírez S, Khalafallah AA, et al. An international consensus statement on the management of postoperative anaemia after major surgical procedures. Anaesthesia. (2018) 73:1418–31. doi: 10.1111/anae.14358
5. Hayn D, Kreiner K, Kastner P, Breznik N, Hofmann A, Gombotz H, et al. Data driven methods for predicting blood transfusion needs in elective surgery. Stud Health Technol Inform. (2016) 223:9–16.
6. Woodman R, Ferrucci L, Guralnik J. Anemia in older adults. Curr Opin Hematol. (2005) 12:123–8. doi: 10.1097/01.moh.0000154030.13020.85
7. Gómez Ramírez S, Remacha Sevilla ÁF, Muñoz Gómez M. Anaemia in the elderly. Med Clin (Barc). (2017) 149:496–503. doi: 10.1016/j.medcli.2017.06.025
8. Najafi M, Faraoni D. Updates on coagulation management in cardiac surgery. J Tehran Heart Cent. (2014) 9:99–103.
9. Flores RM, Park BJ, Dycoco J, Aronova A, Hirth Y, Rizk NP, et al. Lobectomy by video-assisted thoracic surgery (VATS) versus thoracotomy for lung cancer. J Thorac Cardiovasc Surg. (2009) 138:11–8. doi: 10.1016/j.jtcvs.2009.03.030
10. Kawachi R, Tsukada H, Nakazato Y, Takei H, Koshi-ishi Y, Goya T. Morbidity in video-assisted thoracoscopic lobectomy for clinical stage I non-small cell lung cancer: is VATS lobectomy really safe? Thorac Cardiovasc Surg. (2009) 57:156–9. doi: 10.1055/s-2008-1039267
11. Keyes B, Giles E. Massive intraoperative blood loss secondary to pulmonary artery injury during a video-assisted thorascopic surgery: the importance of protocols and preparedness. Cureus. (2017) 9:e1357. doi: 10.7759/cureus.1357
12. Peña-Rosas JP. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information System. Geneva: World Health Organization. WHO/NMH/NHD/MNM/11.1 (2011). Available online at: https://www.academia.edu/4215770/WHO_Haemoglobin_concentrations_for_the_diagnosis_of_anaemia_and_assessment_of_severity_Vitamin_and_Mineral_Nutrition_Information_System_Geneva_World_Health_Organization_2011_WHO_NMH_NHD_MNM_11_1_ (accessed August 18, 2021).
13. Kim T-G, Lee S-H, Shin S, Cho J-H, Kim K-W, Ha I-H. Sex-related associations among anemia, body mass index, and kidney function in Koreans: a cross-sectional study with propensity analysis. Medicine. (2021) 100:e23990. doi: 10.1097/MD.0000000000023990
14. Beyth RJ, Landefeld CS. Anticoagulants in older patients. A safety perspective. Drugs Aging. (1995) 6:45–54. doi: 10.2165/00002512-199506010-00004
15. Levine MN, Raskob G, Beyth RJ, Kearon C, Schulman S. Hemorrhagic complications of anticoagulant treatment: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. (2004) 126:287S–310S. doi: 10.1378/chest.126.3_suppl.287S
16. Palareti G, Leali N, Coccheri S, Poggi M, Manotti C, D'Angelo A, et al. Bleeding complications of oral anticoagulant treatment: an inception-cohort, prospective collaborative study (ISCOAT) Italian Study on Complications of Oral Anticoagulant Therapy. Lancet Lond Engl. (1996) 348:423–8. doi: 10.1016/s0140-6736(96)01109-9
17. Steffensen FH, Kristensen K, Ejlersen E, Dahlerup JF, Sørensen HT. Major haemorrhagic complications during oral anticoagulant therapy in a Danish population-based cohort. J Intern Med. (1997) 242:497–503. doi: 10.1111/j.1365-2796.1997.tb00023.x
18. Grogan EL, Jones DR. VATS lobectomy is better than open thoracotomy: what is the evidence for short-term outcomes? Thorac Surg Clin. (2008) 18:249–58. doi: 10.1016/j.thorsurg.2008.04.007
19. Papiashvilli M, Sasson L, Azzam S, Hayat H, Schreiber L, Ezri T, et al. Video-assisted thoracic surgery lobectomy versus lobectomy by thoracotomy for lung cancer: pilot study. Innov Phila Pa. (2013) 8:6–11. doi: 10.1097/IMI.0b013e31828d5f15
20. Whitson BA, Groth SS, Duval SJ, Swanson SJ, Maddaus MA. Surgery for early-stage non-small cell lung cancer: a systematic review of the video-assisted thoracoscopic surgery versus thoracotomy approaches to lobectomy. Ann Thorac Surg. (2008) 86:2008–16; discussion 2016–8. doi: 10.1016/j.athoracsur.2008.07.009
21. Karkouti K. Transfusion and risk of acute kidney injury in cardiac surgery. Br J Anaesth. (2012) 109(Suppl 1):i29–38. doi: 10.1093/bja/aes422
22. Choi YJ, Kim S-O, Sim JH, Hahm K-D. Postoperative anemia is associated with acute kidney injury in patients undergoing total hip replacement arthroplasty: a retrospective study. Anesth Analg. (2016) 122:1923–8. doi: 10.1213/ANE.0000000000001003
23. Grant MC, Whitman GJ, Savage WJ, Ness PM, Frank SM. Clinical predictors of postoperative hemoglobin drift. Transfusion (Paris). (2014) 54:1460–8. doi: 10.1111/trf.12491
24. George TJ, Beaty CA, Kilic A, Haggerty KA, Frank SM, Savage WJ, et al. Hemoglobin drift after cardiac surgery. Ann Thorac Surg. (2012) 94:703–9. doi: 10.1016/j.athoracsur.2012.03.038
Keywords: postoperative anemia, thoracic surgery, open thoracotomy, hemoglobin, prothrombin
Citation: Lang Z, Wu Y and Bao M (2021) Coagulation Status and Surgical Approach as Predictors of Postoperative Anemia in Patients Undergoing Thoracic Surgery: A Retrospective Study. Front. Surg. 8:744810. doi: 10.3389/fsurg.2021.744810
Received: 21 July 2021; Accepted: 26 August 2021;
Published: 21 September 2021.
Edited by:
Hasan Fevzi Batirel, Marmara University, TurkeyReviewed by:
Michel Gonzalez, Centre Hospitalier Universitaire Vaudois (CHUV), SwitzerlandAyten Saraçoglu, Marmara University, Turkey
Copyright © 2021 Lang, Wu and Bao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Minwei Bao, MTM4MTgwODkwOTAmI3gwMDA0MDsxMzkuY29t
†These authors have contributed equally to this work